Title: Insomnia; and Other Disorders of Sleep
Author: Henry M. Lyman
Release date: August 7, 2013 [eBook #43415]
Language: English
Credits: Produced by The Online Distributed Proofreading Team at
http://www.pgdp.net (This file was produced from images
generously made available by The Internet Archive.)
AND OTHER
Disorders of Sleep.
BY
HENRY M. LYMAN, A.M., M.D.,
Professor of Physiology, and of Diseases of the Nervous System, in Rush Medical
College; Professor of Theory and Practice of Medicine, in the
Woman’s Medical College; and Physician to the
Presbyterian Hospital, Chicago, Ill.
CHICAGO:
W. T. KEENER,
96 WASHINGTON STREET.
1885.
COPYRIGHT, 1885.
R. R. DONNELLEY & SONS, PRINTERS, CHICAGO.
| Tired Nature’s sweet restorer, balmy sleep. —Young. |
The regularly recurring incidence of natural sleep forms one of the most important subjects for physiological investigation. Were it an event of rare occurrence, it would excite a degree of astonishment and alarm equal to the agitation now experienced by the spectator of an ordinary attack of syncope or of epileptic convulsion. But, so completely does the recurrence of sleep harmonize with all the other facts of life that we are as indifferent to its nature as we are to every other healthy function of the body. It is only when the mind has undertaken a critical observation of the bodily and mental changes which accompany and condition the phenomenon that we begin to comprehend its wonderful character. Ushered in by a waning activity of body and mind that no effort of the will can long resist, nothing could more forcibly suggest the idea of approaching dissolution if, from the very earliest period of unconscious infancy, we had not been accustomed to the dominion of this imperious necessity. The remarkable likeness between the fading of consciousness in sleep and its extinction[Pg iv] in death has, in all ages and among all people, arrested the attention of poets and philosophers of every degree.
Soft repose,
A living semblance of the grave,
sang old Thomas Miller; and, describing, in Milton’s stately verse, the close of his first day in the garden of Eden, Adam says:
Gentle sleep
First found me, and with soft oppression seized
My drowsy sense, untroubled, though I thought
I then was passing to my former state
Insensible, and forthwith to dissolve.
How wonderful is death,
Death and his brother, Sleep!
exclaims Shelley, echoing the marvellous strains that have come down to us from the days of Homer and Hesiod. In that venerable literature Sleep and Death are represented as twin brothers, sons of Night; dwelling in the lower world of spirits, whence they come forth to perform the will of the Olympian Gods.
The prosaic genius of our scientific generation no longer tolerates such lively exercise of the imagination. The splendid anthropomorphism of the Hebrew poet, looking out upon the silent night, and cheering his soul with the sonorous exclamation,
Behold, he that keepeth Israel
Shall neither slumber nor sleep
·····
For so he giveth his beloved sleep,
has become a mere memory of childhood. Wordsworth[Pg v] understood the full significance of this change when he wrote:
There was a time when meadow, grove, and stream,
The earth, and every common sight,
To me did seem
Apparelled in celestial light,
The glory and the freshness of a dream.
It is not now as it has been of yore;
Turn whereso’er I may,
By night or day,
The things which I have seen I now can see no more!
... I know, where’er I go,
That there has passed away a glory from the earth.
If, however, despite the loss of much that was beautiful and attractive in the myths of antiquity, we take advantage of the
Years that bring the philosophic mind,
we shall surely find in the scientific investigation of sleep enough to awaken “thoughts too deep for” words.
THE NATURE AND CAUSE OF SLEEP.
Definition of sleep — The invasion of sleep — The hypnagogic state — Depth and duration of sleep — Diagrammatic illustration of the phases of sleep — Modifications of physiological functions produced by sleep — Effect of sleep upon the processes of respiration, circulation, calorification, secretion, and nutrition — Consequences of the progressive invasion of the nervous system by sleep — Effect upon the organs of special sense — Effects observed in the muscular apparatus of the body — Condition of intellectual functions during the invasion of sleep — Does the mind ever sleep? — Arguments adduced by Sir William Hamilton and others to prove the continued activity of the mind during the sleep of the brain — Reasons for supposing that the mind may sleep — Variability of the depth of sleep — Experiments of Kohlshüter to estimate the degree of variation — Alternation of day and night considered as a cause of sleep — Diminution of sensation a cause of sleep — Illustrative observation by Strümpell — Fatigue a cause of sleep — Hypothesis of Obersteiner regarding the cause of sleep — Hypothesis of Pflüger — Production of artificial sleep by impregnation of the brain with narcotic substances — Analogous production of natural sleep by accumulation of cerebral waste-products — Observations regarding the duration of sensory impressions requisite for the excitement of conscious perception — Difference between syncope and sleep — Observations of Mosso regarding the state of the cerebral circulation during sleep — Cause of the change in the cerebral circulation during sleep — Molecular conditions necessary for the production of sleep — Somnolence — Sleeping Dropsy, or Maladie du Sommeil — Coma — Lethargy — Apparent death — Lucid lethargy. 1
INSOMNIA, OR WAKEFULNESS.
Causes of insomnia — Affections of the organs of special sense — Effects of light — Effect of sound — Impressions upon the organs of smell and taste — Disturbances caused by a high temperature — Atmospheric and electrical disturbances — Effects produced by cold — Hibernation of animals — Disturbances of sleep occasioned by painful sensations — Disorders of the sympathetic nerves — Morbid states of the central nervous organs — Disorders of circulation and nutrition — Hyperæmia of the brain — Anæmia and starvation of the brain — Effects of tea and coffee — Effect of alcohol — Inflammations, degenerations, and tumors affecting the brain — Excitement of the brain by diseased conditions of the blood. 38
REMEDIES FOR INSOMNIA.
Serious consequences of insomnia — Its relation to cerebral diseases — Treatment of insomnia by moderation and control of the cerebral circulation — Remedial agents — Nervous stimulants and nervous sedatives — Heat — Baths — Massage — Electricity — Counter-irritants — Food — Digitalis — Camphor — Musk — Valerian — Cannabis indica — Belladonna — Hyoscyamus — Stramonium — Phosphorus — Acids — Opium — Cold — Alcohol — Paraldehyde — Ether — Chloroform — Chloral — Butylchloral hydrate — Amyl nitrite — Opium and opiates — Bromides — Hops — Gelsemium — Conium. 56
TREATMENT OF INSOMNIA IN PARTICULAR DISEASES.
Insomnia in acute affections of the brain — In insanity — In chronic alcoholism and delirium tremens — In diseases of the heart and blood-vessels — In angina pectoris — In diseases of the respiratory organs — In asthma — In renal diseases — In diseases of the liver — In gastro-intestinal diseases — In febrile conditions — In rheumatism and gout — In lithæmia — In syphilis — In disorders of nutrition — During pregnancy and after parturition — In spasmodic diseases — In childhood — In old age. 92
DREAMS.
Physiology of perception and of dreaming — Definition of the act of dreaming — Revery — Production of illusions and hallucinations by drugs and by disease — Effects of hasheesh — Effects of acute disease — Association of ideas — Memory of past sensations — Dreams produced by excitement of the different organs of sense — Persistence of dream-impressions after waking — Experience of M. Baillarger — Of Professor Jessen — Belief of savages in the reality of dreams — Sensory dreams — Intellectual dreams — Repetition of dreams — Incoherence of dreams — Cause of the superior vividness of certain dreams — Duration of dreams — Dreams excited by morbid states of the body — Prophetic dreams — Their causes — Clairvoyant dreams — Hallucinatory dreams — Sir Edmund Hornby’s experience — Hallucinations — Case related by Dr. E. H. Clarke — Revelation through dreams — Revival of memory in dreams. 116
SOMNAMBULISM.
Causes of somnambulism — Physiology of somnambulism — Varieties of the disorder — Maury’s classification — Classification of Ball and Chambard — Diagrammatic representation of their classification — Somnambulic lethargy — Illustrative cases — Somnambulic dreams — Night terrors — Somnolentia or sleep-drunkenness — Sleep-walking — Illustrative cases — Condition of the special senses in somnambulism — Relation of memory to the somnambulic paroxysm — Illustrative cases — Occasional recollection of incidents connected with the somnambulic dream — Resemblances between the somnambulic state and the condition of post-epileptic mania — Somnambulic visions — J. P. Frank’s case — Mesnet’s case — Somnambulic life — Its likeness with the double-consciousness of certain forms of epilepsy — Illustrative cases — General theory of somnambulism. 166
ARTIFICIAL SOMNAMBULISM OR HYPNOTISM.
Antiquity of the phenomena of hypnotism — Modern observations — Physical conditions favorable to the phenomena — Methods of inducing the hypnotic state — Duration of hypnotic sleep — Rudimentary states of hypnotism — Investigations of the Society for Psychical Research — Mind-reading — Physiological explanation of the process — Charcot’s observations on artificial somnambulism — Cataleptic variety of the hypnotic state — Lethargic variety — Somnambulic variety — Hypnotic clairvoyance — Exalted sensibility of the brain in hypnotic states — Susceptibility to suggestions from without — Phenomena of so-called spiritualism — Table-rapping — Planchette — Therapeutical employment of hypnotism — Metaphysical healing. 212
THE NATURE AND CAUSE OF SLEEP.
| Worn out, friend, is every theory, But green the golden tree of life. —Goethe. |
Natural sleep is that condition of physiological repose in which the molecular movements of the brain are no longer fully and clearly projected upon the field of consciousness. This condition is universally observed in all healthy animals; and its recurrence is intimately associated with the diurnal revolution of the earth, and the succession of day and night. The disappearance of daylight is, for the majority of living creatures, the signal for cessation of active life. Though its onset may be for a time delayed by an effort of the will, the need of rest at length overcomes all opposition, and the most untoward circumstances cannot then prevent the access of unconsciousness. The story of the sailor-boy, sleeping on “the high and giddy mast,” is familiar to every one. An officer in the United States Navy has assured me of more than one instance in which men had fallen asleep under his own eyes, oppressed by exhaustion, during the roar of a long continued bombardment. Thus produced, the relation of cause and effect between weariness and sleep becomes very apparent. The refreshing influence of such repose points clearly to the restorative[Pg 2] character of the physiological processes which persist during the suspension of consciousness. It also renders evident the final cause of that periodical interruption of activity which the brain experiences in common with every other living structure.
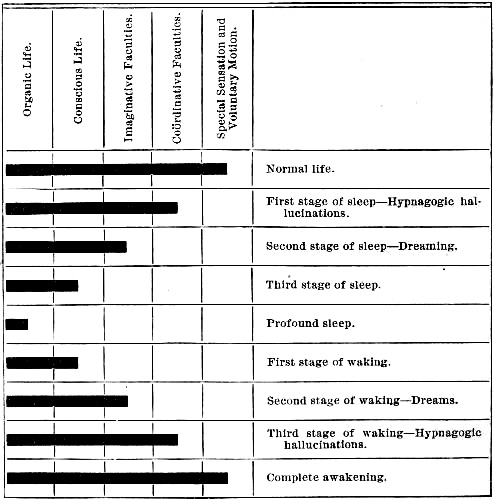
Sleep is usually preceded for some time by a feeling of sleepiness. This sensation, like the analogous sensations of hunger and thirst, represents in some measure the progressive diminution of energy throughout the entire body; but it is chiefly expressive of the failure of cerebral energy. It produces a sense of general heaviness and intellectual dullness; the special senses become less alert, the eyelids droop, numerous groups of muscles experience the spasmodic contraction of yawning, the head drops forward and is recovered with a jerk, the limbs relax, and the whole body tends to assume a position convenient for repose. Every school-boy who has been compelled to pass an evening hour at a dull lecture, under the eye of a martinet monitor, will testify to the suffering which attends any unusual prolongation of this period. But, if the natural course of events be not obstructed, the stage of mere sleepiness is soon passed, and the introductory stage of sleep is entered. This is a state in which the individual is neither awake nor fully asleep. It is known as the hypnagogic state. During this period the phenomena of simple sleepiness become exaggerated to such a degree that the attitude of repose is assumed without effort if the body be permitted to follow the natural inclination of its different members. The eyes close, the other senses become inactive, though the sense of hearing is the most[Pg 3] persistent. Released in considerable measure from the control of the brain, the reflex energy of the spinal cord is at first somewhat exalted. Witness the fibrillary twitching of the muscles, and the convulsive state, which may often be observed during the stage of somnolence after severe fatigue. The uneasy sleeper may even be roused to complete wakefulness by such involuntary movements. But, as sleep becomes more profound, the reflex functions of the cord are also weakened.[1] As the sensory organs retire from action, the intellectual faculties lose their equilibrium. First, the power of volition ceases. Then the logical association of ideas comes to an end. The reasoning faculty disappears, and judgment is suspended. We become, therefore, no longer capable of surprise or astonishment at the vagaries of memory and of imagination, the only faculties that remain in action. To their more or less unfettered activity we owe the presentation in consciousness of those disorderly pictures which, occurring in this stage of imperfect sleep, have been termed hypnagogic hallucinations.[2] During the early moments of this period an observant person may often retain a power of reasoning sufficient to remark the fact of dreaming, and this effort of attention may produce a partial awakening; but, usually, the subsidence of cerebral function is progressive and rapid. The fire of imagination fades, the field of consciousness becomes less and less vividly illuminated, the entire nervous apparatus yields to the advancing tide, and, finally, the dominion of sleep is fully[Pg 4] confirmed. The sleeper knows nothing of the external world, and has lost all consciousness of his own existence. But the duration of profound repose is brief. From the end of the first hour the depth of sleep, at first, rapidly, then, more gradually, subsides. Dreams disturb its tranquility, mental activity increases, the power of volition revives, and, at the end of six or eight hours, the individual is once more awake. The subjoined diagram, borrowed from the Dictionaire Encyclopédique des Sciences Médicales, will facilitate the apprehension of these successive phases in the course of sleep:
[Pg 5]It was formerly believed that during the time of sleep all the processes of assimilation and nutrition throughout the body are increased,—in short, that it is the season of repair for the waste of tissue incurred during the hours of wakeful activity. While it is true that in sleep the expenditure of force is greatly reduced, the more exact researches of modern physiologists indicate a universal reduction in the rate of all the vital processes. The final result, however, is a general renewal of energy, because the aggregate income of the tissues is greater than their outgo during the suspension of conscious activity. The following observations make very apparent the fact of a reduction of physiological activity:
Respiration.—The process of breathing is conducted with greater deliberation during the period of sleep. This reduction is one of the most notable of the circumstances that first attract the attention of the spectator who observes a sleeping person. The average number of respirations per minute, in an adult of twenty-five to thirty years of age, is sixteen. Quetelet remarked[3] that during sleep this number was diminished by about one-fourth. The same fact has been recorded by other observers.[4] Mosso has also noted the fact[5] that there is a change in the type of respiration, the movements during sleep become less diaphragmatic and more largely costal. He furthermore observed that during the waking period the act of inspiration consumed 8-12 of the complete[Pg 6] respiratory phase, but during sleep it was prolonged till it occupied 10-12 of the same cycle. The interval between the end of expiration and the commencement of inspiration was also obliterated by sleep. Notwithstanding this relative increase of inspiratory motion, the quantity of air that passes through the lungs is considerably reduced by reason of the diminished action of the diaphragm. A corresponding reduction of the gaseous exchanges between the blood and the external air has been determined by the experiments of Pettenkofer and Voit, Boussingault, Lewin, and other equally competent observers.[6]
Circulation.—During sleep the heart beats less frequently than during the waking hours. Though a portion of this delay must be attributed to the recumbent position, sleep does still further retard the movement of the heart. My own observations upon children in bed exhibit a difference of twelve to sixteen beats between the pulsations when awake and asleep. According to Trousseau[7] the average number of pulsations observed in a group of thirty children, varying in age from fifteen days to six months, was 140 when awake and 121 when asleep. In another group of twenty-nine children, between the ages of six months and twenty-one months, the average was 128 when awake and 112 when asleep. The observations of Hohl and Allix[8] indicate that among very young children the difference between the pulse of sleep and the pulse of wakefulness may equal forty beats. According to[Pg 7] Guy (loc. cit.) the pulse is more variable in the morning than during the afternoon or evening.
Temperature.—Aside from the almost hourly fluctuations of the bodily temperature, a noticeable sinking of the temperature-curve is observed during the hours of sleep. This alone is sufficient to indicate a diminished rate of combustion in the tissues. Boussingault found[9] that a dove which consumed 255 millegrammes of carbon every hour while awake, oxidized only 162 millegrammes when asleep. Scharling also observed that the quantities of carbon successively oxidized by the same man when asleep and awake bore to each other the ratio of 1:1.237. The observations of Demme[10] indicate that increase of bodily temperature during the hours of sleep must be considered as the result of pathological processes in the tissues. The observations of Allix (loc. cit.), made upon sixteen children during the first twelve days after birth, showed an average fall of 0°.38 C. during the hours of sleep. Eight children, between five and sixteen months old, exhibited a similar depression of 0°.56 C.; while ten children, ranging in age from twenty months to four years of age, averaged 0°.34 C. less when asleep than when awake.
The well-known experiments of Chossat, who found that the temperature of pigeons was from 0°.70 C. to 0°.90 C. higher at noon than at midnight, may not be considered satisfactory evidence of the depressing influence of sleep, because it is true that the diurnal variations of temperature which are conditioned by[Pg 8] the vital activities of every animal might be sufficient to account for these differences. The experiments of Horvath[11] are more convincing. This observer found that the marmots upon which he experimented were accustomed to sleep during the winter for about four days continuously, and would then remain awake for an equal length of time. “During the sleeping period they can be cooled down to such a degree that a thermometer introduced into the rectum to the depth of an inch and a half indicated only 3°F. above the freezing point. The temperature rose rapidly after the animal awoke, so that in the course of an hour it was 3°F. higher; at the close of the second hour 9°F. higher, and at the end of the next half hour about 27°F. * * Neither respiration nor the muscular movements were correspondingly augmented.” This observation clearly shows the powerful influence of cerebral activity upon the liberation of heat within the body.
Secretion.—The functions of the numerous glands throughout the body are diminished during sleep. The tears dry up, and the cornea receives less moisture. Hence the stickiness of the margins of the eyelids during the sleep of a patient suffering with conjunctivitis. He can open his eyes, on awaking, only after sufficient time has elapsed to revive the lachrymal flow. Exner[12] remarks the diminution of pathological secretion in nasal catarrh during the hours of sleep. The mouth in like manner ceases to receive its full quota of saliva, and its cavity quickly dries if the lips remain open. The secretions of the gastro-intestinal glands[Pg 9] vary with the contents of the alimentary canal; but in general they are considerably diminished, and digestion is correspondingly retarded during the hours of sleep. The quantity of urine is lessened during sleep.[13] The elimination of urea and of other excrementitious matters is less during the night than by day.[14] Unless increased by disease, or by accidental circumstances connected with atmospheric temperature and unnecessary clothing, the perspiration is also diminished.
Nutrition.—All the molecular processes of nutrition are reduced by sleep. The lowering of the bodily temperature has been already indicated. The observations of Helmholtz[15] indicate that the actual liberation of heat in the tissues is but little more than one-third of the amount set free in an equal period of time during the waking hours. The numerous experiments[16] of Boussingault, Henneberg, Scharling, E. Smith, Liebermeister, Pettenkofer, Voit, and Lewin, clearly indicate the fact that during sleep less oxygen is absorbed, and less carbonic acid gas is discharged, by the tissues. Voit found that while, during the daytime, 435 grammes of oxygen were taken in by a working man, only 326 grammes were needed by the same individual during the nocturnal half of the day. Artificial sleep occasioned by chloral hydrate produced a similar reduction in the consumption of oxygen and in the formation of[Pg 10] carbonic acid gas. Under the influence of morphine the reduction of CO2. reached 27 per cent., and the diminution of oxygen amounted to 34 per cent. of the quantities furnished during wakeful activity. The comparatively small reduction (only 6 per cent.) in the decomposition of the nitrogenous elements of the body during the same period, exhibits the close relation between the metamorphosis of the non-nitrogenous elements of the tissues and the amount of bodily activity.
The experiments of Pettenkofer and Voit, to which allusion has just been made, serve also to illustrate the fact that all tissue changes are increased by every excitement of the sensory organs of the body, but are diminished by the subsidence of peripheral irritations. Hence the importance of quiet and darkness when we seek to induce that state of the body in which molecular processes should reach their minimum. Since every act of perception is attended by an outburst of refuse matter from the nervous tissue, the quantity of such excrementitious discharge in any given period of time becomes in some sort a measure of the vital activity of the organism. Conclusive proof of the diminution of vital function during sleep is thus obtained.
It must not, however, be inferred that the general reduction of tissue-change, which has thus been established, during the hours of sleep, is evidence of a universal and uniform reduction of function throughout the body. Sleep seldom falls at once with equal force upon every organ; its invasion is progressive. Consequently, certain structures may be fast asleep, while[Pg 11] others are partly awake,—while still other portions of the organism may be in a condition of activity greatly in excess of their ordinary wakeful function. Upon this fact depend the phenomena of dreams and the various forms of somnambulism. The special senses are usually overcome by sleep before the muscular apparatus yields, and the cerebro-spinal nervous centres are the last of all to succumb. The eyes, for example, cease to see clearly before the eyelids droop, or the muscles of the neck give way in the act of nodding. The senses of touch and of taste fail next in order, as in the case of the infant gourmand, who may be seen falling asleep at supper,—his mouth yet filled with untasted sweets from the table before him. The sense of smell is more persistent, and its exercise is sometimes an obstacle to the invasion of sleep. Witness the effect of powerful odors upon certain persons. The perfume of flowering plants in the sleeping chamber is sometimes decidedly annoying on this account. A lady of my acquaintance was once awakened out of a sound sleep by the smell of tobacco smoke from the pipe of a thoughtless burglar who had quietly entered a distant apartment of the house. A sudden change of wind, deluging a city with the vapors of a glue-factory or rendering establishment, may in like manner disturb the slumbers of thousands of people.
The sense of hearing seems to be the most persistent of all the special senses. It is not a very uncommon thing for persons to be awakened by the sound of their own snoring; or, if not actually aroused by the noise, to remain in a condition of repose which seems to be sustained and cheered by the regular rhythm of[Pg 12] its own music. As a general rule, however, it is noteworthy that, when not wholly dormant, each sense finds its sphere of activity greatly narrowed by the fact of sleep. Consequently the range of perception, if not wholly obliterated, is greatly limited during the time of sleep.
While it is true that sleep arrests the voluntary activities of the muscles, it is also a fact that all the muscles do not yield at once or in equal degree. The extensors of the neck, and the supporters of the spinal column, are the first to fail. The patient begins to nod, and is inclined to fall forward, before consciousness ceases. The muscles of respiration and of circulation continue to contract, though at a diminished rate. The vermicular movements of the intestinal coats persist, and in certain conditions of ill-health their exaggerated contractions may become a cause of imperfect repose. Reflex movements may always be excited during natural sleep. Tickling the sole of the foot will cause retraction of the limb; and before the complete establishment of sleep, a certain exaltation of the spinal reflexes may be observed. Young children may frequently be seen in the act of suction with their lips, as if at the breast; and the smile of the sleeping infant is a matter of daily remark in every nursery. The influence of dreams as an excitant of muscular movement will be hereafter discussed.
The variation of intellectual function which appears in sleep serves to measure its profundity and to indicate the extent of its invasion. The act of perception being dependent upon sensation, it is to be observed that the range of perception diminishes so[Pg 13] soon as the organs of sense begin to yield. Its intensity may not immediately fail, but the breadth of its scope is narrowed. Sometimes, however, the act of conscious perception is arrested before the organs of sense are sealed. The sleepy reader may continue to eye the page before him, perhaps even to read aloud for a considerable time after he has ceased to derive any meaning from the words of the book. In such cases the organs of perception and conception and association of ideas slumber before the bonds of connection between the will and the muscular organs have been completely relaxed. Such an example affords a valuable illustration of the division of the brain into separate mechanisms which, though most intimately related, are nevertheless partially independent of each other. Sleep may operate like an invasive disease, falling with unequal incidence upon the different structures that make up the mass of the brain, paralyzing one portion, while simply benumbing another, and even arousing to excessive activity a third. Consequently the intellectual functions may be very unequally disturbed, and the order of their subsidence may be considerably varied; but, as a general rule, the physiological relations of the faculties are respected, so that as sensation diminishes, perception fails, the conception of ideas is correspondingly hindered, and the association of such ideas as are still projected upon the field of consciousness becomes more imperfect. The loss of the power of association implies the destruction of memory and the impossibility of exercising the reasoning faculty or of forming those judgments upon which every act of volition is based. When the brain[Pg 14] has at length been so far overwhelmed that physical impressions can no longer reach the field of consciousness, all manifestation of intellectual life is at an end, and the sleeper sleeps a dreamless sleep that leaves no trace behind.
It is assumed in the last sentence that the brain may become so far transformed by sleep that it ceases for the time to be capable of function as the instrument of thought. This conclusion has been questioned by the very highest authorities. Sir William Hamilton, Exner, and many others have instituted numerous experiments to test the possibility of a dreamless sleep. Causing themselves to be suddenly aroused at all hours of the night, they invariably found themselves at the instant of awaking occupied with the course of a dream. Hence it has been inferred that the mind is always alert, even when the body is most thoroughly asleep. In explanation of the fact that consciousness contains after deep sleep no trace of such mental activity, it is claimed that the act of dreaming of which we are aware at the moment of waking is proof of intellectual function during the moments which preceded that incident, and that we are merely forgetful of all similar processes that occurred during undisturbed sleep. The unconsciousness of sleep, according to this theory, is not real—it is only apparent through failure of the memory. If this be true, memory is the only intellectual faculty of whose inaction we can be sure. The period of deep sleep might then be, for all we know to the contrary, a period of the most intense and exalted mental activity. But, if so, it is quite worthless as a constituent of our conscious existence.[Pg 15] It may also be objected with equal reason that the dreams which unquestionably occupy the field of consciousness at the instant of waking are probably excited by the impressions which terminate sleep. The process of waking, though often very greatly hurried, is by no means absolutely instantaneous. As we shall learn, the time requisite for the evolution of a dream may be indefinitely brief. Consequently, it seems better in all such instances to assign the period of dreaming to the time of diminishing slumber that corresponds to the disturbance by which sleep was terminated.
The only reason for any hesitation in the acceptance of such a proposition consists in the reluctance of many philosophers to admit the possibility of any interruption in the active life of a spiritual being, such as man is conceived to be. But it is difficult to comprehend any valid reason for the denial of such interruption. Every form of force, of which we have any knowledge, is subject to fluctuations in the course of its phenomenal manifestation. When a physical force ceases to exhibit itself in an active state, and passes into a potential modification, we are not compelled to regard it as extinguished. It is merely latent or inhibited, but always ready to take its place again among the kinetic forces of nature. In like manner there seems to be no good reason why that spiritual force or congeries of forces which constitutes the mind of man may not experience analogous transformations in successive periods of action and of repose. Such periods of rest occur in sleep, in coma, in disease and disorganization of the brain. The mind sleeps, it does not cease to[Pg 16] exist—probably not even when death dissolves its material substratum.
That the depth of sleep is exceedingly variable is evident in the experience of every one. A German physiologist[17] has made a rough estimate of the soundness of sleep by comparing the loudness of the noises necessary to wake the subject of experiment at regular intervals during the course of the night. He arranged a gong with a pendulum attachment, and noted the length of the stroke which produced a sound sufficiently loud to awaken the patient. In this way the different degrees of intensity of the awakening noise could be calculated, and the corresponding depth of sleep could be estimated. It was thus concluded that the depth of sleep increases rapidly during the first hour, at the end of which time it has reached its maximum. During the next half hour it diminishes as rapidly as it had increased in the first half hour. During the next hour it still further diminishes, almost as much as it increased during the second half hour. The remaining ten half hours of the experiment were occupied by a comparatively light and gradually diminishing slumber, until the vanishing point of sleep was reached at the expiration of eight hours from its commencement. This observation corresponds with the general opinion that sleep is deepest in the early part of the night. For the same reason dreams and[Pg 17] wakefulness are most frequent during the early watches of the morning.
When considering the causes of sleep it is needful to exclude from view those artificial varieties of sleep that are produced by the various narcotic drugs, as well as the counterfeits of sleep which result from diseased conditions of the body. It is comparatively easy to frame hypotheses in explanation of such interruptions of our conscious life; but, when we attempt to formulate a theory which shall satisfactorily account for the occurrence of natural sleep in healthy animals, the task becomes exceedingly difficult.
First among the causes of sleep may be reckoned the alternation of day and night. With the disappearance of sunlight all nature sinks into a condition of repose.
“The night brings sleep
To the greenwoods deep,
To the bird of the woods its nest;
To care soft hours,
To life new powers,
To the sick and the weary—rest!”
In this tendency to nightly inaction man shares with all other living creatures. His body thus testifies to the intimacy of its relations with all portions of the solar system. Originated in the tropical regions of the earth, where day and night are nearly equal, we find in all parts of the world the same hereditary need of a period of rest, nearly coincident with the duration of the shorter nights of the tropical year. Had the birth-place of primeval man been situated within the Arctic circle, it is probable that his hours of sleep might have differed considerably from the[Pg 18] number now needed by the average individual. So powerful are the necessities thus dependent upon the harmony between our organization and the movements of the earth, that if the habit be formed of sleeping at other hours than those which are usually devoted to that purpose, the full complement of sleep is still needful to satisfy the demand for rest.
Prominent among the causes which predispose to sleep at night is the cessation of a majority of the sensations that are continually pouring in upon the brain during the period of daylight. Hence the necessity for seclusion in darkened rooms, from which the noises of the daytime are shut out, if one would sleep during the long days of the arctic summer, or if one would enjoy a midday nap at any season of the year. The close dependence of wakefulness upon the constant activity of the organs of sensation, is well illustrated by a case related in Hermann’s Handbuch der Physiologie, Vol. II, Part 2, p. 295. A young man had been reduced by disease to such a condition of general anæsthesia that the right eye and the left ear were the only remaining paths of sensation between his brain and the external world. Whenever the sound eye and ear were bandaged so as to cut off all communication with the brain, the patient invariably fell asleep in the course of two or three minutes after the interruption of sensation. In like manner, some people, even in perfect health, are able to sleep at any time by simply lying down and closing the eyes. Such persons, however, are not often very highly gifted in the intellectual sphere. They generally belong to a class of men whose lives are laborious and liable to great irregularity and fatigue.[Pg 19] Such people labor in the open air, where every organ of sense is in a state of continual excitement. As soon, therefore, as they can find a quiet corner from which the commotion of the elements is excluded, it is only necessary to close the eyes—the principal avenue of communication with the outside world—and sleep begins at once. This is especially true if severe bodily exertion has preceded the opportunity for repose.
Fatigue of any sort is one of the most energetic causes of sleep. The impossibility of long sustained exertion is a fact almost too familiar to attract attention. Every muscle must be suffered to rest for a time after contraction before it can be again contracted. Even the heart and the muscles of respiration must be allowed to enjoy regular periods of repose many times each minute. These are examples of local rest, not involving the entire body. But if the whole body participate in any violent action, every part will manifest a consequent disposition to rest. Witness the effects of the venereal act. Every muscle is relaxed; the brain, which has officiated as the supreme source of energy, experiences exhaustion, and sleep frequently terminates the voluptuous paroxysm. In like manner, sensations of severe pain, if sufficiently prolonged, become a cause of sleep. Prisoners upon the rack have slept through sheer exhaustion while undergoing the horrors of torture. Little children frequently fall into a deep sleep immediately after painful, though comparatively bloodless, surgical operations performed without anæsthetics. The depressing emotions, even, may so fatigue the brain as to induce sound sleep through reaction from previous[Pg 20] excitement. Every wearied portion of the body must rest; and when the brain thus rests, sleep is the consequence.
Impressed by the force of such considerations, certain physiologists[18] have reasoned from the analogies suggested by a study of the results of muscular fatigue, and have suggested an hypothesis accounting for the occurrence of sleep by a supposed loading of the cerebral tissues with the acid products of their own disassimilation during wakeful activity. The acid reaction of the brain and of the nerves after exertion, corresponding with the development of acids in the muscular tissues during contraction, suggested the probability that an excessive presence of lactic acid and its sodic compounds might be the real cause of cerebral torpor and sleep. Could this hypothesis be proved, ordinary sleep would take its place along with the states of unconsciousness induced by anæsthetics and hypnotics, and the lactate of sodium should be found the very best of medicines for the relief of wakefulness. Its administration for this purpose, however, has yielded only the most discordant and unsatisfactory results. The fatigue theory, moreover, is insufficient, since it furnishes no explanation of the invincible stupefaction produced by cold, nor does it render intelligible the unbroken sleep of the unborn child.
Far more comprehensive is the hypothesis advanced[Pg 21] by Pflüger.[19] According to this view, the state of wakefulness is maintained by a certain degree of activity in the cortical substance of the brain. Like all other bodily organs, this substance is renovated by the assimilation of nutrient materials derived from the blood. By this process oxygen is stored up in chemical combination, forming “explosive compounds,” whose precise composition is not fully understood. When for any reason the supply of oxygen is insufficient, as in hemorrhage, producing cerebral anæmia, or in impregnation of the red blood corpuscles with carbonic oxide or chloroform, or other substances capable of excluding oxygen from the hemoglobin of the corpuscle, the cerebral tissues are imperfectly renovated. The explosive constituents of the cortical protoplasm are then inadequately renewed after mental activity, and the sensitive portions of the brain are no longer fitted to manifest the highest forms of intelligent activity. But, when nothing interferes with healthy nutrition, the requisite degree of instability in the protoplasm of the brain is effected by intussusception of oxygen. Under the influence of the various nervous impressions which reach the brain, the unstable protoplasmic compounds break up into simpler forms. The motion thus liberated by these “explosions” of excitable matter is, in some way at present utterly inconceivable, projected upon the field of consciousness where the mind dwells; and we are thus brought into conscious relation with the external world.
That the capacity for thus signalling across the[Pg 22] gulf which divides matter from mind is the result of a certain perfection and complexity of physical structure is rendered probable by the utter failure of the infra-cortical organs alone to impress the conscious intelligence by any amount of independent activity. The same thing is also indicated by the unconscious sleep of the rudimentary fœtal brain, and by the brevity of the intervals of wakefulness which mark the life of the new born babe. That this capacity is dependent upon a special mobility of the atoms of the brain, is shown by the speedy cessation of intelligence which follows great reduction of temperature, as in hibernation, or during exposure to severe frost. That its exercise is largely dependent upon the activity of the senses is proved by interference with their function, as in the case above quoted (see p. 18) from the observations of Strümpell.
The dependence of the waking state upon the presence and activity of a sufficient quantity of a peculiarly unstable form of protoplasm in the brain is an hypothesis which presents no great difficulty of comprehension. But how may we explain the lapse from the intelligent vivacity of that waking state into the unconscious inactivity of sleep? I have elsewhere[20] discussed the manner in which artificial sleep is produced by impregnation of the brain with anæsthetic substances that interfere with sensibility, and finally produce stupefaction, by hindering the normal processes of intra-molecular oxidation in the protoplasm of the nervous tissues. The same general line of argument may be extended to cover the action of every narcotic[Pg 23] agent with which the living substance of the body may become surcharged. Accepting, then, the hypothesis advocated by Obersteiner and Preyer, it becomes an easy thing to account for the gradual onset of sleep by supposing an accumulation of the “fatigue producing” products of intra-molecular oxidation. But we cannot thus explain the rapid and, as it were, voluntary passage from wide awakefulness into a condition of deep sleep, such as may be commonly observed among sailors and others who have formed the habit of going at once to sleep at regularly recurring hours of the day or night. Certain writers have endeavored to account for this fact by imagining a special mechanism at the base of the brain (choroid plexuses of the fourth ventricle, etc.,) by means of which the current of the blood through the brain may be voluntarily diminished, with a consequent arrest of conscious activity. But, still adhering to the hypothesis of Pflüger, we shall obtain a clearer explanation of the facts by considering the phenomena connected with the succession of impressions upon the organs of sense. It has been ascertained[21] that such impressions must persist for a certain measurable length of time in order to excite conscious perception. A sound must be prolonged for at least fourteen-hundredths of a second, a ray of light must agitate the retina for about eighteen to twenty-hundredths of a second, an ordinary contact with the surface of the skin must continue from thirteen to eighteen-hundredths of a second, in order to awaken any knowledge of sound and light and tactile sensation. For the simplest act of perception from two to four-hundredths[Pg 24] of a second are necessary. It is, therefore, perfectly reasonable to suppose that when the “explosive material” of the brain has been sufficiently “dampened” by the accumulation of acid refuse which accompanies prolonged cerebral effort, the impressions of sense may no longer suffice to excite in the cortical protoplasm vibrations of sufficient length, or following each other in sufficiently rapid succession, to sustain consciousness. The cortex of the brain may then be likened to a body of water into which bubbles of partially soluble gas are introduced from below. When the bubbles are large, and when they follow each other rapidly, a continual effervescence is maintained upon the surface of the water. But if the size of the bubbles be reduced, or if the solvent capacity of the liquid be increased, the surface will become almost, if not quite, perfectly tranquil. In some such way, without any great danger of error, may we picture forth the manner in which the generation of ideas in the field of consciousness is related to the molecular movements in the space occupied by the protoplasmic substance of the brain. Returning, now, to the rapid induction of sleep, we find that it is usually the experience of people who lead an active life in the open air, and are compelled to endure frequent interruption of their rest. The sailor who is trained to work four hours on deck, and then to sleep four hours below, has been virtually transformed by this habit into a denizen of a planet where the days and the nights are each but four hours long. His bodily functions become accommodated to this condition; his nervous organs store up in sleep a supply of oxygenated protoplasm sufficient only for an active[Pg 25] period of four or five hours; so that, when the watch on deck is ended, he is in a state as well qualified for sleep as a laborer on shore at the close of a day of twelve or fifteen hours. Moreover, the majority of those who can thus easily fall asleep are individuals whose waking life is almost entirely sustained by external impressions. So soon, therefore, as such excitants are shut out by closing the eyes in a place of shelter from the sounds and turmoil of the air, comparatively little remains for the stimulation of ordinary consciousness, and sleep readily supervenes through mere lack of cerebral excitement, especially if the excitable matter of the brain has been previously overwhelmed by the products of active exertion.
That analogous, though not identical, predisposition to unconsciousness may also be rapidly induced by modifications of the cerebral circulation is proved by the sudden reduction of cerebral excitability and consciousness which occurs during the act of fainting. In this counterfeit presentment of sleep the important part played by variations of the blood current through the brain is so conspicuous that certain writers have attempted to show that genuine sleep is the result of a diminution in the flow of blood to the cortex of the brain. An ingenious physician has even attempted to relieve insomnia very much as a surgeon might undertake to cure a popliteal aneurism—by placing tourniquets on the arteries leading to the affected part. But the mere fact that syncope produces unconsciousness does not prove that “cerebral anæmia” should be elevated to the rank of the principal cause of natural sleep. The nervous process is the primary factor.[Pg 26] The circulation of the blood is everywhere under the immediate control of the nervous system. Consequently, every change in the condition of the nervous structures is followed by a corresponding change in the state of the circulating apparatus. Wherever an organ is aroused to activity, so delicate are the adjustments by which it is connected with the brain and with the heart that it is at once irrigated by an increased flow of blood. When its functional activity subsides, the same mechanism provides for a corresponding reduction in the supply of blood to its tissues. The brain itself forms no exception to this law. This has been admirably shown by the observations of Professor Mosso, of Turin.[22] The learned professor enjoyed the rare opportunity of observing three individuals who had suffered the loss of a considerable portion of the bony walls of the cranium, exposing the surface of the cerebrum, and affording a view of the pulsation of the vessels of the brain. With the aid of the cardiograph, the sphygmograph, the hydrosphygmograph, and the plethosphygmograph, it became possible to register the circulation of the blood in the brain, and to compare that portion of its course with the coincident circulation in other parts of the body. It was thus shown that every increase of emotional or intellectual activity was attended by an increase in the activity of the cerebral circulation. This increase was procured at the expense of other portions of the body, which exhibited a coincident reduction in the amount of blood received from the heart. The occurrence of sleep caused a[Pg 27] diminution in the number of respirations, and a fall of six or eight beats in the pulse. The volume of the brain and its temperature were at the same time slightly reduced, through the diversion of blood from the head to other regions of the body. The consequent dilatation of the vessels in the extremities was readily demonstrated by the use of the plethosphygmograph. The extreme sensitiveness of the nervous centers was further illustrated by the fact that if, during sleep, a ray of light were directed upon the eyelids, or if any organ of sense were moderately excited without waking the patient, his respiration was at once accelerated; the heart began to beat more rapidly, the vessels of the extremities contracted, and the blood flowed more freely into the brain. Similar results accompanied the act of dreaming. The return of full consciousness on waking was followed by an immediate increase in the activity of the intra-cranial circulation.
The extreme susceptibility of the brain to influences proceeding from artificial disturbances in the circulation, was exhibited in the case of one of Professor Mosso’s patients. By compression of the carotid arteries, unconsciousness was induced, and an attack of convulsions was aroused. In no other part of the body can a corresponding disturbance of function be so quickly produced by similar means. A limb may be rendered bloodless for nearly half an hour, by the application of an elastic bandage, and yet its sensory nerves will remain capable of transmitting impressions from the periphery. But in this case, compression of the carotids for only eight seconds was sufficient to[Pg 28] abolish consciousness and to excite convulsive movements.
In all such observations it is worthy of note that the nervous impression is the primary event so long as artificial disturbances are not intruded. The changes of blood-pressure and circulation were invariably secondary to the excitement of nerve tissue. Sleep, therefore, must be regarded as the cause, rather than the consequence, of the so-called cerebral anæmia which obtains in the substance of the brain during repose. This condition of “anæmia” is nothing more than the relatively lower state of circulation which may be remarked in every organ of the body during periods of inactivity. Every impression upon the sensory structures of the brain occasions a corresponding liberation of motion in those structures. The movement thus initiated arouses the vaso-dilator nerves of the cerebral vessels and excites the vaso-constrictor nerves of all other portions of the vascular apparatus. Hence the superior vascularity of the brain so long as the organs of sense are fresh and receptive. Hence the diminishing and varying vascularity of the different departments of the brain as sleep becomes more or less profound. These modifications of the brain and of its circulation are well illustrated by the effects of a moderate degree of cold applied to the cutaneous nerves of the body, as not unfrequently happens when the night grows cool towards morning. The disturbance of the sensitive nerves of the skin is transmitted to the brain. The excitement of this organ causes dilatation of its vessels, and increased irritability of the cortical instrument of perception. This becomes the[Pg 29] starting point for the projection of impulses upon the field of consciousness, producing dreams, or even a complete awakening from sleep.
The cause of sleep must, therefore, be sought in the molecular structure of the brain, rather than in fluctuations of the blood-current. In the present state of our knowledge it must be negatively represented as the consequence of a deficiency in the amount of movable oxygen in the nervous tissue. This deficiency may be the result of immaturity, as in the fœtus, or in the new-born infant; or it may result from the accumulation of an excess of the waste-products of intra-molecular oxidation during functional activity—products which hinder the further passage of oxygen into stable combination with the oxidizable elements of protoplasm. Sleep thus produced differs from the artificial sleep induced by narcotic drugs, in the fact that its cause is self-generated by the instrument of thought, while narcotic stupor is caused by the intrusion of substances derived from without—substances which, like the natural refuse of the living cells, more or less completely hinder the processes of oxygenation and oxidation within the tissues of the body. Hence the states of healthy sleeping and waking must necessarily be self-limited and regularly successive; while the state of narcotism is purely accidental, and its duration exactly corresponds with the variable length of the period during which the body may remain impregnated with the hypnotic agent.
Certain morbid forms of sleep further illustrate its dependence upon the persistence of depression in the functional activity of the brain. For some persons[Pg 30] this seems to constitute their normal condition. They are either excessively fat, red-faced, and soaked with beer, or they are pale, anæmic, and pulpy, with flabby muscles and a feeble circulation. They fall asleep whenever left to themselves, and never seem to be fully aroused to active life. The fat boy who figures so amusingly in The Pickwick Papers, furnishes a life-like picture of this variety of somnolence.
The introductory stage of the eruptive fevers is often characterized by somnolence. It also frequently appears as the forerunner of coma in the various diseases which terminate in unconsciousness and death. A singular example of this has been observed among the negro inhabitants of the Atlantic coast of tropical Africa. The disorder is known to English writers as sleeping dropsy; by the French it is called maladie du sommeil. It is characterized by daily paroxysms of somnolence which tend to become more and more continuous and profound until they are finally merged in fatal coma. For our knowledge of the disease we are chiefly indebted to the description by Clark,[23] an English surgeon who practised in Sierra Leone, and to the monograph by Guerin,[24] a French naval surgeon, who had enjoyed exceptional opportunities for observation among the laborers who had been carried from Africa to the island of Martinique. Similar cases have been occasionally reported in other regions of the world, but it is among the Africans that it has been principally remarked. The onset of the malady is[Pg 31] gradual, commencing with a slight frontal headache. After a few days a disposition to sleep after meals is noted. This becomes increasingly urgent, and the intervals of sleep are prolonged until at length the patient becomes continually soperose. The waking periods are marked by a sluggish state of the intellectual faculties. The pulse is not accelerated, and it remains full and soft. The veins of the sclerotic are turgid, and the eyeball seems unusually prominent. The temperature does not increase, but rather tends to diminish its figure. The skin is dry and moderately cool. The tongue continues moist, and is covered with a white fur. The bowels and the bladder are regularly emptied, and the appetite persists with considerable vigor. Finally, the patient becomes completely comatose, and dies quietly. Sometimes, however, the evolution of the disease is less tranquil. Epileptiform convulsions, followed by progressively deepening periods of coma, interrupt its course, and a continuous muscular agitation marks the closing scene. At the same time the pulse grows weaker and more frequent until its movements cease in death. Recovery is almost unknown, though the duration of the disease often varies from three months to a year or longer. Examination of the body after death yields very negative results; the sinuses and larger vessels of the brain are engorged with blood, but no evidence of inflammation is anywhere apparent. The other organs present no pathological alterations whatever. These observations seem to indicate that the disease originates in some form of general blood-poisoning, rather than in any local inflammation or degeneration. Dr.[Pg 32] Clark has called attention to an enlargement of the cervical glands as a feature of the malady. According to Dr. G. H. Bachelder,[25] the native physicians cure the disease by extirpation of the affected glands. He has also observed an initial lesion in the nasal mucous membrane. If this be confirmed, the malady will take its place among the forms of somnolence produced by infection of the blood.
Between the profound unconsciousness of natural sleep and coma may be placed the distinction that the one is always the consequence of healthy physiological processes, while the other is always the result either of injury, of disease, or of some form of intoxication. Comatose unconsciousness may be the result of cerebral compression caused by injury of the head, or by the presence of an inflammatory exudation. Intra-cranial tumors, embolisms, thrombi, diseases of the cerebral arteries, and degenerations of the brain,—in short, every morbid change of which the liquids and the solids within the cranium are capable—may become the cause of coma. Toxæmic conditions of the circulating fluids of the body may benumb the brain with comatose sleep. Few diseases, therefore, exist without the possibility of coma as one of their consequences—a coma which, however, must not be confounded with the genuine sleep which sometimes occupies the larger part of convalescence from acute illness. During such convalescence there is a reversion to the infantile type of nutrition with all its need of prolonged and frequent periods of repose. Like normal sleep, the comatose condition admits considerable variation of[Pg 33] intensity. The patient may sometimes be partially roused, as from the coma of alcoholic intoxication, and he may finally recover complete consciousness; but very often the reverse is the fact. The coma deepens into paralysis of the respiratory centres, and death concludes existence without the slightest manifestation of sensibility or intelligence.
Lethargy is a pathological variety of sleep, in which the repose of the body is even more complete than in coma. The victim of coma often presents a countenance suffused with blood; the pulse beats vigorously, and respiration may become stertorous. But in lethargy the abolition of bodily movement is almost absolute. In the milder forms of this disorder the patient may be partially roused, so as to attempt an answer when addressed, appearing like a person in very deep sleep; but in the majority of cases he remains insensible, unconscious, and utterly irresponsive to ordinary forms of irritation. Respiration and circulation are reduced to a minimum, and may, even for a time, become imperceptible. Uncomplicated with hysteria, the disorder is rapidly fatal, but, according to Rosenthal,[26] hysterical lethargy is never mortal.
Many examples of this disease have been afforded by the records of apparent death. I am well acquainted with a lady who, in early childhood, had been laid out for burial at the supposed termination of some infantile illness. Her mother alone insisted that the child was still alive. After some time spent in weeping and expostulation, she applied a blister to the thorax of the babe. This soon excited evidences of painful[Pg 34] irritation, followed by a complete recovery. Still more instructive is the case, narrated by Rosenthal,[27] of a young woman, twenty-four years of age, who, in consequence of violent emotional excitement, became unconscious, and presented no signs of life, though tested by placing a mirror before the mouth, and by dropping melted sealing-wax upon the skin. On raising her eyelids, the pupils gave no reaction to light; the limbs remained perfectly flaccid, and the radial arteries were pulseless. Careful auscultation, however, detected a very feeble and intermittent sound in the cardiac region. The walls of the chest exhibited no movement, but the lateral surfaces of the abdomen presented a slow and almost imperceptible oscillation. Gentle faradization of the muscles and nerves of the face, arm, and hand, excited definite muscular contractions. By this method Rosenthal became satisfied that, although the patient had remained for thirty-two hours in this condition, she was only apparently dead. In fact, after continuing forty-four hours in a state of suspended animation, she awoke spontaneously, made a rapid recovery, and seemed to enjoy as comfortable health as an excitable, nervous temperament would permit.
Certain authors make a distinction between lethargy and apparent death; but the difference is one of degree rather than of kind. The movements of respiration and of circulation, though greatly enfeebled, are readily observed in ordinary forms of lethargy; but in apparent death the pulse can no longer be discovered, and nothing more than the faintest sound can be[Pg 35] distinguished in the region of the heart. It, therefore, becomes important to have within reach a crucial test of the persistence of general vitality. Such evidence, according to Rosenthal, is furnished by the faradaic current. Within two or three hours after actual death, the muscles cease to respond to the induced current; but in apparent death this form of electro-muscular contractility never disappears. Every other test that has been proposed has failed under certain circumstances. Observation of the changes in muscular temperature during electrical excitation is a method better adapted to the laboratory than for clinical practice.
Lucid lethargy.—In certain cases of apparent death the patient exhibits all the external appearance of suspended animation, but the power of conscious perception does not cease. The senses of sight and hearing remain, and are, perhaps, intensified by inhibition of the power of voluntary movement. The sufferer sees and hears; perception, emotion, memory, the power of reasoning, judgment, volition, all persist. Only the power of executing voluntary movements is lacking.
The victims of this variety of apparent death are usually women, or men who are characterized by a feminine nervous organization. Great mental excitement, fatigue, semi-starvation, and exhausting diseases, are the principal exciting causes of the event. The following case, related by my friend, Dr. P. S. Hayes, of Chicago, illustrates the phenomena of lucid lethargy. The patient was a female physician, about thirty years of age, unmarried, and consumptively inclined. During the course of a long and wearisome[Pg 36] hospital service, she was prostrated with typhoid fever. Placing herself under the immediate care of my informant, she was also attended by several of the most eminent physicians in the city. After a long and exhausting illness she appeared to be dying. In the presence of her physician, and surrounded by her relatives, she ceased to breathe. The pulse stopped, life seemed to have gone out. Bottles of hot water were applied to the limbs, and various restoratives were employed. After a considerable time she began again to breathe, and a gradual recovery followed. During the whole time of apparent death, consciousness had been preserved. She seemed to be looking down from a point above her bed; she could see the doctor feeling for her pulse, and was grieved by the sorrow of her friends. Ordinary sensation was temporarily suspended, and she could not distinguish the contact of the hot-water bottles that were applied to her limbs, though actually scalded by their excessive heat. Borne upon the wings of an excited imagination, she thought herself permitted to look into heaven, but was not suffered to enter its gates. In this exaltation of the imagination the reasoning faculties also shared, so that certain philosophical problems which had previously baffled her intellect were now perfectly comprehensible, and the memory of their solution persisted after recovery.
Many similar narratives have been duly authenticated, but the limits of the present chapter will not permit a discussion which properly belongs to an investigation of the phenomena of trance. The important fact for present consideration is the[Pg 37] persistence of conscious life, despite the appearance of death. In this preservation of consciousness, notwithstanding the temporary suspension of certain kinds of sensibility and the power of voluntary motion, may be discovered a relationship between the phenomena of lucid lethargy and various disturbances of sleep, which will be considered in a succeeding chapter.
INSOMNIA, OR WAKEFULNESS.
| Sleep, gentle sleep, Nature’s soft nurse, how have I frighted thee That thou no more wilt weigh mine eyelids down And steep my senses in forgetfulness? —King Henry IV, Second Part. |
We have seen that the condition of normal sleep is determined by a peculiar molecular state of the substance of the brain—a modification regularly alternating with that by means of which the condition of wakefulness is sustained. We have also seen that sleep is liable to variations in its intensity, and that its course may be partially interrupted by dreams, or even by a more or less complete resumption of the movements of locomotion, constituting the different varieties of somnambulism. Our attention must now be directed to the consideration of those greater disturbances of sleep which either serve to prevent its full development, or else to actually interrupt its course, rendering it incomplete and fragmentary, or even abolishing it altogether. But, inasmuch as the healthy brain, when associated with a healthy body, can only by an extraordinary effort of the will be kept awake beyond a certain period, and then only for a short time beyond the ordinary interval of wakefulness, it follows that the study of the usual causes of insomnia must be an[Pg 39] investigation of morbid conditions of the bodily functions. Sleeplessness, therefore, must result, 1st, from a disturbance of the peripheral sensory organs of the nervous system; 2nd, from disordered conditions of the sensory nerves and nerve tracts; 3rd, from morbid states of the brain; 4th, from any or all of these conditions operating in association with each other. We may, therefore, consider, I, Insomnia caused by irritation of the peripheral portions of the sensory apparatus; and, II, Insomnia caused by morbid states of the central nervous organs.
I. Insomnia caused by irritation of the peripheral portions of the sensory apparatus.
Irritation of the sensory apparatus may be ranked in three classes:
1. Affections of the organs of special sense.
2. Affections of the nerves of common sensation.
3. Affections of the sympathetic nerves.
1. Affections of the organs of special sense.—Prominent among these is the effect of light upon the eye. The darkness of night favors sleep; the presence of light hinders its incidence and renders it less profound. During the gloom of a total eclipse animals seek their shelter; birds hide themselves in their nests; domestic fowls arrange themselves upon the roost, and seem quite disconcerted by the speedy return of sunlight. Children often find it difficult to sleep in an illuminated room. I have known nurses who would sit with a wakeful infant under a powerful gaslight till after midnight, and then would express their surprise that the baby persisted in gazing at the flame instead of going quietly to sleep. The inhabitants of[Pg 40] Northern Europe find it necessary to darken their sleeping rooms during the long polar day; and travelers in such regions often suffer for want of the natural sleep which only darkness affords. Judge Caton, writing of his travels in Norway[28] says: “We longed for darkness and for night. Do what we could to darken the windows to keep out the light, still it was not night as nature makes it, and which the habit of a lifetime had rendered necessary to sound repose. Artificial darkness, especially when incomplete, is as far from night as artificial light is from day.... These sunny nights can hardly conduce to health, they steal away so much of sleep. One does not readily get sleepy in the sunshine, and then we are so apt to forget to look at the watch to see if it is time to retire.”
In the tropical regions of the world it is usual for the inhabitants to sleep during the middle of the day; but they take great pains to exclude the light from their houses during the hours of sleep. The Pacific Islanders cover their faces with the bed clothes for the purpose of excluding the light while attempting to sleep. Repose thus obtained in the daytime often serves to convert the night into a season of wakefulness. The Africans sleep and dream away the heated hours of the day, and give up considerable portions of the night to festivity in the open air—a practice which undoubtedly contributes to the permanence of an inferior grade of social life.
Sudden illumination of the sleeping room will frequently awaken the sleeper. During the great fire in Chicago, A. D. 1871, many persons were thus aroused[Pg 41] from their slumbers as the flames lighted up the streets adjoining their houses. One of my acquaintances was awakened one night by a flash of light from the lantern of a burglar who was moving noiselessly about her chamber. The experience of almost every one will testify to the effects of sheet-lightning silently illuminating the sky by night. Dreams, also, are not unfrequently excited by the incidence of light upon the closed eyelids.[29]
The sense of hearing is one of the most persistent of the special senses during the incidence of sleep. It is perhaps the most excitable of these senses during the period of repose. Long after the subject has become immersed in sleep his auditory apparatus remains sensitive to sounds. Dreams are often produced by impressions upon the ear. Often in sleep it seems as if the sense of hearing remained wakeful and watchful for expected signals, as when an alarm clock serves to arouse the sleeper at an appointed hour. Sometimes the sleeper may be shaken and tumbled about in his bed without waking, but if he be addressed by name he will usually reply. It is scarcely probable that the auditory apparatus is any more wakeful than other portions of the nervous system, but its external portions remain during sleep more completely exposed and adapted to the reception of impressions than is possible for the eye and for the organs of touch and taste.
The persistent sensitiveness of the ear during sleep is not so much a capacity for noticing sounds as a sensibility to variations in sonorous impressions.[Pg 42] Thus a steady and monotonous noise may, if long continued, serve to render one sleepy; but the sudden cessation of the same sound will awaken every one. Slowly lulled to sleep by the incessant rumble of the engine upon one of the old-fashioned Long Island Sound steamboats, how immediate the awakening of a whole cabin full of people, when the wheels were suddenly stopped! A recent traveler in Guiana[30] relates a curious experience with an Indian magician who undertook to cure him of a slight headache and fever. The method of cure consisted in placing the patient at night in his hammock, while the magician kept up a hideous succession of yells and shouts, shaking the walls and roof of the house with an uproar which never ceased for six hours. Before long the patient passed into a kind of fitful sleep or stupor, during which he seemed to be suspended in a surging ocean of sound. When the noise died away, as if growing fainter in the distance, he would rouse up into a semi-conscious state, but when it again increased he would fall back into stupor. At last, when the noise finally ceased, he awoke completely, but without the slightest relief from headache—an experience quite illustrative of the manner in which the brain may be affected by sound.
It is not often that the sense of smell becomes the avenue of impressions that interfere with sleep. So different are the capacities of individuals in this particular that an odor which might severely annoy one person, would pass almost unnoticed by another. Large cities are sometimes invaded by overwhelming[Pg 43] stenches from the various factories which spring up in their neighborhood. While it is seldom true that the vapors discharged by such establishments are directly deleterious to health, they may become indirectly a cause of ill-health through the wakefulness occasioned by them among weakly invalids. The smell of smoke in a bed-chamber sometimes serves to awaken a sleeper, giving warning of the outbreak of a fire in the building. Less energetic odors may disturb the depth of sleep without actually waking the patient. Thus Maury records[31] that when he was made to inhale the vapor of cologne water while asleep, he dreamed of being in the shop of a perfumer.
Excitement of the sense of taste would, doubtless, operate in a similar manner; but it is so difficult to arouse this sense without at the same time irritating the nerves of common sensation about the mouth, that very little can be said regarding the matter. Dreams of gustatory sensations are usually of subjective origin, dependent upon some reflex movement, or upon some agitation of the organ of memory, within the brain.
If, with Sir William Thompson,[32] we recognize a sixth sense—the sense of temperature—it must be admitted that through the varying sensations of heat and cold, sleep can be greatly disturbed. Every one will recall to mind the story told by Dugald Stewart, of a gentleman who dreamed of walking over heated lava on Mt. Ætna when a bottle of hot water was placed against his feet, in bed, on account of some slight[Pg 44] indisposition. The temperature of the air is one of the most important factors in the determination of sleep. A high temperature keeps every one awake—a fact well known among the unfortunate denizens of the garrets in our great cities. Not only is wakefulness the direct result of heat, but it is aggravated and embittered by the accompaniments of a torrid climate—insects, foul air, and cutaneous disorders. In the East Indies, so difficult is sleep under such conditions that the wealthy inhabitants compel their servants to cool them all night with the punkah, a large, swinging fan, suspended above the bed, and kept in motion by means of a cord leading outside of the bed-room to the verandah, where the punkah-wallah sits and pulls the string while his master sleeps. So powerful is the force of habit in the organization of the automatic apparatus of the body that, though these punkah-pullers often fall asleep, they still continue, without interruption, the successive movements by which the fan is kept in operation.
The evil effects of a high temperature are greatly aggravated by the presence of humidity in the atmosphere. Dampness interferes with the process of exhalation from the surface of the body, which, consequently, tends to become overheated. The tissues, under such circumstances, are imperfectly defecated, and rapidly pass into a condition of imperfect nutrition. This depresses all the functions of the body, and renders the nervous system inordinately irritable. Sleep cannot be profound and refreshing, because of the over-excitable state of the brain. During the long, hot season in tropical countries, it often becomes[Pg 45] necessary to seek a temporary retreat among the highlands and mountains, in order to find a climate sufficiently dry and cool to furnish the condition for refreshing sleep. For the same reason many of the inhabitants of the Southern United States are forced to spend the summer months in the invigorating atmosphere of Minnesota and Northern Michigan. One of the most delightful of experiences may be procured on any warm day in summer by embarking, at Chicago, upon one of the steamboats bound to Mackinac. At the wharf, in the hottest and dirtiest part of the city, all is dust, perspiration, and discomfort. The wide cabins are filled with people who are tired, thirsty, and discouraged. Sickly, squalling babies swarm in numbers sufficient to drive one mad. As the sun goes down, the signal-whistle sounds, head-lines and stern-lines are quickly cast off, the propeller churns the mire behind the boat. Slowly swings the huge fabric away from the shore, gliding between the walls of sun-scorched brick that line the stream on either side. At last the light-house at the mouth of the river is passed, and we are out upon the blue waves of Lake Michigan, with a heavenly breeze searching every crack and cranny of the hull. New life animates every form, and presently a great silence pervades the brilliant cabins. The children have left their woes behind, and, for the first time, in many weeks, perhaps, they and their weary mothers sleep the sleep of innocence and peace.
The dependence of a high atmospheric temperature upon the direction of the wind renders the course of the aerial currents a matter of great importance in[Pg 46] relation to sleep. The southerly winds which, in the northern hemisphere, are hot and enervating, always produce an increase of wakefulness. The winds that blow from the heated deserts of Africa, Arabia, and Australia, are greatly dreaded upon this account, as well as for the other numerous discomforts which fly in their train. Their cessation, and their replacement by a cool, polar current brings relief at once. The changes thus produced in the electrical condition of the atmosphere doubtless contribute more than is usually known to these results. A cloudless sky gives evidence of positive electricity, which is much stronger in winter than in summer.[33] Clouds are sometimes positive and sometimes negative. According to Fonssagrives[34] the atmospheric electricity is positive during northerly winds, and negative during the prevalence of winds from the southerly quarters of the horizon. Great disturbances of the electrical condition of bodies is often observed during the occurrence of the sirocco in North Africa. Arago has related the case of an officer in the French army[35] who saw sparks of electricity leaping from his epaulettes at every blast of the sirocco encountered on a march in the neighborhood of Algiers. Such atmospheric disturbances often produce very disagreeable effects upon persons of a nervous temperament. According to Fonssagrives (loc. cit.) such patients frequently experience, during the prevalence of storms which traverse great distances, a high degree of insomnia, together with headache, pains in the[Pg 47] limbs, joints, and old injuries, and a general indefinable sensation of discomfort. S. Weir Mitchell has carefully traced the connection between these phenomena and the variations of barometric pressure which accompany the revolving storms that cross the continent in a northeasterly direction.[36]
Though the effect of a high atmospheric temperature is unfavorable to sleep, an excessive temperature produces the opposite condition. Stupor rather than sleep is the consequence of insolation and of exposure to great heat from artificial sources. This is a pathological process, and, therefore, must not be mistaken for natural sleep. It may result either from cerebral congestion, or from cardiac exhaustion, and is characterized by an extraordinary bodily temperature and a high rate of mortality.[37] So elaborate are the arrangements for the preservation of a uniform temperature throughout the body that it is practically impossible for a sunstroke to occur unless the regulative apparatus has been previously deranged by ill-health.
Excessive cold operates in like manner to produce a condition of stupor that tends to a fatal termination. But moderate degrees of cold act as excitants of wakefulness. By effecting a contraction of the vessels of the skin cutaneous circulation is impeded. The venous side of the circulatory apparatus becomes overloaded with blood; the exhalation of carbonic acid and the production of heat are reduced. The discomfort that results from this disturbance of the natural functions[Pg 48] of the tissues is sufficient to arouse the brain to wakefulness, just as an imperfect oxidation of the blood serves to excite the respiratory centre in the medulla oblongata. It is hardly necessary to allude in this connection to the increased flow of blood through the brain occasioned by this as by every other excitement of the sensorium. Local refrigeration of any portion of the body thus acts as a painful excitant of the cerebrum, and produces wakefulness, very much as distention of the intestines with gas will keep one awake. It is for this reason almost impossible to sleep with cold feet. Conditions of this sort are pathological, and are far in excess of the agreeable coolness which favors sleep. The effects of progressive diminution of the temperature of the air are well illustrated by the hibernation of animals.[38] As the temperature of the air diminishes, in winter, animals like the marmot fall into a species of sleep. Their movements of respiration and circulation are greatly reduced, and their bodily temperature falls, though it always remains several degrees above the temperature of the surrounding air. So long as the average degree of cold is maintained, the little creature sleeps naturally; but, if the air becomes extraordinarily cold, the physiological repose of the animal is disturbed. It becomes uneasy, wakes up, and seeks a warmer retreat. Too great a degree of cold thus becomes a cause of wakefulness. If the animal under these circumstances fails to secure protection against a falling temperature, it passes into a state of lethargy that is often fatal—a pathological condition being substituted for the physiological sleep[Pg 49] of ordinary hibernation. In like manner the human animal may experience the threefold effects of refrigeration: first a pleasing coolness that favors sleep; then an uneasy sensation of cold which causes wakefulness; and, finally, a lethargy that paralyzes all the functions of the body and terminates in death.
2. Affections of the nerves of common sensation.—Chief among the causes of sleeplessness thus produced is pain. This is a modification of feeling, caused by excessive or extraordinary excitement of the peripheral nerves of sensation. The seat of the excitement may be in the skin or in the deeper tissues of the body. Cutaneous pain may be caused by the activity of various insects, like flies, mosquitos, fleas and bedbugs, or by the presence of certain parasites, such as the itch-mite, or by ordinary diseases of the skin, of which notable examples are found in erysipelas, erythema, urticaria, lichen, prurigo, certain varieties of eczema and psoriasis. The troublesome forms of pruritus which accompany icterus, or which may occur without any clearly defined cause, are frequent causes of wakefulness. The last mentioned disorder must, however, be sometimes recognized as a consequence of central nervous disorder, rather than a result of peripheral disease. Witness the frightful itching sometimes experienced during the progress of chronic myelitis. All kinds of injuries, wounds, ulcers, and other local inflammations are common causes of insomnia by reason of the painful impressions transmitted from them to the brain. Hence the great importance of anodynes and hypnotic remedies in the course of surgical practice. Diseases or injuries of[Pg 50] the various peripheral nerves are notable causes of sleeplessness. Witness the horrible wakefulness caused by neuritis and by neuralgia. The development of neuromata in the stumps of amputated limbs may thus become a most painful cause of insomnia. Inflammations which encroach upon sensitive nerves produce intense pain with consequent loss of sleep. Of this very conspicuous examples are furnished by spinal meningitis, and by the effects of local periostitis causing compression of the branches of the fifth pair of nerves.
3. Affections of the sympathetic nerves.—So much still remains to be learned concerning the pathological functions of the sympathetic nerves that it is impossible to assign with any great degree of precision the exact amount of interference with sleep that may depend upon disordered conditions of this portion of the nervous system. Since their principal functions consist in the regulation of the flow of blood and lymph throughout the body, and in the control of the processes of nutrition, calorification, secretion and excretion, it follows that any considerable derangement of their healthy action must be represented by a corresponding disturbance of the brain. This may reach the field of consciousness in the form of pain, and thus may become a cause of sleeplessness. In all the phenomena of inflammation sympathetic nerves play an active part. In certain portions of the body, as in the principal viscera, and in the periosteal covering of the bones, they are the interstitial nerves of the structures. When the body is in a healthy condition these nerves convey impulses of a sensory character which do not[Pg 51] reach the cerebral organ of conscious sensation. But in certain morbid states they become inordinately sensitive, and they then serve to convey and probably also to magnify sensations to an extent that may cause exquisite pain with all its consequences. Witness the pain experienced during the various forms of colic. Rheumatic inflammations, pleurisy, pericarditis, peritonitis, cystitis, metritis, ovaritis, gastro-enteritis, and other similar diseases owe their principal suffering to the affection of the sympathetic nerves connected with the respective organs which become the seat of pain. Including with the sympathetic nerve the pneumogastric nerve, which occupies a functional position between the strictly peripheral and the ganglionic nerves, all the various forms of pain and uneasiness experienced in the region of the heart and of the lungs may be assigned to this system of nerves. Thus the various species of respiratory disturbance, such as asthma and dyspnœa from any cause, and the forms of palpitation and other cardiac disorder may become causes of wakefulness. In like manner the vague and uneasy sensations associated with certain varieties of dyspepsia are frequent sources of sleeplessness, not merely by reason of the pain which they occasion, but also because of the general disorders of nutrition with which they are associated.
II. Insomnia caused by morbid states of the central nervous organs.
So intimately connected are the spinal cord and the brain that their disorders may properly be considered together. These may be classified as:
[Pg 52]1. Disorders of circulation and nutrition.
2. Inflammations and degenerations.
3. Neoplastic encroachments.
Disorders of circulation and nutrition.—Hyperæmia of the brain is a frequent cause of wakefulness. This may be maintained by an unconscious effort of the organ of the will under the influence of any great and unusual excitement of the mind. So soon as the mental excitement is allayed, the excessive afflux of blood subsides, and the brain becomes fitted for sleep. But, if excitement be too far prolonged, the nutrition of the nervous centres suffers, and the regulative apparatus of the cerebral circulation becomes exhausted, so that the brain cannot rest, because its inhibitory centres have lost their power of control over the lower ganglia of the organ. The cerebro-spinal centres are then in a condition analogous to that of a locomotive engine on which the engineer can no longer regulate the production and distribution of steam. Such a condition is usually the result of numerous antecedent causes. Long hours of work, scanty or improper food, insufficient sleep, bad hygienic surroundings and habits, with indulgence in the use of narcotics and stimulants, are among the most common causes of the disorder.
Active hyperæmia of the nervous centers has been above mentioned as the consequence of cerebral function under unfavorable conditions. But, as the disorder persists, its type undergoes a change. We still speak of the disorder as functional in its character, but it continually tends to become organic. No visible alterations, perhaps, can be detected, but, evidently, there are radical changes in the substance of the nervous tissue. Nutrition suffers throughout the body to[Pg 53] a degree that attracts attention. The blood diminishes in quantity and quality, till the patient becomes notably anæmic. In this condition the brain is inordinately excitable. It is incapable of sustained activity, and the patient may even be oppressed by an inclination to constant drowsiness; yet he will be unable to sleep soundly, and his sleep will be continually agitated by dreams. This state is one of the constant accompaniments of slow starvation. The molecular structure of the nervous organs seems to be so slightly constructed, under such circumstances, that its equilibrium is disturbed by the most trifling incidents. It may be likened to a lofty wall of bricks laid up without mortar—“if a fox go up,” the entire structure may be thrown down with a tremendous noise. Thus the anæmic and irritable brain will react excessively under the slightest impression; consciousness is invaded by perceptions which would never arise under normal conditions of the nervous tissue; and the mind is continually aroused. This form of wakefulness is very frequent among women who have become anæmic, and among patients who are slowly convalescing from exhausting diseases.
It is impossible in every instance to decide whether a given state of wakefulness is the result of cerebral hyperæmia or anæmia. In the one case the persistence of wakeful activity of the mind is due to excitement of the cerebral cells, accompanied by a lavish irrigation of their substance with the plasma of the blood. In the other case the excitement is occasioned, not so much by increased afflux of the blood, as by a morbid instability of the nervous substance. The outcome in both[Pg 54] cases is very similar—mental excitement and wakefulness.
In a third class of cases the agitation of the brain is produced by the direct action of certain chemical agents upon the cortical substance. Tea and coffee are familiar examples of such agents. The caffeine, by virtue of which they produce their effect, when transported to the brain, enters into combination with its protoplasm in such a way as to stimulate molecular movement. Perception is thus quickened, and the mind is aroused. Sleep is postponed until the effect of the stimulant has subsided. This form of wakefulness is quite different from that produced by alcoholic drinks. These operate, when taken in small quantities, to favor cerebral equilibrium—and consequent equanimity—by producing a general dilatation of the smaller blood-vessels. Their anæsthetic influence is favorable to sleep, under such circumstances. But, if frequently repeated, these doses of alcohol modify the nutrition of the nervous system until, at last, a condition of irritable weakness is reached, in which wakefulness of a most distressing character is experienced.
Inflammations, degenerations, and neoplasms.—The early stages of inflammation involving the central nervous organs are marked by that form of insomnia which is associated with active hyperæmia. The headache and painful delirium which accompany the different varieties of meningitis, are causes of a wakefulness that persists until the brain is merged in the coma of compression. The interstitial changes which cause the various forms of insanity, are in like manner causes of[Pg 55] wakefulness. Local injuries and degenerations of brain-substance, tubercular deposits upon the meningies, and all the different forms of intra-cranial tumor, are causes of wakefulness, both by reason of the direct irritation which they produce, and by reason of the circulatory disturbances which arise in their neighborhood.
Finally, it must be observed that wakefulness may result from excitement of the brain by irritating substances transported through the blood from distant centers of disease in remote organs of the body, or derived from articles that have been absorbed with the food and drink, or with the air that enters the lungs. Thus wakefulness may accompany cutaneous disorders that interfere with perspiration. Imperfect elimination through the liver, kidneys and intestines, leaves the blood charged with excrementitious substances which arouse the brain to wakefulness. In like manner, various poisons, like lead, arsenic, etc., different miasms of telluric origin, the products of putrefaction, and the various animal contagia, may produce insomnia by their prejudicial effect upon the nutrition of the nervous structures throughout the body.
REMEDIES FOR INSOMNIA.
| O, true apothecary! Thy drugs are quick. —Romeo and Juliet. |
An occasional attack of wakefulness may fall to the lot of any one as a consequence of the various disturbances of health or equanimity of mind to which all are liable. Occurring as an accident in a state of health, it produces merely a feeling of lassitude and weariness during the subsequent day. This soon disappears, after a night of refreshing sleep, and the subject is nothing worse for the incident. But the recurrence of the disorder is a thing to be deprecated, not only for the reason that it denotes a departure from the physiological order of life, but because its frequent repetition prevents the adequate repair of the tissues of the body. The great function of nutrition suffers as a consequence, and the patient rapidly falls into a condition of premature old age. When this takes place as a result of some temporary error of hygiene, or as a consequence of diseases which admit of successful treatment, the patient may be restored to health by judicious management, but lost youth and elasticity of the tissues can never be fully regained. The most formidable cases of insomnia are those for which no adequate cause can be recognized in the habits, mode[Pg 57] of life, and state of health of the patient. Grave and permanent disorder of the brain is then to be feared. Such wakefulness is a frequent precursor of acute meningitis in children and adults. It frequently ushers in the early, insidious, formative stage of tubercular meningitis, and of the infective fevers—notably typhoid fever. It forms one of the most suspicious symptoms among the introductory phenomena of insanity; and during the course of protracted diseases, its intrusion is an omen of most unfavorable augury. It will, therefore, be found useful to consider with some degree of detail the circumstances under which insomnia may occur, and the best means of averting its onset.
A severely logical reference to previous doctrines regarding the condition of the brain during sleep, has led many authors to consider the therapeutical treatment of insomnia chiefly as a matter of modification of the cerebral circulation. Sleep has been supposed to depend upon a comparatively bloodless state of the brain, and wakefulness upon the contrary state. For such theorists the treatment of insomnia consists very simply in the use of agents which are supposed to be efficacious in reducing the flow of blood through the head. Tourniquets, placed upon the carotid arteries, occupy a position of great honor in the armamentarium of such people. Recognizing the fact that changes in the force of the circulation accompany and sustain every change in the activity of the cerebral cortex, we, however, attach the greatest importance to the condition of the nervous substance itself. For a clear understanding of the proper mode of medication, it is[Pg 58] important to ascertain whether the cerebral substance is in a state of normal activity, or whether it is in a state of healthy, but excessive, activity, or whether its seeming excitement is merely the result of irritable weakness. Since these opposite conditions may declare themselves during the course of any disease in which insomnia may become a troublesome phenomenon, it is impossible to make a classification of diseases upon the basis of these different states of the brain. It will, therefore, be found more useful to consider the subject of sleeplessness as it ordinarily presents itself during the clinical progress of the several forms of disease. It will, then, appear that the type of insomnia is liable to variation with the course of each individual malady; and its treatment must vary accordingly.
Before proceeding to a discussion of the therapeutics of insomnia in connection with particular diseases, it will be advantageous to pass briefly in review the different remedies which are useful in the treatment of wakefulness. These may be divided into two classes: Nervous stimulants, and nervous sedatives. Among the first may be also reckoned food, heat, baths, and counter-irritants. Like all nervous stimulants, they promote the complete and harmonious action of all parts of the nervous system, favoring that equilibrium of the circulation which is most favorable to the development of sleep. The second class of agents comprises all such remedies as act directly upon the nervous tissue of the brain, depressing its functional activity, and hushing to rest those particular organs which, by their undue excitement, serve to keep the[Pg 59] remainder in a state of wakefulness. All these substances produce decided effects upon the spinal cord and the peripheral nerves, but it is their operation upon the brain which principally interests us in connection with insomnia.
| Nervous Stimulants. | Nervous Sedatives. | |
| Heat. Baths. Massage. Electricity. Counter-irritants. Food. Digitalis. Camphor. Musk. Valerian. Cannabis indica. Belladonna. Hyoscyamus. Stramonium. Phosphorus. Acids. Opium. |
Cold. Alcohol. Paraldehyde. Ether. Chloroform. Chloral. Butylchloral hydrate. Amyl nitrite. Opium and opiates. Bromides. Hops. Gelsemium. Conium. |
NERVOUS STIMULANTS.
It may at first sight seem to be a contradiction in terms when it is asserted that sleep may result from the administration of a nervous stimulant. This does occur, but only indirectly, and as a consequence of a restoration of energy to those portions of the nervous system which serve to moderate the activity of the organ of the mind—the cortex of the cerebrum.
Heat, for example, is an undoubted stimulant. When added to the body in quantity sufficient to overcome chilliness, it tends to equalize the circulation of[Pg 60] the blood, and produces throughout the body a nervous equilibrium that prevents any particular organ or member from arousing the others to wakefulness.
Baths.—The application of heat in the form of a warm bath constitutes one of the most admirable means of tranquilizing the brain. Children who are restless at night are delightfully soothed by a warm bath every night and morning. The water should be of an agreeable temperature—this is better than any exact figure upon the scale of a thermometer—and the bath should not last lounger than ten minutes. Similar baths exercise a happy effect upon adult patients who are moderately feverish, nervous, and wakeful. If strong enough, they may take a full bath at bedtime; but if too feeble to leave the bed, gentle sponging with warm water will prove most refreshing, and will usually be followed by restful sleep. The well-known derivative effects of hot foot baths scarcely need to be more than mentioned in this connection.
Turkish baths form an invaluable adjuvant in the treatment of chronic cases of insomnia arising from rheumatic, gouty, and dyspeptic disorders of the health. The copious perspiration induced by the heated air of the hot chamber is depurative, while the cold douche and the massage with which the bath is concluded have a powerful effect to stimulate all the functions of the body. By this means the brain is enabled to resume a healthier mode of action, and sleep follows as a matter of course.
Massage.—This constitutes a process of rubbing and kneading the body. It has been practiced from time immemorial among the oriental races and the[Pg 61] Pacific Islanders as a means of relief from fatigue of every kind. Among the Japanese the practice of massage is a monopoly in the hands of the blind, who are thus enabled to support themselves. Various modifications of the oriental method have been introduced under the names of percussion, shampooing, and the Swedish movement cure. They all possess the common features of friction applied with the hand to the skin, compression of the muscles with the hands, and passive movements of the different articulations of the limbs and body. For effecting all these processes nothing has yet surpassed the Sandwich Island lomi-lomi as practised by the court-retainers of the ancient chiefs. As a means of relieving fatigue, and of removing muscular soreness, after violent exertions of every kind, it is far superior to the imitations performed by European and American professional masseurs and masseuses. Nervous headaches, the pains that accompany spinal irritation, and all conditions of restlessness and wakefulness which depend upon exhaustion are relieved by this method. The well-known soothing influence of a mother’s hand stroking the face and forehead of her sleepless child, is an example of only one of the effects thus produced by the skillful masseur. These salutary results must be assigned to the uniform friction of the skin, causing the liberation of heat, and modifying the electrical conditions of the body. By this, the impressions derived from the peripheral nerves are reduced to a more harmonious series. The circulation of blood and lymph is rendered more active in the substance of the muscles, and all the processes of nutrition are thus[Pg 62] stimulated to a degree that restores the equilibrium of function throughout the nervous system. Being no longer irritated by suffering portions of the body with which it is connected, the brain then yields to the effects of its own fatigue, and sleep supervenes.
Electricity is chiefly useful in those cases where it is impossible to discover anything but cerebrasthenia as the cause of wakefulness. According to Beard and Rockwell,[39] sleep may result from the use of any one of the different methods of electrization. The passage of a moderate current, either galvanic or faradaic, through any portion of the body often produces a temporary feeling of sleepiness; but the long continued employment of electricity is needful to effect those changes in cerebral nutrition which are necessary for a permanent cure of insomnia. In cases of sleeplessness caused by worry and overwork, great benefit is often experienced from the daily passage of the faradaic current from the back of the neck, or from the pit of the stomach, to the feet. Static electricity, and the electric bath, are also very effective in many cases of so-called spinal irritation and insomnia.
Counter-irritants are substances which are applied to the surface of the body for the purpose of communicating to the superficial sensory nerves impulses (irritation) which may serve to inhibit the morbid functions of distant or central nervous structures. Various explanations of this process have been presented; notably a most ingenious argument by Dr. T. Lauder Brunton[40] in favor of the theory of inhibition[Pg 63] by interference of vibrations—impulses from the periphery interfering with vibrations originating in morbid conditions of the central nervous organs—very much as darkness is produced by the interference of luminous undulations, and silence is effected by interference of sonorous waves in the atmosphere. This hypothesis is the one that is most conformable to the present requirements of science, and is hereby accepted as the most satisfactory explanation of the action of counter-irritants.
The drugs in general use for the purpose of counter-irritation are cantharides, capsicum, mustard, thapsia, turpentine, aconite, and croton oil. Cups, leeches, and certain special applications of electricity, also owe much of their virtue to the same power of modifying functions at a distance. Under the influence of all these agents the molecular vibrations of the brain may be profoundly influenced; pain may be annulled, and sleep be procured. The circulation of the blood is so powerfully affected by these measures that their good effects are usually attributed to the circulatory changes thus produced. But, as in all other modifications of the circulation, the nervous tissues and the vascular channels must first be reached by influences unconnected with the blood itself before its current can be diverted from one region to another. The inhibitory action upon the nervous organs is the primary effect. The diversion of the circulation is a secondary consequence, by which, undoubtedly, the degree of nervous change can be estimated, and by which the inhibitory effects in the brain are intensified and sustained.
Food.—In a considerable number of cases of[Pg 64] insomnia, its cause lies in an irritable weakness of the nervous tissues. Exhausted by overwork, or debilitated by the loss of blood, or half-starved during the course of a long illness like typhoid fever, a condition of wakefulness may be established which will add to the dangers experienced by the patient. In this state there is great restlessness—the sufferer experiences no severe pain, but he cannot lie still. This form of sleepless agitation is often encountered during the later stages of exhausting diseases; and, if not properly treated, it soon leads to a fatal termination. The most important remedy for such distress is found in food. This must be soluble, diffusible, stimulant, and nutritive. Milk, alcohol, eggs, and meat-juice, are the typical representatives of such food. Milk should be as fresh as possible, and should be slightly salted, in order to hinder the formation of hard curds in the stomach. For young children it may be peptonized with advantage by gently heating one pint of milk with five grains of sodium carbonate and five grains of pancreatic extract dissolved in half a pint of water. The mixture may be sufficiently warmed by placing it in a bottle immersed for half an hour in a jug of hot water (Fairchild). By this process the milk is partly digested before it is drank, thus relieving the alimentary canal of a corresponding amount of work.
Furnished in the form of koumiss, milk is not only presented in a digestible form, but the alcohol and the acids yielded by its fermentation are powerful aids to the process of digestion. Fermented milk forms a considerable portion of the daily food of the nomad tribes of Central Asia, and it is highly esteemed among the[Pg 65] Russians in the treatment of pulmonary consumption. It is useful in all diseases affecting the digestive organs, and can often be tolerated, even by very young children, when nothing else will remain in the stomach. Considerable mystery is made of its preparation by those who sell it for an enormous price; but its composition is really very simple, and its actual cost is within the reach of every one. The following formula for its preparation has given great satisfaction to many of my patients:
Dilute five quarts of milk with three quarts of hot water. When lukewarm, add half a cupfull of sugar of milk (which can be obtained from any wholesale druggist), and one bottle of well fermented koumiss (or a little yeast). Stir the mixture thoroughly, and let it stand in an open jar, at a temperature of about 72° F., till it begins to curdle. Then stir in half a cupfull of pulverized coffee sugar, and cork tightly in champagne bottles with the best velvet corks. The bottles should be kept quite cool, as fermentation proceeds very briskly, and will break the containers if left in a warm room. A large ice-box is the best receiver during hot weather. The koumiss thus prepared is ready for use at the end of a week. It may be most conveniently drawn from the bottle with a champagne tap. The entire cost of the article need not exceed seven cents a bottle.
Sleeplessness caused by chronic dyspepsia will often yield to a diet of koumiss, when every other remedy has failed. When the stomach is very intolerant, it should at first be taken in very small doses, repeated as often as every hour. It will soon become[Pg 66] possible for the same patient to drink two or three quarts each day.
Eggs form one of the most nutritious and easily digested articles of diet. They should be taken uncooked, beaten up with milk to which a small quantity of wine or spirits and sugar have been added. A glass of eggnogg, thus prepared, is invaluable in the insomnia of fevers and other conditions of exhaustion.
Meat-juice can be procured in numerous forms. The various soluble extracts of meat, Valentine’s liquid extract of beef, Murdoch’s liquid food, all represent the juice that oozes from rare beef. Its nutritive value is not very great, but it possesses considerable energy as a stimulant. Meat juice, therefore, occupies an important place as an excitant of those functions which must be aroused in order to secure the proper digestion of other articles of food. It should, therefore, be administered in connection with them. As the ordinary meat extracts are frequently very unpalatable, they may be administered in fresh broth or soup, to which they give body and energy without unpleasantly affecting their savory taste.
Neurasthenic patients, whose insomnia results from physical exhaustion, should never retire at night without taking some form of light and easily digested food. A simple slice of bread, or a piece of plain sponge-cake, with a glass of koumiss, forms an excellent model for such a meal.
Digitalis is only indirectly useful as an hypnotic. In cases of cardiac disease, with enfeeblement of the heart, dyspnoea, dropsy, and sleeplessness, digitalis is[Pg 67] often of the greatest service. It has also been highly recommended in delirium tremens. Administered in the form of an infusion, it has been given in doses of a tablespoonful, every four hours, with apparently good effect. Its use is indicated in cases characterized by weakness of the heart, with a rapid and feeble pulse. Under its influence the state of the circulation improves, delirium ceases, and sleep occurs.
Camphor.—This substance is not an hypnotic, but it forms a valuable addition to various hypnotic compounds. It is a cerebral stimulant, and aids in the establishment of that nervous tranquility which favors the incidence of sleep. It may, therefore, be advantageously associated with opiates in the restlessness and insomnia of exhaustion. Tully’s Powder, a valuable substitute for Dover’s Powder, contains camphor. This renders it preferable to the ordinary opiates in typhoid fever, and in other exhausting diseases.
Musk, the dried secretion of the preputial follicles of the musk-deer, is a substance which, on account of its high price, is rarely used as an hypnotic. Given in doses of ten grains, every two or three hours, it is exceedingly valuable (Stillé and Maisch) for the relief of “all those nervous phenomena which are represented by the term ataxia, and among them subsultus tendinum, mild muttering delirium, floccitation, muscæ volitantes, and hiccough, with a small, frequent, tremulous or irregular pulse, without coma and without collapse. Under these circumstances musk tends to produce refreshing sleep, while it calms muscular spasm and favors perspiration, while the pulse grows fuller, more regular, and less frequent.... In[Pg 68] proportion as ataxic prevail over adynamic phenomena is musk advantageous.” Such conditions are chiefly encountered in typhus, typhoid fever, the eruptive fevers, and pneumonia. Musk is very efficacious for the relief of “wakefulness resulting from combined mental and bodily fatigue—such cases, in fact, as are benefitted by valerian, camphor, asafetida, and ammonia.”
Valerian and its different preparations form a typical class of agents which indirectly favor sleep by their gently stimulant effect upon the brain. They are all useful in quieting that form of hysterical excitement to which women are liable during the “change of life.” That form of restlessness, usually resulting from fatigue, in which the patient feels as if she cannot sit still, is often relieved very promptly by the valerianate of ammonia. Wakefulness caused by neuralgic pains, or by exhaustion, often yields readily to scruple doses of valerianate of zinc or ammonia. The elixir of the valerianate of ammonia is a very elegant preparation of the drug.
Cannabis Indica.—A cerebral stimulant which produces, at first, an agreeable exaltation of the mental faculties. This is followed by a condition of delirium, succeeded in its turn by sleep. It is, therefore, impossible to use the drug for merely hypnotic purposes; but it is a useful adjuvant, in small doses, to other hypnotic remedies. Given in doses of ½-1 grain, it may be advantageously associated with opiates, or with hyoscyamus or belladonna in cases which do not easily tolerate the preparations of opium. The tannate of cannabin, given in doses varying from five to ten[Pg 69] grains, has been recommended as an hypnotic; but, like the extract from which it is derived, its effects are rather uncertain. The pure alkaloid, cannabin, has been recently introduced as a soporific, in doses of three-quarters of a grain to a grain and a half. According to Stillé and Maisch, the wakefulness caused by the itching of eczema may be relieved by the use of cannabis indica. The uneasy sleep attendant upon ungratified sexual appetite may also be relieved in the same way, since the drug is decidedly anti-aphrodisiac.
Belladonna is not directly hypnotic, unless given in poisonous doses, but its medicinal operation tends to overcome certain conditions that hinder sleep. By its anti-spasmodic effects it relieves many forms of spasm which would otherwise interfere with sleep. Spasmodic asthma furnishes an example of such an affection. This may be relieved by the hypodermic injection of atropine. Whooping cough is another disease which may be largely controlled by the internal administration of the drug, especially by inhalation of a spray that has been medicated with belladonna. Neuralgia, especially the form that involves the head, face, and intercostal nerves, is greatly mitigated by the use of belladonna, or its alkaloid, atropia. Its association with opiates seems to increase their hypnotic effect, while at the same time neutralizing their disagreeable action. According to Curci,[41] it opposes the tendency of opiates to cause cerebral hyperæmia. For this reason it is generally advisable to combine sulphate of atropia with sulphate of morphia for hypodermic use. Of the former 1-100—1-80 grain may[Pg 70] be used with ¼ grain of the latter. Certain patients are exceedingly intolerant of belladonna and its derivatives, a fact that must be kept in mind, especially when using the alkaloid, atropia. Fatal consequences are very rare, but uncomfortable dryness of the throat, dilatation of the pupils, and some degree of delirium are not uncommon. At the same time it must be admitted that in many instances relief from suffering is not obtained until these physiological effects of the drug have been manifested.
Hyoscyamus.—As might be inferred from their close botanical relationship, hyoscyamus and belladonna present many points of similarity. Their alkaloids are almost identical in chemical and physiological properties. The extract of belladonna is considerably stronger than the extract of hyoscyamus. Like other solanaceous plants, this is powerfully narcotic and anodyne. Sleep is produced only by the use of the drug in large doses, which also tend to excite delirium, sometimes even reaching to the height of maniacal fury. Children tolerate hyoscyamus in doses proportionally larger than can be taken by adults. By many physicians it is considered the hypnotic par excellence for children. In the various forms of insanity the tranquilizing influence of hyoscyamus is highly esteemed. The derivative preparations, hyoscyamine and hyoscyamia, are preferable for use in this class of cases. The first may be given in doses of 1-16—1 grain; the latter is much more powerful, and should be given in doses not exceeding 1-100 grain until the degree of its tolerance has been ascertained.
Stramonium.—This is another of the solanaceous[Pg 71] plants, possessing many qualities like those found in belladonna. It is not directly hypnotic. Poisonous doses produce delirium and persistent insomnia. But its anti-spasmodic effect upon the paroxysm of nervous asthma renders it indirectly hypnotic in that affection. For the relief of bronchial spasm the smoke of the dried leaves should be inhaled in considerable quantity. It may be smoked in a pipe; or, mixed with saltpetre, it may be made to smoulder upon a tin plate, while the smoke is drawn by inspiration into the lungs. Various kinds of medicated pastiles have been prepared, to effect a similar result by furnishing the drug in a convenient form for use. Tobacco and lobelia operate in a very similar manner upon all spasmodic affections of the respiratory passages; but their energy is almost too great for the comfort of the patient.
Phosphorus.—Bartholow has recommended this drug in “cases of wakefulness dependent on cerebral anæmia and exhaustion,” and in “the wakefulness of the aged, accompanied with muscular cramps, feebleness of memory, giddiness, and trembling of the voluntary muscles on exertion.” In minute doses, it is true that phosphorus acts as an irritant of nervous tissue. It promotes destructive changes in the tissues of the body, and thus produces a temporary excitement which may favor the processes of nutrition. Indirectly, it may thus prove beneficial in many cases of cerebral exhaustion; but as a direct hypnotic it will be found of very little service. It should be given in doses of 1-100 grain every four hours.
Acids.—In those forms of sleeplessness which are dependent upon disordered conditions of the digestive[Pg 72] apparatus, acids are often useful. Their topical effects upon the mucous membrane of the stomach are stimulant and alterative; hence they are useful in atonic dyspepsia, where there is deficient secretion of the gastric juice. In such cases hydrochloric acid and lactic acid are useful. The first should be given, in doses of five drops diluted with half a pint of water, after each meal. Lactic acid may be given in doses of one or two teaspoonfuls, similarly diluted. It has been asserted, on theoretical grounds, that lactic acid and the lactate of sodium are directly hypnotic, but its experimental use has never given satisfactory results. Phosphoric acid has been used in the same way, with very similar effects. An impure solution of phosphoric acid, known as Horsford’s Acid Phosphate, has been extensively used for its supposed hypnotic properties. It assists digestion, stimulates the kidneys, and by its general diffusion promotes molecular activity throughout the body. It is thus indirectly beneficial in cases of insomnia. No small part of the benefits thus obtained must, however, be ascribed to the water with which these acids are diluted. When the liver becomes sluggish in its action, nitric acid, in doses of five drops diluted with half a pint of water, may be taken every four hours with great advantage. Thus used, the mineral acids may often yield invaluable service in the treatment of insomnia occasioned by cachectic conditions of the body—notably such as are produced by malaria, oxaluria, and the so-called phosphatic and rheumatic diatheses.
NERVOUS SEDATIVES.
The remedies thus far considered are but indirectly hypnotic in their effects, though exceedingly valuable as agents for the production of conditions favorable to sleep. We may now pass to the consideration of a class of remedies which operate more directly upon the brain to depress its energy. They are, therefore, called nervous sedatives, and they include the majority of narcotic substances.
Cold.—The operation of cold upon the body has already been sufficiently considered. It only remains to note the effects of cold applied through the agency of baths and local refrigerants. A full account of the theory and practice of hydrotherapeutics can be found in the second volume of Von Ziemssen’s Handbuch der Allgemeinen Therapie. The English reader will find the subject treated at sufficient length in Ringer’s Handbook of Therapeutics.
According to Ringer, the sitz-bath, taken at a temperature between 60° and 80° F., is very useful to soothe “an irritable restless state of the nervous system.” It should be employed once or twice a day, from five to thirty minutes at a time. Among other beneficial consequences is the promotion of quiet sleep.
For the relief of the pungent heat and restlessness which add so much to the danger of the specific fevers cold baths have been highly recommended. These have been employed with great energy in many of the German hospitals; and often with great benefit to the patient. The preferable method is the one advised by Von Ziemssen and Immerman. The patient is placed[Pg 74] in a tub of water at 95° F. This is very gradually cooled down, in the course of half an hour, to 60° F. The bath should be repeated from three to five times a day, according to the temperature of the patient. By this method of treatment the patient is made more comfortable; he becomes less restless or delirious, and secures a larger amount of refreshing sleep.
The difficulty of administering such a laborious course of baths outside of a well equipped hospital renders its adoption almost impossible in private practice. Here the physician must rely upon assiduous sponging with water of an agreeable temperature. In severe cases, such as measles before the appearance of the eruption, scarlet fever during the period of heat and agitation, and typhoid fever during the corresponding stage, great benefit will be derived from the cold wet sheet. In order to humor the prejudices of the laity, this should be wrung out of warm water and applied with sufficient deliberation to insure its considerable loss of heat. A blanket should first be spread upon an empty bed; the wet sheet should be spread over the blanket. The patient must be placed naked upon the sheet, which should then be drawn around the entire body, and the blanket may be folded around the whole package. Children generally insist upon leaving their arms uncovered. This may be allowed with safety in many cases, but generally a wet napkin should cover the upper part of the chest and the neck which cannot be reached with the sheet when the arms are exposed. After remaining from half an hour to two hours in the pack, the patient becomes comparatively cool and quiet, and the eruption, if[Pg 75] delayed, begins to appear. Sleep often occurs as an immediate consequence of the relief thus obtained.
Similar good results may be secured by the use of cold affusion in cases of high temperature and great restlessness. I well remember a little boy, about eight years old, whom I once found rolling and tossing and burning up with scarlet fever. Calling for an empty wash-tub, I had him stripped and placed upright in the tub. I then began to pour cold water over him from a large pitcher. Scarcely had the water touched his skin, before he seized the pitcher, and began to drink from it. He was permitted to completely slake his thirst, and then the affusion was resumed. After four or five gallons of water had been thus poured over him, he was wiped dry, and was returned to his bed, where he immediately turned upon his side, and fell into a peaceful sleep. A few more affusions relieved him from danger, and he made a rapid recovery. Were people less afraid of such measures, a considerable portion of the danger in fevers might be obviated. Great discretion, however, is necessary in the application of such treatment, for Ringer states that he has “seen a child, suffering from scarlet fever, killed by an over-energetic employment of cold.” The temperature of the patient should be carefully noted, and its reduction below the normal standard should never be permitted.
Anæsthetics.—All anæsthetics are hypnotics. In other words, they possess the power to abolish consciousness, and thus to produce a condition resembling sleep. This is effected by the direct action of the anæsthetic substance upon the cellular structure of the[Pg 76] brain, reducing the molecular movements of the living protoplasm below the degree requisite for the excitement of consciousness. This sedative effect is preceded by a brief period of cerebral exaltation, occasioned by the disturbances caused by the first introduction of the drug into the current of the circulation.[42] It is with the subsequent hypnotic effect only that we are now concerned. Of the numerous anæsthetic substances that have been discovered, but few comparatively have been found sufficiently manageable and safe for general use. These are alcohol, paraldehyde, ether, compound spirits of ether, chloroform, chloral, butylic chloral, and amylic nitrite.
Alcohol.—The hypnotic effect of alcoholic drinks is very decided, though not speedily manifested unless the beverage be taken in considerable quantity. Distilled liquors produce the effect of alcohol in its simplest form; wines, containing various forms of ether, arouse the nervous system more thoroughly and agreeably than the pure alcoholic stimulants. Beer and porter are rendered more powerfully narcotic by the active principle of hops which they contain. The nutritive substances held in solution by these last render them peculiarly appropriate in cases that require nourishment as well as rest. The considerable quantity in which they must be taken, renders them inconvenient for use in cases of severe illness. Wines and distilled liquors are then most available.
Alcohol is principally useful as an hypnotic when wakefulness is associated with great bodily exhaustion,[Pg 77] such as may be experienced in advanced stages of the infective fevers. In such cases the heart is weakened, the pulse is rapid and feeble, the muscular apparatus is wasted and irritable, the blood is diminished in volume and tends to accumulate in the venous channels. Under such conditions the patient is usually delirious, tossing from side to side, and quite deprived of sleep. An ounce of brandy, repeated at intervals varying according to the severity of the symptoms, and given with milk and egg, in the familiar form of eggnogg, will often quiet this harassing restlessness, and will procure refreshing sleep. The temperature of the patient will then decline; the tongue will grow moist; and the delirium will diminish or subside altogether. Sometimes, however, a contrary result is observed. Alcohol should then be administered with a sparing hand, and it will probably be necessary to resort to the bromides or other cerebral sedatives.
The great exhaustion which is manifested in delirium tremens sometimes requires the use of alcohol to support the patient, so that sleep may be procured. It is in such cases advisable to combine the administration of capsicum with that of alcohol. According to Ringer, capsicum should be given for this purpose in scruple doses, made into a bolus with honey, and repeated every three hours.
Wakefulness caused by neuralgic pains is speedily relieved by full doses of alcohol. The various species of abdominal and pelvic neuralgia may thus be temporarily suspended. In like manner the “rheumatic” pains which afflict the overworked and underfed poor[Pg 78] may be calmed for a season sufficient to procure sleep. The obvious dangers attendant upon such medication, however, need no comment.
Old people not unfrequently suffer with a form of insomnia that is associated with feeble and painful digestion. This is probably caused by insufficient gastro-intestinal secretion. The use of wine containing a large proportion of compound ethers gives relief through the improvement in digestion consequent upon the stimulant effect of small doses of alcohol and ether. Under their influence the digestive fluids are more abundantly secreted, and all the bodily functions are quickened. Such good results, however, only follow the moderate use of the stimulant. It must never be taken in quantity sufficient to affect the intellectual functions, or to disturb any of the normal processes of life. The best results, so far as digestion is concerned, are obtained by the use of wine with the meals; but a night-cap, in the form of hot toddy, is sometimes necessary in addition. This is especially useful if there be any form of irritative cough or local excitement, such as the aged sometimes experience.
The insomnia that attends excessive fatigue may be very quickly relieved by the use of food and alcohol. For this purpose any form of alcoholic drink will be found useful. The quantity administered should only be sufficient to produce a uniform and general vascular relaxation. By this means the circulation is equalized throughout the body, and the brain passes into a state of tranquil sleep. Any excess in the use of alcohol under such conditions will be followed by headache and discomfort on awaking. In all cases the[Pg 79] intoxicating dose of alcohol must be avoided, if its truly hypnotic effect be desired.
Paraldehyde.—This is a derivative from ethyl alcohol. It is, when pure, a colorless liquid, with an agreeable odor, somewhat like that of ether. It is soluble in the proportion of one part in eight or nine of water. It may be used internally in doses varying from forty-five to one hundred and sixty grains. A watery solution, containing one part to ten, has been recommended for internal administration. It may also be given in milk or in beer. M. Yvon[43] recommends the following formula:
| Paraldehyde, | Gr. 20.0 | |
| Spirit, | 100.0 | |
| Syr. Simpl., | 75.0 | |
| Tr. Vanillæ, | 5.0 |
An ounce of this mixture contains forty-five grains of paraldehyde. When taken it should be still further diluted with sweetened water, or with beer, to obviate, as far as possible, the disagreeable taste of the drug. Sleep follows after the lapse of about half an hour, and continues from five to seven hours. The physiological action of the medicine is very similar to that of chloral hydrate, and its use is indicated in the same class of cases to which that drug is appropriate. By many it is considered the preferable hypnotic. It has found considerable employment in the insane asylums of Europe, and in other institutions where disagreeable medication is no obstacle to experiment. In private[Pg 80] practice the peculiar taste and smell of the article, and its pungent effect upon the mucous membranes of the alimentary canal, render its exhibition more difficult. But the weight of testimony is in its favor as an hypnotic in all cases, uncomplicated with disease of the stomach, in which insomnia is not dependent upon pain, and is associated with cerebral hyperæmia. Its administration is followed by no unpleasant consequences. Among the insane it is particularly recommended during periods of excitement and wakefulness. It has been employed with great satisfaction[44] in cases of insomnia during the course of such varied diseases as emphysema, bronchitis, phthisis, nervous and spinal disorders, diseases of the heart, jaundice, chronic rheumatism, and insomnia from other unrecognized causes. Undoubtedly, with greater skill in its purification and exhibition, it will become one of the most valuable of hypnotic remedies. Almost useless for the relief of pain, it is indicated in cases of uncomplicated insomnia. Having very little power, in moderate doses, to depress the action of the heart, it is preferable to chloral hydrate in cardiac diseases and debility. Sleep procured with doses of fifteen to sixty grains is calm and refreshing, and is not followed by any disagreeable consequence. A certain degree of tolerance is gradually established, so that larger doses may become necessary. It has been given in quantities amounting to three drachms; but, if large doses be given before the development of tolerance, the patient will experience headache, uneasiness, nausea, and vomiting, after waking from the sleep thus induced.[Pg 81] Another advantage possessed by paraldehyde consists in the absence of the period of excitement produced by chloral before the advent of sleep. It is an hypnotic, without narcotic properties, limiting its effects chiefly to the brain, and leaving the spinal cord in a condition nearly like that of natural sleep.
Ether, though possessed of the greatest value as an agent for the production of artificial anæsthesia, is rarely used as a mere hypnotic. Diluted with alcohol and ethereal oil, it forms the Compound Spirit of Ether, or Hoffmann’s Anodyne. In this form it is well adapted for internal administration. It is thus very serviceable in the treatment of those forms of insomnia associated with nervous irritability and hysteria. For the relief of wakefulness dependent upon a languid circulation, with cold feet and flatulence, the anodyne may be given in half-drachm doses well diluted with ice water, and repeated every fifteen minutes till relief is obtained. Nearly all forms of painful or spasmodic disturbance unattended by fever may be thus relieved. For this reason it is particularly useful in the treatment of uterine colic and in sleeplessness after childbirth, when opiates cannot be tolerated, or are contra-indicated on account of their tendency to excite the brain.
Chloroform, like ether, is an agent too powerful and too evanescent for use as a simple hypnotic. But for the relief of intense suffering caused by nervous irritation and spasm it is without any superior. In certain minor affections of a spasmodic character it, therefore, forms a valuable adjuvant to other remedies. Diluted with alcohol it forms the spirit of chloroform,[Pg 82] a remedy which is useful in all cases for which the compound spirit of ether is usually prescribed. In this form it is an excellent addition to various mixtures designed for the relief of spasmodic coughs by which sleep is disturbed. Ringer recommends it in the treatment of the irritative cough so characteristic of fibroid phthisis. It should also be used in cases of spasmodic asthma. The asthmatic paroxysm may frequently be arrested by inhalations of the vapor of chloroform or ether; but, unfortunately, the lungs soon become tolerant of these agents, and they then cease to afford relief. The valuable mixture known by the name chlorodyne owes a considerable portion of its efficacy to the presence of chloroform as one of its ingredients.
Chloral.—Until the recent introduction of paraldehyde, chloral hydrate has for many years held the first rank as an hypnotic. It is particularly useful in wakefulness occasioned by exhaustion of the nervous centres. The conclusions of all experienced observers have been most concisely stated as follows:[45] “Chloral appears to be indicated when sleeplessness is dependent upon a vascularity due to exhaustion rather than to primary excitement of the brain; thus it has been found useful when loss of sleep follows severe and prolonged mental application or excitement of feeling, or accompanies the general debility following acute diseases attended with delirium or severe pain, or is associated with acute mania, especially of the puerperal form. The somewhat analogous condition which exists in delirium tremens is very amenable to this medicine, especially in the forming stage of the affection known[Pg 83] as ‘the horrors,’ and which so frequently follows surgical injuries in drunkards; it is useful also when great nervous excitement and restlessness are associated with extravagant phantasms. Nevertheless, its depressing effects are to be guarded against in this affection as in the different forms of insanity.” This caution is directed against the frequent and repeated employment of the article in chronic cases, on account of the vasomotor paralysis and general cachexia thus induced. It is now claimed that many of these consequences may be avoided by the substitution of paraldehyde in the place of chloral, but it has been shown[46] that similar effects may follow the long continued use of this substitute.
Chloral is usually administered by the mouth in doses, for adults, of twenty to thirty grains, dissolved in sweetened peppermint water. If the first dose does not procure sleep, it may be followed at the expiration of an hour by a second dose of twenty grains. This seldom fails to induce refreshing sleep. When the medicine cannot be tolerated by the stomach it may be given by enema in milk. For this purpose a drachm of chloral should be suspended with the white of an egg in half a teacupful of milk.
Butylchloral hydrate.—This substance has been recommended as a substitute for chloral hydrate, in cases of cardiac weakness, on account of its being less powerful to depress the action of the heart. It is principally useful for the relief of facial neuralgia and hemicrania. As an hypnotic it is seldom used. For this purpose it may be given in a solution like that of[Pg 84] chloral hydrate. For a simple anodyne effect the medicine may be given in five-grain doses, repeated every half hour or hour. As a means of procuring sleep it may be given in doses ranging from fifteen to forty-five grains. Liebreich has given the medicine in drachm doses, and recommended it as an hypnotic superior to chloral hydrate. It is useful in the sleeplessness of headaches, neuralgia, dysmenorrhœa, and chronic phthisis.
Amyl nitrite.—This drug has been recommended for the relief of insomnia resulting from the opium habit. Ringer considers it useful in the flushes of heat and other forms of discomfort which sometimes interfere with the sleep of women during the change of life. It should be inhaled in the form of vapor, from a handkerchief upon which five drops have been poured. The quantity will need to be gradually increased, as the system becomes tolerant of its effects. The stimulant effect of the medicine renders its use in this manner probably less dangerous than the similar employment of chloroform. Unlike the other anæsthetics above mentioned, it causes a hyperæmic condition of the brain, and is, for this reason, a useful hypnotic in cases of aortic obstruction with an insufficient cerebral circulation and consequent wakefulness.
Opium and opiates.—There seems to be no agreement among experimental physiologists regarding the manner in which opium produces its effects upon the body. By some it is ranked as a stimulant; by others it is considered a sedative. These different opinions are probably due on the one hand to differences in the[Pg 85] dose and strength of the opiates employed, and on the other to idiosyncrasies on the part of the individuals subjected to experiment. The soporific effect of the drug appears to result from its direct action upon the substance of the brain. Under its influence the blood tends to accumulate in the veins, and loses its bright arterial hue. Small doses are said to contract the capillaries of the body, while they are dilated by excessive doses of the drug. From this it may be inferred that opium acts, like many other narcotics, as an irritant of the tissues when given in minute quantity, and as a paralyzing agent when a certain relative amount is exceeded. The experiments of Curci[47] indicate that under the influence of irritating doses of morphia the brain becomes hyperæmic.
Opium is a remarkably complex substance, no less than nineteen different alkaloids having been separated from it. Of these, however, only one has stood the test of therapeutical experiment—morphia. Several other constituent alkaloids, notably codeia, have been lauded as hypnotics, but they are, at their best, far inferior to morphia, and may well be omitted from the list of sleep producers. But, though the soporific properties of opium are chiefly due to the morphia which it contains, there are certain points of difference between the action of the two medicines that often render a choice desirable. According to Stillé and Maisch,[48] morphia does not stimulate circulation and the nervous system as much as opium, and its narcotic effects are less decided and speedy, though its after[Pg 86] effects are more enduring. Opium increases the bodily temperature and sense of heat; morphia produces the last effect, but diminishes the temperature. Opium at first increases the frequency of the pulse, while morphia diminishes it. Opium is of the two the less liable to excite nausea and vomiting; hence the superiority of the tinctures and aqueous solutions of opium when nausea is specially feared.
Of all the remedies for the relief of pain opiates are the most effectual. Before the introduction of the alcoholic hypnotics and the bromides, they constituted the principal agents in the treatment of insomnia. Even at the present time they are indispensable for the relief of all forms of sleeplessness dependent upon pain. A combination of chloral hydrate, sodium bromide, and morphine forms one of the most generally useful hypnotic compounds ever employed.
Under ordinary circumstances morphia is the preferable opiate for the relief of insomnia. The sulphate is most frequently employed, but the acetate and the tartrate have been recommended on account of their supposed superiority in the formation of solutions that are unirritating and permanent in their character. The hypodermic method of administration forms the most prompt and efficient mode of procuring the effect of the medicine. It should be given in a dose of quarter of a grain about an hour before the time when sleep is desired. For some patients a longer time is necessary to develop its hypnotic effect. To children the hypnotic dose must sometimes be given at three o’clock in the afternoon in order to induce sleep at nine o’clock in the evening. As the effect of opiates is highly[Pg 87] stimulant to the sweat-glands, and is often productive of nausea, it is advisable to associate atropine with morphine when thus given. For an adult the hundredth of a grain of atropine may be given with every quarter of a grain of morphine. The soothing and agreeable effects of morphia are thus intensified, while its disagreeable tendencies are reduced to a minimum. The injection should be made into the loose areolar tissue between the skin and the muscles. Its location is a matter of little importance so far as the relief of pain is concerned; but the neighborhood of the blood vessels should be avoided, since alarming symptoms have been observed after injection into a vein. The outer aspect of the arm near the insertion of the deltoid muscle is a favorite site for puncture. If, for any reason, the hypodermic use of morphia cannot be employed, it may be introduced into the rectum either in solution or in a suppository. The bowel should first be washed out with an enema of warm water; the opiate may then be introduced. The dose thus exhibited need scarcely exceed that usually given by the mouth; but, if the rectum is not previously cleansed, a double, or even triple, dose may be required.
As an hypnotic morphia is chiefly useful in phthisis, in cardiac dyspnœa, in diseases of the stomach which cause insomnia, in fevers with prostration and delirium, in delirium tremens, in mania, and in the majority of painful or spasmodic diseases. If the patient be violently excited, the opiate should be combined with small doses of tartar emetic, ipecac, or tincture of aconite. But in the chronic diseases it is desirable to avoid its continuous administration, not only on account[Pg 88] of the risk of creating the opium habit, but also by reason of the injurious effects of the drug upon digestion and nutrition.
Codeine is a mild hypnotic which may be used in doses about twice as large as those of morphine. It is expensive and not very efficient, but may be sometimes prescribed with advantage when moral considerations render the use of ordinary opiates inexpedient.
Lactucarium may be classed with the weaker opiates. It possesses very little value. Its fluid extract is sometimes prescribed at night to allay the cough of pulmonary consumption, so as to favor sleep.
Bromides.—According to Mitchell, Echeverria, and Bartholow, the soporific energy of the bromides may be ranked as follows: Lithium bromide first, sodium bromide second, potassium bromide third. Hammond praises calcium bromide. Hydrobromic acid is also employed as an hypnotic in certain cases. As a clinical fact the bromides of sodium and potassium are most frequently employed for the relief of insomnia. Of these the second is most useful when sleeplessness is associated with the phenomena of irritability; the first is less energetic in its effects upon the motor structures of the body.
The bromides act upon the protoplasmic constituents of the body, directly inhibiting their functional energy. Upon the spinal cord they act to diminish reflex excitability. Under their influence the receptivity and functional capacity of the brain is reduced. The minute blood vessels contract in consequence of the inactivity of the tissues which they supply. A lethargic sleep is thus induced.
[Pg 89]For the reasons above stated the bromides find their greatest opportunity for usefulness in cases of over-excitement and exhaustion of the brain. When the cortical cells have degenerated into a condition of irritable weakness, characterized by inordinate instability of substance, the bromides serve to steady the fabric by retarding those movements of disintegration which produce morbid wakefulness. Almost useless in cases marked by active congestion of the brain, they are invaluable in the insomnia produced by excessive mental exertion, care, emotion, worry and fatigue. The wakefulness of hysteria, of asthenic mania, and of sexual excitement, is often greatly relieved by the administration of the bromides. The prodromic stage of delirium tremens, before any violent outbreak, and the wakefulness of convalescence from acute diseases are often cured by their use. Mental disturbances and morbid impulses associated with pregnancy or the puerperal state may be dispelled in the same way. The screaming fits of night terrors in children are benefitted by these medicines. They seem to increase the efficacy of chloral, chloroform, ether, cannabis indica, hyoscyamus, belladonna, and the opiates.
The hypnotic dose of hydrobromic acid is twenty-five grains, largely diluted with sweetened water. For this reason, and for its disagreeable taste, it is not an eligible preparation. Lithium and calcium bromides may be given in scruple doses every hour or two till sleep is produced. Sodium and potassium bromides should be given in doses of thirty or forty grains every two hours.
It is sometimes remarked that instead of favoring[Pg 90] sleep the bromides only increase wakefulness. In such cases opiates and alcoholic stimulants are usually indicated.
Hops.—The principal sedative constituent of this plant is the yellow glandular powder found in the strobiles; this is called lupulin. Hops do not exhibit any directly narcotic property; but they serve to allay nervous excitement, and thus favor the occurrence of sleep. They are principally useful in cases of irritability of the bladder and sexual organs; in dyspepsia caused by irritable weakness of the stomach; and in the exhaustion of delirium tremens. The infusion is the best preparation for internal use. It may be taken in doses of one or two ounces, as required. Lupulin may be given in doses of ten grains or more. Its fluid extract is prescribed, fifteen or twenty minims in sweetened water whenever needed. The best method, however, of securing the beneficial effects of the medicine consists in the administration of a mild beer that is rich in hops. A glass at bedtime often forms a sufficient hypnotic.
Gelsemium is a very powerful agent for depressing the pulse and the functional activity of the spinal cord. It thus favors the induction of sleep in cases attended with violent excitement, such as may be witnessed in acute mania. It has been employed in the treatment of delirium tremens; but the poisonous qualities of the plant render its use somewhat dangerous. The toxic effects are sometimes developed quite suddenly, and in a manner very alarming to the laity. For these reasons it is not to be recommended as a soporific,[Pg 91] unless the patient can be continually under the eye of the physician or of an intelligent nurse.
Conium has been found useful in the insomnia of mania, not through any narcotic property of its own, but by reason of its sedative effects upon the spinal cord and nerves. Under its influence the excitement of the patient is so far reduced that other hypnotic remedies can produce their effect. For this purpose Squibb’s fluid extract, in doses of about one-third of a drachm, or one-sixtieth of a grain of coniine, may be given sufficiently often to repress excitement. The alkaloid may be given hypodermically, and in gradually increasing doses. With it should be associated other remedies, like hyoscyamus and chloral hydrate, in order to procure sleep.[49]
TREATMENT OF INSOMNIA IN PARTICULAR DISEASES.
| Take thou this phial, being then in bed, And this distilled liquor drink thou off; When presently, through all thy veins shall run A cold and drowsy humor, which shall seize Each vital spirit. —Romeo and Juliet. |
Excluding from consideration all cases of insomnia arising from painful injuries or diseases of the external portions of the body, which belong to the province of surgical therapeutics, we may profitably commence with the variety of wakefulness that is excited by disorder of the brain and its membranes. This includes the different forms of meningitis, the cerebral disturbances which constitute insanity, cerebral exhaustion, and chronic alcoholism.
Insomnia in acute affections of the brain.—Acute intra-cranial inflammations may result from general diseases, like rheumatism, the eruptive fevers, tubercular infiltration, insolation, the development of tumors, or syphilitic growths. In all such cases the earlier stages are marked by a painful exaggeration of cerebral function which renders sleep impossible. The wakefulness of this stage soon becomes complicated with delirium; and the whole is finally merged in a fatal coma. Cerebral excitement is the principal[Pg 93] feature which arrests attention. This is accompanied by an inordinate determination of blood to the head, producing that cerebral hyperæmia which figures so largely in the works of the humoral pathologists. The treatment of acute inflammation becomes the best means of relieving this excitement, allaying the hyperæmia, and procuring sleep. The treatment should be derivative, counter-irritant, and calmative. The first indication must be fulfilled by the exhibition of an active purge. Ten grains of calomel with five grains of sodium bicarbonate may be given for this purpose. Leeches or wet cups should be applied to the temples, or to the back of the neck. The feet should be placed for a short time in a hot foot-bath, and an ice-cap must be drawn over the scalp. The internal medication must consist of arterial sedatives and cerebral depressants. For the first, tincture of aconite forms an admirable example—better even than the tartar emetic so much lauded by Graves. Aconite may be given with the bromides. When sleeplessness in an acute meningitis is accompanied by severe pain, an excellent combination will be found in the following:
| ℞ | Morph. Sulph. | gr. ¼ | |
| Chloral Hydrat, | |||
| Sodii Bromid. ā ā | ℨ iv. | ||
| Tr. Aconit., rad. | gtt. xxv. | ||
| Tr. Cardam. Co. | ℨ i. | ||
| Aquæ, q. s. ad. | ℥ i. |
Sig.—A teaspoonful every two hours, till relieved.
As the disease progresses, the quantity of morphia should be reduced. In epidemic cerebro-spinal[Pg 94] meningitis, opiates may be safely employed in much larger doses than are tolerated in the simple forms of the disease. When in doubt regarding the proper hypnotic the bromides alone should be used. Chloral hydrate may also be safely employed in the first and second stages of meningitis; but if given in full doses near the close of the second stage it sometimes seems to hasten the appearance of coma.
Insomnia in insanity.—Persistent insomnia is often one of the premonitory symptoms of insanity. It is likely to present itself as a most formidable complication at any stage of the disease. To consider aright the relations that exist between sleeplessness and insanity would far exceed the limits of this work; we can only review the leading indications for its treatment. It is occasioned either by an excited state of the brain, accompanied by hyperæmia and general functional exaltation, or by an exhausted and irritable condition of the cerebral substance. The first of these two varieties of wakefulness is encountered in cases of violent maniacal excitement where the disorder is comparatively recent, and the bodily vigor has not been depressed by long continued disease. The indications for treatment call for sedative measures. Leeches behind the ears and the application of the ice-cap are sometimes of great service. Derivative action upon the bowels with aloetic purgatives has often yielded good results. In like manner, hot mustard foot baths are recommended. The soothing effect of a warm bath at 90°-95° F. is sometimes sufficient to calm excitement, and to induce sleep. The combined effect of cold applications to the scalp and a warm bath to the[Pg 95] general surface is still more tranquillizing. This method of treatment is particularly useful in maniacal forms of insanity, and in certain cases of melancholia—especially those in which the skin is dry and the secretions are disordered.
Cold affusions and shower baths have been employed for their revulsive and sedative effect in mania. This mode of treatment is sometimes effectual, but is not without risk.
The medicinal treatment of insomnia is frequently facilitated by the measures above indicated. In cases of great excitement with restlessness and bodily agitation, it is desirable to arrest the movements which are wearying the patient and keeping him awake. This may be accomplished by the use of conium, as indicated by Kiernan (loc. cit.). Twenty minims of Squibb’s fluid extract may be given for the first dose. Half this quantity should be repeated every half hour until the patient becomes quite calm. Bromide of potassium and hydrate of chloral in drachm doses should be given in connection with conium. Recently, paraldehyde has been employed as a substitute for chloral. These remedies reduce cerebral excitement, and favor the induction of sleep which is at least refreshing, if not curative of the disease. They should not, however, be used habitually, for fear of producing the characteristic consequences of over-dosing with such drugs.
The varieties of insanity in which depression and exhaustion are the prominent features require different management. Nutritious food, alcoholic restoratives and stimulant doses of opiate remedies are most[Pg 96] serviceable. The sleeplessness of melancholia and of paretic dementia may be thus relieved. Opium may be given in the form of a pill, or in the deodorized tincture. The old fashioned “black-drop” is highly esteemed by some. Others prefer the salts of morphia. If cerebral hyperæmia be present in these cases, it is usually associated with asthenic conditions of the brain, indicated by paleness of the face and weakness of the pulse. The hyperæmic state is then easily overcome by the administration of alcohol or of chloral with an opiate. If opiates alone are given in cases of insanity with great depression, there is danger that death by syncope may occur, precisely as it sometimes happens in delirium tremens when treated with large and frequent doses of opium.
Cases are occasionally encountered which receive no relief from opiates. The remedy seems only to aggravate the existing irritability and insomnia. For such patients the tincture of hyoscyamus may be employed in doses ranging from two to four or even six drachms. Associated with bromide of potassium and hydrate of chloral, it has been used with great success. Spitzka prefers the simple tincture rather than the fashionable alkaloid, hyoscyamia.
Cannabis indica associated with bromide of potassium is a useful hypnotic in cases of moderate depression and excitement. Clouston finds as a result of his experiments that “forty-five grains of bromide of potassium and forty-five minims of the tincture of cannabis indica are rather more than equivalent to a drachm of laudanum as a means of allaying maniacal[Pg 97] excitement.”[50] In his recent work,[51] the same author deprecates the use of opiates in states of depression, and advises the substitution of tincture of cannabis indica (x min.) and bromide of potassium (xx grs.). He also emphasizes the importance of abundant exercise in the open air, as the best hypnotic in every case that can be trusted abroad.
Insomnia in Chronic Alcoholism and Delirium Tremens.—The insomnia of chronic alcoholism is dependent upon the extensive morbid changes produced in the digestive apparatus and in the nervous system by the habitual use of alcoholic drinks. Sleep becomes greatly disturbed and unrefreshing. It is frequently broken by horrible dreams. The successful treatment of this condition requires complete abandonment of the use of alcohol, and a general correction of the condition of the alimentary canal. For the immediate relief of insomnia, full doses of bromide of sodium will be of service. Strong infusions of hops may be given ad libitum. Cannabis indica, in the form of the extract, so as to avoid the use of alcohol in the tincture, is of service. Hypodermic injections of morphia are frequently employed, but should be avoided if possible, for fear of the opium habit. Chloral hydrate is exceedingly useful, but should be given in milk, and as seldom as possible, for fear of adding to the injuries already sustained by the stomach. For the same reason the use of paraldehyde in such cases is quite inadmissable.
When chronic alcoholism has culminated in delirium[Pg 98] tremens, more energetic measures become necessary in order to procure sleep. If the patient be of a vigorous constitution, and if the delirium be very active, tartar emetic with morphia may be given, as advised by Graves. Large doses of tincture of digitalis, sometimes reaching an ounce every four hours, were used by Jones, of Jersey. Capsicum, in scruple doses every three hours, is said to induce sleep in many cases of delirium,[52] especially in exhausted conditions of the circulatory organs. Hydrate of chloral and bromide of sodium, each in scruple doses, may be given every two hours. Opiates should be used with moderation, and all attempts to induce profound narcosis should be avoided. Drachm doses of tincture of cannabis indica and of compound spirit of ether, may be given when a diffusible stimulant must be associated with the soporific. In desperate cases it is sometimes necessary to resort to inhalation of ether, but if sudden death should occur, it would be popularly ascribed to the effects of the anæsthetic. By reason of a certain tendency to death from syncope during this disease, it is imprudent to place such patients under the influence of chloroform or the other stronger anæsthetics.
Insomnia in diseases of the heart and blood vessels.—I can fully indorse the opinion of Ringer regarding the beneficial effects of morphia in the treatment of the wakefulness caused by advanced diseases of the circulatory organs, “In such a case, the comfort afforded by a hypodermic injection is almost incredible.... In cardiac dyspnœa, a sixth of a grain twice or three times a week often suffices, but the dose and frequency[Pg 99] in severe cases must be gradually increased to a quarter of a grain each night. Doctors are often afraid to administer morphia in the case of a patient propped up in bed, with livid ears, nose and nails, with distended jugulars and dropsical extremities, with weak, frequent and irregular pulse. They dread lest the morphia should weaken the heart, make the patient worse, if not kill him outright. This fear is quite groundless,” if the opiate be given in moderate doses. It is the stimulant effect of the medicine that is safe and useful.
When wakefulness is caused by angina pectoris, or by simple cardiac neuralgia, such as sometimes follows excessive use of tobacco, relief may be obtained through the exhibition of alcoholic stimulants, hydrate of chloral, or nitrite of amyl. These remedies act more speedily than morphia, and may be associated with it, to the great advantage of the patient. They should not be habitually used, however, in cases of cardiac exhaustion, as their chronic employment favors accumulation of blood in the right side of the heart, with a tendency to paralysis of the cardiac muscles. It is in stenosis of the coronary arteries, and in aortic obstruction, that nitrite of amyl and nitro-glycerine are most useful. The insomnia that results from the remote consequences of these diseases is often relieved by remedies which assist the circulation of blood. For this purpose digitalis is the most useful stimulant in mitral disease; nitro-glycerine, in aortic valvular lesion.
Insomnia in diseases of the respiratory organs.—Pleuritic pain and its consequent wakefulness may be[Pg 100] relieved with opiates, guarded by appropriate vascular sedatives. Dover’s powder, or morphia and aconite, form excellent examples of the remedies most useful, so long as the lungs are not overwhelmed by excessive exudations into the pleural cavities. Pneumonia and bronchitis are accompanied by wakefulness, in their earlier stages, as a consequence of harassing cough. This may be allayed by the judicious use of expectorants and sedatives. If symptoms of asphyxia appear, indicated by blueness of the lips and nails, opiates should never be given. Respiratory stimulants are then indicated, and sleep must be allured by the use of alcoholic beverages and moderate doses of chloral hydrate, with musk and camphor. The early, irritative cough of incipient pulmonary consumption may be soothed with camphor and opium. Paregoric and a demulcent, like Iceland moss tea, or flaxseed tea slightly acidulated with lemon-juice, form an excellent type of such a compound. But the chronic duration of the disease renders the constant use of opiates undesirable. Chloral hydrate, for the same reason, cannot be given without intermission. It is well in such cases to employ the different alcoholic beverages at bedtime. Inhalation of warm vapor, and respiration of air charged with ether, or carbolic acid, will often quiet an irritative cough. In advanced cases belladonna is useful, to check the profuse sweating and to calm the thoracic pain that hinders sleep. In the later stages of the disease, when relief from suffering is the only end in view, morphia and dilute hydrocyanic acid will often render quite tolerable the few remaining nights of life.
[Pg 101]One of the most distressing forms of insomnia is occasioned by the different varieties of asthma. Dyspnœa is the feature that is common to them all, and is the principal exciting cause of wakefulness. In recent cases, which are characterized by spasm, the various anti-spasmodics are useful. Tincture of lobelia, tartar emetic, and ipecac, are of great service. Inhalations of ether or of chloroform, or of nitrite of amyl, will often cut short a paroxysm; but the nervous system soon becomes tolerant of their action. Chloral hydrate and alcoholic stimulants are less vigorous, and cannot be long tolerated by the stomach, especially if there be a gouty diathesis behind the disease. The fumes of burning pastiles containing nitre and stramonium leaves are often of great service if so breathed as to thoroughly fill the lungs with the smoke. In like manner, the smoke from smouldering nitre-paper, or from cigarettes that have been dipped in an arsenical solution, is sometimes useful. Air charged with ozone has been found curative in some inveterate cases. Hyoscyamus, belladonna, and tobacco, have been recommended. It may even become necessary to employ hypodermic injections of morphia.
If, however, the disease should resist all these anti-spasmodics and soporifics, besides the remedies addressed to the predisposing causes of the malady, the only thing that remains is a change of locality. Many very desperate cases have thus been restored to health and comfort.
Insomnia in renal disease.—In the acute forms of renal disorder this is usually caused by pain and fever. It is, therefore, to be relieved with opiates given in[Pg 102] connection with such arterial sedatives and diaphoretics as each individual case may require. But the tendency of inflammatory diseases of the kidney to merge in uræmia must not be forgotten, and the soporific must be used in such cases with great caution. For this reason hyoscyamus is often preferable to an opiate. In extreme dropsical conditions the measures that are useful for the reduction of anasarca constitute the most efficient means for the induction of sleep. In nephritic colic pain is too severe to admit of any rest while it lasts. The general treatment of colic is all that can occupy the attention until relief is secured. The dyspnœa and wakefulness sometimes experienced in advanced cases of Bright’s disease may be greatly relieved by the judicious use of morphia, very much as in the similar disorder occasioned by chronic diseases of the heart.
Insomnia in diseases of the liver.—Inasmuch as the majority of these diseases interfere with the formation and proper discharge of bile it is desirable to avoid, as far as possible, the use of opiates in the disturbances of sleep that are so commonly consequent upon disorder of the liver. Simple restlessness at night can usually be obviated by the ordinary treatment that is remedial of the disease by which it is caused. But it often happens that hypnotic remedies must also be employed. Hyoscyamus, belladonna, chloral hydrate, and compound spirit of ether, are frequently useful. Sometimes when the evacuations exhibit a deficiency of biliary coloring matter, a grain of opium, with a few grains of calomel, forms a very efficient hypnotic. Alcoholic soporifics are not well tolerated when the[Pg 103] gastro-intestinal mucous membrane is diseased. Biliary colic demands treatment similar to that that is required in nephritic attacks. Warm baths, fomentations, and a broad belt of oiled silk around the body, are very grateful, and are favorable to the induction of sleep. A course of nitro-muriatic acid, internally and externally, is often useful when wakefulness is associated with torpidity of the liver.[53]
Insomnia in gastro-intestinal diseases.—In acute inflammatory conditions of the stomach and bowels, sleep must be invited by the use of opiates. Bismuth and morphia, with hydrocyanic acid, are the favorite means of obtaining relief. Opium in solid form is sometimes preferable when a slowly developed and long continued impression is desired. Warm baths and hot poultices also give great relief.
In all chronic affections of the alimentary canal opiates must be used with great caution, for fear of the opium habit, unless the case be incurable. Cancer of the stomach requires their free use. The milder disorders should be managed largely with hygienic treatment. The diet should be so regulated as to prevent the liberation of gas in the intestines, for their distention in this way is fatal to refreshing sleep. A gentle aperient or a large injection of warm water, often proves itself decidedly soporific in such cases. Catarrhal conditions of the mucous membrane prohibit the entire class of alcoholic and ethereal soporifics. Nervous and atonic dyspepsias are often benefitted by the use of bitter beer, and by drachm doses of brandy or whisky largely diluted. These should be taken at[Pg 104] mealtime, or with food at bedtime. A glass of hot water shortly before retiring is often useful.
The relief of insomnia in dyspeptic derangement, however, must not be sought through the administration of anodynes and hypnotics alone. Only when the entire life of the patient has been regulated upon a physiological basis can refreshing sleep be obtained. Change of habits, change of occupation, change of locality—these are the only curative measures in a vast number of the cases of wakefulness that occur in modern life. Alcohol, tobacco, tea, coffee, foul air, late hours, and mental excitement, are the principal causes which must be abolished before healthy sleep can be enjoyed.
Insomnia in febrile conditions.—In the early stages of all acute fevers wakefulness is a very common incident. It is then occasioned by irritation of the brain, and must, therefore, be relieved with opiates. If the patient is not depressed by the disease, the opium should be associated with tartar emetic or aconite, or ipecac. Dover’s powder is very useful in such conditions. In malarial fevers wakefulness should be combatted with full doses of quinine in addition to the opiate. Gelsemium is sometimes a very satisfactory remedy—especially in the febrile attacks to which children are liable. If any evidence of cerebral hyperæmia be observed, it is well to give chloral hydrate and the bromides. Hyoscyamus, belladonna, and cannabis indica are useful when the pupils are contracted and when spasmodic symptoms are present. Lukewarm baths, wet packs, and cool sponging are exceedingly[Pg 105] grateful, and often assist in the evolution of a suppressed eruption in the exanthematous fevers.
In the later stages of fever a condition of cerebral exhaustion is sometimes encountered. Irritable weakness caused by starvation of the brain is the prominent feature. The pulse is small and weak. The patient tosses and rolls from side to side. He is perhaps greatly emaciated by an illness of considerable duration. An elevated temperature requires frequent sponging of the body.
Opium, alcohol, and liquid food, are the best hypnotics in such cases. The acetum opii and the deodorized tincture of opium are among the best preparations of the drug, by reason of their stimulant effect. The equivalent of two grains of opium with a full glass of eggnogg, will often procure sleep for such a patient. If there be evidence of blood stasis, with blueness of the nails, hypostatic pneumonia, etc., musk and strychnia should be given in place of opium, and the circulation should be assisted with carbonate of ammonia, as follows:
| ℞ | Ammon. carb., | gr. v. | |
| Spt. chloroform, | gtt. xx. | ||
| Aq. camphor, | ℥ ss. |
To be given in a little milk, as required. Chloral and the bromides are of comparatively little value in all cases where there is considerable depression of the vital forces.
Insomnia in rheumatism and gout.—Opium in a diaphoretic preparation, and associated with alkalies or with colchicum, has always been the most approved[Pg 106] remedy for sleeplessness in the acute forms of these painful diseases. Salicylic acid and the salicylates have in great measure superseded the use of opiates for the relief of pain and wakefulness in rheumatism, but they are not always efficient. Opiates, with or without chloral, must then be used. Sometimes a painful case that has resisted all other remedial agents yields promptly to the action of a series of blisters. The chronic forms of rheumatism require the use of stimulant diaphoretics, anodyne liniments containing chloroform and belladonna, and chloral hydrate, or even a Dover’s powder, at night.
Acute gout is rarely seen in this country, but its rudimentary forms, described by Da Costa as lithæmia,[54] are not uncommon. They are associated with wakefulness of a very troublesome character, which only yields to a persistent and long continued course of treatment directed against the diathesis. Careful regulation of the diet, change of air, and anti-arthritic remedies, are of infinitely greater service than any particular hypnotic drug.
Insomnia in syphilis.—In advanced stages of syphilitic cachexia, a variety of wakefulness independent of pain is sometimes observed. It is marked by a tendency to wake at a fixed hour of the night, frequently about two o’clock in the morning, after which time sleep is impossible. The symptoms of constitutional disease are not prominent in these cases, but the history and the evident cachexia make their nature apparent. They usually yield to a mercurial treatment. In their comparative freedom from severe pain, such[Pg 107] patients present a striking contrast to certain cases of syphilitic rheumatism, or neuralgia. The nocturnal suffering in such instances is frightful. It can be finally overcome by anti-syphilitic treatment; but, while waiting for the radical cure, palliatives are needed. Chlorodyne and similar combinations of all the anodyne drugs afford the most effectual means of relief. I have sometimes found it necessary to increase the dose until the characteristic delirium produced by solanaceous drugs was manifested. The relief thus procured sometimes continues for many days after the cessation of hypnotic medication.
Insomnia in various disorders of nutrition.—The wakefulness experienced by syphilitic patients is not peculiar to their cachexia. It is a result of blood disorder and impoverishment that is common among the victims of rheumatism, lithæmia, syphilis, malarial poisoning, cancerous dyscrasia, chronic toxæmia of every form, and ordinary anæmia. Imperfect blood supply deteriorates the nutrition of the brain, and renders it so excitable that sleep is interrupted so soon as the period of profound repose is past. This occupies about four hours (see p. 16), hence the patient who falls asleep at ten o’clock is ready to wake up at two in the morning, and only sleeps again, if at all, when wearied with tossing till daylight. Such patients often derive great benefit from a morning nap thus obtained between the hours of five and seven.
The most successful treatment of this variety of insomnia is that form of medication which is addressed to the particular cause of the cachexia or dyscrasia. But the palliative treatment necessitated by the[Pg 108] immediate suffering of the patient will often tax to the uttermost the ingenuity of the physician. Usually, there is a chronic atonic dyspepsia, or a chronic catarrhal gastro-enteritis, or a combination of both conditions, to be remedied. Gently stimulating laxatives are needed for the relief of these disorders. An animal diet is most easily digested. Milk and rare beefsteaks supply this form of nutriment, to which must be added oranges, grapes and lemons, to prevent the development of incipient scurvy. The kidneys may be excited with small doses of iodide of potassium or chlorate of potassium. Only after a considerable course of elimination are “tonics” admissible. For the immediate relief of the insomnia by which the patient is exhausted, a rather complex method is needful. Such subjects often pass the day in tolerable comfort, but, as evening advances, the wearied brain becomes irritable, and bedtime finds the patient in an excited state which cannot be easily overcome by large and repeated doses of chloral. Paraldehyde is too disagreeable to be used with impunity, and only towards morning does the sufferer yield to the narcotism induced by successive doses of chloral and bromide. A night thus occupied adds nothing to the vigor of the individual, and its frequent repetition will most surely lead to starvation of the nerve-centers,—perhaps to consequent “chloral-mania.”
When the tendency to cerebral irritation becomes thus apparent, great assistance can be obtained by a resort to the use of opium, combined with tartar emetic and camphor. A pill containing one grain each of opium and camphor, with one-twelfth or one-sixteenth[Pg 109] of a grain of tartar emetic, should be given early in the evening. This calms the brain, and prepares the way for a moderate dose of chloral at bedtime. In this way sleep can be procured with much less expenditure of nervous force and medicine than is wasted in the ordinary routine method. The rest thus obtained is followed by less depression than when it follows stupefaction with large quantities of an exciting narcotic.
Insomnia during pregnancy, and after parturition.—Closely akin to the insomnia of anæmia is the wakefulness experienced by hysterical subjects. The irritable weakness of their brains renders them peculiarly liable to disturbances of sleep. The state of pregnancy often serves to fill their nights with excitement sufficient to interfere with quiet rest. Loss of blood during parturition, by the induction of temporary anæmia, may greatly aggravate this condition.
The suppression of nervous irritability is the principal indication for treatment. This may be temporarily accomplished by the use of the bromides. But these must be reinforced by an ample dietary, with stimulant nervines and anti-spasmodics. Good wine, camphor, valerian, hyoscyamus, cannabis indica, and occasional doses of opium, will generally suffice to induce the needful repose. If confinement in bed precludes muscular movement for any length of time, passive exercise must be secured through the aid of massage.
Insomnia in spasmodic diseases.—This class of ailments will usually be encountered among patients who are enfeebled by unfavorable[Pg 110] conditions of health, either congenital or acquired. Together with the specific treatment appropriate to the particular disorder, it often becomes necessary to make use of hypnotic remedies against sleeplessness. Thus chorea may sometimes reach a degree of inveteracy that renders sleep impossible. Alcohol and chloral hydrate must then be given in large and frequent doses. A laryngeal catarrh may excite spasmodic croup—a disorder speedily relieved with chloral hydrate. Old people of a nervous temperament sometimes experience paroxysms of a similar character, interfering with sleep whenever they suffer a catarrhal attack. Liberal doses of assafœtida and a Dover’s powder at night, associated with a course of antilithic treatment, afford great relief. Iodide of potassium, in the majority of asthmatic affections; the bromides and gelsemium in cases marked by excitability of the spinal cord; valerian, musk, assafœtida, camphor, and carbonate of ammonia, in cases of cerebro-spinal weakness and irritability; oxide of zinc, quinine, and chloral hydrate, when weariness and exhaustion are connected with a hyperæmic condition of the brain; such are the principal remedies against this variety of insomnia. Convulsions, if frequently repeated, may be subdued by the inhalation of ether or chloroform, until a sufficient quantity of the bromide of potassium can be introduced into the system.
Insomnia in childhood.—According to Vierordt,[55] the duration of sleep in the first week of life is only interrupted by the act of nursing. During the first month the infant should sleep at least two hours after[Pg 111] each meal, waking only three or four hours out of the twenty-four. This period gradually increases; but, when a year old, the healthy child still sleeps more than he wakes. During the second and third years, he should sleep for ten or eleven hours at night, besides a nap of two hours in the daytime. After the fourth or fifth year, the daily nap may be discontinued. The fifth and sixth years require ten hours of sleep at night. From the seventh to the eleventh year, nine hours are needed. After the twelfth year, eight hours are sufficient.
The causes of wakefulness are as numerous among children as among adults. Jacobi[56] insists upon the importance of attention to the ventilation of the bed-chamber, and to the quality of the bed. Everything must be light, airy and cool. He gives utterance to universal experience when he asserts that great heat can be endured by day without harm, if only the night brings coolness and rest.
Hunger is sometimes a cause of wakefulness among young children. Partial starvation endured for a considerable time induces somnolence. The opposite condition of repletion may also excite wakefulness through painful distension of the stomach and bowels. Earache, terminating in abscess, often prevents sleep, sometimes without discovery of the cause until a discharge of pus enlightens the diagnosis. Persistent wakefulness without evident cause should arouse a suspicion of incipient tubercular meningitis. Slight elevations of temperature at night sometimes occasion[Pg 112] sleeplessness, which may be overcome with quinine in doses of two to five grains at bedtime.
Wakefulness sometimes occurs merely as the result of a bad habit. This is usually observed among delicate children of a nervous temperament, whose inclinations have never been thwarted. Such patients have been sometimes cured, after the failure of a long and expensive course of treatment with homœopathic globules, by the adoption of a systematic moral training reinforced by an occasional forcible application of the parental hand to the gluteal region of the child. Of course such a method must not be recommended without certain knowledge that no lurking disease of the nervous system has escaped detection. Fretfulness and wakefulness are not associated with proper living and good health. Their cause must generally be sought upon the surface of the body and in its internal cavities.
Much relief in the insomnia of children can be obtained from the use of lukewarm baths at bedtime. Supper should be a light but sufficient meal. Every disorder of digestion should be regulated as it occurs. Painful affections may be quieted with Dover’s powder. Feverish and irritable conditions yield frequently to aperients, or to gelsemium and quinine. Night terrors and screaming fits should be calmed with chloral hydrate and the bromide of sodium. As a general sedative and hypnotic for children hyoscyamus has an excellent reputation. It may be given in considerable doses with perfect safety and the best results. For patients in early life it seems to fill the[Pg 113] place occupied by cannabis indica in the medication of adults.
Insomnia in old age.—The highest physical perfection is reached before the fortieth year of life. Between this age and the forty-fifth year man’s vigor begins to decline. The power of accommodation diminishes, necessitating the use of spectacles; adipose tissues begin to load the body; the hair grows thin, and begins to bleach. The processes of nutrition and of disassimilation become more sluggish; the appetites and passions gradually subside. Sometimes the moderation of nervous excitability thus effected permits indulgences of the appetite for food that were impossible during earlier years—the nervous dyspeptic can tolerate dainties which would formerly have been unendurable. Less disturbed by the solicitations of sense, the powers of reasoning and of judgment enlarge their authority. Under favorable circumstances this period of life may continue for about twenty years, when old age develops. From the sixtieth to the eightieth year the progress of decline is rapidly accelerated, and life is normally terminated between the eightieth and eighty-fifth years of existence. The rare examples of greater longevity are too few in number to warrant the assumption that a century of years is the physiological complement of life.
As old age advances, the time of sleep is slightly abridged. The moderated activity of the body requires only a diminished rate of repair to make good the waste of the tissues. Less sleep, therefore, is needed. But the liability of age to the incidence of arthritic diseases, rheumatism, and disorders of the heart,[Pg 114] blood vessels, digestive apparatus, and urinary organs, renders the period of decline particularly subject to those varieties of sleeplessness which depend upon such derangements of health. The nutrition of the brain suffers under such circumstances, and the substance of the organ becomes morbidly irritable. Insomnia among the aged often owes its cause to these unwholesome conditions. The biography of the celebrated Carlyle affords numerous illustrations of this variety of wakefulness. Disease of the cerebral blood vessels sometimes originates a series of changes differing only in degree and intensity from the classical type of chronic periencephalitis. This is characterized by many of the minor phenomena of general paresis, only occasionally rising to the level of that disease. Wakefulness is one of the most troublesome symptoms of this disorder. Its management requires attention to all the details of excretion and nutrition. The diet must be carefully selected with reference to failure of the digestive function. Milk and water should be preferred for drink, and the great emunctory organs of the body must be carefully stimulated and sustained. A judicious choice of climate may accomplish much for the comfort of the patient. The mild, insular climate of Florida, or of New Providence, or of the Sandwich Islands, affords superior advantages for the relief of sleepless sufferers in the northern temperate zone of the American continent, who need the soothing influence of a continual open air bath.
During the latest stages of decline, when the cortex of the brain has become considerably atrophied, the opposite of wakefulness is experienced. Intellectual[Pg 115] operations become less vigorous, and the patient passes lengthening periods of time in sleep. This is a genuine relapse into the apathy of infancy. The apparatus of thought is worn out, and the old man sinks gradually into the sleep from which there is no awakening.
The treatment of insomnia, therefore, resolves itself into the removal of all special and temporary causes of wakefulness, with attention to the general hygiene of the patient, and careful regulation of his diet, habits, and occupation. Pain must be quelled with anodynes. Cerebral excitement must be calmed, in sthenic cases, with anti-spasmodics and sedatives—in asthenic subjects it must be overcome with food and nervous stimulants. Since many patients present a combination of these apparently opposite conditions, there is room for a great display of penetration and tact in the management of complex cases. While seeking for the immediate relief of present suffering, the ulterior consequences of treatment must always be kept in view, and the particular cachexia or dyscrasia must be thoroughly appreciated by the physician in his choice of remedies.
DREAMS.
| Behold, this dreamer cometh! Genesis, XXXVII, 19. |
The harmonious activity of all parts of the nervous system is indispensable to the highest exercise of the conscious mind. Healthy intellectual life is the perfectly balanced outcome of the complex polygon of forces which has its seat within the brain. In the waking condition this “moving equilibrium,” as it has been happily termed,[57] is sustained by the convergent impulses which are continually entering the brain through the pathways afforded by the several senses. Our waking hours are occupied with the ideas and with the associated trains of thought which are thus projected upon the field of consciousness. As a consequence of the harmonious function of the organs of sense, each one supplementing and correcting the information furnished by the others, a continuous process of perception and logical thought is maintained. But, along with the procession of ideas which are clearly conceived by the mind, the field of consciousness is also invaded by a cloud of half formed perceptions, which are too imperfect and fleeting to occupy the attention. As in the act of vision, though the[Pg 117] periphery of the visual field is crowded with a whole world of objects dimly perceived without challenging particular attention, only the center of that field furnishing clear images to the brain, so the eye of the mind comprehends only a few of the impressions which enter the sphere of consciousness. The swarm of unnoticed perceptions, however, is none the less the result of abiding sensory impressions graven in the substance of the brain, from which, through the action of memory, they may at any favorable moment reënter consciousness. Sleep does not wholly arrest this process. A certain amount of projection into the field of consciousness continues, even during profound repose; and the ideas thus aroused form the material of our dreams.
It has already been remarked that the invasion of sleep is not an instantaneous process. One by one the senses fall asleep, and long before the final cessation of their activity, sleepiness hinders their function. Hence a progressive narrowing of the range of external perception; hence a reduction of the vividness of impressions derived from the outside world; hence, also, a simplification of the actions and reactions which constitute the “polygon of forces” active within the brain. But the suppression of certain lines in this polygon does not suppress life, nor does it necessarily destroy consciousness. It only occasions a redistribution of force, and a proportionate narrowing of the stream of related ideas. Since this process of suppression, just mentioned, is not an absolute quantity, but a variable factor, the polygon of physical forces within the brain and the corresponding succession of[Pg 118] ideas in consciousness must necessarily be in a state of continual change. Consequently, our dreams must be as variable as the clouds that drift upon the currents of the air. As, on a hot day in summer, when the equatorial draught has ceased to guide the wind, we may observe all manner of local tides among the masses of vapor which arise from the earth, so, in sleep, when the guiding influence of the senses is withdrawn, the ideas that still arise are chiefly dependent for their origin and association upon the automatic and endogenous activities of the brain. Undisturbed by impulses from the external world, the brain seems then to become more sensitive to impressions that have their origin within the body. An overloaded stomach, an enfeebled heart, a turgid sexual apparatus, or an irritable nervous ganglion, may become the source of irregular and uncompensated impulses which, without disturbing the organs of special sense, may invade the cerebral cortex, and may there set in motion a whole battery of mechanisms whose influence upon consciousness would remain quite unnoticed were the external senses in full operation.
Still another cause for the production of dreams is to be found in the more or less complete suspension of the power of volition which accompanies sleep. Every act of attention is the result of exercise of the will. But the perfect exercise of the will is dependent upon the perfect development and wakefulness of the brain. So soon as sleep begins to invade the brain, the will begins to lose its normal incitement to action, and finally it becomes almost wholly disconnected from the muscular organs. In this state the sleeper may desire[Pg 119] to perform some act—he may wish to move his limbs or to cry out aloud, but he can move neither hand nor foot, he cannot utter a sound. In other instances a partial connection between the will and the locomotive organs persists, and various orderly movements can still be produced. In like manner the control of the will over the succession and association of ideas may be either wholly, or only partially, lost in sleep. The deeper the sleep the more complete the loss of such control; hence the greater incoherence as well as feebleness of impression which is characteristic of dreams when sleep is profound. The vivid and panoramic succession of visual conceptions which constitutes a “vision,” occurs during light and partial sleep, when the will is still capable of in some measure guiding the procession of ideas.
For a similar reason the higher faculty of judgment, and especially the power of arriving at moral conclusions, is in great measure suspended during sleep. Like the power of volition, the activity of the moral sense is dependent upon a certain functional perfection in the brain. When the capacity of the brain is depressed by drugs or by disease, or by sleep, the moral sensibilities are the first to disappear. Hence the non-moral character of the impressions usually experienced during the act of dreaming. We feel neither surprise nor regret at the incidents of ordinary dreams. It is only when the border line of wakefulness is reached that the dreamer feels ashamed of walking naked in his dream, or feels compunction for an act of crime, or experiences emotions of joy or sorrow in connection with the incidents of his vision.
[Pg 120]A dream may, therefore, be defined as the occupation of the field of consciousness during sleep by a succession of ideas more or less completely withdrawn from the guidance of the senses and from the control of the will. A great variety of dreams may thus be admitted, ranging all the way from those products of mere absence of mind which constitute revery, down to the faintest and feeblest stirrings of consciousness which have been always observed during the act of waking from the profoundest sleep.
Considerable light may be thrown upon the production of dreams if we consider attentively the manner in which illusions and hallucinations are excited by the use of drugs or by disease during the waking state. When engaged in experimenting upon myself with different medicines, I once took a dose of hasheesh sufficient to produce the peculiar effects of the drug. Sitting quietly in my chair, the first unusual sensation was an agreeable feeling of coolness diffusing itself over the surface of the body, as if some one were gently fanning me on a hot day. A feeling of causeless amusement began to occupy my mind. I seemed to be smiling all over without any apparent reason for hilarity. Then the walls of the room in which I sat seemed to recede to a vast distance. My attention became riveted upon a little picture which hung against the wall before me. It was a sunset scene, painted upon a canvas scarcely larger than my hand. As the wall upon which it was placed seemed to recede, the canvas expanded until I beheld a glorious landscape bounded by a range of snow-capped mountains flushed with purple light from the setting sun. As I sat,[Pg 121] admiring this splendid scene, the gilded frame of the painting became alive with winged fairies and cherubs, peeping out from behind the moulding, and bending over its margin to look into the picture. Then the ceiling of the room and the sky of the picture seemed to blend in one common expanse of ethereal blue; the sunlight faded from the mountain peaks; stars began to appear in the firmament; the little imps and fairies disappeared; and, presently, everything resumed its natural appearance.
In this experience the departure from healthy cerebral function consisted in an exaltation of certain forms of sensibility while others were depressed. The succession of visual images was initiated by the visible objects around me, but it was enriched by the association of ideas furnished through the stimulation of memory. The sunset glow, the snow-capped mountains, the starry sky, were familiar objects, suggested from memory by the items grouped in the picture. In like manner, the cherubs who climbed upon its gilded frame were merely the glorified products of memory, probably suggested by the fact that it was a picture upon which my attention was fixed—one picture reminding me of others which I had seen. The loss of proportion in the view—the exaggeration and distortion of all the relations of time and space, which made the unreal seem real, and conferred grandeur upon commonplace objects, was undoubtedly occasioned by a modification in the molecular structure of the organs of special sense and of perception under the influence of hasheesh. The change thus effected was of a character to diminish the force of sensory impressions[Pg 122] derived through the aid of the muscles and nerves of the eye and the ear and the skin, while at the same time exaggerating the processes of memory and association in connection with impressions originating within the brain. In this way was produced a sort of confusion between the external world and the ideal world within, rendering it difficult to distinguish the one from the other. Hence the impossibility of estimating aright the relation of time and space to the visual impressions upon which attention was fixed. The result was a waking dream which differed from ordinary revery chiefly in the intensity of the impressions that occupied the mind.
A somewhat similar process is sometimes experienced as a consequence of cerebral disorder unconnected with the effects of drugs. During the invasion of measles, having taken no medicine but sage tea, I remember, as night approached, a strange succession of illusions. My head seemed to expand to the size of a bushel basket; then it would slowly contract again. My body seemed to grow out of shape into the most distorted forms of rickets. Audible sounds seemed to come from the most remote distances. Impending shadows of a great darkness hovered over the bed. Waves of heat, and tingling darts of numbness traversed my limbs. These singular and rather uncomfortable sensations continued until relieved by an ordinary Dover’s powder.
In this experience the confusion of ideas, though less agreeable, was essentially similar to that occasioned by the action of the hasheesh. In both cases there was the same diminution of the intensity of[Pg 123] external sensation accompanied by an exaggeration of internal impressions. The brain and the nerves were in a condition of irritable weakness, caused by disease, which interfered with the normal generation and association of ideas. Having thus partially escaped from the control of the senses and the will, the mutilated succession of ideas which reached the field of consciousness could only be perceived as a series of illusions. Here, again, was a waking dream, of origin and course analogous to the illusions and hallucinations which accompany every form of delirium.
It is not alone under the influence of disease or of drugs that the automatic action of the brain furnishes ideas for the inspection of the mind. Riding, one day, in a street-car, and reading a philosophical work, I came upon a paragraph devoted to a discussion of the doctrine of the association of ideas. Immediately, out of memory, flashed a momentary vision of the quarter deck of the old frigate, United States, upon which appeared the figure of a very small midshipman, talking to a gigantic personage, the captain of the ship. This was an incident which I had actually witnessed forty years before. I was, at first, somewhat puzzled in the attempt to account for the occurrence of a vision so apparently incongruous with the subject matter of the book; but a little reflection convinced me that the exciting cause of this seemingly involuntary act of memory was really the idea of association suggested by the book. This had unconsciously aroused the apparatus of association in the brain, and the particular scene thus brought before the mind had been further suggested by the circumstance that the last object,[Pg 124] external to the printed page, upon which I had fixed my attention, was a large ship, lying in the river, near the bridge, just crossed by the car in which I rode.
Numerous other examples of a similar character might be related to illustrate the fact that the brain is a reservoir of sensory impressions, some of which, at the moment of their original incidence, have aroused the mind to a greater or less degree of conscious attention, and have then all lapsed into a latent or potential condition. But, though latent, they are none the less persistent, and only await the suppression of other inhibitory forces to become once more capable of arousing attention. Such inhibitory impulses are continually furnished by the action of the sensory organs on the one hand, and by the energy of the mind upon the other. So soon, therefore, as the organs of sense and of voluntary impulse are sealed with sleep, if the remaining portions of the brain are still operative, and are left to their own unrestrained activity, a more or less disorderly series of ideas occupies the mind. This constitutes a dream. The difference, therefore, between waking thought and a dream is analogous to the difference between a page upon which the words have been arranged in a rational order, and another page upon which some of the same words have been set down at random. Inasmuch as the majority of our sensations are derived through the organs of sight, and since the larger portion of the sensory region of the cortex of the brain is concerned in the act of vision, it is no more than might be expected that the ideas suggested in sleep should generally proceed from the visual apparatus of the brain. The superior power of visual[Pg 125] impressions to attract attention may also serve to explain the fact that the majority of dreams are composed of images that were originally perceived in the act of vision. Hence our dreams, for the most part, constitute a series of pictures undisturbed by sound, or by other forms of sensation. But this is not always so. It is highly probable that when the organs of external sense are allowed to sleep without disturbance, our dreams consist of visual impressions alone. But, if any unusual sound, or smell, or other sensation is experienced during sleep, it may penetrate the field of consciousness, and may become the starting point of a dream quite filled with sounds. Thus a young lady, who had passed the evening at a musical concert, was aroused, soon after retiring, by the striking of a clock which had been recently placed in her chamber. At the moment of waking, she was dreaming of an orchestral performance of Wagner’s music. Doubtless the dream was suggested by the unaccustomed sound of the clock.
The possibility of thus suggesting, and in some degree guiding, the form and course of a dream, has been often demonstrated.[58] One of my early schoolmates, a boy of remarkably susceptible nervous temperament, furnished an excellent example of this species of direction. Tickling his nose with a straw made him dream that a dragon-fly was assaulting his face. On another occasion, a few drops of vinegar placed upon his tongue caused him to dream of eating oranges. Again, one of his companions roguishly breathing in his ear the statement that the schoolmaster was after[Pg 126] him with a long rattan, he bounded out of bed, and could scarcely be restrained from bursting out of doors in his evident alarm. I was myself awakened, one night, by the ringing, as it seemed, of my doorbell; but, hastening at once to the door, no one was there. As I was expecting a call from a certain patient, I concluded that the bell had been rung by an impatient messenger who could not wait. Falling again asleep, I was a second time startled by a similar ring. Looking out of the window above the door, it was evident that no one was there. I finally concluded that the sound must have been perceived in a dream, and I recalled the fact that each time, as I woke, the sound of a carriage, passing the house, had attracted my attention. Undoubtedly, the state of expectancy in which I was sleeping had operated as the predisposing cause of dreaming, and the noise of wheels upon the pavement had served as the exciting cause of a dream in which the sound-vibrations communicated to the brain had produced by an association of ideas the particular perception which, though asleep, I was waiting to receive.
In certain cases the impression produced by a dream is so vivid that a considerable time after waking must elapse before it can be relegated to its true position in the world of hallucinations. Dreaming, once, that my wife called to me from another room, I instantly awoke; and only the fact that she was with me could satisfy me that it was all a dream. Taine[59] relates that “M. Baillarger dreamed one night that a certain person had been appointed editor of a newspaper; in the morning[Pg 127] he believed it to be true, and mentioned it to several persons who were interested to hear it;—the effect of the dream persisted all the forenoon, as strongly as that of a real sensation; at last, about three o’clock, as he was stepping into his carriage, the illusion passed off; he comprehended that he had been dreaming.”
The following incident from the experience of Prof. Jessen, physician to the insane asylum in Homheim, near Kiel,[60] still further illustrates this form of hallucination:
“On a wintry morning,” writes the professor, “between five and six o’clock, I was aroused, as I thought, by the head nurse, who reported to me that some people had come for one of the male patients, and who at the same time asked me whether I had any particular orders to give. I replied that the patient might depart, and after he had left the room I turned around to go to sleep again. All at once it struck me that I had previously not heard anything regarding the intended departure of this patient, but that only the prospective departure of a woman of the same name had been reported to me. This compelled me to inquire more particularly after the circumstances, and accordingly I lighted a candle, rose, dressed myself, and went to the room of the head nurse. To my surprise I found him only half dressed, and, in reply to my inquiry after the people who had called for the patient, he said, with an expression of astonishment, that he did not know anything of it, as he had but just left his bed, and no one had called him. This answer did[Pg 128] not arouse my consciousness, but I rejoined that then the steward must have been in my room, and that I should accordingly go to see and ask him regarding the matter. When descending a few steps in the middle of the corridor which led to the room of the steward, I suddenly became conscious of having dreamed only what until that moment I had believed to be an experience whose reality I had not doubted in the least.”
In some instances the fact of having dreamed is never recognized, and the dreamer carries through life the delusion that his vision was an actual occurrence. Among the Indians of Guiana, and the same thing is true of many other savages, dreams are looked upon as actual events in which the dreamer is visited by spirits or even by other living men. A recent English traveler[61] says: “It becomes important, therefore, fully to recognize the complete belief of the Indian in the reality of his dream-life, and in the unbroken continuity of this with his working life. It is easy to show this belief by many incidents which came under my notice. For instance, one morning, when it was important to me to get away from a camp on the Essequibo River, at which I had been detained for some days by the illness of some of my Indian companions, I found that one of the invalids, a young Macusi, though better in health, was so enraged against me that he refused to stir, for he declared that, with great want of consideration for his weak health, I had taken him out during the night and had made him haul[Pg 129] the canoe up a series of difficult cataracts. Nothing could persuade him that this was but a dream, and it was some time before he was so far pacified as to throw himself sulkily into the bottom of the canoe. At that time we were all suffering from a great scarcity of food, and hunger having its usual effect in producing vivid dreams, similar effects frequently occurred. More than once the men declared in the morning that some absent men, whom they named, had come during the night and had beaten or otherwise maltreated them; and they insisted upon much rubbing of the bruised parts of their bodies.”
It is highly probable that from these facts, and from others of a similar character, may be derived the true explanation of many of the supposed examples of intercourse with divine or angelic persons which occupy so important a place in early mythology. An incident in the childhood of the prophet Samuel can scarcely admit of any other interpretation. In other cases, notwithstanding the intensity of the dream, its true character is recognized by the dreamer during the very act of vision. Thus, I once dreamed that I saw a young girl standing before me. So vivid was the perception, that the actual presence of such a person could not have produced a more perfect impression upon the waking brain. Yet, at the same instant, I comprehended the fact that it was merely a dream, and remarked the difference between the intensity of the visual image in this and in other dreams. Such speedy recognition of the hallucination does not always accompany the act of waking out of a dream. In some cases, as we shall have occasion to see, the images[Pg 130] which have figured in a dream are still perceived for a certain period of time after awaking.
The majority of dreams are composed of visual images. The dreamer looks upon a picture which changes silently before his eyes, without appealing to any other sense than that of sight. But in certain cases any other sense may become excited, producing illusions or hallucinations as perfect as the images of healthy vision. They may be suggested by external impressions, as in my dream of a ring at the door bell, which proved to be an auditory illusion excited by the sound of passing carriage wheels; or they may, at least apparently, find their starting point in accidental states of the bodily organization. If attention be paid to this matter, it will be observed that all unusual modes of dreaming, and all extraordinary vividness of dream-impressions can be connected with some departure from the physiological conditions of quiet sleep. Either disease, or exhaustion, or emotional disturbance, or narcotic intoxication of the brain may be noted as the immediate cause of such derangement of the cerebral functions. After drinking several cups of coffee before retiring, I dreamed of a large yellow flower which exhaled a very fragrant odor. During the same night I also dreamed of drinking wine, which agreeably excited the senses of taste and of smell. Upon another occasion, having been disturbed by the entrance of burglars into my house, I dreamed that a burglar was fumbling under my pillow, and was raising my head and shoulders with the mattress upon which I slept. I seemed to feel the changes of pressure and of contact as distinctly as if awake. The connection[Pg 131] of voluptuous illusions with erotic dreams is too familiar to require particular mention.
Dreams are not always limited to the revival and combination of the images of sensation. Intellectual combinations are sometimes thus presented to the mind. The most familiar illustrations of this fact are furnished by the experience of mathematicians who have worked out mathematical problems in their dreams. One of my patients, an expert book-keeper, dreamed of adding up six columns of figures at once. In the morning he still remembered his dream; and, on adding up the columns, found that he had actually produced the right sum in each case. A college student of my acquaintance, who was puzzled by a geometrical proposition, wrote out the correct solution during his sleep. This was something more than simple dreaming; it trenched upon actual somnambulism. Another acquaintance dreamed of being in heaven, and, while there, experienced relief from doubt regarding certain theological doctrines which had previously exercised his mind. I have myself composed several sentences during the course of a dream, and have, while dreaming, sometimes esteemed them worthy of preservation; but my waking recollection has never coincided in this particular with the opinions formed during sleep.
Great difference between dreams may be remarked in their coherence and continuity of evolution. Some are composed of the most inconsistent elements without order or logical arrangement. In others the incidents follow very closely in the line of a natural and rational development, so that the dreamer seems to be present[Pg 132] as a spectator of a perfectly coherent drama. It is probable that these differences depend upon variations in the degree of completeness with which the different parts of the brain and of the body are overwhelmed by sleep. If different and widely separated portions are sufficiently wakeful to suggest ideas to the mind, the resulting congeries will consist of discordant and incoherent elements. But if wakefulness is limited to a particular organ of the body or to a circumscribed territory of the brain, the resulting impressions in consciousness should be correspondingly restricted, and will manifest a more orderly connection with each other. In some cases a tendency to simultaneous wakefulness of particular portions of the cerebral register seems to become habitual, so that the same set of ideas may be often renewed in the same order during sleep, constituting a repetition of the same dream. In this way I have frequently dreamed of a volcanic eruption of molten lava from a lofty mountain. This frequent revival of the same train of images is probably due to the fact that in childhood I actually witnessed a volcanic outbreak, and that a very highly colored picture of Vesuvius in eruption hangs in my sitting room, so that my brain has become profoundly impressed with this particular image. When other portions of the brain are asleep, if the special region concerned with this picture be aroused, the mind receives the same impression which it received when first excited by that portion of the organ of memory.
As a general thing, however, dreams do not possess any such compactness
and coherence. They are usually derived from many different portions of
the[Pg 133] cerebral organ, even when they seem to exhibit a fluently connected
course. Thus, I dreamed, one night, that I was walking in a garden filled
with peculiar oriental shrubbery. In this garden I discovered one of my
brothers and a friend, who is widely known in literary circles, engaged in
flying a kite. With great adroitness they had succeeded in causing the
kite-string to describe in the air the outline of the letter Z. I
congratulated them on the adoption of so truly scientific a method of
kite-flying; telling them, also, that I had once succeeded in making a
kite-string describe a fourth line, thus:  As they expressed
surprise at this, I told them that in the May number of the Atlantic
Monthly, for 1883, they would find an article on this method of
kite-flying, written by Oliver Wendell Holmes.
As they expressed
surprise at this, I told them that in the May number of the Atlantic
Monthly, for 1883, they would find an article on this method of
kite-flying, written by Oliver Wendell Holmes.
Nothing can seem more absurd than such a sequence of ideas. They follow each other without a break, yet without any logical coherence, very like the order in which ideas arise to occupy the mind of an insane person. Indeed, such dreams suggest the doctrine that the condition of a dreamer’s brain is functionally identical with what obtains in certain forms of insanity. At first sight it would seem as if such a dream could have no possible basis in fact. But a brief retrospection enabled me to trace each individual item to its source in memory, and I was able to construct the following key to the vision: During the previous evening I had been examining a number of East Indian photographs. Among the most remarkable of them was a picture of the glorious gardens of the Taj, at Agra. Another represented the ruined Buddhist[Pg 134] tower at Sarnath, a structure remarkable for the numerous triangular figures carved as ornaments upon its sides. Hence the garden and the zigzag kite-string in the dream. During the day before, while conversing with a neighbor regarding the financial misfortunes of an acquaintance, I had remarked that if he had stopped kite-flying, and had settled down to legitimate business at last, he would doubtless do well in the future. Hence the kite. I had recently received an interesting letter from my literary friend in which he had mentioned my brother. Hence the two principal actors of the dream. Just before retiring, that night, I had discussed with my wife the subject of subscribing for a number of periodical magazines. Hence the Atlantic Monthly; and, as the celebrated Oliver Wendell Holmes was the author most intimately associated in my mind with that periodical, his introduction among the characters of the dream followed most naturally in accordance with the law of the association of ideas.
The question is continually asked, why are certain dreams so vivid and so easily remembered, while others are of the faintest and most evanescent character? My own experience leads me to believe that there is a morbid element underlying all unusually vivid dreams. It is not merely because of differences in the depth of sleep. The flitting fancies which occupy the introduction and the termination of sleep, rarely possess any power to fix the attention or to linger in memory. But, if the body be disturbed by anything which causes a departure from the even course of health, such as follows unusual or violent emotion, or an attack[Pg 135] of illness, or an insufficient alimentation, or great and sudden changes of atmospheric pressure, the visions of the night become wonderfully exaggerated in every particular. During a voyage at sea, while suffering considerably with thirst, one night I dreamed that a fountain of sparkling water suddenly appeared before me. A young girl dipped a pitcher in the flowing stream, and held it out, all dripping with delicious coolness, for me to drink. Pressing eagerly forward, I awoke, to find myself sitting up in my narrow berth, with hands extended for the draught. Every narrative of shipwreck is filled with similar experiences. Slow starvation is always accompanied by dreams of singular intensity and persistence. As an illustration of the corresponding influence of previous emotion, I may cite the experience of a friend who had been greatly shocked by reading the account of the manner in which the lunatic, Freeman, had killed his little son in imitation of Abraham’s contemplated sacrifice of Isaac. This gentleman dreamed that he was about to sacrifice his favorite daughter. He called her to him; told her that he was about to cut off her head as a religious sacrifice; and took up the knife for that purpose. She exclaimed, “Oh, papa! I have never disobeyed you yet!” and extended her neck, to receive the fatal stroke, when he awoke, trembling in every limb, and drenched with perspiration. For a long time the horror of this dream affected him as terribly as if it had been an actual experience.
It is usually difficult to arrive at any exact estimate of the time occupied by a dream; but it appears certain that in some instances the succession of images[Pg 136] excited during sleep must be exceedingly rapid. Abercrombie, in his work on the “Intellectual Powers and the Investigation of Truth,” p. 275, has related several illustrative examples of this fact. In my own experience, one night, as I lay half asleep, I heard the watchman on his round, as usual, examining the fastenings of my front door. At once I began to dream that I was revisiting my father’s house, the home of my childhood. The family were at breakfast in the front parlor, while I walked through the back rooms, examining the doors and the windows, and found it impossible to close and to fasten them. I then took a bath, dressed myself, and walked out into a large garden behind the house. It was filled with tropical trees, of which some were young. The old ones, which I recognized after an absence of thirty years, astonished me by their surprising luxuriance. A lovely, trailing convolvulus, in full bloom, attracted my admiration. After walking for some time I came upon a plum tree which was very small when I left home, and had now reached a height not exceeding twelve feet. This slow growth excited considerable surprise on my part. Returning to the house, I passed the day with my parents, and, at night, undertook to shut up the house, but could not fasten any of the doors or windows. This caused me great uneasiness, for there was a large gypsy camp not far from the east end of the building. My anxiety was presently justified by a noise in the parlor. Hastening to the door, and looking into the room, I saw a large painting disappearing through a hole in the wall next to the encampment of thieves. I immediately cried out, to frighten away the robbers; and was awakened[Pg 137] by my wife, shaking me, and asking what was the matter, just in time to hear the watchman walking down the front steps, after the completion of the investigation which had suggested my dream.
Another experience may serve to illustrate the fact that dreams are greatly intensified by illness, and that their duration may be exceedingly brief. Suffering, one night, from an attack of intestinal colic, marked by a rapid succession of painful paroxysms, between which, however, I fell asleep without the aid of medicine, I dreamed in one of these snatches of slumber that I was walking with my brother on the road to the volcano of Kilauea. In my hand were four diamond shirt buttons. They were white, and were covered with fine asbestos wool. My brother’s wife expressed serious doubts regarding their value; but I at once reminded her that the Emperor of China had given to the English Ambassador, for presentation to the Queen of England, a number of diamonds which were so rough and so cheap in appearance that the ambassador, who was also a marquis, could not suppress his contempt as he received the gift. But, when carried to London, and cut by the royal jewelers, their brilliance had astonished everyone. I now desired to deposit my diamonds with a jeweler, for safe-keeping. My brother recommended a house near the volcano, but I had seen another, a few squares further up the road, and accordingly resorted thither. Not finding any satisfactory evidence of business, I retraced my steps to the place first recommended. Entering the door, I found myself in a narrow room, with a long, low counter on one side. Behind this were several[Pg 138] men, and several cases filled with jewelry. I handed my buttons to a large, good-looking fellow, who was bustling around in his shirt-sleeves. He immediately put one of the jewels into his mouth, when I heard something crack, as if either his teeth or the diamond had split. Consoling myself with the recollection that, if broken, a diamond could be mended with cement, I asked for a certificate of deposit. While this was being written, the entire building slipped away from over us, and glided down the slope of the mountain, towards the ocean, leaving us, and all that had been within the house, uncovered in the open air. This did not disconcert any one. The jeweler finished his writing; I pocketed the receipt, and with my brother pursued our walk through the mountain forests beyond the crater of the volcano. Presently we arrived at an eminence from which we could look down upon the ocean, and could see the line of the coast prolonged for many miles on either side of a cape of land. The western coast was very grand—mountain promontories rising behind each other as far as the eye could reach. Having feasted our eyes with this magnificent panorama of earth and sea and sky, we turned away in the direction of a grove, in which was visible a large building of stone, with castellated walls, and turrets with pointed roofs at the corners. My brother informed me that this was a German settlement, called Little Clacius. Approaching the castle, we were received in a magnificent hall by a beautiful woman who offered to conduct us through the building. She led us through a series of lofty rooms, splendidly painted, gilded, frescoed, and furnished with inlaid tables and polished[Pg 139] chairs. On either side were ranged large vases, in which grew what I seemed instinctively to recognize by the name of the Lace Mimosa—each plant consisting of a flat sheet of green lace-work, like a coralline, studded with lovely pale yellow blossoms. Passing through three such rooms, we entered a fourth, across the floor of which our fair guide whirled herself with a pirouette into the presence of a young woman clad in a richly figured dressing-gown, drawn lightly around her form as she sat in an easy chair, nursing her baby. We were formally introduced to this lady, who received us with the most evident indifference, a circumstance which gave us no concern, for the view from the open window at once engrossed my attention. Directly before me was a shining river, pouring down the mountain side and falling about fifteen feet into a deep dark pool that widened beneath the window from which I gazed. High banks, covered with magnificent trees, sloped down into the water, and cast their shadows across its rippling surface, forming a most charming landscape. The breadth of the scene, the depth of the coloring, the perfection and the multiplicity of all the details that pressed upon the attention, could not have been surpassed in vividness by any real existence. I was admiring the view, and was beginning to feel surprised that so large a river could exist in such a place, when I was suddenly awakened by a renewal of the intermittent pain.
In this example each individual detail could have been easily traced to its source in memory. Pictures, and actually existent scenery furnished the detached items which were combined in a brain that for the time[Pg 140] being was released from the control of the reason and the will. Irritated by painful sensations the brain was inordinately excitable, and sleep was less profound. Hence the remarkable intensity of the pictures which were presented to the eye of the mind. The indescribable richness and variety of the vision was probably due to the fact of extensive bodily disturbance, opening a wide range of territory from which impressions were communicated to the morbidly sensitive brain. The unusual permanence of the whole dream in memory may be explained by the observation of Maury, that the ease with which dreams are recollected varies inversely with the depth of the sleep in which they occur. Dreams which are produced in sound sleep are seldom recalled after waking, because they are but slightly connected with impressions received by the brain during wakefulness.[62] But dreams which occupy the mind when sleep is light and partial are excited by cerebral movements which are closely associated with external impressions that originate either at the moment of awaking or immediately after that event; consequently, the bond of union between the ideas of the dream and our waking ideas is nearly if not quite as perfect as the bonds which serve to connect the thoughts that occupy any portion of our conscious life. Hence such dreams are more easily reproduced from memory by any disposition that arouses a retrograde association of ideas.
The dream above related, though excited by an unhealthy condition of the body, was not at all disagreeable. But it is often the case that disorders of[Pg 141] particular organs serve to originate visions with special and evident characteristics related to their source. Thus, one of my patients, during an attack of uterine and hemorrhoidal congestion, would dream that a heavy weight had been laid upon the lower part of the abdomen. On another occasion, having gone to sleep, apparently in perfect health, she dreamed of a terrible pain in the head, and that her husband and a physician were applying a cupping glass to the back of her neck. This woke her up, and she found that she was actually suffering with a very severe headache. Another lady, shortly after confinement, dreamed that her baby had teeth, and that it was biting her nipple. Next day she discovered a tender spot in the breast, which rapidly developed a mammary abscess. Forbes Winslow[63] has collected a considerable number of similar cases. In certain instances not only have dreams been originated by special local pain, but the incipient stages of insanity have been revealed by exaggerated dreams. One of my patients, for a considerable time before the evolution of an attack of melancholia, would dream, every night, that a big black dog came into her bed. Another, who suffered with cardiac palpitation, caused by excessive tea-drinking, was often visited in sleep by a mocking imp who seated himself upon the pit of her stomach, and pressed her ribs together with his hands.
The distress or alarm which accompanies such dreams is sometimes sufficient to arouse the sleeper. Often, however, he strives, in his vision, to escape from some impending horror, or to lift up his voice in[Pg 142] a cry for help, but the will is powerless to reach the necessary muscles, and no movement results. In such cases the portion of the brain in which the will resides is awake, but the conducting fibres which intervene between the cortex of the brain and the locomotive ganglia in the cerebro-spinal axis are asleep, and cannot be sufficiently aroused to transmit the impulses derived from the action of the will.
In all ages of the world a belief in the prophetic character of certain dreams has prevailed. Numerous examples are recorded in which a warning intimation of approaching disaster has been thus received. Thus the holy evangelist, St. Matthew, relates that Joseph, the husband of Mary, was guided by dreams to escape with his family from the murderous designs of Herod and of his son Archelaus. The literature of the middle ages is filled with similar narratives. Coming down to recent times, it is not difficult to gather numerous examples of dreams which have been excited by presentiments of good or evil. A lady who was about to embark upon the ill-fated steamer Arctic, dreamed so vividly of shipwreck that she refused to take passage, and thus escaped the frightful disaster which overwhelmed the ship and its numerous passengers. Max Simon[64] relates the case of a lady who, in spite of a similar warning, embarked upon a steamship and lost her life, through the explosion of the boiler during the voyage. On another occasion[65] a noble lady dreamed that a wing of the palace in which her children were sleeping was about to fall down. Starting[Pg 143] up, she called her waiting maids, and insisted that they should bring the children to her chamber. The women endeavored to calm her agitation, quoting an old proverb to the effect that “dreams go by contraries.” As she persisted in her commands, they feigned obedience, but soon returned to say that the young princes were sleeping too quietly to be removed. The princess would not be thus composed; and at last the servants reluctantly brought the little boys from their room. They had scarcely reached their mother’s apartments, when the disaster of which she had dreamed was realized, and the bedroom from which they had just been carried, was crushed into a mass of ruins.
The ancient explanation of such events consisted in a reference to the Deity, who was supposed to address his favorites through the medium of dreams. The modern skeptical explanation views all such revelations as mere accidents. Among the myriads of dreamers, say the “five-sense philosophers,” the infinite variety of combinations which disturb the brain during sleep, cannot fail to produce occasionally such coincidences. When these are of a striking character, the seemingly prophetic vision is remembered, but the cases of discrepancies between vision and result are not recorded, and are soon forgotten. This opinion may very probably be correct in the vast majority of instances; but, if so, we are not in a position to assert any scientific demonstration of the fact. There is, moreover, so far as the ancient religious view is concerned, a certain transcendental sense in which it is true that God may guide his creatures through the agency of dreams, as well as in a thousand other different ways; but this[Pg 144] metaphysical process we can no more comprehend than we can understand or explain the interaction of mind and matter in the brain. The psycho-physiologist must content himself, at present, with the attempt to show that it may not be incompatible with natural law for coming events to cast their shadows before them through the forms of a dream. The following observations lend color to such a possibility.
The extraordinary susceptibility of the brain during certain conditions of sleep has already been noted as a cause for the superior vividness of coloring and intensity of action which sometimes characterizes our dreams. In this respect a slightly morbid condition of the brain, comparable to the effects of hasheesh, probably exists. In such cases the brain may be disturbed to a degree sufficient for the awakening of consciousness by causes that would ordinarily be powerless to reveal themselves. Recording his experience of an earthquake at Lesina, in the night of Sept. 8, 1884, Buschick states, in the Journal of the Austrian Meteorological Society, that a few seconds before the shock he was awakened with a feeling of strange discomfort and apprehension. Once before, on a similar occasion, he had been in like manner aroused from sleep just before the commencement of an earthquake, probably by a feeble and ordinarily imperceptible agitation of the soil. At a time when I was for many months severely overtasked, I always woke up in the night whenever about to receive a call to a patient. Before the sound of footsteps became audible on the sidewalk, I would wake. Presently some one would be heard, approaching the house, and then the[Pg 145] doorbell would ring. So often was this experience repeated, that I learned to expect a summons whenever awakened during the night. Gradually, however, as my health improved with rest, this morbid excitability disappeared, and has never been renewed. It seems probable that in this example the sensitiveness of the brain during sleep was so great that audible impressions were received with vigor sufficient to awake consciousness before they were sufficiently strong to arrest the attention when actually awake. The extreme sensibility of the brain, under certain conditions, to impressions from a distance, is further illustrated by the experience of persons laboring under diseases which produce serious departures from a healthy cerebral circulation. Thus, one of my patients, while suffering with cerebral hyperæmia, could hear children talking half a mile away, at a distance where no one else could hear them. This susceptibility is doubtless the foundation of many well authenticated cases of presentiment. Another of my patients, a lady of remarkably sensitive nervous organization, though otherwise in apparently good health, was one evening lying alone upon her bed. Suddenly, she became greatly agitated with the conviction that something had happened to her husband, who had not yet returned from his place of business. He presently, however, came quietly into the house, and greeted his wife as usual. She exclaimed at once, “What has happened to you, my dear?” “Nothing,” he replied. “Yes,” she said, “something has happened, just now; I felt that you were in trouble.” “Oh, yes,” answered he, after a moment’s reflection, “as I was passing by the park, on my way home, two men[Pg 146] tried to stop my horse, but I whipped up, and got away from them without any trouble.”
On another occasion the same patient was one day suddenly oppressed by a conviction that something had happened to her mother and sister, who were driving together at some distance from home. After a short time they actually returned in a sorry plight, without their carriage. The horse had run away, upsetting them upon the road.
In all these cases it is worthy of remark that there was present an unusual degree of cerebral erethism. Solicitude, weariness, anxiety, inordinate irritability of the brain. It is possible that under such conditions one may hear premonitory sounds, may in some sort feel distant agitations which our healthy organs are usually incapable of apprehending. When such a brain during sleep is unoccupied with the ordinary objects of sensation, feeble impulses, which usually remain unnoticed, may sometimes suffice to arrest the attention. We may thus explain the possibility of impressions derived from distant events passing into the consciousness of a dreamer, and arousing hallucinations of which the immediate cerebral mechanism is the same as that of the ordinary hypnagogic hallucination. Thus, the Rev. Canon Warburton relates the following experience[66]:
“Somewhere about the year 1848 I went up from Oxford to stay a day or two with my brother.... When I got to his chambers I found a note on the table apologising for his absence, and saying that he had gone to a dance somewhere in the West End, and[Pg 147] intended to be home soon after one o’clock. Instead of going to bed, I dozed in an arm-chair, but started up wide awake exactly at one, ejaculating, ‘By Jove, he’s down!’ and seeing him come out of a drawing-room into a brightly illuminated landing, catching his foot in the edge of the top stair, and falling headlong, just saving himself by his elbows and hands. (The house was one which I had never seen, nor did I know where it was.) Thinking very little of the matter, I fell a-doze again for half an hour, and was awakened by my brother suddenly coming in and saying, ‘Oh, there you are! I have just had as narrow an escape of breaking my neck as I ever had in my life. Coming out of the ball-room, I caught my foot, and tumbled full length down the stairs.’”
An incident of this character might very properly be ranked as a mere coincidence, were it not for the fact that it is one only of a considerable number of well attested acts of vision connected either with the hypnagogic state or with the act of dreaming itself. The comparative rarity of such events lends them a marvelous aspect; yet there is really nothing about them any more wonderful or preternatural than the demonstrated possibility of telegraphic signaling across the sea without the intervention of an electric wire.[67] Under ordinary circumstances a metallic conductor must serve as the avenue of communication between distant stations; but if a sufficiently sensitive piece of apparatus be placed in contact with the water on either side of an arm of the sea, communications may be[Pg 148] transmitted from one to the other by a diffusion of impulses through the entire body of water.
In like manner we ordinarily see and hear and feel as a consequence of cerebral excitement occasioned by specific impressions concentrated through the organs of sight and hearing and touch. But it is quite reasonable to believe in the possible existence of a brain so delicately organized as to be capable of reacting to impressions which are too diffuse and too feeble to arouse the ordinary apparatus of sensation. With such a brain it might be possible to experience perception without eye-sight. Evidence furnished by the facts of somnambulism and hypnotism indicates that the receptivity of the brain may become temporarily exalted to a degree which warrants the inference that clairvoyance itself may be thus brought within the capacity of certain peculiarly sensitive organizations. The same extraordinary receptivity occasionally seems to attend the act of dreaming. For example, one of my acquaintances, a lady of a highly wrought nervous temperament, the wife of a distinguished physician in a neighboring State, dreamed one night that a favorite cousin, a beautiful little girl, who lived at a distance of twelve or fifteen miles, was very dangerously ill. She saw the child lying on its mother’s lap, evidently at the point of death, when some one brought a tub of warm water and proceeded to give the patient a bath. This revived the little one so that she recovered. The dream made a very considerable impression upon my friend, by reason of its peculiar character, and because dreaming was for her a very unusual experience. Next morning she rose as usual, but during the forenoon[Pg 149] she was startled by the receipt of a message requesting her to come at once to the house of her uncle, as his little daughter had been taken suddenly ill with the croup, and had expired during the preceding night. Hastening to the bereaved household, she found her aunt sitting with the dead child on her lap, precisely as she had appeared in the dream. The little girl had been suddenly attacked during the night, and, as she lay gasping in her mother’s arms, some one advised a warm bath, and brought a tub of water into the room for that purpose. Unfortunately, just as they were hopefully preparing to dip the child into the water, she had ceased to breathe.
The lack of conformity between the conclusion of this dream and the actual fact reminds one of the blurring of the images that are transferred from one brain to another in the acts of telepathy recently investigated by the Society for Psychical Research. Something similar is frequently observed in connection with the phenomena of hypnotism. The hypnotised subject does not always perceive clearly or wholly the sensation that is suggested by the agent who operates upon his brain.
For another example of apparently clairvoyant dreaming, I am indebted to a friend, a well-known gentleman of unimpeachable veracity, who, when a young man in the army, during the war of the great rebellion, was taken very ill, and was sent home to New England from one of the most remote outposts of the campaign. No one of his family had the slightest information or suspicion of his illness, until the night before his arrival, when his father dreamed that the[Pg 150] absent son was sick, and would arrive the next day, at an hour unusual for travelers coming from the South. So vivid was this dream, and so powerful was its influence upon the mind of the dreamer, that he went at the specified hour to the railway station, with a carriage full of blankets and pillows, to receive his son. When the train arrived, and the invalid actually appeared, the mutual astonishment of father and son can better be imagined than described.
In a recent work on hypnotism,[68] Fischer has related several personal experiences of a similar transfer of impressions during the waking state. It is highly probable that if such impressions are received by a sleeping brain, they may operate like other suggestive irritants to produce dreams, which may be sometimes so vigorously projected upon the consciousness of the dreamer that he may be awakened, and may still perceive the evolution of his dream as an hallucination, even after waking. Thus, on one occasion, during a malarial fever, I dreamed of seeing a friend who lived at a great distance. So vivid was the impression that I started up awake; and there, at the foot of the bed, in broad daylight, was my friend, looking calmly at me. Several seconds, at least, were required to dissipate the vision. In an article already quoted,[69] Sir Edmund Hornby, late Chief Judge of the Supreme Consular Court of China and Japan, “who describes himself as ‘a lawyer by education, family, and tradition, wanting in imagination, and no believer in miracles,’” relates[Pg 151] his experience of a similar spectral visitation. After stating that “it was his habit at Shanghai to allow reporters to come to his house in the evening, to get his written judgment for the next day’s paper,” he says:
“They generally availed themselves of the opportunity, especially one reporter, who was also the editor of an evening paper. He was a peculiar man, reticent about himself, and I imagine had a history. In appearance he was also peculiar. I only knew him as a reporter, and had no other relations with him. On the day when the event occurred, in 1875 or 1876, I went to my study an hour or two after dinner, and wrote out my judgment. It was then about half-past eleven. I rang for the butler, gave him the envelope, and told him to give it to the reporter who should call for it. I was in bed before twelve. I am a very light sleeper, and my wife a very heavy one. Indeed, it is difficult to rouse her out of her first sleep. The bed—a French one—faced the fire-place; on the mantel-piece was a clock, and the gas in the chandelier was turned down, but only so low as to admit of my seeing the time at any time of the night, for—waking easily and frequently—I often smoked a cigarette before I went to sleep again, and always desired to know the hour.
“I had gone to sleep, when I was awakened by hearing a tap at the study door, but thinking it might be the butler—looking to see if the fire were safe and the gas turned off—I turned over with the view of getting to sleep again. Before I did so, I heard a tap at my bed-room door. Still thinking it might be the butler, who might have something to say, I said,[Pg 152] ‘Come in.’ The door opened, and, to my surprise, in walked Mr. ——. I sat up and said, ‘You have mistaken the door; but the butler has the judgment, so go and get it.’ Instead of leaving the room he came to the foot edge of the bed. I said, ‘Mr. ——, you forget yourself! Have the goodness to walk out directly. This is rather an abuse of my favor.’ He looked deadly pale, but was dressed in his usual dress, and was certainly quite sober, and said, ‘I know that I am guilty of an unwarrantable intrusion, but finding that you were not in your study I have ventured to come here.’ I was losing my temper, but something in the man’s manner disinclined me to jump out of bed to eject him by force. So I said, simply, ‘This is too bad, really; pray, leave the room at once.’ Instead of doing so he put one hand on the foot-rail, and gently, and as if in pain, sat down on the foot of the bed. I glanced at the clock, and saw that it was about twenty minutes past one. I said, ‘The butler has had the judgment since half-past eleven; go and get it.’ He said, ‘Pray forgive me; if you knew all the circumstances, you would. Time presses. Pray give me a précis of your judgment, and I will take a note in my book of it,’ drawing his reporter’s book out of his breast pocket. I said, ‘I will do nothing of the kind. Go down stairs, find the butler, and don’t disturb me—you will wake my wife—otherwise I shall have to put you out!’ He slightly moved his hand. I said, ‘Who let you in?’ He answered, ‘No one.’ ‘Confound it,’ I said, ‘What the devil do you mean? Are you drunk?’ He replied, ‘No, and never shall be again; but I pray your lordship give me your decision, for my time is short.’ I[Pg 153] said, ‘You don’t seem to care about my time, and this is the last time I will ever allow a reporter in my house.’ He stopped me short, saying, ‘This is the last time I shall ever see you anywhere.’
“Well, fearful that this commotion might arouse and frighten my wife, I shortly gave him the gist of my judgment in as few words as I could. He seemed to be taking it down in short-hand; it might have taken two or three minutes. When I finished, he rose, thanked me for excusing his intrusion and for the consideration I had always shown him and his colleagues, opened the door and went away. I looked at the clock; it was on the stroke of half-past one.
(Lady Hornby now awoke, thinking she had heard talking; and her husband told her what had happened, and repeated the account when dressing next morning.)
“I went to the court a little before ten. The usher came into my room to robe me, when he said, ‘A sad thing happened last night, sir. Poor —— was found dead in his room.’ I said, ‘Bless my soul! dear me! What did he die of, and when?’ ‘Well, sir, it appears he went up to his room as usual at ten to work at his papers. His wife went up about twelve to ask him when he would be ready for bed. He said, “I have only the judge’s judgment to get ready, and then I have finished.” As he did not come, she went up again, about a quarter to one, to his room and peeped in, and thought she saw him writing, but she did not disturb him. At half-past one she again went to him and spoke to him at the door. As he did not answer she thought he had fallen asleep, so she went up to rouse[Pg 154] him. To her horror he was dead. On the floor was his note book, which I have brought away. She sent for the doctor, who arrived a little after two, and said he had been dead, he concluded, about an hour.’ I looked at the note book. There was the usual heading:
“‘In the Supreme Court, before the Chief Judge.
—— v. ——
“‘The Chief Judge gave judgment this morning in this case to the following effect’—and then followed a few lines of indecipherable shorthand.
“I sent for the magistrate who would act as coroner, and desired him to examine Mr. ——’s wife and servants as to whether Mr. —— had left his home, or could possibly have left it without their knowledge, between eleven and one on the previous night. The result of the inquest showed he died of some form of heart disease, and had not, and could not have left the house without the knowledge of at least his wife, if not of his servants. Not wishing to air my ‘spiritual experience’ for the benefit of the press or the public, I kept the matter at the time to myself, only mentioning it to my Puisne Judge and to one or two friends; but when I got home to tiffin I asked my wife to tell me as nearly as she could remember what I had said to her during the night, and I made a brief note of her replies and of the facts.
“As I said then, so I say now—I was not asleep, but wide awake. After a lapse of nine years my memory is quite clear on the subject. I have not the least doubt, I saw the man—have not the least doubt that the conversation took place between us.
[Pg 155]“I may add that I had examined the butler in the morning—who had given me back the MS. in the envelope when I went to the court after breakfast—as to whether he had locked the door as usual, and if any one could have got in. He said that he had done everything as usual, adding that no one could have got in if even he had not locked the door, as there was no handle outside—which there was not. I examined the coolies and other servants, who all said they opened the door as usual that morning—turned the key and undid the chains, and I have no doubt they spoke the truth. The servants’ apartments were separated from the house, but communicated with it by the gallery at the back, some distance from the entrance hall.
“The reporter’s residence was about a mile and a quarter from where I lived, and his infirmities prevented him from walking any distance except slowly; in fact, he almost invariably drove.
“Edmund Hornby.”
The publication of this remarkable story led to its correction in several important particulars. From the North China Herald (August, 1884) it appears that not only was Sir Edmund’s memory defective in connection with several of the minor details of the narrative, but he had also been either wholly misinformed, or was quite forgetful regarding the actual time of the editor’s death. That person was, in fact, alive and in his usual health at the time of his supposed apparition in the judge’s chamber, and did not die till between eight and nine o’clock on the same morning. He had “attended a temperance committee meeting the night before, and had left about half-past ten in good health[Pg 156] and excellent spirits.... He slept at home, rose shortly before eight, and visited his office to arrange some matter for that day’s paper. He then returned to his room to dress, and in a few minutes afterward was found dead upon the floor.”
Between these conflicting witnesses it is of course impossible to decide. But for our purpose that is quite unnecessary. It is clear that Sir Edmund believed that the visible image of an acquaintance had appeared before him in his chamber at night. It is also evident that the judge was a man whose nerves had been damaged, probably by tobacco—for he was a “light sleeper”—waking often, and indulging in the luxury of a cigarette during the course of the night. If we may credit the writer in the Herald, his brain was in a process of deterioration, proved by the decidedly treacherous character of his memory. The whole story, therefore, becomes exceedingly instructive as an illustration of the manner in which a belief in apparitions may be originated. The most probable explanation of the incident is found in the hypothesis of a dream excited in an irritable brain that had been aroused by the preparation of the manuscript which had occupied the thoughts of the judge immediately before retiring for the night. The course of this dream was so vivid that the sleeper awoke, but continued, like some other dreamers similarly awakened, to witness the evolution of his vision in the form of a genuine hallucination. A remarkable example of a similar production of hallucination through disease of the brain is related by the late Dr. E. H. Clarke.[70] One of his patients, a[Pg 157] vigorous old gentleman, of eighty years, a great lover of music, and a frequent attendant at operas and concerts, retired one night at the usual hour, and in his usual health. He soon fell asleep, “and slept well till about two A. M., when he was awakened by the sound of music, which seemed to come from the street near his house. Thinking a serenade was going on, he got up to ascertain where it was, but discovered nothing. The sound ceased when he arose. On returning to bed, he heard the sound of music again, and was at the same time surprised by the appearance of three persons, standing near each other in his chamber, opposite the foot of his bed. It was his habit to sleep with the gaslight burning feebly, near the head of his bed. He turned the gas on to its full power, and inspected the intruders. They appeared to be musicians, who were humming and singing, as if in preparation for a musical performance. He rang a bell, which summoned his man servant. John soon arrived, and was ordered to put the strangers out. ‘There is nobody here, sir,’ was John’s reply to the order. For a moment Mr. A. was not only amazed, but alarmed. ‘What!’ he exclaimed, ‘do you see no one there?’ ‘No one,’ said John. ‘Go where those chairs are, and move them,’ was Mr. A.’s next direction. John did so. The strangers stepped aside, but did not go out. By this time Mr. A. had gathered his wits about him, and was satisfied that he was the victim of a hallucination; and he determined to observe its phenomena carefully. Accordingly, he bade his servant depart, and prepared to watch his visitors. But they were so life-like and human, that he was again staggered, and recalling[Pg 158] John, told him to go for the house-keeper. She soon came, and on being interrogated, confirmed John’s statements that there were no strangers in the chamber and no sounds to be heard. Convinced by the testimony of two witnesses, Mr. A. yielded to the decision of his reason, and again resolved to go on with the investigation of the strange phenomena. The musicians had now resumed their position, near the window and opposite the foot of the bed. Mr. A. turned the light of the gas full upon them. He looked at his watch, which marked the hour of half-past two. He then arranged his pillows, so as to sit almost upright in bed, and waited for the next scene of the play. He was able to note the size, form, dress, and faces of the performers. One was a large man, who bore some resemblance to Brignoli. The two others were of less size, and shorter stature than their companions. All were habited in dress coats, with white waist coats, and wore white cravats and white gloves. After a little time spent in coughing and clearing their throats, they began to sing. They sang at first a few simple airs, ‘Sweet Home’ among others. They then attempted more difficult music, and gave selections from Beethoven and Mozart. Between the pieces they chatted with each other in a foreign language, which Mr. A. took to be Italian, but they did not address him. Occasionally they changed their position, turned in various directions, and part of the time sat down. Mr. A. said the singing was excellent; he had rarely heard better. After the first feeling of surprise and amazement had passed away, he enjoyed the music exceedingly. The performance continued in this way for some time, when[Pg 159] it suddenly came to an end. The singing ceased, and the singers vanished. He looked at his watch, and found that the time was four o’clock. The concert in his brain had lasted nearly an hour and a half, almost the length of an ordinary concert. He reflected for a while upon this strange occurrence, but not being able to arrive at any satisfactory explanation of it, he turned his gas down and went to sleep. The next morning he called at my office, as previously stated, to ascertain if possible what pranks his brain had been playing, and if he should regard them as warning of his approaching departure.”
In this case the patient was suffering from “a moderate degree of deafness, persistent tinnitus aurium, occasional vertigo, and slight loss of memory.” Towards the close of life, two or three years later, “incoherence, delirium, stupor, and the like, indicated with sufficient certainty the presence of severe cerebral disease.” The remarkable hallucination which he experienced was undoubtedly the product of the morbid changes which were progressing in his brain.
These cases form an ascending series which illustrates the receptive and constructive capacities of the human brain when its sensory apparatus has become unusually or morbidly excitable. But this preternatural mobility may display itself in other departments besides those of mere sense-perception. The sphere of pure intellect may thus be invaded by ideas springing from impressions which address the reasoning faculties alone, so that in sleep a dream may lead the judgment to decisive conclusions that were scarcely recognized or heeded during the hours of wakefulness.[Pg 160] In this way we may learn to understand how the anxieties experienced by the husband of the Virgin Mary may have ripened into a dream, of intensity sufficient to guide his subsequent action. Nothing could be more natural for one, like him, ignorant of physiology and of second causes in general, than the ascription of such an event to the immediate intervention of the Great First Cause—the only cause which he could rationally apprehend. Hence the universal primitive belief that in dreams God spake to man. Upon this belief was laid the foundation of many of the religious convictions which have grown and ripened with the progress of the race until their shadowy origin has been well nigh forgotten.
Many are wont to affirm that the age of illumination through the intervention of dreams is past, but there is no good reason for the belief that such dreams may not still occur. A lady, carefully educated in the doctrines of the popular theology, had been very much distressed by the unruly behavior of her only child, a little imp who had scarcely learned to talk. While thus depressed in spirits she dreamed that the Day of Judgment had come. She found herself with her husband and child and the whole human race assembled upon the face of the earth, waiting in agony for the awful decision of their fate. Finally the heavens were opened, and Jesus appeared, dividing the wicked from the good. As he drew near the place where she was standing, she could no longer endure her anxiety regarding the destiny of her daughter; she rushed forward, and implored the Divine Judge to spare her child. With a look of ineffable compassion he assured[Pg 161] the trembling suppliant that her prayer was granted, and she awoke in a state of great agitation, but much comforted as to the future of her little girl, who in due course of time grew up to be a very exemplary young woman. Now, if the dream of Joseph was a revelation, a dream like this is quite as worthy of similar estimation. They both occurred as the result of analogous conditions of the brain and mind, and were both excited by second causes of a similar character. It is impossible for any one to show that the relation between the First Cause and either set of second causes was any more intimate and special in one case than in the other.
The wonderful exaltation of certain faculties during the unequal sleep of the different organs of the mind, is usually to be considered as something relative rather than absolute. But there is little reason to doubt that sometimes the excitement of the waking portions of the brain does really transcend the ordinary functional capacity of the structure. Under such conditions the undivided concentration of attention upon the comparatively limited circle of ideas which are thus produced, greatly increases the intensity of the resulting impressions upon the mind in consciousness. Hence the grandeur of the visions which may thus arise; hence, also, the possibility of their construction in accordance with fact rather than with fancy; as in the case of the visions of the ancient Hebrew prophets. As the darkness of night, by shutting out the earth from sight, opens our eyes to the glory of the starry sky, so, in like manner, sleep, by closing the senses against the distractions of the external world, may sometimes[Pg 162] afford the conditions enabling a richly gifted intellect to comprehend the course and the destination of those deep and silent streams of thought which move on, unnoticed during the hours of wakeful life.
Whatever may be true of this matter of fore-sight, it is certain that under similar conditions the memory of past events may be so quickened as to yield results quite comparable with actual clairvoyance. A good illustration of this has been recorded by Abercrombie.[71] A gentleman named Rowland had been prosecuted for certain arrears of tithe which he believed had been long previously paid by his deceased father. “But, after an industrious search among his father’s papers, an investigation of the public records, and a careful inquiry among all persons who had transacted law business for his father, no evidence could be discovered to support his defence. The period was now near at hand when he conceived the loss of his lawsuit to be inevitable, and he had formed his determination to ride to Edinburgh next day and make the best bargain he could in the way of compromise. He went to bed with this resolution, and, with all the circumstances of the case floating upon his mind, had a dream to the following purpose: His father, who had been many years dead, appeared to him, as he thought, and asked him why he was disturbed in his mind. In dreams men are not surprised at such apparitions. Mr. R. thought that he informed his father of the cause of his distress, adding that the payment of a considerable sum of money was the more unpleasant to him because he had a strong consciousness that it was not due, though he[Pg 163] was unable to recover any evidence in support of his belief. ‘You are right, my son,’ replied the paternal shade; ‘I did acquire right to these teinds, for payment of which you are now prosecuted. The papers relating to the transaction are in the hands of Mr. ——, a writer (or attorney), who is now retired from professional business, and resides at Inveresk, near Edinburgh. He was a person whom I employed on that occasion for a particular reason, but who never, on any other occasion, transacted business on my account. It is very possible,’ pursued the vision, ‘that Mr. —— may have forgotten a matter which is now of a very old date; but you may call it to his recollection by this token—that when I came to pay his account there was difficulty in getting change for a Portugal piece of gold, and that we were forced to drink out the balance at a tavern.’
“Mr. R. awoke in the morning with all the events of the vision impressed on his mind, and thought it worth while to ride across the country to Inveresk, instead of going to Edinburgh. When he came there he waited on the gentleman mentioned in the dream, a very old man; without saying anything of the vision, he inquired whether he remembered having conducted such a matter for his deceased father. The old gentleman could not at first bring the circumstance to his recollection, but, on mention of the Portugal piece of gold, the whole returned upon his memory; he made an immediate search for the papers and recovered them, so that Mr. R. carried to Edinburgh the documents necessary to gain the cause which he was on the verge of losing.”
[Pg 164]Here it would be a valuable addition to knowledge if the parties in the history just related could be subjected to intelligent interrogation. Enough, however, may be discovered in the narrative to render it certain that the dream was merely a revival in consciousness of knowledge that had been long previously forgotten. There was a vague recollection of some such information evidently struggling for recognition; otherwise Mr. R. could not have held the belief in spite of the lack of evidence, that his father had paid the tithes in dispute. He had probably heard from his father some account of a transaction which had taken place so long before that the only surviving actor, the aged lawyer, had forgotten everything about it, and could only recall the event through the associations connected with the Portugal piece of gold. In the lawyer’s case the cerebral register only needed the stimulus afforded by the association of ideas, in order to make it again place before the mind impressions which had long subsided below the level of consciousness. For Mr. R., sleep afforded the limitation of cerebral function needful for a concentration of attention sufficient to penetrate to the level of the residual vibrations which persisted as the sole representatives of the original impressions through which his knowledge of the event had been primitively obtained. Parallel examples are furnished by the cases of individuals who, upon their death-beds, during the dissolution of the brain, have resumed a long disused vocabulary, speaking the language and thinking the thoughts of their childhood. “He ‘babbled of green fields,’” said Mistress Quickly, narrating the closing scenes in the life of the famous[Pg 165] Sir John Falstaff. Dr. Rush[72] relates the case of a learned Italian gentleman who, “in the beginning of the yellow fever which terminated his life, ... spoke English only; in the middle of the disease, he spoke French only; but on the day of his death, he spoke only in the language of his native country.” In like manner the old Swedish settlers in Philadelphia who had forgotten their native language, or, at least, had not spoken it for half a century, would pray in Swedish on their death-beds.[73] Sleep and dissolution operate alike to release the lower levels of the mnemonic apparatus from the overshadowing influence of later impressions, so that, like an ancient palimpsest, it presents once more its long-forgotten characters for inspection by the mind.
SOMNAMBULISM.
A great perturbation in nature! to receive at once the benefit of sleep, and do the effects of watching.
—Macbeth.
We have seen that in certain cases dreams manifest a tendency to pass into action. Thus, the dream with which I was on one occasion occupied became so amusing that I was awakened by a paroxysm of laughter that continued for some time after the termination of the dream. Sometimes the actions which are thus determined become more complicated, but do not suffice to arouse the sleeper. He continues to dream, and to act out his dream. This constitutes the ordinary form of somnambulism. It is a special affection of the nervous system encountered chiefly among persons of a decidedly neurotic constitution—especially among the victims of hysteria, epilepsy, and insanity. Sometimes occurring in cases apparently characterized by perfect health, it will usually be discovered by careful inquiry that the subject is nevertheless connected by near relationship with a neurotic stock. In a third class of patients the neuropathic diathesis is not congenital, but is the acquired result of particular injuries or diseases of the head. It is also observed sometimes as a consequence of transitory functional disturbances of the brain connected with the period of convalescence from[Pg 167] diseases that profoundly affect the nutrition of the nervous system. In all cases, however, it is probable that a special nervous temperament exists as a predisposing cause of the phenomena, for the majority of people can sustain injuries of the head, or of the peripheral nervous system, and can pass through all kinds of illness without exhibiting any tendency to somnambulism. As the nervous temperament is the peculiar property of children and of the female sex, it is among them that the affection is usually observed. Before the age of puberty, however, the differential peculiarities of sex are not sufficient to produce any great preponderance in either direction; and small boys are, therefore, perhaps as frequently somnambulistic as their little sisters. Like other neuropathic disorders, this predisposition is frequently met with as an hereditary attribute which may be handed down from generation to generation. Occurring in the experience of young children, it frequently ceases when they arrive at years of maturity. Not always, however, thus ceasing as a consequence of improvement in the general health, but because of the substitution of some more serious disorder.
The phenomena of ordinary somnambulism are manifested, like the dreams out of which they arise, during the period of sleep. But, while dreams most frequently occur during the later portion of the night, after the deepest sleep is past, somnambulism usually occurs in the earlier part of the night, during the deepest sleep. As a consequence of this fact, consciousness is seldom affected by the molecular play of the brain during the somnambulic excursion. The[Pg 168] sleepwalker knows nothing, and remembers nothing of the incidents in which he has been an active agent; while the dreamer seems to be more nearly awake. His consciousness is partially aroused by the play of memory and of imagination, and he can remember the spectacle which constituted his dream. The phenomena of somnambulism necessitate the participation of a larger number of faculties than are needed for the production of a dream, but their activities are coördinated upon a plane, so to speak, lower than the platform upon which the elements of dreams are arranged. Consequently, though the elements of the somnambulic process may be far more numerous and various than the elements of a dream, they may be less capable of rising into the realm of consciousness. Such a process may differ from the phenomena of ordinary life only in the fact of unconsciousness; and, when concluded, it leaves no traces in the memory of the waking state. In other instances, on the contrary, so many nervous functions may be suppressed, and so great may be the intensity of the remaining cerebral processes, that the resulting phenomena scarcely differ from an ordinary dream in which consciousness is aroused, and the waking memory is durably impressed. Between these extremes lie opportunities for an indefinite number of combinations; consequently the forms and degrees of somnambulism present a very great variety of manifestation. Maury[74] reduces these to five principal forms: First, simple movement of the limbs in connection with that partial sleep of the intellectual faculties which produces ordinary dreams. Second,[Pg 169] somniation, a state in which the patient unconsciously performs such actions as have become so far habitual that, though complicated in their character, they constitute genuine cerebral reflexes. Third, noctambulism, or sleep-walking, in which the action, though complicated in its character, and different from the ordinary waking occupations of the patient, appears to be the result of automatic processes, constituting a dream that is acted out in time and space. Fourth, somnambulism with exaltation of the faculties, producing delirium with conscious movements during the crisis. Fifth, somnambulic life, or double consciousness, in which, with the exception of certain special modifications of intelligence, the conduct of the patient during the paroxysm does not perceptibly differ from that of the waking state, so that the subject seems to experience two successive though disconnected personalities.
The exact relation between these different degrees of somnambulism has been further elucidated by MM. Ball and Chambard.[75] Starting with the proposition that normal healthy existence is a state in which the functions of organic life furnish a basis for nervous sensibility and motion, by means of which the imaginative faculties (imagination and memory), associated with the coördinative faculties (attention, judgment, volition), are sufficiently stimulated to maintain a state of consciousness, they show that the first stage of sleep consists in the suppression of bodily motion and sensibility. The second stage consists in the further suppression of the coördinative faculties. The third stage is marked by the loss of memory and imagination. In[Pg 170] the most profound and perfect sleep the functions of organic life alone remain. The process of awaking consists in the revival of the faculties in the inverse order of their extinction. Dreams occur during the period in which motion, sensation, and the coördinative faculties are in abeyance; but somnambulism may accompany each of the stages of sleep. Its simplest form is perhaps the rarest; corresponding to Maury’s fifth variety. In this form the functions of organic life are intact; motion and sensibility seem unchanged; the intellectual faculties display their usual activity; but the ordinary consciousness is never aroused. So far as the normal life of the subject is concerned, he is active, sensible, intelligent, but unconscious; and when the paroxysm is terminated memory contains no account of its events. Such paroxysms may occur but once in the life-time of an individual, or they may be repeated at stated intervals, constituting an alternate succession of mental states without connection in consciousness. This is called the somnambulic life, or double consciousness, several examples of which will be related upon another page.
The second form of somnambulism results from the abolition of consciousness and the more or less complete suppression of the coördinative faculties of the mind. Memory and imagination, released in great measure from the control of the higher intellectual faculties, and excited by such vestiges of sensation as still persist, create a species of delirium in which mutilated sensations, half formed thoughts and disproportioned volitions combine to produce a variety of[Pg 171] actions. In this condition the patient dreams, and acts out his dream. He is a somnambulic dreamer.
In the third degree of somnambulism, consciousness and the entire range of intellectual faculties have disappeared. The individual resembles a creature from which the cerebral hemispheres have been removed. He is little better than a living automaton, guided only by impressions received from without. In this condition the movements of the body may become wholly responsive to the will of another—a prominent characteristic of artificial somnambulism or hypnotism.
A fourth degree of somnambulism is marked by the disappearance of consciousness, intellect, sensibility, and the power of motion. Only the lower functions of organic life remain. The patient merely lives, he neither thinks nor acts. This constitutes the state of somnambulic lethargy, a condition which differs from deep sleep only in the fact that under the influence of external impulses or of partial awaking it may easily pass into the second form of the affection, the somnambulic dream.
Such is the classification of MM. Ball and Chambard. It possesses the merit of great precision and clearness. If the warning which its authors themselves utter against its too literal acceptance be respected, it will be found to afford a very convenient explanation of the manner in which the various degrees of somnambulism are reached. But it must be remembered that between these pronounced and definite forms exist a great number of intermediate degrees. Partial revivals and temporary resurrections of the higher[Pg 172] faculties of the mind may intrude themselves among the activities which depend upon lower functions; as, for example, when the ordinary unconsciousness of lethargy is briefly interrupted by an event which may remain permanently fixed in memory after waking, even though all other concurrent incidents were unnoticed and left no trace behind. Keeping this caution in mind, the following diagram will be found useful:
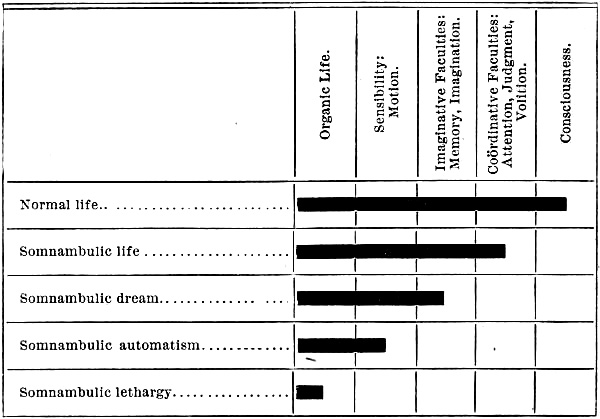
The close parallel between this diagram and the one on page 4, which illustrates the course of sleep, will be at once remarked. The difference between the two states cannot be thus diagrammatically expressed. It is the difference between sleep in a healthy, normal subject, and sleep as modified by the somnambulistic temperament. This may be either the result of disease or of congenital defect of cerebral organization. What the particular structural[Pg 173] difference may be, it must be impossible to decide, until it shall become possible to state the reason why one brain shall behave only in a normal manner, while another presents all the vagaries of hysteria, somnambulism,—perhaps even of insanity. That the affection is hereditary is a matter of common observation. One of my patients who is somnambulistic—walking in his sleep, climbing over the roof of his house, etc.—is the son of a father who was also a noctambulist, and who once fractured his leg by falling from a step as he was walking down stairs in his sleep. A grand-daughter is both a somniloquist and a somnambulist.
Returning now to the classification adopted by Ball and Chambard, it will be found interesting to consider a few illustrative examples of the different forms and degrees of the affection under consideration.
Somnambulic Lethargy.—This condition represents the form which outwardly resembles profound sleep. It may occur as a paroxysm without relation to other forms of the affection, or, according to my own observation, more frequently associated with other forms of somnambulism. Thus, one of my patients, a lady about thirty-five years of age, having accidentally fallen into the hands of a noted empiric, by whom, for a slight attack of tonsillitis, she was vigorously dosed with atropia, digitalis and calabar bean, finally passed into a somnambulic state corresponding to the somnambulic life of the preceding table. This continued about five weeks, when she became completely lethargic, and was transferred to my care. In this condition she remained unconscious, almost perfectly[Pg 174] insensible, with pupils somewhat contracted and sluggish before the light, with a feeble and slightly accelerated pulse, a moderately elevated temperature, bowels and bladder insensible to their contents, mouth and throat filled with an offensive mucous secretion. By great urgency she could be sufficiently roused to open her mouth, so as to permit cleansing the cavity, and to swallow liquid food. Swallowing was effected very slowly, and only after the liquid had remained for some time in the fauces. At the end of about three weeks the patient began to exhibit more vitality. She could be more easily aroused, began to dream and to have hallucinations that were finally prolonged out of sleep into wakefulness. In the course of a few hours she was fully herself again, after eight weeks of unconsciousness.
This form of lethargy is characterized by the complete unconsciousness which persists during its course. Its duration is variable, sometimes continuing for a few minutes only; sometimes lasting through many days and weeks. Dr. W. T. Gairdner, Professor of Medicine in the University of Glasgow,[76] reports the case of a woman who remained for over one hundred and sixty days in a condition of lethargic stupor. “The patient was the mother of a family, and had lived a strictly domestic and (up to a short time before her seizure) healthy and regular life. There were no peculiar moral and religious problems to perplex the situation. There was no history of inveterate hysteria, or of long continued rapt contemplation; nor has there been the slightest evidence of any craving after[Pg 175] notoriety, either before the attack or since its termination. The moral atmosphere, in short, surrounding the phenomena, is altogether unfavorable to exaggeration and imposture, for which, indeed, no reasonable motive can be assigned. Nevertheless, under these very commonplace conditions, concurring with some degree of melancholy or mental despondency after delivery, but during a convalescence otherwise normal, Mrs. McI—— presents to our notice a condition of suspended consciousness and disordered innervation in no degree less extreme than the ‘trances’ or cataleptic attacks which have been recorded as the result of the most aggravated hysteria, or as the miracles of religious ecstasy and profound mental emotion. She becomes for the long period of over one hundred and sixty days continuously an almost mindless automaton, connected with the external world only through a few insignificant reflexes and through the organic functions. She is fed, almost without resistance, through the stomach-tube; she defecates and urinates (during much the greater part of the time) unconsciously; she is absolutely passive as regards everything that demands spontaneous movement, and betrays almost no sign of sensation, general or special, when subjected to the severest tests that can be applied short of physical injury. But while her senses were thus shut, and her volitions in suspense to an extent much beyond ordinary sleep, there was, nevertheless, a sleep within the sleep. The periodicity of day and night was maintained by some change in the condition of the innervation, of which snoring was the sole indication. She was not convulsed, nor paralyzed, nor delirious;[Pg 176] the singing, laughing, weeping, adoring ecstasies of hysteria and of religious excitement were wholly wanting; nor were there during many months such intervals of normal consciousness as are observed in almost all the recorded cases of hysterical coma and of catalepsy. The statue-like pose, moreover, and the flexibilitas cerea of typical catalepsy, are absent in this case. The return to consciousness was followed or accompanied by a return of all the normal functions of mind and body; there is now no incoherence, nor even distorted perceptions, as of a dream-life occupying the somnolent imagination for months, and therefore all the more hard to reconcile with realities. She is self-possessed, but unobtrusive, easily managed, and betraying only natural emotion; she persists in maintaining that the whole period of the apparent unconsciousness is a complete blank to her recollection. She is grateful for her recovery, but manifests no craving for sympathy, and no tendency, as yet, to revert to any morbid condition of despondency, such as was described at the commencement of the attack. In connection with this last point, although there is no evidence of her having been personally insane, it is not to be denied that her family history contains strong presumptions of a hereditary predisposition bearing in that direction.”
These cases must not be confounded with the examples of lucid lethargy, to which allusion has been made in a previous chapter. Somnambulic lethargy is a condition in which the cerebrum is wholly inert. In lucid lethargy, although there is complete loss of general sensibility and of the power of voluntary motion, the field of consciousness is continually[Pg 177] enlightened by perceptions derived from one or more of the special senses, so that the subject is conscious of much that transpires in his immediate neighborhood. These two forms of lethargy sometimes alternate in the experience of the same individual, constituting a portion of the indefinitely varied manifestations of hystero-epilepsy. Grasset relates the case[77] of a little girl, ten years old, who suffered with various forms of hysteria, which were finally replaced by attacks of stupor, lasting several hours. After a time these crises of “nervous sleep” were transformed into more ordinary attacks of somnambulism, in which, “although the child’s eyes are shut, she sees and hears everything during the crises, knows who comes into the room by their step and walk. If anything unpleasant is said to her, or if they threaten to wet her, or make her smell something, she gets angry, and pushes everything violently away that is offered to her. She replies by signs to all questions, and if she wants anything, asks for it by gesture: if she wants to drink, she puts her finger to her lips as if in the act of sucking, and if not understood, becomes irritated, gets up, and leads the father or mother to the sideboard or cupboard, where the things she wants are, and always with the eyes shut. She is able to go through the whole house, I do not say quite alone, because they do not allow her to walk alone, but with help, and she directs the way wherever she wishes to go. During the crises she even sometimes amuses herself with a little dog, which she makes jump over a stick resting on the cross-bars of two chairs opposite each other;[Pg 178] and according as she wishes the dog to jump higher or lower, she moves the stick to the lower or higher bars of the chairs, and that with eyes always shut spasmodically. During the whole attack she cannot talk; but towards the end she speaks, although not yet recovered from her state of somnambulism. When the crisis is over, the child remembers nothing of what she has said or done in her sleep, and is much surprised at everything told her.”
Somnambulic Dreams.—The preceding cases illustrate the variable character of the manifestations of somnambulism, and may also serve as an introduction to the more common form of the affection, in which the patient experiences a dream, probably excited by the same causes that produce ordinary dreams, and also acts out his dream. The differences between an ordinary dream and a somnambulic dream lie in the fact that the one produces an often vivid impression upon consciousness and memory, while the other is entirely expended upon the organs of external expression. Starting probably from the same portion of the brain, the physiological dream sets in motion the cortical structures which are in immediate relation with conscious memory; the impulses of the somnambulic dream, on the contrary, are directed towards the lower portions of the nervous system, where they serve to excite the organs of locomotion and expression, which are destitute of every form of mnemonic register. Consequently, the somnambulist retains no recollection of the incidents of his dream.
The simplest form of this affection is presented by the restless child who talks, cries out, and brandishes[Pg 179] its fists in sleep. In the majority of instances these manifestations create little more disturbance than the half uttered yelping of a dog that barks in its sleep. But in some cases the outbreak assumes a distressing, if not an alarming character, constituting the affection known by the name of night terrors. The disorder is usually observed in young children of a highly nervous temperament, before the conclusion of their second dentition. The little patients are generally of neurotic lineage. Insanity, hysteria, neurasthenia, epilepsy, chorea, and nervous dyspepsia, are often discovered among their near relatives. Not unfrequently they have been, or will become, choreic. The attack is often preceded by symptoms of indigestion and constipation; but the exciting cause may be usually traced in the commotion of a brain that has been wearied by the exertions of the previous day. The child starts up out of an apparently sound sleep, crying with seeming alarm, calling for his mother, and staring wildly around, with every possible expression of terror. Sometimes he jumps from his couch, and runs headlong into a corner, or seeks concealment under the bed, as if escaping from some frightful object. The eyes are open, tears flow, perspiration covers the skin, there is the greatest excitement, and the little one, clinging convulsively to its parent, will not be quieted. Only after a number of minutes does the child seem to recover the power of recognizing his friends. Presently, however, he lies down, and falls immediately asleep, waking in the morning without the slightest remembrance of the unpleasant event.
Such paroxysms occur during the early part of the[Pg 180] night, one or two hours after bedtime, when sleep is passing from its maximum intensity to an inferior degree of depth. This, moreover, is the time when the controlling power of the sensory apparatus over other portions of the nervous system has already reached its minimum. The spinal centres and those intra-cranial ganglia which do not share in the full measure of this repose are therefore in a condition of relative exaltation. Disturbances of internal origin, consequently, produce inordinate excitement of these waking portions of the nervous apparatus. The abnormal quality of this excitement is attested both by the history of the patient, and by the fact that it does not pervade the whole brain. The distribution of motion through the cerebrum is hindered, so that certain portions of the organ remain asleep while other regions are thrown into a state of tumultuous uproar. Such disconnection of the different organs of the nervous system, by withdrawing particular ganglia from the inhibitory influence of the other centres, gives opportunity for violent explosions of nervous force.
Somewhat similar in their origin are those acts of unconscious violence which sometimes occur during the process of sudden awakening out of sound sleep. The patient is usually a deep but uneasy sleeper, who is only aroused imperfectly and with difficulty when the attempt to awaken him is made. Under such circumstances the disturbance to which he is subjected serves as the exciting cause of a dream which, like the ordinary somnambulist, he puts into action before he is fully waked. On recovering complete consciousness,[Pg 181] he may retain no recollection of the events of his dream, and may also experience as great a degree of astonishment at the results of his violence as if he had taken no part in its display. A gentleman of my acquaintance, who had suffered considerable uneasiness regarding burglars, was, one night, startled by a noise in his room. Jumping up suddenly, he grasped a pistol and fired it in the direction of a figure dimly perceived near the bed. On waking fully out of sleep, he found that he had inflicted a wound upon the hand of his wife whose movements had disturbed him. Another unfortunate, who was once under my observation for undoubted insanity, was in like manner aroused out of sleep by a supposed noise, probably heard in a dream. With a pistol in each hand, he commenced firing wildly in every direction, fatally wounding his wife who was in bed at his side. When completely awakened he had no recollection of what had occurred, and was overwhelmed by the event.
Wharton and Stillé[78] have collected a number of similar examples of this disorder, to which the term somnolentia or sleep-drunkenness has been applied. Its connection with morbid disturbance of the brain is usually very evident. Obviously, the moral responsibility of the agent in such cases is identical with that of the ordinary somnambulist, or of the subject of epileptic mania.
Ordinarily, however, the somnambulic dream is less agitated. The patient merely continues the movements with which he was occupied at the moment of falling asleep, as in the case of Galen, who, though[Pg 182] long an unbeliever of the tales regarding sleepy soldiers who had unconsciously continued to march with their comrades, at last found himself in a similar manner walking a considerable distance after he had been overtaken by sleep while journeying on foot. In other cases the phenomena though intimately connected with the daily occupations of the subject, present themselves in a form somewhat detached from the waking life. Such are the common experiences of children who get out of bed, and walk around the house, seeking their playthings, or pulling their clothes out of the drawers in which they have been laid. Sometimes the events of the day have evidently suggested the deeds of the night. One of my little acquaintances will leave her bed, walk into another room, seat herself by her mother’s work-basket, thread a needle, and proceed to sew up the imaginary holes in her dress. One of my early playmates, in like manner, after puzzling over a difficult sum in arithmetic, before retiring, arose in his sleep, took paper and a pencil from his mother’s desk, and proceeded before her eyes to work out the correct answer. Another, tempted probably by a vision of ripe grapes upon the trellis, climbed out of his window upon the roof of a shed. Unfortunately, the certainty with which somnambulists usually direct their movements seemed to fail him. He fell heavily to the ground, where he awoke to find himself seriously injured.
An excellent example of a still more complicated series of actions during somnambulism is quoted by P. Max Simon.[79] It illustrates a majority of the facts[Pg 183] which have been already brought forward, and will well reward careful consideration. “A young clergyman was in the habit of getting up in his sleep, taking paper, composing and writing sermons. When he had finished a page, he would read it over, if an action performed without the assistance of sight can be called reading. If dissatisfied with anything, he would blot it out, and then write the corrections with great accuracy in their appropriate place above the line. In one of these sermons he made a correction which was quite remarkable. Having in one place written the words ce divin enfant, on revising the page he decided to substitute the word adorable instead of the word divin. He therefore blotted out this last word and placed the other immediately over it; then, perceiving the word ce, which was proper enough before the word divin, lacked the terminal letter t that was needed before a vowel, he very adroitly added the necessary letter, so that the amended sentence correctly read cet adorable enfant. In order to ascertain whether the somnambulist made any use of his eyes, a cardboard was placed under his chin in such a way as to completely obstruct the view of the paper upon the table; but he continued to write without paying any attention to the obstacle. In order to ascertain whether he was aware of the presence of the objects which were before his eyes, the paper upon which he was writing was taken away, and a number of other sheets were successively slipped into its place; but he always noticed the substitution, because they differed in size. When an exactly similar piece was substituted, he accepted it as his own, and wrote down the corrections at the points which[Pg 184] corresponded exactly with the writing upon the page which had been removed. It was by means of this ingenious stratagem that some of his nocturnal compositions were preserved.
“The most astonishing thing of all,” continues the author of this article, “was the exact composition of music. A cane served him as a ruler. With it he ruled at equal distances the five necessary lines, putting in their proper place the clef, the flats and the sharps. Finally, he inscribed the notes, at first all in outline, but, when he had finished, he blackened those which should be dark. The words of the song were written below. On one occasion he happened to write them with too large a hand, so that they were not placed directly under their corresponding notes. He soon perceived this defect, and, in order to amend it, he blotted out what he had done by drawing his hand over it, and then rewrote the line of music lower down the page with all the precision imaginable.
“Another singular thing of a different sort, which was not less remarkable. One night, in the middle of winter, he dreamed that he was walking on the bank of a river, and saw a child fall into the water where he was drowning. The severity of the cold did not hinder him from hurrying to the rescue. He threw himself at full length upon his bed, in the position of a man who is swimming, and imitated all his movements. After having fatigued himself for some time with this exercise, he felt a portion of the coverlid gathered in a heap on one corner of the bed. He believed this to be the child; grasped it in one hand, and with the other went through the motions of swimming back to the[Pg 185] bank of the supposed river. There he laid down his burden, and came out, shivering and chattering his teeth as if he were really getting out of an icy river. To the bystanders he said that he was freezing, and would die of cold, that his blood was all turned to ice; he must have a glass of brandy to warm him. Not having any, they gave him some water which chanced to be in the room; he tasted it, recognized the deception, and called, with greater emphasis than before, for brandy, insisting upon the magnitude of the danger which threatened his health. A glass of liquor was finally given to him; he drank it with pleasure, and spoke of the great relief which it afforded him. Notwithstanding all these incidents, he did not wake, but went to bed, and slept most profoundly.”
An equally instructive case is related by my distinguished colleague, Prof. J. Adams Allen.[80] The subject of the observation was a medical student who resided in Professor Allen’s house during a portion of the time covered by the narrative.
“About the summer of 1847, a somewhat dilapidated bass-viol, which was a kind of heir-loom in the family, was brought into the house, and he devoted spare moments to learning how to play upon it. Unfortunately, the antiquity of the instrument had told upon its keys, and unless they were wetted at each time of use, it would not remain in tune. He was determined, however, to command its notes, and succeeded. His somnambulic walks, thereafter, led him from his chamber to the parlor, and to the bass-viol, and the family would be awakened in the small hours[Pg 186] by the inevitable tuning up prelude, mingled with slipping of the old keys, and quiet objurgations upon his part. Sometimes the bridge would fall down when the keys slipped, and sometimes a string would snap or escape from the keys, nevertheless he would persevere, repair damages, tune up, and then execute all varieties of music of which the machine was capable, not unfrequently accompanying it with his voice. All this would be done in total darkness. When any one entered the room with a light, he took not the least notice, although when spoken to he would reply in monosyllables or with considerable asperity. His face was usually flushed, although sometimes pale—the features immobile and passive, the eye open, pupil dilated, the surface glazed, and the lids apparently motionless. The extremities warm and the pulse full, frequent and soft. Very often the skin would be bathed with free perspiration. Remarkably sensitive to titillations when awake, there seemed total absence of reflex movements from this cause whilst in the somnambulic state.
“As he extended his acquaintance with music and musical instruments, his feats became wonderful. Whilst in attendance upon the Medical College at La Porte, the household looked forward with high anticipations to the hours when his skillful touch of the melodeon would wake them. He had a voice of the purest tone and very considerable compass, in fact of rare sweetness. I am enabled to say from a multitude of observations, that he played with a precision and skill while asleep that he could not approximate while awake. Besides this, he would execute music which he[Pg 187] had heard, perhaps, but once, the evening previous or after a long interval—no note of which he could recall in his waking moments. His memory here seemed wonderfully exalted. If interrupted, he was irritable in the extreme, but would go on with his music exactly from the point of interruption.
“Among the numberless exhibitions of his somnambulism, I have time only to notice a few of the most striking.
“Whilst attending lectures at Ann Arbor, where I was then lecturing on Physiology, I requested his assistance in enlarging some of the drawings illustrative of minute anatomy and histology, for use in class demonstrations. He entered into the work with great zeal, and proved very expert and rapid in execution. One evening, previous to the day on which I was about to lecture on the kidney, I wished the cuts in Carpenter’s Physiology, illustrating the tubular arrangement, etc., were ready. He had an engagement for the evening, but said he would try and prepare them in the morning. During the night he rose, dressed himself, played a few tunes on the guitar, part of the time singing (and, by the way, the guitar was about as dilapidated as the bass-viol before noticed, and he had to knot one or two of the strings first), and then arranged the drawing paper, prepared his India ink and brushes, took the parallels and pencils and laid off the space, and worked for half an hour or more rapidly and perfectly, nearly completing the figures on pp. 596 and 597 of Carpenter’s Principles, in the edition of 1853.... These drawings are now in the series used for illustration in Rush Medical College. Although we[Pg 188] had a light in the room while watching him, he went on with his work entirely regardless of it. Before completing the work, he went to bed and slept until the usual hour in the morning, when at the breakfast he asked if he had been up in the night, as he had dreamed that he had. This was the only time he ever remembered even dreaming about being up or occupied in anything. He had by this time become so fully aware of his habits, that nothing of the sort astonished him. Shortly after this he went to spend the night with a fellow student, but a little after midnight he rose, dressed himself, and went out, followed by the other gentleman, walked down to the Exchange Hotel, where there were a number of his acquaintances and others waiting for a train of cars due at that time. Some one rallied him on his being out so late, but being cautioned by his companion, they did not attempt to awake him, but watched his movements. On being invited, he took a glass of ale, and then said he would only have time to go home and get his dinner before the afternoon lecture hour. He walked with his friend to our door, and was indignant to find it locked. His room-mate (a cousin) admitted him and awakened myself and wife. He asked if dinner was ready, and seemed astonished that it was not; then said he would get a drink of water and be off, ‘for old D. (one of the faculty) would be mad if he was late.’ I told him he had plenty of time and he need not be in a hurry. He then walked into the kitchen, drank a tumblerful of water, and, looking up to the clock, although it was totally dark, remarked the time, and started for the front door. I then told him that I was[Pg 189] not feeling well, was pretty blue, and wished he would sit down and play euchre with us. This seemed to please him, and he took off his overcoat and said he had as lief play until ‘old D.’ was through lecturing, as to go.
“His cousin sat down at the table with us, and we played ‘three-handed (cut-throat) euchre.’ He paid not the slightest attention to us, although we passed the cards backwards and forwards between us, exchanging hands, and everything we could do to attract his attention. He dealt the cards in his turn, correctly, and played ‘according to Hoyle.’ In one hand, spades were trumps, and he held the jack of clubs. Clubs being led, he first threw down this jack, then quickly picked it up, saying, ‘I forgot that was the left bower.’ It is somewhat humiliating to record that, notwithstanding our tricks and devices, he beat us in the game.
“On its conclusion, he got up hastily and insisted upon going to the college. We only prevented him this time, by throwing water in his face—the only method, by the way, in which we could awake him without great violence. Pungent odors, ammonia, camphor, etc., he seemed to disregard, or merely pushed away the object.
“On regaining consciousness, he always appeared like one stunned, or suffering from a severe shock. The influence upon the pulse and nervous system was always so severe, that we never awaked him at these times if we could avoid it.
“Whenever a little out of health, as from trifling attacks of indigestion, or after watching with the sick,[Pg 190] or fatigue, he would be sure to be up and doing something notable in the somnambulic state.
“One of the most remarkable of his exploits occurred several years after the incident just given. I think it was in 1860 or 1861.... In the rounds of his practice he had a patient, about whom he was very anxious. It was in the coldest winter weather, and the residence of the patient was about two miles distant. Visiting him early in the evening, he found him in a state so unsatisfactory, that he informed the family that if he did not find him better the next visit, he should change the medicine entirely. On rising the next morning, he went to the barn to put his horse to the cutter for an early start. He was a little puzzled at finding things somewhat misplaced, but supposed some person had been at the stable in search of a missing article. On visiting the patient, he was gratified to find a marked improvement. He inquired when the improvement commenced, and was answered, ‘Immediately after taking the powders which he had given in the night.’ The truth flashed upon him at once, but concealing his emotion, he inquired, with as careless an air as he could assume, ‘About what time was it when I was here?’ They replied, ‘Between two and three o’clock.’ This proved to have been the case, as he was afterwards told by the family where he boarded. He had been giving the patient some fluid medicine, which he ordered discontinued, and then put up several powders, such as he had concluded upon the night previous, combining them as usual, and administering the first one himself.”
The foregoing examples illustrate the fact that[Pg 191] ordinary vision is not necessary to guide the movements of the somnambulist. Sometimes the patient walks about with open eyes; on other occasions they are firmly closed. It is generally admitted that the tactile and muscular senses are greatly exalted, so that they furnish guiding sensations which are sufficient to direct the most complicated movements. The history of the medical student observed by Dr. Allen shows how preternaturally sensitive the organs of vision may become—actually seeing the clock in the dark during the somnambulic paroxysm. When one considers the remarkably hyperæsthetic condition of the senses in certain other forms of nervous disorder, it is not surprising that sensory impressions which would be wholly neglected in a healthy waking state, may become sufficient to excite perceptions and to guide the movements which they have aroused. It is undoubtedly true that in certain cases the somnambulist does derive some information through the medium of the eyes—does really see; but it is also a fact that he only sees, hears, tastes and feels the objects which are immediately related with the action of his dream. It appears also that an impression derived from any organ of sense may suffice to arouse any other or all of the internal organs of perception, so that the patient seems to see, to hear, and even to taste objects which he knows only through the sense of touch. Sometimes the image thus externalized coincides with the actual reality; but often this is not the case, as, in the experience of the young clergyman, the somnambulist seemed to see the paper which he only perceived through contact with his fingers. The[Pg 192] image thus created corresponded exactly with the external fact; but when a similar contact with a pile of bed-clothes excited the illusion of a drowning child in his grasp, the internal image did not in the least correspond with the external object, and he probably derived no information through the sense of sight in either case. In another instance, however, as we shall learn upon another page, the subject is so far dependent upon the sense of sight that its obstruction is sufficient to arrest his movements, as certainly as if he were awake.
Ordinarily the memory is not impressed by the events of the somnambulic dream, but we have already learned that it is sometimes affected precisely as in common dreaming. One of my little acquaintances could not find her night-dress when she went to bed one night. She was therefore obliged to wear a gown that was old and ragged. Later in the evening her sister discovered the missing garment, and laid it over a chair in the bed-room. In the morning the night-dresses had changed place, and the ragged one occupied the chair. This occasioned considerable surprise, until the child remembered that during the night she had dreamed that two of her playmates had come to sleep with her, and that she felt so mortified at being seen in a ragged dress that she got out of bed and changed her night-gown. Sometimes the events of a somnambulic paroxysm are remembered during a subsequent attack, though they are forgotten during the interval, as in a case, reported by Macario, of a young girl who had been violated during somnambulic sleep. On awaking she had no idea of anything[Pg 193] that had occurred, but during a subsequent paroxysm she told her mother all that had happened.[81] In certain cases a dim recollection of some particular incident may be retained, as in the case of my patient who was for eight weeks in the somnambulic state. On recovery, the only thing that she could remember was a momentary glimpse of some one who was holding up his fingers before her eyes. Meeting the physician, subsequently to her recovery, who had thus attempted to arouse her attention, she recognized in his countenance the features which had momentarily impressed her consciousness during the period of somnambulic life.
It is seldom observed that somnambulism is attended with dangerous tendencies, yet they are sometimes present. One of my patients once took by mistake ninety grains of chloral at a single dose. While under its effects she got out of bed, walked into her sister’s room, shook her fist in her face, and swore furiously at her. On awaking, next morning, she was greatly shocked by the account of this dreadful behavior, so utterly at variance with her usual temper and character. Another somnambulic patient one night rushed into her mother’s room, violently accusing her of stealing her pocket-book, and threatening vengeance if it were not returned. Such patients sometimes mislay the articles with which they occupy themselves during a paroxysm, and on waking they erroneously infer that they have been robbed. Sometimes, as in the celebrated case related by Mesnet, the natural propensities of the individual seem to be released from all restraint,[Pg 194] and brutal instincts guide the actions of the somnambulist, who then steals, or eats and drinks with the voracity of a savage. Ball and Chambard (loc. cit.) have collected a number of examples in which impulses to suicide or other forms of violence were manifested under such circumstances. Obviously, where the moral sense is asleep, and where the affection is the result of causes beyond the control of the patient, he cannot be held morally responsible for the consequences of such actions. His condition closely resembles that of the victim of epileptic mania who delivers himself during a paroxysm to all degrees of furious and homicidal violence, without retaining the slightest recollection of the fact after its conclusion. The closeness of the parallel between these two disorders is rendered further apparent by the circumstance that although all memory of the events of epileptic mania is usually abolished, it does sometimes persist after the termination of the attack. Thus, one of my epileptic patients for a time manifested symptoms of insanity after every fit. During one of these paroxysms he imagined that the sparrows on the housetop were all singing a particular tune which had attracted his attention shortly before the convulsion. Then it seemed to him that the breathing of his sleeping child whispered the same tune. Placing his hand upon the bosom of his wife, her breathing assumed the same musical character. Calling upon his family to listen to the wonderful music, they all asserted that they too could hear it. It was a considerable time after his recovery before he could be convinced that this vividly remembered experience was a pure illusion. The members[Pg 195] of his family had been cautioned against contradicting their father during his paroxysms; consequently, when he asked if they could hear the melody which delighted him, they answered affirmatively, and thus confirmed him in his delusion. To the ordinary form of epileptic mania such paroxysms sustain a relation similar to that subsisting between ordinary dreams and the somnambulic experience.
In like manner as it is often remarked that certain dreams betray a condition of unusual cerebral excitement, so do certain cases of somnambulism manifest a delirious exaltation of the faculties in action. This characteristic often belongs to the night-terrors of children. It is a condition in which the brain is occupied by the scenery of a vivid and highly dramatic vision which dominates the actions of the subject. This was most conspicuously shown in the following case, from J. P. Frank,[82] and in certain periods of the paroxysms observed by Mesnet (p. 198). Frank’s patient was a healthy and well nurtured young German girl, who during the wars of 1812 had been terribly alarmed by a party of French soldiers who had broken into the house and threatened to kill her father. The next day at the same hour she passed into a somnambulic state, which lasted till sunset. After a brief introductory period of agitation, she uttered a deep sigh, which was rather a sob than a sigh, and fell into a profound sleep. Presently she smiled, her countenance seemed lighted with inspiration, her right arm was raised in the air, and the left was directed towards the earth. In this cataleptic attitude she remained for[Pg 196] about a minute. She then seemed to have decided what to do; from an imaginary cartridge-box behind her back she pulled out a cartridge, bit off the end, poured out the powder upon her fist as if she were priming a musket. She then went through the motions of loading a gun, ramming down the wad with an imaginary ramrod, and cried out in French, a language which she had never heard before: “Marche! Ou est le baron? Sacré nom de Dieu!” Repeating the violent ejaculations and threats addressed by the soldiers to her father, she exhibited the utmost terror; her body was covered with a cold sweat, and she seemed ready to faint away. At this moment she woke up, called impatiently for her handkerchief, with which she wiped the perspiration from her face, and resumed her ordinary avocations as if nothing had happened.
Still more remarkable was the case reported by Dr. Mesnet.[83] From the excellent translation prepared by T. J. Huse, M. D.,[84] the following sketch has been outlined:
The patient, aet. 27 years, received in one of the battles near Sedan, during the Franco-Prussian war, a bullet wound which fractured the left parietal bone. His right arm was almost immediately paralyzed; after a few minutes the paralysis involved the right leg, and he lost consciousness. It was only after the lapse of three weeks that he recovered his senses. He was finally taken to Paris, where the paralysis gradually disappeared. From a period some three or four months after the reception of the injury, he began to[Pg 197] manifest periodical attacks of somnambulism, at intervals of fifteen to thirty days with an average duration of fifteen to thirty hours. During the whole of this time his life presented two essentially distinct phases—the one normal, the other pathological. In the normal condition he was able to gain a livelihood. He had been a clerk in several houses, a singer in a café, and while in the hospital had made himself useful and agreeable. The somnambulic attacks which he experienced were characterized by an instantaneous onset, resulting in the abolition of all his senses except the tactile sense. Sight was perhaps partially persistent, for on many occasions he seemed to be impressed by brilliant objects, but he was obliged to employ the sense of touch in order to understand their form, volume, etc. During all these crises his gait was easy, his attitude calm, his countenance peaceful; his eyes were widely open, with dilated pupils; the forehead and brows were contracted; there was an incessant nystagmus, indicating a disordered state in the brain; he was continually mumbling or muttering. When walking in a familiar locality he moved with perfect freedom; but if in a strange place, or if obstacles were placed in his way, he examined the obstructions by feeling of them with his hands, and turned easily aside. If any attempt was made to change his direction, or to quicken or retard his pace, he allowed himself to be directed like a mere automaton, continuing to walk in any way thus chosen for him. He would also eat, drink, smoke, dress himself, walk out, and retire to bed as usual. These processes seemed to be effected as a result of previous habit, without any actual[Pg 198] consciousness or feeling. He ate voraciously without discernment, and drank in the same manner ordinary wine, wine of quinine, water, assafœtida, without exhibiting any evidence of sensation whatever.
While under treatment in the Saint Antoine Hospital, this patient was carefully studied by Dr. Mesnet and by Alfred Maury, the celebrated author. They found that by means of impressions upon his tactile sensibility it was possible during any one of his paroxysms to suggest certain modes of action which were reproduced whenever he was again placed in the same conditions. Thus, “he was promenading in the garden, under a grove of trees, when some one put back into his hand the cane which he had let fall a few moments previously. He felt of it, turned his hand several times around the curved handle of the cane, became attentive, seemed to listen, and suddenly cried out, ‘hurry!’ then, ‘there they are! there are at least twenty of them, to the two of us! we shall get the better of them!’ and then, carrying his hand behind his back, as if to get a cartridge, he went through the movements of loading his musket, crouched at full length in the grass, concealing his head behind a tree, in the posture of a sharp-shooter, and following with his gun at his shoulder all the movements of the enemy whom he seemed to see close at hand. This scene often repeated in detail during the course of the observations, has seemed to each of us the most complete expression of an hallucination called up by an illusion of touch, which, giving to a cane the properties of a gun, awakened in this person remembrances[Pg 199] of his last campaign, and reproduced the struggle in which he was so grievously wounded.”
On another occasion the patient was at the end of a corridor, near a door that was locked; he “passed his hands over this door, found the knob, grasped it, and attempted to open it; failing to accomplish this, he sought for the keyhole, then for the key, which, however, was not there; then, passing his fingers over the screws which secured the lock, he endeavored to seize them and turn them for the purpose of detaching the lock. This entire series of actions bears witness to an effort of his mind connected with the object before him. He was on the point of leaving the door and turning towards another room, when I held up before his eyes a bunch of seven or eight keys; he did not see them; I jingled them loudly at his ear; he did not notice them; placing them in his hand, he immediately took hold of them, and tried them one by one in the keyhole, without finding the single one which could fit; he then left the place, and went into one of the wards, taking in his passage various articles with which he filled his pockets; at length he came to a little table used for the records of the wards. He then passed his hands over the table, but it was empty; in feeling of it, however, he came across the handle of a drawer; opening it, he took up a pen, and all at once this pen suggested to him the idea of writing; for at that moment he began to ransack the drawer, taking out and placing on the table several sheets of paper, and also an inkstand. He then sat down and commenced a letter, in which he recommended himself to his commanding officer for his good conduct and bravery, and made application for the[Pg 200] military medal. This letter was written with many mistakes in it, but these were identical as regards expression and orthography with all that we have seen him make in his healthy state. While the patient was writing, he aided us in an experiment that encouraged to immediately examine in what degree the sense of sight assisted in the performance of this action. The facility with which he traced his letters, and followed the lines upon the paper, left no doubt concerning the exercise of vision upon the writing; but, in order to make the proof satisfactory, we have several times interposed a thick plate of sheet-iron between his hands and his eyes when he was writing; and, although all the visual rays were intercepted, he did not immediately break off the line he had begun; he still continued to trace a few words written in an almost illegible manner with the letters entangled in each other; then finally he stopped without manifesting either discontent or impatience. The obstacle removed, he finished the uncompleted line, and began another. The sense of sight was therefore in full activity, and essential to the written expression of the patient.” Other observations showed that the sense of sight was only roused at the instance of touch, and that its exercise remained limited to those objects alone with which it was actually connected by the touch.
On another occasion he passed through a long ward of patients, “taking indiscriminately every article that came within his reach, and concealing them afterwards under the quilt, under a mattress, under a chair-cover, and under a pile of sheets. Arrived in the garden, he took from his pocket a book of cigarette papers, opened[Pg 201] it, and detached a leaf from it; then took out his tobacco and rolled a cigarette with the dexterity of one who is accustomed to this proceeding. He searched for his match-box, lighted his cigarette with a match, which falling still burning on the ground, he extinguished by placing his foot upon it; then smoked his cigarette while strolling back and forth to the entire extent of the garden, without any of these actions presenting the slightest deviation in their manner from the ordinary method. Everything that he did was the faithful reproduction of his ordinary round of life.
“This first cigarette terminated, he prepared to make another, when we stepped up and began to interpose obstacles.... He searched vainly in his pocket for his tobacco, as we had filched it. He searched for it in another pocket, going through all his clothes until he came back to look for it in the first pocket, when his face expressed surprise. I offered him his tobacco-pouch, but he did not perceive it; I held it near his eyes, yet he still did not perceive it; even when I shook it just in front of his nose, he did not notice it. But when I placed it in contact with his hand, he seized it and completed his cigarette directly. Just as he was about to light his cigarette with one of his matches, I blew it out and offered him instead a lighted match which I held in my own hand; he did not perceive it; I brought it so close to his eyes as to singe a few lashes, yet he still did not perceive it, neither did he make the slightest motion of blinking.... The patient sees certain objects and does not perceive others; his sense of sight receives[Pg 202] impressions from all objects in personal relation with himself through the touch, and does not receive impressions, on the contrary, from things external to him; he perceives his own match, but does not perceive mine.”
During the course of this observation the patient gave evidence that the memory of his former occupation as a professional singer had been revived. He began to hum some of the familiar airs, and then proceeded to his room in the hospital, where he carefully dressed himself as if for a public performance. “On his bed he chanced to meet with several numbers of a periodical romance, which he turned rapidly over without finding that for which he was searching.... I took one of those numbers, rolled it up, and putting it into his hand in that condition, satisfied his want by this semblance of a roll of music, for he then took his cane, and traversed the ward with a slow step, well contented. When stopped on his way, for the purpose of taking off the coat he was wearing (which had been foisted on him by one of the observers), he permitted it without offering any resistance.... At this moment the sun lit up with a bright ray a glass window that closed the lodge on the side towards the court.... This ray must have given him the impression of a footlight, for he at once placed himself before it, readjusted his toilet, opened the roll of paper which he carried in his hand, and softly hummed an air, running his eyes over the pages as he slowly turned them, and marking with his hand a measure that was perfectly rhythmical. Then he sang aloud, in a highly agreeable manner, giving his song the correct expression, a patriotic ballad to which we all[Pg 203] listened with pleasure. This first selection terminated, he sang a second, and afterwards a third. We then saw him take out his handkerchief to wipe his face. I offered him a wine-glass of a strong mixture of vinegar and water, which he did not notice; I placed the glass under his nose without his perceiving the smell of the vinegar; I put it into his hand, and he drank it without complaining of any unpleasant sensation.”
The conclusions which may be drawn from this remarkable history have been sufficiently expressed by Dr. Mesnet[85] in the following words:
“The disturbance which these functional perversions of the nervous system bring into the course of life, extends not only to the organs of sense, and to intellectual actions properly so called, but it also sometimes awakens some instinctive excitation which surrenders the individual without any defence, and destitute of rational discernment, to the most deplorable impulses. He acts with the semblance of a freedom which he does not possess; he seems to prepare and to combine certain actions in the light of conscious volition, when he is in reality only a blind instrument, obedient to the irresistible mandates of an unconscious impulse.”
The bearing of these conclusions upon the question of the moral responsibility of the somnambulist needs no further advertisement.
The likeness of certain features of such cases to the phenomena of hypnotism is worthy of note. In this particular there is an evident likeness between the[Pg 204] cerebral susceptibility of the ordinary dreamer, the somnambulist, and the hypnotised subject. All are alike in a condition which renders their imagination and their volition subservient to guiding sensations from without, so that their movements may be directed by the will of another. We have seen how the course of an ordinary dream may be modified by such suggestions. The history of the patient just related, illustrates the manner in which the actions of a somnambulic dreamer may be controlled by the will of a spectator. The ordinary phenomena of hypnotism exhibit the same subjection to the will of another. It is probable that a considerable part of the superior notoriety which belongs to this feature of hypnotism, is due merely to the fact that natural somnambulism is rarely made the object of such experiments and observations as are daily applied to the subjects of artificial somnambulism.
Somnambulic Life.—We come now to the last term of the series, the simplest, yet perhaps the rarest form of the affection. In this form, the patient seems perfectly awake; he is in possession of all his senses; he is capable of sustained and rational volition; he lives and behaves, in short, like any other person. But his life is divided into periods which are, so far as consciousness is concerned, completely distinct from each other. This double-consciousness may be exhibited but once in a lifetime, or it may be frequently repeated, so that the patient oscillates between the two states until it becomes doubtful which is the natural condition and which is the acquired. These states of double-consciousness are divided from each other by a[Pg 205] more or less complete break in the chain of memory. The residual strata which, so to speak, have been deposited from the sea of events upon the floor of memory, have become broken and “faulted.” The line of rupture marks the division between the two fields of consciousness; they no longer lie in the same plane, consequently there can be little or no continuity of memory between them. The events which transpire in one state affect the mind so long as, and whenever it is in connection with the cerebral register which is fitted to that state; as soon as the connection is shifted, the mind takes cognizance of the events that are recorded upon the other portion of the register, but, for want of physical continuity between the different portions of the record, the mind cannot at once receive a continuously connected report from the entire organ of recollection. From this results a mode of life essentially similar to the life of certain epileptics who are ushered by each seizure into a state of apparently conscious activity of which they have no recollection after recovery. Thus, one of my epileptic patients, who was subject to seizures, both of the convulsive and the non-convulsive form of the disease, on one occasion left home, after a fit, and traveled a considerable distance into the country, putting up for the night at taverns and farm houses, and apparently behaving like any other respectable citizen. It was three weeks before he came to himself. On recovering his normal consciousness, the period of his wanderings was a perfect blank in his memory. Such attacks are usually of shorter duration, and are more frequently associated with hysteria; bearing to[Pg 206] the hysterical paroxysm the same relation which they share with the epileptic fit. When the predisposing temperament exists, a great variety of excitations may serve to produce the phenomena, so that unless careful observation is employed, the truly somnambulic character of the paroxysm may easily be overlooked. Thus, the true nature of the affection was not suspected by the early attendants of the patient who became the subject of lethargic stupor, as related on page 173. Under the influence of powerful drugs acting upon a highly sensitive nervous organization, she became, at first, “hystericky.” She manifested great distress, complained bitterly of her sufferings, passed through the ordeal of several consultations, was subjected to a considerable surgical operation, and only ceased to appear conscious at the expiration of five weeks, when she passed into the lethargic state previously described. At the time of my first visit, just before the commencement of stupor, she walked into the room where I was waiting, greeted me with her usual affability, gave me some account of her sensations, and neither did nor said anything that could lead me to suspect that she was not in her normal frame of mind. But, with the exception of the single incident mentioned on page 193, the entire period from the commencement of her medication to the close of the lethargic stupor was utterly blotted out of her recollection.
Macnish[86] relates a similar case of a young lady who “unexpectedly, and without any forewarning, fell into a profound sleep which continued several hours beyond[Pg 207] the ordinary term. On waking, she was discovered to have lost every trace of acquired knowledge. Her memory was tabula rasa—all vestiges, both of words and things, were obliterated and gone. It was found necessary for her to learn everything again. She even acquired, by new efforts, the art of spelling, reading, writing, and calculating; and gradually became acquainted with the persons and objects around, like a being for the first time brought into the world. In these exercises she made considerable proficiency. But, after a few months, another fit of somnolency supervened. On rousing from it, she found herself restored to the state she was in before the first paroxysm; but was wholly ignorant of every event and occurrence that had befallen her afterward. During four years and upwards she has passed periodically from one state to the other, always after a long and sound sleep.... The former condition of her existence she now calls the Old State, and the latter the New State; and she is as unconscious of her double character as two distinct persons are of their respective natures. For example, in her old state she possesses all the original knowledge; in her new state only what she acquired since. If a lady or gentleman be introduced to her in the old state, or vice versa (and so of all other matters), to know them satisfactorily she must learn them in both states. In the old state, she possesses fine powers of penmanship, while in the new, she writes a poor, awkward hand, not having had time or means to become expert. Both the lady and her family are now capable of conducting the affair without embarrassment. By simply knowing whether she is in the old[Pg 208] or new state, they regulate the intercourse, and govern themselves accordingly.”
Another remarkable case was reported at length by Dr. Azam, of Bordeaux.[87] The principal facts are given in a translation by Dr. J. I. Tucker in the Chicago Journal of Nervous and Mental Disease.[88] The patient was a young woman who began to exhibit the symptoms of hysteria at the age of puberty, and from that time till the present, a period of nearly thirty years, she has lived a double life, passing alternately from normal life into somnambulic life. These transitions were ushered in by a sharp pain in both temples, followed by a species of stupor, lasting about ten minutes. She would then open her eyes, apparently awake, and would remain in the condition of somnambulic life for an hour or two, when the languor and sleepiness would reappear for a few minutes, after which she would awaken in her normal state. At first these paroxysms were renewed every five or six hours; but, as she grew older, they occurred less frequently, and were greatly prolonged, until, finally, the periods of somnambulic life considerably exceeded the duration of normal life. During normal life she was hypochondriacal, hysterical, and a sufferer with neuralgia. During somnambulic life she was free from pain, lively, imaginative, and coquettish. While in this state of existence she remembered the events of her entire life—normal or otherwise; but on returning to her natural mode of life, she retained no recollection of her somnambulic periods.[Pg 209] Memory, during normal life, was limited to anterior normal periods. As time advanced, this peculiar mode of existence became an increasing source of inconvenience and mental distress, often leading the superficial observer to suppose that she was insane.
This case differs from the others in the circumstance that the period of somnambulic life was more vigorous and healthy than the ordinary condition. This seems to suggest an explanation of the forgetfulness which marked the period of normal life. During that period the functions of the brain were depressed, so that its molecular movements could not reach the level of the field of consciousness occupied during the second period. Other observations, such as that of Sir Henry Holland,[89] who, while exhausted by fatigue, lost all recollection of the German language until he was restored by rest and food, indicate that such defects of memory depend upon a deficient nutrition of the brain substance—a condition which is undoubtedly associated with an enfeebled cerebral circulation. We may, therefore, suppose that in Dr. Azam’s case the paroxysms of somnambulic life were induced by periodical discharges of force within the brain, causing an improvement in the circulation of blood, and a corresponding gain in health and general vivacity. Such exaltation of the faculties would be perfectly consistent with an exercise of memory covering all the events of life. But, when, as in cases like that reported by Macnish, and by myself, somnambulic life is the result either of disease or simple somnambulic sleep, it is a condition in which, as in physiological sleep, the cerebral functions, taken[Pg 210] as a whole, are depressed rather than exalted. The resulting train of ideas is developed upon a plane below the level of ordinary consciousness, and is, consequently, as easily forgotten as the dreams which are developed during sleep.
Such, then, are the principal characteristics of somnambulism—a state in which dreams are supplemented by more or less complete and appropriate action; ordinarily without subsequent recollection of either dream or action. The somnambulic dream usually occurs during or soon after the period of deepest sleep, when the influences of the external world are most completely suppressed. Released from the control of its sensory portion, the remainder of the brain awakens, and becomes aroused to a condition of relative exaltation. No longer distracted by the solicitations of external sense, the attention is concentrated upon the hallucinations which constitute the dream. In the simpler forms of noctambulism only the automatic locomotive apparatus is awakened, and the sleeper moves in accordance with the impressions derived from habit, aided by actual exaltation of the muscular and tactile senses. But, in some of the more complicated cases, a certain amount of special sensibility seems to exist. The patient is capable of exercising just that amount of perception which is necessary to accomplish his purpose, though blind and deaf and insensible to every other impression. The more complete the waking of the sense-organs, the closer the resemblance to the condition of ordinary life, or even to the condition of ecstasy, in which cerebral exaltation is the prominent feature, and in which the power of recollection[Pg 211] generally persists. Accordingly, it sometimes happens that the somnambulist can recall the events of his paroxysm. In such cases the power of recollection is due to the same conditions that control the recollection of our ordinary dreams. But the phenomena of ordinary somnambulism are as completely as possible removed from all connection with the mental actions which arise directly from the operation of the senses. By reason of such isolation the ordinary association of ideas affords no help to the memory, and the dream remains in oblivion. Alfred Maury expresses the opinion[90] that the principal cause of forgetfulness of the events of somnambulism consists in the exhaustion of the cerebral elements through the intensity of the excitement to which they have been subjected during the paroxysm. Doubtless this, in certain cases, may contribute to the loss of memory, but it should be remembered that the excitement may be relative rather than absolute. Certain elements wake while others are asleep; and these waking cells may be aroused to a degree far in excess of what is usual during the sleep of the brain without attaining to the level of their diurnal activity. The mind, undisturbed by external impressions, gives its attention to the operation of these waking organs, and a dream with all its consequences, somnambulic or otherwise, is the result. In other words, the plane of consciousness, so to speak, is lowered in sleep to the level of these molecular vibrations. But when the entire brain has been completely reawakened, the residual vibrations of those elements which yielded the physical basis of the dream, and[Pg 212] which, had they originally occurred during the waking state, might have persisted with energy sufficient to furnish a groundwork for recollection of the ideas which they had first suggested, are no longer sufficiently forcible to be felt in consciousness. Recollection of mental states thus generated must necessarily be impossible under such conditions. Sometimes, however, the somnambulist who, while awake, had forgotten all the incidents of his somnambulic experience, can remember, in a subsequent paroxysm, all that occurred during the preceding attack. Facts of this kind have been observed in the waking life of certain hysterical persons, but the apparent doubling of their personality is connected with the waking state, or with its semblance, while in ordinary somnambulism it is only during sleep that the alternations of memory and forgetfulness occur. A similar recollection of previous visions is sometimes experienced in dreams, showing a close relationship between the dreams of sleep and of somnambulism. The bond of association between events thus isolated in time must be sought in a renewal of like conditions of the brain during the successive periods of somnambulic exaltation. We must suppose that the molecules which were in a state of excitement during the first paroxysm are again aroused in a similar manner after a period of waking quiescence. If, during sleep, their movements, though of an exalted character, have only just sufficed to arouse consciousness in the form of a dream, it is scarcely probable that during the phase of comparative inactivity which supervenes when the whole brain is awake, their residual motion could disturb the sphere of[Pg 213] consciousness. Hence the time occupied by their somnambulic vigor must remain a blank in memory during the waking state. But, when the original state of relative exaltation has been reproduced by a second paroxysm of disorder, if the same molecular movements be in any way renewed, the conditions of memory are fulfilled; consciousness is once more aroused as before, and the patient remembers the dream or the events of the previous attack.
ARTIFICIAL SOMNAMBULISM OR HYPNOTISM.
| There are more things in heaven and earth, Horatio, Than are dreamt of in your philosophy. —Hamlet. |
The phenomena of somnambulism are of apparently spontaneous origin, during ordinary sleep. But from the remotest antiquity it has been known that certain persons may be thrown into an artificial sleep which closely resembles the condition of the somnambulist. Such a degree of susceptibility is not common to all persons. Heidenhain, experimenting upon his class of medical students, found only one in twelve who was thus susceptible. My own experiments lead me to think that American medical students are less easily influenced in this direction. Charcot, whose field of observation covers the inmates of the Salpêtrière Hospital, finds the best examples of the hypnotic state among the hystero-epileptic females in that asylum. To the experiments of Heidenhain, in Germany, of Braid, in England, and of Charcot, in France, we are indebted for the most thoroughly scientific observation and interpretation of the phenomena of hypnotism.
The antecedent physical condition most favorable to the development of the hypnotic state is a highly unstable constitution of the nervous system. For this[Pg 215] reason the larger number of qualified subjects is furnished by the female sex—especially by those who possess the hysterical temperament. Frequent repetition of hypnotic exercises renders the subject still more susceptible. Heidenhain was, at first, inclined to the belief that such experiences were not prejudicial to the health of the subject, but the observations of Harting, in the University of Utrecht, and of Milne-Edwards, in Paris,[91] have demonstrated the fact of danger to the health of animals subjected to similar experiments. Hysterical patients have often exhibited considerable exhaustion after hypnotic exhibition in the hospitals of Paris (Charcot and Richer), consequently, it cannot be admitted that the practice is devoid of risk to the health of the individual.
Numerous methods of inducing the hypnotic state have been employed. The greater number consist in artificial modification of the condition of the brain through the agency of sensory impressions originated upon the periphery of the body. The simplest form of such influence is presented by the results of gentle friction of the skin with the palm of the hand or the tips of the fingers. Many an aching head has thus been relieved, many a restless sufferer soothed to sleep. In like manner, a susceptible subject may be hypnotized by any continuous and gentle excitement of the senses of sight, hearing, and touch. Concentration of the attention upon a brilliant object, like a piece of polished metal or a small mirror, especially if it be placed a little above the level of the eyes, and so near that considerable convergence of the eyeballs is[Pg 216] necessary for distinct vision, affords a very efficient means of inducing artificial somnambulism. Certain persons may be readily hypnotized by gently pressing the eyelids together, and at the same time making slight pressure upon the eyeballs. Others pass into this condition by merely closing their eyes, and remaining motionless in a quiet room.
The phenomena of artificial somnambulism are frequently developed through the agency of impressions derived directly from the sphere of consciousness. The intellectual effort of trying to sit still and think of nothing is sometimes sufficient to induce the hypnotic state. The ordinary devices by means of which wakeful people are taught to beguile sleep, by counting, or by repeating long lists of names, etc., all belong to this category. Compulsory attention to any continuous intellectual process, like adding up a column of figures, or trying to read a dull book, is sometimes effectual. If, with these, or with similar acts of attention, be associated the expectation that something unusual is about to occur, as when the individual is aware of being the subject of an experiment, the evolution of the somnambulic condition is greatly facilitated. Thus, one of the most recent methods, consists in merely sitting, for half an hour or more, with the back towards the patient. Attention, curiosity, and expectation, are thus excited, and a susceptible person soon begins to manifest some of the numerous and various forms of the hypnotic state. Heidenhain caused one of his students thus to go to sleep in broad daylight, by simply assuring him that he should hypnotize him from a distance at a particular hour of the afternoon. The[Pg 217] monks of Mt. Athos were accustomed to hypnotize themselves by fixing their eyes and their thoughts upon the navel; hence the reputation of omphaloscopy as an aid to ecstatic meditation.
The duration of hypnotic sleep is as variable as that of its prototype in natural somnambulism. The patient usually wakes spontaneously, after a few minutes or hours. Sometimes, however, the period of insensibility is greatly prolonged. If it be desirable to awaken the subject of experiment, a simple reversal of the movements by which sleep was induced may suffice. The paroxysm may be terminated by almost any sudden and energetic appeal to the senses, like an electric shock, a sudden illumination of the eye with vivid light, or a sharp puff of air upon the face.
The simplest phenomena connected with the hypnotic state are those transferences of cerebral perceptions which have been investigated by the Society for Psychical Research.[92] Certain sensitive persons, when blindfolded, are capable of reproducing with considerable accuracy visual images that have been impressed upon the mind of another. The sensitive subject is blindfolded and placed before a table with pencil and paper. Another person then goes out of the room, and gazes at some kind of drawing, geometrical figure, or other object selected without possibility of collusion with the subject of experiment. This person then returns to the room, and places his hand upon the head of the subject, at the same time fixing his attention upon the mental picture of the object. Presently the blindfolded subject takes the pencil and reproduces on[Pg 218] paper a rough drawing of the object in question. In some cases it is found possible to effect this transfer of impressions without actual physical contact,—the agent merely standing behind the sensitive subject and concentrating his thought upon the selected object. Closely akin to this is the method of muscle-reading, popularly known as mind-reading. The sensitive is blindfolded, and then presses against his forehead the hand of the person by whom he is to be guided. Almost immediately a tremor pervades his muscles, and he yields all his movements to the guiding influence of the individual with whom he is in contact. If now an object be concealed in any place that is known to the agent, the concentration of that person’s attention upon the hiding place suffices to direct the “mind-reader,” who immediately drags his companion to the given locality.
The explanation of these phenomena consists in a recognition of the fact that certain persons are gifted with nervous organs which are sensitive and responsive to nervous impulses and muscular movements that are too delicate for recognition by the percipient apparatus of ordinary mankind. The more complicated forms of artificial somnambulism result from the complication and exaggeration of the results of this inordinate sensitiveness through the agency of artificial sleep. As in natural somnambulism, so in the hypnotic state, certain organs become totally anæsthetic, while the sensibility of others is wonderfully exalted. Cutaneous sensation may be completely abolished, and the patient may become utterly insensible to every painful impression. The reflex functions may be[Pg 219] either suppressed or exaggerated, and the special senses of sight and hearing may be exalted to the highest degree. While in this condition the hyperæsthetic condition of the brain renders the subject peculiarly susceptible to impressions from the will of another, so that all his actions are obedient to the guiding influence of the person under whose control he has passed.
According to Charcot,[93] three principal types of artificial somnambulism may be remarked among the hysterical subjects upon whom he experimented: (1) the cataleptic, (2) the lethargic, and (3) the somnambulic. Of these the first may be developed primarily by any abrupt and powerful impression upon a sensory organ. Gazing upon a brilliant light, fixing the eyes upon a piece of polished metal, or upon the shining eyes of a second person, the sudden clangor of a Chinese gong, may suffice to induce the cataleptic state. Dumontpallier[94] reports the case of a young woman who accidentally hypnotized herself by gazing into the mirror before which she was dressing her hair. This cataleptic state may also be secondarily induced by merely opening the eyes of a patient in whom a condition of hypnotic lethargy has been previously developed. If only one eye be thus opened, the corresponding side of the body alone becomes cataleptic. Closing the eyes causes the disappearance of this symptom, with complete restoration of the purely lethargic state. During the cataleptic condition the several tendinous reflexes disappear, neuro-muscular hyper-excitability[Pg 220] ceases, the skin becomes insensible, but the special senses, particularly those of sight and hearing, maintain a partial activity. In this half-awakened state the senses may become avenues of suggestion from without for the production of movements; but, if left to themselves, the limbs remain motionless.
The lethargic state may be induced by simply pressing together the eyelids of the subject, or by causing him to fix his gaze upon some definite object. The paroxysm begins with a deep inspiration, causing a peculiar laryngeal sound, followed sometimes by the appearance of a little foam on the lips. The eyelids are either wholly or partially closed, and are in a state of continual tremulous motion. The eyeballs are generally turned upwards and inwards. The muscles are completely relaxed. The tendinous reflexes are exaggerated; pressure over a muscle, or upon a nerve, arouses a peculiar contracture of synergic muscles and groups of muscles that are supplied by the excited nerve trunk. The facial muscles, however, do not thus become contractured; they merely contract during the application of the stimulus. If the lethargic subject be rendered cataleptic by opening the eyes, these contractures persist even after waking; and they can only be dispelled by renewing the lethargic state before resorting to pressure upon the antagonistic muscles—the process by which contractures peculiar to this species of lethargy may always be annulled. By the approach of a magnet to a contractured limb, the rigidity may be completely transferred to the corresponding muscles upon the opposite side of the body. If upon a limb of a lethargic subject who has been[Pg 221] rendered cataleptic by opening the eyes, an Esmarch’s band be applied, pressure over the bloodless muscles excites no contracture until the band is removed. A contracture is then developed, and it may be transferred to the opposite limb by the approach of a magnet. To this phenomenon has been applied the term latent contracture.
The extraordinary muscular excitability manifested by these subjects is further illustrated by an observation recorded by Dumontpallier.[95] If one end of an India rubber tube, half an inch in diameter, and five or six yards in length, be applied over a muscle in the leg, and if the other end be in like manner connected with a watch, every movement of the second hand will be followed by a slight contraction in the muscle. The same result follows connection with the wire of a telephone; and, if a microphone be introduced into the circuit, the incidence of a ray of light upon the instrument, or even its reflection from the conjunctival surface of the eye of a spectator, will arouse a responsive muscular contraction. Charcot has also seen muscular motion upon the opposite side of the body when a mild galvanic current was applied to the parietal surface of the skull, presumably over the motor centres of the corresponding half of the brain.
During these manifestations of muscular hyper-excitability, there is complete insensibility to pain, but the senses of sight and hearing seem to preserve some degree of activity. The subject, however, does not often exhibit any susceptibility to influence by suggestion.
[Pg 222]The somnambulic state may be directly induced by fixed attention with the eyes, by feeble and monotonous excitement of the senses, by passing the hands over the face and arms of the subject, and by many other processes of analogous character. This variety constitutes the ordinary form of hypnotic sleep. It may be very easily developed during either the lethargic or the cataleptic state as a consequence of pressure or of gentle friction upon the top of the head. Thus Heidenhain, in the course of his experiments, caused muscular paralysis by rubbing the scalp. Friction of one side of the head occasioned paralysis of the opposite side of the body without notable affection of the consciousness of the subject. The eyes and the eyelids behave as in the lethargic state. The subject seems to be asleep, but there is less muscular relaxation than in the lethargic variety. There is no exaggeration of the tendinous reflexes, and muscular hyper-excitability is absent. But by lightly touching or breathing upon the surface of a limb, its muscles may be thrown into a condition of rigidity which differs from the contracture of the lethargic state, in the fact that it does not yield to excitement of the antagonistic muscles, though yielding readily to a sudden repetition of the same form of excitement by which it was originally produced. Thus a subject under my own observation who, by pressure upon the eyeballs, was rendered insensible to every form of painful stimulation, would immediately pass into a state of perfect rigidity, if his limbs and body were rubbed for a few seconds with the palm of the hand. While in this condition, if the heels were placed upon[Pg 223] a chair and the back of the head upon another, not only could the entire weight of the body be thus supported, but also the additional weight of another full-grown man, sitting upon his body, without causing any more yielding than if it had been a log of wood that was lying across the chairs. From the immobility of the cataleptic state this rigidity differs by its greater degree of resistance to passive motion. Though insensibility to pain may be perfectly developed in this state, there is generally an exalted condition of certain forms of cutaneous sensibility, and of the muscular sense. Strange perversions of other special senses are sometimes remarked. Thus, Cohn[96] discovered that a patient who was naturally color-blind, was able, when unilaterally hypnotized, “to distinguish colors which were otherwise undistinguishable.” Conversely, when the cataleptic state is induced, the healthy eye becomes incapable of discerning colors. Spasm of accommodation is also present, and is one of the earliest demonstrable symptoms of the hypnotic condition.
These remarkable exaggerations and perversions of sensibility have been the cause on the one hand, of much skepticism regarding the verity of the phenomena of hypnotism, and, on the other, of much credulity, extending even to a belief in the existence of supernatural and miraculous powers. The extraordinary character of these experiences is well illustrated by the following letter from Lieut. J. M. Brooke, of the United States Navy, to President Wayland, of Brown University. It may be found in “Wayland’s Intellectual Philosophy.”
[Pg 224]“Washington, Oct. 27th, 1851.
“SirIt affords me pleasure to comply with your request, made through my brother William, relative to some experiments performed on board the United States steamer ‘Princeton,’ in the latter part of the year 1847, she being then on a cruise in the Mediterranean. Nathaniel Bishop, the subject of the experiments, was a mulatto, about twenty-six years of age, in good health, but of an excitable disposition. The first experiment was of the magnetic or mesmeric sleep, which overpowered him in thirty minutes from the commencement of the passes made in the ordinary way, accompanied with a steadfast gaze and effort of the will that he should sleep.
“In this state he was insensible to all voices but mine, unless I directed or willed him to hear others; he was also insensible to such amount of pain as one might inflict without injury, that is, what would have been pain to another. He would obey my directions to whistle, dance or sing. When aroused from this sleep he had no recollection of what occurred while in it. That such an influence could be exerted, I was already aware, having previously witnessed satisfactory experiments. Of clairvoyance I had never been convinced; indeed, considered it nothing but a sort of dreaming produced by the will of the operator. I became aware of its truth rather through accident than design.
“It happened, one day, that some of my brother officers asked a question which the others could not answer. Bishop, who had been a few moments before in a mesmeric sleep, gave the desired information, speaking with confidence and apparent accuracy. As the information related to something which it seemed almost impossible to know without seeing, we were very much surprised. It struck me that he might be clairvoyant; and I at once asked him to tell me the time by a watch kept in the binnacle, on the spar or upper deck, we being on the berth or lower deck. He answered correctly, as I found upon looking at the watch, allowing eight or nine seconds for time occupied in getting on deck. I then asked him many questions with regard to objects at a distance, which he answered, and, as far as I could ascertain, correctly.
“For example, one evening, while at anchor in the port of Genoa, the captain was on shore. I asked Bishop, in the presence of several officers, where the captain then was. He replied, ‘At the opera with Mr. Lester, the consul.’ ‘What does he say?’ I inquired. Bishop appeared to listen, and in a moment replied: ‘The captain tells Mr. Lester that he was much pleased with the port of Xavia; that the authorities treated him with much consideration.’ Upon this, one of the officers laughed, and said that when the captain returned he would ask him. He did so, saying, ‘Captain, we have been listening to your conversation[Pg 225] while on shore.’ ‘Very well,’ remarked the captain, ‘what did I say?’ expecting some jest. Then the officer repeated what the captain had said of Xavia and its authorities. ‘Ah,’ said the captain, ‘who was at the opera? I did not see any of the officers there.’ The lieutenant then explained the matter. The captain confirmed its truth, and seemed much surprised, as there had been no other communication with the shore during the evening. I may remark that we touched at several ports between Xavia and Genoa.
“On another occasion, an officer being on shore, I directed Bishop to examine his pockets; he made several motions with his hands, as if actually drawing something from the officer’s pockets, saying, ‘Here is a handkerchief and a box; what a curious thing! full of little white sticks with blue ends. What are they, Mr. Brooke?’ I replied, ‘Perhaps they are matches.’ ‘So they are,’ he exclaimed. My companion, expecting the officer mentioned, went on deck, and meeting him at the gangway, asked, ‘What have you in your pockets?’ ‘Nothing,’ he replied. ‘But have you not a box of matches?’ ‘Oh, yes!’ said he. ‘How did you know it? I bought them just before I came on board. The matches are peculiar, made of white wax with blue ends.’
“The surgeons of the ‘Princeton’ ridiculed these experiments, upon which I requested one of them (Farquharson) to test for himself, which he consented to do. With some care he placed Bishop and myself in one corner of the apartment, and then took a position some ten feet distant, concealing between his hands a watch, the long hand of which traversed the dial. He first asked for a description of the watch. To which Bishop replied, ‘’Tis a funny watch, the second hand jumps.’
“The doctor then asked him to tell the minute and second, which he did; directly afterwards exclaiming, ‘The second hand has stopped!’ which was the case, Dr. Farquharson having stopped it. ‘Well,’ said the doctor, ‘to what second does it point, and to what hour, and what minute is it now?’ Bishop answered correctly, adding, ‘’Tis going again.’ He then told twice in succession the minute and second.
“The doctor was convinced, saying that it was contrary to reason, but he must believe. I then proposed that the doctor should mark; and directed Bishop to look in his mother’s house, in Lancaster, Pa., (where he had never been) for a clock; he said there was one, and told the time by it; one of the officers calculated the difference in time for the longitudes of Lancaster and Genoa, and the clock was found to agree within five minutes of the watch time.”
Such clairvoyance is very rare; in fact, it is difficult, at first thought, to believe in its existence. Nor should[Pg 226] its alleged possession be credited in any instance until all possibility of deception has been excluded. The example just related seems to be, in this respect, one of the best, for the reason of its occurrence in a little group of men whose isolation and thorough acquaintance with each other must have reduced the chances of simulation to the lowest degree. When carefully considered, moreover, it is apparent that the exaltation of the functions of sight and of hearing in this case was not different in kind or in degree from that that has already been recorded in connection with certain cases of natural somnambulism and of dreaming. The condition of the brain is probably identical in all such instances; it is the mode of its induction that is subject to variation. The remarkable feature of the hypnotic state consists in its production at the pleasure of either the subject or of the agent under whose control he has passed; whereas the phenomena of natural somnambulism and of the clairvoyant dream occur only during sleep, and independently of the will of the patient.
Another singular fact in this connection is the receptivity of the hypnotized brain for suggestions from the minds of other persons. Usually, the patient is insensible to all communications which do not emanate from the agent by whom he is held in control; but in certain cases it is probable that the brain is more or less open to impressions of a particular sort from any source. Numerous examples illustrate the manner in which the course of an ordinary dream may be thus directed. The hypnotic dream is far more easily modified by suggestions from without. The simplest examples of this are exhibited by the[Pg 227] hypnotized subject who walks, jumps, lies down, executes every variety of pantomime, in obedience to the commands of his director. Somewhat more complicated are the actions that are developed through excitement of the imitative faculties. Every movement of the director that can be perceived by the subject will be at once reproduced. Dr. Fischer relates[97] the case of a patient who, although exceedingly ignorant of the art of music, was able, during the hypnotic paroxysm, to sing with Jenny Lind all kinds of songs, so accurately that it was impossible to distinguish their separate voices. Expression of the various emotions and passions may also be provoked by merely placing the subject in the several attitudes characteristic of such feelings.
In the lower grades of the hypnotic state, consciousness is not abolished, and the subsequent recollection of events during the experience may be quite perfect. In such cases illusions and hallucinations, that were excited by suggestions from the controlling mind of another, survive in memory, and become the causes of serious delusion. Witness, for example, the manner in which excitable people, partially hypnotized in a so-called “spiritual circle,” believe in the reality of the illusions which have occupied their powers of perception during a “seance.” To this inferior grade of self-induced hypnotism belong all those conditions of sensory hyperæsthesia by means of which certain persons are enabled to read the hidden thoughts of others. This capacity is, essentially, a mere exaltation of that power which all mankind shares in a greater or less[Pg 228] degree. In every instance it has been remarked that the ordinary “medium” can only respond correctly to questions for which the true answer is present in the mind of the questioner. To all other interrogatories the replies are delivered purely under the influence of random suggestion. In some cases the pathway of communication lies through actual bodily contact, as in ordinary “mind-reading,” where the invisible molecular oscillations of the muscular elements of one person serve to guide the perceptions and movements of another. But, more frequently, the transmission of ideas is effected through the action of the facial and ocular muscles. From these organs of expression the “table-rapper,” or the “planchette-writer,” reads the unspoken thoughts of the questioner, in a manner very like, yet vastly more delicate than that by which deaf mutes are taught to interpret the movements of the lips of persons with whom they converse. This fact is clearly illustrated by the experience of Maury,[98] in an interview with a celebrated table-rapper who, without the slightest hesitation, made known to him the age, name, and date of death of a brother whom he had lost. She also gave the same information regarding his father, and pronounced the names of other persons upon whom he had fixed his attention. But, if he turned away his face, or if he concealed his eyes so that the woman could no longer scrutinize their expression, her responses became entirely uncertain and destitute of conformity with fact.
The induction of the hypnotic state, if not too often repeated, is sometimes of considerable service in the[Pg 229] relief of various functional disorders of a painful character. This fact, enthusiastically announced, many years ago, by Dr. Braid, has recently been freshly brought forward through the experiments of Fischer,[99] Wiehe,[100] Rieger,[101] and others. In our own country this method of treatment has not yet been adopted by many in the medical profession, though its efficacy in a particular class of cases is not denied. Outside of professional circles, however, it is exploited to a considerable extent under the strange misnomer of Metaphysical Healing. But, as De Watteville has truly remarked,[102] “the time is near when the curative influence of hypnotism will be submitted to the same scrutiny as its physiological and psychological import has undergone.”
THE END.
Acids, 71
hydrobromic, 88
hydrochloric, 72
hydrocyanic, 100
hydrocyanic, in gastric disease, 103
lactic, 72
nitric, 72
nitro-muriatic, in hepatic insomnia, 103
phosphoric, 72
Aconite, 63, 93, 100
Africa, maladie du sommeil of, 30
winds from the deserts of, effect of, 46
Africans, habits of, regarding sleep, 40
victims of the maladie du sommeil, 30
Alcohol, 76
effect of, upon the brain, 54
in angina pectoris, 99
in asthma, 101
in chorea, 110
in dyspepsia, 103
in fever, 105
in hepatic diseases, 102
Allen, Prof. J. Adams, case of somnambulism observed by, 185
Allix, observations of, regarding bodily temperature in sleep, 7
Allix and Hohl, observations of, regarding the pulse in sleep, 6
Aloetic purgatives in insanity, 94
Ammonia, in fever, 105
Amyl nitrite, 84
in angina pectoris, 99
in asthma, 101
Anæmia of the brain, 53
Anæsthetics, 75
Angelic visitors, delusions regarding, 129
Angina pectoris, 99
Anti-spasmodic effects of belladonna, 69
Apparent death, 34
crucial test of, 35
Arabia, effects of wind from the deserts of, 46
Arago, observations of, regarding atmospheric electricity, 46
Arsenic, in asthma, 101
Atropia, 69
Atropine, use of, with opiates, 87
Artificial sleep, effect of, upon the process of oxidation, 9
mode of production of, 22
Artificial somnambulism, 214
cataleptic form of, 219
lethargic form of, 220
recollection of the events of, 227
somnambulic form of, 222
three varieties of, 219
Assafœtida, use of, in insomnia, 110
Assimilation, rate of, in sleep, 5
Association of ideas, cessation of, in sleep, 3
effect of, 123
Asphyxia, 100
Asthma, insomnia caused by, 101
relieved by atropine, 69
relieved by chloroform, 82
relieved by ether, 82
relieved by iodide of potassium, 110
relieved by lobelia, 71
relieved by stramonium, 71
relieved by tobacco, 71
Atmospheric electricity, effects of, 46
Australia, effect of winds from the deserts of, 46
Azam, a case of somnambulic life observed by, 208
Bachelder, Dr. G. H., observations of, on the maladie du sommeil, 32
Baillarger, hallucination excited by dreaming, 126
Ball and Chambard, classification of the varieties of somnambulism, 169
Baths, use of, as nervous stimulants, 60
cold, 73, 95
in fever, 104
in insomnia, 112
in scarlet fever, 76
shower, 95
warm, 94
Bartholow, on the use of phosphorus, 71
Beard and Rockwell, on the use of electricity, 62
Beer, effect of, 76
Belladonna, 69, 100
use of, in asthma, 101
use of, in fever, 104
use of, in hepatic diseases, 102
Bismuth, use of, in gastric diseases, 103
[Pg 232]
Bladder, insomnia in irritability of, 90
Blisters, use of, in rheumatism, 106
Blood, control of its circulation by the nervous system, 26
Bombardment, sleep during, 1
Boussingault, experiments of, on the process of oxidation in the tissues, 9
observations of, on respiration in sleep, 6
observations of, regarding the bodily temperature in sleep, 7
Brain, consequences of inordinate excitability of, 159, 161
exalted receptivity of, during the waking state, 150
exalted susceptibility of, in sleep and dreaming, 144, 150
the, its division into separate mechanisms, 13
the, a reservoir of sensory impressions, 124
Brandy, use of, in wakefulness, 77
Bromide of potassium, use of, in insanity, 95
of sodium, use of, in chronic alcoholism, 97
of sodium, use of, in delirium tremens, 98
Bromides, the, 88
use of, in convulsions, 110
use of, in delirium, 77
use of, in fever, 104
use of, in night terrors, 112
use of, in pregnancy, and after parturition, 109
use of, with chloral and morphia, 86
Brooke, Lieut. J. M., observations of, regarding hypnotic clairvoyance, 224
Bronchitis, insomnia caused by, 100
insomnia of, relieved with paraldehyde, 80
Brunton, Dr. T. Lauder, his theory of counter-irritation, 62
Butylchloral hydrate, 83
Buschick, experience of, in waking before earthquakes, 144
Caffeine, effect of, upon the brain, 54
Camphor, 67
use of, in asphyxia, 100
use of, in fevers, 105
use of, in the insomnia of cachexia, 108
use of, after parturition, 109
Cannabin, 69
Cannabin tannate, 68
Cannabis indica, 68
anti-aphrodisiac effect of, 69
use of, in delirium tremens, 98
use of, in fever, 104
use of, in insanity, 96, 97
use of, in pregnancy, 109
use of, as a substitute for hyoscyamus, 113
Cantharides, 63
Capsicum, 63
Capsicum, use of, in the insomnia of delirium tremens, 77, 98
Carbolic acid, vapor of, for relief of cough, 100
Carbon, oxidation of, during sleep, 7
Carbonic acid gas, discharge of, during sleep, 9
Cardiac debility, use of butylchloral in, 83
Cardiac disease, insomnia of, treated with paraldehyde, 80
treated with digitalis, 66
Cardiac dyspnœa, relieved with opiates, 87, 98
Cardiac neuralgia, 99
Carotid arteries, compression of, for relief of insomnia, 25, 27, 57
Cataleptic form of artificial somnambulism, 219
Catarrh, nasal, effect of sleep upon, 8
Caton, Judge John D., on the difficulty of sleep during the continuous daylight of summer in Norway, 40
Cerebral activity, effect of, upon bodily temperature, 8
Cerebral anæmia and its cause during sleep, 25, 28
use of phosphorus for, 71
Cerebral circulation, dependence of consciousness upon, 25, 27
during sleep, observations upon, by Professor Mosso, 26
Cerebral exhaustion, benefited by the use of phosphorus, 71
in fever, 105
Cerebral hyperæmia, effects of, 145
insomnia of, treatment with paraldehyde, 80
Cerebral irritation in cachectic states, 108
Cerebro-spinal meningitis, use of opiates in, 93
Cerebro-spinal weakness, 110
Change of life, use of valerian during, 68
Chicago, embarkation from, 45
the great fire in, 40
Child-birth, insomnia after, 81
Chloral, 82
Chloral hydrate, influence of, upon oxidation in the tissues, 9
association of, with morphia and bromides, 86
use of, in angina pectoris, 99
use of, in asthma, 101
use of, in cachexias with insomnia, 109
use of, in chorea, 110
use of, in chronic alcoholism, 97
use of, in delirium tremens, 98
use of, in fevers, 104
use of, in hepatic diseases, 102
use of, in insanity, 95
use of, in meningitis, 94
use of, in night terrors, 112
use of, in respiratory diseases, 100
Chlorodyne, 82
[Pg 233]use of, in syphilitic neuralgia, 107
Chloroform, 81
use of, in asthma, 101
use of, in convulsions, 110
spirit of, in the treatment of fevers, 105
Chossat, observations of, on the temperature of pigeons, 7
Circulation of blood, its regulation by the nervous system, 26
disorders of, 52
modified by counter-irritation, 63
state of, during sleep, 6
Clairvoyance, hypothetical explanation of, 148
in dreams, 146, 148, 149
in dreaming, and in natural somnambulism, 226
in the hypnotic state, 224
Clark, observations of, on the sleeping dropsy, 30
Codeia, 85
Codeine, 88
Coffee, effects of, upon the brain, 54
Cold, a nervous sedative, 73
Cold baths, 73
Cold, excessive, a cause of stupor, 47
Colic, uterine, relief of, 81
Color-blindness, effect of hypnotism upon, 223
Coma, 32
Coniine, 91
Conium, 90, 95
Consciousness, duration of the sensations required for its excitement, 23
state of, during sleep, 14
Convulsions, excited by compression of the carotid arteries, 27
treatment of, 110
Cough, spasmodic, treatment with spirit of chloroform, 82
Counter irritants, 62
Croton oil, 63
Cups, counter irritation with, 63, 93
Curci, observations of, regarding belladonna, 69
regarding morphia, 85
Cutaneous disorders, causes of insomnia, 55
DaCosta, on lithæmia, 106
Darkness, favorable to sleep, 18
Day and night, alternation of, a cause of sleep, 17
Death, apparent, 34
test of, 35
Degeneration of the brain, 55
Demme, observations of, on bodily temperature in sleep, 7
Delirium, 54
excited by hyoscyamus, 70
excited by stramonium, 71
of exhaustion, 77
treatment of, with musk, 67
Delirium tremens, treatment of, with alcohol, 77
with bromides, 89
with capsicum, 77
with chloral, 82
with digitalis, 67
Delusions, caused by dreams, 128
Depressing emotions, a cause of sleep, 19
Diagram, illustrating the stages of sleep, 4
the varieties of somnambulism, 172
Digitalis, indirectly hypnotic effect of, 66
treatment of delirium tremens with, 98
Diminution of energy, represented by sleepiness, 2
Disease and dissolution, revival of memory in, 165
Dover’s powder, 67, 100, 104, 110, 112
Double consciousness, 204, 206
Dreams, 116
analysis of, 133
at the moment of waking, 14
brevity of, 15
causes of, 118
cause of special vividness of, 134
clairvoyant, 146, 148, 149
coherence of, 131
definition of, 120
dependence of, upon partial sleep of the brain, 11
duration of, 135
excited by gustatory sensation, 43, 125, 130
by heat, 43
by painful diseases, 141
by sensory impressions during sleep, 29
by sounds, 41
incoherence of, 133
intellectual combinations in, 131
mode of their production, 124
primitive belief in the divine origin of, 160
prophetic, 142, 143
recollection of, 140
relation of, to depth of sleep, 4
relation of, to waking hallucinations, 126
resemblance of, to the mental processes of insanity, 133
revival of memory in, 162
somnambulic, 178
state of volition during, 141
suggested by external impulses, 125, 130
theory of, 116
waking, 123
Dropsy, treatment of, with digitalis, 66
Dumontpallier, case of self-hypnotism related by, 219
Duration of sleep, 110
Dyspnœa, cardiac, 98
treatment of, with digitalis, 66
Dyspeptic insomnia, 104
East Indies, climate of, a cause of insomnia, 44
Eggs, as an article of food, 66
Electrical test of apparent death, 35
Electricity, atmospheric, 46
use of, 62, 63
[Pg 234]
Emphysema, insomnia of, relieved with paraldehyde, 80
Energy, diminution of, represented by sleepiness, 2
renewal of, by sleep, 5
Epilepsy, double consciousness in, 205
Ether, hypnotic effect of, 81
inhalation of, 98
use of, in asthma, 101
use of, in convulsions, 110
use of, in irritative cough, 100
Ether, compound spirit of, 81
use of, in delirium tremens, 98
use of, in hepatic diseases, 102
Excrementitious substances, causes of insomnia, 55
Exhaustion, a cause of sleep, 19
relief of with alcoholic stimulants, 76
states of, 64
use of musk in, 68
Exner, experiments of, to test the possibility of dreamless sleep, 14
Eye, state of its secretions during sleep, 8
Facial neuralgia, treatment of, with butylchloral, 83
Fainting, a counterfeit of sleep, 25
Fatigue, a cause of sleep, 19
Fatigue theory of sleep, 20
Fevers, eruptive, treatment of with musk, 68
infective, 57
typhoid, 57
treatment of with cold baths, 73
Flaxseed tea, 100
Florida, climate of, in insomnia, 114
Fonssagrives, observations of, regarding atmospheric electricity and insomnia, 46
Food, lack of, a cause of insomnia, 63
Foot-baths, hot, in the treatment of insomnia, 93, 94
Force, fluctuations of, 15
kinetic, 15
potential, 15
Frank, J. P., case of somnambulism related by, 195
Functional nervous disorders, treatment of with hypnotism, 229
Gairdner, W. T., case of somnambulic lethargy reported by, 174
Gastro-intestinal glands, state of their secretions during sleep, 8
Gelsemium, 90
treatment of fever with, 104
use of, in the wakefulness of children, 112
Generation of ideas, relation of, to molecular movements in the brain, 24
Grasset, case of somnambulism related by, 177
Guérin, observations of, on the maladie du sommeil, 30
Guiana, delusions among the Indians of, founded upon dreams, 128
travels in, 42
Guy, observations of, regarding the pulse in sleep, 7
Hallucination, case of, related by Dr. E. H. Clarke, 156
experienced by Sir Edmund Hornby, 150
production of, by drugs, 120
sometimes excited by dreams, 126, 150
Hamilton, Sir William, experiments of, on the possibility of dreamless sleep, 14
Hasheesh, visions excited by, 120
Hayes, Dr. P. S., case of lucid lethargy reported by, 35
Headache, 54
Hearing, persistence of during sleep, 41
sense of, during sleep, 11
Heart, pulsation of, in sleep, 6
Heat, a cause of insomnia, 44
a nervous stimulant, 59
effects of excessive, 47
liberation of, during sleep, 9
Heidenhain, observations of, on hypnotism, 214
Helmholtz, observations of, on liberation of heat during sleep, 9
Hemicrania, treatment of, with butylchloral, 83
Henneberg, experiments of, on oxidation in the tissues, 9
Hibernation, phenomena of, 48
Hoffmann’s anodyne, 81
Hohl and Allix, observations of, on the pulse in sleep, 6
Holland, Sir Henry, observations of, regarding the loss of memory during exhaustion, 209
Hops, 90
treatment of chronic alcoholism with, 97
Hornby, Sir Edmund, experience of hallucination, 150
Horsford’s Acid Phosphate, 72
Horvath, observations of, on the temperature of hibernating marmots, 8
Hunger, 2
Hydrobromic acid, 88
Hydrochloric acid, useful in atonic dyspepsia, 72
Hydrocyanic acid, 100
in gastric diseases, 103
Hyosciamia, 70, 96
Hyosciamine, 70
Hyoscyamus, 70
use of, after parturition, 109
use of, in asthma, 101
use of, in fever, 104
use of, in hepatic diseases, 102
use of, in insanity, 96
use of, in insomnia of children, 112
use of, in renal diseases, 102
Hyperæmia of the brain, 52, 54, 110
Hypnagogic hallucinations, 3, 4
Hypnagogic state, 2
Hypnotic sleep, duration of, 217
Hypnotic sleep, clairvoyance in, 224
[Pg 235]condition of the special senses in, 223
conditions favorable to, 214
exaltation of the imitative faculty during, 227
methods of inducing, 215
perception during, 149
Hypnotism, 214
likeness of, to somnambulism, 203
observations of Braid, 214, 229
observations of Charcot, 214, 219, 221
observations of Cohn, 223
observations of De Watteville, 229
observations of Dumontpallier, 219, 221
observations of Fischer, 150, 227
observations of Harting, 215
observations of Heidenhain, 214, 215, 216, 222
observations of Milne-Edwards, 215
observations of Rieger, 229
observations of Wiehe, 229
receptivity of the brain to suggestions during, 226
suggestion of ideas during, 226
therapeutical use of, 228
Hysteria, a cause of double consciousness, 205
Hysterical excitement, treatment of, 68
Ice-cap, in the treatment of acute affections of the brain, 93
Iceland moss, for the relief of cough, 100
Ideas, their dependence upon molecular movements in the brain, 24
Illusions, excited by disease and by drugs, 120, 122
Imagination, persistence of, in sleep, 3
Imitative faculties, exaltation of, in hypnotic states, 227
Immermann, on cold baths, 73
Impulses to violence during somnambulism, 193
Im Thurn, Everard F., on dreams among the Indians of Guiana, 128
Indians, of Guiana, magic practices among, 42
Inflammations affecting the brain, 54
Inhalations, medicated, 100
Injuries of the brain, 55
Insanity, 54, 57, 70, 133
Insomnia, 38
Insomnia, causes of, 39
caused by aortic obstruction, 84
caused by asthma, 101
caused by cardiac disorders, 51
caused by cold, 47
caused by contagia of animal origin, 55
caused by cutaneous disorders, 49, 55
caused by dyspepsia, 51
caused by electrical disturbances, 46
caused by excrementitious substances, 55
caused by fatigue, 78
caused by heat, 44, 46
caused by heat and humidity, 44
caused by icterus, 49
caused by inflammations, 50
caused by insects, 49
caused by itching in myelitis, 49
caused by itch-mite, 49
caused by light, 39
caused by malaria, 72
caused by meningitis, 50
caused by miasms, 55
caused by morbid states of the central nervous organs, 51
caused by neuralgia, 50
caused by neuritis, 50
caused by neuromata, 50
caused by oxaluria, 72
caused by pain, 49
caused by parasites, 49
caused by periostitis, 50
caused by phosphatic diathesis, 72
caused by pneumogastric disorder, 51
caused by poisons, 55
caused by products of putrefaction, 55
caused by respiratory disorders, 51
caused by rheumatic diathesis, 72
caused by sounds, 41
caused by smells, 42
caused by stramonium, 71
caused by sympathetic nerve disorder, 50
Insomnia, occurrence of, after childbirth, 81
occurrence of, after parturition, 109
occurrence of, during acute affections of the brain, 92
occurrence of, during bronchitis, 80
occurrence of, during cardiac diseases, 66, 80, 87
occurrence of, during change of life in women, 84
occurrence of, during childhood, 110
occurrence of, during chorea, 110
occurrence of, during chronic alcoholism, 97
occurrence of, during chronic phthisis, 84
occurrence of, during delirium tremens, 87, 90, 97
occurrence of, during diseases of the heart and blood-vessels, 98
occurrence of, during diseases of the liver, 102
occurrence of, during diseases of the respiratory organs, 99
occurrence of, during disorders of nutrition, 107
occurrence of, during dysmenorrhœa, 84
occurrence of, during emphysema, 80
occurrence of, during febrile conditions and fevers, 87, 104
occurrence of, during gastric and intestinal disorders, 87, 103
occurrence of, during gout and rheumatism, 103, 107
occurrence of, during headache, 84
[Pg 236]occurrence of, during hysteria, 81, 89
occurrence of, during insanity, 94
occurrence of, during irritability of the bladder, 90
occurrence of, during irritability of the sexual organs, 90
occurrence of, during irritative dyspepsia, 90
occurrence of, during jaundice, 80
occurrence of, during lithæmia, 106, 107
occurrence of, during mania, 87, 89, 90
occurrence of, during melancholia, 96
occurrence of, during mental exhaustion, 89
occurrence of, during nervous disorders, 80
occurrence of, during neuralgia, 84
occurrence of, during old age, 78, 113
occurrence of, during opium habit, 84
occurrence of, during paretic dementia, 96
occurrence of, during phthisis, 80, 87
occurrence of, during pregnancy, 89, 109
occurrence of, during the puerperal state, 89
occurrence of, during renal diseases, 101
occurrence of, during rheumatism and gout, 105, 107
occurrence of, during sexual excitement, 89
occurrence of, during spasmodic diseases, 109
occurrence of, during states of exhaustion, 67
occurrence of, during syphilis, 106, 107
Insomnia, relation of, to states of the cerebral circulation, 57
relief of, by compression of the carotid arteries, 25
Iodide of potassium, treatment of asthma with, 110
Ipecac, treatment of asthma with, 101
Irritability of the brain, 53, 54
Itching of eczema, relieved with cannabis indica, 69
Jacobi, A., on wakefulness of children, 111
Japanese, use of massage among, 61
Jaundice, insomnia of, treatment with paraldehyde, 80
Jessen, case of hallucination caused by dreaming, 127
Joseph, St., dreams of, 142, 160
Judgment, suspension of, during sleep, 3
Kohlschütter, experiments of, to measure the depth of sleep, 16
Koumiss, 64
Lactic acid, hypnotic effects of, 72
Lactate of sodium, hypnotic effects of, 20, 72
Lactucarium, 88
Latent contracture, 221
Leeches, use of, 63, 93, 94
Lethargic form of artificial somnambulism, 220
Lethargy, 33
produced by excessive cold, 48
Lewin, observations of, on respiration during sleep, 6
experiments of, on oxidation in the tissues, 9
Liebermeister, experiments of, on oxidation in the tissues, 9
Life, normal, 4
possibility of intermissions in its active manifestation, 15
Light, interference of, with sleep, 40, 41
Liquors, effects of, 76
Lithæmia, a cause of insomnia, 106
Lithium bromide, 88
Lobelia, anti-spasmodic effects of, 71, 101
Lomi-lomi, 61
Lucid lethargy, 35
contrasted with somnambulic lethargy, 176
Lupulin, 90
Macario, case of somnambulism, reported by, 192
Mackinac, voyage to, 45
Macnish, case of somnambulic life, reported by, 206
Maladie du sommeil, 30
Malaria, treatment of insomnia, caused by, 72
Mania, use of chloral in, 82
Marmot, hibernation of, 48
temperature of, during hibernation, 8
Massage, 60, 109
Matter and mind, communication between, 22
Maury, A., classification of the varieties of somnambulism, 168
experience of, with table-rapping, 228
theory of, regarding forgetfulness of the events of somnambulism, 211
Measles, use of baths in, 74
Meat juice, 66
Memory, effect of physical exhaustion, 209
exaltation of, in somnambulism, 187
persistence of, in sleep, 3
relation of, to phenomena of somnambulism, 192
revival of, during disease and dissolution, 165
revival of, during dreaming, 162
Meningitis, 54, 57
Mental activity during sleep, 14
Mesnet, case of somnambulism related by, 196
Metaphysical healing, 229
Michigan, Lake, voyage upon, 45
Northern, summer climate of, favorable to sleep, 45
Milk, peptonized, 64
Mind and matter, communication between, 22
alternate states of action and repose, 15
sleep of, 15
state of, during sleep, 14
[Pg 237]
Mind-reading, 218, 227
Minnesota, summer climate of, favorable to sleep, 45
Mitchell, S. Weir, observations of, regarding effect of variable barometric pressure, 47
Molecular movement, its relation to the generation of ideas, 24
Moral responsibility in somnambulism, 203
Morphia, 97, 98, 100, 101
Morphine, influence of, on oxidation in the tissues, 10
Mosso, Professor, on the circulation of blood during sleep, 26
on respiration during sleep, 5
Mouth, condition of, during sleep, 8
Muscles, effect of sleep upon, 12
fibrillary twitching of, during sleep, 3
Muscle-reading, 218
Musk, 67, 100, 105
Mustard, 63
Nasal catarrh, state of secretion during sleep, 8
Narcotic stupor, 29
Nerves, of common sensation, affections of, 39, 49
pneumogastric, 51
sympathetic, affections of, causes of insomnia, 50
Nervous disorders, insomnia of, relieved with paraldehyde, 80
hypnotic treatment of, 229
Nervous irritation, effect of, on tissue change, 10
sedatives, 58, 59
stimulants, 58, 59
system, its control over the circulatory apparatus, 26
Neuralgia, cardiac, 99
treatment of, with alcohol, 77
treatment of, with belladonna, 69
treatment of, with preparations of valerian, 68
Neurasthenic patients, 66
New Providence, climate of, beneficial in insomnia, 114
Night and day, alternation of, a cause of sleep, 17
Night terrors, 179
treatment of, 89, 112
Nitric acid, 72
Noctambulism, 169
Noise, sleep prevented by, 41
North China Herald, criticism of Sir E. Hornby’s narrative, 155
Norway, difficulty of sleeping during the summer, 40
Nutrition, effect of sleep upon, 5, 9
disorders of, 52
Obersteiner, his theory of sleep, 20
Odors, effect of, upon sleep, 11
Old age, decline of life in, 113
Omphaloscopy, 217
Opium and opiates, 84, 98
Opiates, use of, in treatment of cachexias, 108
use of, in treatment of fever, 104, 105
use of, in treatment of gastric disease, 103
use of, in treatment of insanity, 96
use of, in treatment of renal diseases, 102
use of, in treatment of rheumatism, 105
Oxaluria, insomnia caused by, 72
Oxygen, absorption of, during sleep, 9
Ozone, use of, in the treatment of asthma, 101
Pacific Islanders, habits of, regarding sleep in the daytime, 40
use of massage among, 61
Pain, a cause of sleep, 19
Paraldehyde, 79, 95, 97, 108
Paregoric, 100
Perception, effect of, upon nervous tissue, 10
duration of, necessary to arouse consciousness, 23
range of, circumscribed by sleep, 12
transfer of, in telepathy and hypnotism, 217
Percussion, 61
Perspiration, secretion of, during sleep, 9
Pettenkofer, experiments of, on oxidation in the tissues, 9
experiments of, on respiration in sleep, 6
Pettenkofer and Voit, on tissue changes, 10
Pflüger, hypothesis of, regarding the cause of sleep, 21
Phosphatic diathesis, a cause of insomnia, 72
Phosphoric acid, 72
Phosphorus, 71
Phthisis, cough of, relieved with lactucarium, 88
insomnia of, relieved with paraldehyde, 80
treatment of, with opiates, 87
Physiological activity, reduction of, during sleep, 5
Physiological cause of somnambulism, 180
Planchette-writing, 228
Pleuritic pain, 99
Pneumogastric nerves, insomnia caused by affections of, 51
Pneumonia, 68, 100
Porter, effects of, 76
Potassium bromide, 88
Preyer, his theory of sleep, 20
Psychical Research, Society for, investigations by, 149, 217
Pulse, state of, during sleep, 6
Punkah, use of, to promote sleep, 44
Quetelet, observations of, on respiration during sleep, 5
Quinine and opium, use of, in fever, 104
[Pg 238]
Reasoning powers, arrest of, during sleep, 3
Recollection of the events of artificial somnambulism, 227
of the events of natural somnambulism, 188
Reflex movements during sleep, 12
Refrigeration, threefold effect of, 49
Relation between molecular movement and the generation of ideas, 24
Respiration during sleep, 5
Revelation through dreams, 160
Revery, nature of, 120
Rheumatic diathesis, a cause of insomnia, 72
Rosenthal, observations of, regarding lethargy, 33, 34
observations regarding apparent death, 35
Rush, Dr., observations of, on the revival of memory in dissolution, 165
Sailors, sleeping during a bombardment, 1
Sailor-boy, sleeping on a mast, 1
Salicylic acid, treatment of rheumatism with, 106
Saliva, secretion of, during sleep, 8
Samuel the prophet, dream of, 129
Sandwich Islands, climate of, for relief of insomnia, 114
Scarlet fever, treatment of, with baths, 74, 75
Scharling, observations of, regarding bodily temperature during sleep, 7
experiments of, on oxidation in the tissues, 9
Screaming fits of children, 112
Secretion, state of, during sleep, 8
Sedatives, nervous, 59, 73
Self-hypnotism, 219
Sensory excitement, effect of, upon the cerebral circulation, 27, 28
Sensory organs, condition of, during somnambulism, 191
Sexual organs, irritability of, 90
Shampooing, 61
Simon, P. Max, case of somnambulism related by, 182
dream related by, 142
Sleep, affected by certain winds, 45
artificial, mode of its production, 22
caused by the alternation of day and night, 17
caused by depressing emotions, 19
caused by exhaustion, 19
caused by fatigue, 19
caused by painful impressions, 19
caused by the venereal act, 19
definition of, 1
dreamless, 14
duration of, 4, 110
effects of its invasion upon the intellectual faculties, 13
effect of, upon consciousness, 13, 14
fatigue theory of, 20
favored by darkness, 18
favored by the suppression of sensation, 18
hindered by heat, 44
hindered by light, 39
hindered by smells, 42
hindered by sounds, 41
introductory stage of, 2
invasion of, 10, 117
measure of its depth by the experiments of Kohlschütter, 16
Obersteiner’s theory of, 20
Pflüger’s hypothesis regarding the cause of, 21
preceded by sleepiness, 2
Preyer’s theory of, 20
rapid induction of, in certain cases, 24
relation between the duration of, and the average length of the night, 17
stages of, 4
the cause of, 29
unequal incidence of, upon different portions of the brain, 13
Sleep-drunkenness, 180, 181
Sleepiness, precursive of sleep, 2
Sleeping dropsy, 30
Sleeplessness, causes of, 39
Smells, abolition of sleep by, 42
Smile, during sleep, 12
Smith, E., experiments of, on oxidation in the tissues, 9
Snoring, occasional interruption of sleep by, 11
Society for Psychical Research, investigations by, 149, 217
Sodium bromide, 88
Somniation, 169
Somnambulic dreams, 171, 178, 181
recollections of, 188
Somnambulic form of artificial somnambulism, 222
Somnambulic lethargy, 171, 173
contrasted with lucid lethargy, 176
Somnambulic life, 169, 204
a case of, 206
a case of, related by Azam, 208
a case of, related by Macnish, 206
Somnambulism, 166
artificial, 214
case of, related by Prof. J. Adams Allen, 185
case of, related by J. P. Frank, 195
case of, related by Macario, 192
case of, related by Mesnet, 196
case of, related by P. Max Simon, 182
causes of, 166
condition of sensory organs during, 191
dependence of, upon partial sleep of the brain, 11
likeness of, to hypnotism, 203
moral responsibility in, 203
phenomena of, 167, 210
physiological cause of, 180
relation of memory with events of, 192
[Pg 239]varieties of, according to A. Maury, 168
varieties of, according to Ball and Chambard, 169
varieties of, diagrammatically exhibited, 172
violent impulses during, 193
Somnolence, 30
Somnolentia, 180, 181
Sound, effect of, to hinder sleep, 42
effect of, to induce sleep, 42
Spasmodic croup, 110
Special sense organs, affections of, 39
Special senses, condition of, during invasion of sleep, 11
perversion of, during the hypnotic state, 223
Spinal cord, irritability of, 110
reflex energy of, during sleep, 3
Spinal irritation, 62
Spirit of chloroform, 81
Spiritual circle, manifestations in, 227
Stewart, Dugald, observation of, 43
Stimulants after parturition, 109
in fever, 105
nervous, 59
Stramonium, 70, 101
Strümpell, observations of, regarding sleep produced by suppression of sensation, 18
Strychnia, 105
Stupor produced by excessive heat or cold, 47
Subsultus tendinum, treatment of, with musk, 67
Suction, involuntary, during infantile sleep, 12
Suppression of sensation, a cause of sleep, 18
Swedish movement cure, 61
Sympathetic nerves, affections of, 39, 50
Table-rapping, method of communication in, 228
Tannate of cannabin, 68
Tartar emetic, use of, in asthma, 101
use of, in delirium tremens, 98
use of, in fever, 104
use of, with opium, 108
Taste, relation of, to insomnia, 43
Tea, effect of, upon the brain, 54
Telegraphy without a wire, through water, 147
Telepathy, investigation of, by the Society for Psychical Research, 149
Temperature, of the body, during sleep, 7
sense of, 43
Thapsia, 63
Theory of sleep, Obersteiner’s, 20
Pflüger’s, 21
Preyer’s, 20
Thirst, 2
Thompson, Sir William, his doctrine concerning a sixth sense, 43
Tickling, effect of during sleep, 12
Tobacco, anti-spasmodic effect of, 71, 99, 101
Transfer of perceptions, 217
Trousseau, observations of, on the pulse during sleep, 6
Tuberculosis of the cerebral membranes, 55
Tully’s Powder, 67
Tumors of the brain, 55
Turkish baths, 60
Turpentine, 63
Typhoid fever, insomnia during, 64
treatment of, with baths, 74
treatment of, with musk, 68
treatment of, with Tully’s Powder, 67
Typhus fever, treatment of, with musk, 68
Unconsciousness, produced by compression of the carotid arteries, 27
relation of, to modifications of the cerebral circulation, 25
Urea, elimination of, during sleep, 9
Urine, secretion of, during sleep, 9
Uterine colic, 81
Valerian, 68, 109
Valerianate of ammonia, 68
of zinc, 68
Venereal act, a cause of sleep, 19
Vierordt, observations of, on the duration of sleep, 110
Visions, character of, 119
of the ancient prophets, 161
Voit, observations of, on oxidation in the tissues, 9
on respiration during sleep, 6
Volition, cessation of, during sleep, 3
Wakefulness, 38
causes of, 39
dependence of, upon instability of cerebral protoplasm, 22
Warburton, Rev. Canon, clairvoyant dream of, 146
Weariness, a cause of sleep, 1
Wharton and Stillé, on sleep-drunkenness, 181
Whooping-cough, treatment of, with belladonna, 69
Wind, effect of, upon sleep, 45
Wine, effects of, 76
use of, in the insomnia of old age, 78
Ziemssen, von, on the use of baths, 73
Footnotes:
[1] Rosenbach, Zeitschr. f. klin. med. 1881. Brain, Vol. IV, p. 138.
[2] Alfred Maury, Le Sommeil et les Rêves, Chap. IV.
[3] Hermann’s Handbuch der Physiologie, Vol. IV, Part II, p. 98.
[4] Handbuch der Kinderkrankheiten, Vol. I, p. 346.
[5] Handbuch der Physiologie, Vol. IV, Pt. II, p. 217.
[6] Op. cit., pp. 142 and 456.
[7] Dic. Encyc. des Sci. Méd., Art. Sommeil, pp. 277.
[8] Quoted by Vierordt, Handbuch der Kinderkrankheiten, Vol. I, p. 307.
[9] Dic. Encyc. des. Méd., Ie série, t. XV, p. 75.
[10] Handbuch der Kinderkrankheiten, Vol. I, p. 383.
[11] Carpenter’s Physiology, 8th edition, p. 560.
[12] Handbuch der Physiologie, Vol. II, Pt. II, p. 297.
[13] Quincke, Archiv. f. Experim. Pathol., Vol. VII, p. 115.
[14] Carpenter’s Physiology, 8th edition, p. 526, Handbuch der Kinderkrankheiten, 2d edition, Vol. I, p. 373.
[15] Dic. Encyc. des Sci. Méd., IIIe Série, Vol. X, p. 268.
[16] Handbuch der Physiologie, Vol. V, p. 142-156.
[17] Kohlschütter, Messungen der Festigkeit des Schlafes. Dissert. Leipzig, 1862, und Zeitschrift f. rat. Med., 1863. Quoted, Hermann’s Handbuch der Physiologie, Vol. II, Pt. II, p. 295.
[18] Obersteiner, Zur Theorie des Schlafes, Zeitschr. f. Psych. XXIX. Preyer, Ueber die Ursachen des Schlafes. Vortrag. Stuttgart bei Enke. 1877, und centralbl. f. d. Med. Wiss. 1875. S. 577.
[19] Theorie des Schlafes. Arch. f. d. ges. Physiol. X, 468.
[20] Artificial Anæsthesia and Anæsthetics, pp. 15-17.
[21] Carpenter’s Physiology, 8th ed., p. 852.
[22] Sulla Circolazione del Sangue nel Cervello dell’Uomo. Abstract in Brain, Vol. IV, p. 100.
[23] Transactions of the London Epidemiological Society, Vol. I, p. 116.
[24] De la maladie du sommeil, 1869.
[25] The Medical Record, July 1, 1882, p. 23.
[26] Real. Encyc. der ges. Heilkunde, VIII, 276.
[27] Op. cit. p. 276.
[28] A Summer in Norway, by John Dean Caton, pp. 251 and 311.
[29] A. Maury, op. cit., p. 156.
[30] Among the Indians of Guiana. By Everard F. Im Thurn.
[31] Le Sommeil et les Rêves, p. 154.
[32] Nature, Vol. XXIX, pp. 438-462.
[33] Ganot’s Physics.
[34] Dic. Encyc. des Sci. Méd., Art. Climat.
[35] Comptes-rendus Acad. des Sci., 1840, t. XI, p. 823.
[36] Am. Journ. Med. Sci., April, 1877, p. 305.
[37] A remarkable illustration of this will be found related in The Lancet, July 26, 1884, p. 112.
[38] Dic. Encyc. des Sci. Méd., Art. Froid, p. 139.
[39] Medical and Surgical Electricity, 4th ed., p. 413.
[40] Nature, March, 1883.
[41] Lo Sperimentale, April, 1884.
[42] Artificial Anæsthesia and Anæsthetics, pp. 20-28. William Wood & Co., New York, 1881.
[43] Bull. gén. de Thérap., 1884, 2º Livr.
[44] Centralblatt für klin. med., 1884. Nr. 12.
[45] The National Dispensatory, 1884, p. 433.
[46] Deutsche Med. wochenschr., 1883, Nr. 49.
[47] Lo Sperimentale, April, 1884.
[48] The National Dispensatory, 1884, p. 993.
[49] Kiernan, Journ. Nerv. and Mental Diseases, Vol. X, p. 234.
[50] Psychological Medicine, Bucknill and Tuke, 4th ed., p. 731.
[51] Clinical Lectures on Mental Diseases.
[52] Ringer’s Therapeutics, 10th ed., p. 421.
[53] C. H. Jones, Functional Nervous Disorders, p. 284.
[54] Am. Jour. Med. Sci., Oct., 1881, p. 313.
[55] Handbuch der Kinderkrankheiten, Vol. I., p. 214.
[56] Op. cit., Vol. I., Pt. 2, p. 153.
[57] Herbert Spencer, First Principles, p. 486.
[58] A. Maury. Le Sommeil et les Rêves, p. 154.
[59] On Intelligence, p. 61.
[60] Wharton and Stillé’s Medical Jurisprudence, Third Edition, Vol. I, p. 482.
[61] Among the Indians of Guiana. By Everard F. Im Thurn. London: 1883, p. 344.
[62] A. Maury, Le Sommeil et les Rêves, p. 219 et seq.
[63] Obscure Diseases of the Brain and Mind. Philadelphia, 1866, pp. 394-398.
[64] Le Monde des Rêves, p. 88.
[65] Op. cit., p. 91.
[66] The Nineteenth Century, July, 1884, p. 71.
[67] Nature, October, 16, 1884, p. 596.
[68] Lebensmagnetismus oder Hypnotismus, von Dr. E. L. Fischer, pp. 71-73.
[69] The Nineteenth Century, July, 1884, p. 89.
[70] Visions: A Study of False Sight, p. 39.
[71] Inquiries concerning the Intellectual Powers, tenth edition, p. 283.
[72] Medical Inquiries and Observations upon Diseases of the Mind, p. 277.
[73] Loc. cit.
[74] Le Sommeil et les Rêves, p. 248.
[75] Dic. Encyc. des Sci. Méd., Article Somnambulisme Naturel.
[76] The Lancet, Dec. 22, 1883, p. 1,078, and Jan. 5, 1884, p 5.
[77] Brain, Jan., 1884, p. 454.
[78] Medical Jurisprudence, 3d ed., Vol. I, pp. 464-471.
[79] Le Monde des Rêves, p. 257.
[80] Chicago Medical Journal, 1869, p. 650.
[81] Maury, Le Sommeil et les Rêves, p. 234.
[82] Pathologie interne.
[83] L’ Union Médicale, July 21st and 23d, 1874.
[84] Chicago Journ. of Nervous and Mental Diseases, Vol. II, p. 48.
[85] Loc. cit.
[86] Philosophy of Sleep, p. 167.
[87] Revue Scientifique, May 20, Sept. 16, 1876; Dec. 22, 1877; March 8, 1879.
[88] Vol. III, p. 584.
[89] Chapters on Mental Physiology, p. 160.
[90] Le Sommeil et les Rêves, p. 226.
[91] Lancet, July 29, 1882, p. 164.
[92] Transactions of the Society, etc., Vols. I, II, III.
[93] Le Progrès Médical, Feb. 18, 1882, p. 124.
[94] Le Progrès Médical, March 25, 1882, p. 223.
[95] Le Progrès Médical, Jan. 14, 1882, p. 25.
[96] Brain, Vol. III, p. 394.
[97] Op. cit., p. 18.
[98] Le Sommeil et les Rêves, p. 361.
[99] Op. cit.
[100] Berlin. Klin. Wochenschr, January, 1884.
[101] Der Hypnotismus, Jena, 1884.
[102] Brain, July, 1884, p. 278.