Transcriber’s Note:
The cover image was created by the transcriber and is placed in the public domain.
THE
SEXUAL LIFE OF WOMAN
IN ITS
PHYSIOLOGICAL, PATHOLOGICAL AND HYGIENIC ASPECTS
BY
E. HEINRICH KISCH, M. D.
Professor of the German Medical Faculty of the University of Prague; Physician to the Hospital and Spa of Marienbad; Member of the Board of Health, Etc., Etc.
ONLY AUTHORIZED TRANSLATION INTO THE ENGLISH LANGUAGE FROM THE GERMAN BY
M. EDEN PAUL, M. D.
WITH 97 ILLUSTRATIONS IN THE TEXT
NEW YORK
REBMAN COMPANY
1123 BROADWAY
Copyright, 1910, by
REBMAN CO., NEW YORK
All Rights Reserved
Printed in America
TO MY ONLY SON
FRANZ KISCH, M. D.
AS A TOKEN OF PATERNAL AFFECTION
I DEDICATE THIS BOOK
v
PREFACE.
The sexual life of woman—the appearance of the first indications
of sexual activity, the development of that activity and its
culmination in sexual maturity, the decline of that activity and its
ultimate extinction in sexual death—the entire process of the most
perfect work of natural creation—has throughout all ages kindled
the inspiration of poets, aroused the enthusiasm of artists, and supplied
thinkers with inexhaustible material for reflection.
In the following pages, this sexual life of woman will be considered
both in relation to the female genital organs, and in relation
to the feminine organism as a whole; in relation both to the physical
and to the mental development of the individual; and in relation
alike to the state of health and to the processes of disease. Thus
from the standpoint of clinical investigation and of practical experience,
the book will be a contribution towards the solution of the
sexual problem, nowadays recognized as one of supreme importance.
It is thirty years since I published a work on the histological
changes that occur in the ovaries during the climacteric period
(Archiv. für Gynecologie, Vol. xii, Section 3); and ever since that
time, the influence exerted upon the general health of women by the
physiological and pathological processes occurring in their reproductive
organs, has been to me a favourite subject for observation
and experiment. The result of these studies is incorporated in my
monographs, “The Climacteric Period in Women” (Erlangen,
1874), “Sterility in Women” (2nd Ed., Vienna, 1895), “The
Uterus and the Heart” (Leipzig, 1898), and in various contributions
to medical periodicals. I now have a welcome opportunity of drawing
a general picture of sexual activity in women, and of illuminating
this picture both by the light of my own experience and by numerous
references to the works of other authors. In passing, I have devoted
considerable attention to questions of education and personal
hygiene, both of which are greatly influenced by the processes
of the sexual life. Thus, I hope, the work will be rendered more
interesting to the physician, and the general picture it is intended to
convey will be more fully characterized by contemporary actuality.
Natural divisions of the subject are, I consider, furnished by the
three great landmarks of the sexual life of woman: the onset of
menstruation—the menarche: the culmination of sexual activity—the
vimenacme; and the cessation of menstruation—the menopause.
These several sexual epochs are differentiated by characteristic
anatomical states of the reproductive organs, by the external configuration
of the feminine body, by functional effects throughout
the entire organism, and, finally, by pathological disturbances of
the normal vital processes.
Thus in separate chapters a description is given of sexual processes,
a detailed exposition of which will be vainly sought in the
textbooks of gynecology, yet which are none the less of far-reaching
importance in relation to the physical, mental, and social well-being
of women, and in relation also to the development of human society;
such topics are, the sexual impulse, copulation, fertility, sterility, the
employment of means for the prevention of conception, the determination
of sex, sexual hygiene. To the topics of pregnancy, parturition,
lying-in, and lactation, since these are adequately discussed in
works on midwifery, but little space has here been allotted.
It is my earnest hope that physicians and biologists may derive
benefit from the book equal in amount to the pleasure I have gained
in the work of writing it.
vii
TABLE OF CONTENTS.
|
|
|
|
PAGE |
| |
The Sexual Life of Woman—Introduction |
1 |
| |
| I. |
The Sexual Epoch of the Menarche |
37 |
| |
| |
|
First Appearance of Menstruation |
45 |
| |
| |
|
Anatomical Changes in the Female Genital Organs at the Period of the Menarche |
50 |
| |
| |
|
Menarche Praecox et Tardiva |
78 |
| |
|
|
Precocious and Retarded Menstrual Activity |
78 |
| |
| |
|
Pathology of the Menarche |
82 |
| |
|
|
Anomalies of Menstruation |
83 |
| |
|
|
Inflammatory Processes |
87 |
| |
|
|
Disorders of Haematopoiesis |
89 |
| |
|
|
Cardiac Disorders |
94 |
| |
|
|
Diseases of the Nervous System |
99 |
| |
|
|
Masturbation |
104 |
| |
|
|
Disorders of Digestion |
107 |
| |
|
|
Diseases of the Respiratory Organs |
107 |
| |
|
|
Diseases of the Organs of the Senses |
108 |
| |
|
|
Hygiene during the Menarche |
111 |
| |
|
|
Menstruation |
128 |
| |
|
|
Pathology of Menstruation |
143 |
| |
|
|
Amenorrhœa, Menorrhagia, and Dysmenorrhœa |
160 |
| |
|
|
Vicarious Menstruation |
164 |
| |
| |
|
The Sexual Impulse |
166 |
| |
| |
|
Nymphomania, Anæsthesia and Psychopathia Sexualis |
184 |
| |
| II. |
The Sexual Epoch of the Menacme |
200 |
| |
| |
|
Anatomical Changes in the Female Genital Organs in the Period of the Menacme |
209 |
| |
| |
|
Pathology of the Menacme |
218 |
| |
|
|
Dyspepsia Uterina |
227 |
| |
|
|
Cardiopathia Uterina |
235 |
| |
|
|
Nervous Diseases Secondary to Diseases of the Genital Organs |
243 |
| |
| |
|
Competence for Marriage of Women suffering from Disease |
250 |
| |
| |
|
Hygiene during the Menacme |
261 |
| |
| |
|
Copulation and Conception |
284 |
| |
|
|
Copulation |
284 |
| |
|
|
Conception |
304 |
| |
|
|
Pathology of Copulation |
323 |
| |
|
|
Vaginismus |
337 |
| |
|
|
Cardiac Troubles Due to Sexual Intercourse |
344 |
| |
|
|
Dyspareunia |
347 |
| |
| |
|
Fertility in Women |
363 |
| |
|
|
The Restriction of Fertility and the Use of Means for the Prevention of Pregnancy |
388 |
| |
| |
|
The Determination of Sex |
420 |
| |
|
|
I. Statistical Investigations |
422 |
| |
|
|
II. Anatomical Investigations |
446 |
| |
|
|
III. Experimental Investigations |
452 |
| |
| |
|
Sterility in Women |
462 |
| |
|
|
Incapacity for Ovulation |
470 |
| |
|
|
Interference with Conjugation, Conditions Preventing Access of the Spermatozoa to the Ovum |
487 |
| |
|
|
Diseases of the Ovaries and the Fallopian Tubes |
489 |
| |
|
|
Diseases of the Uterus |
494 |
| |
|
|
Pathological Changes in the Cervix Uteri |
501 |
| viii |
|
|
Displacements of the Uterus |
515 |
| |
|
|
Myoma of the Uterus |
523 |
| |
|
|
Diseases of the Vagina and the Vulva |
526 |
| |
|
|
Secretions of the Genital Organs |
528 |
| |
|
|
A. Absolute |
540 |
| |
|
|
B. Relative Sterility |
540 |
| |
|
|
Sexual Sensibility in Women |
542 |
| |
|
|
Incapacity for Incubation of the Ovum |
549 |
| |
|
|
Only-Child-Sterility |
561 |
| |
|
|
Operative Sterility |
563 |
| |
|
|
Table Showing the Causes of Sterility in Women |
569 |
| |
| III. |
The Sexual Epoch of the Menopause |
571 |
| |
| |
|
The Menopause |
571 |
| |
| |
|
Changes in the Female Reproductive Organs at the Menopause |
583 |
| |
| |
|
The Time of the Menopause |
593 |
| |
| |
|
The Age at which the Menopause occurs |
593 |
| |
|
|
1. Race |
594 |
| |
|
|
2. The Age at which the Menarche Occurred |
595 |
| |
|
|
3. The Woman’s Sexual Activity |
597 |
| |
|
|
4. The Social Circumstances of the Woman’s Life |
599 |
| |
|
|
5. General Constitutional and Pathological Conditions |
599 |
| |
|
|
6. Premature, Delayed, and Sudden Onset of the Menopause |
600 |
| |
| |
|
Pathology of the Menopause |
608 |
| |
|
|
Diseases of the Genital Organs |
608 |
| |
|
|
Diseases of the Organs of Circulation |
620 |
| |
|
|
Diseases of the Digestive Organs |
630 |
| |
|
|
Diseases of the Skin |
632 |
| |
|
|
Disorders of Metabolism |
635 |
| |
|
|
Diseases of the Nervous System |
637 |
| |
|
|
Climacteric Psychoses |
643 |
| |
| |
|
Hygiene during the Menopause |
653 |
ix
LIST OF ILLUSTRATIONS (Kisch).
| Fig. |
|
Page |
| 1. |
Curve of the sexual life of woman from the tenth to the sixtieth year of life |
4 |
| 2. |
Portion of the pelvic viscera in the female, etc. |
9 |
| 3. |
The distribution of the pudic nerve in the female perineal and pubic regions |
11 |
| 4. |
The distribution of the lateral sacral arteries, etc. |
14 |
| 5. |
Curve of menstrual cycle |
19 |
| 6. |
Curve of rhythmical variations |
20 |
| 7. |
Curve of beauty of woman. |
24 |
| 8. |
Internal genital organs of new-born female infant |
51 |
| 9. |
Reproductive organs of a new-born female infant |
52 |
| 10. |
Internal genital organs of a girl aged eight years |
52 |
| 11. |
Reproductive organs of a girl aged ten years |
53 |
| 12. |
Female external genital organs of a virgin |
54 |
| 13. |
The external genital organs of a virgin |
55 |
| 14. |
Sagittal section of the female pelvis |
56 |
| 15. |
Primitive follicles |
58 |
| 16. |
Ripening follicles |
61 |
| 17. |
Graafian follicles |
62 |
| 18. |
Annular Hymen |
64 |
| 19. |
Annular Hymen |
64 |
| 20. |
Semilunar Hymen |
65 |
| 21. |
Annular Hymen with Congenital Symmetrical Indentations |
65 |
| 22. |
Fimbriate Hymen |
65 |
| 23. |
Deflorated Fimbriate Hymen |
65 |
| 24. |
Septate Annular Hymen |
67 |
| 25. |
Septate Semilunar Hymen |
67 |
| 26. |
Extremely tough Annular Hymen with an obliquely disposed Septum |
67 |
| 27. |
Septate Hymen with Apertures of unequal Size |
67 |
| 28. |
Septate Hymen with Apertures of unequal Size |
68 |
| 29. |
Hymen with rudimentary Septum |
68 |
| 30. |
Hymen with posterior rudimentary Septum |
68 |
| 31. |
Labiate Hymen with posterior rudimentary Septum |
68 |
| 32. |
Hymen with anterior rudimentary Septum |
69 |
| 33. |
Hymen with anterior rudimentary Septum projecting in a opiniform Manner |
69 |
| 34. |
Hymen with anterior and posterior rudimentary Septa |
69 |
| 35. |
Hymen with filiform Process projecting from the anterior Margin |
69 |
| 36. |
Hymen in which there are two symmetrically disposed thinned Areas. The left of these is perforated |
69 |
| 37. |
Very unusual form of Hymen |
70 |
| 38. |
Semilunar Hymen with cicatrized Lacerations in its Border |
70 |
| 39. |
Deflorated Semilunar Hymen with laterally disposed symmetrical Lacerations |
70 |
| 40. |
Deflorated Annular Hymen with several cicatrized Lacerations |
70 |
| 41. |
A. Septate Hymen in which defloration has been effected through one of the Apertures. U. Urethra. Cl. Clitoris. H. Cicatrized Margin. C. Septum. B. Lateral view of Septum |
70 |
| 42. |
Deflorated Septate Hymen |
71 |
| x43. |
Hymen with larger anterior and smaller posterior Apertures |
71 |
| 44. |
Carunculæ Myrtiformes in a Primipara |
71 |
| 45. |
Vaginal Inlet of a Multipara, without Carunculæ Myrtiformes. Slight Prolapse of Anterior and Posterior Vaginal Walls |
71 |
| 46. |
The breast of a virgin aged eighteen years |
73 |
| 47. |
Horizontal section through the female breast |
75 |
| 48. |
The female pudendum, or vulva, with the labia majora |
204 |
| 49. |
Vestibule of the vagina, with the labia minora or nymphæ, etc |
205 |
| 50. |
The uterus, the left Fallopian tube and the left ovary, etc |
207 |
| 51. |
Female internal genital organs in the fully developed state |
208 |
| 52. |
Sagittal Section through the Cervix Uteri of a Woman twenty-six years of age. Dendriform branched glands |
217 |
| 53. |
Cervix of a Woman seventy-two years of age, with glands that have undergone cystic degeneration |
217 |
| 54. |
Sagittal Section through the Cervix Uteri of a Woman sixty-five years of age. The glands have undergone cystic degeneration |
217 |
| 55. |
First Stage. A. Entrance of a Spermatozoon into the Ovum of Ascaris Megalocephala. B. After preparations by M. Nussbaum. (Half of the ova only are depicted) |
306 |
| 56. |
Ovum of Asterakanthion ten minutes after Fertilization |
306 |
| 57. |
Fusion of Male Pro-nucleus and Female Pro-nucleus to form the Segmentation Nucleus of the Fertilized Ovum |
306 |
| 58. |
Passage of Spermatozoon through the Zona Pellucida of the Ovum of Asterakanthion |
307 |
| 59. |
Ovum of Scorpæna Scrofa Thirty-five Minutes after Fertilization |
307 |
| 60. |
Male Pro-nucleus and Female Pro-nucleus in Fertilized Ovum of Frog, prior to the Formation of the Segmentation Nucleus |
307 |
| 61. |
a. b. c. Prostatic calculi from normal semen, d. Spermatozoa. e. Large and small cells, some containing granules, as morphological elements of semen. f. Spermatozoon distorted by imbibition of water. g. Crystals (after Bizzozero) |
311 |
| 62. |
Normal Semen |
311 |
| 63. |
Semen consisting chiefly of sperm-crystals, cylindrical epithelium, and small granules exhibiting molecular movement—but containing no spermatozoa |
315 |
| 64. |
Oligozoöspermia. a. Living Spermatozoa, b. Dead Spermatozoa, c. Pus Corpuscles, d. Erythrocyte, e. Seminal granules |
317 |
| 65. |
Septate Hymen, the septum having a tendinous consistency |
324 |
| 66. |
|
326 |
| 67. |
Lipoma of the Right labium majus, including the Vaginal Inlet |
328 |
| 68. |
“Hottentot Apron” in an adult Woman, hanging down between the thighs (after Zweifel) |
329 |
| 69. |
Elephantiasis of the Labia Majora |
330 |
| 70. |
Congenital Atrophy of the Uterus (after Virchow), oi, Ostium internum; oe, Ostium externum |
500 |
| 71. |
|
500 |
| 72. |
Normal Shape of the Portio Vaginalis |
503 |
| 73. |
Conoidal Shape of the Portio Vaginalis |
503 |
| 74. |
“Apron-Shaped” Vaginal Portion, a. Greatly elongated anterior lip; b. Shorter posterior lip of the cervix |
504 |
| 75. |
“Beak-Shaped” Vaginal Portion. Posterior aspect |
504 |
| 76. |
Simple Hypertrophy of the Portio Vaginalis, which projected from the Vulva |
506 |
| 77. |
Elongated Cervix, bent upwards |
506 |
| 78. |
Cervical Polypus, originating from an Ovulum Nabothi |
510 |
| 79. |
Ectropium in a Case of Bilateral Laceration of the Cervix (after A. Martin) |
514 |
| 80. |
Anteflexio Uteri (after A. Martin) |
518 |
| 81. |
Retroflexio Uteri (after A. Martin) |
520 |
| xi82. |
Mucus from the Cervical Canal, taken one hour after sexual intercourse, from a woman suffering from chronic endometritis. Among the epithelial cells, pus cells, and finely granular masses, we see a few motionless, dead spermatozoa |
531 |
| 83. |
Uterine Mucous Membrane in Endometritis (after A. Martin) |
554 |
| 84. |
Sagittal section through the ovary of a girl aged sixteen |
583 |
| 85. |
Sagittal section through the ovary of a woman aged seventy-two years |
584 |
| 86. |
Diagrammatic Representation of the Graafian Follicle |
585 |
| 87. |
Ovary of a Girl aged nineteen years (Normal Size) |
585 |
| 88. |
Ovary of a Woman seventy-two years of age (Normal Size) |
585 |
| 89. |
|
586 |
| 90. |
|
587 |
| 91. |
|
588 |
| 92. |
Sagittal Section through the Cervix of a Woman twenty-six years of age. Dendriform branched glands |
588 |
| 93. |
Sagittal Section through the Cervix of a Woman sixty-five years of age. Glands which have undergone Cystic Degeneration |
589 |
| 94. |
Cervix of a Woman seventy years of age. The Cervical Glands have undergone Cystic Degeneration |
589 |
| 95. |
Ovula Nabothi in the Portio Vaginalis |
590 |
| 96. |
Vesicle (Ovula Nabothi) from the Uterine Mucous Membrane |
591 |
| 97. |
Mucous Glands undergoing Cystic Degeneration |
592 |
1
THE SEXUAL LIFE OF WOMAN.
By the sexual life of woman we understand the reciprocal action
between the physiological functions and pathological states of the
female genital organs on the one hand and the entire female organism
in its physical and mental relations on the other; and the object
of this book is to give a complete account of the influence exercised
by the reproductive organs, during the time of their development,
their maturity, and their involution, on the life history of woman.
From the earliest days of the medical art this sexual life of
woman has aroused in the leaders of medical thought the highest
interest, and for this reason great attention has been directed, not
only to the anatomy of the genital organs and to the diseases of
the reproductive system, but also to the individual manifestations of
sexual activity and to the influence exercised by these on the female
organism as a whole.
Several works by Hippocrates are extant on this subject, among
which may be mentioned: περι Γυναικειης Φυσεος,[1] a treatise on the
physiology and pathology of woman; περι Αφορων,[2] which discusses
sterility in women; περι παρθενιων,[3] a treatise on the pathological
states of virgins. These writings of Hippocrates contain some
very remarkable observations on the influence exercised by disorders
of the reproductive organs on the general health of women.
Aristotle wrote at some length on the functions of the female
genital organs. In the writings of Aretæus and Galen on the diseases
of women we find striking observations, as for instance, in
Galen’s De Locis Affectis,[4] which contains a “Statement of the
Similarity and Dissimilarity of Man and Woman.” Another notable
work is that of Albertus Magnus, entitled De Secretis Mulierum.[5]
The numerous works on the diseases of women published in the
sixteenth century consisted for the most part of a repetition of the
observations of ancient writers. The gynecological treatises of the
2eighteenth century, however, bore witness to an increased knowledge
of the anatomy of the female reproductive organs, and were
illumined by Haller’s researches on the functions of these organs.
The subject with which we are especially concerned is discussed
in a work by Boireau-Laffecteur, Essai sur les Maladies Physiques
et Morales des femmes,[6] Paris, 1793; and also in Marie-Clement’s
Considerations Physiologiques sur les Diverses Epoques de la Vie
des Femmes,[7] Paris, 1803. the same connection we must mention
von Humboldt’s treatise, Ueber den Geschlechtsunterschied und
dessen Einfluss auf die organische Natur.[8] The first comprehensive
work in which an exhaustive inquiry was made into the functional
disorders of the female genital organs and the relation of these
disorders to the female organism as a whole and to the physical
and mental peculiarities of woman was Busch’s: Das Geschlechtsleben
des Weibes,[9] Leipzig, 1839.
In the second half of the nineteenth century a very large number
of monographs were published, investigating and describing the
reflex disturbances produced alike in the individual organs and in
the nervous system as a whole by changes in the uterus and its
annexa. Many of these works will be mentioned more particularly
in the course of this treatise.
The sexual life, based upon the purpose, so important to every
creature, of the propagation of the species, possesses in the female
sex a vital significance enormously greater than sexual activity
possesses in the male. From the very beginning of sexuality, when
the idea of a bisexual differentiation dawns for the first time in the
brain of the little girl, down to the sexual death of the withered
matron, who laments the loss of her sexual potency, physical and
mental activity, work and thought, function and sensation, arise for
the most part, wittingly or unwittingly, from that germinal energy
which is the manifestation of the unalterable law that the existing
organism endeavors to reproduce its kind.
Every phase of the sexual life of woman, from the threshold of
puberty to the extinction of sexual activity, the first appearance of
menstruation, the complete development of the sexual organs, the
act of copulation, conception, pregnancy, parturition, and the puerperium,
finally the involutionary process which accompanies the
cessation of menstruation at the climacteric period—every one of
3these sexual phases entails consecutive physiological processes and
pathological changes alike in the individual organs and in the nutritive
condition of the entire organism, in the functions of the
cardio-vascular apparatus, of the brain and the nerves, of the skin
and the sense-organs, in the processes of digestion and general metabolism.
Herein we see a striking illustration of the old saying of
von Helmont, propter solum uterum mulier est quod est;[10] also
of the similar aphorism of Hippocrates, uterus omnium causa morborum
qui mulieres infestant;[11] a conception summed up by Goethe
in the words of Mephistopheles:
“Es ist ihr ewig Weh und Ach
So tausendfach
Aus einem Punkte zu kurieren.”
Just as in a tree the process of growth is made manifest to the
superficial observer by the pleasure he feels at the sight of the buds
and blossoms, by the refreshment he obtains from the fruit, and by
the sadness which the withering of the leaves causes him, so in the
sexual life of woman there are landmarks which no one can possibly
overlook, by means of which three great epochs are distinguished.
These are: puberty (the menarche), recognized by the
first appearance of menstruation and the awakening of the sexual
impulse; sexual maturity (the menacme), in the fully developed
woman, characterized by the functions of copulation and reproduction;
and sexual involution (the menopause), in which we see the
gradual decline and ultimate extinction of sexual power and all its
manifestations. In all these three epochs the sexual life of woman
not only affects the hidden domain of the genital organs, but controls
also all the vegetative, physical, and mental processes of the
body, and is clearly and incontestably apparent in all vital manifestations.
What Madame de Staël said of love is indeed true of the
entire sexual life of woman: l’amour n’est qu’unc épisode de la vie
de l’homme; c’est l’histoire tout entière de la femme.[12].
The sexual life of woman is coextensive with the peculiar vital
activity of the female sex, for it endures from the moment when
4individuality first begins to develop out of the indifferent stage of
childhood until the decline into the dead-level of senility.
To illustrate this fact, I have drawn up a curve of the sexual life
of woman, making use of the statistical data available in central
Europe regarding the age at which menstruation first appears, the
age at which maidens marry, the age at which the largest number
of women give birth to a child, and the age at which menstruation
ceases; and reducing the figures to averages. * denotes the fifteenth
year of life, as the average age at the menarche; ** denotes
the twenty-second year of life as the average age at marriage;
*** denotes the thirty-second year of life, in which woman exhibits
her maximum fecundity; **** denotes the forty-sixth year of life
as the average age at the menopause. (Fig. 1.)
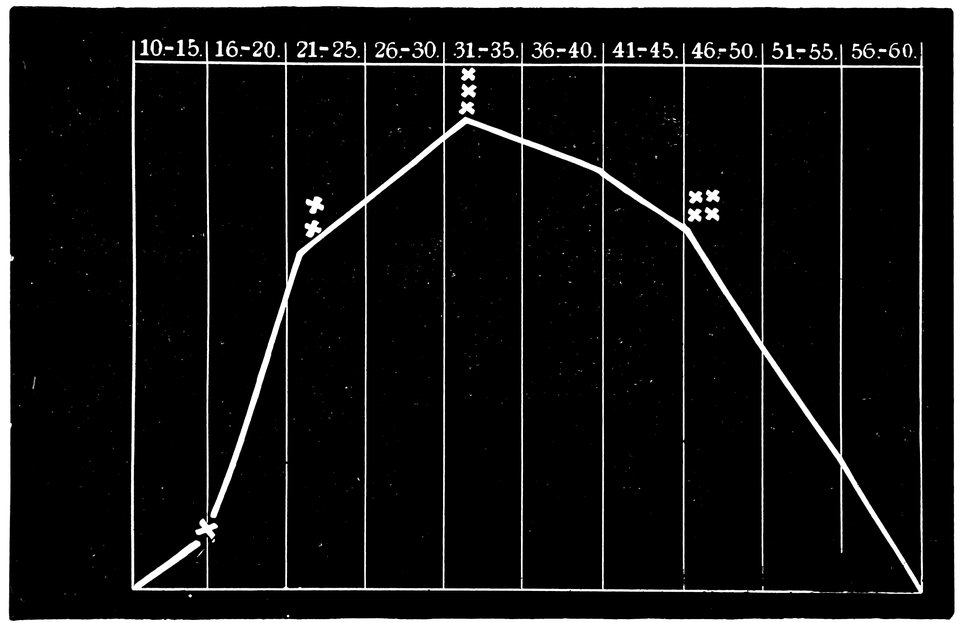
Fig. 1.—Curve of the sexual life of woman from the tenth to the sixtieth year of life.
Not in this respect alone, however, is the sexual life of woman
of paramount importance; it is, in addition, the mainspring of
the well-being and progress of the family, of the nation, of the
entire human race. In the evolution of man from the primitive
state in which he existed merely for the performance of vegetative
functions up to the highest stage of contemporary culture, in the
history of all races and of all times, the sexual life has been a most
5potent determining factor. With that life, religion, philosophy,
ethics, natural science, and hygiene, have been most intimately related;
for that life, they have furnished precepts and laws. The
history of the sexual life is identical with the history of human
culture.
In a primitive condition of society, among people living in a state
of nature and among the lower races of mankind, the sexual life of
woman possesses no great general interest, the female being merely
a chattel; the ownership of this chattel, moreover, being often
temporary and transient. The investigations of anthropologists
have shown that among primitive people this form of property is
neither highly esteemed nor carefully safeguarded. In such societies
no restraint is imposed on the sexual impulse, which is gratified
without shame and without formality. No hindrance is offered
to the mutual intercourse of the two sexes. Chastity in the females
is not prized by the males, nor do the latter compete for the favors
of the former. Procreation is no more than a gregarious impulse
of the masses among whom the common ownership of all booty is
a matter of tribal custom. The woman has no disposing power
over that which every one desires and which every one has the right
to demand. Very gradually, however, a change takes place in
this respect, so that in every period of social life since the very
earliest, the modesty of young girls, the high valuation put upon
the preservation of virginity, the ethical approbation of chastity in
the wife, respect for the duties and rights of the mother, the reverence
felt for the matron—all these, throughout the sexual life of
woman, have had a civilizing, ennobling, and elevating effect.
Thus, as family life has become developed, and as love and
marriage have been more highly esteemed, woman has become
the much-prized embodiment of all that is beautiful and good,
of all that is summed up in the idea of the “housewife,” and
her sexual life has been more completely, more ideally admired.
The danger is not remote, however, that the leveling tendencies of
the present day, and an inclination to despise the sexual life of
woman, far from resulting in a further elevation of the social
status of womanhood, will result rather in its abasement.
The Bible, as we may expect from the patriarchal relationships of
the women of that time, bears witness to the worth of woman, and,
whilst esteeming child-bearing, refers to yet higher duties. Precise
religious and social precepts are furnished for all the phases of
sexual life.
6In classical antiquity, also, we see that woman rose to some extent
above the low position she had previously occupied in the family
circle and in society at large. Both among the Greeks and among the
Romans, there was open to women a more intimate place in social life
and a more influential rôle in the life of the family, than would have
been their portion regarded merely in relation to their child-bearing
activity. Amongst the Germans in the very earliest times, chastity
gave rise to purer and more moral sexual relations; whereas among
the Slavonic peoples the conception of woman as the childbearer
continued to dominate these relations.
In consequence of the diffusion of Christianity, woman became
man’s companion and equal, and her life, the sexual life included,
acquired a deeper significance, owing to the stress which that religion
laid on chastity as a virtue, and as a result of the educational
influence of woman in the family circle.
With the progress of civilization the sexual life of woman comes
to exhibit its activities only within the bounds of morality and law,
which in human society have replaced the crude rule of nature, and
have supplied regulations adapted to the changing phases of sexual
vital manifestations. The wise adaptation of these regulations requires,
however, a full understanding of the mental and physical
processes, an exact recognition of the bodily states and intellectual
sensibilities, of woman regarded as a sexual being.
Modern culture and the social organization of the present day,
in association with the resulting sexual neuropathy of women, have
exercised on their sexual life an influence as powerful as it is unfavorable,
manifesting itself in the overpowering frequency of the
diseases of women. In one of the most thoughtful books ever written
on the subject of woman, Michelet’s L’Amour,[13] the author remarks
that every century is characterized by the prevalence of certain
diseases: thus, in the thirteenth century, leprosy was the dominant
disease; the fourteenth century was devastated by bubonic
plague, then known as the black death; the sixteenth century witnessed
the appearance of syphilis; finally, as regards the nineteenth
century, “se siècle sera nommé celui des maladies de la matrice”.[14]
It is certain that the education and mode of life of the modern
woman belonging to the so-called upper classes are, as far as sexual
matters are concerned, in direct opposition to those that are agreeable
to nature and those that the laws of health demand.
7Even before sexual development begins, before the physical ripening
of the reproductive organs to functional activity, the imagination
of young girls is often prematurely occupied with sexual ideas in
consequence of unsuitable literature, owing to visits to theatres and
exhibitions, or on account of social intercourse with young men
who are not overscrupulous in the selection of topics for conversation.
From the time of puberty up to the time of marriage the
growing woman is under the influence of the now awakened sexual
impulse, which experiences ever-renewed stimulation. A sedentary
mode of life, unsuitable nutriment, and the early enjoyment of alcoholic
beverages, exhibit their inevitable result in the frequency with
which, in this epoch of the sexual life, chlorotic blood-changes, neurasthenic
conditions, and diverse symptoms of irritation of the genital
organs, make their appearance. Thus, when marriage, so often unduly
postponed in consequence of the condition of modern society,
does at length take place, it is apt to find the woman not only fully
enlightened as regards sexual matters, but often in a state of
nervous weakness from sexual stimulation, one of the type whose
characteristics have been happily summed up by the French writer
Prévost in the expression demi-vierge.[15] The conjunction of this
state of affairs in the bride with the frequent partial impotence of
the bridegroom, who has already dissipated the greater part of his
virile power before entering upon marriage, leads often to the
appearance of vaginismus and other sexual neuroses in young married
women. Even more disastrous in its consequences as regards
the future sexual life of the wife is the ever-increasing frequency
of gonorrhœal infection in the first days of marital intercourse, with
all the evil results of that infection. On the other hand, an ever-larger
proportion of girls belonging to the “middle and upper
classes,” abstaining alike from the good and the evil results of marriage,
falls under the yoke of sexual impulses denied satisfaction or
gratified by abnormal means, and suffers in consequence both physically
and mentally. Further sources of injury arising from the
conditions of modern social life are to be found in the neglect by
women of the well-to-do classes of the duty of suckling their children,
and in the ever-increasing frequency with which the women
of these classes, after giving birth to one or two children, resort to
the use of measures for the prevention of pregnancy, which result in
serious consequences as regards both the nervous system and the
genital organs of the women concerned. Thus there comes an
accelerated ebb in the sexual life, leading to a premature appearance
8of the general phenomena of senility, with a cessation of the menstrual
flow. The modern wife, who claims the right to lead the life
that best pleases her, will be more rapidly overtaken by sexual death.
For the elucidation of the manifold reflex and other processes
which are dependent upon or accompany the sexual phases of
woman, we must in the first place consider the anatomical changes
and physiological functions of the female reproductive organs characteristic
of the several periods of sexual life which have already
been distinguished. We must not fail also to take into consideration
the mental states which accompany and characterize these respective
phases.
The anatomical changes which occur in the female genital organs
during these different phases of sexual life give rise to a number of
manifold local stimuli, increasing and decreasing, varying greatly
in intensity and area of distribution, upon which depend the reflex
effects and remote manifestations in the sphere of the nervous and
circulatory systems.
We must first consider the changes in the ovaries, which play an
etiologically important part. At the onset of puberty, the follicular
masses of the ovary exhibit a more active growth, the follicles increase
in size, with their contained ova they approach the surface,
and finally, by the bursting of the follicles, the ova are extruded.
Then, in the life-phase in which conception occurs, and under the
influence of the hyperæmia of all the pelvic viscera that accompanies
this process, a notable development of the corpus luteum takes
place, this latter body reaching its maximum size in the eleventh
week of pregnancy, subsequently undergoing involution and leading
to the formation of a considerable scar. Finally, in the critical
period of life in which the menstrual flow ceases, a continually increasing
growth and new formation of connective tissue-stroma
takes place in the ovaries at the expense of their cellular constituents,
and a regressive metamorphosis of the graafian follicles occurs.
In association with these sexual processes there ensues a series
of striking changes in the shape and consistency of the ovaries, affecting
both the surface and the parenchyma of these organs, and
capable of stimulating the nervous ramifications in their tissue.
In this connection it is worthy of note that the branches supplying
the ovaries from the spermatic plexuses of the sympathetic contain
a considerable proportion of sensory fibres.
Quite as significant, moreover, as the changes in the ovaries, are
those which, in the course of the sexual life, the uterus undergoes,
in shape and size, in its muscular substance and mucous lining, and
in its vascular and nervous supply.
9
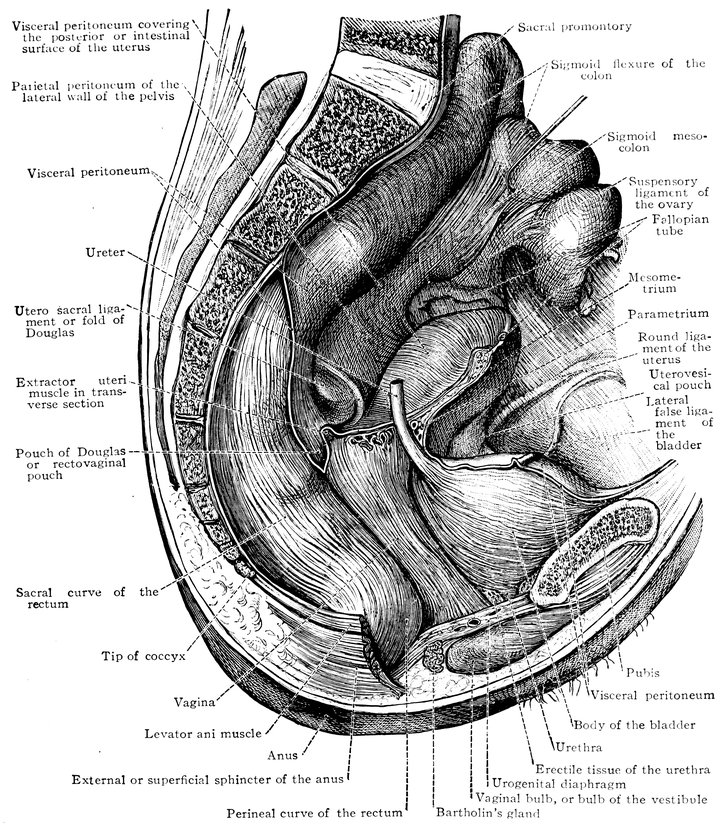
Fig. 2.—Portion of the pelvic viscera in the female, and their relation to the muscles of the pelvic outlet (or perineal muscles), shown in the left half of the pelvis, seen from the right side.—The parametrium. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
10At the time of puberty the infantile uterus undergoes changes
affecting both its external form and the shape of its interior cavity.
The body of the uterus enlarges to the size characteristic of sexual
maturity, and its mucous membrane becomes the seat of periodic
changes. This waxing and waning growth and transformation of
the uterine mucous membrane continues throughout the period of
menstrual activity, the most superficial layers of the membrane
being shed during menstruation, a process followed by regeneration,
which is itself succeeded by the premenstrual thickening. When
conception occurs, still more extensive changes ensue, the fertilized
ovum becoming imbedded in the uterine mucous membrane, and the
pregnant uterus, in shape and structure and in the respective relations
of the body and neck of the organ, in the increasing distension
of its veins and the increasing size of its nerves, becoming
adapted to the important functions it has now to fulfil. When these
have been fulfilled, and, parturition having taken place, the uterus
is empty once more, the organ again adapts itself to altered circumstances
by the process of involution. Later, in the climacteric
period, a slow regressive process occurs, the outward manifestation
of which is the cessation of the menstrual flow, characterized anatomically
by atrophy of the muscular tissue of the uterus and of
its vascular apparatus, by the dessication of its mucous membrane,
by obliteration of the lumen of the uterine cavity, and ultimately by
senile degeneration and atrophy of the now entirely functionless
organ, so that it becomes an insignificant, cicatrized, solid body.
Next to the ovaries and the uterus, it is the pelvic fascia which
in its entire architectonic structure as well as in its individual parts
undergoes the most notable changes in consequence of the processes
of generation.
A short account of the nerves and blood vessels of the female
genital organs appears indispensable, to facilitate the comprehension
of the manner in which sexual processes are influenced by the
nervous system, and to demonstrate the intimate connection between
the blood-supply of the genital apparatus and the general
circulation.
The complex nervous network of the female sexual organs is
supplied by spinal as well as by sympathetic fibres, the fibres from
the two systems anastomosing in a very intimate manner.
11
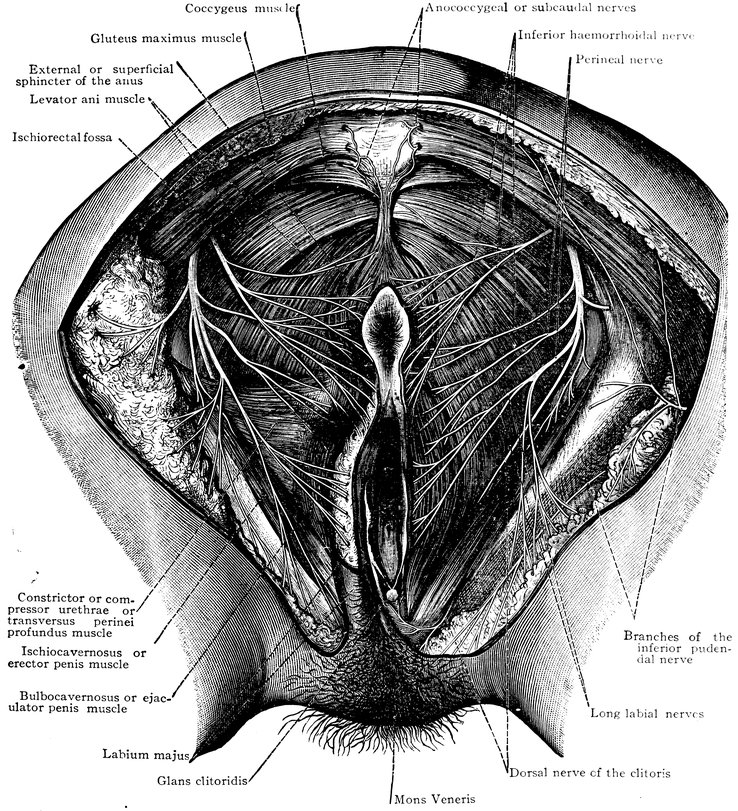
Fig. 3.—The distribution of the pudic nerve, n. pudendus, in the female perineal and pubic regions. The trunk of the pubic nerve, n. pudendus, is covered by the gluteus maximus muscle. On the right side of the body the branches of the inferior pudendal nerve, rami perineales, nervi cutanei fermoris posterioris have been dissected out; but the branches of this nerve to the labium majus have been cut short. The formation of the anococcygeal or subcaudal nerves, nn. anococcygei, out of the posterior primary division of the coccygeal nerve and out of the perforating branches which arise from the anterior primary divisions of the fourth and fifth sacral nerves and the coccygeal nerve. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
12The greater number of the spinal nerves distributed to the
genital organs arise from the lumbar portion of the spinal cord,
pass as rami communicantes to the first four lumbar ganglia of the
great sympathetic cord, whence they proceed to the series of
symmetrical (paired) and asymmetrical (azygos) sympathetic
plexuses in front of, and adjacent to the abdominal aorta, which
already contain afferent and efferent spinal fibres derived from the
pneumogastric, phrenic, and splanchnic nerves. A small number
only of coarse nerve-filaments, a larger number of fine nerve-filaments,
derived from the sacral nerves, proceed direct to the
internal genital organs; many of these fibres enter the lower extremity
of the pelvic or inferior hypogastric pleans, some pass to
the cervical ganglia of the uterus. Below the bifurcation of the
aorta and in front of the sacral promontory, a large number of the
uterine nerves, both of spinal and of sympathetic origin, unite to
form an azygos plexus which has been shown by experiment to
possess great functional importance. Anatomically this constitutes
the upper undivided portion of the hypogastric plexus, which
is the downward continuation of the abdominal aortic sympathetic
plexus; but inasmuch as it is the principal channel of nervous impulses
to the uterus it is often known at the present day as the
great uterine plexus (plexus uterinus magnus). The nerves to
the ovary and Fallopian tube (ovarian nerves) are derived from
the spermatic (ovarian) plexus, an offshoot of the renal plexus;
as the spermatic plexus descends, it is reinforced by branches from
the abdominal aortic plexus, these branches often arising from
a small ganglion (spermatic ganglion). The hypogastric or great
uterine plexus, single and median above, divides below into the
paired pelvic or inferior hypogastric plexuses, which pass downward
and forward on either side of the rectum; these plexuses are
reinforced by spinal elements derived from the sacral nerves.
Before the terminal expansions of the pelvic or inferior hypogastric
plexus enter the tissues of the internal genital organs, the
bladder, and the rectum, small masses of ganglionic matter are interspersed
among the nerve fibres.
To the above general sketch, which has been based on the
synoptical description of Chrobak von Rosthorn, must be added
a more detailed account of the innervation of the ovaries, this
branch of the subject being of especial importance. The nerves of
the ovary are derived from the sympathetic system, in part from
the spermatic ganglion, in part from the second renal ganglion,
and in part from the superior mesenteric plexus. The nerves of
13the ovary are for the most part vascular nerves, which unite before
entering the ovary to form the ovarian plexus, and then pass into
the hilum with the vessels, envelop the vessels of the medullary
layer, and thence pass to the follicular region; exceedingly
numerous, they form a close-meshed network, surrounding all the
vessels up to the finest capillary ramifications; those fibres which
terminate in the capillary walls and those also which reach the
follicles are regarded by Riese as sensory. The great trunks of
the uterine nerves are transversely disposed in relation to the great
lateral vessels of the uterus, and passing inward toward the mucous
membrane they break up into pencils of filaments; the uterine
nerves proper are distributed for the most part to the muscular
substance. In the Fallopian tubes, the nerves form arches around
the lumen of the tube; some fibres also pass to the longitudinal
folds of the mucous membrane.
This expansion of the nerves of the cerebrospinal and sympathetic
systems in the female reproductive organs manifests the
multiple interconnection of the two systems in this region, and
proves beyond doubt that the sensory nerves of the genital organs
have manifold connections with the motor tracts of the whole
organism on the one hand and with the sensory ganglia of the central
nervous system on the other, and in addition with the vasomotor
centres and with efferent motor and secretory fibres.
As regards the vascular system of the female genital organs, the
latter are supplied by the internal iliac artery. One of the two
terminal branches of the common iliac, the internal iliac artery,
descends into the pelvis over the sacro-iliac synchondrosis. Its
branches may be arranged in four groups: anterior group, the
hypogastric, iliolumbar, and obturator arteries; posterior group,
the lateral sacral, gluteal, and sciatic arteries; internal group, the
inferior vesical, uterine, and middle haemorrhoidal arteries; inferior
group, comprising a single artery only, the internal pudic;
the uterine artery supplies the uterus and the vaginal fornices; the
ovarian artery supplies the ovary, the Fallopian tube, and the broad
ligament of the uterus; the vaginal, cervicovaginal, or vesico-vaginal
artery supplies the vagina; the internal pudic artery supplies
the vestibule and the clitoris; the superior and inferior external
pudic arteries (branches of the femoral artery) supply the labia
majora. The veins of the female genital organs correspond in
general to the arteries in their course and nomenclature, and empty
their blood into the internal iliac vein.
14
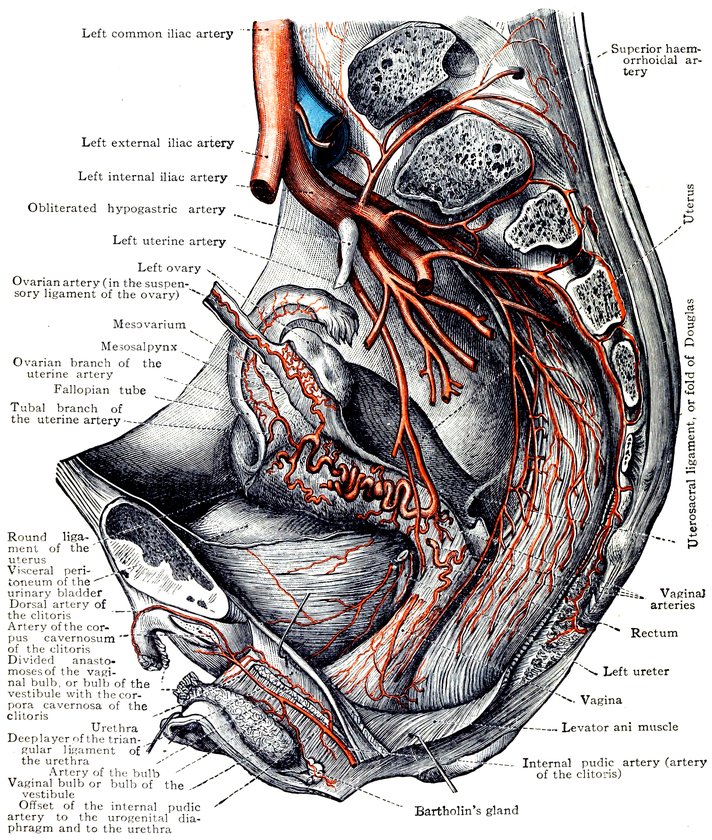
Fig. 4.—The distribution of the lateral sacral arteries, the superior haemorrhoidal or superior rectal artery, the uterine artery, the ovarian artery and the distal portion of the internal pudic artery. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
15Attention must also be paid to the extremely rich lymphatic
vascular system of the female genital apparatus. The body of the
uterus and the annexa of that organ, the neck of the uterus and
the vaginal fornices, the middle segment of the vagina, the lower
segment of the vagina, the vestibule and the external genital
organs—each of these possesses an independent set of lymphatic
vessels, leading moreover to independent groups of lymphatic
glands. It may be said that the lymph from the vulva passes to
the inguinal glands, that from the vagina and the neck of the
uterus to the internal and the external iliac lympathic glands, that
from the upper part of the uterus and also that from the ovaries
and Fallopian tubes to the median group of lumbar lymphatic
glands (also known, from their position in front of the aorta and the
vena cava, as the aortic lymphatic glands) (Chrobak von Rosthorn).
The important influence which the genital processes exercise on
the female organism as a whole is established not only by the
anatomical relations just described but also by a number of physiological
investigations and experiments and by the result of operations
on the female genital organs.
Thermic and mechanical stimulation of the female genitals has,
as my own experiments have shown, a notable influence on the
heart and the general circulation. In these experiments, when
uterine douches were given at temperatures of 4° C. (39° F.) and
45° C. (113° F.), the reflex nervous impulse which resulted from
these manipulations had a two-fold influence on the circulation,
manifesting itself first by an immediate and considerable augmentation
in the functional activity of the heart, the frequency of which
was increased in a degree proportional to the nervous sensibility
of the individual, and secondly by a notable rise in blood pressure.
With a view to determining the influence of stimulation of the
ovary on blood-pressure, Röhrig carried out some experiments on
bitches, from which it appeared that electrical stimulation of the
ovary invariably produced a remarkable increase in the general
blood-pressure, an increase ranging from twelve to twenty-four
millimeters of mercury. It further appeared in the course of these
experiments that toward the end of the period of stimulation the
rise in blood-pressure was always followed by a decline; to which,
however, a renewed rise of blood-pressure succeeded after the
stimulation was discontinued, provided the duration of this had not
been excessive. Only after this second rise was the normal mean
blood-pressure regained. Finally it was established that the pronounced
16phenomena of vagus-irritation exhibited by the curve
during and immediately after the stimulation of the ovary were
invariable concomitants of the rise of blood-pressure produced by
such stimulation.
According to the observations of Federns, the blood-pressure
undergoes a rhythmical change between one menstrual period and
the next, the pressure curve being normally at its lowest at the
time of the commencement of the flow, and at its highest at some
time during the two days immediately preceding the flow. This
rhythmical change of blood-pressure manifests itself also some
time before the first onset of menstruation, when the approach of
puberty is indicated only by the menstrual molimina.
Observations made by Kretschy in a patient with a gastric fistula
have proved the influence exercised on gastric digestion by the
physiological processes occurring in the female reproductive organs.
In this patient, his attention was especially directed to determining
at what period of digestion the secretion of acid by the stomach
attains its maximum, and how that secretion increases and
diminishes. He observed that the digestion of breakfast was completed
in four and one-half hours, the acid-maximum occurring in
the fourth hour, and the reaction of the gastric contents becoming
neutral one and one-half hours later. This apparently constant
acid-curve began, however, to become irregular as soon as the
first symptoms of the approach of menstruation became apparent.
When the flow had actually begun, he found that the reaction
of the gastric contents remained acid throughout the entire day.
As soon as the flow was over, the normal acid-curve was immediately
reëstablished.
These observations have been confirmed by Fleischer. This
investigator carried out his researches in menstruating women
with normal stomachs, and found that with the appearance of
the catamenia the process of digestion was almost always notably
retarded, but that with the diminution and cessation of the flow
digestion returned to the normal.
By stimulation of the central segment of the divided hypogastric
or great uterine plexus, Cyon was able to provoke vomiting, a confirmation
of the well-known physiological fact that irritative disturbances
of the female reproductive organs have a reflex influence on
the vomiting centre.
It is also clearly established that diverse stimulation of peripheral
nerves, those for instance of the mammary gland, of the
internal genitals, or of the epigastrium, is capable of affecting the
motor centre of the uterus.
Worthy of note also are Strassmann’s experiments, showing that
17rise of pressure in the ovary causes swelling and structural
changes in the uterine mucous membrane.
Striking also are Neusser’s discoveries that during menstruation
there is an increase in the eosinophil cells of the blood, and that
by the intermediation of the sympathetic nervous system the
ovaries exercise an influence on the hæmatopoietic function of
the red marrow of the bones. Most noteworthy is the connection
between the functional activity of the ovaries and osteomalacia.
In this disease of metabolism we have to do, according to Fehling’s
now generally accepted assumption, with a trophoneurosis of the
bones, a stimulation of the vasodilator nerves of the osteal vessels,
dependent on a reflex impulse from the ovaries. The connecting
path between the ovaries and the bones Neusser finds in this case
also in the sympathetic nervous system.
The reflex influence exercised on the heart and the general circulation
has been shown also by the results of operations on the
female genital organs. In cases in which the ovaries have been
removed, or in which these organs have been roughly handled,
Hegar has noticed a great diminution in the frequency of the
pulse, sometimes even cessation of the heart’s action. In similar
circumstances Champonière also observed as a rule diminished
frequency of the pulse, but in some cases increased frequency.
Mariagalli and Negri have described tachycardia following laparotomy
and the extirpation of double pyosalpinx. Bonvalot has
published cases in which, in consequence of vaginal or intra-uterine
injections, in consequence of simple examination, and in consequence
of the performance of version, sudden death has resulted
from cardiac syncope.
The psychical influences which proceed from the female genital
organs in the different periods of sexual life have also great significance
for the organism as a whole. Manifold impulses both
stimulating and depressing arising in the reproductive organs affect
the workings of the mind. The maiden at puberty is affected by
the knowledge of sexuality; the sexually mature woman, by the
desire for sexual satisfaction, and by the yearning for motherhood;
the wife, by the processes of pregnancy, parturition, and
suckling, or, on the other hand by the distressing consciousness of
sterility; the woman at the climacteric period, by the knowledge of
the disappearance of her sexual potency. The mind is further
sympathetically influenced by the stimulation of the terminals of
the sensory nerves in the genital organs. Through the increase
of such stimulation, through its spread to adjacent nerves and
nerve tracts and to the entire nervous system, the mind is affected,
18directly by irradiation, or indirectly by vasomotor processes and
spinal hyperæsthesia.
Psychical manifestations and the nervous states associated with
these are somewhat frequently, and even actual psychoses occasionally,
encountered in the various phases of the sexual life of
woman, sometimes taking the form of violent sexual storms, which
may indeed, as ordinary menstrual reflexes, accompany every catamenial
period.
Of great interest are the facts which have, in recent times especially,
been scientifically established, pointing to a certain periodicity,
to an undulatory movement of the general bodily functions of the
female organism, dependent upon the sexual life. The observations
of Goodman, Jacobi, von Ott, Rabuteau, Reinl and Schichareff,
have shown that in woman the principal vital processes pursue a
cycle made up of stages of increased and diminished intensity, and
that this periodicity of the chief general processes of vital activity
finds expression also in the functions of the reproductive organs.
Goodman has compared this play of general vital functions to an
undulatory movement. According to this writer, a woman’s life
is passed in stages, each of which corresponds in duration with a
single menstrual cycle. Each of these stages exhibits two distinct
halves, in which the vital processes are respectively ebbing and
flowing: in the latter we see an increase of all vital processes, a
larger heat production, a rise in blood-pressure, and an increased
excretion of urea; in the former we see, on the contrary, that all
these vital processes display a diminished intensity. The moment
when the period of increased vital activity is at an end, the moment
when the ebb begins, corresponds, according to Goodman, to the
commencement of the catamenial discharge.
Goodman sought for verification of this undulatory theory of the
sexual life of woman in certain data regarding the bodily temperature
and the blood-pressure. A more extensive research was
undertaken by Jacobi, who, as the result of her observations, came
to the following conclusions. In eight cases she noticed in the premenstrual
epoch a rise of temperature ranging from 0.05° C. to
0.44° C. (0.09° F.–0.79° F.); and during the catamenial discharge
a gradual fall of 0.039° C.–0.25° C. (0.072° F.–0.45° F.), never
less, that is to say, than a quarter of a degree Centigrade; but in the
majority of cases the temperature did not, while the catamenia lasted,
regain the normal mean. She further observed in the generality
of cases an increased excretion of urea during the premenstrual
epoch; and a notable fall in blood-pressure during menstruation.
Reinl’s observations on healthy women, in whom menstruation
ran a normal course, showed that in the great majority of cases in
19the premenstrual epoch the temperature was elevated as compared
with that of the interval, that in eleven out of twelve cases the
temperature gradually declined during menstruation, to fall in three-fourths
of the cases below the mean temperature of the entire interval,
and exhibiting in the post-menstrual epoch a still further depression,
giving place, however, to a somewhat higher mean temperature
during the first half of the interval. In the second half of the interval
a higher mean temperature was observed than in the first
half.
If we make a graphic representation of the mean differences in
temperature commonly observed throughout the various stages of
an entire menstrual cycle, we see that the curve does in fact take the
form of a wave. That drawn by Reinl is shown in the following
figure: (Fig. 5.)
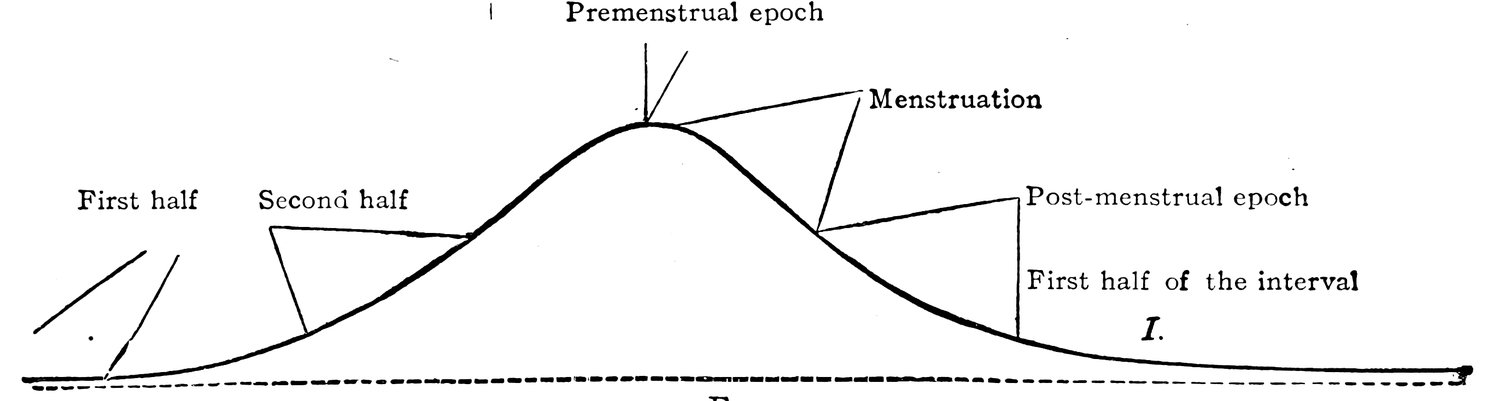
The rising portion of the wave, the beginning of the tidal flow,
corresponds to the second half of the interval; the height of the tidal
flow, the crest of the wave, corresponds to the premenstrual epoch.
As the flow gives place to the ebb, as the wave begins to decline,
we come to the actual period of the catamenial discharge; later in
the ebb is the post-menstrual epoch, and the lowest portion of the
declining wave corresponds to the first half of the interval. Rhythmic
changes corresponding to those observed in the temperature
have been recorded—at least in isolated stages of the menstrual
cycle—affecting the blood-pressure by Jacobi and by von Ott, affecting
the excretion of urea by Jacobi and by Rabuteau, and affecting
the pulse by Hennig. It is evident that the vital activity of the
organism attains its maximum shortly before menstruation; and
that with or immediately before the appearance of the catamenial
discharge, a decline of that activity commences.
Schrader, through his researches on metabolism during menstruation
in relation to the condition of the bodily functions during this
process, has established that immediately before menstruation the
elimination of nitrogen in the fæces and the urine is at its lowest,
a fact which indicates that at this period of the menstrual cycle
the disintegration of albumen in the body is notably diminished.
20Von Ott found in thirteen cases out of fourteen that at the beginning
of the catamenial discharge or just before a considerable
fall in blood-pressure occurred, and that throughout the flow the
pressure almost always remained below the mean, no rise taking
place till menstruation was finished; this fall in blood-pressure during
menstruation was more considerable than could be accounted
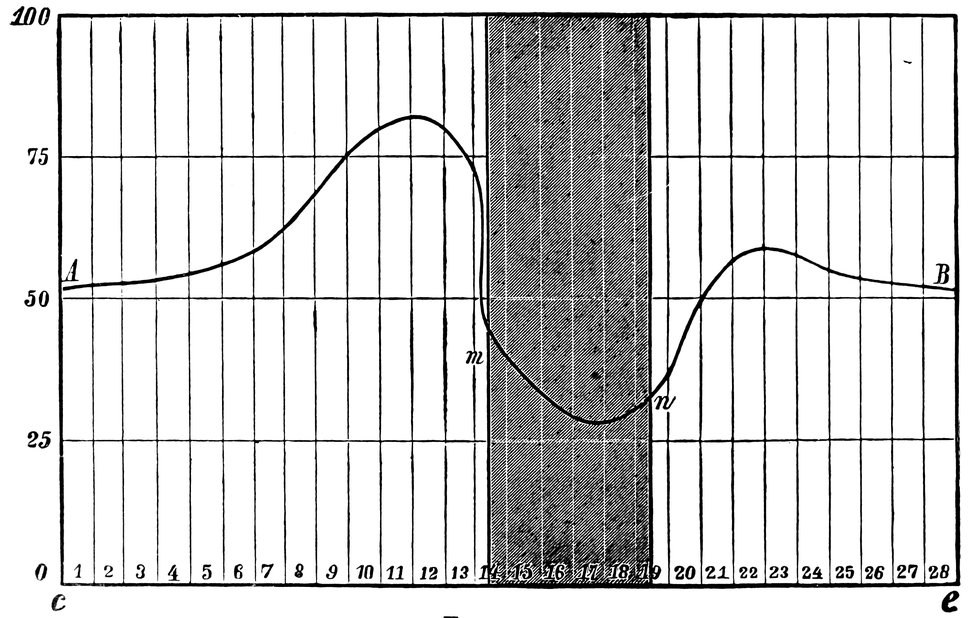
for by the moderate hæmorrhage. The same author, in conjunction
with Schichareff, examined fifty-seven healthy women in respect
of heat-radiation, muscular power, respiratory capacity, expiratory
and inspiratory power, and tendon-reflexes. He found that the
energy of the functions of the female body increased before the
beginning of menstruation, but declined with or immediately before
the appearance of the catamenial discharge. He exhibited this
rhythmical variation in the vital processes by means of the following
curve, in which the line A B represents these physiological variations,
whilst on the abscissa line c e, the days of observation are recorded,
and the interval m n represents the menstrual period.
The degree of intensity of the united functions is indicated by the
numbers 0–100 on the ordinate.
Still another point of view from which the influences affecting
the female organism as a whole may be regarded has very recently
become apparent in consequence of the doctrine of Brown-Séquard
relating to the internal secretions of ductless glands. As regards the
female reproductive glands, which in consequence of their structure
must be referred to the group of ductless glands, and yet owing to
21their secretory function must be classed among secreting glands
(so that the nature of the ovary is that of a secreting gland without
an excretory duct), it would appear that these glands are not concerned
only with the specific female reproductive functions of menstruation
and ovulation, but that they also exercise a powerful influence
on the nutritive processes, on metabolism and hæmatopoiesis,
and on growth and development in their mental as well as their
physical relations.
It is supposed that these glands under normal conditions enrich
the blood with certain substances, which in part assist in
hæmatopoiesis, and in part by regulating the vascular tone in the
various organs are concerned in the normal processes of assimilation
and general metabolism. According to Etienne and Demange,
ovariin possesses an oxidising power similar to that possessed by
spermin. Thus it becomes easy to understand how disturbances in
the functions of the ovaries give rise to disturbances in the
processes of general metabolism and of assimilation. Some go
even further, though in doing so they leave the ground of assured
fact, suggesting that the ovary in certain circumstances produces
toxins, or that the normal ovary possesses an antitoxic function,
and speaking of an occasional ovarian auto-intoxication of the
body or of a menstrual intoxication. Thus, chlorosis is by some
regarded as a disturbance of hæmatopoiesis, dependent on an abnormal
condition of the female reproductive organs during the
period of development, and referable to a disturbance of the internal
secretion of the ovaries (Charrin, von Noorden, Salmon, Etienne,
and Demange). And it is now generally assumed, the assumption
being based on the observations recently made concerning the organo-therapeutic
employment of the chemical constituents of the
ovary, that many of the disorders, and especially those connected
with the vasomotor system, common during the climacteric period,
are dependent on the deficiency of the products of the internal
secretion of the ovary that accompanies the cessation of the menses.
Recent experimental investigations on this subject have shown
that the interconnection between the female genital organs and the
organism as a whole, between the functions of the reproductive
organs and the functions of other organs, does not depend on
nervous influences only, but that in this interconnection the blood
vascular system and the lymphatic vascular system also play their
parts. Goltz has proved by actual experiment that the nervous influence
on menstruation and ovulation is not the only determinant.
In a bitch, he divided the spinal cord at the level of the first lumbar
vertebra, and observed, as soon as the animal had recovered from the
operation, the appearance of the usual signs of heat; the bitch was
22impregnated, and gave birth to one living and two dead puppies;
lactation and sucking took place as in a normal animal. When the
bitch was killed and the body examined it was found that no reunion
had taken place in the severed spinal cord. The experiments of
Halban gave similar results. He found that in apes, if the ovaries
are removed from their normal situation and successfully transplanted
to some region remote from the genital organs, the animals
remain capable of menstruating. But if the ovaries, which have
been transplanted beneath the skin or beneath the peritoneum, are
subsequently entirely removed, menstruation, which has continued
regularly after the first operation, ceases altogether after the second.
It follows from these experiments that the cessation of the menstrual
process may be considered to be brought about through the intermediation
of the lymphatic or blood-vascular system, by the absence
of a kind of internal secretion.
Loewy and Richter have further proved by experiment that in
spayed bitches the consumption of nitrogen is less by about 20
per cent. and the entire gaseous interchange less by about 9 per
cent., as compared with what takes place in normal animals, and
that this change in respiratory metabolism lasts for a long time
after the oöphorectomy, for as much as nine to twelve months. If
dried ovaries are given to such animals in their food, the gaseous
interchange rises to the former level and even higher.
The undulatory movement of the vital processes in woman is
apparently in some way dependent on ovulation, though the nature
of the connection has not hitherto been fully elucidated. This view
is confirmed by the fact that no such rhythmic variation in the
bodily functions can be detected either in girls under thirteen years
of age, or in women from fifty-eight to eighty years of age in
whom menstrual activity has entirely disappeared. The menstrual
rhythm begins at puberty and ends when ovulation ceases.
A further contribution to the doctrine of the undulatory movement
of the vital processes in woman is to be found in my own
observations that pathological symptoms which have become manifest
before and at the time of the first onset of menstruation, and
have given but little trouble throughout the period of developed
and regular sexual activity, are apt when menstruation ceases to
recrudesce, and to become as prominent as they were at the commencement
of the sexual life. Women who at the time of puberty
suffered from cardiac troubles, from digestive disturbances, or from
various forms of nervous irritation, and in whom as they grew up
these disorders passed more or less into abeyance, are apt at the
climacteric period to exhibit, as I have frequently been able to
observe, a violent return of these symptoms, in the form, as the
23case may be, of tachycardia, of dyspeptic troubles, or of psychoneuroses.
In this connection we may mention an observation of
Potain’s, who distinguishes a peculiar form of chlorosis, occurring in
individuals of delicate constitution, which, though apparently cured,
reappears at the menopause.
Related to the sexual life of woman is another attribute, one intimately
connected with the idea of the female sex, and one which
since the primeval days of humanity has filled men with delight and
poets with inspiration—the attribute of beauty.
The beauty of woman, a prominent secondary sexual character,
makes its first appearance at puberty, when the girl’s form, hitherto
undifferentiated in its external bodily configuration, begins to assume
a soft and rounded appearance, when the features become
regular, the breasts enlarge, and the pubic hair begins to grow—when,
in short, to the primary sexual characters already existing,
the secondary sexual characters are superadded.
Feminine beauty continues to increase until the attainment of
sexual maturity. In her third decade woman arrives at the acme
of her sexual life and at the same time attains the perfection of her
beauty.
The ensuing sexual phases, pregnancy, parturition, and lactation,
entail a decline in beauty, not rapid indeed, but advancing gradually,
with the slow yet sure-footed pace of time. The organic revolutions
accompanying these processes leave traces recorded upon the surface
of the body in conspicuous and indelible characters. The illnesses,
also, which so often accompany the fulfilment of sexual
functions, in injuring health impair also beauty.
A woman who has given birth to and nursed an infant begins to
lay on fat, and this tendency to obesity becomes more pronounced
as the climacteric period approaches. The breasts become inelastic
and pendent, the abdomen becomes ungracefully prominent; the
tonicity of the entire organism gradually declines, and, in consequence
of the loss of elasticity in the subcutaneous cellular tissue,
the dreaded wrinkles make their appearance and the features become
wizened. Beauty is a thing of the past. With the cessation
of the sexual life the external secondary sexual characters disappear,
and the old woman is even farther removed than the old man from
our conception of beauty.
As Mantegazza insists, the beauties peculiar to women are one and
all sexual; they depend, that is to say, upon the peculiar functions
that nature has allotted to woman in the great mystery of procreation.
One of the most vivid and poetical descriptions in ancient or
modern literature of these secondary sexual characters on which
feminine beauty depends is to be found in the Song of Solomon.
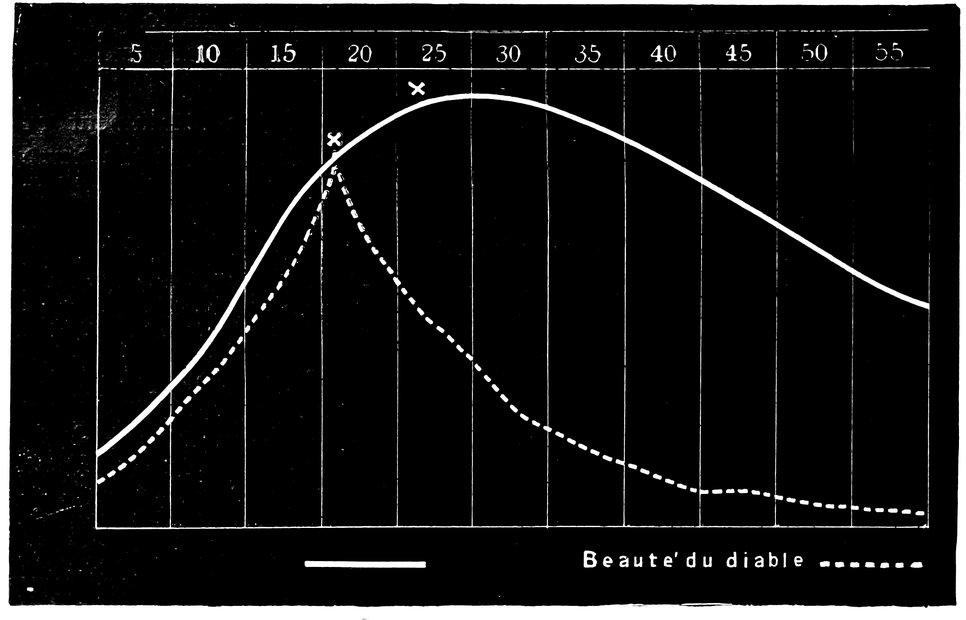
24In the following figure (Fig. 7) the curve of beauty of woman
is given as drawn up by Stratz. In one case it may rise very
quickly, to decline with equal quickness—the so-called beauté du
diable;[16] in other cases, again, the curve rises very slowly, and
declines also very slowly, the culmination of the curve being in
this case attained later, and when attained being absolutely higher,
than in the case of the steeper curve.
The age at which the maximum of beauty is attained is a very
variable one. In the southern races this often occurs as early as
the fourteenth or fifteenth year of life; but in the peoples of the
Teutonic stock, Germans, Dutch, Scandinavians, and English, not
as a rule before the twentieth year, and it may be even later. Stratz
has known cases in which women did not attain the prime of
their beauty until the thirtieth and even the thirty-third year. The
same author, a most competent authority as regards the subject
of feminine beauty, affirms that a beautiful woman is most beautiful
when the period of maximum beauty coincides in her case with
the first month of her first pregnancy. With the commencement
of pregnancy the processes of nutrition are accelerated, all the
tissues are tensely filled, the skin is more delicately and at the same
time more brightly tinted owing to the greater activity of the circulation,
the breasts become firmer and more elastic. Thus the
attractive characteristics of beauty at its fullest maturity become
25enhanced, but for a short time only, since the enlargement of the
abdomen in the further course of pregnancy impairs the harmony
of the figure. Finally we must point out, before dismissing this
subject, that women of the so-called better classes arrive as a rule
at maturity later, and remain beautiful for a longer period, than
women of the working classes.
The degree to which the female organism as a whole is influenced
by the processes of the sexual life that occur in the genital
organ depends upon many of the characteristics that combine to
make up the individuality. Inherited characteristics, temperament,
and race, play a great part in this connection; and not less
important than these are the social conditions, the environment, in
which the women under consideration pass their life. Thus,
among women belonging to the poorer, labouring classes, the reflex
manifestations in other organs dependent upon the processes of
the genital organs are less frequent and less intense than among
women belonging to the well-to-do strata of society and to the
cultured classes; less also in the country than in large towns. In
phlegmatic individuals, such manifestations exhibit less intensity
than in those of an active, ardent temperament; they are less frequent
in persons with a powerful constitution than in those endowed
by inheritance with an unstable nervous system. Finally,
they are less often encountered among families whose upbringing
has aimed at hardening the constitution and at inculcating the
control of instinctive impulses, than among those in whom from
early childhood sensibility and impulsiveness have been given a
loose rein.
Extremely variable also are the sympathetic disturbances and
morbid states which depend on the processes of the sexual life of
woman. “Le cri de l’organe souffrant ne vient pas de l’utérus,
mais de tout l’organisme,”[17] says Courty. And a large number of
isolated observations has shown how complex are the relations
between the healthy and unhealthy female genital organs and the
other organs of the body as well as the organism as a whole.
Precise and incontestable proofs exist of such relations between
the female genital organs and morbid changes in the eye and ear,
the skin, the respiratory organs, and the vascular and nervous
systems.
The influence exercised by the reproductive system on the general
vital processes of woman is indicated also by the general
statistics of mortality and the incidence of disease. Mortality in
women, the earliest years of childhood being left out of consideration,
26is at its highest precisely during the great sexual epochs,
namely at the time of puberty, during pregnancy, during the puerperium,
and at the climacteric period. The complete performance
of the reproductive functions entails a higher proportion of illnesses
and death; and statistical records show that the mortality
of married women between twenty and forty years of age, during
the period, that is to say, in which in consequence of marriage
they fulfil the duties of sexual intercourse and procreation, and are
exposed to the dangers connected with these sexual acts, is much
higher than the mortality of unmarried women of corresponding
ages. Infection with the gonococcus and with the virus of syphilis,
chronic salpingitis, metritis, and parametritis, the manifold diseases
of pregnancy, the diseases of the puerperium, the various displacements
of the uterus, osteomalacia—all these are pathological
states the dependence of which upon the sexual life of the married
or at any rate sexually active woman is indisputable. But the
complete renunciation of sexual activity appears also to exercise
an injurious influence on the health, and to give rise or at least
predispose to morbid manifestations. Hysteria, for instance,
chlorosis, uterine myomata, and various neuroses, have long been
supposed to depend in part upon such renunciation, though the
causal connection cannot be regarded as yet fully established.
Especially true as regards woman, indeed, is that which Ribbing
says concerning the sexual life in general: “Since all human life
and being has its origin in sexual relations, these sexual relations
may be regarded as the heart of humanity. We may work day and
night for the good of humanity, we may sacrifice for that good
our time and our blood, but all this work and all this sacrifice
appear to me to remain useless if we neglect and despise the sexual
life, the eternally self-renewing elementary school of true altruism.”
From the vital phase in which, marked by the visible manifestations
of puberty and by the first appearance of menstruation,
ovulation is assumed to begin, the sexual life of woman continues
to the period of life in which, marked by the climacteric cessation
of menstruation, ovulation also ceases. The total duration of this
sexual period in woman’s life is usually about thirty years; but it is
subject to great variations, from six to forty-six years according
to the available statistics, these variations depending upon climate,
race, constitution, and the sexual activity of the person under
consideration.
The duration and the intensity of the sexual life of woman depends
upon a series of external conditions affecting the individual,
but especially upon the inherited predispositions, upon the constitutional
conditions, upon the varying vital power of the individual.
27My own observations have led me to formulate, as a general law,
that the earlier a woman (climatic and social conditions being
similar in the cases under comparison) arrives at puberty, the
earlier, that is to say, that menstruation first makes its appearance,
the greater will be the intensity and the longer the duration of
sexual activity, the more will the woman in question be predisposed
to bear many children, the more powerfully will the sexual impulse
manifest itself in her, and the later will the menopause
appear. It seems that in such women a more intense vitality animates
the reproductive system, bringing about an earlier ripening
of ova, a more favorable predisposition on the part of these ova
to fertilization by the spermatozoa, a livelier manifestation of
sexual sensibility, and a longer duration of ovarian functional
activity.
My general views on this subject are embodied in the following
propositions:
1. The duration of sexual activity is less in the women belonging
to the countries of southern Europe than in those belonging
to the countries of northern Europe. It would appear that in
those climates in which ovulation begins sooner and menstruation
first appears at an earlier age, the menopause also appears earlier;
but that, on the contrary, in those climates in which puberty is
late in its appearance, the decline of sexual activity is similarly
postponed.
2. Women in our mid-European climates, in whom puberty
appears at an early age, the first menstruation occurring between
the ages of thirteen and sixteen, exhibit a more prolonged duration
of the sexual life, of menstrual functional activity, than women
in whom menstruation begins late, between the ages of seventeen
and twenty. Extremely early appearance of the first menstruation—so
early as to be altogether abnormal—has, however, the
same significance as abnormally late onset of menstruation; both
indicate that the sexual life will be of short duration.
3. Women whose reproductive organs have been the seat of a
sufficient amount of functional activity, who have had frequent
sexual intercourse, have given birth to several children, and have
themselves suckled their children, have a sexual life of longer duration,
as manifested by the continuance of menstruation, than women
whose circumstances have been just the opposite of these, unmarried
women, for instance, women early widowed, and barren women.
Sexual intercourse at a very early age, however, accelerates the
onset of the climacteric period and the termination of the sexual
life. The same result follows severe or too frequent confinements.
4. The sexual life has a shorter duration in the women of the
laboring classes and belonging to the lower strata of social life, as
28compared with upper class and well-to-do women. Bodily hardships,
grief, and anxiety also hasten the onset of sexual death.
5. Women who are weakly and always ailing have a shorter
sexual life than women who are powerfully built and always in
good health. When irregularities and disorders have appeared in
the various sexual phases, the decline of sexual activity occurs
earlier than in women whose functions have in this respect been
normal. Certain constitutional conditions, such as extreme obesity,
certain acute diseases, such as typhoid fever, malaria, and cholera,
and certain diseases of the uterus and its annexa, chronic inflammatory
conditions for instance, bring about a notable shortening of
the duration of the sexual life.
In 500 cases that have come under my own observation, the
women concerned belonging to very various nationalities, the duration
of the sexual life, as witnessed by the continuance of menstruation,
was as follows:
Menstruation continued for:
| 6 years in |
1 woman. |
| 7 years in |
1 woman. |
| 9 years in |
2 women. |
| 11 years in |
4 women. |
| 15 years in |
6 women. |
| 16 years in |
8 women. |
| 17 years in |
12 women. |
| 18 years in |
15 women. |
| 19 years in |
9 women. |
| 20 years in |
6 women. |
| 21 years in |
18 women. |
| 22 years in |
20 women. |
| 23 years in |
24 women. |
| 24 years in |
18 women. |
| 25 years in |
16 women. |
| 26 years in |
25 women. |
| 27 years in |
26 women. |
| 28 years in |
29 women. |
| 29 years in |
36 women. |
| 30 years in |
22 women. |
| 31 years in |
32 women. |
| 32 years in |
49 women. |
| 33 years in |
31 women. |
| 34 years in |
26 women. |
| 35 years in |
12 women. |
| 36 years in |
12 women. |
| 37 years in |
10 women. |
| 38 years in |
8 women. |
| 39 years in |
6 women. |
| 40 years in |
2 women. |
| 43 years in |
2 women. |
| 45 years in |
1 woman. |
| 46 years in |
1 woman. |
Thus we see that the duration of the sexual life varies from 6 to
46 years. The most frequent duration is one of 32 years, next to
this one of 29, next again, 31, 33, and 37 years, respectively. In
6 women only did the duration of the sexual life exceed 40 years,
and in 4 only was it less than 11 years. In half of all my cases the
duration of the sexual life was between 27 and 34 years, and from
these figures we obtain an average duration of about 30 years.
For North Germany, Krieger gives data from which it appears
that in this region the average duration of the sexual life is 30.49
years. In more than half of the 722 cases recorded by this writer
the duration was between 31 and 37 years. In isolated cases the
duration was very short, not exceeding 8, 9, or 10 years, or, on the
other hand, as long as 47 years; whilst the number of cases increased
fairly regularly up to the duration of 34 years, and thereafter
again diminished.
As regards Austria, Szukits has collected information in the
case of 269 women, and found, in these, that the duration of the
sexual life varied from 12 to 45 years. The average duration was
2929.16 years; in more than half of the women, the period of sexual
activity lasted from 21 to 30 years; the shortest period observed
was 12 years, the longest 45 years.
The period of sexual activity lasted:
| 12 years in |
2 women. |
| 14 years in |
1 woman. |
| 15 years in |
2 women. |
| 17 years in |
3 women. |
| 19 years in |
3 women. |
| 20 years in |
17 women. |
| 21 years in |
10 women. |
| 22 years in |
7 women. |
| 23 years in |
5 women. |
| 24 years in |
17 women. |
| 25 years in |
7 women. |
| 26 years in |
13 women. |
| 27 years in |
5 women. |
| 28 years in |
26 women. |
| 29 years in |
18 women. |
| 30 years in |
17 women. |
| 31 years in |
8 women. |
| 32 years in |
8 women. |
| 33 years in |
13 women. |
| 34 years in |
8 women. |
| 35 years in |
18 women. |
| 36 years in |
19 women. |
| 37 years in |
14 women. |
| 38 years in |
9 women. |
| 39 years in |
8 women. |
| 40 years in |
1 woman. |
| 42 years in |
1 woman. |
| 43 years in |
1 woman. |
| 44 years in |
2 women. |
| 45 years in |
2 women. |
In Poland, according to Raciborski, the duration of sexual activity
is in Jewesses 23 years, but in women of Slavonic blood 31 years.
In France, according to Courty and Puech, the usual duration of
the sexual life is from 28 to 30 years.
According to Puech, among 10 women menstrual activity lasted:
| 33 years in |
2 women. |
| 35 years in |
1 woman. |
| 36 years in |
2 women. |
| 39 years in |
2 women. |
| 43 years in |
2 women. |
| 44½ years in |
1 woman. |
Brierre de Boismont gives the following particulars of the duration
of menstrual activity in 178 Frenchwomen:
| 5 years in |
1 woman. |
| 6 years in |
1 woman. |
| 8 years in |
1 woman. |
| 11 years in |
1 woman. |
| 16 years in |
4 women. |
| 17 years in |
4 women. |
| 18 years in |
1 woman. |
| 19 years in |
3 women. |
| 20 years in |
3 women. |
| 21 years in |
4 women. |
| 22 years in |
3 women. |
| 23 years in |
12 women. |
| 24 years in |
8 women. |
| 25 years in |
8 women. |
| 26 years in |
11 women. |
| 27 years in |
7 women. |
| 28 years in |
6 women. |
| 29 years in |
7 women. |
| 30 years in |
13 women. |
| 31 years in |
13 women. |
| 32 years in |
9 women. |
| 33 years in |
9 women. |
| 34 years in |
7 women. |
| 35 years in |
5 women. |
| 36 years in |
10 women. |
| 37 years in |
6 women. |
| 38 years in |
5 women. |
| 39 years in |
2 women. |
| 40 years in |
7 women. |
| 41 years in |
1 woman. |
| 42 years in |
3 women. |
| 44 years in |
2 women. |
| 48 years in |
1 woman. |
For England, Tilt gives the mean duration of menstrual activity,
as observed in 500 women, as 31.21 years; it varies between 11
and 47 years; there are more cases with a period of 34 years
than with any other integral number of years. Tilt found the duration
to be:
| 11 years in |
1 woman. |
| 13 years in |
1 woman. |
| 15 years in |
3 women. |
| 16 years in |
1 woman. |
| 17 years in |
2 women. |
| 18 years in |
4 women. |
| 19 years in |
1 woman. |
| 20 years in |
3 women. |
| 21 years in |
6 women. |
| 22 years in |
11 women. |
| 23 years in |
11 women. |
| 24 years in |
10 women. |
| 25 years in |
22 women. |
| 26 years in |
11 women. |
| 27 years in |
25 women. |
| 28 years in |
29 women. |
| 29 years in |
35 women. |
| 30 years in |
36 women. |
| 31 years in |
33 women. |
| 32 years in |
38 women. |
| 33 years in |
35 women. |
| 34 years in |
49 women. |
| 35 years in |
33 women. |
| 36 years in |
26 women. |
| 37 years in |
16 women. |
| 38 years in |
15 women. |
| 39 years in |
15 women. |
| 40 years in |
6 women. |
| 41 years in |
4 women. |
| 42 years in |
7 women. |
| 43 years in |
5 women. |
| 44 years in |
3 women. |
| 45 years in |
1 woman. |
| 46 years in |
1 woman. |
| 47 years in |
3 women. |
30For London the average figure is 34 years; for Paris, 30 years;
for Vienna, 29 years; and for Berlin, 34 years.
From the data of various observers obtained from diverse nationalities,
the following table has been compiled, exhibiting the
mean duration of the sexual life:
| Comparative Table Showing the Duration of the Sexual Life in Various Nationalities. |
|---|
| |
|
Germany. |
Austria. |
France. |
England. |
Denmark. |
Norway. |
Russia. |
| Number of Cases |
722 |
265 |
178 |
500 |
312 |
391 |
100 |
| Mean duration of menstrual activity, in years |
30.4 |
29.1 |
29.1 |
31.8 |
27.9 |
32 |
31 |
| Observers’ names |
Krieger, L. Mayer. |
Szukits. |
Brierre de Boismont. |
Whitehead. |
Hannover. |
Faye & Vogt. |
Lieven. |
In the temperate zone the sexual life of woman lasts longer than
in the colder and subarctic regions. Still more favorable is the contrast
between the temperate zone and the countries of the tropics, in
which the duration of the period of menstrual activity is limited to
eighteen or twenty years. According to some isolated observations
the duration of sexual activity in Arabian women in Africa was as
little as nine years.
A certain influence on the duration of the sexual life is exercised
by the commencement of menstruation at an earlier or later age than
the average. The total duration of menstrual activity is more
variable in women who begin to menstruate early than in women
who begin to menstruate late, in whom the duration of the sexual
life is a more regular one. In those women who begin to menstruate
early the mean duration of the sexual life is about thirty-three
years, in those who begin to menstruate late it is about twenty-seven
years.
The following data, based on the observation of 250 cases, are
published by W. Guy, regarding the duration of the sexual life,
that is to say of menstrual activity, in women beginning to menstruate
early and those beginning to menstruate late, respectively:
| Menstruation began. |
Duration of the sexual life. |
| In |
5 cases in the 8th to the 10th year |
Averaging 36.60 years. |
| In |
70 cases in the 11th to the 13th year |
Averaging 33.65 years. |
| In |
110 cases in the 14th to the 16th year |
Averaging 30.85 years. |
| In |
56 cases in the 17th to the 19th year |
Averaging 28.35 years. |
| In |
9 cases in the 20th year or later |
Averaging 20.45 years. |
31A further analysis of these 250 cases is given by Guy in the following
table:
| First appearance of menstruation. |
Average age at which menstruation ceased, in years. |
Duration of menstrual activity. |
| In |
1 case in the |
8th year |
42 |
34 years. |
| In |
2 cases in the |
9th year |
46 |
37 years. |
| In |
2 cases in the |
10th year |
47 |
37 years. |
| In |
10 cases in the |
11th year |
47.10 |
36.10 years. |
| In |
29 cases in the |
12th year |
45.34 |
33.34 years. |
| In |
31 cases in the |
13th year |
46.16 |
33.16 years. |
| In |
39 cases in the |
14th year |
45.33 |
31.33 years. |
| In |
40 cases in the |
15th year |
46.30 |
31.30 years. |
| In |
41 cases in the |
16th year |
46.14 |
30.14 years. |
| In |
26 cases in the |
17th year |
45.18 |
28.18 years. |
| In |
19 cases in the |
18th year |
46.87 |
28.87 years. |
| In |
11 cases in the |
19th year |
46.18 |
27.18 years. |
| In |
5 cases in the |
20th year |
40.80 |
20.80 years. |
| In |
3 cases in the |
21st year |
41.66 |
20.66 years. |
| In |
1 case in the |
23d year |
41 |
18 years. |
Hannover also gives data respecting the relation between the duration
of menstrual activity and the early or late appearance of menstruation.
These data are tabulated as follows:
| First appearance of menstruation. |
Average age at which menstruation ceased, in years. |
Duration of menstrual activity. |
| In |
5 cases in the |
12th year |
47.80 |
35.80 years. |
| In |
10 cases in the |
13th year |
45.89 |
32.89 years. |
| In |
50 cases in the |
14th year |
44.98 |
30.98 years. |
| In |
34 cases in the |
15th year |
45.56 |
30.56 years. |
| In |
38 cases in the |
16th year |
44.13 |
29.13 years. |
| In |
36 cases in the |
17th year |
43.00 |
26.00 years. |
| In |
49 cases in the |
18th year |
44.96 |
26.96 years. |
| In |
33 cases in the |
19th year |
44.79 |
25.79 years. |
| In |
38 cases in the |
20th year |
45.36 |
25.36 years. |
| In |
10 cases in the |
21st year |
44.10 |
23.10 years. |
| In |
4 cases in the |
22d year |
43.50 |
21.50 years. |
| In |
3 cases in the |
23d year |
44.33 |
21.33 years. |
| In |
4 cases in the |
24th year |
39.50 |
15.50 years. |
Totals: In 412 cases the average age at the menopause was
44.82, and the average duration of menstrual activity was 27.973
years.
From the tables of L. Mayer, Krieger has instituted a comparison
between the duration of menstrual activity in 101 women who
began to menstruate early and 180 women who began to menstruate
late, finding in the case of the former a mean duration of 33.673
years, and in the case of the latter a mean duration of 27.344
years, showing therefore a sexual life longer on an average by 6.429
years in those in whom puberty was early as compared with those
in whom puberty was late.
From the tables of Tilt, based on the observation of 164 cases,
76 women in whom menstruation appeared early and 88 in whom
32it appeared late, we learn that among the former the shortest duration
of menstrual activity was 18 years, among the latter 12
years; among the former the longest duration was 37 years, among
the latter only 33. The majority of those who began to menstruate
early continued to menstruate for 28, 31, 32, 33, 34, 35, 36, 38, or
39 years; those who began to menstruate late, for 23, 27, 28, 30,
or 31 years. The mean duration of the sexual life in those who
began to menstruate early was 33.66 years; in those who began
to menstruate late it was 28.28 years. Since the average duration
of the menstrual function is given by Tilt as 31.33 years, those who
began to menstruate early exceeded this average by 2.33 years,
while those who began to menstruate late exhibited a duration of
menstrual activity of at least three years less than the average.
In addition to climate, nationality, and the age at which menstruation
begins, the sexual activity of women also exercises an influence
on the duration of their sexual life, and of especial importance
in this connection are the number of children born, and exercise
or neglect of the function of lactation. From my own observations
on this matter it appears, that in women who are healthy
and of powerful constitution, whose reproductive organs have been
sufficiently exercised, who have given birth to several children
and have suckled these children themselves, the duration of menstrual
activity is in general notably longer than in women whose
circumstances have been just the opposite in these respects. Among
the women in my own series of cases in whom menstrual activity
lasted longest, of the 177 women in whom menstruation ceased between
the forty-fifth and the fiftieth year of life, 1 only was unmarried,
2 were married but childless, 32 married with 1 or 2
children only, and 142 married and with more than 2 children; of
the 89 women in whom menstruation ceased between the fiftieth
and the fifty-fifth year of life, none were either unmarried or childless,
19 were married with 1 or 2 children, 17 married and with
more than 2 children; of the 17 women in whom menstruation
ceased later than the fifty-fifth year of life, there were 2 only with
less than 2 children, but 10 who had each given birth to from 6 to 8
children. A similar influence is exercised by the function of
lactation. Among 40 women who had not suckled their children,
the average duration of menstrual activity was 4 years less than the
general mean.
As regards the conditions of life, L. Mayer affirms that the duration
of sexual activity among well-to-do women is on the average
a year and a half longer than among women of the working classes.
Metschnikoff has drawn attention to the remarkable disharmony
in the development of three of the phases of the sexual life of
33woman, inasmuch as the sexual impulse, the union of the sexes,
and the capacity for procreation, which, considering their nature
and purpose, might have been expected to be attuned so as to act
in harmony, exhibit as a matter of fact no such relation; the different
factors of the sexual function develop independently and
unharmoniously. In a child not yet fitted to fulfil the function of
procreation, the sexual impulse will none the less make its appearance,
and be liable to misuse. In the girl the pelvis does not attain
that complete development which fits it for the process of parturition
until toward the age of twenty, whilst puberty occurs at the age
of sixteen. “A girl of ten is capable of aspiring to play the part of
a woman, but not before the age of sixteen is she fitted to play that
part, nor indeed fitted to become a mother before the age of twenty.”
In general, we may say, regarding the women of our own part
of the world, that in those who are healthy, who lead a regular
life, are well fed, free from the pressure of anxieties, with their
sexual functions sufficiently exercised, the duration of the sexual
life is longer than in women whose circumstances are the reverse
of those just enumerated. It is a sign of decadence when women of
the well-to-do classes, leading a life of ease, manifest a diminished
duration of the sexual life. The greatest physical power and the
highest ethical development are associated with a lengthening of
life in general, and associated also with a lengthening alike in the
sexual life of woman and the sexual potency of man. A decline in
morals and culture entails a diminution of sexual vital capacity,
this being true alike of individuals, of families, and of nations.
Woman is venerated and valued the more, the longer the duration
of her sexual life; a woman in whom the sexual life is short quickly
loses value and significance, both in domestic and in social circles.
The social significance of the sexual life of woman is disproportionately
greater and farther reaching than the sexuality of the male,
as the former is concerned with the fundamental principles of human
social life, influencing the constitution of the family, and controlling
the good of the coming race. Sexual purity, which to the youth is a
romantic dream, is to the maiden a vital condition of existence; adultery,
in the husband a pardonable transgression, is in the wife an
overwhelming sin committed against family life. To the freedom
of the male in affairs of love is opposed the strict restraint of the
female, based on monogamic marriage. The sexual needs and
desires of the female are transformed in an ideal manner by means
of the feeling of duty of the wife and mother; the violent pressure
of the sexual impulse is restrained by the opposition of ethical
forces. When this restraint fails, the running off the rails that ensues
has a far profounder influence in the case of the female than
34of the male, an influence not limited to her own personality, but
dragging down the whole family into the abyss of consequences,
into the depths of moral and physical destruction.
Though in nature everywhere the same, the sexual life of woman
exhibits in the various gradations of social life different outward
manifestations, from the brutal sexual congress that does not greatly
shun publicity, to the modern would-be philosophical free love. And
throughout all variations the two darkest points remain, the illegitimate
child and venereal infection, both of which entail upon the
woman the most unspeakable anxieties and the greatest possible
misery, whilst the man who is in either case to blame passes comparatively
unscathed.
The social sexual position of woman suffers most at the present
day from the mature age at which under existing social conditions
men are alone able to marry and from the ever-increasing number of
cases of venereal infection. In both these directions social science
and medical skill must work hand in hand for the amelioration of
the sexual life of woman.
On the twentieth century falls the duty of furnishing a solution
for these problems. Contesting voices are heard on all sides. Tolstoi’s
rigid demand for complete sexual abstinence, the exhortation
of the professors of the German universities to their students in
favor of moral purity, the associations for the official prevention
of venereal diseases, the agitation among young men in favor of
abstinence from sexual intercourse before marriage, finally, the
clamorous voices of the supporters of women’s rights—all these
are influences within the sphere of sexual morality, which must lead
slowly but surely to extensive social changes in the sexual life of
women.
The discussion of the sexual life of woman, which for many
centuries was concealed by a thick veil from the eyes of the profane,
or was viewed only through the frosted glass of poetical metaphor,
has in recent times assumed a quite revolting character. Not only
have the acquired liberties and the social aims of the present day
a tendency to give to women in general a freer and higher position,
to emancipate them from the bonds in which owing to the conditions
of family life they have so long been shackled, but some members
of the women’s rights party go even farther, and demand for
women greater freedom in the sphere of sexual activity.
With this end in view the sexual life of woman is used as the fulcrum
of the lever, and is withdrawn from the twilight into the
open light of day, or indeed too often into a dazzling and altogether
false illumination. Women writers especially, who have hitherto
been accustomed to delude themselves and the world with sensational
35representations of the feminine soul, of feminine modesty,
and the fineness of feminine sensibility in matters sexual, now find
their greatest joy in unveiling themselves and their sisters before
the face of all the world, and in discussing in the plainest language
the most intimate processes of the genital organs. In writings
exhibiting but little good taste, though all the more temperament,
they emphasize again and again one side only of the sexual life,
to wit, the sexual impulse, the force of which is intentionally exaggerated
to a high degree, so that it is described as a mighty current
of passion, which may with great pains be held in check for a
season, but must ultimately break loose, and with devastating rage
must overwhelm everything which has hitherto been regarded as
discipline and good morals. Young girls, even, step down into the
arena to take part in the contest concerning the reform that is
to take place in the relations between men and women. Especially
sensational in this connection was Eine für Viele. Aus dem Tagebuche
eines Mädchens von Vera,[18] a book which, totally ignoring
the biological differentiation of the sexes and their diverse sociological
course of development, goes so far as to insist that from the
man entering upon marriage, as from the woman, sexual purity
and virginity are to be demanded. (The heroine of the book commits
suicide because her lover has in earlier years had experience of
sexual intercourse.)
From a mistaken standpoint other supporters of women’s rights
oppose the ideal method in sex-relations, life-long monogamy, and
the ideal of sexual sensibility, motherhood, and they put forward
quite new sexual pretensions on behalf of women, as belonging to
them by natural right. Upon these pretensions it is the duty of
physicians, who truly know and truly prize womanhood, to pass their
judgment, and that judgment, which will find ample justification
in the ensuing descriptions of the individual phases of the sexual life
of woman, is that the modern movement on behalf of the emancipation
of women goes much too far. We do not, however, mean to
imply that this movement is totally unjustified.
The growing girl must not, as has hitherto been the case, be kept
in a state of ignorance (which is indeed in most cases apparent
merely) regarding the sexual processes of her own body, she must
no longer, when she asks to be informed concerning these matters,
be put off with conventional lies and prevarication. But her enlightenment
must not be effected in such a manner as to lead to
excitement and excessive stimulation, to the awakening of slumbering
feelings, and to the conversion of fantasy into a devouring
flame. Sexual enlightenment must not be made an excuse for the
36unchaining of sensibility. When about to be married, a woman
should certainly be instructed regarding her sexual duties and
rights, and enter as one well informed into the act in which she is
to play a leading part. But she ought not, with the excessive
valuation of herself attained in recent times, to regard the man
as her enemy, as one whom she is always justified in fighting and
always ready to fight with the equal weapons of sexual transgression.
It cannot be doubted that the ideal of “pure marriage” at
an early age is one greatly to be prized as the foundation of a
powerful future generation; but the real nature of the male must
not be overlooked, nor must his sexual honor be put to too difficult
a test. We regard as reasonable the modern demand of woman
that in marriage her individuality should not be buried, and that
space should be given for the development of her personality; but
every sober-minded person will reject the “moral demand” for
“ideal passion” in accordance with “entire mutual freedom” in
the sexual relation between man and wife, and will regard such
free love as social insanity and as a barbaric retrogression toward
the rude sexual habits of savage peoples. Further, in view of the
continually increasing intensity of the struggle for existence and in
view of the difficulties of the task of rearing children, we cannot
fail to recognize that it is not right for women to be overburdened
with the task of reproduction, and that she does not live simply
and solely for the bearing of children—but those rush to the other
extreme who undervalue motherhood and the duties of maternity,
who speak scornfully of the woman who is “a mother, and a
mother only,” who despise women whom they regard merely as
“means for the production of children,” and who employ all possible
methods to free women from the pressing claims of nature and
of society.
In all social circumstances, and in all times the great principle of
sexual morality must dominate the sexual life of woman. As the
ethical characteristics of the three great epochs in that sexual life
we recognize the purity of the maiden, the faithfulness of the wife,
and the love of the mother. But within the limits imposed by these
demands it is still possible to satisfy the modern claim for a free
development of the personality, and to accommodate the circumstances
of the sexual life to the individual vital needs and vital
claims of the present day.
37
I. THE SEXUAL EPOCH OF THE MENARCHE.
The term menarche (μήν, a month, ἀρχή, the beginning) was
introduced by me into medical literature to denote the period of
life in which, as a sign of puberty, menstruation first makes its appearance.
The age at which this occurs is subject to variations depending
upon race, occupation, hereditary tendencies, and climate; but in
Germany and Austria the average age at puberty is 14 or 15, the
extreme limits being 12 to 19.
Until about the age of 13, the physical differentiation of the
sexes, except for the anatomical peculiarities of the genital organs,
is in our climates a trifling one. But at puberty the important
changes occur by which the sexes are so strikingly differentiated.
Whereas in the growing boy all physical change takes the form
of increasing strength and energy, in the development of the girl,
we note the appearances of the rounded outlines so characteristic
of womanhood. At the same time the voice alters, becoming less
sharp, with a softer quality, and yet a fuller tone; and we may
observe that young brunettes have commonly a contralto voice,
young blondes, more often a soprano. The intellectual changes undergone
by the girl at puberty are no less extensive and characteristic
than the physical changes. In brief, the undifferentiated, neuter
girl is transformed into a young woman, endowed with all the attributes,
mental and bodily, characteristic of femininity.
As regards the age at which the menarche usually occurs, and
the manner in which its occurrence is anticipated or retarded by the
various influences already mentioned, the following propositions may
be put forward, based on the available statistics and observations:
1. Climate is an important factor. In the torrid zone, menstruation
appears at a very early age, on the average from 11 to 14; in
the temperate zone, it appears later, on the average from the age of
13 to 16; in the frigid zone, later still, on the average from the age
of 15 to 18. The mean temperature of the atmosphere appears to
have a direct influence on the age at which menstruation begins,
the hotter the climate, the earlier being the menarche. The height
of the place of residence above the sea level and its distance from
the coast also have a certain influence.
382. Race and constitution have a distinct influence upon the age
at which menstruation makes its appearance. In women of the
Semitic races the menarche occurs earlier than in women of the
Aryan races. The average age at which menstruation begins is
in Jewish girls, from 14 to 15; in Magyar girls from 15 to 16; in
German girls from 16 to 16½; and in Slavonic girls from 16 to 17.
In general the menarche is earlier in girls of a sanguine, lively
temperament and a powerful constitution than in girls of a phlegmatic
temperament and a weakly constitution; further, other things
being equal, menstruation appears earlier in brunettes, girls with
black hair, thick skin, dark eyes, and a dark complexion, than it appears
in blondes, girls with light hair, thin skin, blue eyes, and a fair
complexion.
3. The age at which menstruation begins is also affected by the
conditions of life and the social circumstances. In the higher
circles of society, in the upper, well-to-do classes, menstruation
appears earlier than among women of the laboring classes, who
are compelled to strive for their daily bread. Amongst upper-class
girls the menarche occurs at the age of 14 in one-fourth of
their number, whereas among lower-class girls barely one-sixth
begin to menstruate at the age of 14.
In large towns, again, menstruation appears earlier than in small
towns, whilst in the open country the menarche is still further delayed.
In the women of Paris the average age at the menarche is
14 years and 6 months, in the women of smaller French towns it is
14 years and 9 months, in French countrywomen it is 14 years and
10 months.
How far the mode of nutrition is concerned in the production of
these results is not yet determined.
4. The time of the menarche appears to be influenced by inheritance
to this extent, that the daughters of women who began to
menstruate early begin themselves to menstruate at an early age,
whereas in other families we observe that both mothers and
daughters began to menstruate late. But this relation is by no
means a constant one.
Ploss has collected observations made in various countries and
towns regarding the age at which menstruation begins, and the
mean results of these observations are given below.
The average age at which menstruation began was:
| In Swedish Lapland |
18 years, |
0 months, |
0 days. |
| In Christiania |
16 years, |
9 months, |
25 days. |
| In Copenhagen |
16 years, |
9 months, |
12 days. |
| In Munich |
16 years, |
5 months, |
12 days. |
| In Göttingen |
16 years, |
2 months, |
2 days. |
| In Vienna |
15 years, |
8 months, |
15 days. |
| In Berlin |
15 years, |
7 months, |
6 days. |
| 39In Stockholm |
15 years, |
6 months, |
22 days. |
| In Manchester |
15 years, |
6 months, |
0 days. |
| In Warsaw |
15 years, |
1 month, |
23 days. |
| In London, between |
15 years, |
1 month, |
4 days. |
| and |
14 years, |
9 months, |
9 days. |
| In Paris, between |
15 years, |
7 months, |
18 days. |
| and |
14 years, |
5 months, |
17 days. |
| In Madeira |
14 years, |
3 months, |
0 days. |
| In Montpellier |
14 years, |
2 months, |
0 days. |
| In Corfu |
14 years, |
0 months, |
0 days. |
| In Marseilles |
13 years, |
11 months, |
11 days. |
| In Calcutta |
12 years, |
6 months, |
0 days. |
| In Egypt |
10 years, |
0 months, |
0 days. |
The collective results of the investigations of French authors
regarding the average age at which menstruation first appears are
given in the following table:
| I. In Temperate Climates: |
|---|
| |
| Observer. |
Place. |
No. of Cases. |
Average Age. |
| |
| De Soye |
Paris |
1,000 |
15 years, |
0 months. |
| Dubois |
Paris |
600 |
15 years, |
3 months. |
| Raciborski |
Paris |
200 |
14 years, |
5 months. |
| M. Despines |
Paris |
85 |
14 years, |
11 months. |
| Arau |
Paris |
100 |
15 years, |
4 months. |
| Courty |
Montpellier |
600 |
14 years, |
3 months. |
| Puech |
Nîmes |
941 |
14 years, |
2 months. |
| M. Despines |
Toulon |
43 |
14 years, |
1 month. |
| M. Despines |
Marseilles |
25 |
14 years, |
1 month. |
| Puech |
Toulon |
144 |
14 years, |
1 month. |
| Grey |
London |
1,498 |
15 years, |
6 months. |
| Lee & Murphy |
London |
1,719 |
15 years, |
6 month |
| Torisiano |
Corfu |
33 |
14 years, |
6 months. |
| Lebrun |
Warsaw |
100 |
15 years, |
1 month. |
from these observations we obtain an average of 15 years.
| II. In Cold Climates: |
|---|
| |
| Observer. |
Place. |
No. of Cases. |
Average Age. |
| |
| Ravn |
Copenhagen |
3,840 |
16 years, |
9 months. |
| Frugel |
Christiania |
157 |
16 years, |
6 months. |
| Dubois |
Russia |
600 |
16 years, |
8 months. |
| Faye |
Norway |
100 |
15 years, |
6 months. |
| Lundborg |
Esquimaux |
16 |
15 years, |
6 months. |
| Wistrand |
Stockholm |
100 |
15 years, |
7 months. |
from these observations we obtain an average of 16 years and 3
months.
| III. In Hot Climates: |
|---|
| |
| Observer. |
Place. |
No. of Cases. |
Average Age. |
| |
| Goodeve |
Calcutta |
239 |
12 years, |
5 months. |
| Lith |
Deccan |
217 |
13 years, |
5 months. |
| Robertson |
Calcutta |
540 |
12 years, |
6 months. |
| Webb |
Calcutta |
39 |
12 years, |
5 months. |
| Dubois |
Asia |
600 |
12 years, |
11 months. |
from these observations we obtain an average of 12 years and 7
months.
40In 6,550 cases collected by Krieger menstruation first appeared:
| At the age of: |
|---|
| |
| 9 years in |
1 instance. |
| 10 years in |
7 instances. |
| 11 years in |
43 instances. |
| 12 years in |
184 instances. |
| 13 years in |
605 instances. |
| 14 years in |
1193 instances. |
| 15 years in |
1240 instances. |
| 16 years in |
1026 instances. |
| 17 years in |
758 instances. |
| 18 years in |
582 instances. |
| 19 years in |
425 instances. |
| 20 years in |
281 instances. |
| 21 years in |
111 instances. |
| 22 years in |
55 instances. |
| 23 years in |
15 instances. |
| 24 years in |
15 instances. |
| 25 years in |
1 instance. |
| 26 years in |
4 instances. |
| 27 years in |
2 instances. |
| 28 years in |
1 instance. |
| 29 years in |
1 instance. |
From these figures it appears that in the 6,550 cases under consideration,
the age 15 was that at which the first appearance of
menstruation was most frequently observed, namely in 1,240
instances, or 18.9 per cent. The age 14 comes next, with
1,193 instances, or 18.2 per cent. The case in this series in which
menstruation appeared earliest, namely in the ninth year, was observed
by Mayer, the girl being a blonde of average height, good
family, and German descent; the case in which menstruation
appeared latest, namely in the twenty-ninth year, was that of a
woman living in Berlin, who was sickly and chlorotic up to the
time of her marriage, and in whom menstruation did not appear
until some years after that event.
As regards climatic influences, all the data at our disposal prove
that the hotter the climate the earlier the menarche. According
to Marc d’Espine the age at puberty varies in an almost geometrical
ratio with the mean annual temperature.
The dependence of the menarche upon climatic influences is
clearly shown by the statistical data collected from various regions
of the world. We append the general compilation of Gebhard
dealing with this question.
A. Europe.
For Europe the data furnished by Ploss are grouped by Gebhard
in the following manner.
1. Northern Europe.
The average age at which menstruation first appears, according
to the older statistics, is in Swedish Lapland 18, in Norway, 16.12.
In Copenhagen it is 16.75, in St. Petersburg 14.5.
More recent statistics for Finland are furnished by Engström.
41Among 3,500 women of pure Finnish descent, he found that menstruation
began:
| At the age of: |
|---|
| |
| 8 years in |
2 instances. |
| 9 years in |
2 instances. |
| 10 years in |
4 instances. |
| 11 years in |
41 instances. |
| 12 years in |
178 instances. |
| 13 years in |
458 instances. |
| 14 years in |
715 instances. |
| 15 years in |
778 instances. |
| 16 years in |
614 instances. |
| 17 years in |
369 instances. |
| 18 years in |
195 instances. |
| 19 years in |
91 instances. |
| 20 years in |
31 instances. |
| 21 years in |
8 instances. |
| 22 years in |
10 instances. |
| 23 years in |
2 instances. |
| 24 years in |
1 instance. |
| 25 years in |
0 instance. |
| 26 years in |
1 instance. |
Thus, in nearly half of all Finnish women, menstruation begins
with the completion of the fourteenth and fifteenth years. The
statistics include women of all classes of society.
At the Pirogoff Congress Grusdeff furnished particulars of the
first onset of menstruation in Russia among 10,000 women. Menstruation
began:
| At the age of: |
|---|
| |
| 9 years in |
1 instance. |
| 10 years in |
4 instances. |
| 11 years in |
31 instances. |
| 12 years in |
244 instances. |
| 13 years in |
864 instances. |
| 14 years in |
1641 instances. |
| 15 years in |
1795 instances. |
| 16 years in |
2012 instances. |
| 17 years in |
1692 instances. |
| 18 years in |
910 instances. |
| 19 years in |
498 instances. |
| 20 years in |
183 instances. |
| 21 years in |
65 instances. |
| 22 years in |
19 instances. |
| 23 years in |
5 instances. |
| 24 years in |
3 instances. |
| 32 years in |
1 instance. |
In women of German race living in Russia puberty was earliest,
occurring at the average age of 15.16 years; in Finnish women
it was latest, occurring at the average age of 16.17 years.
2. Middle Europe.
In Germany, according to the tables of Krieger and L. Mayer,
who have recorded 11,500 cases in all, menstruation begins most
commonly (in 18.931 per cent. of the cases) at the age of 15; the
next most frequent age is 14 (18.213 per cent. of the cases).
For Berlin, in a number of cases collected from the lower classes
of society, we find the average age for the first appearance of menstruation
to be 16.18 years.
Notwithstanding the more northerly situation of Berlin, the
average age at puberty is somewhat less than in Munich, situated
4½ degrees to the southward, for the reason that the retardation dependent
upon altitude makes itself manifest in the latter town, which
is situate about 500 metres (1,640 feet) higher above the sea level.
Whereas in Berlin 18 per cent. of all cases begin to menstruate at
the age of 14, and 19 per cent. at the age of 15, in Munich the two
42leading years are 15 with a percentage of 17½, and 16 with a percentage
of 18¾.
In Great Britain, according to Krieger, the average age at which
menstruation begins is 15 years, 1 month, and 5 days. For Manchester
the age given is 15 years, 6 months, and 23 days. In France,
according to the calculation of Brierre de Boismont, the most frequent
age for the first onset of menstruation is 16. In Paris the
average age is 14 years, 6 months, and 14 days. Bohemia, Upper
and Lower Austria, and Moravia have an average age of 16 years
and 2 to 3 months.
3. Southern Europe.
In Southern Europe the influence of the higher mean temperature
manifests itself. The average age at which Spanish girls begin
to menstruate is 12. In Northern and Middle Italy the most frequent
age is 14; in Southern Italy, 13. In Lyons the average age
at which menstruation begins is 14 years, 5 months, and 29 days;
in Marseilles and Toulon it is 13 years and 10 months. For Hungary,
Doktor gives the statistics of 9,600 cases. In 22⅓ per cent.
menstruation began at the age of 15; in 20½ per cent. at the age of
16, and in 10 per cent. at the age of 17. The earliest age among
these cases was 8 years; the latest, 33 years. (The latter must no
doubt be regarded as pathological.)
B. Asia.
In Palestine puberty most commonly occurs at the age of 13;
in Turkey even as early as 10. Rouvier calculated the average of
742 cases observed in Syria to be the age of 12. As regards Persian
women, the data vary between the age of 14 for the northern part
of the country and the age of 9 or 10 for the southern. According
to Joubert’s data in 46.4 per cent. of the indigens of India, menstruation
begins at the age of 12 or 13. Similar figures are given for
Ceylon and for Siam. In Japan menstruation most frequently begins
at the age of 14, sometimes as early as 13; mothers of 15 are
by no means rarities in this country, but for menstruation to begin
before the age of 12 is considered a very exceptional occurrence.
According to a table dealing with 584 women of Tokio menstruation began:
| At the age of: |
|---|
| |
| 11 years in |
2 instances. |
| 12 years in |
2 instances. |
| 13 years in |
26 instances. |
| 14 years in |
78 instances. |
| 15 years in |
224 instances. |
| 16 years in |
228 instances. |
| 17 years in |
68 instances. |
| 18 years in |
44 instances. |
| 19 years in |
10 instances. |
| 20 years in |
2 instances. |
The data available regarding China are so exceedingly variable
that little importance can be attached to them.
43
C. Africa, Oceania, and America.
The average age at which menstruation begins in the negro
women of Africa is from 10 to 13. In Algeria puberty occurs at
9 or 10 years. Among the Australian indigens, menstruation commonly
begins as early as 8 years, and at the very latest at the age
of 12 years. The data available concerning the indigens of the
Oceanic Archipelago are extremely variable and inexact, but we
cannot go far astray in stating the age of puberty among these to
be from 10 to 13. In tropical South America girls begin to
menstruate from the age of 9 to 14 years. The Indian women of
North America begin to menstruate at the ages of 12, 13, 14, or
even as late as 18 or 20. In the Arctic zone of North America and
in Greenland the onset of menstruation is delayed till 17 and even
till 23 years.
As regards the position in life and the upbringing years it has been
shown by numerous observers that among the well-to-do classes,
whose mode of living is luxurious, and whose social circumstances
allow free play to the imagination, menstruation begins at an earlier
age than among the working classes, whose life is one of want and
privation. According to the statistical data of Mayer’s regarding
6,000 women, menstruation began:
|
In women of the upper classes. |
In women of the lower classes. |
| At the age of 13 years |
11.73 per cent. |
7.06 per cent. |
| At the age of 14 years |
23.90 per cent. |
13.33 per cent. |
| At the age of 15 years |
22.83 per cent. |
14.56 per cent. |
| At the age of 16 years |
14.10 per cent. |
16.53 per cent. |
| At the age of 17 years |
9.60 per cent. |
13.33 per cent. |
From this table we learn that in nearly one-fourth of the girls
of the upper classes puberty occurs at the age of 14, whilst in girls
of the lower classes barely one-sixth begin to menstruate at this
age. The average age at the first menstruation in girls belonging to
the upper classes is seen to be 14.69 years, but in girls belonging
to the lower classes, 16.00 years. According to other observers the
average age at the first menstruation is:
|
Brierre de Boismont. (Paris.) |
Tilt. (London.) |
Krieger. (Berlin.) |
Ravn. (Copenhagen.) |
| Amongst gentle folk and the rich |
13y. 8m. |
13y. 5½m. |
14y. 1m. |
14y. 3m. |
| Amongst the well-to-do middle classes |
14y. 5m. |
14y. 3½m. |
15y. 5m. |
15y. 5½m. |
| Amongst the lower classes |
14y. 10m. |
|
16y. 8m. |
16y. 5½m. |
Comparative observations on women living in towns and women
44living in the country show also that in the former, menstruation
begins on the average at an earlier age. According to Brierre de
Boismont, the average age at the first menstruation is:
| In Paris |
14 years, |
6 months. |
| In small towns |
14 years, |
9 months. |
| In country districts |
14 years, |
10 months. |
Similarly it was found by Ravn that menstruation first occurred:
| In Copenhagen at the average age of |
15 years, 7 months. |
| In industrial towns |
15 years, 4 months. |
| In country districts |
16 years, 5 months. |
Mayer states that the average age at which the first menstruation
occurs is:
| In townswomen |
15.98 years. |
| In countrywomen |
15.20 years. |
In Italy, according to Calderini, in a thousand instances, menstruation
begins at the age of 14 in 280, at the age of 15 in 219, at the
age of 13 in 205, at the age of 12 in 116, at the age of 16 in 89, at
the age of 17 in 55, at the age of 18 in 14, at the age of 11 in 7, at
the age of 10 in 6, and at the age of 20 in 6 instances. In girls attending
town schools, the first menstruation most commonly occurs
in the months of June and August; but in girls attending
country schools most commonly in the spring months.
A certain hereditary predisposition is so far determinant in the
matter of the early or late onset of the first menstruation, that
from a knowledge of the age at which menstruation began in the
mother, we are able with great probability to predict the age at
which it will begin in the daughter. Among fifty cases which I investigated
with this point in view, I found forty-one in which the
daughters of mothers who had begun to menstruate early began
themselves to menstruate early, usually indeed in about the same
year of life; or conversely that when the mother had begun to
menstruate late, late onset of menstruation was usually to be observed
in the daughter also. Tilt relates a case in which a woman
began to menstruate at the age of fourteen, and her daughter and
granddaughter both began to menstruate at the same age. Courty
observed a mother who began to menstruate at the age of eleven,
and whose eight daughters all began to menstruate at the same age.
Gynecologists agree in stating that girls of sanguine temperament
and powerful constitution begin to menstruate earlier than weakly
and phlegmatic individuals. Tilt describes a peculiar ovarian temperament,
in which menstruation begins early; such women have
as a rule striking nervous sensibilities, with a dark complexion and
glistening, longing eyes, always surrounded by dark rings.
45The opinion is general that in girls with black hair, dark eyes,
thick skin, and dark complexion, menstruation begins earlier than
in blondes with blue eyes and delicate white skin. Brierre de Boismont
states in this connection that not fair hair only, but also chestnut-tinted
locks, indicate a late onset of menstruation. L. Mayer
found that:
| Of blondes. |
Of brunettes. |
|
|
| |
| 17.20 per cent. |
18.84 per cent. |
began to menstruate at the age of |
14 |
| 16.89 per cent. |
18.02 per cent. |
began to menstruate at the age of |
15 |
| 15.14 per cent. |
16.59 per cent. |
began to menstruate at the age of |
16 |
According to the same author, the average age at which menstruation
begins is:
| In blondes |
15.55 years. |
| In brunettes |
15.26 years. |
As regards race, it is well known that in Jewesses menstruation
begins at an early age. According to Joachim the age of puberty
varies very greatly among the different races inhabiting Hungary.
The first menstruation appears:
| In Slavonic girls between the ages of |
16 and 17 |
| In Magyar |
15 and 16 |
| In Jewish |
14 and 15 |
| In Styrian |
13 and 14 |
First Appearance of Menstruation.
The first appearance of menstruation is commonly preceded by
various symptoms dependent on the increased flow of blood to the
genital organs. Such symptoms are: Sacrache; dragging sensation
in the loins; an indefinite feeling of pressure in the lower part
of the belly, especially in the region of the uterus and the ovaries,
which region is sometimes also tender on pressure; a slight feeling
of weariness in the lower extremities; sudden flushings or pallors;
alternating sensations of heat and chilliness, sometimes accompanied
by actual though slight change of temperature. In many cases also
there are disturbances in the intestinal evacuations and urinary secretion,
in the process of cutaneous transpiration, and in the functional
activity of the gastro-intestinal canal. A frequently observed
symptom is an increased irritability of the entire nervous system,
with an inclination to melancholy and indefinite amorous desires—symptoms
which Tilt denotes by the term “ovarianismus,” Emmet
by the term “erection,” Lecal by the term “phlogose
amoureuse,” and the older writers by the term “molimina menstrualia.”
The nervous irritability manifests itself already before the appearance
of the menstrual flow by headache and moodiness, weariness,
46nervous irritability, and low spirits; further, by slight changes
in the facial aspect, dark rings round the eyes, spontaneous blushing,
uneasy sensations, epigastric pain, loss of appetite, a sensation of
pressure in the abdomen, palpitation, vertigo, dragging sensations
passing from the loins to the thighs, feeling of weakness and
numbness in the lower extremities—symptoms which often endure
for several months and in such cases tend to lower the resisting
powers of the organism.
Courty enumerates as prodromal symptoms which are observed
in the majority of girls before the first appearance of menstruation:
swelling and tenderness of the breasts, sensation of fulness and
weight in the hypogastric region, moderate intestinal meteorism,
sacrache, aqueo-mucous vaginal discharge, finally, an itching sensation
in the genital organs. These manifestations may also assume
a morbid character, taking the form of violent abdominal and
lumbo-sacral pain, general fatigue and weakness, dyspepsia and
diarrhœa, cephalalgia, various kinds of neuralgia, some degree of
moral aberration. After the first menstruation, two or three months
may elapse before the girl menstruates again, but after the lapse of
a year the flow usually recurs at quite regular periods. Sometimes
the early periods are very violent and recur very frequently, every
twenty days, for instance.
The greatest increase in size and weight occurs in the female
sex at the time of the menarche. Amongst the poorer classes the
greatest development in size and strength occurs between the ages
of 13 and 15 years, whereas in the upper classes of society, those
who ultimately attain the same weight exhibit their greatest growth
at the ages of 12, 13, and 14 years. According to Pagliani the
greatest growth in the female sex always precedes puberty, so that
for example a girl who begins to menstruate at the age of 12 will
grow most rapidly in the year preceding this, whereas a girl who begins
to menstruate at a more advanced age will not undergo her most
rapid phase of growth so early as the age of 11. According to
the observations of Bowditch, A. Hey, Lombroso, Pagliani, and
Ploss, up to the age of 11 or 12 years the growth of girls exceeds
that of boys, but whereas in girls growth ceases suddenly at the age
of 14, in boys growth proceeds regularly up to the age of 16 years.
At birth boys are on the average 1 cm. (⅖″) longer than girls;
but during puberty the female sex catches up the male in height,
or even surpasses it. According to Ploss, a girl of 16 or 17 years
is as tall as a young man of 18 or 19 years.
The earlier development of the female as compared with the
male at the time of puberty is a constant phenomenon, to be observed
in all races, in every climate, and in all strata of society.
47According to the statistical data published by the authors just
quoted, the age of greatest development in the respective sexes is:
|
In the female. |
In the male. |
| |
| As regards weight at the age of |
12 to 14 years. |
14 to 17 years. |
| As regards height at the age of |
12 to 13 years. |
12 to 15 years. |
| As regards respiratory capacity at the age of |
12 to 15 years. |
15 to 17 years. |
| As regards muscular strength at the age of |
12 to 14 years. |
14 to 15 years. |
Puberty occurs in the female on the average about two years
earlier than in the male, and upon this difference the observed differences
in growth also depend.
The menarche in the wider signification of the term includes the
development which occurs at the time of puberty, and continues
through a period of several months, and even years, before complete
sexual maturity is attained; and includes also the time, which may
be considerable, following the first appearance of the menses and
before the regular rhythm of the menstrual function is established
and the full development of the female genital organs is attained.
This time, which forms a notable phase of the sexual life
of woman, is characterized by great changes in the genital organs
and in the vital processes connected therewith, by a strong tendency
to suffer from a series of very various pathological changes and
disorders of function in the principal organs, and a lessened general
resisting power to disease—a change which finds its most definite
expression in the well-established fact that in this period of life
the mortality among females is much greater than among males of
corresponding age. According to the statistical data of Quetelet
and Smits, from the age of 14 to the age of 18 (the period of the
menarche) there are 128 deaths of females for every 100 deaths of
males; and even in the four succeeding years, from the age of 18
to the age of 22, the unfavorable conditions peculiar to sex are
witnessed by 105 deaths of females to every 100 deaths of males.
Many authors draw a distinction between the age of puberty
(from the Latin pubes, puberis), when the growth of the pubic hair
occurs as an external sign of sexual development, and the age of
nubility (from the Latin nubere), when the individual becomes
fitted for marriage. The distinction is a partial one only, inasmuch
as capacity for copulation is attained already at puberty. The law,
however, maintains such a distinction, the Austrian Penal Code,
for example, regarding intercourse with a female less than fourteen
years old as rape, and the German Code likewise punishing
carnal knowledge of a girl under fourteen.
The signs of puberty in girls were noticed and explained in very
early times. From the anthropological studies of Ploss and Bartels
we take the following data regarding this matter. In the Bible we
read (Ezekiel, xvi, 7): “Thy breasts are fashioned and thine hair
48is grown, whereas thou wast naked and bare.” The early Indian
physician, Susruta, refers only to the regular recurrence of menstruation
as a sign of puberty. That a woman is menstruating may
be known by the fact that her face is swollen and bright. In the
Roman Empire Justinian ordained that all young women should be
examined as to the growth or absence of the pubic hair in order to
ascertain if they were ripe for marriage. The early Chinese physicians
recorded that in every woman at the age of fourteen or fifteen
years a monthly flow of blood from the genital organs began,
the period of recurrence being thirty days. The physicians of the
Talmud express themselves variously regarding puberty in women.
In one place they advance as a sign of puberty the growth of the
hair on the genital organs; in another they speak of the notable enlargement
of the breasts, and mention as a sign of more complete
sexual development that the nipples become elastic. Other Talmudists
refer to the appearance of a dark brown coloration in the
areola and to the enlargement of the mons Veneris as signs of
puberty. Savage races regard the first appearance of the menstrual
flow as the only certain sign of puberty, and among many such
races this is the occasion of peculiar ceremonial rites. The attainment
of puberty in savage tribes is often solemnized by the seclusion
of the girls from the time of the first menstruation; they fast during
the period of seclusion, which sometimes terminates in an elaborate
ritual of purification.
For two reasons in particular, the period of the menarche is a
time of storm and stress to women, first on account of the developmental
processes in the genital organs, and secondly on account
of the intellectual changes that occur at this period.
The local cause is to be found in the extensive transformation of
the ovaries and the uterus, by means of which a peculiar and powerful
stimulus, the menstrual stimulus, is elaborated, which has a reflex
influence upon heart and brain, vascular and nervous systems,
and secretory and nutritive processes. Since we know that in every
premenstrual period by the growth of the follicles hyperæmia is
excited in the ovary, by means of which the liquor folliculi is increased
in amount, we can well understand that at the time of the
menarche the ripening of the graafian follicles is accompanied by a
considerable degree of hyperæmia of the ovaries and of the whole of
the genital organs, now undergoing their fullest development, and
we can easily see how this hyperæmia may result in manifold reflex
disturbances. But in addition to these reflex disturbances, we have
once more to take into consideration the as yet imperfectly known
chemical processes which are associated with the ripening and development
of the graafian follicles, and an abnormal course of
49which may give rise to a disordered constitution of the blood, manifesting
itself as chlorosis or in other ways. In connection with the
growth and ripening of the ova, extensive and novel demands are
made on the organism, and these may well endanger metabolic
processes which are not established on a very secure foundation.
The other cause is to be found in the intellectual processes which
occur at this time in the youthfully receptive, highly sensitive
organ of mind, the brain. The girl growing into womanhood, who
with astonishment and stress has witnessed the visible changes in
her body, the outward signs of puberty, as they gradually make
their appearance, receives powerful psychical stimulation which
cannot fail to exercise an influence upon the entire nervous system
and its complex interlacements, alike in the sensory and in the
motor sphere.
The degree to which these influences radiating from the genital
organs make themselves manifest is chiefly dependent upon the
resisting power of the nervous system as a whole, upon the temperament,
the inherited constitution, and the mode of education of
the young girl. In children belonging to families noted for sensibility
and irritability, in dwellers in large cities who have attended
high schools for girls and have at an early age lifted the veil that
covers the sexual processes, the reflex disturbances of the
menarche will be more manifold and will manifest themselves with
greater intensity than in children brought up in country districts,
whose sensibilities are chiefly physical and whose mind is less
susceptible to the influence of external stimuli.
A further important consideration is the time at which the
menarche occurs, and whether on the one hand it is at or near
the average age, or whether on the other, as precocious menstruation,
it is unusually early, anticipating the general bodily development,
or again as retarded menstruation it is unduly delayed. In
some cases of retarded menstruation, the external genital organs
are thoroughly well developed, and it is menstruation only that
remains in abeyance; but in other cases the external genitals are
also backward in development, the pubes and mons Veneris being
but sparsely supplied with hair, and the breasts remaining very
small.
In addition to these abnormal temporal relations of the menarche,
certain other irregularities at the commencement of menstruation
are worthy of note. Thus, the first menstruation may
be normal, but thereafter amenorrhœa may persist for several
months, or if the flow occurs it may be exceedingly scanty, or very
pale in color; on the other hand, menstruation may be very profuse,
lasting many days.
50The environment in which the young girl is placed during the
period of her sexual development has a great influence on the processes
of the sexual life and on the pathological disturbances that
affect these processes.
In working-class families the immoderate physical strain often
thrown upon girls, in many cases continuous movements of the
upper extremities whilst the lower extremities and the pelvis are
absolutely quiescent, or conversely, an excessive employment of
the muscles of the lower extremities—these circumstances in conjunction
with insufficient nutriment, night-work, association when
at work with persons of the opposite sex, and the frequent premature
sexual stimulation, will combine to have a most deleterious
effect.
Amongst country-folk, indeed, the girl has the enjoyment of
fresh air, and as a rule nutritive food, moreover, there are not so
many occasions of nervous stimulation; puberty therefore arrives
more slowly and gives rise to less disturbance; but the ignorance
of the girls very frequently leads to an early experience of coition,
the natural and unnatural consequences of which have then to be
taken into account.
Amongst the better classes of townspeople such hygienic regulations
and educational measures are in common employment that
young girls during the years of development usually receive reasonable
care and attention—but very frequently, intercourse with
older girls, association with young men, visits to theatres, evening-parties,
and balls, and the perusal of stimulating literature, form
unfavorable features of urban life which exercise their inevitable
effects in the sexual sphere. In some cases, fortunately sufficiently
rare, the stimulation of the sexual impulse and the longing
for its satisfaction are so intense, that a kind of demi-vierge is
brought into being, a young woman who is concerned only to
preserve the physical token of virginity, but whose thoughts and
fancies are anything but maidenly. It is to be feared that in consequence
of the excessive freedom in education and the emancipated
independence of feminine youth, these “half-virgins” are
increasing both in number and in intensity, a fact which cannot
fail to increase also the number of sexual maladies and perversions.
Anatomical Changes in the Female Genital Organs in the Period of the Menarche.
The female reproductive organs, which in childhood were in a
comparatively quiescent state, now become powerfully active, as is
witnessed by the changes that occur in the external genitals.
51The soft, hairless vulva of the child becomes enlarged at the
time of the menarche by the deposit of fat, and its substance becomes
tough and elastic. Some time before puberty, fine, pale
hairs make their appearance here and there, but not until puberty
does the hairy covering of the pubic region become more or less
thick. The growth of the denser pubic hair begins with the appearance
of hairs along the middle of the mons Veneris and at the
margins of the labia majora. Early sexual development is commonly
indicated by an early and thick growth of the pubic hair.
In the virgin this hair is smoother and less curly than in the later
course of the sexual life. In certain tribes of negroes it is the
custom for the young unmarried girls to shave off the pubic hair,
which is not allowed to grow freely until after marriage. In some
of the tribes of South Sea Islanders it is customary at puberty to
tattoo the external genitals and the surrounding skin.
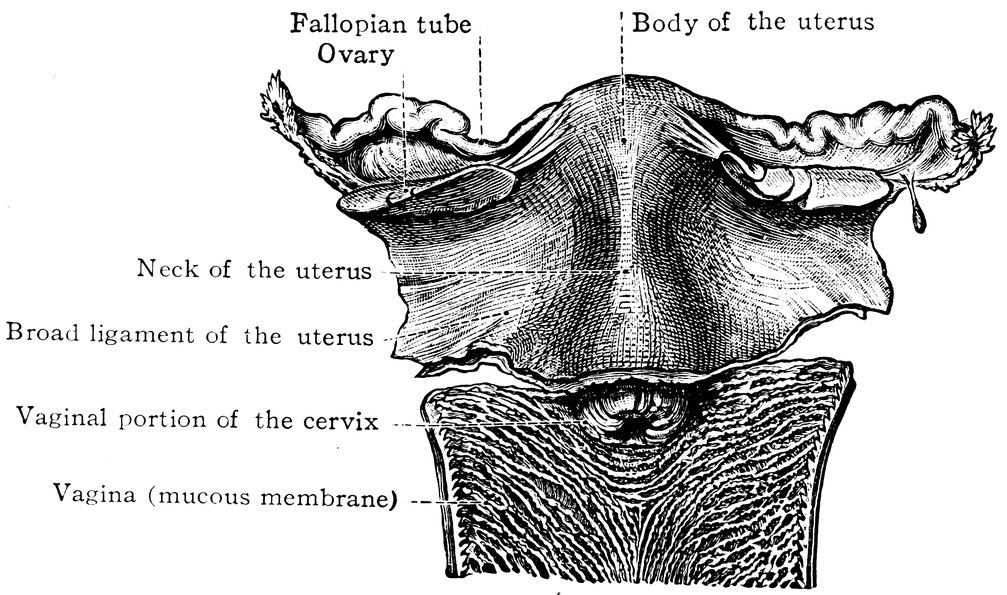
Fig. 8.—Internal genital organs of a new-born, powerfully developed female infant. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
In young virgins the rima urogenitalis or vulval cleft is closed
by the accurate opposition of the labia majora; the labia minora or
nymphæ are delicate in texture, rose-red in color, hairless, free
from fat, and completely covered by the labia majora; whilst the
clitoris is likewise concealed. The sebaceous glands of the labia
minora secrete a smegma which collects especially around the
glans clitoridis, and as it undergoes decomposition diffuses a
peculiar odor, resembling that of old cheese. A wing-like elongation
of the labia minora in young girls, with free secretion and a
generally moist appearance, leads to a suspicion of the practice of
52masturbation. In the virgin the orifice of the vagina is covered by
the hymen.
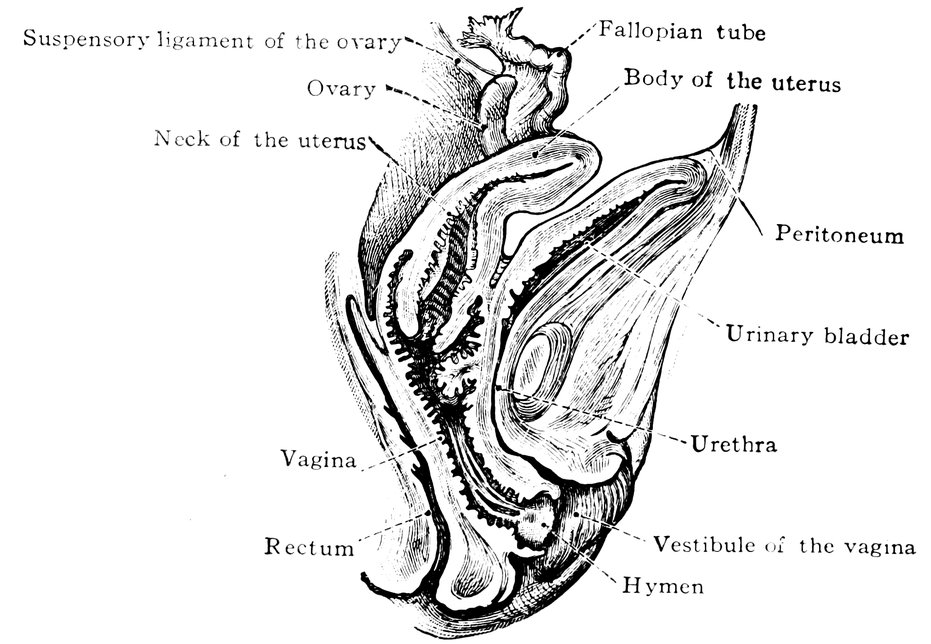
Fig. 9.—Reproductive organs of a new-born, powerfully developed female infant in median sagittal section. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
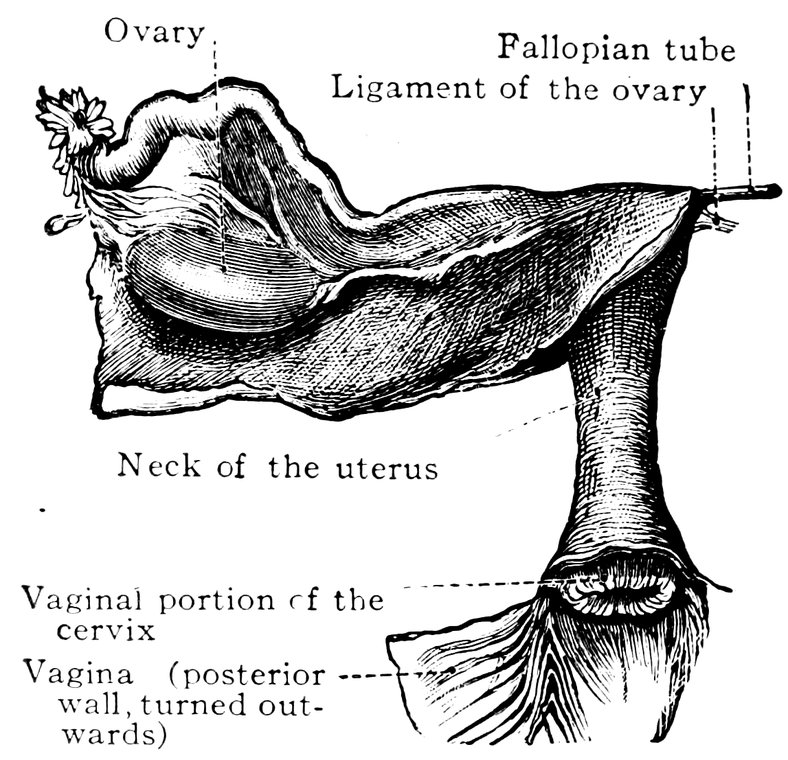
Fig. 10.—Internal genital organs of a girl aged eight years. Seen from behind. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
The entrance to the vagina in the virgin is rounded, the posterior
border of the aperture being deeply concave, whilst the anterior
border is often slightly convex backwards. Where this feature is
53strongly marked, the orifice has a semilunar shape. The posterior
concave border projects forward in the form of a fold, continuous
above with the posterior vaginal wall; this fold is the hymen.
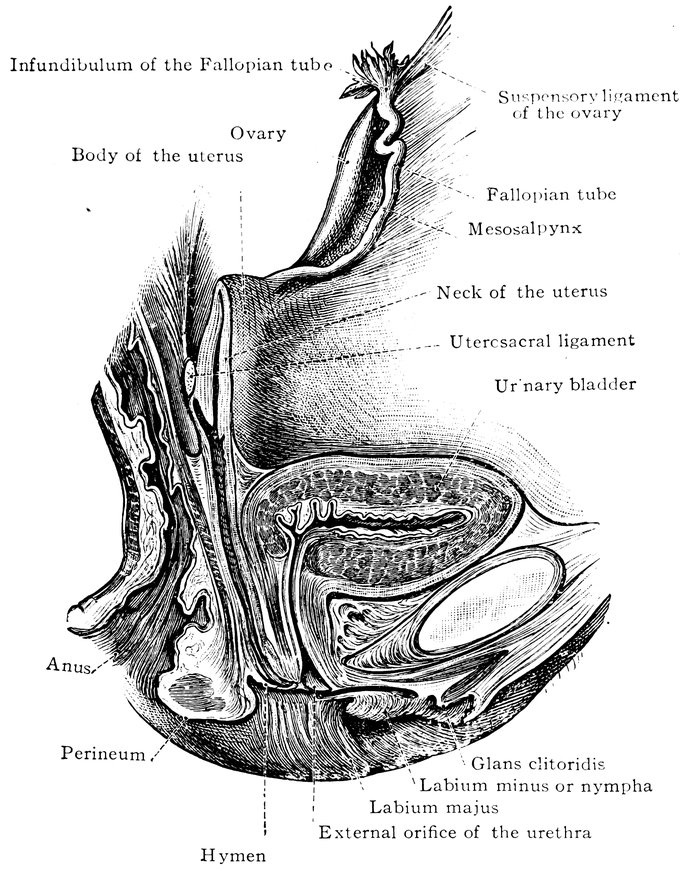
Fig. 11.—Reproductive organs of a girl aged ten years in median sagittal section. Left half. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
54
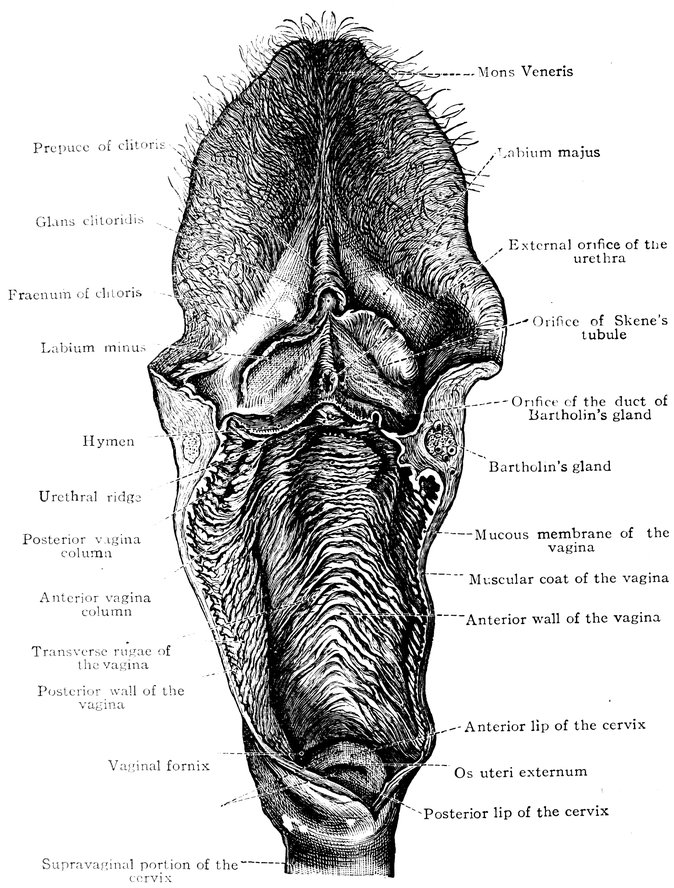
Fig. 12.—Female external genital organs of a virgin, attached to the vagina which has been isolated and opened, and a portion of the cervix uteri, Hymen, etc. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
55
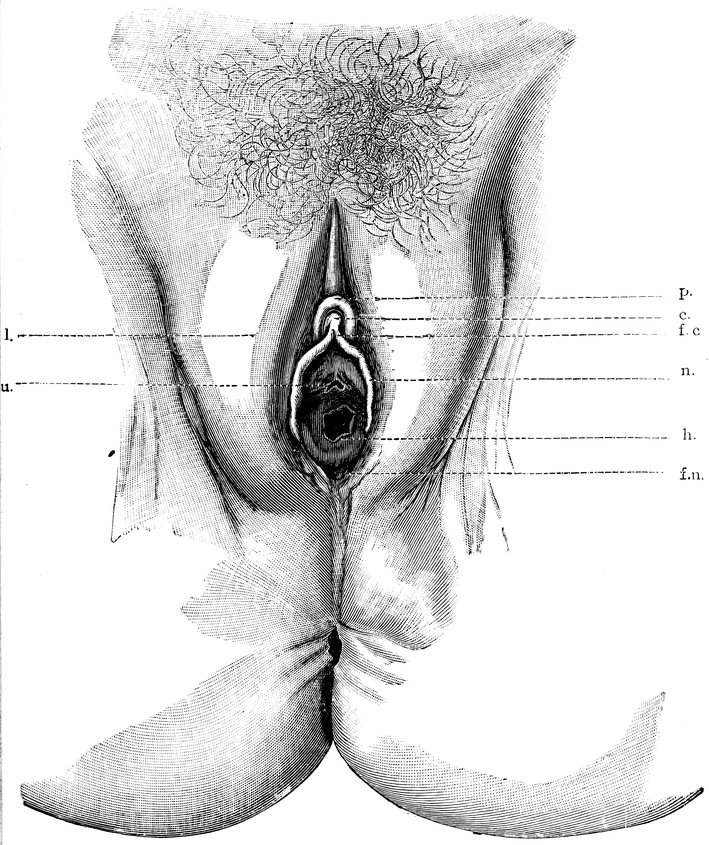
Fig. 13.—The external genital organs of a virgin, drawn apart transversely (after von Preuschen). c. Clitoris. f. c. Frænum of the clitoris. n. Nymphæ. l. Labia majora. o. u. Urethral orifice. h. Hymen. f. n. Fossa navicularis.
56The infantile uterus is so proportioned that its neck (collum vel
cervix uteri) constitutes the larger part of the organ, as much
indeed as two-thirds. Owing to the small size of the body (corpus
uteri), the whole uterus is very flat, and its borders ascend in a
direction almost parallel to each other, diverging somewhat
abruptly into the Fallopian tubes, recalling in some degree the two-horned
embryonic form of the organ (uterus bicornis). The plicæ
palmatæ on the surface of the cervical canal, which make up the
arbor vitæ uterina, are strongly developed; the median longitudinal
ridge bifurcates, and its divisions can be traced on either side
into the uterine orifice of the Fallopian tube (ostium uterinum
tubæ). The lips of the vaginal portion of the cervix are comparatively
speaking very large and terminate in sharp angles. The
vaginal mucous membrane is everywhere beset with long papillæ.
The development of the uterus shortly before puberty consists
chiefly in the enlargement of the body of the uterus, and the growth
of its walls in thickness.
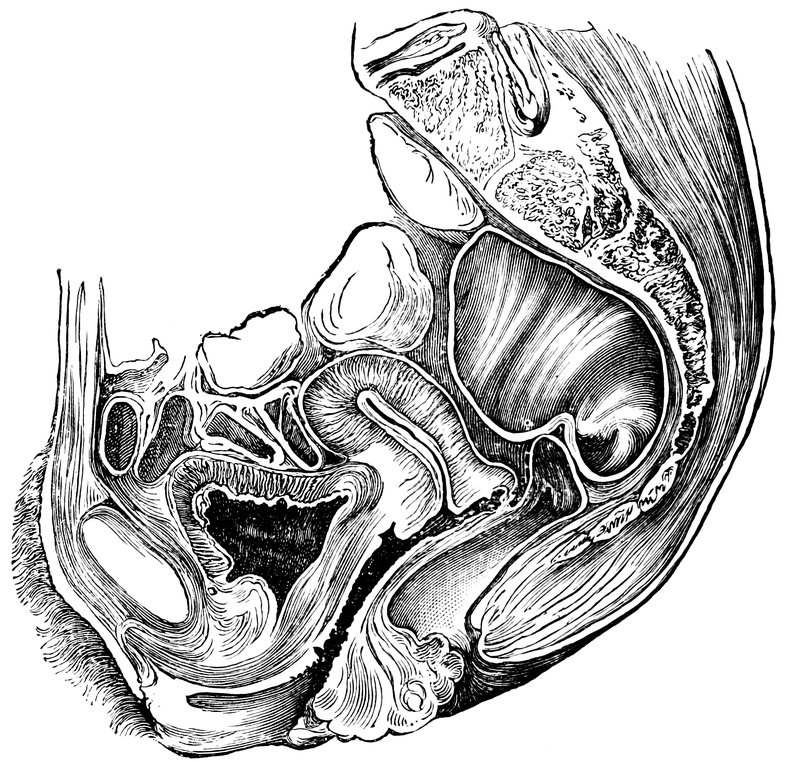
Fig. 14.—Sagittal section of the female pelvis (after Breiolei).
At the time of puberty, according to Toldt, the body of the uterus
in the virgin has already increased till its length is half that of the
entire organ; and at the first appearance of menstruation the body
and neck of the virgin uterus are nearly equal, with perhaps a
slight preponderance in size of the cervix, and the walls of the
uterus have become convex. In consequence of this change the
organ becomes pear-shaped, and the uterine cavity (cavum uteri)
assumes the form of a triangle with moderately incurved sides. The
cervical canal becomes wider in the middle; the margin of the os
uteri becomes smooth and rounded. The walls of the virgin vagina
57are marked with numerous dentate transverse ridges (rugæ),
especially near the lower end and on the anterior walls, the columns
of the vagina (columnæ rugarum), from which the transverse ridges
run to either side at right angles, extend half way up the vagina,
and are of a hard consistence.
The characteristic changes in the ovary at the time of the menarche
originate in the changes undergone by the ovarian follicles. A
large number of small separate follicles is to be found already in
the ovary of the new-born infant. These structures, known as primitive
follicles, are formed by detachment from the egg-tubes that
grow down into the stroma from the superficial germinal epithelium;
they are spheroidal vesicles, enveloped by a single layer of cubical
cells, and their interior is entirely filled by the primitive ovum or
egg-cell. This latter consists of very finely granulated protoplasm
with spherical nucleus and distinct nucleolus, but no trace of an
investing membrane can as yet be discerned. The further development
of the ovarian follicles takes according to Toldt the following
course: A rapid multiplication of the cubical cells that form the
wall of the follicle occurs, so that the ovum is surrounded by two,
three, or several layers of cubical or rounded cells, and the whole
follicle gradually increases in size. At the same time the ovum
assumes an eccentric position in the interior of the follicle. At or
near the middle of the follicle a slit-shaped space now appears,
filled with a clear colorless fluid. As this space gradually enlarges,
the follicle[19] becomes converted into a vesicle filled with fluid, the
wall of which is composed of small cubical cells. Simultaneously
with the growth of the follicle a lamination of the elements of the
surrounding stroma takes place, so that a somewhat sharply defined
capsule is formed. In this condition these glandular structures of
the ovary are known as graafian follicles.[19]
Before puberty, these graafian follicles are small vesicles of a
diameter of one to two millimetres, containing the large unicellular
ova. Each of these consists of an envelope, the zona pellucida (also
known as the zona radiata, or striated membrane of the ovum); an
external granular mass of protoplasm, the vitellus or yolk; a vesicular,
spherical nucleus, the germinal vesicle; and a nucleolus, which
if single is large and prominent, the macula germinativa or germinal
spot. As early as the second year of infancy every imaginable
intermediate stage between the primitive follicle and the fully-developed
vesicular graafian follicle can be observed.
58At the time of puberty certain larger follicles are always to be distinguished,
which have moved inward toward the interior layers
of the ovary, whereas the smaller follicles have a more peripheral
situation; thus, according to Waldeyer, we observe at this time in
a section of the ovary, proceeding from without inward, first the
epithelium, next the fibrous tunic, next the zone of younger follicles,
and finally the zone of older follicles. According to Henle and
Waldeyer, at the commencement of puberty, there are in each ovary
about 36,000 ova, giving a total for the two of 72,000.
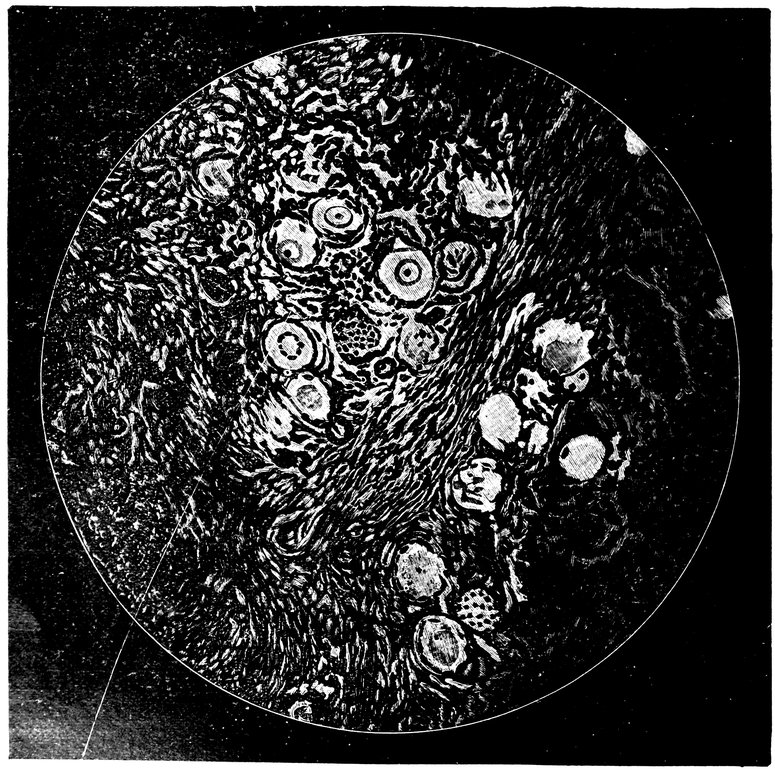
Fig. 15.—Primitive follicles.
In the further course of development of the graafian follicles at
this period, the most advanced now reapproach the surface of the
ovary, so that a fully-matured follicle comes to occupy almost the
entire thickness of the cortical substance, and may even give rise
to a localized bulging of the surface of the organ. In such a mature
follicle, which has attained nearly the size of a pea, we recognize
an outermost connective-tissue investment (theca folliculi), consisting
59of condensed ovarian stroma, in which two layers are distinguished,
sometimes called simply outer tunic and inner tunic, sometimes
known by the names of tunica fibrosa (outer) and tunica propria
(inner), respectively; within this is the cellular layer known
as the membrana granulosa (or stratum granulosum), the portion
of which, now greatly enlarged, immediately surrounding the ovum
is known as the discus proligerus (or cumulus oöphorus); the interspace
between the discus proligerus and the membrana granulosa is
filled with a clear fluid, the liquor folliculi. In consequence of the
continued increase in its fluid contents, the graafian follicle ultimately
bursts along the most prominent portion of the superficial
wall, and the ovum passes out through the rupture, finding its way
under normal conditions into the Fallopian tube and through this
into the uterus. The follicle itself then undergoes a regressive
metamorphosis, forming the corpus luteum, the rent in the envelope
of which, after the absorption of the yellowish semi-fluid contents,
undergoes cicatrization. Contemporaneously with this development
at puberty of the process of ovulation, menstruation also for the
first time makes its appearance, recurring thenceforward at four-weekly
intervals as the regular catamenial discharge.
We append the account given by Pfannenstiel regarding the
ovarian follicles. He writes: “In correspondence with the especial
function of the female reproductive gland, which is to bring to maturity
and to evacuate only after the lapse of a considerable period
and at successive intervals, the ova which it has contained from the
very outset, we find that primitive follicles continue to exist in the
ovary up to the very end of the period of sexual activity, though
naturally in diminishing numbers; and the size and shape of these
primitive follicles remain nearly identical throughout the various
periods of life. As the follicle ripens, the epithelium grows, the cells
becoming cubical with a rounded nucleus, and increasing in number
by cell-division, so that several layers are formed. As soon as these
layers are three or four in number, a space, at first slit-shaped, forms
in the epithelium on the peripheral surface of the ovum; this space
is filled with fluid, known as the liquor folliculi; the peripheral
layer of cells, the membrana granulosa, is thus separated from the
mass of epithelial cells immediately enveloping the ovum, the discus
proligerus, which is situate in the side of the follicle adjacent to
the hilum of the ovary. By the increase of the liquor folliculi the
graafian follicle is formed, a vesicle the envelope of which is formed
by the multilaminar membrana granulosa, whilst in the pole of the
vesicle directed toward the hilum ovarii is the ovum imbedded in
the mass of cells forming the discus proligerus, a mass which has
the form of a truncated cone. The liquor folliculi is formed by
60the epithelium, the nuclei of which disappear by chromatolysis or
by simple atrophy whilst the cell-bodies liquefy in consequence
of albuminous, not fatty, degeneration (Schottländer). Within the
epithelium of the follicle we find the faintly glistening epithelial
vacuoles of Fleming, likewise cells which liquefy and assist in increasing
the bulk of the liquor folliculi. This liquor is a thin, serous
fluid, and contains albumin. * * * Every graafian follicle has a
bilaminar investing membrane, which is formed by the ovarian
stroma. * * * The ovum of the growing follicle increases in
size very slowly indeed, attaining on the average, according to
Nagel, a diameter of 165 to 170 µ, it retains its zona pellucida,
the greater part of the protoplasm of the cell is transformed into
deutoplasm (food-yolk, or yolk-granules), the nucleus assumes an
eccentric position. Between the zona pellucida and the cell-body
a narrow perivitelline space appears. The ovum is then full-grown,
but not yet fully prepared for fertilization; for this, maturation is
required, certain changes in the germinal vesicle, which occur after
the bursting of the follicle. * * * As a rule each follicle contains
a single ovum. But two and even three ova have beyond doubt been
observed in one follicle.”
According to Waldeyer, the bursting of the follicle is not to be
regarded as dependent upon a sudden rise of pressure in its interior,
but as the result of a gradual ripening process. At the deepest
pole of the follicle, which in the course of its development has
now approached the surface of the ovary, an exuberant growth takes
place in the internal layer (tunica propria) of the theca folliculi,
with a profuse formation of new vessels. Here numerous “epithelioid”
cells, the “lutein-cells,” make their appearance. In consequence
of this proliferation of the lutein-cells, the contents of the
follicle are gradually pressed toward the “stigma,” the superficial
pole of the follicle, and the follicle itself is pushed toward the surface
until it finally comes into contact with the germinal epithelium.
Meanwhile the follicular epithelium undergoes fatty degeneration,
alike in the membrana granulosa and in the discus proligerus. In
consequence of the proliferation of the lutein-cells, on the one hand,
and the fatty degeneration of the epithelium, on the other, the follicle
opens at its weakest point, the stigma, and the ovum is extruded,
with the liquor folliculi, and a number of cells belonging to the
follicular epithelium. (To illustrate these changes we have borrowed
Figs. 15, 16, and 17 from the monograph, by Pfannenstiel on
Diseases of the Ovary, in J. Veits’ Handbook of Gynecology.)
The ovaries, which in the new-born female infant are flattened,
ribbon-like bodies one-half to one centimeter (0.2 to 0.4″) in length,
and in childhood are cylindrical, with a perfectly smooth surface,
61assume at the time of puberty a more or less flattened form. During
the menarche they have an elongated oval shape, flattened from
side to side, their average length being 2.5 to 5.0 centimetres (1 to
2″), width 1.5 to 3.0 centimetres (0.59 to 1.18″), thickness 0.6 to
1.4 centimetres (0.24 to 0.55″), weight 5 to 8 grammes (77 to 123
grains). After the repeated occurrence of ovulation, the surface of
the ovary becomes more and more uneven, being thickly covered
with fossæ or scar-like fissures.
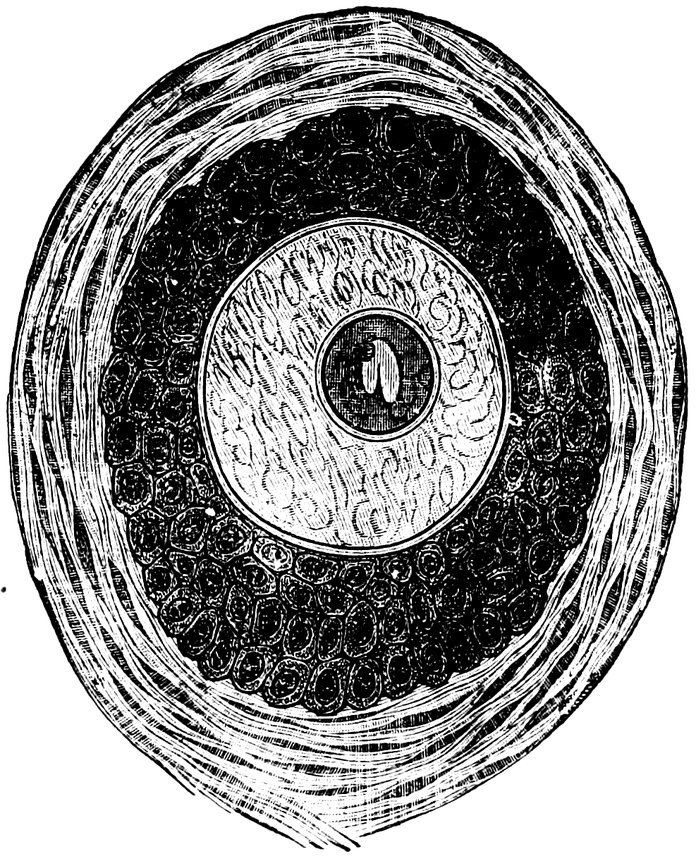
Fig. 16.—Ripening follicles.
The vagina during virgin girlhood is narrow, and its mucous
surface is beset with numerous rugæ, which may be plainly felt as
well as seen. The calibre of the vagina is proportionately less the
younger the girl. The examining finger is gripped by the vaginal
wall as by an india-rubber tube (Maschka). The vaginal portion
of the cervix is felt in the form of a truncated cone, with a smooth
surface, rather dense in consistence; the external os opens at the
bottom of a small depression on its surface, in the form of a short
oval, the long axis of which is transversely directed. Shortly before
the menarche, Bartholin’s glands become noticeable on either side
of the lower end of the vagina between the sphincter muscles.
The clitoris in many cases attains a very large size, and this is apt
to lead to sexual malpractices. According to Hyrtl, in southern
countries the clitoris is larger than in temperate and cold climates.
In the women of Abyssinia and among the Mandingoes and the
Ibboes, the size is portentous, and amongst the first-named, circumcision
of females is a customary operation. It is said that female
slaves belonging to these races are greatly esteemed by the
62ladies of the harem, and are eagerly sought for. In the anatomicopathological
museum at Prague there is a preparation of the female
genital organs with a clitoris as large as the penis of a full-grown
man.
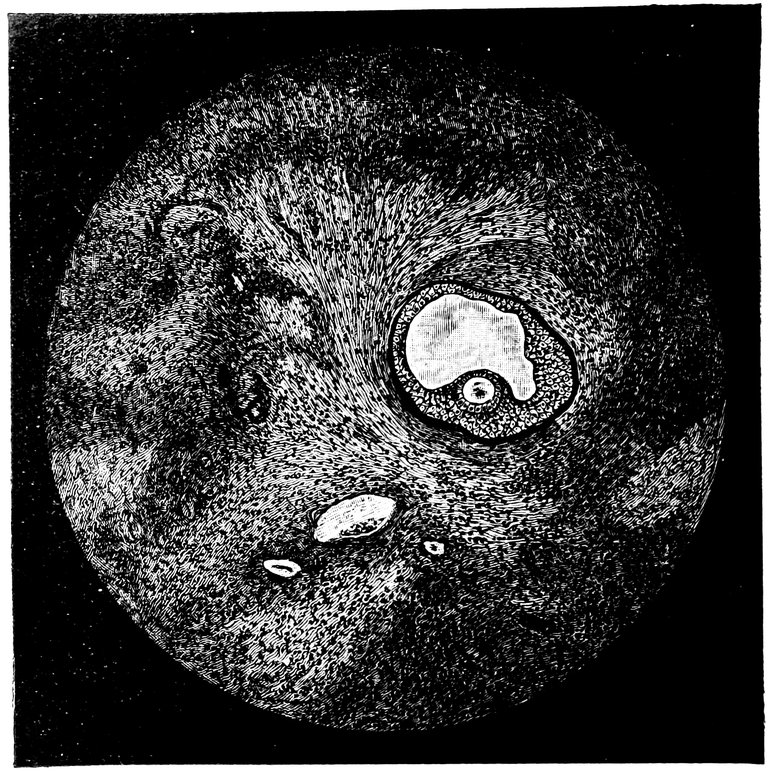
Fig. 17.—Graafian follicles.
Sonini describes “as peculiar to women of Egyptian or Koptic
descent, the presence of a thick, fleshy, but soft and pendent outgrowth
in the pubic region, completely covered with hair,” which
he compares to the hanging caruncle on the bill of the male turkey.
This appendage becomes thicker and longer with advancing years.
Sonini found such an appendage one-half inch in length in a girl of
eight years, one of more than four inches in a woman of twenty to
twenty-five years. Circumcision in girls consists in the removal of
this outgrowth, which hinders copulation; in that part of the world
the operation is usually effected in the seventh or eighth year, just
before puberty.
The circumcision of girls as practiced by Mahommedan peoples
in Africa is said by Ploss and Bartels to consist in abscission of the
labia minora, the clitoris, and the præputium clitoridis. Brehm is
of opinion that the object of the operation is to diminish the intensity
of the sexual impulse, so overpowering among these races;
but others believe that the great enlargement of the clitoris and the
63labia minora usual in those countries is regarded as a serious defect
in beauty, a defect removed by the operation; whilst others again
hold that the circumcision is required for the removal of the hindrance
to copulation presented by the abnormally large clitoris.
Closely related to the operation of circumcision in females, according
to Ploss and Bartels, is the custom peculiar to Africa of infibulation,
wherein, after a preliminary cutting operation like that for circumcision,
the fresh wound surfaces are brought into accurate opposition,
either by sutures or by appropriate bandages, so that when
cicatrization occurs the vulval cleft is closed except for a very small
aperture. The object of infibulation is to enforce on girls complete
abstinence from sexual intercourse. (Before marriage, the vulval
cleft is reopened to an extent corresponding with the size of the
genital organs of the future husband; and when pregnancy occurs,
the opening is still further enlarged before parturition; but after
that event, the wound surfaces are refreshed, and the whole opening
is once more closed). On the other hand, in many savage tribes,
elongation of the labia minora and the clitoris is artificially undertaken
from the earliest years of girlhood, this elongation being regarded
as a beauty.
The parts of the external reproductive organs of the female concerned
in sexual sensation, first described as such by Kobelt,
are already fully developed at the time of the menarche. Of these
parts a small portion only, the glans clitoridis, is visible externally,
surrounded by the præputium clitoridis, a prolongation of the labia
minora, which passes round the front of the clitoris, and sends
from each side a fine process behind the glans to become attached to
its under surface, forming the frænum of the clitoris. The erectile
apparatus of the external genitals is formed by the corpora cavernosa
clitoridis. As two delicately constructed trabecular masses of
erectile tissue, the crura of the clitoris, these are attached on either
side to the inferior or descending rami of the pubic bones; at first
passing upwards parallel to the bones, they subsequently curve downward
as they converge and unite to form the body of the clitoris;
these masses of erectile tissue embrace the sides and the front of
the lower extremity of the vagina. This erectile apparatus, when
the supply of arterial blood is greatly accelerated and at the same
time the outflow of venous blood is diminished, becomes distended
with blood, enlarged and stiffened; the process of erection plays an
important part, as we shall explain more fully later, in the production
of sexual excitement and sexual pleasure during the act of
copulation.
In the virgin and in the earlier phases of the sexual life, the
hymen is so characteristic an organ that its more minute description
would seem desirable.
64The hymen, a fold of mucous membrane, springing from the
periphery of the vaginal orifice, separates as a perforated diaphragm
the vagina from the vulva. Between the two epithelial layers of
which, as a fold of mucous membrane, the hymen consists, is a supporting
layer of connective tissue of variable strength; in other respects
the mucous membrane of the hymen has the same structure
as the mucous membrane of the vagina. On its inner surface the
rugæ and folds of the vaginal mucous membrane are prolonged.
The shape of the hymen is very variable; most commonly its
aperture is more or less central, so that the hymen has a ringed or
semilunar shape.
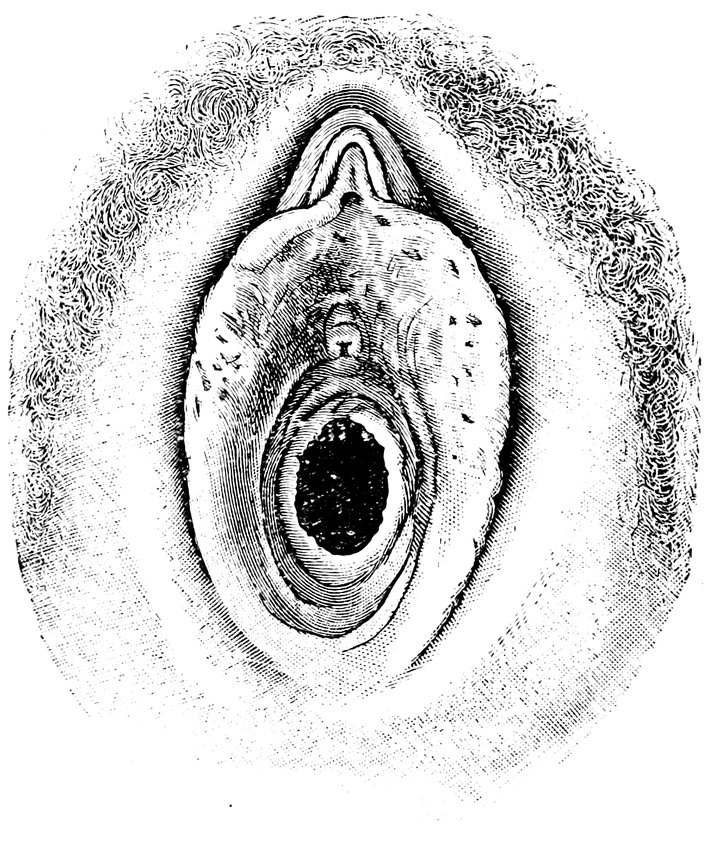

In the new-born female infant, the hymen has the appearance of
a tubular stopper closing the lower end of the vagina; according to
Dohrn it exhibits as a rule one of three typical forms: Hymen
annularis, denticulatus, et linguiformis; the annular, the denticulate,
and the linguiform (or linguliform) hymen. The transverse ridges
on the inner surface of the hymen, prolongations of the rugose
columns of the vagina, are strongly developed. During the girl’s
further growth, in association with the enlargement of the vagina,
the hymen undergoes important changes in form and structure.
Its border becomes thinner and more tense; and in the virgin at the
time of the menarche, the annular hymen is the fundamental type,
subject, however, to extensive variations. In most cases, at any
rate, the aperture in the hymen is more or less centrally situated;
very commonly, however, this opening is crescentic, when we have a
65semilunar hymen, the height of the border posteriorly being much
greater than anteriorly. The consistency of the hymen, its extensibility,
and its thickness, are as variable as its shape.
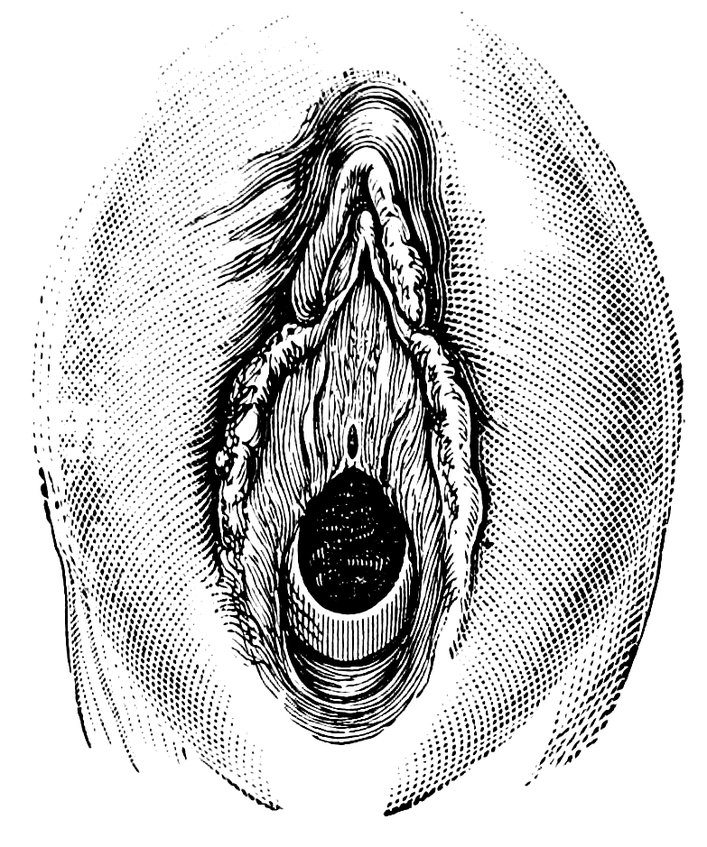
Fig. 20.—Semilunar Hymen.
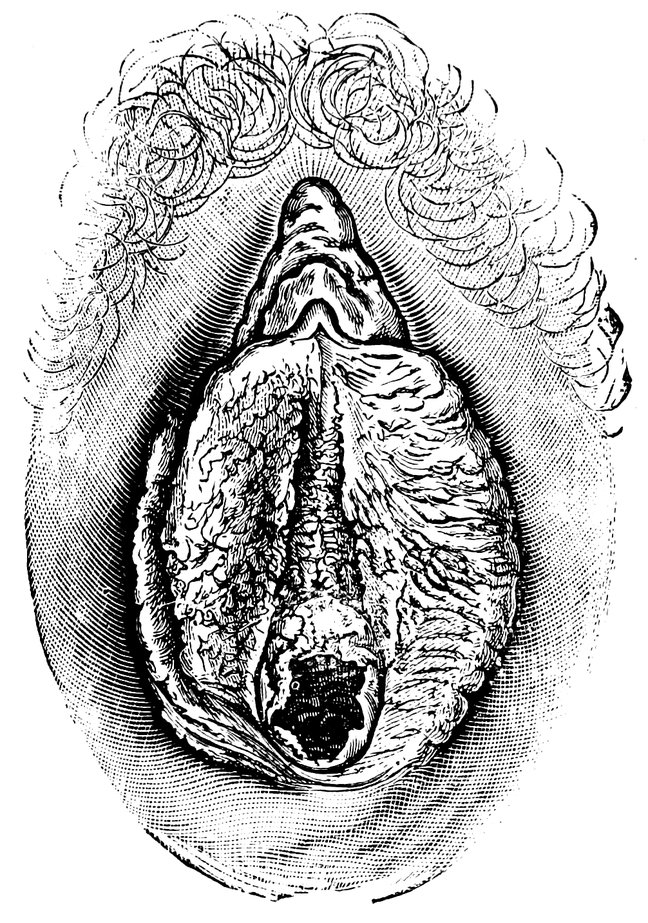
Fig. 21.—Annular Hymen with congenital Symmetrical Indentations.
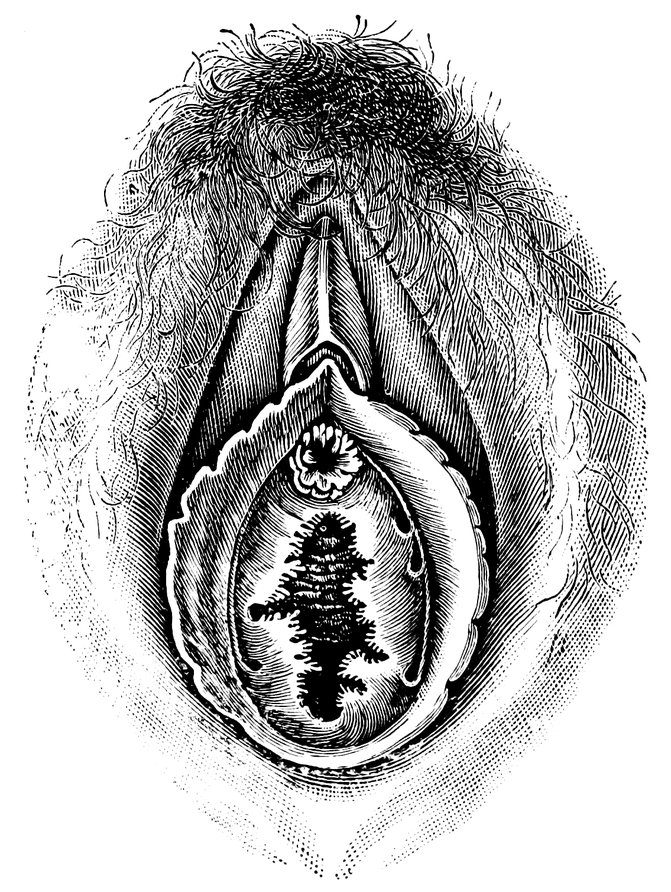
Fig. 22.—Fimbriate Hymen.
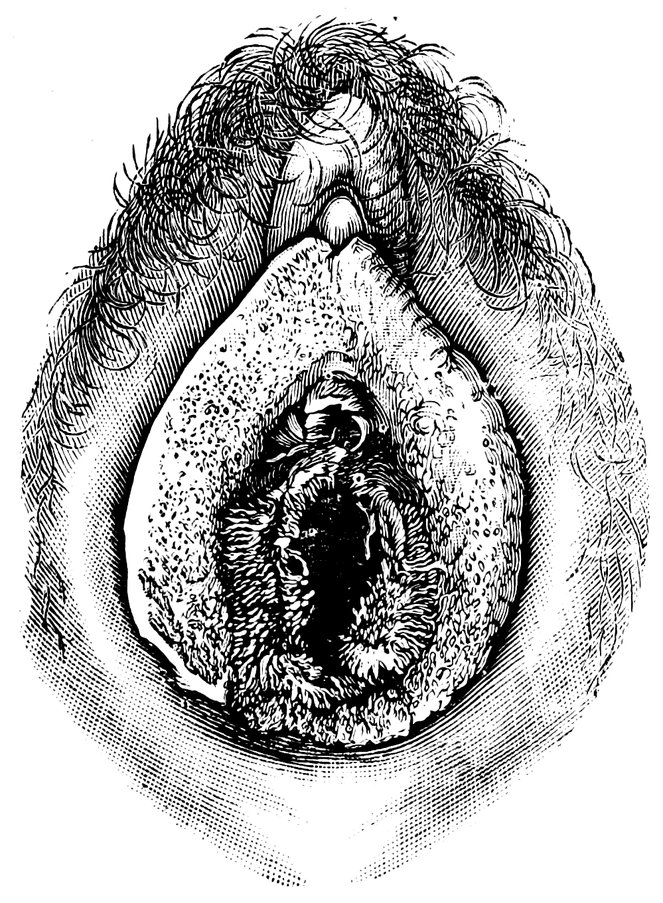
Fig. 23.—Deflorated Fimbriate Hymen.
In the normal position of the reproductive organs the hymen
has very rarely the appearance of a tense membrane; as a rule it
66is folded up, and becomes plainly manifest only when the genital
organs are stretched. The margin of the hymeneal aperture, as a
close examination shows, is sometimes sharp and regular, sometimes
lobulated, with small congenital notches. These congenital notches
are to be distinguished from the lacerations resulting from defloration
by the fact that the former have a smooth border, which is of
the same consistency as the general substance of the hymen. In some
instances the border of the aperture in the hymen is beset with small,
fine villi (villous hymen).
The common varieties of the hymen are thus classified by
Maschka:
1. The annular hymen, in which the membrane when stretched is
seen to have a rounded aperture, which may be central or eccentric;
very often, indeed, the aperture is more toward the upper half of
the hymen, in which case it is not always circular, but frequently
rather ovoid in shape.
2. The semilunar or crescentic hymen, in which the aperture is
eccentrically placed in the upper half of the membrane, in such
a manner that the hymen exhibits a wide surface below the aperture,
which surface narrows at either side as it passes upwards until it
disappears, the two sides failing to reunite above the aperture.
3. The heart-shaped or cordiform hymen, the general shape of
which may be circular, ovoid, or even semilunar, but in which
from the middle of the upper or lower margin a three-cornered
tongue projects across the aperture, which is thus given the form
of the conventional heart of a pack of cards.
4. The infundibuliform hymen has the form of a small projecting
funnel resembling in appearance the invaginated end of the finger
of a glove.
Maschka refers also to the rare condition in which the hymen
is sometimes said to be absent. As a matter of fact, however, in
such cases, it is represented by a very narrow annular eminence, the
genitals being in other respects normal. The smooth character of
the eminence will serve to differentiate it from the remains of a
destroyed hymen. Other rare forms are:
1. The imperforate hymen, an occlusive membrane, entirely
blocking the vaginal orifice. In some cases, however, the hymen
is not absolutely imperforate, a very small, punctiform aperture
being present.
2. The cribriform hymen, a hymen which is “imperforate” in
the sense that there is no opening of a size approaching the normal,
but in which several minute apertures are present.
3. The septate, bridged or divided hymen (hymen bifenestratus,
etc.), exhibits a strip of mucous membrane, most commonly running
67directly from before backward, occasionally, however, somewhat
obliquely, across the aperture in the membrane, which is thus divided
into two equal or unequal parts. In some instances the
process that bridges the aperture of the hymen is expanded in the
vertical plane to form a septum which projects for some distance
into the vagina.
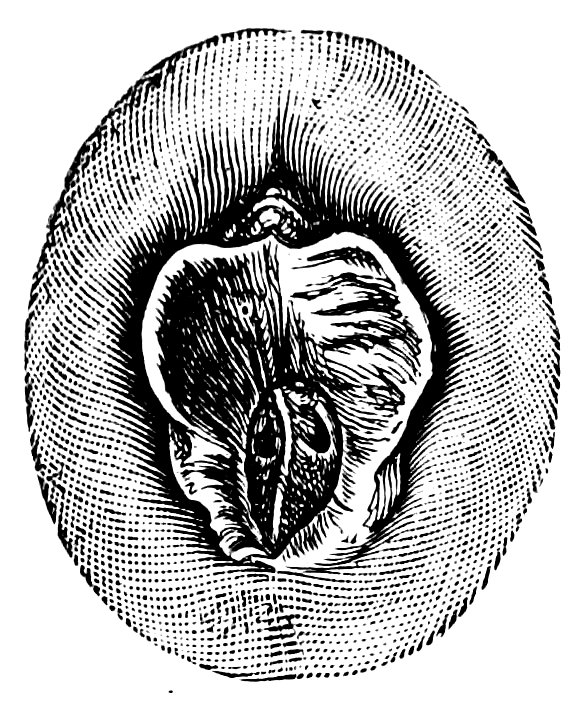
Fig. 24.—Septate Annular Hymen.
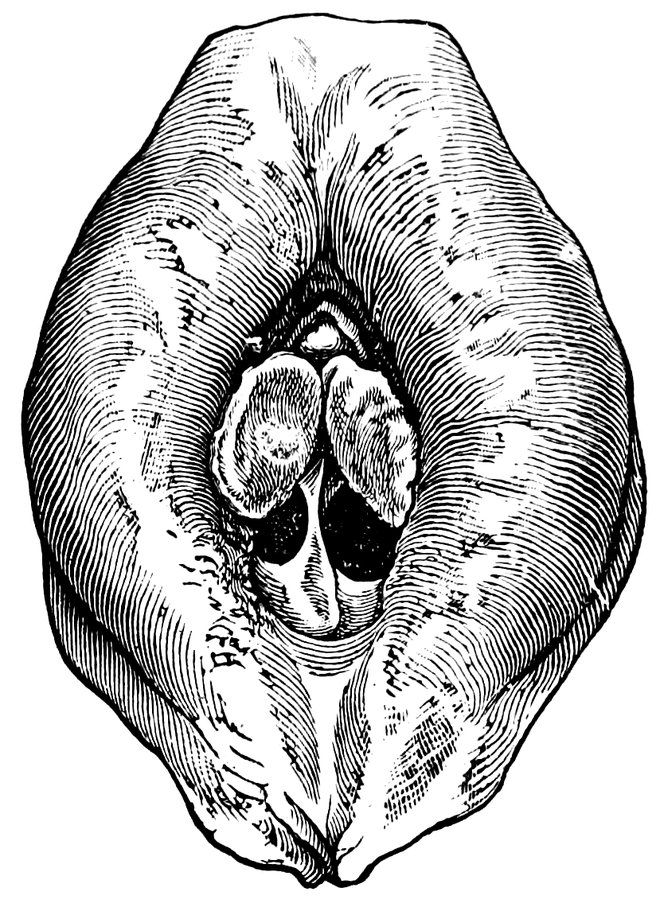
Fig. 25.—Septate Semilunar Hymen.
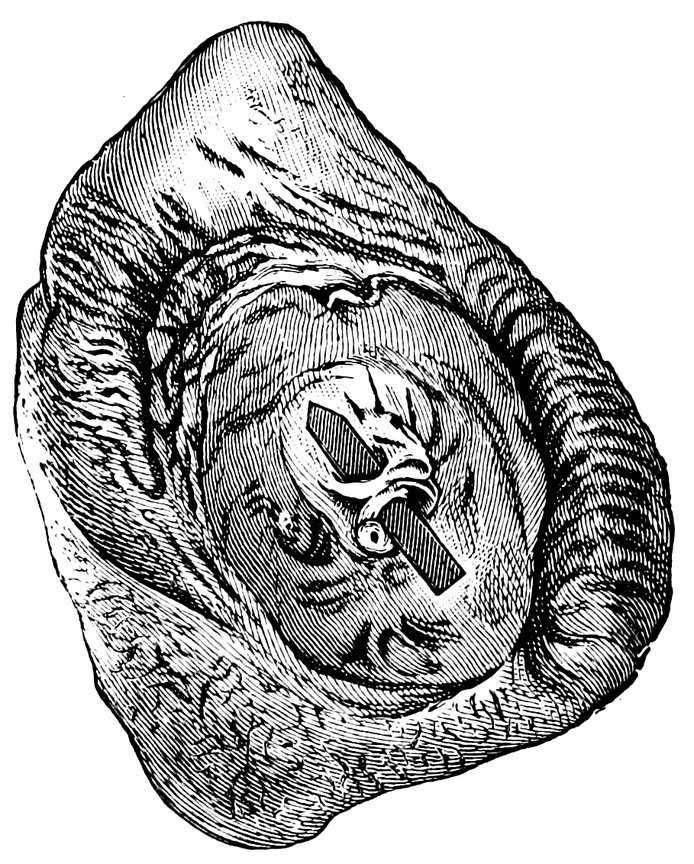
Fig. 26.—Extremely tough Annular Hymen, with an obliquely disposed Septum.
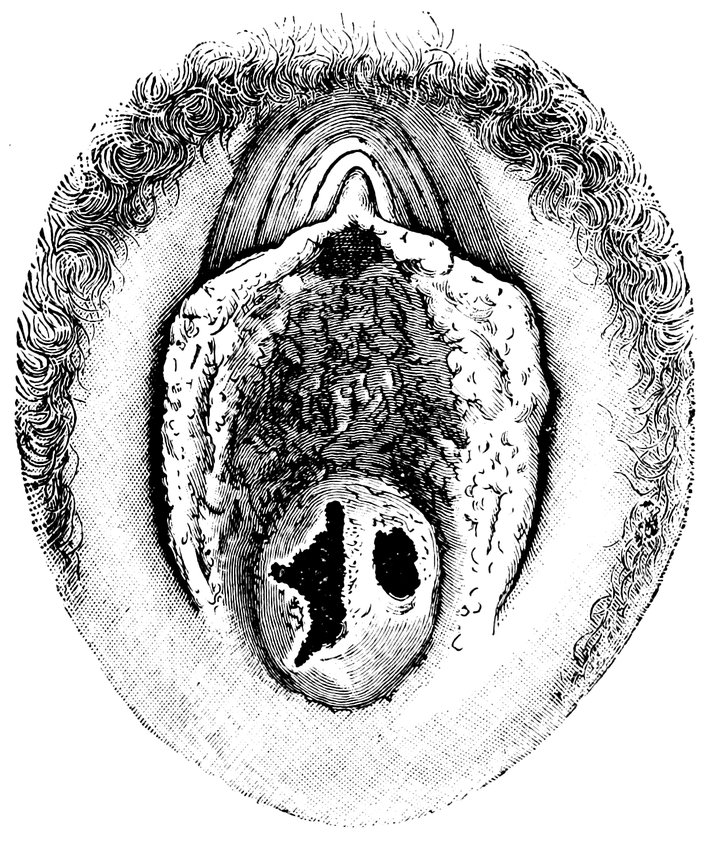
Fig. 27.—Septate Hymen with Apertures of unequal size.
684. The lobate, lobulated, or labiate hymen, which consists
of several (two to four) lobes on either side, each overlapping
the next like the tiles in a roof, whilst the aperture between the
two sides has the form of an antero-posterior slit (Fig. 37); in
some cases the lobes of a lobulated hymen are so disposed that
the membrane has the appearance of a fold of mucous membrane
with a central furrow.
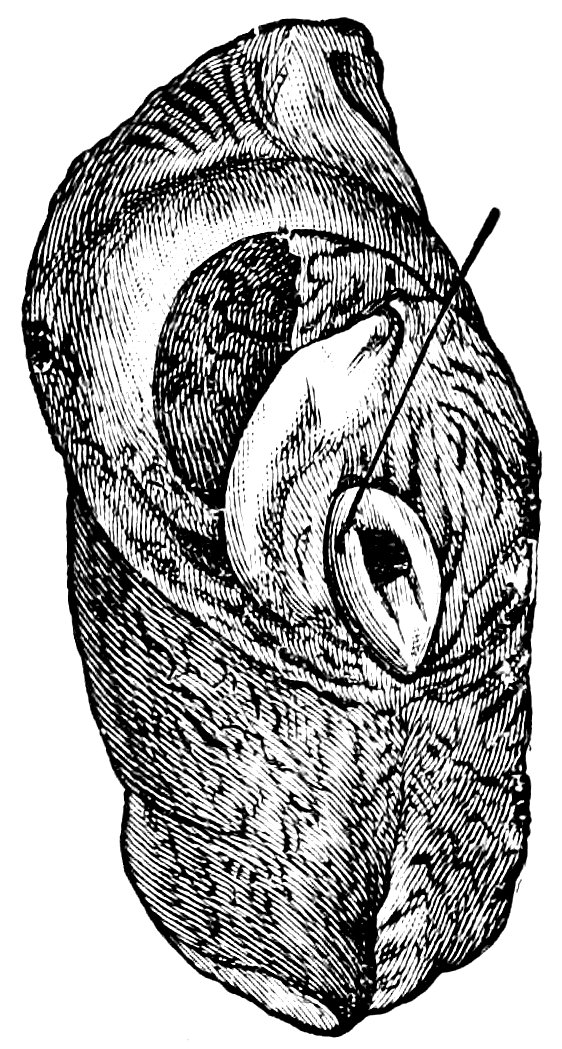
Fig. 28.—Septate Hymen with Apertures of unequal size.
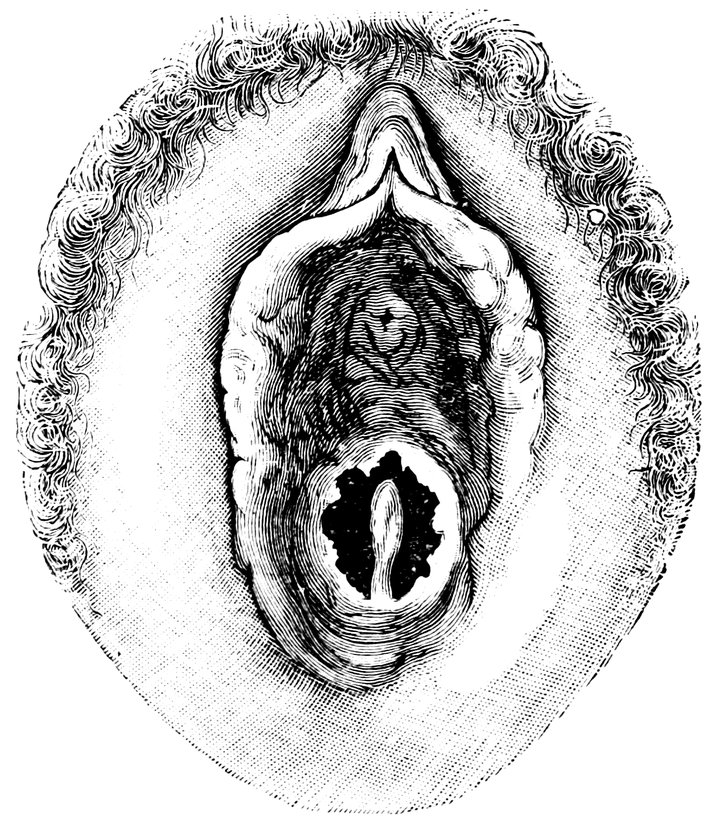
Fig. 29.—Hymen with rudimentary Septum.
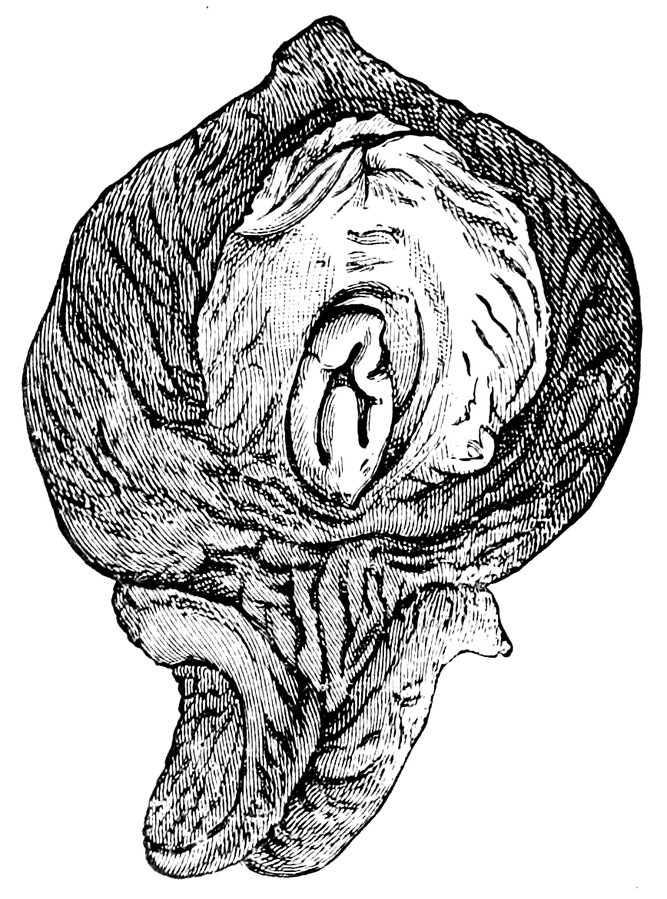
Fig. 30.—Hymen with posterior rudimentary Septum.
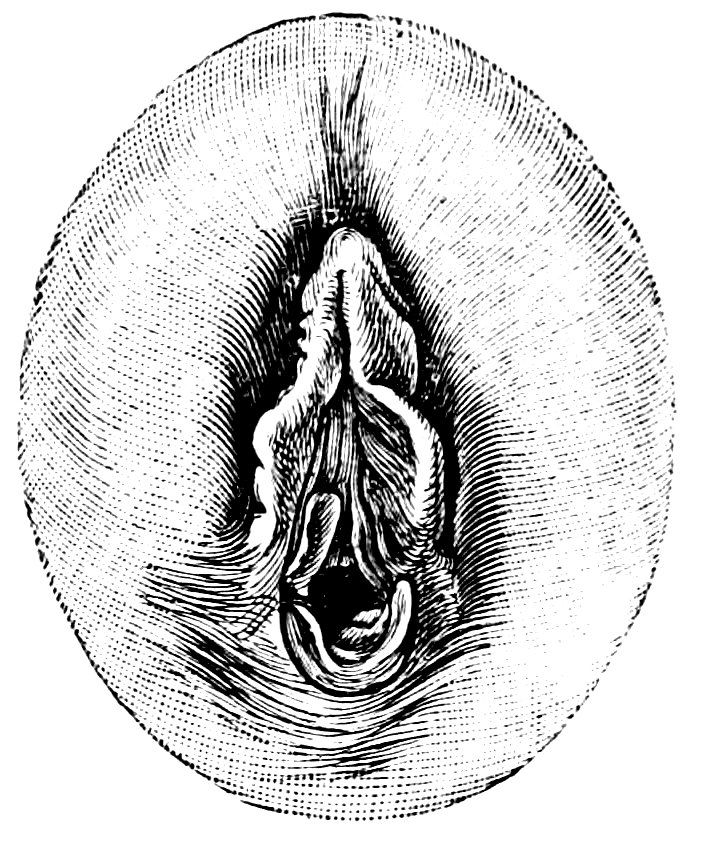
Fig. 31.—Labiate Hymen with posterior rudimentary Septum.
69It is obvious that an imperforate or cribriform hymen, by the
hindrance it offers to the passage of the menstrual discharge, is
liable at the time of the menarche, and as soon as menstruation begins,
to give rise to serious disorder and to pathological states.
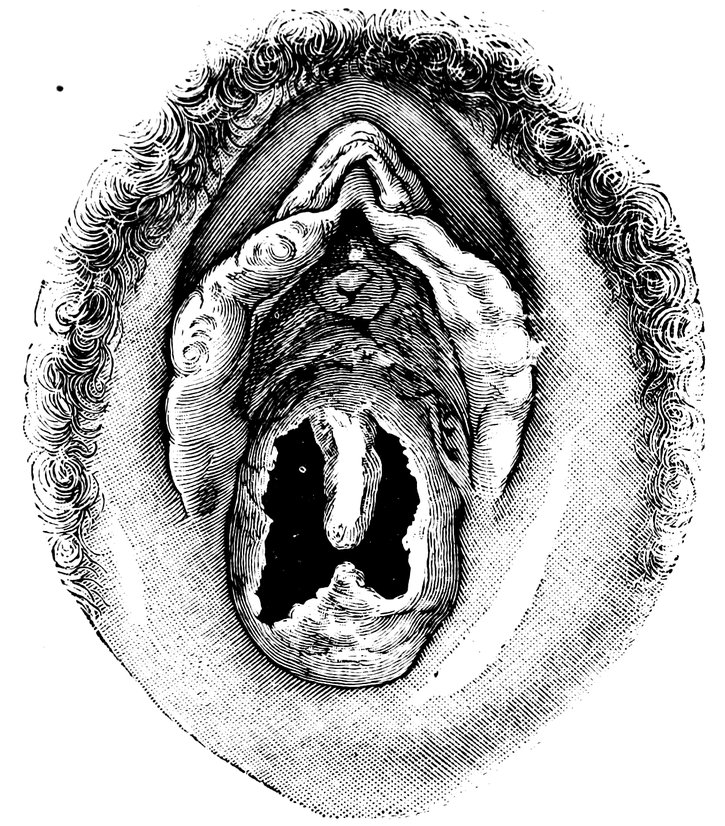
Fig. 32.—Hymen with anterior rudimentary Septum.
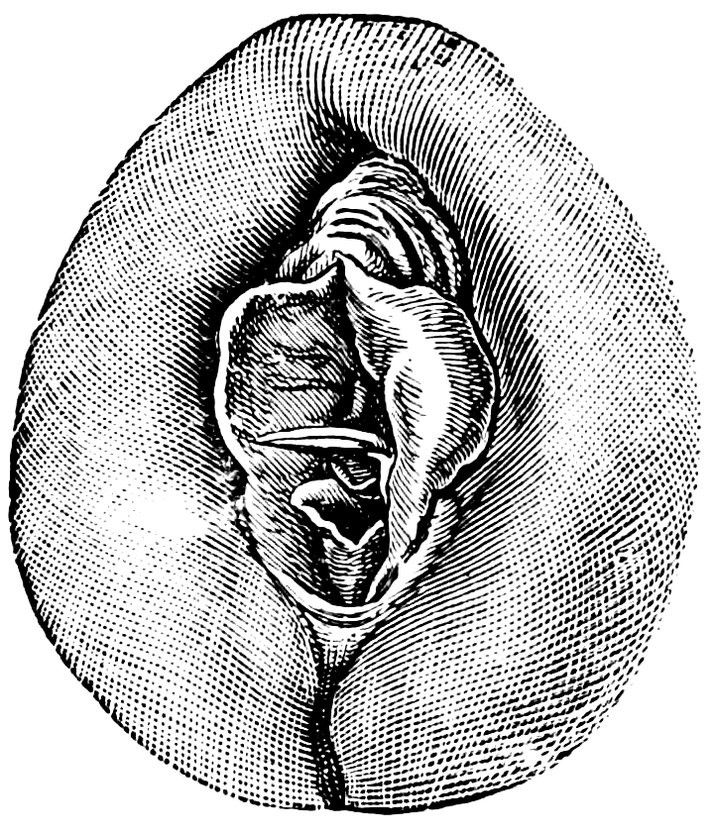
Fig. 33.—Hymen with anterior rudimentary Septum projecting in a opiniform Manner.
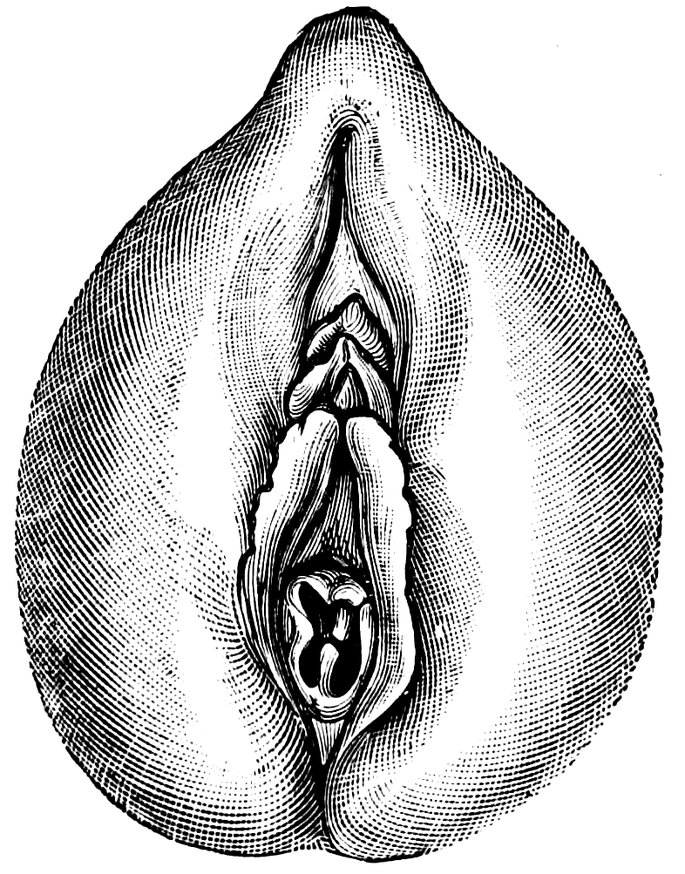
Fig. 34.—Hymen with anterior and posterior rudimentary Septa.

Fig. 35.—Hymen with filiform process projecting from the anterior margin.
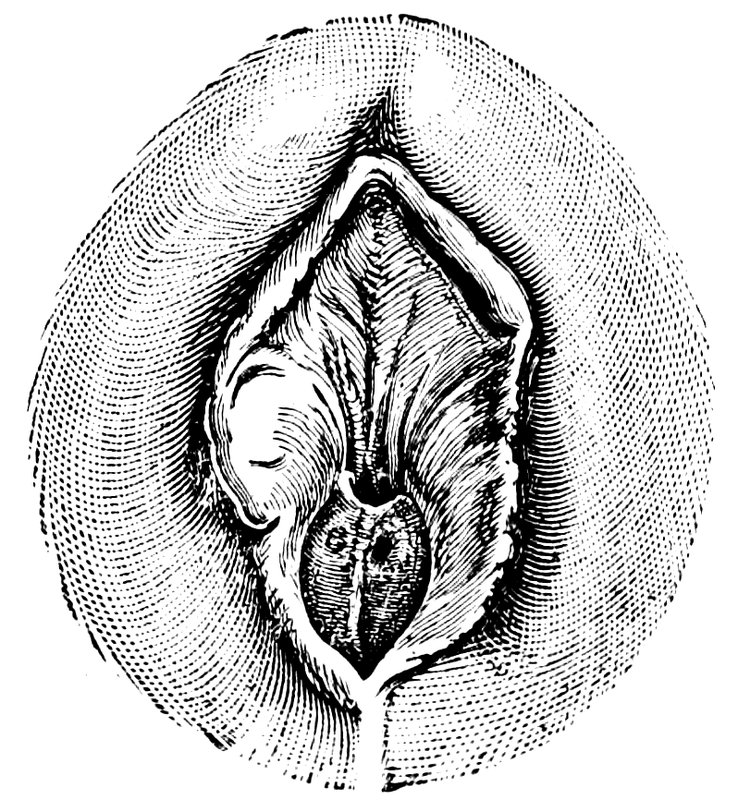
Fig. 36.—Hymen in which there are two symmetrically disposed thinned areas. The left of these is perforated.
The illustrations we append, showing the various forms of the
hymen, are taken from von Hoffmann’s Handbook of Medical Jurisprudence.
(Figs. 18–45.)
70
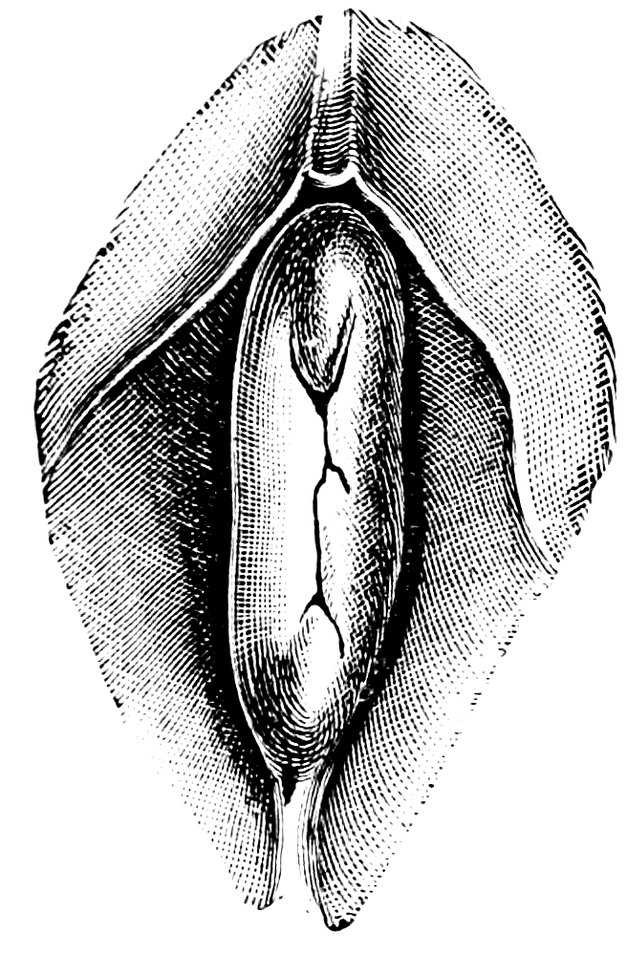
Fig. 37.—Very unusual form of Hymen.
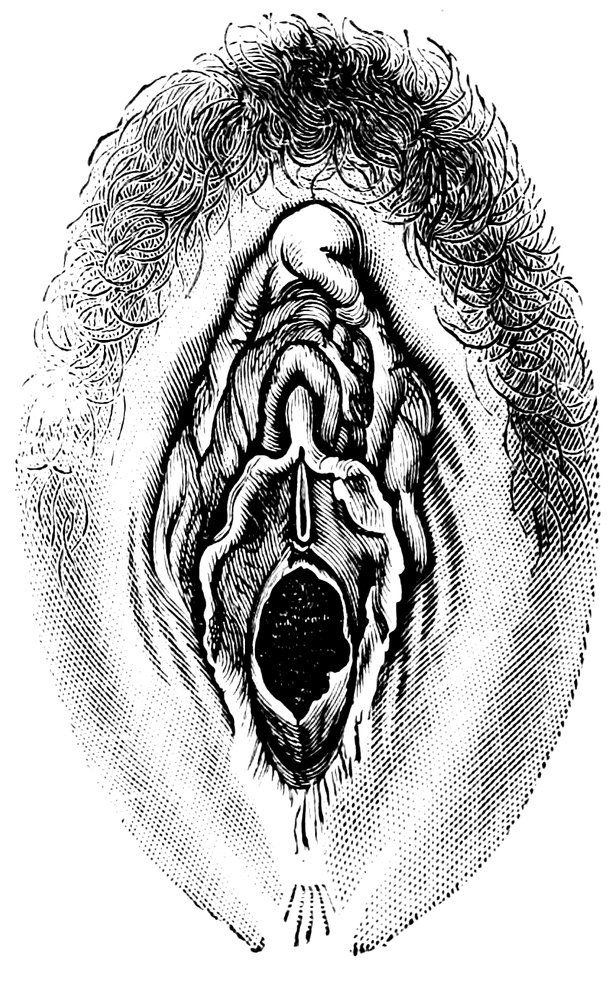
Fig. 38.—Semilunar Hymen with cicatrized Lacerations in its Border.
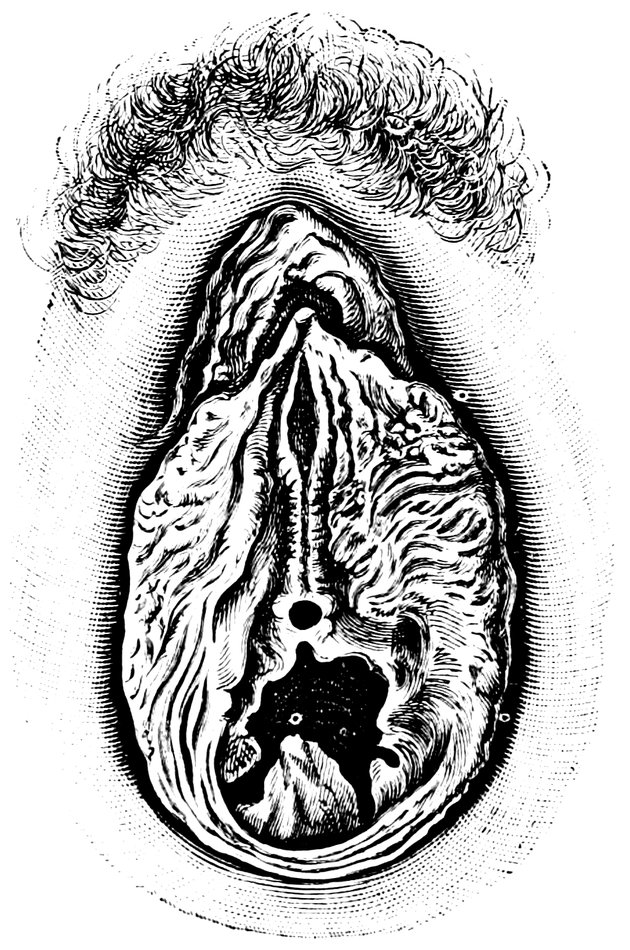
Fig. 39.—Deflorated Semilunar Hymen with laterally disposed Symmetrical Lacerations.
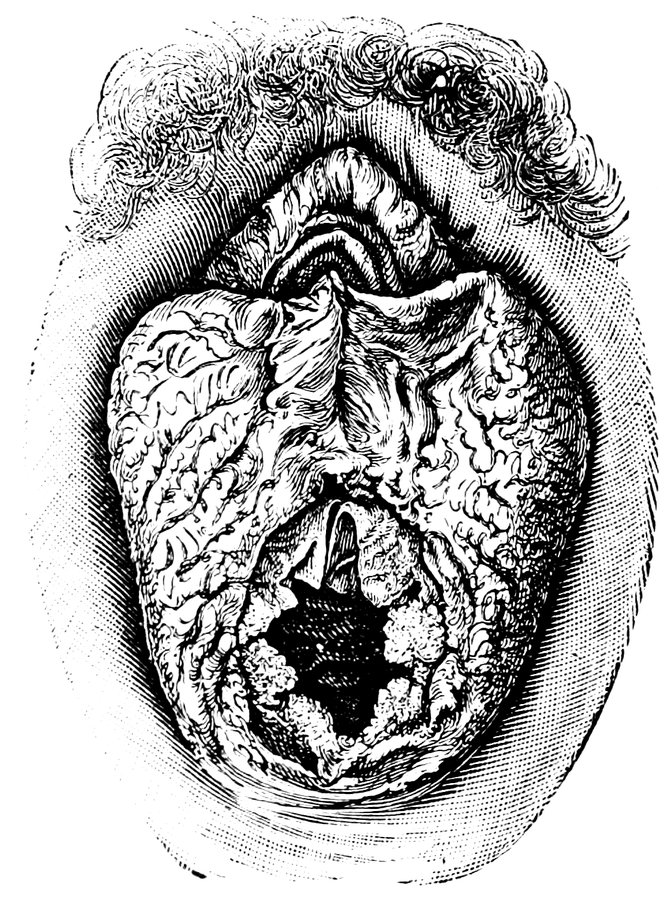
Fig. 40.—Deflorated Annular Hymen with several cicatrized Lacerations.
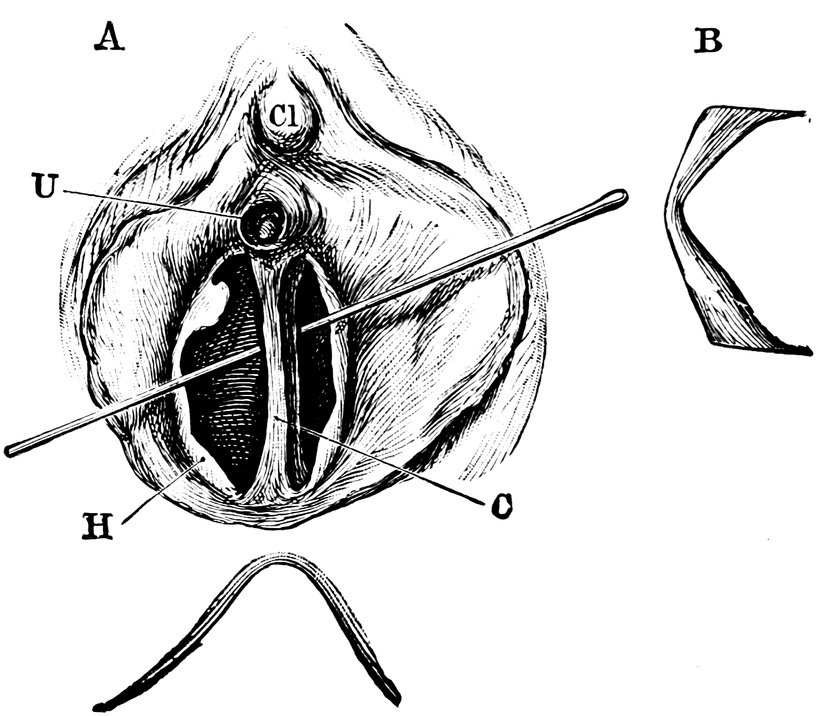
Fig. 41.—A. Septate Hymen in which Defloration has been effected through one of the Apertures. U. Urethra. Cl. Clitoris. H. Cicatrized margin. C. Septum. B. Lateral View of Septum.
In some cases the hymen is exceedingly thin and delicate, so that
it is liable to be torn if handled at all roughly; in other cases, on
the contrary, it may be very firm, thick, and fleshy, interlaced with
strands of connective tissue and muscle, so that it forms a veritable
cuirass for the protection of physical virginity.
71
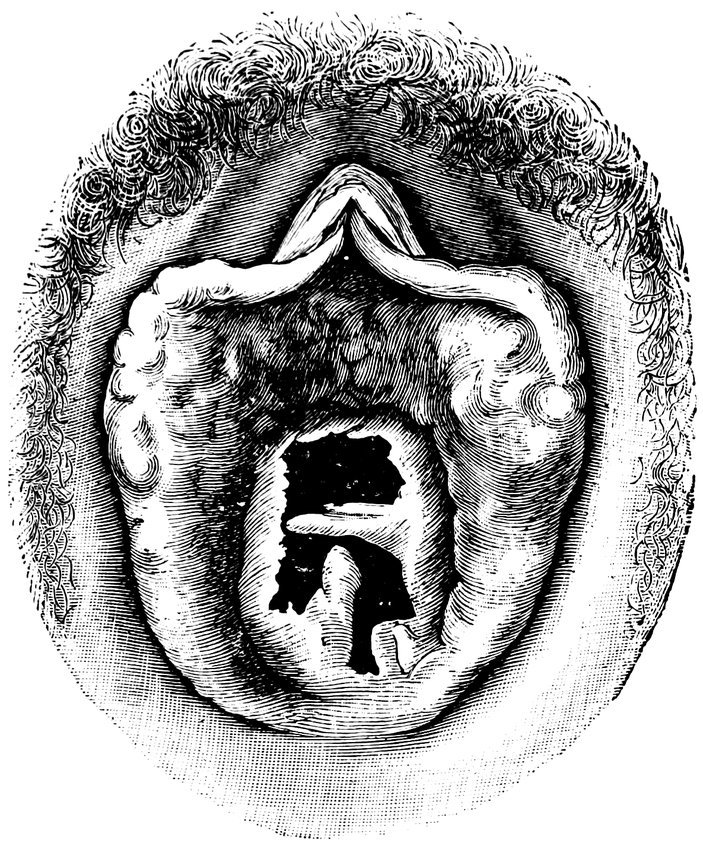
Fig. 42.—Deflorated Septate Hymen.
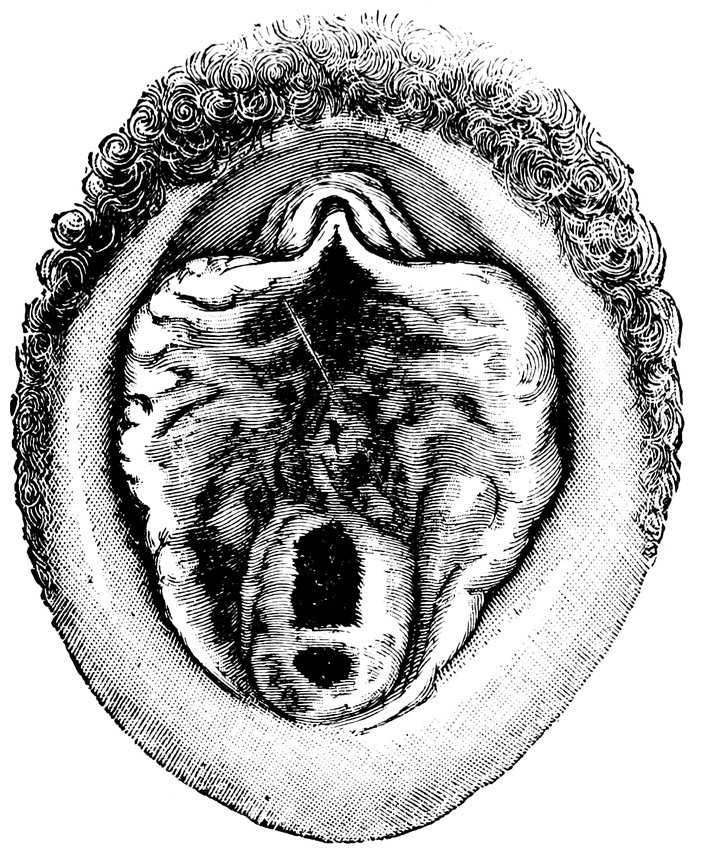
Fig. 43.—Hymen with larger anterior and smaller posterior Apertures.
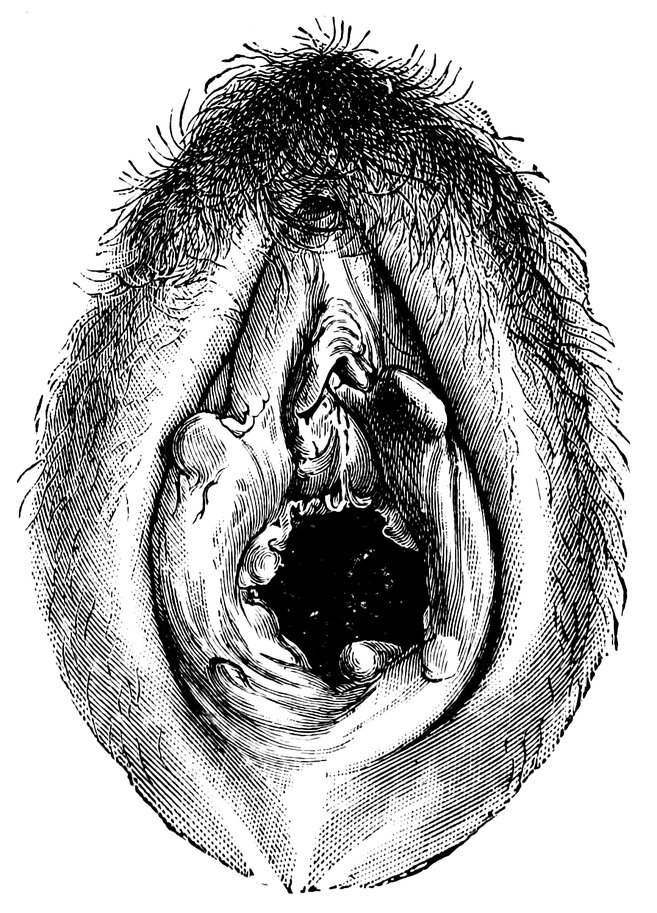
Fig. 44.—Carunculæ Myrtiformes in a Primipara.
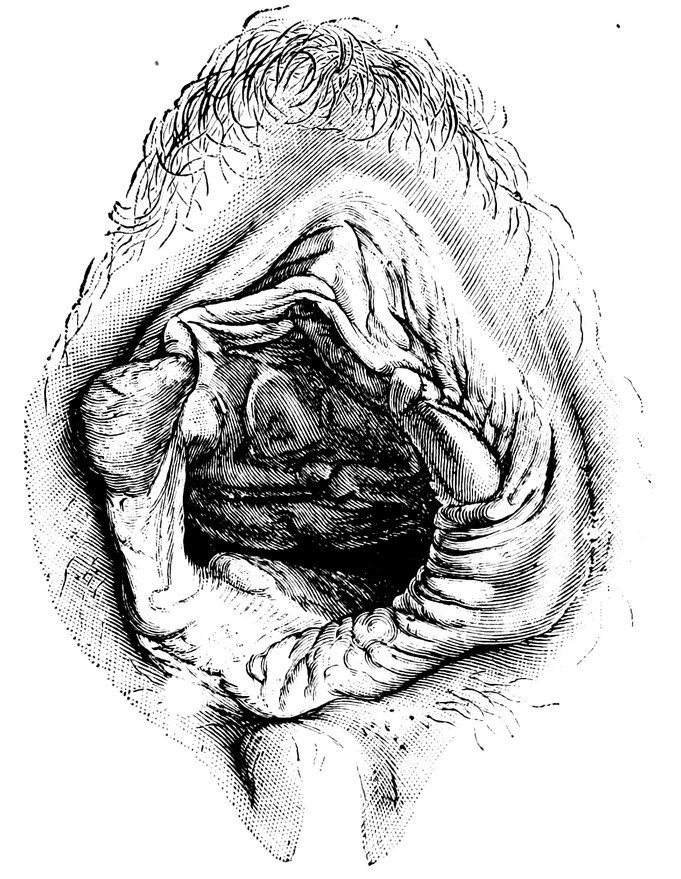
Fig. 45.—Vaginal Inlet of a Multipara, without Carunculæ Myrtiformes. Slight Prolapse of anterior and posterior Vaginal Walls.
As signs of virginity in the female, a knowledge of which is
required, not only for the purposes of medical jurisprudence, but
72for various other reasons, we may enumerate the following anatomical
characteristics of the genital organs. The labia majora
are elastic in consistence and are in close apposition with one another;
the labia minora or nymphæ are covered by the labia majora
and are but little pigmented; the vestibule and the vaginal orifice
are narrow, and the vagina itself is narrow, tense, and markedly
rugose; the hymen is normal and uninjured (this, of course, is the
most trustworthy of all the signs of virginity); the breasts have
the virgin conformation. In opposition to the plea that the hymen
can be destroyed by other causes than defloration, as by a fall,
especially a fall which brings the external genitals in contact with
some hard body, or by diphtheritic, variolous, or syphilitic ulceration,
Maschka maintains that such occurrences are among the greatest
rarities.
On the other hand it is sufficiently well known that the presence
of an uninjured hymen affords no certain assurance of actual virginity.
Cases enough are recorded, both in older and more recent
medical literature, in which even pregnancy occurred in women in
whom the hymen had remained intact, the explanation being that
during copulation penetration of the penis had failed to occur, the
semen being ejaculated on the vulva. Scanzoni and Zweifel have
recorded cases in which the intact hymen offered a hindrance to parturition.
The first-named author explains these occurrences by the
assumption that the hymen was so stout that the penis was unable to
rupture it. Veit remarks that both male and female youth, in these
days of the continued advance of knowledge, are well acquainted
with coitus sine immissione penis, and that very frequently a woman
who is informed that she is pregnant makes answer that this is impossible,
her paramour having assured her that pregnancy could not
occur. On the other hand, cases are met with in which the aperture
in the hymen is a very large one, so large that the penis can penetrate
to the vagina without lacerating the membrane.
Broudardel reports a case of rape in which the lacerated hymen
healed so completely that an expert maintained the integrity of the
membrane, until another pointed out the fine scar.
In general, that we may be assured of the existence of virginity,
we must find the hymen uninjured; and, on the other hand, we
must regard the laceration of the membrane, unless known to be the
result of gynecological examination or other manipulation, as a
proof of defloration.
In ancient times among savage races the integrity of the hymen
was prized as a proof of virginity, and in the Bible also great stress
is laid on this sign in connection with defloration, and its absence
was even regarded as a ground for the death punishment (Deut.
73xxii, 21). But amongst other races the hymen was held in no particular
esteem as a token of virginity.
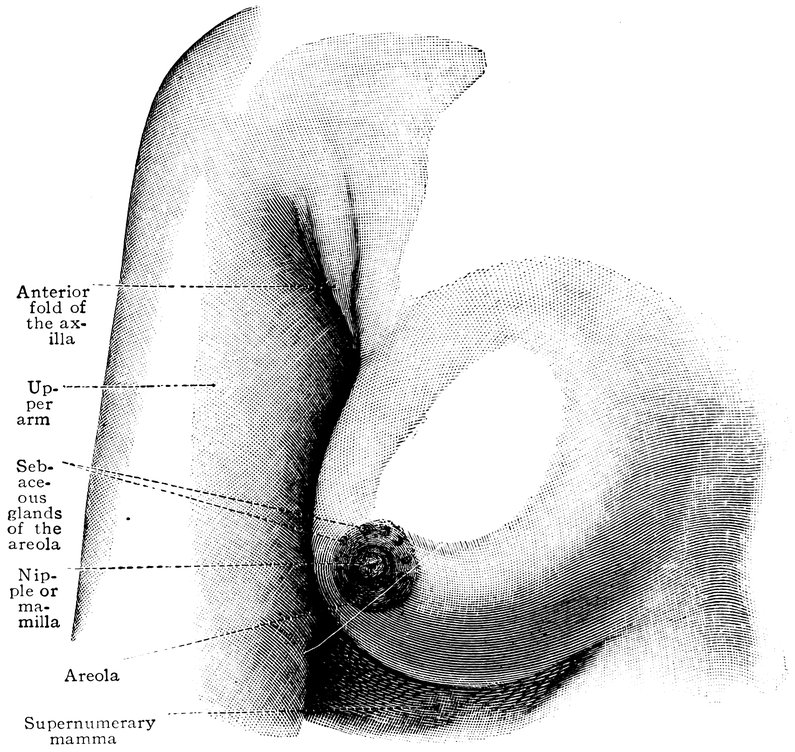
Fig. 46.—Mamma, the breast of a virgin aged eighteen years. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
In ancient times, and even at the present day in the Philippine
Islands, the Ladrone Islands, and certain other islands of the Polynesian
Archipelago, also among many African tribes, the right of
defloration belonged, not to the bridegroom, but to every man belonging
to the same tribe; sometimes on the bridal night all the
men of the tribe had access to the bride, the bridegroom coming
last, but thenceforward having undisputed possession of his wife.
Amongst certain other tribes a similar custom prevails, differing
however in this respect, that the rite of defloration is performed by
a priest or by one of the chiefs of the tribe. In mediæval Europe,
again, the great landed proprietors exercised the well-known jus
primae noctis or droit du seigneur.
In girls at the time of the menarche who have long practiced
masturbation, some of the following indications of the habit will
74be found: Elongation, redness, and general enlargement of the
clitoris; elongation and thickening of the nymphæ, which are also
of a tough consistency and deeply pigmented; flaccidity of the labia
majora; redness of the vaginal orifice; flaccidity of the hymen,
which also may exhibit lacerations, caused by the forcible introduction
of the finger or of some hard foreign body.
Not until the time of the menarche do the breasts attain the
hemispherical form which constitutes one of the graces of young
womanhood, and at the same time these organs assume a firm, elastic
consistency; their size of course varies in different individuals.
The nipple now has a rose-red color, darker in brunettes than in
blondes; it is usually small, sometimes quite inconspicuous, being
withdrawn into a cutaneous furrow. The two breasts when regarded
from the front are seen to diverge from the longitudinal axis
of the body. In some cases even in childhood, before the time of the
menarche, the breasts are powerfully developed, being as large as
an apple or larger. This depends on climate, race, and sexual excitement;
as regards the last of these, early sexual stimulation promotes
premature mammary development.
Although it is unusual for any secretion to appear in the mammary
gland before the occurrence of pregnancy, cases have certainly been
observed in which the breasts of virgins secreted a milk-like fluid,
especially in consequence of sexual excitement or during menstruation.
Thus Maschka observed in a girl the condition of whose
genital organs showed her to be a virgo intacta that pressure on the
breast caused a few drops of an opalescent fluid having the appearance
of milk to exude from the nipple. She acknowledged that
amatory relations had long subsisted between her and a lover who
was in the habit of handling her breasts, and that this always
produced strong sexual excitement. Hofmann also reported that in
two virgins who died during menstruation he was able to express
a drop of milk from the breast.
The most important indication of the general changes occurring
in the external and internal genital organs, the proof that the
young woman has become fitted for the fulfilment of her reproductive
vocation, is the appearance of menstruation, a sanguineous discharge
from the genital organs recurring every four weeks as the
external manifestation of the internal process of ovulation.
The anatomical changes that have already been described as
occurring in the genital organs at the time of the menarche will
serve to elucidate the numerous reflex processes that manifest themselves
at this period of life in so many departments of vital activity.
It is especially the extensive developmental processes in the ovary,
influencing the nerves of that organ, which give rise to centripetal
75stimuli and evoke reflex manifestations. In the working of
the circulatory system, such influences are apparent; and during the
menarche, some time already before the first onset of menstruation,
variations occur in the blood-pressure, and these during menstruation
take the form of a typical undulatory curve.
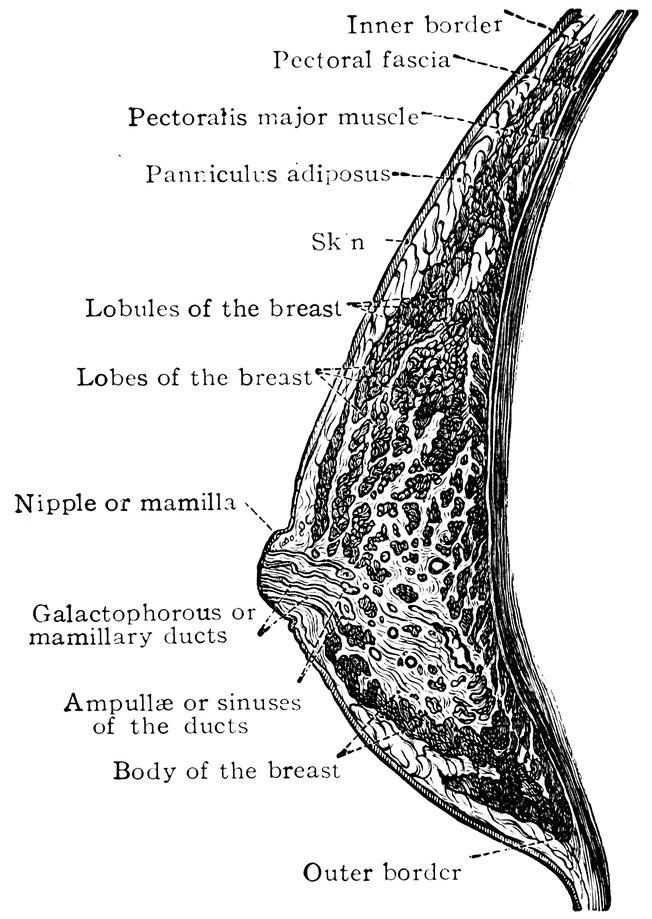
Fig. 47.—Horizontal section through the female breast. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
Thus it becomes comprehensible that even in healthy girls, the
first appearance of the catamenia and likewise the expectation of
the flow induce a certain modification and alteration in the whole
nature and disposition. Girls often lose their previous cheerful and
lively character, becoming quiet, self-absorbed, sometimes even
melancholy; they are disinclined for study, have a repugnance to
all sustained physical or mental activity, become annoyed and snappish
on slight occasion, are restless at night, consider themselves to
be ailing, and so on. During the first menstruation girls commonly
appear pale and anxious, they have blue lines beneath the eyes, the
face has a tired aspect, the movements lack energy, and a general
want of tone combined with an abnormal irritability may be noticed.
Some days before the first menstruation, the vulva, the labia majora
76and minora, and the vaginal mucous membrane, are swollen, the
clitoris becomes conspicuous in consequence of erectile processes, a
slight secretion appears in the genital passage, and the breasts become
sensitive and slightly turgid. The urine deposits a thick
sediment, and occasionally severe strangury is observed. In many
cases, also, digestive disturbances occur, loss of appetite, constipation,
or a tendency to diarrhœa.
The first menstruation usually lasts four or five days. On the
first day the discharge is blood-stained mucus, thereafter becoming
sanguineous. In some cases, the bleeding at the first menstruation
is profuse and of long duration.
It is not always after the first menstruation that the subsequent
discharges follow at the regular intervals of four weeks. In delicate,
anæmic girls the second menstruation may not occur till several
months have elapsed after the first; less often the second menstruation
ensues a fortnight after the first, or even earlier.
At the time of the menarche the sexual impulse, which has hitherto
been dormant, becomes strongly developed. It is evoked at this time
of life by the anatomico-physiological changes undergone by the reproductive
glands; the stimulus aroused by these processes in the
ovary, being conducted to the brain, awakens passion. At the same
time the observation of the growth of the hairy covering on the
genital organs, the development of the breasts, and the appearance
of menstruation, tend to arouse erotic presentiments. The reading
of romances, conversations with female friends, and observation of
the conduct of full-grown persons, convert these presentiments into
clear ideas, and excite the impulse to the production of passionate
sexual sensations, the sexual impulse. How far these stimuli arising
from the reproductive apparatus are encouraged and accentuated,
on the one hand, or repressed and diminished, on the other, depends
on external impressions of various kinds. The environment is the
determinant for the further transformation of the as yet undifferentiated
sexual impulse into the fully-developed copulative and reproductive
impulses.
In his work on the Physiology of Love, Mantegazza describes the
yearning and stress of the awakening sexual life, arising out of the
presentiments, hazy sensations, and impulses, which are felt in the
very earliest period of the developmental phase known as puberty.
In general, in a young girl during the menarche, the sexual impulse
manifests itself rather in the form of semi-conscious reverie,
of platonic love. The adolescent girl exercises her imagination with
the circumstances of her chaste love, her mind turns to this subject
when in solitude, her mood is apt to become melancholy, and
it is the perusal of equivocal novels, or the educational assistance of
77sexually experienced female friends, that transforms the sexual impulse
to a vivid flame.
Some authors believe that a sign of the awakening of the sexual
impulse when directed toward some particular man is a change of
color on the part of the girl when she sees this individual or hears
him spoken of. Palpitation of the heart comes on, the pulse is increased
in frequency, the respiration also, and the voice fails. In
this manner, it is asserted, Galen discovered the love of a Roman
lady, Justa, for the dancer, Pylades.
The psychological reaction of the sexual impulse at the time of
puberty manifests itself, as von Krafft-Ebing points out, in manifold
ways, common to all of which, however, is the emotional state of
the mind, and the need that the strange and new feelings now experienced
should find some objective centre of interest. Such objective
and emotional interests lie ready to hand in religion and
poetry, both of which, after the period of sexual development is at
an end, and the originally incomprehensible desires and impulses
have received an explanation, continue to have intimate relations
with the world of sexual experience. Any one who doubts this must
be reminded of the frequency with which religious fanaticism makes
its appearance at the time of puberty. No less influential is the
sexual factor in the awakening of æsthetic feelings. This world of
the ideal opens itself at the time when the development of the sexual
processes begins. * * * The love of early youth, continues von
Krafft-Ebing, has a romantic, idealizing tendency. In its first manifestations
it is platonic, and willingly exercises itself in poetry and
history. But as the sensibility awakens, the danger arises that this
passion, with its idealizing power, will be transferred to persons of
the opposite sex who in intellectual, physical, and social relations
are by no means all that could be wished. Hence proceed misalliances,
elopements, and seductions, with the entire tragedy of impassioned
love, which conflicts with the dictates of morality and
convention, and sometimes finds its bitter end in suicide or a double
self-destruction. Love in which the senses play too prominent a
part can never be a true and lasting love. For this reason, first
love is as a rule very transitory, since it is in most cases no more
than the first flare of passion. * * * Platonic love is a thing
without existence, a self-deception, a false description of sexual sensations.
Bebel remarks that the number of suicides among women of the
ages of sixteen to twenty-one years is an exceptionally large one,
and he refers this chiefly to unsatisfied sexual impulse, unfortunate
love, secret pregnancy, and to betrayal by men.
78
Menarche Praecox et Tardiva.
(Precocious and Retarded Menstrual Activity.)
By the term precocious menarche we understand the pathological
state in which a typical, four-weekly, sanguineous discharge from
the female genital organs sets in at an abnormally early age, and is
to be regarded as a symptom of a premature sexual development.
Very commonly such children with precocious menstruation and
premature sexual development, exhibit a comparatively high body-weight,
great development of fat, early dentition; they look older
than their years; and they have genital organs that also develop
very early, with hair on the pubes and in the axillæ; the labia
majora and the breasts resemble those of full-grown women, and
the pelvis also has the adult form. Commonly also the sexual impulse
develops early, whilst, in other respects, the intellectual development
lags behind the physical. It is most probably a primary
hyperplasia of the ovaries that gives rise to precocious menstruation,
the ovarian follicles ripening earlier than usual. Frequently other
pathological processes are associated with this early sexual development,
such as general lipomatosis, rachitis, and new growths of the
ovaries. In several cases of this nature, early conception has also
been observed. According to oriental tradition, Khadijah was married
at the age of five years to the prophet Mohammed, who cohabited
with her three years later.
Even if we except those cases in which in earliest infancy there
is a sanguineous discharge from the vagina which remains, however,
an isolated occurrence, or if repeated is repeated a few times
only and at quite unequal intervals (cases in which the bleeding cannot
be regarded as menstrual—such, for instance as were reported
by Eröss of six new-born female infants in whom a sanguineous
discharge from the vagina appeared three or four days after birth
and lasted two to five days, the infants not remaining subsequently
under observation),—numerous well-authenticated cases yet remain
in which menstrual hæmorrhage was observed before the end of
the first year of life. One case, even, is recorded by Bernard in
which from the time of birth to the twelfth year menstruation with
molimina occurred every month, lasting two days; from the twelfth
to the fourteenth year menstruation ceased, recurring subsequently
at irregular intervals.
In the recorded cases of such precocious menstruation the menstruation
recurred as a rule at regular intervals of four weeks; only
in quite exceptional cases were the intervals three to five months.
Some of the most striking and well-authenticated cases of precocious
menstruation recorded in the recent literature of the subject
are appended.
79Observed by Combys: A girl aged 6 years and 2 months had
the appearance of a girl aged 14 or 15; she was a brunette, 3′ 10½″
in height, with full, firm, rounded breasts, girth of chest 28⅓″, mons
Veneris covered with hair, uterus normal on rectal examination,
hymen intact; menstruation had occurred regularly since the second
year of life. Mother and five sisters began to menstruate between
the ages of twelve and fourteen. General condition good.
Case recorded by Diamant: A girl aged 6 years, weight 75
pounds, thighs, buttocks, and breasts developed like those of a sexually
mature woman, axillæ and mons Veneris covered with hair.
Menstruation began at the age of 2 and recurred regularly, the flow
lasting 4 days.
Case recorded by Plyette: A girl with precocious physical development
began to menstruate in the fourth year of life; menstruation
continued regularly with the exception of two monthly periods,
when vicarious epistaxis occurred.
From the collection made by Gebhard of the records of fifty-four
cases of precocious menstruation, giving the first appearance and
the type of menstruation, the development of the breasts, the other
signs of premature sexual development, and any complications that
may have been observed, we extract the age at which the first menstruation
occurred. This was:
| In a new-born |
infant in |
1 case. |
| At the age of |
2 weeks in |
1 case. |
| At the age of |
2 months in |
1 case. |
| At the age of |
3 months in |
1 case. |
| At the age of |
4 months in |
1 case. |
| At the age of |
5 months in |
1 case. |
| At the age of |
7 months in |
1 case. |
| At the age of |
9 months in |
4 cases. |
| At the age of |
10 months in |
2 cases. |
| At the age of |
12 months in |
5 cases. |
| At the age of |
15 months in |
1 case. |
| At the age of |
16 months in |
1 case. |
| At the age of |
18 months in |
2 cases. |
| At the age of |
19 months in |
1 case. |
| At the age of |
22 months in |
1 case. |
| At the age of |
2 years in |
4 cases. |
| At the age of |
2½ years in |
1 case. |
| At the age of |
2 years and 9 months in |
1 case. |
| At the age of |
3 years in |
6 cases. |
| At the age of |
3½ years in |
1 case. |
| At the age of |
4 years in |
4 cases. |
| At the age of |
4 years and 3 months in |
1 case. |
| At the age of |
5 years in |
1 case. |
| At the age of |
5½ years in |
1 case. |
| At the age of |
6 years in |
1 case. |
| At the age of |
6½ years in |
1 case. |
| At the age of |
7 years in |
3 cases. |
| At the age of |
9 years in |
2 cases. |
| At the age of |
11½ years in |
1 case. |
80From this collection of Gebhard’s we learn that in one case menstruation
already existed at birth, and that in a large number of
cases it occurred before the expiration of the first year. In many
cases the development of the breasts preceded the appearance of
menstruation, and was noticed from the time of birth. The vulva
also early exhibited the characteristics seen in the sexually mature
woman. Further, a high body-weight, great development of fat,
and early dentition, were usually seen in these cases, in which, however,
the intellectual development was not in correspondence with
that of the body.
In several of these cases of premature puberty, moreover, sexual
intercourse and even parturition occurred at a very early age. A
girl in whom menstruation began at the age of one year, gave birth
to a child when she was ten years old (Montgomery). A girl who
began to menstruate at the age of nine years, became pregnant
very shortly afterward (d’Outreport). The well-known case recorded
by Haller, in which at birth the pubic hair was already
grown, and in which menstruation began at the age of two years,
was also one of very early pregnancy, the girl giving birth to a
child when nine years old. Another girl in whom at birth the pubes
were already covered with hair began to menstruate when four
years old, copulated regularly from the age of eight, and at nine
years became pregnant, and was delivered of a vesicular mole with
an embryo (Molitor). A girl began to menstruate at the age of two,
had a growth of hair on the pubes and developed mammæ at the
age of three, and became pregnant at the age of eight (Carus).
With these cases must be classed that observed by Martin in America
of a woman who was a grandmother at the age of twenty-six.
Lantier, in his Travels in Greece, speaks of a mother of twenty-five
with a daughter of thirteen.
Observations made by Kussmaul and by Hofmeier prove that in
many cases changes in the ovaries form the probable cause of precocious
menstruation and the other phenomena of premature puberty.
In one case of Hofmeier’s, for instance, of a girl of five with precocious
menstruation, the removal of a rapidly growing ovarian
tumor was followed by the cessation of menstruation, and the pubic
hair, which had been shaved off, did not grow again.
Abnormally early puberty related to the early practice of sexual
intercourse is seen in many prostitutes. This is shown by the following
figures relating to 150 prostitutes in Russia. Sexual intercourse
began:
| In |
1 prostitute at the age of |
9 years. |
| In |
1 prostitute at the age of |
10 years. |
| In |
4 prostitutes at the age of |
12 years. |
| In |
12 prostitutes at the age of |
13 years. |
| 81In |
14 prostitutes at the age of |
14 years. |
| In |
33 prostitutes at the age of |
15 years. |
| In |
36 prostitutes at the age of |
16 years. |
Thus, among the 150 prostitutes, 65 were less than 16 years of age.
Parent-Duchatelet found among 3,517 prostitutes under official
observation, 5.6 per cent. under 17 years of age. There were:
| 2 |
prostitutes under 10 years of age. |
| 3 |
prostitutes under 11 years of age. |
| 3 |
prostitutes under 12 years of age. |
| 6 |
prostitutes under 13 years of age. |
| 20 |
prostitutes under 14 years of age. |
| 51 |
prostitutes under 15 years of age. |
| 111 |
prostitutes under 16 years of age. |
Martineau’s observations also showed that in nearly all prostitutes
the first coitus took place in very early youth. Of 607 prostitutes
there were 489 in whom defloration had occurred between the
ages of 5 and 20 years. According to Grimmaldi and Gurrieri defloration
usually takes place in prostitutes before they attain the age
of 10 years.
Sometimes we find increased sexuality in early life as a pathological
manifestation—psychopathia sexualis. Thus, Esquirol records
the case of a little girl aged four years who undertook improper
manipulations in association with little boys. A female prisoner,
Lombroso writes, had at the age of six years practiced mutual masturbation
with her brother aged seven, and at the age of eight years
underwent defloration; another murderess, while still a schoolgirl,
had conducted herself after the manner of an experienced prostitute.
Laurent reports the case of a girl who from the age of ten was
engaged in sexual malpractices with her brothers and sisters, and
finally underwent defloration at the age of fifteen.
In many cases premature sexual development is manifested by
enlargement of the breasts and growth of the axillary and pubic
hair, and yet menstruation fails to appear. Thus, Kussmaul has observed
girls who while yet children exhibited all the external characteristics
of sexually mature women, but who had not yet begun
to menstruate. Ploss has published a photograph showing in a
girl five years of age the mons Veneris and the labia majora developed
like those of a full-grown young woman, and covered with
long thick hair; in this case, however, not only had menstruation
not yet begun, but the breasts were still in the infantile condition.
The opposite state to menarche praecox is that in which the first
appearance of menstruation is unduly delayed; it may be even till
after the age of twenty. Such a postponement of the menarche
sometimes occurs in girls who exhibit at this period of life an extraordinarily
great general fatty development of the body, or a notably
severe chlorotic state of the blood, or in whom during the years of
82development some sudden and extensive change in the mode of
life has occurred, as for instance when the girl’s place of residence
has been removed from the country to the town, or when she has had
to undertake some completely new kind of physical or mental work.
Raciborski attributes the late appearance of menstruation, at the
ages of 20, 22, 24, or 26, in otherwise healthy girls, to an “apathy
of the sexual sense,” a phrase which does not convey much meaning.
According to Marc d’Espine, puberty occurs early in girls with
dark hair, grey eyes, a delicate white skin, and of a powerful build;
late, on the other hand, in girls with chestnut hair, greenish eyes,
a coarse darkly-pigmented skin, and of a delicate weakly build.
The genitals of girls in whom the first appearance of menstruation
is delayed, frequently exhibit distinct signs of the backwardness
of the reproductive organs in their development. The external genitals,
in such cases, have little if any covering of hair, and are flabby
and relaxed; the body and the fundus of the uterus are shorter and
more slender than usual, the uterus as a whole is small and flaccid,
sometimes anteflexed; the vaginal portion of the cervix is small,
often almost undeveloped, its anterior lip barely projecting above
the surface of the vaginal fornix; the vagina is usually short and
narrow. The ovaries also are flaccid and inelastic, and occasionally
are remarkably small. The breasts are small, the nipples and areolæ
undeveloped.
In other cases, notwithstanding the delay in the appearance of the
menarche, the genital apparatus is developed to a degree quite in
correspondence with the age, but some pathological condition is
present, for instance, the mucous membrane secretes excessively,
exhibits a catarrhal tendency, there are erosions at the os uteri, etc.
Pathology of the Menarche.
A series of disturbances of function and pathological changes in
the organs may occur at the time of the menarche, either directly
connected with the genital organs, or etiologically dependent upon
the changes occurring in these organs.
The commencement of menstruation, as we have already mentioned,
may itself be abnormal in character, being either precocious
(menarche precox), or retarded (menarche tardiva). But even
where menstruation begins in a normal manner, the period of the
menarche may be disturbed by a great number of pathological
phenomena, of which the developmental processes occurring in the
genital organs of the young girl must be regarded as the cause.
First of all, the menstrual hæmorrhage itself may be abnormal in
amount and duration. Then, again, functional disturbances of the
most various character may occur: especially prominent are, disturbances
83of hæmatopoiesis, of the cardiac functions, and of the
nervous system, and constitutional anomalies, which deserve attentive
consideration; in addition we have to mention disorders of
digestion and disorders of the sense-organs, among which latter
certain changes in the skin especially deserve attention.
The diseases of the female genital organs at the time of the
menarche are very various in nature. Whereas during infancy and
early childhood the uterus and its annexa are in a state of complete
quiescence, so that nothing occurs in them to attract attention,
at the approach of puberty these organs emerge from obscurity, and
the percentage of diseases of the reproductive organs suddenly
rises to a great height. In very young girls, among diseases of these
organs, we observe only malformations, malignant tumors, and
gonorrhœal infections, and these pathological states, even, are quite
rare; but at puberty all this is altered, and we have to do with disturbances
of the menstrual function and their consequences, and
with various inflammatory processes, and the period of sexual maturity
offers us an overplus of diseases connected with the reproductive
system, justifying the epigram of the French gynecologist who
defined a sexually mature woman as “un uterus servi par des organes.”[20]
Anomalies of Menstruation.
Not infrequently, though the catamenial flow has appeared at the
usual age and has for a time been regular, pathological disturbances
of this function ensue.
Amenorrhœa at the time of the menarche may depend on complete
aplasia of the ovaries, associated with a rudimentary and imperfect
development of the uterus. In such girls, the development
of whose reproductive system is thus imperfect, the continually expected
menstrual flow fails to appear, in spite of the fact that a
recurrent menstrual discomfort, evoked by the congestion of the
genital organs, recurs at intervals of four weeks; as, for instance,
colicky pains in the abdomen, irritable, nervous states, and mental
disturbances. Further, amenorrhœa may be due to one of the
various forms of atresia of the genital organs, as for instance to
vaginal or hymeneal atresia. In such individuals the first period
passes by without anything to attract attention. But at the second
period, distress will usually be manifested; and from this time forward,
painful contractions of the uterus will continue to occur at
four-weekly intervals, and to become more violent as period succeeds
period, whilst the menstrual discharge is wanting, or, to speak
strictly, fails to find an outlet. The blood collects behind the seat
of atresia, and the accumulation gives rise to pressure symptoms
84affecting the bladder and the rectum, and ultimately also the sacral
nerves.
Menstruation, after its first appearance in normal fashion, may
be suppressed in young girls in consequence of mental impressions,
such as sudden fright; such cases are observed after an escape from
a fire, or after a railway accident. Mental stimuli of less intensity
but longer duration have a similar effect; sometimes these take the
form of auto-suggestion. A well-known instance of the latter
phenomenon is furnished by the case of a girl who, in consequence
either of actual intercourse or it may be merely of too intimate an
embrace with a man, fears she has become pregnant, and actually
suffers from amenorrhœa though pregnancy does not really exist.
I saw a case in which amenorrhœa was thus produced in a girl
seventeen years of age, whose ideas on the process of sexual intercourse
were still far from clear. She had permitted a young man to
kiss her repeatedly and fervently, and to clasp her in a close embrace.
She was then afraid that she had become pregnant; the
catamenial flow, which had been regular since she was fifteen years
old, ceased to appear; and it was not until at length I was consulted,
was able to assure myself that the girl was essentially virgin, and
was, therefore, in a position to reassure her as to her own condition,
that menstruation again became regular.
Functional amenorrhœa may also occur in young girls in consequence
of a sudden change in the conditions of life, a removal from
town to country, for instance, or the reverse, travel in regions where
the climatic conditions differ widely from those hitherto experienced,
or a change from an active to a sedentary kind of occupation. Of
this nature is the following case observed by Winter: Miss Q.,
aged 20; menstruation began at the age of 13 and was regular thereafter;
on three successive occasions amenorrhœa occurred during a
visit to Berlin, in one case lasting 3 months, another 2 months,
and a third 6 weeks, whereas when at home menstruation was regular
though somewhat scanty. There were no molimina. Examination
showed the wall of the uterus to be thin, length of this organ 7
centimetres (2¾″), both ovaries distinctly palpable. Such a form
of amenorrhœa as this, commonly disappears when the girl removes
from the conditions unfavorable to the fulfilment of her
sexual functions to the conditions favorable to that function.
Not infrequently a chill is in young girls the cause of suppression
of the menstrual flow that has hitherto been quite regular, especially
effective in this respect being, standing in cold water, getting
the feet wet, the influence of rain and wind at the menstrual period
on the insufficiently clothed lower extremities, and vaginal injections
with water at too low a temperature. Such cases are common
85among the working classes, especially in washerwomen; but they are
also observed among the well-to-do. An example is given by
Winter: Miss H., aged 19; menstruation began at the age of 13,
regular, at intervals of 4 weeks, the flow lasting 2 to 3 days, and being
normal in amount. Several years ago the patient caught a severe
cold through paddling in cold water during the period. Suppression
of the menses resulted, amenorrhœa being complete for a year and
a half. Then menstruation recommenced, but was irregular, sometimes
anticipating, sometimes postponing the proper period, the
interval being occasionally as long as four months; when it occurred,
the flow was represented by a drop or two of blood only, and dysmenorrhœa
was severe. At each proper period, if the flow failed to
appear, severe molimina occurred in the form of abdominal cramps
and headache. Examination showed the uterus to be normal in
shape, 4½ centimetres (1¾″) in length, with a very thin wall; both
ovaries were palpable, but smaller than normal.
The commonest form of amenorrhœa at this period of life is,
however, the constitutional amenorrhœa associated with chlorosis.
In chlorotic subjects we have to do, not with a symptomatic absence
of the menstrual discharge, but with a failure of the ovarian
function, the graafian follicles failing to ripen. We generally find,
according to Gebhard, that chlorotic girls begin to menstruate at
the usual age, or even earlier. Menstruation recurs once or twice
at irregular intervals, and then gives place to complete amenorrhœa,
it may be suddenly, it may be gradually, the flow on each occasion
being scantier than before. In chlorotic patients, the menstrual
discharge, when present, is very thin and watery, and often contains
a large admixture of mucus derived from the cervical canal
and the cavity of the uterus. The amenorrhœa may be of short
duration; or it may last for a long time; so that it is not until after
the lapse of months or years, and as a rule in consequence of suitable
treatment, that menstruation recurs, being henceforward either
normal in frequency and strength, or on the other hand permanently
scanty and of the postponing type. The associated disorders from
which the patients suffer take the form of headache, dizziness,
syncope, feelings of oppression, disinclination for mental and physical
exertion, and so on. Since in such cases the ripening of the
ovarian follicles also fails to occur, when the amenorrhœa is complete
the menstrual molimina are generally wanting (Gebhard).
Stephenson also states that in girls who have been chlorotic for
a longer or a shorter time, menstruation frequently begins very
early, in any case earlier than in healthy girls.
Usually in these cases various other disorders are associated with
the amenorrhœa, such as colicky pains in the abdomen, sensitiveness
86of the abdominal wall to contact or pressure, headaches, attacks of
hemicrania, general mental depression, and hysterical manifestations.
In chlorotic girls, at the times when menstruation is due, a watery
discharge often occurs, sometimes slightly tinged with blood. Dysmenorrhœa
may also occur at such times.
Attacks of menorrhagia in young girls are usually dependent on
disturbances of the nervous system. Sometimes such an attack
occurs at the very first menstrual period. Occasionally also
menorrhagia may occur in association with chlorosis, to be distinguished
according to Virchow from a rare condition named by
him “menorrhagic chlorosis,” characterized by excessive menstruation
of an anticipating type. The bleeding is in such cases seldom
very profuse, however, but the periods are very long, and the intervals
exceedingly short. Castan regards such profuse menorrhagia
and metrorrhagia occurring in young chlorotic girls, especially at
the commencement of puberty, as of an endoïnfective nature dependent
upon auto-intoxication. The toxins lead to inflammatory
and degenerative changes in the muscular substance of the uterus.
According to Frænkel in these cases the ovaries are usually enlarged,
seldom smaller than normal.
Frœlich has discussed this subject exhaustively in his monograph
on Menorrhagia of Young Girls and Hypertrophy of the Cervix
Uteri.[21] He states that the cases of menorrhagia in young girls
at the time of the menarche may be arranged in two groups. In
one of these the patients are chlorotic, and menstruation is normal
neither in amount nor in duration, but it is the long continuance
of the flow rather than its profuseness that gives rise to danger;
in the cases belonging to the other group the patients are in excellent
health at the commencement of puberty, but menstruation soon
takes the form of long-continued and profuse menorrhagia. Cases
of the latter kind are due to hypertrophy of the cervix uteri and
fungous metritis. Such attacks of menorrhagia in young girls are
seen also in cases of infectious disorders, as in smallpox, measles,
scarlatina, and above all, influenza. The hæmorrhage often begins
in the first days of the infection, and even during the period of incubation,
one or two days before the appearance of the general
symptoms. If the patient is attacked by influenza while menstruating,
the menstrual flow may assume the character of a true menorrhagia.
More often, however, in such cases, we have to do with
an extra-menstrual hæmorrhage, such as may indeed be observed in
girls who have not yet begun to menstruate.
87
Inflammatory Processes.
Chronic metro-endometritis, both corporal and cervical, occurs
occasionally in young girls during the years of development. It
is especially common in chlorotic subjects; and next to these in
girls who are careless about the observance of hygienic precautionary
measures during the menstruation. Thus it may result from physical
exertion among the working classes; and from dancing, skating,
riding, or mountaineering, among girls belonging to the well-to-do
classes, during menstruation. Again, we meet with it in girls who
work very hard at the sewing-machine; and, finally, in those who
have long practiced masturbation. Through uncleanliness at the time
of menstruation, the blood with which chemise and drawers are
stained and the pubic hair soiled, undergoes decomposition, and
this may lead to catarrhal inflammation of the vulva and vagina and
of the endometrium. The most striking symptom in persons thus
affected is the discharge of mucus, which in cervical metro-endometritis
leads to a very moist condition of the external genitals,
and leaves greenish-yellow spots on the under-linen; in corporal
metro-endometritis the discharge is of a thinner consistence, milky
in appearance, and not very abundant. As a result of the endometritis,
the patient suffers from various pains in the body, a feeling
of fulness, sacrache, general sense of fatigue, and diverse nervous
manifestations; sometimes also from dysmenorrhœa, strangury, or
obstinate constipation. In consequence of the great thickening of
the mucous membrane that often occurs, menstruation becomes very
profuse and long-continued, lasting from one to two weeks.
A form of chronic vulvitis, sometimes, though indeed quite rarely,
met with in girls at this time of life, is inflammation of the external
genitals dependent on masturbation. As characteristic signs of this
we may observe an elongation of the nymphæ, the clitoris, or the
præputium clitoridis, and at the same time on the inner surface of
the greatly stretched labiæ we may notice a great increase in the
sebaceous glands, so that the yellowish spots formed by these structures
may be seen beneath the mucous membrane with the unassisted
eye—the mucous surface, indeed, may be slightly uneven in consequence
of their enlargement, so that they resemble small retention-cysts.
The mucous membrane of the vulva between the margin of
the hymen and the nymphæ is moreover, according to Veit’s description
of masturbatory vulvitis, often beset with small pointed excrescences,
the soft furrow between the clitoris and the external
orifice of the urethra being very commonly marked by swelling of
the mucous membrane and the presence of these little outgrowths;
but sometimes also the parts lying to either side of the urethral
orifice may exhibit similar changes. These small structures differ
88entirely from pointed condylomata—they do not branch, they occur
only upon the vulval surface proper, not upon the parts exhibiting
the characters of true skin, and they are non-infecting. More particularly,
it must be remembered, we find these changes principally
in virgins in whom on account of obscure symptoms an examination
of the genital organs has been undertaken, and who suffer in
addition from nervous and hysterical manifestations. The hymen,
when intact, as it usually is in these cases, furnishes objective evidence
that sexual intercourse is not the cause of the patient’s trouble,
and indeed a distinctly ascertainable cause is hard to find. The
patient usually exhibits abnormal sensitiveness and excessive
prudery. Veit is of opinion that the association of all these symptoms
justifies the diagnosis of masturbation as the exciting cause of the
chronic vulvitis; in such cases we may at one time find the mucous
membrane pale, but at a later examination fiery red, and we often
see a clear, transparent secretion exuding from the ducts of Bartholin’s
glands.
In consequence of long-continued masturbation, other pathological
changes may take place in the female genital organs, such as
hypertrophy of the nymphæ, proliferation or glandular hypertrophy
of the uterine mucous membrane, ovarian irritation, pains
in the ovarian region which, in severe attacks, may radiate to the
thighs. These pains become more severe at the menstrual period,
especially at the beginning of that period; and are sometimes also
especially troublesome in the middle of the intermenstrual interval,
in this case usually as a result of great bodily exertion.
These morbid processes in the genital organs of young girls
have long attracted the attention of physicians, and it is more than
sixty years since Bennet described the “virginal metritis” observed
by him in twenty-three virgins. Bonton published in 1887 a monograph
on this condition. Gallard assigns masturbation as its
principal cause.
Retroflexion of the uterus is also sometimes observed in virgins,
induced by the bad habits which are so common in young girls of
retaining the urine for excessively long periods and of neglecting
constipation. The prolonged distension of the bladder leads to a
daily, long-continued stretching of the ligamentous apparatus of
the uterus; the full bladder presses the uterus backwards, and after
the viscus has been emptied, the flaccid ligaments are no longer
able to restore the uterus to its normal position of anteflexion.
The organ is left with its fundus directed backwards, and the intra-abdominal
pressure keeps it permanently in this position; at the
same time, an accumulation of fæces in the rectum, by pressing
the cervix forward, favors this displacement of the uterus. Moreover,
when the uterine tissues are flaccid through malnutrition in
89chlorotic or anæmic subjects, the organ yields more readily to
mechanical influences than it would if its muscular tone was healthy.
Disorders of Hæmatopoiesis.
Chlorosis is in general rightly regarded as a disease of the period
of puberty etiologically dependent on the processes that at this
time of life occur in the genital organs. Its appearance generally
coincides with the menarche, occurring at the age of 14
to 16, or even later, at the age of 19 to 21. As regards the
composition of the blood in chlorosis, investigations have shown
that its hæmoglobin-richness is always diminished; its specific
gravity is proportionately lessened, but the specific gravity of the
serum is normal. The erythrocytes are normal in number, or
only slightly diminished; their shape is sometimes normal, sometimes,
however, poikilocytosis is present. The leucocytes are generally
normal both as regards number and form; myelocytes (Markzellen)
are also described as present in the blood of chlorotic
patients (Neusser, Hammerschlag, Gilbert, Weil); the blood-plates
are normal in number, the alkalinity of the blood also normal, the
isotonicity of the erythrocytes rather low.
The relation of chlorosis to the menarche is variously explained.
Kahane, in his elaborate monograph on chlorosis, regards it as an
independent disease belonging to the group of “disorders of vegetation”
(Kundrat), one which “according to its essential nature is
an expression of the disharmony that obtains between the congenitally
inefficient hæmatopoietic apparatus and the demands made
upon the feminine organism by the processes of puberty.”
An insufficiency of the hæmatopoietic organs as regards their
functional capacity is believed by Kahane to be in the case of women
so far physiological inasmuch as their blood is inferior to that of
men in hæmoglobin-richness and corpuscular richness to the extent
of about 10 per cent. In this way the predisposition of the female
sex to chlorosis may perhaps be explained. A further fact which
must be taken into consideration is the difference between the development
undergone by the respective sexes at puberty. In the
female sex, this development is quickly completed, and has the
characteristics of a revolution; but in the male, the development is
a more gradual one, and has the characteristics of an evolution.
F. A. Hoffmann also regards chlorosis as associated with the
development of the uterus and the establishment of menstruation.
It is possible that these processes exercise some reflex influence;
but we must also remember that the chemical processes involved
in the growth and maturation of the ovarian follicles are still insufficiently
understood, and that it is quite possible that these too
90may have powerful and unaccustomed effects on the organism such
as may well disturb metabolic processes of a somewhat unstable
character.
Grawitz, who regards chlorosis as a vasomotor neurosis in which
disturbances arise in the interchange of fluids between the tissues
and the vessels, refers the appearance of chlorosis at puberty to the
general disposition to disorder exhibited at this age by the vasomotor
system.
Other authors consider chlorosis to be an ovarian auto-intoxication,
believing that under certain conditions the ovaries give off
into the organism certain poisons; or, on the other hand, supposing
that a certain antitoxic function, normally possessed by the ovary,
fails. Von Noorden, for instance, regards chlorosis as a disorder
of blood formation referable to a disturbance of the internal secretion
of the ovary during the developmental period.
Blondel, who also regards ovarian auto-intoxication as causal,
is of opinion that chlorosis is induced by products of decomposition
formed in the organism during the process of growth. As in
childhood the thymus gland, so later in life the ovary, renders these
products innocuous. When this peculiar functional activity of the
ovary is retarded in its appearance, the intoxication effected by the
products of decomposition formed during the process of growth
gives rise to chlorosis.
Meinert, in an interesting manner, brings the harmfulness of
wearing a corset during the years of development into etiological
relations with chlorosis. In the transitional period between childhood
and the age of puberty the wearing of the corset usually begins.
Now Meinert discovered that in chlorosis, as a result of wearing
a corset, a vertical or subvertical position of the stomach ensues
as a partial manifestation of enteroptosis, leading to tension on the
abdominal plexus of the sympathetic, which in turn results in changes
in the blood, and other nervous symptoms. According to this view,
chlorosis is a peculiar general neurosis dependent upon an artificially
induced gastroptosis; this form of enteroptosis being due, not to
relaxation of the suspensory ligaments of the abdominal viscera,
but to pressure exercised by adjacent organs in consequence of a
change in the form of the thorax, which has been permanently
constricted by tight-lacing (fixierter Schnurthorax).
Of importance is the fact that in girls suffering from chlorosis a
condition of hypoplasia of the genital organs is not infrequently
met with. It would seem, not only that imperfect development of
the female genital organs may be a cause of chlorotic changes in
the blood, as appears possible in view of the relations between the
ovaries and the hæmatopoietic organs through the intermediation
91of the sympathetic system; but also that genuine chlorosis and the
anomalies of the genital organs met with in this disease, may perhaps
be common manifestations of some more general disturbance.
According to Virchow, two distinct forms of chlorosis are to be
recognized, one form in which no great abnormalities of the reproductive
apparatus exist, and another form in which imperfections
in the development of the central portion of the vascular system
are associated with similar imperfections in the reproductive apparatus.
In many cases of chlorosis, he found the ovaries small and
imperfectly developed, in an infantile condition; in other cases,
however, they were three times the normal size; the development
of the uterus in such cases usually corresponds with that of the
reproductive glands. With regard to the etiological connection between
chlorosis and developmental disturbances, Virchow inclines
to the view, that in chlorosis a predisposition, either congenital or
else acquired in early youth, must be assumed to exist, but that this
does not manifest itself by the production of actual disorder until
the arrival of puberty; and he considers it likely that primary deficiencies
of the blood and the vascular apparatus hinder the development
of the reproductive apparatus.
Stieda found that in chlorotics displacements of the uterus were
common, with abnormal narrowness of the vagina, absence of the
pubic hair, imperfect development of the pelvis, and the growth
of the breasts interfered with to this extent, that the nipples and
areolæ were abnormally small. He classifies these manifestations
as disturbances of development in the sense that they are among
the so-called stigmata of degeneration. If in chlorotics the breasts
in certain cases have a normally full and rounded appearance, this
appearance is sometimes deceptive, the fulness being due, not to a
proper growth of the parenchymatous mammary tissue, but to an
excessive deposit of fat. Genuine chlorosis, therefore, not referable
to some other primary disorder, is a developmental disorder, in the
sense in which various other stigmata of degeneration met with
in the human body are developmental disorders, and is indeed frequently
associated with other stigmata of degeneration, or with malformations
due to arrest of development, as for instance, an infantile
type of pelvis or of genital organs, abnormalities of the
cranial bones, vaulted palate, the root of the nose broad and depressed,
extreme prognathism.
Hegar also maintains the view that chlorosis is in most cases a
developmental disturbance, the origin of which is not limited to
the so-called years of puberty; it often arises from noxious influences
which are either strictly inherited or began to operate when
the infant was still in her mother’s womb. Frænkel is inclined to
92regard a primary developmental disorder of the genital organs as
the cause of many cases of chlorosis.
Recently, Breuer and Seiler have undertaken experiments on
bitches, which they spayed at the outset of puberty, and from
the results of these experiments it seems probable that a disordered
influence exercised by the ovaries on the blood plays a part, at least,
in the pathological mechanism by which chlorosis is induced.
The intimate relationship believed to exist between chlorosis and
the sexual life of woman finds expression in the opinion, which
dates back to the days of antiquity, and has been widely held even
by physicians, that the disease (hence designated morbus virgineus
or febris amatoria) is due to sexual abstinence in individuals with
powerful sexual impulse, and that for this reason chlorosis is often
cured by marriage. This result of marriage, which, though apparent
merely, may indeed often be witnessed, is explained by
Kahane on the ground, that in very many cases, the symptoms of
chlorosis become less severe after the first five years have elapsed
since the commencement of puberty, the improvement occurring quite
independently of the marriage or continued celibacy of the sufferer.
The influence of marriage in curing chlorosis is thus apparent
merely to this extent, that a very common age for marriage in
women is precisely in the twentieth, twenty-first, or twenty-second
year, when five years have passed since menstruation began. By
this time the organism will to a large extent have become accommodated
to the demands made upon it by the processes of puberty.
Experience also shows that chlorotic girls sometimes continue to
suffer from the various symptoms of chlorosis even after they have
become wives, and that chlorosis is not infrequently rendered more
severe by the puerperium—but in a wife it is no longer customary
to describe such symptoms by the name of chlorosis, they are called
anæmia, hysteria, nervousness, etc. Further, in order to give the
doctrine of morbus virgineus its death-stroke, Kahane directs attention
to the fact that numerous cases of chlorosis are met with in
young girls who are far from practicing sexual abstinence, especially,
for instance, amongst the lower classes, amongst whom it is
hardly customary to wait for marriage before beginning sexual intercourse.
The connection between masturbation and chlorosis,
which has also been widely alleged from the etiological standpoint,
is moreover one that cannot be admitted. On the other hand it is
easy to understand that the erotic reveries which are so often seen
in chlorotic girls are very likely to induce the habit of masturbation.
In young girls at the time of the menarche, especially in those
who suffer from amenorrhœa or from irregular menstruation, the
anæmic form of obesity not infrequently develops. Such patients
93at the time of puberty exhibit signs of marked anæmia in association
with a notable increase in fat. The skin in such cases is always
strikingly pale and of a whitish-yellow color; in bodies which are
in other respects beautiful the bust may have the appearance of a
marble statue. Such girls are strikingly stout, but the fatty tissue
is flaccid, soft, and spongy, and dependent parts readily become
œdematous; the muscular system is generally feeble.
What especially characterises this anæmic form of lipomatosis in
young girls is, that, even in mild forms of the affection, cardiac
symptoms are apt to become prominent. Frequent and violent palpitation
will occur even in the absence of any severe exertion or
especial excitement, often also we see shortness of breath, precordial
pain, anxiety, respiratory distress, and sensations of chilliness
and fatigue.
The principal cause of the obesity in these cases is to be found in
the anæmia, inasmuch as the diminution in the number of the erythrocytes
is a diminution in the number of the oxygen-carriers, and this
entails defective and insufficient oxidation. The deficiency in the
albuminous constituents of the body also gives rise to a rapid and
extensive deposit of fat, the power for the combustion of the fats
absorbed from the food being insufficient. An auxiliary factor in
producing obesity in such anæmic girls is their disinclination to
physical exercise, dependent on the speedy onset of sensations of
fatigue. The long-continued repose of the muscles, and the remaining
almost continuously in close rooms insufficiently supplied
with oxygen, also result in the withdrawal from the blood of the
circulating fat and its deposit as adipose tissue.
Albuminuria at the time of the menarche is a disease of development
which is not infrequently met with in chlorotic girls, as in
adolescent boys. On examination of the urine in such young girls
we detect the presence of a variable quantity of albumin, which is
present especially after severe physical exertion, mental application,
or emotional excitement, whilst the urine secreted at night is usually
free from albumin. The skin is pale, the accessible mucous surfaces
are comparatively colorless, the face is puffy, the eyelids are
œdematous; the patients suffer from various nervous troubles, especially
headache and dizziness, and they are also liable to dyspeptic
disorders.
The cause of this albuminuria of puberty is according to von
Leube in part disordered hæmatopoiesis, in part a slight degree of
cardiac insufficiency with a tendency to stasis. At the time when the
processes of development and the growth of the body in height are
most active, there is not a corresponding increase in the energy of
hæmatopoiesis, and the heart also fails to keep pace with the growth
94of the body and to meet the demands thus made upon it by vigorous
growth and increased energy. In general the capacity of the heart
in such individuals is indeed sufficient to maintain the circulation
through the kidneys; but as soon as the functional activity of the
heart is more strongly taxed and the energy of the circulation consequently
declines, albuminuria occurs—and occurs all the more
readily in consequence of the fact that, the hæmoglobin-richness of
the blood having been lowered by the customary anæmia, the epithelium
of the renal glomeruli is badly nourished and functionally inadequate.
When the period of the menarche is safely passed, when the
menses recur with regularity, and the chlorotic manifestations disappear,
when the process of hæmatopoiesis has improved in quality,
and the growth of the body is completed—when, in short, the functional
equilibrium of all the vital processes becomes re-established,
the albuminuria of puberty ceases. It seems, however, that those
who have suffered in this way are predisposed to a return of the
albuminuria at the climacteric period, when the metabolic balance
is once more disturbed.
Cardiac Disorders.
The commonest cardiac disorder at this period of life is nervous
palpitation, occurring in young girls who are in other respects in
good health, being free from anæmia and from any discoverable
disease of the heart or vessels. That this disorder is dependent on
the sexual processes is indicated by the fact that it first manifests
itself in a stormy manner some time, weeks it may be or months, before
the first appearance of menstruation; recurring at irregular
intervals, the attacks continue till after the first menstruation, and
cease soon after the regular return of the period. Objectively, the
palpitation of the heart manifests itself by an increase in the frequency
and strength of the cardiac impulse, and increased frequency
and tension of the pulse; in a few cases, however, it is perceived
subjectively only by the patient, as a distressing sensation of excessively
frequent and powerful cardiac action. In the former group
of cases, the enhanced activity of the heart is perceptible, not only by
auscultation, by which we usually find the heart-sounds quite pure,
but also by inspection, which shows us the violent agitation of
the thoracic wall and increased pulsation of the carotids. On percussion,
no change is found in the area of cardiac dulness. The
frequency of the pulse is increased, usually reaching 120 to 140
beats per minute; it is full, and may be intermittent or irregular.
In those cases in which the palpitation of the heart is a purely
subjective sensation, we find no increase either in the frequency or
95in the strength of the pulse, which may indeed be less frequent
than normal. With the palpitation is associated a sensation of
strong pulsation in the great vessels of the neck, and often there
is pain on the left side of the lower part of the chest, with a sensation
of shortness of breath, respiratory distress, precordial pain, and
a feeling of pressure upon the chest. Respiration is shallow, and
abnormally frequent. The attacks of palpitation recur daily in some
patients, in others at intervals of several days; they may occur
entirely without exciting cause, or with a cause so trifling that it
would not in a normal subject have produced any nervous excitement;
the duration of the attacks varies from a few minutes to several
hours, and they may occur either by day or by night; in the
intervals between the attacks the functions of the heart and the
arteries are conducted in a normal manner. The pulse-curves I have
obtained during the attacks of palpitation, in those cases in which
the manifestations were objective as well as subjective, exhibit a
high pulse-wave, the upstroke being rapid and steep, the downstroke
also sudden and steep, the predicrotic elevation but little
marked, the dicrotic elevation often very distinct.
Less frequent than such attacks of palpitation recurring at irregular
intervals are paroxysmal attacks of tachycardia, in which
the frequency of the heart and pulse is increased to an enormous
extent. This disorder manifests itself a little time before the first
appearance of menstruation, thenceforward recurring regularly
every three or four weeks, accompanying menstruation, or occurring
at the proper menstrual period if menstruation is in abeyance; the
attacks last several days. This trouble also disappears a few months
after the establishment of menstruation.
Associated with these cardiac troubles are, not constantly indeed,
but in the majority of cases, disturbances of the digestive organs.
From the heart-troubles already described, another group of cases
must be distinguished, which are also observed at the time of the
menarche. They occur in girls in whom the first appearance of
menstruation is strikingly delayed, not having yet begun at the
ages of 18, 19, or 20 years, or in whom considerable irregularities
have occurred in connection with the commencement of menstruation.
In such girls, in whom menstruation has appeared late and
been irregular, or who are perhaps entirely amenorrhoeic, cardiac
troubles may be so pronounced that the physician may be led to
suspect the presence of organic disease of the heart. The most
prominent symptom is frequent and violent palpitation, with strong
pulsation in the carotids, respiratory distress, and feeling of anxiety,
on continued exertion or even on very slight occasion. On percussion,
the heart is not found to be enlarged; on auscultation, the heart-sounds
96are found to be very loud, often with a systolic murmur in
the mitral region, whilst over the lower end of the internal jugular
vein, the humming-top murmur (bruit de diable) is audible. The
pulse is increased in frequency, at times arhythmical, and easily compressible.
The sphygmographic tracing usually shows a subdicrotic
or dicrotic character. The upstroke is not high; the downstroke
descends low, almost to the lowest level of the curve, before the
enlarged dicrotic elevation begins. The skin is always strikingly
pale, pale also are the visible mucous surfaces, the hæmoglobin-richness
and the corpuscular richness of the blood are considerably
diminished, a feeling of fatigue and various other nervous manifestations
are constantly present—in short, in all cases we have to
do with the well-known chlorotic disposition, sometimes in association
with the manifestations of the anæmic form of lipomatosis universalis.
In several such cases, skin affections were also present.
Some suffered from acne vulgaris of the face with the usual
comedones; others perspired profusely from the palms of the hands
and the soles of the feet; others exhibited a bluish coloration of the
nose and the ears.
There is yet a third form of heart trouble, much rarer indeed
than the forms already described, from which young girls sometimes
suffer at the time of the menarche. It occurs in girls who
just before the first appearance of menstruation have grown very
rapidly, “shooting up to a great height.” They are not anæmic,
nor do they appear “nervous;” but they are extremely thin, and
they have grown enormously in height during the previous year.
These individuals also, who in the previous course of their life
have been free from heart trouble, now complain of cardiac distress.
As in the cases previously described, they complain of severe palpitation,
a feeling of fulness in the chest, shortness of breath on
exertion, etc.; but the results of the objective examination are very
different. The cardiac dulness is increased in area, especially in
vertical extent, the apex-beat may be normal in position or displaced
outwards, the impulse is always heaving, abnormally powerful
and resistant, the heart-sounds, especially those of the left ventricle,
are louder than usual, the aortic second sound accentuated,
sometimes ringing, the carotids pulsate visibly. The radial pulse,
the tension of which is abnormally high, can be compressed by the
finger only with difficulty; sometimes it is jerky in character. The
sphygmographic tracing shows a rapid and steep upstroke; in the
downstroke, the predicrotic elevation is much larger than normal
and also nearer the summit of the curve. Thus we see that all the
signs of cardiac hypertrophy are present, hypertrophy, that is to say,
of the left ventricle.
97The cases of this nature that have come under my observation
have not been in girls of the working classes, but among the well-to-do.
We cannot therefore regard them as due to overstrain of the
heart in consequence of excessive bodily exertions, comparable to
the cases met with in young recruits after long marches and violent
exercise. We must rather assume that the development of the female
genital organs has evoked a storm in the cardio-vascular system,
more especially that in some way an increased resistance has
been offered to the work of the heart, and that thus the hypertrophy
has been brought about; though we may suppose that other unfavorable
influences have also been in operation. Such an influence,
in these cases, is the rapid growth of the body, which makes enhanced
demands on the work of the heart; another is furnished by the almost
universally worn unhygienic article of clothing, the cuirass-like
corset, which offers a rigid hindrance to the rapid growth of the
female body, to the development of the breasts, the thorax, and the
upper abdominal organs, and which fails to accommodate itself to
the changing conditions of growth, so that much extra work is
thrown upon the heart. In such young girls we have very frequently
found tight stays, which were worn unchanged without regard to the
growth of the body in length, and which, by pressure on the epigastric
region, elevation of the diaphragm, and limitation of the respiratory
movements of the thorax, actually offered such considerable
resistances to the driving power of the heart, as ultimately to lead
to hypertrophy of the cardiac muscle.
Summing up our observations, we find that at the time of the
menarche cardiac disorders occur in young girls which may be
arranged in three groups of cases:
1. Nervous palpitation and paroxysmal tachycardia in persons in
other respects in good health, the affection appearing shortly before
the commencement of menstruation, and disappearing soon after the
flow is regularly established.
2. Cardiac disorders occurring in young girls suffering from
chlorosis, which itself results from the processes of the menarche.
3. Cardiac hypertrophy developing at the time of the menarche,
and dependent on the circulatory disturbances associated with that
process, its appearance being favored also by rapid growth of the
girl and by unsuitable clothing (tight lacing).
With respect to the activity of the heart and the circulation of the
blood at the time of the menarche, the little-known observations
made by Beneke, on the growth of the heart and arteries in the
various stages of development, deserve especial attention. According
to this writer, the growth of the heart is slow until the age of
fifteen years is attained, but becomes accelerated at the commencement
98of puberty. During this time of puberty, the blood-pressure
attains its highest level, being comparatively low in childhood and
later in life. The development at puberty of the female heart is
less extensive than that of the male heart, and for this reason
throughout adult life the capacity of a woman’s heart is on the
average 25 to 30 cubic centimeters (1.5 to 1.8 cubic inches) less
than that of a man. In women, also, the great arteries are on the
average somewhat smaller than in men. The various arteries do
not develop with equal rapidity throughout the period of growth;
after puberty the common carotid grows very much more slowly
than the common iliac artery, the former vessel being the only
large trunk which has already nearly reached its maximum size at
puberty.
The comparatively great development which the heart undergoes
at the time of puberty is a phenomenon so important alike in its
physiological and its pathological relations that it deserves the special
designation of the puberal development of the heart; the commencement
and the completion of puberty appear beyond question
to be to a large extent dependent upon this development of the
heart and upon the simultaneous rise in the blood-pressure of the
systemic circulation due to the comparative diminution in the
calibre of the arteries.
In the literature of this subject of cardiac disorders during the
menarche, we find only short annotations on palpitation of the heart
in young adolescent girls, and on cardiac manifestations in chlorotic
subjects. Further, the statistical fact that valvular lesions of the
heart are commoner in women than in men is by many authors explained
on the ground that the disturbances of the time of puberty,
which certainly occur more frequently and are more severe in the
female sex than in the male, play an important part in their causation.
Changes also in the vessel, such as cirsoid aneurysm
(angioma arteriale racemosum), are supposed to be connected with
the sexual processes of this period of life. C. Heine maintains that
in consequence of puberty and of the sexual functions that become
established at this period, a telangiectases will not infrequently undergo
transformation into a cirsoid aneurysm; especially in cases
in which menstruation is scanty and irregular, angiectatic tumors
may exhibit a vicarious periodic increase.
Krieger describes nervous palpitation and also “cramps of the
heart”[22] as occurring in girls who have not yet begun to menstruate,
in the form of prodromal manifestations; similar attacks may occur
also at every menstrual period in girls in whom menstruation is
99fully established. In most of these cases the pulse is increased in
the patients who complain of a sensation of anxiety, and speak of feeling
the heart roll, tremble, or flutter, to which is sometimes superadded
a sensation of sudden cessation in its activity. Not infrequently
there is a blowing adventitious sound, masking or accompanying
the heart-sounds; there are also venous murmurs, especially when
the heart-trouble is associated with anæmia or chlorosis. Of the
cases of pseudo-angina pectoris[22] observed by Krieger, the attacks
occurred as prodromal manifestations before the first appearance of
menstruation in 22 per cent. of the cases, after menstruation was
fully established in 78 per cent. of the cases; as regards the relation
of the attacks, in cases of the latter group, to the menstrual period,
they occurred before the flow in 33 per cent., during the flow in 67
per cent.; menstruation was irregular in 10 per cent. of the cases
under observation, in most of the other cases menstruation had
been irregular, but was now regular.
Hennig records a case in which he observed as a prodromal
symptom before the establishment of menstruation the regular recurrence
of congestion of the pelvic organs associated with cardiac
disorder.
Diseases of the Nervous System.
The extensive transformatory processes occurring in the genital
organs of young girls at the time of the menarche, and the powerful
impression which the new thoughts, hopes, and fears excited at
this period of life cannot fail to exercise on the nervous and emotional
life, will enable us to understand how it is that the appearance
of the first menstruation may give rise, especially in neurasthenic
or psychopathic subjects, to manifold nervous disturbances and
also to disorders of the mind.
Amongst the severe neuroses and psychoses liable to occur at the
menarche in those suffering from congenital nervous weakness, in
those the conditions of whose life are very unfavorable, and in those
affected by some sudden disagreeable and powerful influences, we
may enumerate: Hemicrania, precordial pain, hysteria, and epilepsy;
impulsive manifestations, such as bulimia, longings for
various unsuitable things, kleptomania, and pyromania; severe feelings
of anxiety; various forms of psychoses.
On the other hand, the first appearance of menstruation has sometimes
a favorable influence in girls suffering from nervous or
mental disorder. This is seen, for example, in cases of chorea in
100fully developed, rapidly growing girls who have not yet begun to
menstruate; in such subjects the chorea sometimes disappears as
soon as menstruation is regularly established.
Quite frequently, the first appearance of hemicrania in young
girls coincides with the menarche. According to Warner, hemicrania
made its first appearance:
| In |
1 girl of |
3 to |
4 years. |
| In |
2 girls of |
5 to |
6 years. |
| In |
1 girl of |
6 to |
7 years. |
| In |
5 girls of |
8 to |
9 years. |
| In |
5 girls of |
9 to |
10 years. |
| In |
4 girls of |
10 to |
11 years. |
| In |
2 girls of |
11 to |
12 years. |
| In |
4 girls of |
12 to |
13 years. |
| In |
15 girls of |
13 to |
15 years. |
Toothache, according to Holländer, in the early days of puberty
sometimes exhibits the twenty-eight-day type of menstruation. The
same periodicity has been recorded in cases of vicarious bleeding
from the gums in girls suffering from disturbance of the menstrual
function.
In the period of the menarche and before this period, chorea minor
occurs, as a functional disturbance of the motor region of the nervous
system, and especially in girls is it associated with the processes of
the period of physical development. The statistical data supplied
by a number of authors, Hughes, Pye-Smith, Russ, Sée, and Steiner,
show that the proportion of boys to girls affected with chorea minor
is 1 to 2.8, and that of all ages 49 per cent. of the cases occurred
at the ages of 6 to 11 years, 29.8 per cent. at the ages of 11 to 13
years. In several cases, in quite young girls suffering from chorea,
pathological changes were found in the genital organs. Thus, in
24 out of 27 girls from the age of 9 to 15 years affected with chorea,
Marie found the symptom-complex designated by Charcot as ovarie.
Ovarian tenderness was manifested on palpation, and always on
that side on which the chorea had first manifested itself. Leonard
found in a girl aged eleven suffering from chorea, adhesion of
the præputium clitoridis; after the separation of the prepuce, the
chorea disappeared.
As in respect of various nervous affections, so also in respect of
various mental abnormalities, we witness at the time of the menarche
numerous manifestations confirming the statement that, “no spinal
reflex has such widely-opened and easily accessible paths of conduction
toward the organ of mind, as the sexual reflex.” “The menstrual
process,” continues Friedmann, “is the only bodily process
in relation to which the organ of mind somewhat readily loses the
remarkable stability of its equilibrium.”
In the experience of all alienists, it is, speaking generally, the
inherited psychopathic tendency that especially manifests itself at
the time of puberty; and it appears that this predisposition, the
manifestations of which the resisting powers of childhood have
101hitherto been competent to suppress, undergoes a sudden and stormy
development in consequence of the action of the menstrual stimulus,
leading to the unexpected appearance of mental disorders. The
commonest of these are mania and melancholia of the ordinary type,
the prognosis in first attacks being favorable; next in frequency
to these are the psychoses characterized by fixed ideas, which usually
terminate favorably after a short time; finally, we meet with the
moral psychoses of puberty, and the form of melancholia distinguished
by Kahlbaum as Hebephrenie,[23] the prognosis of which
is very unfavorable, for it speedily terminates in dementia, similarly
to the dementia of puberty described by Svetlin, dependent upon or
associated with premature synostosis of the cranial bones. Very
often we witness at puberty the beginning of the periodic varieties
of mental disorder, which develop into periodic menstrual psychoses,
manifesting themselves regularly at the recurrence of every menstrual
period.
The fact that hysteria often first manifests itself at the time of
the first appearance of menstruation was noticed already by Hippocrates,
who indeed believed that the association was sufficiently
explained by the well-known manifold relations between this nervous
disease and disturbances in the female genital organs. The first
hysterical attack often coincides with the first menstruation; or the
first menstruation may lead to the recrudescence of hysteria which
had manifested itself previously, but had passed into abeyance.
We have to deal chiefly with the minor forms, such as uncontrollable
and unconditioned attacks of laughing and crying, globus hystericus,
clavus hystericus, etc.; hysteria major, on the other hand, is very
seldom observed at the time of the menarche. As regards the frequency
of hysteria at the time of puberty, we append certain statistical
data.
Landouzy found:
| 4 cases of hysteria occurring at the ages of |
1 to 10 years. |
| 45 cases of hysteria occurring at the ages of |
10 to 15 years. |
| 105 cases of hysteria occurring at the ages of |
15 to 20 years. |
| 80 cases of hysteria occurring at the ages of |
20 to 25 years. |
After the age of twenty-five is attained, the frequency of hysteria
declines very rapidly.
According to Bernutz, all the statistical data prove that hysteria
in more than half the cases first manifests itself either just before
or simultaneously with the commencement of menstruation. It
seems also that at the time of puberty amenorrhoeic and dysmenorrhœic
102manifestations may give rise to the development of hysteria.
In girls at this time of life, hysteria seldom takes the form of the
great hystero-epileptic crisis, manifesting itself rather as nervous and
moody states of mind, moral changes, weakness of will, in association
with various forms of anæsthesia, spasm, and paralysis.
On the threshold of puberty the girl with a hereditarily neuropathic
disposition may exhibit a tendency to epilepsy. In such cases,
as Kowalewski writes, the patient has sudden attacks of loss of consciousness,
commonly ushered in by a wild scream; during the attacks,
tonic and clonic muscular spasms occur, the patient is completely
insensible, the pupils are dilated and do not react to light,
the pulse-frequency is increased—in short, the typical phenomena
of an epileptic fit are exhibited. The loss of consciousness lasts
from two to three minutes; and when the girl recovers, she remembers
nothing of what has occurred during the fit. Though consciousness
has returned, the mind is still at first somewhat disordered;
but this disorder soon passes off, the girl becomes calm, and
forgets what has happened. The physician is summoned, but in
ninety-nine cases out of a hundred, he assures the relatives that
“the attack is nothing of any consequence—a simple fainting-fit,
the result of menstruation—a transient trouble merely.” A second
“fainting-fit” disturbs the calm of the parents, but the reiterated
authoritative assurance of the physician that “the trouble will soon
pass away” restores their confidence; and they gradually become
accustomed to the “fainting-fits” from which their daughter suffers
at each successive menstrual period. The daughter marries,
and gives birth to neuropathic and psychopathic children, and every
one wonders what can be the cause of this misfortune. Hence it is
necessary to pay careful attention to these “fainting-fits during menstruation.”
In the great majority of cases they are in fact epileptic
seizures, and as such they must be treated. Binswanger points out
that in such cases, in which epilepsy first appears at the commencement
of menstruation, the attacks may continue to accompany menstruation
for several years thenceforward. Already established
epilepsy is said by some authors, Lawson Tait, Tissot, and Marotte,
for instance, to undergo at puberty in young girls an increase both
in the severity and in the frequency of the attack; Esquirol, on the
contrary, attributes to puberty a favorable influence on the course of
epilepsy, a view held already by Hippocrates.
Not infrequently, attacks of precordial pain associated with tachycardia
occur during the first menstruation. These attacks are
usually of short duration.
Acromegaly, a disease regarded as a trophoneurosis, also requires
mention here, this disturbance of growth being considered by several
103authors, and especially by W. Freund, to be in some way connected
with the development of puberty; the tendency to acromegaly, it is
suggested, is produced by the remarkable transmigration that occurs
at puberty of the energy of growth from its accustomed paths into
new channels. The relations which Neusser has shown to exist
between the ovaries on the one hand and the vegetative nervous
system and the process of hæmatopoiesis on the other, give a certain
amount of support to this hypothesis, even though we have no intimate
knowledge of disturbances occurring in the reproductive system
during the period of development, which might have an influence
in the causation of acromegaly.
Of old and of recent observations on the psychoses connected
with the menarche, there is no lack. From the time of Hippocrates
down to the present day, the authorities have continued to report
cases in which the commencement of menstruation proved the exciting
cause of the appearance of psychoses. Rousseau writes of a
girl at the time of the menarche, who before the first appearance of
menstruation suffered from attacks of melancholia and a tendency
to pyromania, and under the influence of the latter tendency she
twice committed acts of incendiarism.
According to Kirn, the psychoses that manifest themselves in the
first period of the commencement of menstruation, sometimes melancholia,
sometimes amentia in the form of slight and transitory
maniacal derangement, more rarely a katatonic[24] condition, may
precede the menarche, or may accompany or follow it.
A special form of psychosis is associated with the menarche (von
Krafft-Ebing, Griesinger, Friedmann, Schönthal). The influence
exercised by puberty in this direction manifests itself in various
ways, and is the more powerful for the reason that several factors
are in operation, each of which exercises an individual influence
upon the type of the psychical affection; these factors are, childhood,
the development of puberty, and the periodicity of the disturbance
exercised by the menstrual reflex. The last named of these
influences is the most potent. It manifests itself in the following
manner: Certain psychoses which develop before the commencement
of menstruation or during the suppression of the flow, undergo
modification when menstruation appears; further, in the typical
menstrual psychoses of psychopathically predisposed girls, the attacks
recur either at the beginning of each period, or, when the flow
is in abeyance, at the dates when it should appear—the menstrual
stimulus thus being the exciting cause of the successive attacks
in an organ of mind whose resisting powers are deficient; and, finally
104a disturbance in the development of menstruation may be, not
merely the exciting cause, but the efficient cause of the psychosis.
In cases of the last kind, which have been observed by Schönthal
and also by Friedmann, who has described them very fully under
the name of primordial menstrual psychosis, we have to do with
young girls in whom the appearance of menstruation is retarded,
or in whom the flow has been suppressed very soon after its commencement.
The girls were as a rule hereditarily well endowed,
and the psychosis thus appeared without warning, like a storm from
a clear sky. Exactly periodical in form and character, the period
of recurrence being three or four weeks, this psychosis clearly
showed its dependence upon menstruation; the individual attacks
usually lasted a few days only, and were characterized by distinct
mental disorder, in the form either of maniacal restlessness, or of
dominant depression; vasomotor disturbances were very prominent,
with disordered pulse, as for instance, a rapid rise in the pulse-wave
just before the onset of the attack, succeeded during the attack by
a correspondingly rapid decline.
Friedmann enumerates a number of the peculiarities that characterize
these attacks. The general course of the malady is an
exceptionally stormy one. The ultimate cure may coincide with
the definite regularization of menstruation; or, in cases in which
menstruation is restored but remains inadequate, the course of the
disorder may become a gentle undulatory one, the violent stimulus
of total suppression being replaced by a more moderate stimulus—here
also, however, a cure ultimately follows when menstruation
at length becomes free as well as regular. But during the height
of the malady a proper development of menstruation is always
wanting. The total duration of the malady may vary from as little
as two to as long as nine months, or even longer. The cure is, however,
ultimately a complete one. The combination of a disturbed and
delayed development of menstruation with a stormy periodic cycle
of attacks of mental disorder, and the ultimately favorable termination,
constitute according to Friedmann the peculiar characteristics
of this form of puberal psychosis.
Masturbation.
Masturbation is sometimes practised in very early childhood,
being then commonly due to local irritation of some kind, as for instance
when threadworms find their way into the vagina. Itching
results, leading the child to rub the genital organs. This rubbing
produces a pleasurable sensation, and gives rise to repeated masturbation.
But in adolescent girls at the time of the menarche, a vague
impulse arises to handle the genital organs, depending upon cerebral
105processes which are themselves the result of sexual sentiments, of
reading, or of conversations with sexually instructed female friends.
This vague impulse may lead to masturbation, and will do so earlier
and more surely if the girl is a neuropsychopath by inheritance.
The local influence of menstrual congestion, however, also plays a
part in provoking the impulse toward masturbation, since at every
period a hyperæsthetic state recurs in the genital organs.
Girls thus addicted have sometimes a very striking general appearance.
They are pale, with a weary expression of countenance,
their eyes are dull-looking and darkly ringed, their movements are
sluggish, they like to spend a long time in bed—signs, however,
which I by no means wish to adduce as characteristic of onanists.
Temperament and mode of life are decisive in determining the
greater or less frequency of the habit of masturbation in young
girls. Girls of a passionate temperament, those also who from
early childhood have been accustomed to mix much with young persons
of the opposite sex, and those, finally, in whom from conversation
on the subject with female friends or from the perusal of erotic
literature, sexual enlightenment has occurred at an early age, experience
the awakening of the sexual impulse earlier and with
greater force, than phlegmatic girls, than those who have grown
up apart from boys, and than those who have been strictly and carefully
brought up. Masturbation may arise either instinctively or
from instruction.
In young girls masturbation is usually effected by friction of the
clitoris; less often by intra-vaginal manipulation, since this is liable
to lead to injury to the hymen. For the former purpose the finger
may be used; or some other article, such as a knot tied in the nightgown,
or a rounded projection on some article of furniture; in
one case the friction was effected by the naked heel. If two female
onanists come together, they practice tribadism, presently to be described.
Opportunity for this practice occurs especially in institutions
in which young girls occupy a common dormitory, and sleep
together without adult supervision.
An experienced physician, Gutceit, is of opinion that in young
girls of 10 to 16 years of age masturbation is on the whole less common
than in boys of the same age, but that on the other hand from
the ages of 18, 19, and 20 onward, “sexual self-gratification is almost
universally practiced by women, even if it be not always practiced
to excess,” an opinion which cannot, however, be regarded as
conclusive. As consequences of masturbation in the female sex,
this author has observed: Fluor albus, menorrhagia, enlargement
and prolapse of the uterus, pains in one or other ovary, hysterical
paroxysms, great pallor.
106L. Löwenfeld remarks that the manifestations of the sexual impulse
are not normally present in the days of childhood. In consequence
of pathological conditions, especially of such as effect the
genital organs, in consequence of chance impressions, or in consequence
of a bad example, sexual passion may indeed be awakened
in children in its fullest intensity. Normally, however, the distinct
manifestation of the sexual impulse is associated with a certain degree
of development, of ripeness, of the reproductive organs. Physiologically,
sexual passion is entirely wanting in young girls before
the age of puberty.
As regards the act of sexual self-gratification, this author distinguishes
two forms of masturbation: (a) Peripheral-mechanical;
(b) mental (psychical onanism). In the former class of cases, the
sexual orgasm is produced solely or chiefly by mechanical stimulation
of the skin or mucous membrane of the genital organs. In
the female sex, in addition to manual stimulation, an extraordinary
variety of hard and soft articles are introduced into the vagina for
this purpose. Many females effect sexual self-gratification by
rubbing and pressing movements of the thighs one against the other,
in which the clitoris is implicated. In psychical onanism, on the
contrary, as Löwenfeld points out, the orgasm is produced solely
by central stimulatory representations, without the assistance of any
manipulation of the genital organs. The ideas that have this effect
are for the most part lascivious trains of thought or the recollection
of previous sexual experiences, on which the attention is concentrated.
If we wish to estimate the harmfulness of the different
forms of masturbation as regards the mind and the nervous system,
psychical onanism must incontestably be regarded as the most
deleterious.
In the female sex onanism is, in Löwenfeld’s opinion, less widely
practiced than in the male; none the less, it is in the former sex
far commoner than is generally believed, a fact on which Eulenburg
likewise insists. Frequently, also, in females, a congenital neuropathic
tendency plays a part in the causation of masturbation, in so
far as this tendency takes the form of premature sexual excitement
or of excessive intensity of the sexual impulse. In the absence of
this tendency, masturbation rarely leads to the production of well-marked
nervous disturbances, and does so only when practiced to
very great excess. Beard reports that in the powerful and full-blooded
working-class girls of the Irish race, masturbation, even
when practiced for many years, did not result in any notable disorder
to health.
As regards the nature of the nervous manifestations met with
in women as a result of masturbation, there develops, according to
107Löwenfeld, in one group of the cases, the sexual form of myelasthenia,
characterized principally by sacrache and lumbago, hyperæsthesia
and paræsthesia in the domain of the genital organs
(ovarie,[25] pruritus vulvæ et vaginæ, etc.), irritable bladder, coccygodynia,
weakness and paræsthesia of the legs (feelings of fatigue
and chilliness), finally, the onset of erotic dreams. In many cases,
in the course of time, to these symptoms are superadded the manifestations
of cerebral and visceral neurasthenia (headache, insomnia,
nervous dyspepsia, palpitation), so that the clinical picture comes
to be one of general neurasthenia. In addition to the neurasthenic
troubles, manifold hysterical manifestations may occur.
Disorders of Digestion.
Disorders of the digestive apparatus are quite common in girls
during the period of puberty, and usually take the form of nervous
dyspepsia. Disturbances of sensibility predominate, with a sensation
of pressure after meals, sometimes increasing to nausea, retching,
and vomiting, as manifestations of general hyperæsthesia of the
gastric mucous membrane, loss of appetite, a pasty or acid disagreeable
taste, sometimes bulimia, perverse sensations of taste, and
pyrosis. Especially in chlorotic girls, periodic attacks of pain occur,
localized in the epigastrium and its neighbourhood, and exhibiting no
relation to the ingestion of food. The free hydrochloric acid varies
in amount, being now normal, now diminished, sometimes also increased.
In chlorotic cases, the symptoms of round ulcer of the
stomach are sometimes observed. Intestinal activity is usually depressed,
peristalsis is diminished, so that more or less obstinate
constipation is one of the most frequent symptoms.
Hypertrophy of the tonsils at the time of puberty is in some way
related to the menstrual processes, whether by the intermediation
of the nervous system or by that of the blood. Eisenhart quotes
observations made by Chassaignac, of girls eighteen or nineteen
years of age with hypertrophy of the tonsils, associated with retarded
puberty, menstruation having begun late and being scanty, and
the breasts being underdeveloped; in one young girl with tonsillar
hypertrophy, one of the breasts had failed to develop properly, but
after the removal of the tonsils it speedily grew to the normal size.
Diseases of the Respiratory Organs.[26]
Not uncommonly at this period of life the growth of a goitre is
observed. The influence of puberty on the growth of the thyroid
108body has indeed been asserted by several authors; and Neudörfer
maintains that precisely during the period of puberty to this body
must be assigned an important regulatory trophic significance for
the nourishment and growth of the reproductive organs. Steinberger
and Sloan record the observation of cases occurring in young
girls in whom, menstruation having first been regular, but having
been suddenly suppressed in consequence of external noxious influences,
a rapidly growing goitre suddenly appeared.
P. Müller states that in many regions, as for instance in Canton
Berne in Switzerland, where the school children exhibit with extraordinary
frequency a hereditary tendency to the formation of goitre,
during the years of childhood these growths are much less frequent
in girls than in boys. At the time of puberty, however, this relation
is entirely changed. Whereas in boys from this time onward no
further growth of the thyroid body is observed, in girls at puberty
the hypertrophy greatly increases, so that very large goitres are
formed. The same author recurs to the earlier observations of
Heidenreich and Schönlein, as well as to those of Friedreich, by
which this influence of puberty is strikingly manifested, and he believes
it to be established by experience that sexual excitement can
produce a transient swelling of the thyroid body. He alludes also to
the remarkable fact that a swelling of the thyroid body, to which a
number of animals show a tendency, occurs chiefly at the time of heat
or rut; this is especially well known to occur in the case of stags.
Similarly, during menstruation, a transient swelling of the thyroid
body can sometimes be detected; the swelling is greater if the menstrual
discharge fails to occur.
Diseases of the Organs of the Senses.
At the time of the menarche in cases in which there is retardation
or some other disturbance in the regular appearance of menstruation,
affections of the eye are observed, which are in part
functional, dependent on reflex influences proceeding directly from
the genital organs without organic changes, and in part are due to
circulatory disturbances. Mooren, S. Cohn, and Power have discussed
the relations between the uterus and the eyes in general, and
also in this especial connection. Of ocular troubles during the
menarche, iridochoroiditis, hæmorrhages into the vitreous body,
long-continued blindness, and pannous keratitis, are mentioned,
which may either disappear with the reestablishment of menstruation
(spontaneous or artificially effected), or may exhibit in
such circumstances a notable alleviation. Chronic inflammatory
states of the conjunctiva, usually of an eczematous nature, which
frequently occur at the time of puberty, often exhibit a relation to
the menstrual process, a monthly exacerbation of the ocular trouble
109coinciding with disordered menstruation, and cure taking place
only when menstruation has become perfectly regular. Vicarious
hæmorrhages into the vitreous body also occur, associated with
disturbances of menstruation, the relapses ceasing as soon as menstruation
becomes regular; such a case was observed by Courserants
in a girl of fourteen years.
Disturbances of hearing have been observed at the time of puberty
in young girls addicted to masturbation; the patients complain of
subjective noises, rising in intensity till actual hallucinations may
be experienced. Lichtenberg reports the case of a strong girl
eighteen years of age, in whom the congestion associated with
puberty was followed by atrophy of the auditory nerve. The same
author, also Ashwell, Law, Puech, Rossi, Stepanow, and Gilles de
la Tourette, have published cases of vicarious menstrual hæmorrhage
from the external auditory meatus, occurring in girls of ages varying
from 14 to 16, 17, 20, and 22 years. Amongst these cases, in some
the auditory organ was in a healthy condition, but in others there
was associated purulent discharge; the bleeding took place from
the ears at the menstrual periods, the proper menstrual discharge
being absent or scanty; after the ear trouble was cured, menstruation
was normal. Of 200 cases of vicarious menstruation, there were,
according to Puech, six in which the vicarious bleeding was from
the ears.
Disturbances of the olfactory sense, taking the form, sometimes
of diminished acuteness of this sense, sometimes of increased acuteness,
and sometimes of perversion, also anomalies in the secretion of
the nasal mucous membrane, either abnormal dryness, or greatly
increased secretion of mucus, come under observation at this period
of life, either as reflex manifestations through the intermediation
of vasomotor nerves at the time of the first appearance of menstruation,
or in consequence of chronic nasal catarrh, which may be connected
with masturbation. In cases in which the menarche is retarded,
vicarious epistaxis may also occur, the bleeding sometimes
being very profuse, in one case, indeed, reported by Fricke, in a
girl seventeen years of age, having a fatal termination. According
to Mackenzie, sexual excitement leads to swelling of the nasal
mucous membrane, and habitual masturbation to chronic nasal
catarrh; the same author asserts that during menstruation, swelling
of the turbinate bodies may always be observed, and that in this
lies the explanation of the fact that many women complain of a
monthly cold in the head as an accompaniment of menstruation.
Diseases of the skin are not uncommon in young girls at the time
of the menarche, and later as an accompaniment of each successive
menstruation. It is a well-known fact that at puberty girls sometimes
lose a hitherto beautiful complexion, and suffer from various
110disfigurements of the skin of the face. These are produced especially
by the profuse secretion of sweat, and by the excessive secretion
of the sebaceous glands, which so often results in acne, an inflammation
of these glands. Ecchymoses also, effusions of blood
into the skin, are observed, especially, as a form of vicarious menstruation,
in cases in which menstruation is irregular. When actual
bleeding occurs from the intact skin, the blood finds its way out
through the sudoriferous ducts—hæmatidrosis occurs; in some
cases, however, the hæmorrhage takes place from areas of skin
altered and injured by disease, from wounds or other injuries, from
ulcers, or from excrescences. Hæmorrhage into the skin occurs
also in the so-called stigmatization, in which condition also an
etiological role has been assigned to menstruation.
In the skin, remark Spietschka and Grünfeld, a new life begins
at the time of the development of puberty, and it is this which first
gives to human beings the external characteristics of sexual maturity.
In certain regions which have hitherto been covered only by fine
downy hairs,[27] thick, strong hairs develop, and at the same time the
general growth of hair becomes more active. These regions are,
the genital region, and the axillæ. This increased growth of hair
is accompanied by a stronger secretion of the sebaceous glands,
which very often is in excess of actual requirements, and may thus
lead to cosmetic disturbances and to various diseases of the skin.
Thus arise the various forms of seborrhœa.[28] The commonest of
these is the formation of comedones, which, at the time of puberty,
may make their appearance especially on the nose, the forehead, and
below the corners of the mouth, but also on other parts of the face
or on the back and the breast; in those regions, that is to say, in
which the sebaceous glands attain a considerable size. The retention
of the sebum may give rise to inflammation, which the access
of micro-organisms converts into suppuration. Thus arises acne
vulgaris. In another form of seborrhœa,[28] the secretion is more
fluid in consistence, and collects on the surface of the skin, furnishing
this with an oily covering—seborrhœa oleosa.[28] This most
111commonly occurs on the face; if the fatty layer is removed, the
skin remains dry for a brief period only, and soon becomes greasy
and shiny once more. Dust readily adheres to the greasy surface,
and this gives the face a dirty appearance. Seborrhœa faciei is
readily converted into eczema.
With the puberal development of the external genital organs is
associated an increase in the sebaceous secretion of these regions.
On the clitoris and its prepuce, and on the folds and in the furrows
of the vulva, in consequence of insufficient cleanliness, an accumulation
of sebum and cast-off epidermic scales readily occurs; such
an accumulation may become rancid, may irritate the skin, and
may thus give rise to erosions and to purulent secretion.
In chlorotic girls at the time of puberty, on account of the anæmic
condition of the blood, eczema is not uncommon, especially on the
hands and the face. On the face, or on the forehead, red papules
appear on circumscribed areas, and become vesicular; raw, weeping
spots are thus formed, and have a very disfiguring appearance.
Such eczema may occur also in connection with disturbances of
menstruation, when the menses are scanty and pale, or when dysmenorrhœa
is present.
At the time when menstruation ought to appear, but fails to do
so, sometimes also, when menstruation is regular, with each successive
period, an eruption of urticaria takes place; it usually disappears
quickly, but in some cases is more persistent; owing to the
intense itching it is always an extremely distressing complaint.
Sometimes it takes the form of urticaria factitia, in which the
skin reacts to every kind of mechanical stimulation, such as rubbing,
scratching, or pressure, all of which alike lead to the formation of
weals, which may be diffused all over the body. Less often in association
with disturbances of menstruation, acute œdema or erythema
are observed.
Finally, we must mention herpes progenitalis, a rather uncommon
acute condition in which, with violent itching and burning sensation,
intense redness and œdematous swelling of the skin, vesicles
form on the præputium clitoridis, the nymphæ, and the inner surface
of the labia majora.
Hygiene During the Menarche.
It is the object of rational hygiene to increase the resisting power
of the organism, which has been depressed by the processes of the
menarche, in order that the increased demands made by the awakened
sexual life may be adequately met.
The principal means for this purpose are, suitable diet, a suitable
mode of life, and the employment of physical therapeutic measures,
112among which strengthening and hardening measures are to be preferred.
The diet should be at once as richly albuminous as possible and
readily digestible, there should be several, four or five, meals every
day; in chlorotic patients food should be taken at regular intervals
of two to three hours. Meat should be a predominant article in the
diet, but fresh vegetables should also be eaten in abundance for the
sake of the nutritive salts they contain; the vegetables rich in compounds
of iron, such as spinach, oats, beans, and lentils, are to be
recommended; fruit, raw or cooked, should also be taken in considerable
quantities. The evening meal[29] should not be too succulent
or too plentiful; it may best consist of soft-boiled eggs, an omelette,
or milk. Alcoholic beverages should be avoided or taken in minimal
quantities; only as a stomachic may a glass of beer or of light wine
be recommended.
Chlorotic patients should even at their first breakfast[29] have a
meal rich in albumin, such as a considerable helping of meat, or a
beefsteak, with rolls, butter, and tea or coffee. Milk should be
taken in small quantities only, not more than a pint to a pint and a
half daily; only when solid food cannot be tolerated should milk be
given freely. Beer and wine are often of value in chlorotic girls
from their stimulant action on digestion and circulation. Half an
hour’s rest before and after meals is useful.
For the bill of fare of these patients I recommend especially:
Roast beef and veal, underdone beefsteak à l’Anglaise, ham; roasted
venison, hare, partridge, grouse, fieldfare, hazel-hen, ptarmigan,
pheasant, chicken, pigeon, turkey, oysters; asparagus, cauliflower,
and spinach. For variety, fish or shellfish may occasionally be
taken. Sweetbread in soup or with sauce forms a very delicious
and easily digestible dish.
Kahane recommends for chlorotic patients the systematic use of
Bavarian beer, to the amount of about two pints daily; it should,
he says, be a beer rather dark in tint, full-brewed, rich in malt, but
containing a comparatively small proportion of hops, alcohol, and
carbonic acid. Jaworski has recommended a dietetic iron-beer, containing
4.7 per cent. of alcohol and from 0.0317 to 0.0644 per cent.
of iron.
When girls are at the same time anæmic and very thin, fat-containing
foods must be taken in abundance, such as milk, butter, and
113cream; also large quantities of carbohydrates. Farinaceous foods,
rice, potatoes, arrowroot, sago, tapioca, oatmeal, barley meal, carrots,
turnips, sweet fruits, grapes, dates, pippins, plums, pears, and
preserved fruits—all these must appear at table more frequently
than usual; beverages, in addition to milk, that are suitable are
chocolate and cocoa, Bavarian beer, and sweet, heavy wines.
The diet-table of such thin chlorotic patients should be as follows:
First breakfast, 7.30 to 8 A. M.: Coffee or cocoa with milk, or a
pint of milk, white bread and butter, honey. Second breakfast, 10
A. M.: Half a pint to a pint of milk, egg and bread and butter, or
sandwiches of sausage, ham, or roast meat. Mid-day dinner, 1 P. M.:
Soup, roast meat with vegetables and potatoes, or fish may take
the place of the soup, sweets to follow. Afternoon, 4 P. M.: Coffee
with milk, or a pint of milk, with bread and butter. Supper, 7.30
P. M.: A plate of meat with accessories. Evening, 9 P. M.: A glass
of milk.
In the treatment of the anæmic form of obesity, to which chlorotic
patients of the better classes are subject, in consequence of sedentary
habits and overfeeding, the diet must be so arranged that albumins
predominate, whilst carbohydrates should be given sparingly, and
as little fat as possible. As the average quantities of the food elements
required in such cases, I suggest, 200 grammes of albumin,
12 grammes of fat, and 100 grammes of carbohydrate.
The quantity of fluid taken must be as small as possible, since
the deprivation of water may result in a proportionate increase in
the solid constituents of the blood, and thus increase its hæmoglobin-richness.
The amount of physical exercise taken by young girls at this
period of life must vary according to the circumstances of each
individual case. In general, we may recommend for them much
active movement, especially in the open air, in order to counteract
the effects of sedentary habits and confinement in close rooms.
Chlorotic patients must, however, be careful to avoid overdoing
their exercise, and in some cases it will be necessary to limit the
amount of this very strictly. In severe cases of chlorosis, Nothnagel,
Hayem, and other authorities recommend complete rest in bed
for from four to six weeks. This rest-cure can be carried out as far
as possible in the open air, and can be combined with systematic
massage and the use of passive movements.
114I have drawn up the following diet-table for obese chlorotic
patients:
|
Quantity in Grammes. |
Contains of |
| Albumin. |
Fat. |
Carbohydrates. |
| Morning: |
|
|
|
|
| Beefsteak |
100 |
38.2 |
1.7 |
|
| A cup of tea |
150 |
0.45 |
|
0.9 |
| White bread |
30 |
2.9 |
0.2 |
18.0 |
| |
|
|
|
|
| Mid-day: |
|
|
|
|
| Meat soup |
100 |
1.1 |
1.5 |
5.7 |
| Roast meat |
200 |
76.4 |
3.4 |
|
| Vegetables |
50 |
0.8 |
0.2 |
4.2 |
| White bread |
50 |
4.8 |
0.4 |
30.0 |
| Light wine |
150 |
|
|
1.0 |
| |
|
|
|
|
| Afternoon: |
|
|
|
|
| A cup of coffee |
120 |
0.2 |
0.67 |
1.7 |
| White bread |
25 |
2.4 |
0.2 |
15.0 |
| |
|
|
|
|
| Evening: |
|
|
|
|
| Roast meat |
200 |
46.4 |
3.4 |
|
| Vegetables |
25 |
0.4 |
0.1 |
2.1 |
| Wine |
150 |
|
|
|
| White bread |
30 |
2.9 |
0.2 |
18.0 |
| Total |
1380 |
206.97 |
11.92 |
97.6 |
| Contains about 1300 calories. |
|
|
|
|
For young girls at this period of life systematic gymnastic exercises
are usually valuable, not only for strengthening the muscular
system and improving the physique during these years of growth,
but also for assisting the functions of respiration, circulation, and
digestion. Beginning with the simplest and easiest exercises of
chamber gymnastics, the girl gradually proceeds to more difficult
and elaborate exercises and to the use of medico-mechanical apparatus.
The clothing of young girls at the time of the menarche must
receive attention to this extent, that all articles of clothing should be
rejected which increase the tendency already existing to hyperæmia
of the genital organs or offer any hindrance to the circulation in
general. Above all, the physician must take his part in the contest
so long and so vainly urged against the corset. But further, all
tight clothing, such as restricts the freedom of movement of the
thorax and the abdomen, tight collars, and tight garters—all these
must be forbidden; moreover excessively warm underclothing, of
the lower extremities especially, which may stimulate the genital
organs, must also be prohibited.
115As regards the night hours, a thick feather bed is unsuitable.
The young girl should sleep on a hair mattress, and the bed clothing
should be light. Eight to nine hours sleep is sufficient; in the words
of the English proverb, “early to bed and early to rise, is the way
to be healthy, and wealthy, and wise.”
To live by rule, with regular hours of work and suitable pauses for
rest, is of great importance. Among the well-to-do classes also
care should be taken that the adolescent girl takes moderate physical
exercise for several hours daily; she should go for a good walk, and
not spend hour after hour recumbent upon a sofa in idle reverie.
Sitting for too long a time, whether engaged in sewing or at the
piano, is harmful; working at the sewing-machine is permissible
for short periods only, and is indeed at this period of life better
altogether avoided. Bicycling is also an unsuitable exercise at this
age and readily leads to masturbation. Lawn tennis and croquet,
on the other hand, are very suitable active open-air games; in
winter, skating may be indulged in if proper precautions are taken
against chill; in summer, swimming and rowing. The reading of
light literature should be kept under supervision; equivocal novels,
such as may give rise to erotic reverie and sensual excitement, must
be strictly forbidden. A watch should be kept for any indications
of the habit of masturbation; and if the habit exists, appropriate
measures should be taken.
Hydrotherapeutic procedures and baths are of great hygienic and
therapeutic importance for girls at the menarche. In healthy girls
at this period of life, a cold sponge-bath lasting one or two minutes,
the temperature of the water ranging from 10° to 20° C. (50° to
63° F.), taken either on rising in the morning or immediately before
going to bed, is a valuable means for hardening the whole body;
equally useful are cold shower-baths, lasting from a few seconds up
to half a minute. If the girl is somewhat anæmic, it will be well
for her to take a glass of warm milk or a cup of tea half an hour
before the bath, in order to guard against too great an abstraction
of heat. Cold bathing in rivers, when available, may also be recommended.
In cases in which a considerable degree of anæmia or
chlorosis is present, cold baths and every form of strong mechanical
stimulation by the use of water, douches and the like, are to be
avoided, since we have to fear both excessive abstraction of heat and
overstimulation of the nerves. In such anæmic and chlorotic
patients, either partial washing with lukewarm water or general
lukewarm baths, the temperature of which may be gradually and
cautiously lowered, either on rising or at bedtime, have a refreshing
and stimulating effect.
In girls who are in other respects healthy, but in whom the menarche
116is delayed, and in whom menstruation, when begun, has been
scanty and irregular, cold sitz-baths of short duration, the abdomen
being simultaneously douched from a considerable height, or cold
shower-baths in combination with powerful abdominal douches, are
often of value.
Recently, hot air and vapor baths have been especially recommended
for girls suffering from chlorosis, at first, by Scholz and
Schubert, in association with phlebotomy, but also without this.
Kühne, for example, has seen the most satisfactory results follow
the simple use of sudatory baths in cases of chlorosis; improvement
was manifested by an increase in the corpuscular richness of the
blood, an increase in the hæmoglobin-richness, and an increase in
the body-weight. In cases of chlorosis, Traugott also has seen
favorable results follow the use of hot air baths and the consequent
diaphoresis.
Still more recently Dehio and especially Rosin have recommended
hot baths for girls suffering from chlorosis. In fifty cases of
chlorosis, in which other methods of treatment had given negative
results, Rosin gave three times a week baths at a temperature
of 40° C. (104° F.), lasting at first a quarter of an hour, but later
half an hour. After the bath, in those strong enough to bear it, a
very short cold douche or cold sponging followed; then the patient
had to lie down for an hour. The treatment was carried out for
from four to six weeks. Each bath by itself had a notable refreshing
effect in these patients, and at the end of the course most of the
cases exhibited an improvement in all their symptoms, such as other
methods of treatment had failed to produce.
The favorable influence exercised by these hot baths, as by steam
bath-cabinets, light baths, sun baths, wet packing, and similar
sudorific measures, may in part be explained by the dehydration of
the system that is thus effected; whilst those who maintain the auto-intoxication
theory of chlorosis may regard the diaphoresis as a
means for the elimination of noxious substances from the body.
Bathing in water aerated with carbonic acid may be recommended
for patients suffering from anæmia and chlorosis at this period of
life, for the reason that such baths can be tolerated at a lower temperature
than baths of ordinary water. The natural mineral waters
containing free carbonic acid, and chalybeate waters rich in carbonic
acid, when used as baths, are effective principally in virtue
of the carbonic acid they contain, which stimulates the skin; this
stimulus being conducted by the nervous system from the periphery
to the nerve-centres, is reflected thence, and by irradiation exercises
a quickening effect on all the processes of nutrition. These baths
are usually taken at a temperature progressively reduced from 32° C.
117to 25° C. (90° F. to 77° F.), and each bath lasts from ten to twenty
minutes; they are in most cases taken every other day only. For
young girls in whom the menarche is delayed, also for chlorotic
patients with amenorrhœa and neuralgic manifestations, chalybeate
peat baths are indicated, which influence the peripheral nerves by the
exercise of a gentle yet considerable thermic stimulus. These chalybeate
peat baths have further been shown to increase the hæmoglobin-richness,
the corpuscular richness, and the specific gravity of
the blood, transitorily after each bath, but to some extent permanently
also, a certain increase enduring after the course is over.
Young girls suffering from disturbances of their general health
dependent upon a scrofulous or rachitic habit of body may with
advantage be sent to brine baths, especially to such as are situated
in the Alps or other mountainous regions. These weakly, lymphatic,
scrofulous girls, suffering from scanty or irregular menstruation,
may also practice sea-bathing with advantage, especially at watering
places on the sea coast, where the waves are powerful. In such
cases, however, it is advisable in the first instance to take artificially
warmed sea-water baths, before proceeding to actual sea-bathing.
If the sensibility of a chlorotic patient is so great that she can
endure neither peat baths nor carbonic acid containing mineral
water baths, we must add to the latter, in order to make their action
milder, decoctions of chamomile, wheat bran, malt, and the like.
In cases in which nervous symptoms predominate, with an
apathetic, melancholic frame of mind, aromatic herb baths are sometimes
useful. For this purpose such herbs should be employed as
contain a notable quantity of ethereal oils, such as sage (salvia officinalis),
wild thyme (thymus serpyllum), hyssop (hyssopus officinalis),
wild marjoram (origanum vulgare), rue (ruta graveolens),
archangel (archangelica officinalis), levisticum (levisticum officinale).
Equally useful are the balsamic pine needle baths, for
which the fluid obtained by the distillation of pine needles (pinus
sylvestris), freshly collected day by day, is employed.
As regards the climatic conditions suitable for adolescent girls
suffering from the disorders of the menarche, from the nervous
conditions associated therewith, and from chlorosis, residence either
in the mountains or at the seaside is especially to be recommended.
An altitude of about 1,200 metres (4,000 feet) is the most suitable,
being that at which the peculiar characteristics of mountain climates
are most fully developed. The influence of such a climate on
hæmatopoiesis has to be taken into consideration, as well as its
special influence on the menstrual function.
Even though it cannot yet be regarded as fully determined
whether the increase observed by Viault, Egger, and Mercier, in the
118corpuscular richness and hæmoglobin-richness of the blood in consequence
of residence in a mountain climate, is lasting or merely
transitory, yet it is certain that the hæmatopoietic organs are favorably
influenced by such residence, and that the good results are
augmented by the stimulating effect mountain air exercises on the
appetite and the digestion. Lombard has moreover observed, that
at a high altitude the menstrual flow is more abundant and dysmenorrhœa
is less common. For young girls, therefore, suffering from
irritable conditions of the heart, increased frequency of the pulse, or
increased arterial tension, and for those also in whom the resisting
power of the organism appears deficient, a visit to a mountain health
resort situated amid forests may be recommended. For scrofulous
girls a visit to the coast of the North Sea is especially suitable. For
the slighter forms of anæmia, a sea voyage, in which the benefits of
sea air can be obtained more fully, and for a longer period, may be
advised; but such a voyage is quite unsuitable for those suffering
from severe anæmia or chlorosis.
Such very weakly, intensely anæmic and chlorotic patients should
spend the winter in some southern health resort.
The skin, in which disturbances so readily occur at the time of
the menarche, requires careful attention, all the more because it is
precisely at this age that young girls have the greatest need of their
personal charms. The skin of the face, which is often disfigured by
comedones and acne, must be carefully guarded against the accumulation
of sebum in the sebaceous glands by sedulous washing with
warm water and a good soap. If the seborrhœic[30] process in these
glands becomes at all severe, ordinary soaps are unsuitable, and a
potash soap must be used, such as sapo viridis, or spiritus saponatus
kalinus, which have great power of dissolving fats.
The best way of dealing with seborrhœa is according to Spietschka
and Grünfeld the following: The washing is best effected in
the evenings, when the skin will not again for many hours be exposed
to the fresh air, to wind, or to dust. Pour into a basin about
a pint of warm water and add from one to two teaspoonfuls of
spirit of soap (equivalent to the linimentum saponis of the
British Pharmacopœia) or as much soft soap as can be taken up on
the end of a table-knife. The water is then stirred vigorously till a
good lather is formed, and with the water and the lather the face is
thoroughly washed. The skin must then be carefully dried, and
thereafter it is well to smear it with some greasy material, such as
boric vaseline, in order to prevent the plugging of the pores with
119dust, and to protect the sebum subsequently exuded from dessication.
On the next day the washing should be repeated only if the face
has become covered with sebum within an hour or two after the
first washing. If the exudation is less free, the eyes only should be
washed with fresh water, whilst the rest of the face should not be
wetted, but merely be wiped with a dry face towel lightly dusted
with toilet powder, in order to remove any accumulation of sebum.
The skin of the genital regions must be carefully cleansed, especially
in cases in which there is a tendency to hypersecretion of the
sebaceous glands, to eczema, or to herpes progenitalis; subsequently
it should be powdered, and pads of absorbent cotton-wool dusted
with toilet powder should be placed in the labial furrows.
It is of great importance that in girls at this time of life gynecological
examination should be undertaken only in cases of the utmost
need, and this restriction should be especially inflexible in the case
of girls with a neuropathic predisposition. Instances have been
observed in which a vaginal examination, the introduction of a
vaginal speculum, or the use of the uterine sound, has determined
the onset of a psychosis. Still more does what has been said hold
true of local treatment in gynecological cases. Repeated passage of
the uterine sound, cauterization of the cervix, and the manipulations
of gynecological massage, make a very deep impression upon the
mind of a girl, and give rise to morbid ideas and erotic storms, so
that even in those with a powerful constitution, various neuroses,
neurasthenic states, and even mental disorders may result. If in
such cases, especially in girls of a neuropathic temperament, gynecological
treatment is quite indispensable, a single, though energetic,
operative procedure is to be preferred to a number of successive,
though taken singly less extensive, manipulations of and in the
female genital organs. The importance of this proposition has
been repeatedly established. Saenger, for instance, points out as a
fact to be regretted that uterine cauterization with mild caustics is
far too frequently undertaken; and Odebrecht from the same standpoint
proclaims the advantage of a single curetting as compared with
milder intra-uterine impressions repeated during a course of treatment
lasting many months. On the other hand, the physician must
bear in mind the fact, established by the record of a very large number
of cases, that in women predisposed to psychoses severe gynecological
operations are apt to lead to the actual appearance of mental
disorders, or to the exacerbation of mental disorders which have
previously been very mild or have merely threatened to appear.
Careful consideration is needed, on the one hand as regards the
severity of the disease of the genital organs, and on the other as
regards the resisting power, temperament, and constitution of the
120girl concerned, and in many cases a consultation between the gynecologist
and the neurologist is expedient.
A very powerful influence on the physical and moral well-being
of the girl at puberty is exercised by her domestic upbringing.
The general truth of Gœthe’s saying, that the circumstances into
which we are born exercise a determining influence on the whole
life, being admitted, we have to remember that this applies with
especial force in the case of girls.
The educational views which obtain at the present day among
the upper ten thousand, are by no means calculated for the production
of a woman healthy in body and sound in mind. From the
time when the young girl becomes sexually developed, the claims
which society makes upon her become pressing. Every day, by a
number of stimuli, her curiosity and her desires are directed toward
sexual matters. Visits to museums, picture galleries, and theatres,
the perusal of modern romances, the free mingling of the sexes in
all places of amusement—all these combine to awaken prematurely
an instinct to which the “old fashioned” methods of education
allowed a much more prolonged slumber. In other cases, the
mother’s supervision of the developing girl is hindered and rendered
insufficient because the mother herself is claimed by her society
duties and taken much away from her home. In addition, the
young brain is overburdened with mental work, the modern idea of
the equality of the sexes in matters of love is instilled, and a desire
is artificially evoked, and is matured by a certain idle vanity, to
indulge the “natural” instincts—to manifest sexual passion and
to indulge it to excess—and thus the modesty so natural and so
becoming to young girls is completely lost. Nourished in such a
soil, neurasthenic and hysterical states, disorders of menstruation,
and masturbation, cannot fail to flourish.
In these respects also a change is requisite, and a mode of upbringing
must be inculcated from which everything likely to inflame
the sexual impulse is removed. For the adolescent girl a systematic
alternation of work and recreation must be arranged. From great
entertainments where she will mix with young men, from theatres,
evening parties, and balls, the young girl at the time of the menarche,
at the period when menstruation commences, must as far as possible
be kept away, and such pleasures must be reserved for a more
advanced stage of this period of development. Intellectual overstrain,
the overtaxing of the young head, must be avoided; the
acquirement of knowledge must take place gradually and slowly,
and in a manner adapted to individual peculiarities. Intercourse
with female friends also requires supervision in respect of the
moral characteristics of these latter. Religious reverie must be
121avoided, but also to be avoided is the modern nihilism in respect
of religion and good morals. Books must be carefully chosen in
order that the imagination may remain pure and in order that girlish
illusions may not be prematurely destroyed. Domestic recreations
in the way of games, music, singing, painting, and other forms of
artistic culture, are of importance for the development of a strenuous
faculty for learning. Travel in regions where the scenery is
beautiful, forms a most valuable means for the ennoblement of the
intellect and the emotions.
Additional matters demanding attention are, as already mentioned,
the suitability of the diet, and proper physical exercise. All
stimulating articles of food are to be avoided, the excessive use of
meat is to be forbidden, and a sufficient mixed diet, containing both
animal and vegetable substances, is to be prescribed. Tea and
coffee should be taken as sparingly as possible, and alcoholic beverages
must be absolutely prohibited. The regulation of the bowels
is of great importance. Young girls should accustom themselves
to evacuate the bowels every day at a fixed hour, the best time to
adopt being either immediately on rising or just after breakfast.
Constipation is very apt to lead to the production of irritable conditions
of the genital organs.
We can point out as a happy instance of modern progress that
the practice of certain physical exercises has actually become the
fashion for young girls. Gymnastics, with or without apparatus,
swimming, skating, and lawn tennis, involve a number of bodily
movements advantageous for the health; and in connection with
most of these the enjoyment of fresh air offers an additional favorable
influence. Bicycling, however, at this period of life is open to
many objections, not only on account of the likelihood of direct
injury to the genital organs now in course of development, but also
on account of the impulse it produces toward onanistic manipulations.
Especial attention must be paid to the clothing, regarding which
the requirements of fashion so often conflict with those of hygiene,
the victory, unfortunately, in most cases falling to the former. The
period of the menarche is indeed usually regarded as the proper
time for the young girl to begin wearing a corset, if it has not been
worn before. In this connection M. Runge makes the significant
remark: “As long as bodice and skirt form the two principal articles
of woman’s clothing, the corset or some similar article cannot be
dispensed with. The vicious features in the corset are its constriction
of the thorax, with the object of giving the woman a
‘figure,’ and the introduction into its substance of strips of whalebone
or steel in order to give firmness to the figure. The harm done by the
122former feature, the compression of the abdominal viscera, the corset
liver (lacing liver, constricted liver, Ger. Schnürleber), the movable
kidney, etc.—all are so well known that they need not be particularly
described. But the strong pressure from above has a deleterious
effect upon the internal genital organs also, leading to
passive hyperæmia and to displacements. The ‘bones’ of the corset
take part in the compression, and they replace the functions of the
muscles of the back. If a woman who has long worn a corset lays
it aside later in life, she complains that she is no longer able to hold
herself upright. In consequence of insufficient work the muscles
of the back have become incapable of keeping the back straight.
The corset, then, must neither constrict the body, nor must it contain
‘bones.’ An article of clothing analogous to the corset is,
however, required for the support of the skirt and the petticoats that
clothe the lower limbs. These latter are usually fastened by means
of bands which encircle the body above the crest of the ilium.
In order to give these bands a sufficient hold, this region of the body
is compressed by the corset. The burden of skirt and petticoats is
thus borne by a furrow, above the pelvis and below or in the region
of the asternal or false ribs, which is in great part artificially produced.
All this is bad. In order to avoid the necessity for any
constriction, the petticoats should be fastened to the corset, and this
latter should be supported from the shoulders by means of shoulder-straps
or braces crossing one another behind. No constriction of
the thorax then occurs, and if the corset has suitable supporting
pouches for the breasts, and the wearer is accustomed to hold herself
erect, the figure of a well-formed woman thus attired is far from
unpleasing, and is, above all, natural. If the weight of skirt and
petticoats is too great to be borne by the shoulders, the burden
can be divided, some being fastened to the corset, others tied round
the waist. This method is less to be commended, but may be regarded
as a permissible middle course. If chemise and drawers are
woven in one piece, as in the ‘combination’ under garment, there
is one article the less to be attached to the corset. Recently a
number of corsets and articles of clothing have been made in accordance
with these principles.
“The growing girl, then, may wear a soft corset with shoulder-straps,
made to measure, to which all the garments clothing the
parts below the waist should be made to fasten. It must unfortunately
be admitted that this rational mode of arranging the clothing
cannot be adapted to the ‘low dress’ which etiquette demands
on so many occasions for evening wear, since with the latter the
shoulder-straps cannot be worn.
“It is most unhygienic for women to wear, as they so often do,
123drawers that are widely open. Both cleanliness and the need for an
equable warmth demand that these garments should be closed between
the thighs, not to speak of other reasons.”
In order to diminish the sexual impulse in girls at the menarche,
where this impulse has developed prematurely or is abnormally intense,
and even in later years with the same end in view, it is necessary,
not merely that the diet should be suitable and non-stimulating
and that the educational environment should be satisfactory, but
above all that there should be regular occupation and regular physical
activity. Ribbing rightly calls attention to his experience in dealing
with animals, that equally in the case of the stallion and of the
mare, the whole of life may without difficulty be passed in complete
abstinence from sexual gratification, provided that the diet is suitable,
being neither too rich nor too meagre, and that the animal has
regular occupation of a nature and degree adapted to its powers.
In these animals a certain amount of disquiet, of restlessness, of
sulky irritability, etc., may indeed be noticed at times, but these
manifestations are to be overcome by mingled gentleness and firmness,
aided now and again also by mild chastisement, but altogether
without any severity. “Chastity,” says Oesterlen, “is possible only
when the mode of life is simple and regular, and is characterized by
appropriate self-command and frugality. For this reason it is rarely
encountered in palaces and similar places, in which from youth
onwards every one can do what he pleases; but just as little is it
really practicable amid conditions of lack of culture, rudeness, and
poverty.”
From the point of view of education, what Moreau wrote a hundred
years ago is of importance: “In the ordinary course of nature
the young woman at the time of the first appearance of menstruation
is still in full possession of those amiable qualities of blamelessness
and chastity which we are accustomed to denote by the term moral
virginity. To an honorable and pure-minded man this beautiful
attribute of budding womanhood is much dearer and more estimable
than physical virginity. By libertines only is the latter regarded
as a most valuable possession, since it furnishes a powerful stimulus
to their jaded imaginations. But moral virginity and physical
virginity are not always and necessarily associated, for either can
be present in the absence of the other. Physical virginity may be
destroyed by diverse forms of violence, and yet moral virginity may
remain pure and uninjured amidst its ruins. Thus the two are
widely different one from the other, widely different also are they in
value and significance.”
What Eulenburg says regarding the prophylaxis of sexual neurasthenia
in general is true regarding the sexual life of the girl at this
124period of life. “What is needed,” he writes, “is the control of
educational influences with these ends in view, that, on the one hand,
the sexual excitability of developing youth shall be diminished and
kept within bounds, and that nevertheless, on the other, the urgently
needed enlightenment shall be afforded to the young people at the
proper time and in a suitable form. How these aims are to be
effected cannot be explained in generally applicable propositions.
It is a matter which must be left to the tact of the parents and of
other members of the family, who will be guided by the insight they
have acquired into the mental life of those concerned. * * *.
Children inclined to onanism must be carefully supervised by day
and by night; they must be protected from all stimulating things
and from bad company; in boarding-schools it is the common dormitories
that require the most strict, most careful, and most continuous
control. In the case of auto-onanists, female as well as
male, we must enquire into the possible existence of local stimulating
influences, among which, in both sexes, oxyuris must be mentioned—but
in truth it is rare for such local conditions to be the
exciting cause of masturbation. A healthy mode of life in respect
of clothing, sleep, and diet, and the systematic practice of bodily
exercises to the point of considerable fatigue, are the most effectual
means of counteracting the noxious propensity to onanism.”
A high degree of freedom permitted to girls from a very early age
is, as Rousseau already maintained, by no means favorable to the
preservation of virginity.
A wise mother or a wise instructress can do much towards the
preservation of physical and moral virginity, by enlightening her
daughter or pupil at the right time and in a proper manner as to
the nature of the sexual processes, and their significance for the
whole life of woman. Ignorance in this respect, equally with pseudo-knowledge,
entails many dangers. I regard it as indispensable that
the adolescent girl should in good time learn from her mother the
nature of menstruation, lest she should first receive enlightenment in
an unfitting manner from some more experienced female friend. The
mother should explain that the impending flow of blood is a natural
process, unattended by danger, but indispensable to the sexual life,
and a characteristic part of the process of “growing up.”
The knotty and important topic of how the young girl may best
receive sexual enlightenment from her mother, is discussed by E.
Stiehl in her notable work “A Maternal Duty.”[31] The authoress
points out that this enlightenment must not take place suddenly
and without apparent motive, but that the mother must in a gentle
125and gradual manner introduce to her child the secrets of nature. A
beginning may be made by teaching the child to observe the nature
and growth of plants; then she may be led to interest herself in
the family life of animals; and thus an easy way is found to answer
the questions connected with reproduction—to answer them in a
manner at once true and befitting.
Let the mother indicate to her child the methods employed by
nature for the preservation of the life of the young plant; let her
demonstrate in a flower the stamens and the pistil as male and
female organs respectively; and let her explain how when the
pollen-grain reaches and fertilizes the tiny ovule in the ovary, this
ovule becomes capable of development into a large seed containing
an active rudimentary plant, which latter itself enlarges to become
a new full-grown specimen of its kind. The opportunity may then
be seized to draw attention to the resemblance between the little
ovules in the ovary of the flower and the minute ova by means of
which all animal life reproduces its kind. Proceeding further, an
earnest and thorough introduction to the sanctity and responsibility,
the perils and duties, of the sexual life, is urgently required by the
young girl before she proceeds either to marriage or to an economically
independent mode of life.
Not only in America and England, but now also in Germany,
there exist excellent books which may actually be put into the
growing girl’s own hands, by means of which she will be introduced
in an intelligent manner to a knowledge of the method of
reproduction in the human species.
Often enough, when the mother is lacking in intelligence or
sympathy, it will be the duty of the physician to give this enlightenment
to the young girl. The interpreter of such tidings at the time
of love’s dawning will be the family doctor, to whom the girl and
her family have been confidently accustomed to turn for information
regarding the bodily state and well-being. He is accustomed
to remove many a veil without any offense to maidenly modesty.
Many sexual disorders and much sexual aberration may thus be
prevented.
Certain definite hygienic rules must now be prescribed. First of
all, the strictest cleanliness must be observed, not only in the intervals,
but also during menstruation. The prejudice against changing
the under linen during the flow must be overcome, and care
must be taken that at this time the external genitals are washed twice
daily with water at a temperature of 26° C. to 28° C. (about 80° F.),
and a wad of absorbent cotton-wool or a piece of clean linen (sponges
are not to be used for this purpose); any article of underclothing
126that becomes soiled with blood must be changed. Most useful are
the so-called “sanitary towels,” made of sterilized absorbent cotton-wool,
fastened to a linen band which surrounds the waist, or simple
pads of absorbent material may be used, kept in place by means of
a bandage. During menstruation, full baths, warm or cold, are to
be avoided, likewise long walks, riding, long journeys by rail,
gymnastics, with or without apparatus, skating, lawn tennis, and
bicycling; dancing, above all, must be prohibited, since it involves
a combination of several noxious influences—the very active movement,
which produces hyperæmia of the genital organs, sexual
excitement, loss of sleep, long hours spent in close rooms, prolonged
voluntary retention of urine, and the risk of a chill. Singing, also,
must be discontinued during menstruation, since otherwise an injury
to the voice is very likely to result. A certain limitation in respect
of physical and mental activity is indicated as a general precautionary
measure during menstruation, but this measure must not be pushed
to excess, so that the habit is acquired of resting completely during
the period, passing the days on a sofa. The favorite practice, in
cases of scanty menstruation, of taking hot foot-baths is to be rejected.
At the conclusion of each menstrual period, however, a tepid
bath should be taken. The knowledge we have now acquired of
the rhythmical “menstrual wave” process (see p. 19 et seq.) points
to the practical conclusion that the physician should not direct his
attention to the actual menstrual period only, but also, and more
than has hitherto been customary, to the premenstrual period, in
which temperature, blood-pressure, and excretion of urea attain
their acme; especially should this be done, with the aim of prescribing
suitable hygienic precautions, in cases in which the menstrual
discharge is very profuse or in which nervous manifestations
accompany menstruation.
Important is it also for the physician to take precautions against
the practice by young girls of unduly prolonged voluntary retention
of the urine, resulting in over-distension of the bladder; also against
the performance of very active movements and against powerful
muscular efforts when the bladder is in a distended state. All of
these are liable to result in displacements of the uterus.
During menstruation the diet should be sufficient, but free from
stimulating elements. When the menstrual flow is greatly in excess,
strong tea and coffee, wine, and beer should be forbidden; conversely,
when menstruation is scanty, an invigorating diet is especially
indicated, and the use of strong wines. According to the investigations
of T. Schrader, in order to maintain the nitrogenous balance
127during menstruation, it is necessary to give the following daily diet,
representing a heat value of 2,013 to 2,076 calories:
| 125–150 |
grammes of fowl. |
| 100 |
grammes of butter. |
| 125–140 |
grammes of white bread. |
| 150 |
grammes of brown bread. |
| 70–80 |
grammes of eggs. |
| 600 |
grammes of coffee. |
| 600 |
grammes of soup. |
| 560 |
grammes of Seltzer water. |
| 20 |
grammes of salt. |
For chlorotic girls the following diet may be recommended during
menstruation. Before rising a pint of milk should be taken slowly,
in sips, during a period not exceeding half an hour; for the first
breakfast (see note to p. 112), tea or coffee with an abundance of
milk, a considerable portion of meat (roast beef, cold fowl, cutlets,
or beefsteak); for the second breakfast, a tumbler of milk, bread,
butter, and a couple of eggs; for mid-day dinner, a good helping of
fresh meat so cooked as to be easily digested, green vegetables,
potatoes, farinaceous pudding, stewed fruit, and a glass of burgundy
or claret; at 4 P. M., coffee and bread and butter, or a
tumbler of milk; at 7 P. M., a similar meal to the mid-day dinner, but
lighter; no supper. In this diet-table, which represents a heat-value
of about 2,200 calories, albumin and fat are present in abundance
(182.8 grammes albumin and 763 grammes fat), but carbohydrates
in small quantity only (176.9 grammes).
For those chlorotic patients who find it difficult to digest much
butcher’s meat, the necessary quantum of albumin must be supplied
by increasing the amount of milk, soup, and the white varieties of
flesh (chicken and the like), giving also a considerable amount of
the more easily digested vegetables, with fruit, beer, and a little
claret. For such cases Desqué has drawn up the following diet-table,
representing 3,290 calories and containing 150 grammes of
albumin, 110.7 grammes of fat, and 449.6 grammes of carbohydrate;
meat is given once a day only:
- 7.30 A. M.—
- Half a pint of milk, 50 grammes roll, 10 grammes butter.
- 10 A. M.—
- 300 grammes apples, strawberries, or cranberries, 50 grammes roll, 10 grammes butter.
- 12.30 P. M.—
- 200 grammes of beefsteak, 100 grammes of macaroni, 300 grammes of bread, 400 grammes of
spinach, 200 grammes of stewed apples or gooseberries.
- 4 P. M.—
- 200 grammes vegetable-peptone-cocoa, 50 grammes roll, 10 grammes butter.
- 7.30 P. M.—
- 200 grammes rice-broth, 500 grammes buttermilk, 100 grammes bread, 10 grammes butter, 200
grammes salad, 300 grammes uncooked pears, 40 grammes curds.
128In cases of profuse metrorrhagia in girls, von Winckel recommends
in addition to rest in the recumbent posture, a diet containing
large quantities of fluid, and much easily assimilable albuminous
nutrient material, all stimulating articles and those likely to cause
nausea and vomiting being avoided. He gives the following diet-table:
- 7 A. M.—
- 250 grammes of milk.
- 9 A. M.—
- 250 grammes of bouillon, 1 egg, 20 grammes of brandy.
- 11 A. M.—
- 250 grammes of milk.
- 1 P. M.—
- 100 grammes of roast meat, 250 grammes of rice-broth with 5 grammes of somatose, and 150
grammes of claret.
- 3 P. M.—
- 250 grammes of milk.
- 5 P. M.—
- 1 egg, 20 grammes of brandy.
- 7 P. M.—
- 250 grammes of bouillon or white soup with 5 grammes of somatose.
As a beverage in the intervals, weak cold tea is allowed. When
the hæmorrhage has ceased, the following beverages are suitable:
oatmeal, cocoa, Pilsener beer (one pint daily), milk (2 to 3 pints
daily), claret (a half bottle daily). For food, the lighter varieties
of meat, 200 to 300 grammes daily, sweetbread, pigeon, ham, nutrient
and easily digestible vegetables, spinach, carrots, and pea-soup,
may be recommended.
In cases of amenorrhœa or scanty menstruation, especially when
due to anæmia or to underfeeding, mental excitement, or over-exertion,
warm baths at a temperature of 28° to 29° R. (90° to
92° F.), rubbing the body with wet towels, and warm sitz-baths,
are of good service.
[Note: Although in this translation the English equivalents of the measures
used on the Continent have as a rule been appended in parenthesis, this has
not been thought necessary in the case of the diet-tables, since even in English
works these are commonly stated in terms of the metric system. It may here
be mentioned that, as regards fluid measures, 250 grammes (a quarter of a
litre) is roughly equivalent to half a pint, an ordinary tumblerful or breakfast-cupful;
and that, as regards solid measures, 30 grammes are equivalent to a
very little more than an avoirdupois ounce.]
Menstruation.
Menstruation is the name given to the process which manifests
itself in the human female after the age of puberty by the discharge
from the genital organs at regular four-weekly intervals of a mucosanguineous
secretion. This discharge is not merely the result of
a local hyperaemic condition, but is the expression of a periodic
excitation of the entire nervous system and blood vascular system,
intimately related with the whole sexual life of woman; this excitation
is itself dependent upon the process of ovulation, an incident in
the series of manifestations that arise from the periodic undulatory
movement in the vital processes of woman.
129The Mosaic law regarded the process of menstruation as unclean
in nature; the menstruating woman was unclean, and must be purified
in a prescribed manner. In the fifteenth chapter of Leviticus,
vv. 19–29, we read: “And if a woman have an issue, and her
issue in her flesh be blood, she shall be put apart seven days: and
whosoever toucheth her shall be unclean until the even. * * *
Every bed whereon she lieth all the days of her issue shall be unto
her as the bed of her separation. * * * But if she be cleansed
of her issue, then she shall number to herself seven days, and after
that she shall be clean. And on the eighth day she shall take unto
her two turtles, or two young pigeons, and bring them unto the
priest, to the door of the tabernacle of the congregation.”
In a similar manner the adherents of the faith of Islam regard
a menstruating woman as unclean.
This view is found also in the earliest medical writings, alike
in the early Indian book of Susruta and in the later writings of
Hippocrates, and it persists to the present day in the use of the
expression “monthly purification.” Susruta teaches that in India
menstruation begins at the age of twelve, and recurs monthly, the
flow lasting three days. In the Jewish Talmud it is asserted (see
“La Médécine du Talmud,” by Dr. Rabbinowicz) that menstruation
begins as soon as the girl has two hairs on the pubic region, or at
the age of twelve, even in the absence of any growth of the pubic
hair. The menstrual blood is quite peculiar in its characters. Thus,
Raschi relates, the mother of the King of Persia exhibited sixty
varieties of blood, and among them Rabba was able to detect which
was the menstrual blood. According to a rabbinical authority, a
woman can become pregnant as soon as she has completed her
twelfth year. As signs of puberty, Rabbi Jossé mentions the appearance
of a fold beneath the nipple, Rabbi Akiba, the erection of
the nipples, Rabbi d’Azai, the appearance of a dark areola around
the nipples, Rabbi Jossé, the recession of the nipple under pressure
followed by its gradual protrusion when the pressure is removed,
also the softening of the mons Veneris (in consequence of the deposit
of fat in its substance). As prodromal signs of the first appearance
of menstruation, the Talmud mentions, pain in the region of the
umbilicus and in the uterus, flatulence, shivering, white flux, heaviness
in the head and the limbs, and nausea.
The blood discharged during menstruation has certain peculiar
properties. It is always fluid, and rarely contains fibrinous clots,
it is always mixed with a larger or smaller quantity of mucus, which
gives it a sticky character; the reaction is alkaline, the smell characteristic.
Only when the bleeding is very profuse are coagulated
masses evacuated. On microscopical examination of menstrual
130blood, we detect erythrocytes and leucocytes, the proportional number
of the latter being greater than in pure blood; there is an admixture
also of epithelium from the genital mucous membranes,
cylindrical cells from the uterus, flattened cells from the superficial
layers of the stratified scaly epithelium of the vagina, also various
micro-organisms and granular detritus. At the beginning of each
menstruation, the admixture of mucus is greatest, so that the discharge
sometimes has the appearance of blood-stained mucus; but
during the height of the discharge the consistency is almost that of
pure blood. The quantity of blood lost at each period is said to vary
from 90 to 240 grammes (about 3 to 8 fluid ounces); but in tropical
climates the average is said to be 600 grammes (20 ounces). According
to the accurate analysis of Denis, menstrual fluid contains
in a thousand parts:
| Total solid constituents |
|
175.00 |
| |
Comprising |
|
|
| |
|
Fat |
3.90 |
|
| |
|
Blood-corpuscles |
64.40 |
|
| |
|
Albumin |
48.30 |
|
| |
|
Extractives |
1.10 |
|
| |
|
Salts |
12.00 |
|
| |
|
Mucus |
45.30 |
|
| |
|
|
|
|
| Water |
|
825.00 |
| |
|
|
|
|
Both the quality and the quantity of the blood are subject to
great variations. Thus, for instance, Bouchardat estimates the solid
constituents at 99.20 per mille, Vogel at 161 per mille, and Simon
at 215 per mille. The amount of blood discharged during menstruation
depends upon the temperament, the constitution, and the occupation,
of the woman concerned. It is greater in vivacious
brunettes than in phlegmatic blondes, greater in southern women
than in those dwelling in the north, greater in town dwellers than in
women living in the open plains, greater in those whose mode of
life is sedentary than in those engaged in some active occupation.
Similar considerations apply with regard to the duration of each
period. The mean duration is in the great majority of cases from
four to five days, being generally the same in successive periods
in the same individual; in exceptional cases the flow may last a
week or more. Menstruation lasting more than eight days must be
regarded as abnormal.
Krieger has collected data relating to the duration of the individual
periods. He found the duration constant in the great majority
of cases, i. e., 93.285 per cent.; but variable in a small minority,
i. e., 6.715 per cent.
131The periods in which the duration was regular did not always last
precisely the same number of days, the duration in many cases
being 3 to 4 days, 5 to 6 days, etc.; but the same duration recurred
regularly at each successive period, so that all these instances must
be reckoned among the periods of regular duration. The duration
must be regarded as irregular or variable in those cases in which
the variation was from 2 to 4 days, 3 to 8 days, etc. Sometimes
a regular three-day or five-day period becomes transformed into an
eight-day period; or conversely an eight-day period into a four-day
period.
Among the cases in which the duration was regular, it amounted
| Most frequently to 8 days, in |
26.695 per cent. |
| Next in frequency was a duration of 3 days, in |
20.762 per cent. |
| Next, a duration of 4 days, in |
16.949 per cent. |
| Next, a duration of 5 days, in |
11.864 per cent. |
L. Mayer has also drawn a distinction between constant and
variable duration of the menstrual periods. Among 4,927 women,
he found 4,542 (92.185%) in whom the duration was constant, and
385 (7.815%) in whom it was variable. Of the constant periods,
the duration was:
| 8 days in |
1182 women, that is in |
26.024 per cent. |
| 4 days in |
829 women, that is in |
18.252 per cent. |
| 3 days in |
731 women, that is in |
16.094 per cent. |
| 5 days in |
730 women, that is in |
16.072 per cent. |
An extremely short duration, less than 24 hours, was found in
70 women, an extremely long duration, 7 to 14 days, was found in
175 women, and finally a duration exceeding 14 days was found in
19 women.
The mean duration in these cases was 5.387 days.
The results obtained by Szukits, who investigated the duration of
the periods in 1,013 women, are somewhat divergent from the above.
He found:
| A duration of a few hours only in |
95 women, that is in |
9.38 per cent. |
| A duration of 1 to 2 days in |
66 women, that is in |
6.51 per cent. |
| A duration of 3 days in |
407 women, that is in |
40.17 per cent. |
| A duration of 4 days in |
171 women, that is in |
16.88 per cent. |
| A duration of 5 to 6 days in |
115 women, that is in |
11.35 per cent. |
| A duration of 7 to 8 days in |
118 women, that is in |
11.63 per cent. |
| A duration of 9 days and upwards in |
41 women, that is in |
4.05 per cent. |
The mean duration in these cases was 3.87 days.
The mean duration of the menstrual flow is:
| In Paris |
5 |
days. |
| In London |
4.6 |
days. |
| In Berlin |
4.5 |
days. |
| In Copenhagen |
4.3 |
days (according to Mayer, 5.3 days). |
| In Austria |
3.8 |
days. |
132The interval between one menstruation and the next (the period
that elapses, that is to say, between the commencement of one period
and the commencement of the next) is in the great majority of
cases twenty-eight days. The recurrence in many women is extraordinarily
exact, not merely as regards the day, but even as regards
the hour of the day. The twenty-eight-day type of menstruation is
found in about 70 per cent. of the cases; in the remainder, the thirty-day
type is most frequent, and next to that the twenty-one-day type.
The periodicity of menstruation in any individual may however be
very irregular.
The quantity of blood lost during menstruation varies within wide
limits; according to approximate estimates the usual loss at a single
period is from 90 to 240 grammes (about 3 to 8 fluid ounces). The
following summary statement is made by Krieger regarding the
quantity lost in different social circumstances and in various nationalities:
The amount of blood lost and the duration of the flow are less in
strong, healthy women, leading an occupied, active, and regular life,
especially in countrywomen and in women who are poor and chaste,
than it is in delicate, weakly women, leading a sedentary life, whose
diet is abundant and stimulating, and who are accustomed to an
ultra-luxurious and enervating existence. In nuns, for example, the
quantity of the menstrual discharge gradually declines; shortly after
their entrance into the cloister, various irregularities are apt to
occur, but ultimately the flow becomes exceedingly scanty and lasts
for a single day only. Climate also has a great influence, for in hot
countries women usually menstruate very abundantly, whilst in
cold countries the flow is scanty, and often appears only in the
warmer months of the year. Of the Lapp and Samoyede women
this was already reported by Linnæus and Virey. Tilt further relates
that Eskimo women menstruate only during the summer
months, and even then scantily. In southern France, according to
Courty, the quantity varies from 120 to 240 grammes (about 4 to
8 ounces); but it may rise to 300, 350, and even to 500 grammes
(about 10, 12, and 16½ fluid ounces). In the tropics, severe menorrhagia
is said to be common; and the fact was already known to
Blumbenbach, that women of European descent born in the tropics
not infrequently succumb to hæmorrhage during childbirth.
L. Mayer has endeavored to determine the relations between the
quantity and the quality of the discharge, and distinguishes the
regular composition, when a considerable quantity of dark-tinted,
fluid blood is passed, from the irregular composition, when a small
quantity of blood, usually pale in color, is passed, or an excessive
quantity of dark blood, often coagulated, or a discharge of varying
composition.
133Of 4,542 women questioned by Mayer in regard to this matter,
there were:
2,998, that is 66.006 per cent., in whom the composition was regular.
1,544, that is 33.994 per cent., in whom the composition was irregular.
and among the latter the discharge was
| Scanty and for the most part pale in |
511; that is |
12.250 per cent. |
| Profuse or profuse and coagulated in |
838; that is |
18.428 per cent. |
| Variable in |
196; that is |
4.315 per cent. |
Investigation regarding the individual variations that occur in
this respect among women, showed that blondes usually menstruate
more profusely than brunettes, and that in the former also the
duration of the individual periods is longer.
The loss of blood must be considered less in respect of its absolute
quantity than in respect of the effect which continued observation
shows its loss to have upon the organism. If the loss of blood continues
to have an effect after the flow has ceased, if a woman recovers
but slowly, or even fails to recover fully from one loss before
another begins, if symptoms of increasing anæmia become apparent,
the bleeding must be regarded as a pathological perversion
of normal menstruation. Pathological is it also if the menstrual
flow does not exhibit the normal slowly rising and slowly declining
curve, but sets in profusely, ceases or almost ceases for a time, and
then again suddenly recurs. In some cases the flow is not profuse,
but lasts for a long time, and owing to this long duration it has a
debilitating effect, especially in anæmic and chlorotic individuals.
As a rule, in normal menstruation, the admixture of the alkaline
cervical mucus suffices to keep the menstrual discharge fluid and to
prevent the formation of fibrin. On the other hand, the discharge
of coagulated masses of blood will alone suffice to indicate an abnormally
free and rapid flow of blood.
The commonest type of menstruation is the more or less regular
recurrence of the flow at intervals of twenty-eight days. Variations
in this respect are, however, very frequent, and are dependent upon
constitution, position in life, and race. In general it may be said
that in persons of strong constitution, the type of menstruation is
much more regular, than in persons of a weakly, delicate constitution;
that in vivacious, ardent natures the menses more readily
anticipate the expected period of their return, whereas in those of
a flaccid, lymphatic temperament a retardation is more likely to
occur; and that amongst women of the upper classes of society the
type of menstruation is far more frequently irregular than amongst
women of the working classes and amongst countrywomen.
Whereas in many women the regularity of the menstrual rhythm
134is so precise that the flow recurs, not merely at regular intervals of
twenty-eight days, but even time after time at exactly the same
hour of the day—in other cases the interval between two periods
may vary from twenty-one to thirty days.
L. Mayer, who made observations on the type of menstruation
in 5,671 women, and tabulated his results, distinguishes between
constant and inconstant intervals. Among the constant intervals he
enumerates those forms, both regular and irregular, which do not
during the whole life of the individual undergo transformation into
another form, but remain always of the same type. If, for instance,
in any individual the interval is always either two or eight weeks, in
that woman menstruation is indeed irregular, but constant in type.
If, however, for some years she menstruates at intervals either of two
or of eight weeks, and then proceeds to menstruate at intervals of
four weeks, her menstruation is of the inconstant type. Mayer
found among his 5,671 cases
| The constant type in 4,981 women, that is in |
87.83 per cent. |
| The inconstant type in 690 women, that is in |
12.16 per cent. |
Of the cases in which the type was constant there were 69.68
per cent. in which the regular period of four weeks obtained, and
20.31 per cent. in which it was irregular in the sense above defined.
Among these latter, the commonest periods were 15 to 21 days and
22 to 27 days. The same author observed the irregular type of
menstruation in nearly one-fourth of the women belonging to the
well-to-do classes.
According to the observations of Krieger on 481 cases in which
the periods were regular, that is, in which the intervals in each case
were equal in duration, the time from the commencement of one
period to the commencement of the next was:
| 28 days in |
70.80 per cent. |
| 30 days in |
13.74 per cent. |
| 21 days in |
1.66 per cent. |
| 27 days in |
1.45 per cent. |
As regards the season in which menstruation first appears, Krieger
states that in one-half of the women examined by him menstruation
had begun in the autumn season, in the month of September,
October, or November.
Szukits, as a result of an investigation into the menstrual functions
of Austrian women, determined that among 1,013 women menstruation
occurred:
| Every 28 to 30 days in |
642 women. |
| Every 8 to 21 days in |
169 women. |
| Every 35 to 56 days in |
128 women. |
| And was quite irregular in |
74 women. |
135In 500 Jewish women, Hirsch found that menstruation occurred:
| 23 days after the beginning of the last menstruation in |
19 |
| 24 days after the beginning of the last menstruation in |
29 |
| 25 days after the beginning of the last menstruation in |
36 |
| 26 days after the beginning of the last menstruation in |
56 |
| 27 days after the beginning of the last menstruation in |
62 |
| 28 days after the beginning of the last menstruation in |
73 |
| |
|
| |
275 |
| |
|
and in the remaining cases at other intervals than those stated. He
is, therefore, of opinion that in the majority of Jewish women the
type of menstruation is shorter then twenty-nine days.
According to Brierre de Boismont, among 100 women menstruation
recurred:
| Every 4 weeks in |
61 women. |
| Every 3 weeks in |
28 women. |
| Every 2 weeks in |
1 woman. |
| And at various irregular periods in |
10 women. |
Tilt found among 100 women that menstruation recurred:
| Every 4 weeks in |
77 women. |
| Every 3 weeks in |
17 women. |
| Every 2 weeks in |
1 woman. |
| Every 6 weeks in |
5 women. |
Foster instituted inquiries regarding this matter in 56 healthy
women. In 380 periods, 45 recurred after an interval of 28 days,
225 after a shorter interval than this, 110 after a longer interval.
The duration of the flow varied from 1 to 14 days; most commonly
it lasted from 3 to 5 days.
A peculiar change in the type of menstruation sometimes manifests
itself in this way, that in women in whom the regular four-weekly
type of menstruation has prevailed, exactly in the middle
of this four-weekly period the menstrual molimina, with or without
menstrual discharge, make their appearance; the patient suffers
from pain in the lower belly, sacrache, sensation of weight, and
bearing-down pains. Courty, Dubois, and Pajot Négrier have described
such cases of molimen utérin intermenstruel, which Tilt
denotes by the term remittent menstruation.
From the earliest times the process of menstruation has attracted
the attention of natural philosophers, and has led them to formulate
hypotheses and to institute investigations, especially in order to
ascertain whether the connection between ovulation and menstruation
is one of temporal succession merely, or whether the relation
is a causal one.
From Hippocrates and Galen downwards until well beyond the
middle ages, the view of the father of medicine was generally accepted,
136that menstruation is a purificatory process by means of which
materials harmful to the organism are eliminated from the body—a
view which finds expression also in the religious and legal ordinances
of all times.
A new epoch of scientific research into the nature of menstruation
began with de Graaf’s discovery of the ovarian follicles (1672).
This discovery did not, indeed, bring ovulation and menstruation
into immediate relationship, but it certainly paved the way for the
opinion expressed by Sintemma, a countryman of de Graaf, that the
ova, even in virgins, leave the ovary spontaneously, and by their
contact with the capillary terminations of the bloodvessels give
rise to the menstrual bleeding (1728).
As a result of anatomical investigations, Négrier, in 1840, was
the first to establish the thesis that in women suffering from congenital
absence of the ovaries, menstruation never occurs; that after
the loss of the ovaries, menstruation always ceases; that during
pregnancy and lactation and during the climacteric period, ovulation
ceases; and that a relation of temporal succession obtains between
ovulation and menstruation. This close relation between the two
processes was maintained also by Gendrin at about the same date.
Later, Girdwood, by post mortem research, proved that the number
of scars in the ovary coincides with the number of previous menstruations.
Brierre de Boismont, in his exhaustive work on Menstruation,
lays stress on the view that the periodically recurring ovulation
furnishes the impulse for the menstrual flow. First among German
investigators, Bischoff upheld the opinion that maturation and discharge
of ova are spontaneous processes occurring independently
of sexual intercourse, and compared heat or rut in other animals
to menstruation in women—a view shared by Pouchet and Coste.
Ovulation occurs simultaneously with the menstrual flow, and the
follicles burst toward the end of menstruation.
Pflüger, in his important work on the significance and cause of
menstruation, has demonstrated the causal connection between menstruation
and ovulation. The bleeding and the discharge of the
ova are according to him joint effects of a common cause. It is
not the bursting of the follicle, but the ripening of the follicle, that
gives rise to the menstrual congestion. The pressure of the growing
follicle on the surrounding ovarian tissue gives rise to a continued
stimulation of the ovarian nerves; the summation of these stimuli,
which after the lapse of a certain time attain always a certain degree
of intensity, results in a reflex from the spinal cord taking the
form of great congestion of the genital organs; this congestion leads,
on the one hand, to hæmorrhage from the uterine mucous membrane,
137and, on the other hand, and as a rule simultaneously, to the bursting
of the ovarian follicle. The swelling and granulation of the
uterine mucous membrane at every menstrual period signifies nothing
else than the commencement of the formation of the decidua.
Nägele already mentioned the view, that inasmuch as immediately
after the first appearance of menstruation a woman has become
capable of reproducing the species, each process of menstruation
must be regarded as a renewal of the exhausted faculty for conception.
Pflüger’s teaching has been opposed by Sigismund, who, whilst
admitting the periodicity of ovulation and menstruation, yet regards
the two processes, in the uterus the formation of the menstrual
decidua, in the ovary the rupture of the graafian follicle, as
independent of one another, even though they occur simultaneously.
Should fertilization occur, the ovum implants itself in the prepared
soil; should fertilization fail to occur, the menstrual hæmorrhage
ensues. Thus, the occurrence of menstruation indicates that fertilization
of the ovum has failed to occur. On this theory, then, the
ovum that is fertilized belongs to the first period missed, whereas
Pflüger assumes that when pregnancy occurs, it is always the ovum
belonging to the time of the previous menstruation—the last
actual menstrual discharge—that is fertilized.
Löwenhardt, in his work on the Diagnosis and Duration of Pregnancy,
advances the same views as Sigismund. The fertilized ovum,
in his opinion also, is that of the first period missed; and since at
the time at which he believes fertilization to occur the ovum is
certainly still in the ovary, fertilization, on this theory, must always
take place in the ovary itself, and the fertilized ovum cannot begin
its intra-uterine life till a month has elapsed after fertilization.
Reichert, Kundrat, Engelmann, and Williams, basing their views
on anatomical data, are of opinion that ovulation recurs periodically,
and that the extrusion of the ovum occurs not before but after the
commencement of menstruation.
According to Hensen, the observed facts support the view that
the follicles burst as a rule toward the end of menstruation; anticipation
or postponement of the opening of the follicle (conception
before or after menstruation) would, however, appear not to be
impossible.
Leopold, who assumes that menstruation may occur without ovulation
and ovulation without menstruation, maintains on anatomical
grounds that the rupture of the graafian follicle occurs chiefly during
menstruation, under the influence of the swelling due to
menstrual congestion. Menstruation with ovulation he believes to
be a common occurrence, menstruation without ovulation, an unusual
138occurrence. Further, it is certain that, at the time when the
periodic bleeding is due, ovulation may occur, even though the
menstrual discharge fails to make its appearance (ovulation without
menstruation).
Chazan and Gläveke also adhere to the generally accepted view
that ovulation is a periodic process, usually but not necessarily
synchronous with menstruation.
Strassmann bases on clinical facts and on experiments the following
view of the connection between ovulation and menstruation.
The principal processes in the organism of the sexually mature
woman run their course in a periodic rhythm resembling an undulatory
movement, the acme of which occurs in the antemenstrual
period with the aim of preparing for the development of an infantile
organism. Whilst an ovum is maturing in the ovary, in the
uterus, in dependence upon this maturation, the antemenstrual
mucous membrane, fitted for the reception and nutrition of the
fertilized ovum, is also undergoing development. At the acme of
the undulatory movement, the graafian follicle ruptures and the
ovum is liberated, to undergo fertilization in the infundibulum of
the Fallopian tube. If fertilization fails to occur, or if for any
reason the graafian follicle fails to rupture, then, in consequence of
and at the time of the highest intra-ovarian tension, at the time, when
the rupture of the follicle usually occurs, the extrusion of blood from
the capillaries of the uterine mucous membrane begins. The intermediation
between the ovary and the uterus is probably effected by
means of the sympathetic ganglion in the ovary discovered by
Elizabeth Winterhalter, and effected in this manner, that the stimulus
proceeding from the ripening follicle passes along the nerve-fibrils
surrounding the follicle to the processes of the nerve cells
of this sympathetic ganglion, accumulating in these cells till a certain
degree of intensity has been reached, and then, by means of
other processes and of the vasomotor nerves, influencing the vessels
of the uterus.
Gebhard likewise believes menstruation to be dependent on the
ovarian function, and thinks that it is probably brought about in a
reflex manner by the gradual growth of the ovarian follicles. It
appears that most commonly at the time of menstruation a graafian
follicle ripe to bursting is to be found in the ovary, but to this rule
there are many exceptions. We cannot exclude the possibility, that
the ovum from a follicle that burst after the commencement of the
menstrual flow may be fertilized; but more commonly the ovum
that is fertilized is that of the first period missed. The sudden
decline in vital energy that occurs just before menstruation is explained
by Gebhard as a kind of atavism, dependent on the fact
139that many of the lower animals, butterflies, for instance, succumb
as soon as they have fulfilled their duty of reproducing the species.
A number of modern investigators, however, deny that any relation,
temporal or causal, exists between ovulation and menstruation,
and affirm that the latter process is quite independent of the
former.
Thus, Christopher Martin maintains that a special menstrual
centre exists in the lumbar portion of the spinal cord, the impulses
from which proceed to the uterus by way of the splanchnic plexus,
the ovarian plexus, or perhaps by both. Similar views are held by
Lawson Tait, Collins, and Johnstone, who severally maintain that
the ovaries are no more concerned in the production of menstruation
than any other organ of the body—the liver, for instance.
They direct attention to the periodicity that occurs in the functional
activity of various other organs, in respiratory and cardiac activity,
for instance, both of which undergo rhythmical changes as a result
of nervous influences. The cessation of menstruation after
oöphorectomy they attribute, not to the cessation of ovulation, but
to the division of the nerves which run across the broad ligaments
of the uterus and upon which menstruation depends. Heat and
rut in animals have a different significance from menstruation. The
latter process is induced by civilization and by the adoption of the
upright posture.
But, taking all this into consideration, we must hold fast to the
fundamental principles, that ovulation occurs at that period of life,
and only at that period, during which menstruation proceeds regularly;
that ovulation begins when externally and in the whole development
of the girl the signs of sexual maturity manifest themselves;
and that ovulation ceases at the climacteric, when menstruation
also ceases. We must regard as rare exceptions to this rule
cases in which ovulation begins before the menarche and persists
after the menopause.
A physiological interruption of menstruation occurs during pregnancy
and lactation; it seems improbable, however, that during this
interval ovulation also is in abeyance. It is established by anatomical
investigations that ovulation and menstruation commonly occur
in association; but that menstruation sometimes, though rarely, occurs
in the absence of ovulation; and, finally, that intermenstrual
ovulation is also a rare occurrence. In the majority of cases, either
just before or just after the commencement of the menstrual flow,
rupture of a graafian follicle occurs. After complete oöphorectomy,
menstruation ceases; it is only when functionally active portions
of ovarian tissue have been left behind, that menstruation continues
to occur. In the absence of the ovaries, the menstrual function is
140in abeyance; hence, for the performance of that function, the
presence of ripening ovarian follicles and of other follicles capable
of ripening later, is an indispensable requisite.
A certain analogy between heat and rut in animals and menstruation
in women may, according to the investigations of Bischoff,
Hegar, Strassmann, and others, certainly be maintained. Heat
or rut is a process occurring in mammals, dependent on the reproductive
glands, characterized by an increase in sexual and general
excitability, with congestion of the pudendum and the vagina,
swelling of the sebaceous glands of the external genitals, and increased
secretion; from the vulval cleft there flows a peculiar, strong-smelling
mucus, often tinted red from admixture with blood; there
is frequent micturition, the uterine glands are swollen, the Fallopian
tubes are also swollen, and are soft and erected. A well-developed
menstrual bleeding, analogous to that which occurs in the human
species, occurs, among the lower animals, only in apes. Maturation
of ova precedes the period of heat, and rupture of the graafian
follicle occurs during that period.
Heat or rut occurs in animals at certain seasons of the year,
which may, according to the species and the mode of life of the
animal concerned, be in spring, summer, autumn, or winter. The
season of heat or rut has further several periods of heat, each
lasting several days, and among domesticated animals, mares, cows,
and bitches, succeeding one another at intervals of three or four
weeks; in wild animals, rut occurs once only in the year. In animals,
sexual intercourse takes place during the time of the menstrual
discharge, and during this time also the capacity for conception is
increased; in the absence of heat, the genital organs are in a more
quiescent condition. In this connection, the experiments on animals
made by Strassmann, with a view to determining the influence
upon the uterus of rise of pressure in the ovary, are of great
interest; these experiments showed that a rise of intra-ovarian
pressure, produced by the injection of fluid into the parenchyma
of the ovary, led to changes in the endometrium and the external
genital organs corresponding to those occurring in an animal on
heat.
In the human species, however, in contradistinction to what occurs
in the lower animals, there is a certain disinclination, on the
part of the male at any rate, to sexual intercourse during menstruation.
The human female moreover, notwithstanding the periodicity
of her sexual life, is at all times capable of conception; this capability
is not confined to any particular part of the intermenstrual period,
for conception may occur at any time during that period, and has
even been known to result from intercourse during menstruation.
141This peculiar characteristic of the human reproductive capacity has
been regarded as compensatory, furnished by nature in her continual
endeavour for the perpetuation of the species, to counteract the restricting
influences imposed by civilization on the normal process
of reproduction.
Credible observations even exist, indicating that among many
primitive peoples, in whom at the time of puberty no social laws
hinder the limitless exercise of the reproductive functions, this
capacity on the part of woman to conceive at any time has no
existence, and that the reproductive capacity of such human beings
is, like that of the lower animals, confined to a certain season of
the year. Thus, G. Schlesinger reports of the Ainus of the island
of Yezo, “A friend of mine in Sapporo believes himself to have
observed that the Ainus have a certain definite rutting period, and
that in them, as in many of the lower animals, the process of reproducing
the species occurs only at a certain season of the year.”
An identical statement is current concerning the Indians of Western
America.
The mucous membrane of the uterus undergoes during menstruation
important changes, and a question much disputed is, whether
in the course of menstruation the whole of the uterine mucous
membrane is removed, or a part only, whether it is shed in its entire
thickness, or is at least deprived of its epithelium. According to
the observations made by Leopold on dead bodies, the mucous membrane
of the uterus becomes swollen shortly before the commencement
of the menstrual discharge, until, partly in consequence of
cellular proliferation, partly in consequence of œdematous infiltration,
and partly in consequence of enlargement of the lymph-spaces,
it attains a thickness of 6 to 7 millimetres (¼ of an inch). The
superficial capillaries are notably enlarged, and an effusion of blood-elements
continues for several days, without the occurrence of any
fatty degeneration in the tissues. The epithelium and the most
superficial cell-layers of the mucous membrane are, however, undermined
and shed. No complete destruction of the mucous membrane
occurs, however, and fatty degeneration forms no part of the menstrual
process as such.
Möricke, who examined portions of the uterine mucous membrane
removed with the curette during menstruation from living
women, found the superficial layers of the mucous membrane to
be intact, and he regards the shedding of the epithelium described
by other authorities as cadaveric phenomenon. Sinéty, who also
found the uterine mucous membrane intact during menstruation,
adheres to the same view.
Von Kahlden concludes, as a result of investigations made post
142mortem, that during menstruation the greater part of the mucous
membrane, not the superficial epithelium only, but the stroma itself
down to its deepest layers, is shed. According to von Tassenbroek
and Mendes le Leon, however, the most superficial layers only are
shed during menstruation.
According to Westphalen, whose investigations were made, partly
on masses removed by the curette, and partly on freshly extirpated
uteri, a sanguineo-serous infiltration of the mucous membrane begins
about ten days before menstruation. Great vascular dilatation occurs
only just before menstruation. The uterine glands undergo
enlargement, and during and immediately after the flow, numerous
shed epithelium cells occupy the lumen of the glands. For the rest,
however, in the interior of the uterus shortly after menstruation,
we find an almost continuous epithelial covering. Some days after
menstruation, the proper regeneration of the mucous membrane
occurs.
Mandl, who examined totally extirpated uteri, asserts that during
menstruation the epithelial covering of the mucous membrane is
never completely lost, but that just as little does it remain completely
intact. The regeneration of the lost areas of epithelium proceeds
even during menstruation.
The researches of Kundrat and Engelmann on uteri obtained post mortem
led these authors to describe as follows the anatomical
changes that occur in the uterine mucous membrane at the time
of the catamenial hæmorrhage. In the premenstrual epoch a round-cell
infiltration occurs in the interglandular tissue, the lumina of
the uterine glands become enlarged, and the bloodvessels dilated;
subsequently, fatty degeneration of the superficial epithelium and
the epithelium of the glands occurs, leading to laceration of the
vessels and destruction of the affected area of tissue; after the
cessation of the bleeding, regeneration of the mucous membrane
occurs.
According to Gebhard, three stages may be distinguished. The
first stage is that of premenstrual congestion, or stage of engorgement:
the capillary vessels of the mucous membrane become distended
with blood, the membrane itself becomes softened, the meshes
of the stroma become enlarged and are filled with the morphological
constituents of the blood, subepithelial hæmatomata are formed.
The second stage is that in which the blood finds its way to the exterior:
owing to the turgescence of the mucous membrane the blood
is able to exude between the cells of the intact epithelium; further,
the epithelium becomes lacerated in various places where hæmatomata
have formed beneath it, allowing the blood to exude through
the apertures thus formed; shreds of epithelium may be washed
143away by the blood-stream. The third stage is that of post-menstrual
regeneration: the swelling of the mucous membrane disappears, the
detached areas of epithelium readhere, the blood effused into the
interstices of the tissue is reabsorbed, or is in part transformed
into yellowish-brown flakes of pigment. According to Gebhard’s
view, during menstruation destruction of the uterine mucous membrane
does not occur. At no time is the membrane denuded of
large areas of epithelium; a very active process of regeneration occurs,
however, in the superficial epithelium and the epithelium of
the glands, which fits the uterine mucosa for the reception of the
fertilized ovum by keeping it in an ever-young and renovated condition.
The mucous membrane of the cervix takes part in menstruation
at most by an increased secretion of mucus.
According to Landau and Rheinstein, the mucous membrane of
the Fallopian tubes contributes to the menstrual hæmorrhage; Fritsch
and Strassmann, however, are opposed to the view that there is a
regular tubal menstruation.
Pathology of Menstruation.
Only a small proportion of girls and women are entirely free,
at the time of menstruation, from all change both in their bodily
and in their mental state. A very great majority complain of feeling
more or less unwell, of sensations of weight and pressure in
the hypogastric region, of a general feeling of languor, loss of
appetite, headache, irritability, sometimes of an inclination to weep;
in women, a change in the intensity of the sexual impulse manifests
itself, an increase in some, a decrease in others.
Not infrequently during menstruation, the cardiac activity is
notably affected, so that, regularly at the commencement of each
period, disagreeable sensations occur in the cardiac region, with
increased frequency of the heart’s action; or complaint is made
of coldness and dampness of the hands, of icy coldness of the feet,
which feel as if “dead” to half way up the calves, and cannot be
warmed—phenomena which, in the cases under consideration,
occur only at the time of menstruation, and are to be regarded as
manifestations of the menstrual reflex.
I examined 140 women in whom the heart and the vascular system
were normal, during a number of successive menstrual periods,
and in 12 of these women, either at the commencement or during
the course of the flow, I observed an increase in the frequency of
the heart to the extent of from 12 to 28 beats per minute; in young
girls, a systolic murmur was sometimes audible during menstruation,
but was inaudible in the intermenstrual intervals. In all these
persons, menstruation was regular; there was no abnormality in respect
144either of the duration or of the quantity of the flow. The
heart in these cases was, therefore, affected by the normal menstrual
process.
A remarkable illustration of the alleged influence of menstrual disturbances
on the pulse is reported by de Villeneuve, who states
that Chinese physicians, being accustomed to feel the pulse in
many different arteries, are able, by a comparison of the characters
of the pulse in the two arms, to determine whether a woman menstruates
regularly or irregularly.
Many women and girls show well-marked menstrual molimina,
uneasy or actually painful local sensations in the genital organs,
sacrache, painful uterine contractions, and disturbances of the
general constitutional state, which are dependent upon menstrual
congestion of the pelvic organs, upon local engorgement; sometimes
such symptoms are the result of uterine contractions caused by
hyperæmia of the uterus, and these cases often take a paroxysmal
form.
Important disturbances of the general constitutional state result
from sudden suppression of the normal menstrual flow, such as
may be the effect of a severe chill, of sudden mental impressions,
even of errors in diet or the use of certain drugs, and may sometimes
follow artificial withdrawal of blood.
In many women, a few days or it may be a few hours only before
every menstruation, changing manifestations of manifold disorders
may recur. Among these may be mentioned, general excitement
of the nervous system, notable alteration in the voice,
strong inclination to sadness, tearfulness, erotic longings, great irritability
and sensitiveness of the sensory system, drowsiness, flushings
of the face, giddiness, swooning. The appetite is impaired,
the breath has a disagreeable smell, the digestion is disturbed, there
is a tendency to diarrhœa; the facial aspect may be altered, there
are blue rings round the eyes, eruptions on the skin, tendency to
sweating, palpitation and feeling of anxiety, and a sensation in the
extremities as if they had been beaten. Local symptoms also occur:
disturbances of the function of micturition, swelling of the breasts,
pains and colics in the renal region, feeling of warmth in the genital
organs, pruritus vulvæ, sensation of weight in the uterus, and a
strong impulse toward coition. The secretions may be pathological,
sometimes there are profuse sweats, sometimes profuse mucous or
bilious diarrhœa, whilst the urine may either be very abundant,
almost colorless, and nearly free from saline matter, or thick and
overladen with phosphates and urates.
Schauta writes regarding the complex of menstrual phenomena
which occur in normal menstruation: “In the process of menstruation,
145blood and sanguineous mucus find their way through a
mucous canal, the normal calibre of which is merely a capillary
fissure. If the flow is slow, without the formation of coagula, and
if the passage through the cervix is free, very gentle contractions
of the uterine muscle suffice on the whole, as the blood exudes into
the cavity of the uterus, to expel it into the vagina. Without such
contractions, menstruation is hardly conceivable. Physiologically,
they are characterized by a bearing-down sensation, passing down
toward the thighs, and by pains in the back. It is rarely, that no
pain at all is experienced; there are some women, however, who
affirm that in their case menstruation begins quite unexpectedly,
and without the slightest warning; but it does not follow that contractions
of the uterus do not occur in these women also during
menstruation. * * * The local disturbances which occur as an
accompaniment even of physiological menstruation are, a sensation
of fulness and weight in the pelvis, and pains in the lower part
of the back, and these probably all result from the uterine contractions.
The general disturbances of a reflex nature consist of
tenderness on pressure in the epigastrium, headaches, general sense
of languor, irritability, and an inclination to shed tears. Among
changes in the functions of remote organs may be mentioned, swelling
of the breasts, of the vocal cords, and of the thyroid body, increased
respiratory capacity shortly before menstruation followed
by rapid decrease during the flow, tendency to diarrhœa, nausea,
vomiting, flatulence, salivation, profuse secretion of the sebaceous
glands of the vulva, increased secretion of sweat, tendency to the
formation of acne pustules. The mental condition also exhibits
as a rule a considerable change during menstruation, even in cases
which cannot in any sense be regarded as pathological. In many
instances, an apparently normal woman may during menstruation
exhibit a mental state so abnormal that we are led to speak of it
as a menstrual psychosis. Apart from this, however, it appears that
during menstruation the mental life of woman never remains entirely
unaffected. Finally, we must mention certain changes in the
sense-organs which not infrequently accompany menstruation, such
as herpes conjunctivæ, exophthalmos, limitation of the visual field,
and swelling of the nasal turbinate bodies.”
In the digestive organs, during the menstrual process, changes in
the secretions of the glands, nausea, vomiting, and flatulence are not
infrequently observed. In one-half of the women concerning whose
state during menstruation Krieger made inquiries, he found, especially
just before and during the discharge, a tendency to diarrhœa,
or at least to more copious and more frequent evacuations of the
bowels than occurred at other times. On the surface of the tongue,
146at the premenstrual epoch, a pronounced exfoliation of the epithelium
may occur, so that in some instances the papillæ are entirely
exposed.
Not infrequently hyperæmia of the liver appears to be connected
with the menstrual process; and by many observers, among whom
Senator and Fleischmann may be mentioned, jaundice, slight or intense,
has been seen to occur during menstruation. In a case of
long-standing amenorrhœa, Duncan noted the appearance of a
transient vicarious jaundice, apparently reflex in its origin. In some
cases, jaundice precedes menstruation, and disappears as the flow
becomes established.
In the respiratory organs also, menstrual changes frequently occur.
According to von Ott, respiratory capacity attains a maximum
shortly before menstruation, and diminishes rather rapidly during the
flow; the expiratory power is similarly affected. In the larynx, according
to Bottermund, great swelling of the posterior wall occurs
during menstruation, whereby the closure of the glottis is hindered,
and a rapid onset of fatigue ensues in the muscles that perform this
action when the woman sings or speaks; the fulness of the voice
is also diminished. More or less extensive swelling of the thyroid
body[32] occurs during the menstrual period. According to Fliess,
in most women, the inferior, sometimes the middle and the inferior
nasal turbinate bodies are greatly swollen; sometimes also the tubercula
septi are swollen. It is said that the right half of the nose is
more frequently and more intensely swollen than the left half.
Epistaxis is sometimes observed at the menstrual periods.
In the urinary organs, the influence of the menstrual period is
manifested by a change in the urine. According to Schrader, the
elimination of urea is diminished shortly before menstruation; according
to Laval, the elimination of uric acid undergoes a sudden
diminution on the second day of the flow, followed by an increase
on the third day, subsequently rising above the normal level. This
change is to be attributed, not to any excitation of the genital
organs, but to the loss of blood.
Hebra already drew attention to the connection between diseases
of the skin and the physiological and pathological processes occurring
in the female genital organs; and emphasized the fact that for
the cure of certain eruptions, local treatment of the disorder of the
reproductive organs was requisite. He gave four examples of such
eruptions: 1, an acute attack of eczema, which disappeared only
after the removal of a badly fitting pessary; 2, in a chlorotic girl,
two large red spots on the cheeks disappeared when menstruation
was established; 3, improvement of a skin-affection when a coexisting
147disorder of the genital organs received appropriate treatment,
followed by recrudescence of the skin trouble when the genital
disorder became more severe; 4, a case of obstinate seborrhœa, lasting
for many years, which disappeared only when the patient became
pregnant, for the first time, seven years after her marriage.
Similar cases have been recorded by subsequent observers, and
numerous monographs have been published on menstrual skin-eruptions.
Schramm, for instance, reports the case of a woman in
whom at each menstrual period tubercles and papules appeared on
the backs of the hands and on the neck; and the same author mentions
another case in which during menstruation red papules arranged
in rows appeared on the back. Wilhelm observed dark blue
macules, the size of hazelnuts, which appeared on the thighs shortly
before menstruation and disappeared when the flow was over. Of
two cases of menstrual disorder of the skin reported by Stiller, in
one, an itching eruption appeared on the upper and the lower extremities;
in the other, small red papules appeared on the dorsum of
the hands and feet. Other cases of menstrual skin-eruptions were
published by Joseph, Pauli, Janovsky, and Schwing. Sometimes at
the menstrual periods severe pruritus vulvæ occurs, due, no doubt,
to the temporary increase in the secretion of the menstrual passages,
and to the more active influence exercised by this secretion on the
vulva.
In two cases in which the menstrual flow was in abeyance, Heitzmann
observed affections of the skin. In one of these, a young
woman aged twenty who had not yet begun to menstruate, there
appeared every four weeks isolated papules surrounded by a bright
red areola, itching so violently that scratching resulted. In the
other, macules the size of a lentil, of a light red or dark red color,
appeared, and lasted two or three days; when menstruation became
regular, fresh crops no longer formed.
Schauta, in a case of chronic oöphoritis, observed the regular recurrence
of urticaria at each successive menstrual period. The
suffering being very great, the rest at night being greatly disturbed
during the periods of eruption, and the patient’s general health declining
more and more in consequence, extirpation of the ovaries
was undertaken, and the operation resulted in a complete cure.
Schauta further observed that in cases of obstinate skin-affections
of unknown causation occurring in persons of the female sex, some
disorder of the genital organs was nearly always present; moreover,
in many of these cases, as soon as the genital disorder was
cured by appropriate measures, the skin-affection disappeared spontaneously
and without any further treatment. He had been able to
collect twenty-six cases of this nature, in which an indubitable
148connection obtained between disease of the skin and disease of
the reproductive system. The forms of affection of the genital
organs chiefly noticed in this association were, retroflexion and
retroversion of the uterus, erosion and ectropium or eversion of
the cervix (chronic cervical catarrh), chronic endometritis,
oöphoritis, and salpingitis, and finally with especial frequency
uterine myomata; the skin-diseases observed were, acne, eczema,
disorders of pigmentation, psoriasis, lichen, and urticaria.
During menstruation we observe not infrequently a number of
changes in the skin, such as hyperidrosis, acne, seborrhœa, erythema,
and the form of dermatitis known as erysipelas of menstruation;
sometimes also effusion of blood into the skin as a form of vicarious
menstruation, and peculiar forms of cutaneous œdema. In many
women during menstruation the secretion of sweat is markedly increased
every month; in exceptional cases, menstruation is vicariously
replaced by profuse sweating. In association with menstruation
we frequently observe excessive secretion of the sebaceous
glands, especially of those of the hairy scalp. Often urticaria manifests
itself as a recurrent menstrual eruption. In cases of scanty
menstruation and of amenorrhœa, discoloration and excessive pigmentation
of the skin may occur, sometimes taking the form (as
also in pregnancy) of chloasma uterinum. Sometimes also in these
cases the formation of dark rings round the eyes, already seen in
slighter degree as an accompaniment of normal menstruation, is
excessive.
In the organ of vision, changes associated with menstruation have
been recorded by various observers. Hordeolum menstruale (menstrual
stye) may recur month after month at the menstrual periods
as an exacerbation of a chronic conjunctivitis. Herpes of the ocular
or palpebral conjunctive and eczematous affections may be connected
with menstruation; also exophthalmos may occur during
menstruation in association with swelling of the thyroid body and
palpitation of the heart (H. Cohn); again, as an accompaniment of
normal menstruation, severe papillitis with retinal hæmorrhages
may occur (Heber). According to the investigations of Finkelstein,
a limitation of the field of vision may be noticed during menstruation,
beginning on the first, second, or third day of the flow, attaining
its greatest intensity on the third or fourth day of the flow,
and gradually disappearing during the three or four days next
ensuing.
The organ of hearing is stated by Haug to be affected during
menstruation, inasmuch as congestive redness and swelling of the
external ear, of the external auditory meatus, and of the skin over the
mastoid process, sometimes occurs; occasionally also, periodic neuralgia
manifests itself at the menstrual periods.
149In the circulatory organs, as already mentioned, normal menstruation
quite frequently manifests its influence by the production of
disorders of greater or less severity, referable to the stimulus of
ovulation. In 8.5 per cent. of the women of whom I have made
inquiries with regard to this matter, palpitation of the heart of
variable severity occurred during menstruation, and was most frequent
and most severe on the first and second days of the flow.
Associated with the palpitation in some cases were, vasomotor disturbances,
transient feelings of heat, a sense of congestion in the
head, and profuse perspiration without apparent cause. The day
before the commencement of the flow, the blood-pressure rises considerably,
but falls rapidly during the flow. This menstrual rise
in blood-pressure is accompanied by a rise in temperature and an
increase in metabolic activity. The influence of menstruation on
the heart is most powerfully displayed in cases in which for some
reason a disturbance occurs of the normal appearance or normal
course of menstruation.
Disorders of menstruation likely to give rise to cardiac disorders
are, amenorrhœa, menorrhagia, and dysmenorrhœa.
Amenorrhœa is especially apt to induce cardiac disorder in cases
in which, in consequence of some sudden impression, such as a
fright or a severe chill, menstruation, which began at puberty in
normal fashion and subsequently recurred with perfect regularity,
has undergone sudden and complete suppression; also in cases in
which severe anæmia or obesity has rapidly led to the onset of
amenorrhœa. In such cases, attacks of tachycardia sometimes occur,
it may be at irregular intervals, or it may be exhibiting a
menstrual rhythm, the cardiac affection manifesting itself always
a few days before the date at which menstruation ought to begin.
In these cases, also, systolic murmurs are not infrequently audible.
In cases in which menstruation is very painful, the dysmenorrhœa
may give rise to attacks of colic or to convulsive seizures, whether
the dysmenorrhœa is itself due to inadequacy or to complete suppression
of the flow, to metritis, to anteflexion, to new growths in
the uterus, or, finally, to diseases of the ovaries or to pathological
disorders of ovulation. Among the various disorders associated
with dysmenorrhœa, heart troubles are not infrequent, most often
taking the form of reflex neuroses, evoked by the stimulus of the
pain in the genital organs; but it has also been asserted that an
acute dilatation of the heart occurs in these attacks.
Very threatening cardiac symptoms as an accompaniment of
severe dysmenorrhœa have been seen by me especially in the case
of two women, one of whom was in the thirties and the other in
the forties. The attacks took the form of increased frequency of
150the heart’s action, with severe cardiac dyspnœa on trifling exertion,
sense of suffocation, and intense anxiety. This severe cardiac and
respiratory distress was a sequel to the appearance of severe dysmenorrhœa,
and was relieved as soon as the course of menstruation
became regular and painless; but the cardiac trouble recurred
in association with each successive attack of dysmenorrhœa. In
one of these two women, the dysmenorrhœa was the result of extreme
anteflexion of the uterus; in the other woman, the cause of
the dysmenorrhœa was not apparent. I was unable to decide with
certainty whether in these cases an acute dilatation of the heart
occurred. French authorities, who describe similar cardiac trouble
resulting from diseases of the liver and the stomach by the name
of asystolic gastrohépatique (Potain), give the following explanation
of its mode of occurrence. The intra-abdominal plexus of the
sympathetic is stimulated, this stimulus is reflected to the lungs, in
which organs it gives rise to vaso-constriction, resulting in increased
tension in the lesser circulation; in consequence of this the right
heart has difficulty in emptying itself, when weak it undergoes dilatation,
and a moderate or extreme tricuspid insufficiency ensues. We
have to do, then, in these cases, with reflex symptoms, with a reflex
arc, the starting point of which is the sensory nerve-terminals in the
abdomen, the afferent tract of which is formed by the sympathetic
and pneumogastric nerves, and the efferent tract of which passes
along the pulmonary sympathetic nerves.
In other cases of dysmenorrhœa we observed signs of cardiac
weakness; the pulse was small, very frequent, and barely perceptible,
the face became suddenly pale, the hands and feet were cold; complete
syncope sometimes occurred.
Menorrhagia sometimes leads to cardiac symptoms, owing to the
severity of the anæmia which follows extensive and long-continued
loss of blood; sometimes, however, the heart troubles associated
with menorrhagia are reflex manifestations, dependent on the disease
which has also caused the menorrhagia, endometritis, it may
be, new growths, lukæmia, or scurvy. Sometimes here also we
observe transient attacks of acute dilatation of the heart.
Nervous disturbances during menstruation, which are so frequent
that Emmet regards it as abnormal for a menstruating
woman to be entirely free from pain and from uneasy sensations,
are divided by Windscheid into two classes, general nervous disorders,
and local nervous manifestations. Among general disorders,
the commonest is a general bodily incapacity; in women, who in
other respects are quite healthy, during menstruation everything
will be too great an exertion, and fatigue speedily ensues on
the performance of occupations which at other times are undertaken
151without the slightest difficulty. Another common nervous
disorder is an uneasy sensation in the head, it may be a feeling of
weight or pressure, sometimes described as a feeling as if an iron
band were compressing the forehead. Slight mental irritation is
commonly present also, the woman is capricious, her mental equilibrium
is disturbed. Very common also are vasomotor disturbances,
transient feelings of heat, a sense of congestion in the head, or an
outbreak of perspiration. Among local nervous disturbances, Windscheid
enumerates, pains in the back (occasionally and erroneously
described as spinal irritation), sacrache, pains in the lower extremities,
which by preference generally take the course of the great
sciatic nerves. Pains in the abdomen also frequently accompany
menstruation; these may be diffused over the whole abdomen, or
may predominate in the two hypochondriac regions. Disorders of
the sense-organs sometimes occurring during menstruation are, the
flickering of objects before the eyes, photophobia, and tinnitus
aurium. The heart may also be affected with palpitation in association
with these nervous disturbances; the stomach may exhibit
associated disorder in the form of cardialgia, or more frequently in
the form of vomiting, this latter being very frequent at the outset of
the flow. Less common is profuse diarrhœa, pain in the anus, or
spasm of the sphincter ani.
The intensity of such nervous manifestations during menstruation
is dependent upon the woman’s general state of nutrition, upon
the degree of instability of her nervous system, and upon her occupation.
Robust and powerful women, regularly employed in the
open air, such as the wives and daughters of farmers and agricultural
laborers, are much less affected by the nerve-weakening influences
of menstruation than the sedentary and anæmic town-dwelling
women, whether these latter belong to the higher classes of
society and are addicted to nerve-straining enjoyments, or to the
class of shop-girls, seamstresses, and factory-women, whose employment
is apt to lead to nervous exhaustion.
As regards the forms of neuralgia most apt to accompany menstruation,
Windscheid mentions trigeminal neuralgia as the commonest,
especially affecting the first division of the nerve, and producing
localized pains which are to be distinguished from the headaches
already mentioned. They are characterized by their intensity
and their persistence in spite of anti-neuralgic treatment, and by their
spontaneous disappearance as soon as menstruation is over. According
to the same author, the relations between hemicrania and
the process of menstruation are indisputable; at the very least it
must be admitted that menstruation predisposes to an attack of
hemicrania.
152Cases also occur in which convulsions almost invariably accompany
menstruation, convulsions which are to be regarded as symptoms
of hysteria.
The extraordinarily powerful influence which the menstrual
stimulus exercises on the mind is shown by the frequency with
which the slighter psychopathic states occur as an accompaniment
even of normal menstruation, these manifestations being sometimes
melancholic in type, sometimes maniacal or erotic, and, when of
long duration, leading ultimately to pronounced mental disorder.
This influence of the menstrual stimulus is yet more potent in cases
in which important changes in the course of menstruation have
occurred, in cases, for instance, of suppressed, painful, or irregular
menstruation. In this connection, however, in order to avoid a
confusion of cause and effect, we must carefully bear in mind, that
it is a much commoner causal sequence for psychical disorders to
disturb the normal course of menstruation, than for disorders of
menstruation to evoke psychical disorders. This view has only quite
recently become established, and for this reason it is necessary to
regard such data when obtained from the writings of the older
gynecologists in a somewhat critical spirit.
By the modern alienist, the influence of the menstrual reflex on
mental affections is recognized only in cases in which a proper valuation
of the predisposing causes has been made, in such cases as the
following: First, we have to recognize the modifying influence
exercised by the menstrual stimulus on established psychoses, inasmuch
as these latter not infrequently undergo cure when previously
irregular menstruation has become regular, and, moreover, the recurrence
or the first appearance of menstruation has often a powerful
influence on the course of some established mental disorder.
In some cases this influence is a strikingly favorable one on psychoses
that have developed before the commencement of menstruation,
or during the suppression of that function; it may be, however,
and, indeed, more frequently is, an unfavorable influence, inasmuch
as such a psychosis, on the first appearance or on the reappearance of
menstruation, may assume a menstrual type, the attacks becoming
more frequent or more violent with the successive recurrence of
each menstrual or premenstrual period. This is the history of the
typical menstrual psychosis.
Again, certain processes of the sexual life, disorders of menstruation,
diseases of the genital organs, operations on these organs, and
the processes of the climacteric, influence the origin and the character
of mental disorder, generally giving rise to chronic affective insanity
(insanity of the emotions and feelings) or to paranoia
(chronic delusional insanity, insanity of the intellect). The menstrual
153stimulus must in these cases be regarded as a psychopathically
exciting physical cause.
Further, physical disturbances may equally affect the menstrual
function and the functions of the mind, rendering the exact causal
sequence in such cases a difficult one to determine; and, conversely,
the circumstances that restore the normal working of the mind may
also regulate the menstrual function.
Finally, we may have to do with isolated sporadic occurrences in
which the exciting influence of menstrual processes may be traced.
Thus, for the outbreak of a periodical menstrual psychosis, an especial
temporal predisposition must exist, connected with the great
developmental epoch of the sexual life.
There is, for instance, a group of transitory states occurring during
menstruation, and taking the form of disorders of the intelligence
or of explosive emotional states; such may be witnessed, not
in those suffering from psychopathic predisposition, but in quite
healthy individuals.
The successive menstruations as they recur regularly throughout
the course of the sexual life may, just like the first menstruation,
though with diminished intensity, give rise to manifestations of
nervous and mental disorders. In many women who are in other
respects healthy, we see during menstruation, hemicrania, nervous
irritability, ill-temper, low-spiritedness, and even hysterical and
epileptic attacks; these occur chiefly on the first and second days of
the flow, and disappear altogether toward the end of the period.
These manifestations are more severe in individuals weakened by
profuse losses of blood or by chronic disorder in various organs,
more severe also in those predisposed to such disturbances in consequence
of neuropathic inheritance, more severe in women suffering
from menorrhagia and dysmenorrhœa, and from any kind of
mental stress.
In his work on the influence of the so-called menstrual wave on
the course of mental disorders, Schüle remarks that the mental
equilibrium even of a perfectly healthy woman is not a stable one,
but is subject to a series of oscillations. “The menstrual period,”
he continues, “has a distinct influence on woman’s mental equilibrium.
Even in those whose nervous system is a healthy one, menstruation
evokes a state, now of depression, now of excitement; in
neurotic women, on the other hand, menstruation may give rise to
nervous diseases which may equally exhibit the characteristics of
depression or the characteristics of excitement. In nervously predisposed
women, the influence of regularly established menstruation,
even when the circumstances are favorable, is pretty much the
same as the influence of menstruation when it first makes its appearance;
154the influence is merely somewhat weaker in so far as the
woman has learned to endure and to be patient. The menstrual
state, in nervously predisposed women, evokes the particular neurosis
to which the individual happens to be liable. The disorders most
commonly met with in this association are, hysteria, hemicrania,
swimming in the head, epileptic paroxysms, toothache, and neurasthenia.”
Especially frequent during menstruation is hemicrania. Sometimes
hemicrania may begin a day or two before menstruation, as a
prodromal sign, and may accompany its whole course, becoming,
however, less severe toward the end of the flow. Hysteria most
commonly manifests itself in association with menstruation by a
depressed emotional state, by tearfulness, by complaints made without
sufficient grounds, by globus hystericus or clavus hystericus;
sometimes also by paroxysms of muscular spasm; very rarely by
hystero-epileptic seizures. Epilepsy may occur either by day or by
night. Nocturnal seizures usually occur without any apparent external
cause, as a result of the central stimulus; diurnal attacks,
on the other hand, have usually some external exciting cause.
Often, however, years may elapse without any attack of major
epilepsy occurring, the disease manifesting itself in one or more of
the many varieties of the minor form (petit mal), as transient
absences of mind, attacks of vertigo, etc.
The nervous disturbance in a menstruating woman may be so
great as to lead to the production of psychoses. The question of
the existence of a menstrual insanity sui generis has been answered
by many alienists in the affirmative; by others, however, who see
in the alleged cases nothing specific, it has been answered in the
negative. The relation of menstruation to the mental disorder may
be a double one: 1, menstruation may occur repeatedly in the
course of an already established mental disorder; 2, menstruation
and its morbid variations may favor the occurrence of psychoses
that exist already in a latent form, and may lead to the origination
of psychoses to which the organism is predisposed.
In the former connection, Brierre de Boismont undertook an investigation
which showed that in women suffering from mental
disorder, an exacerbation of that disorder was to be observed during
menstruation. Schlager, who regards the menstrual process as
possessing when anomalous a high significance for the development
and course of mental disturbances, observed that in 33 per
cent. of women suffering from mental disorder, the menstrual state
had an unfavorable influence upon the course of that disorder, inasmuch
as it led to an increased irritability; in the rest of the
cases, however, menstruation was without influence upon the course
155of the ordinary chronic psychoses. In the cases that were unfavorably
influenced, epileptic attacks usually became more frequent,
and chronic melancholia became much more profound. Schröder
observed in chronic forms of melancholia that during menstruation
the sadness became intolerable and was associated with a
suicidal tendency; in chronic maniacal forms of mental disorder,
the excitement underwent an increase during menstruation. Von
Krafft-Ebing, as a result of his investigations into insanity during
menstruation, came to similar conclusions with regard to the unfavorable
influence of the menstrual process. Algeri likewise states
that menstruation notably aggravates the cerebral symptoms in the
course of mental disorders.
Other authors, Marcé and Kowalewski for instance, whilst emphasizing
the powerful influence exerted by menstruation on any
existing psychosis, point out that in some instances, as in states of
mental and physical depression, this influence is for the worse; but
in other instances, especially in states of maniacal excitement, the
condition of the patient undergoes notable amelioration during menstruation.
Schäfer also, in his researches into the relations between
the processes of menstruation and psychoses, discovered that
anomalies in the course of menstruation ran almost parallel with
anomalies in the course of mental activity.
In psychopathically predisposed women, disorders of menstruation,
such as amenorrhœa, delayed menstruation, and dysmenorrhœa,
are more effective than the normal process of menstruation in evoking
manifestations of psychical abnormalities previously latent, and
in leading to attacks of precordial anxiety, pathological emotional
states, melancholic seizures, epilepsy in all its varieties, and impulsive
manifestations, such as pyromania, kleptomania, infanticide,
homicide, etc. As results of a special predisposition may appear
in this connection, congenital imbecility, idiocy, melancholia, and
chronic weak-mindedness.
A rich literature exists of cases in which mental abnormalities
occurred in psychopathically predisposed individuals as a result of
menstruation. Thus, von Krafft-Ebing reports a case in which,
during menstruation, a mentally undeveloped woman murdered her
husband; and another case in which to chronic weak-mindedness
and chronic delusional insanity were superadded during menstruation
peculiar attacks having the character of psychical storms. Tuke
reports a case in which a mother, in a state of alcoholic excess during
menstruation, murdered her daughter. Pelmann records acts
of pyromania committed during menstruation by a girl seventeen
years of age. Mabille records a case in which a woman suffering
from severe mental disorder was affected during menstruation by
156impulsive kleptomania, whilst after the periods the memory of what
had happened passed away. Philo-Indicus records the case of a
woman suffering from severe neuropathy who at the menstrual
periods exhibited great irritability, experienced marked sexual excitement,
and had suicidal impulses, and who on one occasion attempted
to murder a female friend who had refused to assist her
in the practice of sexual aberrations. Giraud describes a woman
suffering from passive melancholia, in whom during menstruation
horrible fantastic ideas occurred. Ball records the case of a woman
who suffered always from acute mental disorder during menstruation,
and who, in one of these attacks, murdered her son. Kowalewski
reports a case of chronic imbecility, in which during menstruation
attacks of precordial anxiety developed, and in the course of
one of these attacks the patient set fire to her own house. “In
such cases,” remarks Kowalewski, “menstruation represents the
last drop that makes the full goblet overflow.”
In addition, we meet with cases in which the influence of menstruation
is so powerful that it must be regarded as the principal
cause of the psychosis. We must then speak of a true menstrual
psychosis, the impulse to which is supplied by the normal or abnormal
changes occurring in the process of menstruation, and
characterized by the menstrual periodicity and the brief duration
of the attacks. These are the characteristics of the menstrual psychoses
of the menarche and of the climacteric period; and such
cases occur also during the period of full menstrual activity.
The menstrual psychosis most commonly makes its appearance
shortly before the flow, becomes less severe with the establishment
of the flow, and disappears when the flow ceases; in other cases,
the psychosis appears toward the end of menstruation, and speedily
passes away; or, again, in amenorrhoeic cases, the attacks of mental
disorder replace the proper menstrual flow, and become less severe
or disappear entirely as soon as the flow is regularly re-established.
The commonest forms of these menstrual psychoses are, melancholia,
mania, irresistible impulses, acute amentia, in rare cases alternating
insanity (folie circulaire) in which the periods of alternation assume
the menstrual rhythm. The duration of these psychoses is
usually short, from a few days up to a fortnight; there may be only
a single attack, or there may be a number of attacks presenting
precisely similar characters.
The consciousness may be more or less disturbed. Von Krafft-Ebing
points out, as a very dangerous peculiarity of the menstrual
psychoses, that the fact that the morbid process has once occurred
in connection with menstruation furnishes in itself a sufficient reason
for the recurrence of such attacks, which are dependent on
157constantly repeated functional changes in the brain closely
analogous to those that occur in epilepsy. When the menstrual
insanity recurs frequently, it gradually becomes less acute in its
characters and more protracted in its course; the lucid intervals are
less clearly indicated and shorter in duration; and thus in course of
time the mental disorder may be transformed into chronic imbecility—a
transformation liable to occur in all forms of periodic psychosis.
In such cases we must always assume the existence of a certain lack
of resisting power on the part of the organism, especially of the
nervous system, which amounts to a congenital predisposition. During
the period of full menstrual activity, the favorable soil for the
cultivation of such disorders is usually furnished by anomalies of
menstruation, by difficult labor and its consequences, severe losses
of blood, prolonged lactation, physical over-exertion, and mental
shock and stress.
In the development under the influence of menstruation of such
periodic acute mental disorders, we may observe various gradations,
as for instance short, syncope-like cataleptic seizures, states of
hallucinatory confusion lasting several hours or several days, disordered
consciousness, and even severe mania.
Such a case was observed by Wille. Under the influence of menstruation
and of a trifling source of mental disturbance (having
soldiers billeted on them in a quiet country village), a young woman
aged twenty-one, whose mental health had previously been good,
had a sudden attack of anxiety, succeeded by a violent but transitory
mania, lasting five or six hours; after a short free interval came
another attack, this time lasting several days. Similar cases were
recorded by Friedmann. A blooming and healthy maid-servant
eighteen years of age (some mental unsoundness was recorded in
both grandfather and aunt on the maternal side) fell asleep in a
chair a few days before menstruation, awakened with a start, was
subsequently disordered in mind, though tranquil, with many
hallucinations, listening to voices which repeated monotonously
“they come,” was drowsy, and slow to answer when spoken to. On
the third day she was recovered, her mind being clear and normal;
she was not fully aware of what had happened. Since this attack,
her mind has been free from disorder, during menstruation as well
as at other times. She is said to have had a similar attack about
four years ago, that is, at the commencement of puberty.—A girl
aged thirteen, quite healthy, not nervous, physically rather powerful,
with quite healthy family history. Complaints of having
suffered for two days from general sense of depression with pains
in the abdomen; during the afternoon was lying on a sofa, but
suddenly sprang up, looked extremely anxious and confused, ran
158about the room, begged to be protected from the black man, etc.,
her speech was disconnected, gabbling, and difficult to understand.
After two hours she became quiet, and fell into a sound sleep, from
which she awoke calm and quite forgetful of what had passed. On
the following day menstruation appeared for the first time, with
abdominal pains, but without any mental abnormality. During the
subsequent six years she has remained quite well.
Since the days of antiquity an extremely important part has been
assigned to suppression of the menses in the production of mental
disorders; but in the opinion of modern alienists, who are opposed
to the old humoral pathology, no more is to be recognized in this
connection than the ordinary menstrual stimulus, which, indeed,
when the soil is already prepared, may furnish a causal determinant
for an increase in the intensity of an already existing anomalous
mental condition. Quite recently numerous cases have been published
in which such an influence has been recognized as powerful.
Von Krafft-Ebing writes: “In isolated cases, as a sequel of sudden
cessation of the menstrual flow, generally, due to a fright or to a
chill, the development of insanity (usually acute mania) has been
observed, and the suppression of menstruation has been regarded as
the causal determinant. It is indeed conceivable that the connection
between the two events is supplied by a collateral vicarious congestion
of the brain. As a rule, however, the psychosis and the suppression
of menstruation are the coeffects of the same cause, and
are both of vasomotor origin.”
Mairet reports a case of violent mental disorder of a maniacal
type, associated with chorea, occurring at puberty, the exciting cause
of which, in a constitution hereditarily predisposed to insanity, he
believed to be suppression of the menses. Diamant had under observation
a girl in whom, at the age of six years, menstruation ceased,
having previously been regular since the age of two years; after the
suppression of menstruation, violent epileptiform seizures set in,
occurring at what should have been the menstrual periods. Westphal
described a case of infanticide committed in a state of melancholia
at the proper menstrual period, the menses being suppressed.
Menstrual psychoses are observed for the most part in comparatively
young women; after the age of thirty-five they are uncommon.
Among von Krafft-Ebing’s cases there were:
| 4 patients between the ages of |
15 and 20 years. |
| 6 patients between the ages of |
20 and 25 years. |
| 2 patients between the ages of |
25 and 30 years. |
| 6 patients between the ages of |
30 and 35 years. |
| 2 patients above the age of |
35 years. |
The same author insists that for the development of a menstrual
psychosis a predisposition on the part of the brain must exist, either
159in the form of an inherited predisposition, or in the form of a primary
mental disorder, or, finally, as the result of some special exciting
cause, such as emotional disturbance, the abuse of alcohol, or bodily
illness. Among 19 cases observed by von Krafft-Ebing
| 12 |
were hereditarily predisposed. |
| 4 |
had previously exhibited great nervousness during menstruation. |
| 7 |
suffered from primary mental weakness. |
Very remarkable is the influence, demonstrated especially by
Lombroso, exercised by menstruation on the commission of certain
crimes. Of eighty women taken into custody for resisting the police,
there were nine only who were not menstruating at the time. Four
notorious murderesses and one woman convicted of arson were all
menstruating at the times when their crimes were committed.
Krugenstein found evidence of menstruation in the bodies of 107
women who committed suicide. Thefts committed by ladies in the
great shops of Paris are most commonly effected during menstruation,
as was found by Legrand du Saulle to be the case in thirty
five instances out of fifty-six investigated by him in respect to this
matter. According to the same author, hysterical girls who steal
articles of clothing, bottles of scent, and the like, from the counters
of shops, are almost always menstruating at the time.
Von Krafft-Ebing puts forward the following propositions with
regard to the forensic significance of offences committed by women
during menstruation: 1. The mental integrity of a menstruating
woman is questionable from the forensic standpoint. 2. In the case
of women on trial for any offence, the point should be determined
whether that offence was committed at a menstrual period. 3. An
inquiry into the mental condition is expedient in cases in which
such a coincidence is established; light is thrown on the matter when
investigation shows the existence of hereditary predisposition, when
we learn that psychopathic manifestations have occurred at previous
menstrual periods, or when the very nature of the offence is one
suggesting the presence of mental disorder. 4. A recognition of
the powerful influence which the menstrual process exercises upon
the mental life should lead, even in cases in which no menstrual
psychosis has been proved to exist, to the admission of extenuating
circumstances in apportioning the punishment for the offence. 5. In
the case of the commission of a punishable act during menstruation
by a weak-minded individual, we must as a rule admit the plea of
irresponsibility—at any rate in the case of an offence committed under
the influence of strong emotion. 6. Persons who have been discharged
without punishment on the plea of mental disorder accompanying
menstruation must be regarded as dangerous to the community,
and should always be under careful supervision during the
menstrual periods.
160
Amenorrhœa, Menorrhagia, and Dysmenorrhœa.
Amenorrhœa, permanent or transient abnormal lack of the menstrual
flow, may depend upon anatomical changes in the genital
organs, upon incomplete development or absence of the uterus and
the ovaries, upon enduring or transient defective nutrition or
upon atrophy of these organs, or upon parenchymatous disease
of the ovaries; or it may be due to functional disturbances of ovarian
activity, itself dependent upon changes in the nervous system, upon
constitutional diseases, or upon general nutritive disturbances in
the body. Among the latter conditions must be especially mentioned
chlorosis, obesity, diabetes, chronic alcoholism, and morphinism,
myxoedema, exophthalmic goitre, etc.
The amenorrhœa that occurs at the time of the menarche has
already been described in connection with the symptomatology of
that period.
If in cases of amenorrhœa the ovaries continue to perform their
functions, we frequently witness severe and painful menstrual
molimina, occurring periodically at the times when the flow might
be expected, but fails to appear. In cases of atrophy of the uterus
and the ovaries, we see complete and permanent amenorrhœa without
any discomfort. As a kind of vicarious menstruation, in certain
cases of amenorrhœa, we see hæmorrhages into the vitreous body
or conjunctival hæmorrhages; also, as more extensive disturbances
of the visual organs, interstitial keratitis, disseminated choroiditis,
intermittent amaurosis, acute retrobulbar neuritis, amblyopia, and
limitation of the field of vision.
Mooren publishes the following cases, showing the influence of
amaurosis on the eye. A girl aged fourteen, with severe bilateral
pannous keratitis, was amenorrhoeic notwithstanding the existence
of well-marked menstrual molimina. Every four weeks, at the times
when the menstrual flow should have appeared, the corneal inflammation
became more severe; it became amenable to treatment for
the first time a year later, when the menstrual flow had become
established. A peasant woman, twenty-eight years of age, had never
menstruated; the uterus was badly developed; every month an intolerable
heat and swelling of the face recurred. Since the age of
fifteen she had suffered from bilateral interstitial keratitis, which
had resisted all treatment, and had been subject every four weeks
to a recurrent exacerbation of this trouble, lasting several days. The
exhibition of powerful emmenagogues and the use of Friedrichshall
water brought about on a few occasions a scanty discharge of blood.
The comfort to the patient, relieved as if by miracle from her pain
and photophobia, was most remarkable. Unfortunately, however,
this state of comparative happiness lasted from twelve to fourteen
161weeks only, after which, in spite of everything that was tried, there
was no further recurrence of menstruation, and the condition of the
eyes relapsed to what had existed for thirteen years. In other cases
described by Mooren the amenorrhœa was complicated with disseminated
choroiditis and with posterior sclero-choroiditis.
Beer reports a case of retrobulbar neuritis occurring with amenorrhœa,
consequent on infantile aplasia of the uterus. An interesting
case was recorded by Dunn of a girl fifteen years of age, who had
not yet begun to menstruate, and who suffered from interstitial
keratitis, with severe photophobia. The ocular symptoms vanished
with extreme rapidity as soon as menstruation first appeared.
Napier observed complete blindness, without discernible anatomical
cause, associated with amenorrhœa of sudden onset; the amaurosis
disappeared as soon as menstruation was re-established.
Striking and manifold are the disturbances of the nervous system
which may be caused by amenorrhœa, ranging from increased irritability,
hyperæsthesia of various nerve tracts, neuralgia, and the
like, to severe psychoses.
Barnes reports a case of mental disturbance consequent upon
amenorrhœa in a woman twenty-seven years of age, who had begun
to menstruate when sixteen years old, and in whom the menses
had been suppressed a year earlier when she was informed of the
sudden death of her father. From that time a progressively increasing
weakness of the mind was observed. In a case recorded by
Macnaughton Jones the mental depression consequent on amenorrhœa
was so great that it led to an attempt at suicide.
Lawrence observed in young girls who from any cause suffered
from amenorrhœa, that an increased pigmentation of the skin sometimes
occurred, analogous to that met with in Addison’s disease.
This amenorrhoeic pigmentation he compares to the chloasma that
is seen in pregnant women.
By menorrhagia we understand the occurrence of typical discharges
of blood from the uterus, occurring at more or less regular
intervals and differing from normal menstruation in respect either
of the greater intensity or of the longer duration of the hæmorrhage;
whereas by metrorrhagia we understand the occurrence of atypical
discharge of blood from the uterus, which is related to menstruation
neither in respect to its causation nor in respect to the time of its
appearance.
Menorrhagia may be due to local changes in the genital organs,
to organic diseases of other organs, and to general diseases.
Local changes which may give rise to menorrhagia are, active
hyperæmia and passive hyperæmia (hyperæmia from engorgement)
of the genital organs, such hyperæmia being itself due to sexual excitement,
162especially when ungratified, to violent physical exercise, or
to chill during menstruation; menorrhagia is also liable to occur
when the abdominal circulation is disturbed by extreme obesity or by
the presence of tumors, also in connection with endometritis, uterine
myomata, erosions of the cervix, etc. Diseases of organs other
than those belonging to the reproductive system which are especially
likely to give rise to severe bleeding are, disease of the heart,
such as valvular incompetence, lung disease, and nephritis. General
diseases in which menorrhagia may occur are, anæmia, chlorosis,
hæmophilia, scurvy, scarlatina, cholera, smallpox, influenza, and
obesity.
Through severe loss of blood in menorrhagia, whether the bleeding
be sudden and profuse or more moderate but long continued, a
condition of chronic anæmia results, with all its threatening consequences
to the health and the life of the woman affected. She becomes
pale and weak, unfitted for any great physical or mental
exertion, and is liable to attacks of cardiac enfeeblement and to
fainting fits; in some cases degenerative changes ensue in the cardiac
muscle.
Dysmenorrhœa is characterized by severe pain occurring before,
during, and after menstruation. The pain is caused either by abnormally
powerful contractions of the uterus or else by abnormal sensitiveness
of that organ. Abnormally powerful contractions are
caused by various mechanical hindrances to the normal processes of
menstruation; abnormal sensitiveness is due to inflammatory and congestive
states of the uterus and its annexa or to a general increase
of nervous sensibility.
Schauta, therefore, distinguishes a mechanical, an inflammatory,
and a nervous form of dysmenorrhœa. Mechanical dysmenorrhœa
is most frequently due to stenosis or flexion of the canal of the
cervix in some part of its course from the internal to the external
os, dependent upon malformation or flexion of the uterus, hyperplasia
of the mucous membrane, chronic metritis, scarring resulting
from operative procedures, uterine polypi, etc. In inflammatory
dysmenorrhœa we have to do “either with an inflammatory process
or with excessive tension of the intrapelvic organs, dependent
upon abnormal distension of their blood vessels.” To the same
category belong ovarian dysmenorrhœa, and dysmenorrhœa due
to inflammatory changes in the Fallopian tubes and to pelvic peritonitis.
In nervous dysmenorrhœa, no anatomical cause is apparent,
but the uterine contractions normally occurring during menstruation,
and the normal congestive distension of the intrapelvic organs
at that period, become extremely painful, in consequence of a
morbid increase in the sensibility of the nervous system.
163The influence of dysmenorrhœa on the general condition of the
woman suffering from it is often a very potent one.
The normal undulatory course of the bodily temperature—which
as Reinl has shown, undergoes a gradual rise until shortly before
the appearance of the menstrual flow, gradually falls during menstruation,
and continues to fall for a time after menstruation is over—undergoes
a change in cases of dysmenorrhœa due to anteflexion
of the uterus, parametritis, or salpingitis, inasmuch as in these cases
the acme of the temperature curve is reached actually during menstruation
and the decline of temperature comes, not at the commencement
of the menstrual flow, but often only after the flow has ceased.
The curve of blood pressure and the curve indicating the excretion
of urea are similarly affected in these cases.
As symptoms in other organs occurring in cases of dysmenorrhœa
Schauta mentions “sensations of heat, coldness of the feet, retching
and vomiting, cramps of the stomach and of the voluntary muscles,
general disorders of nutrition, loss of appetite, strangury, constipation,
dyspepsia, headache, and finally hysteria. As symptoms
of the latter affection we may notice, anæsthesia, hyperæthesia of
certain parts of the abdomen, attacks of cramp, paralysis, uterine
cough, hiccough, spasm of the glottis, epileptiform seizures. The
repeated severe attacks of pain may seriously disturb the nervous
system, leading to the appearance of general neuroses and psychoses.
Frequently we observe, as a peculiar accompaniment of dysmenorrhœa,
changes in the fulness of the blood vessels of the face and
also in other regions of the skin, in consequence of vascular paralysis.
In other cases, actual effusion of blood occurs, and, as a sequel
of this, deposits of pigment; and the semicircles beneath the eyes
may become so dark as to look as if they had been artificially tinted
(Macnaughton Jones). In one case, during menstruation periodic
swelling of the gums was observed (Regnier). Finally, in association
with dysmenorrhœa, various forms of neuralgia, changes in
refraction, and slight attacks of neuritis and retinitis may occur.”
One of the commonest symptoms and sequelæ is headache, sometimes
in the form of hemicrania, which may be associated with
dyspeptic manifestations, sometimes diffused over the whole surface
of the skull.
Dyspepsia is a very frequent associate of dysmenorrhœa. Thus
we meet with pain and tenderness in the gastric region, nausea,
vomiting, and also cardialgia. Sometimes the liver becomes enlarged
and tender on pressure; in many cases also jaundice is
witnessed.
Gebhard refers to another phenomenon which may be classed
under the head of dysmenorrhœa, from the character of the pain
164that is experienced, even though this pain is not felt at the menstrual
periods, but in the intermenstrual epoch. This is the so-called
intermediate dysmenorrhœa (intermenstrual pain, Ger.
Mittelschmerz). In the character of the localized pain, intermediate
dysmenorrhœa closely resembles ordinary dysmenorrhœa; it
recurs often with precise regularity on certain days during the intermenstrual
interval. Croom distinguishes three forms of intermediate
dysmenorrhœa; that in which there is no discharge at all from the
uterus, that in which there is a sanguineous discharge, and that in
which there is a clear watery discharge. The first form he attributes
to asynchronism in the processes of ovulation and menstruation;
the second form, to endometritis with disintegration of the mucous
membrane; the third, to a kind of hydrops tubæ profluens (profluent
dropsy of the Fallopian tubes—hydrosalpinx in which the fluid
accumulates in the tube, and at a certain stage of its accumulation
flows into the uterus). Cases of intermediate dysmenorrhœa are
somewhat rare, if we eliminate the cases in which pains occur in
the intermenstrual epoch in consequence of disease of the uterine
annexa. Inflammatory manifestations may be discovered in nearly
all typical cases of intermediate dysmenorrhœa.
Long-continued dysmenorrhœa may give rise to numerous hysterical
troubles, general convulsive seizures, local muscular spasm
and paralysis, hiccough, spasm of the glottis, uterine cough, twitching
and spasm of various groups of voluntary muscles. In some
cases we see fully developed epileptic convulsions, with complete
loss of consciousness and immobility of the pupils. Finally, psychoses
may arise in association with dysmenorrhœa.
In cases of pathological changes in menstruation, a carefully arranged
hygiene at the menstrual periods is of importance both for
prophylactic and for therapeutic purposes, and in this connection
I may refer to what I have written in the section on Hygiene during
the Menarche. In cases of dysmenorrhœa a certain amount of
repose and precaution are needed during the flow, with avoidance of
chill, scrupulous cleanliness, and regulation of the bowels. In cases
of amenorrhœa we must prescribe attention to the general nutrition
by means of an easily digested roborant diet, as much fresh air as
possible, and systematic bodily exercise. In these cases, bicycling,
lawn tennis, and suitable gymnastics are often of value; also baths,
in the form of warm general baths, hot sitz baths, and hot foot baths.
Vicarious Menstruation.
In cases in which, in consequence of morbid conditions of the
uterus, the ovaries, or the organism as a whole, the menstrual flow
has at the time of the menarche either failed entirely to appear or
165been exceedingly scanty, hæmorrhages from other organs have since
ancient times been witnessed, and these hæmorrhages have been
regarded as vicarious menstruation. The congestion that occurs
during menstruation is not limited to the genital organs, and when
the flow of blood from the uterus fails to occur, the organism seeks
another outlet, in order to restore the disturbed equilibrium of blood
distribution, and vicarious hæmorrhages take place from the mouth,
the nose, the intestines, the anus, the gums, the mammæ, the ears,
and the lungs; or hæmorrhages occur in the brain, the nerves, or
the eyes.
Although it must be admitted that confusion has often occurred
between vicarious menstruation and hæmorrhages dependent on
pre-existing genuine organic disease, such as hæmoptysis due to
pulmonary tuberculosis, or hæmatemesis due to gastric ulcer, still the
existence of a true vicarious menstruation must be regarded as fully
established.
Thus, Fricker, Fleischmann, Obermeier, Beigel, Withrow, Plyette,
and Parsons observed vicarious epistaxis; Watson, Decaisne, Edebohls,
Fischel, and Seeligmann, vicarious hæmatemesis; Franchi,
Hotte, Ratgen, Voigt, and Windmüller, vicarious hæmoptysis;
Dunlap, vicarious gingival hæmorrhage; Law and Petiteau, vicarious
otorrhagia; Heusinger and le Fort, vicarious hæmorrhages, occurring
variously from the anus, bladder, hand, ear, nipple, stomach,
and nose; Baumgarten, vicarious hæmorrhage from the vocal cords
and trachea; Hahn, from the bladder; Kerley, in the thyroid body;
Gallemairts, in the eyes. Puech found, in the cases he collected, that
vicarious menstrual hæmorrhage occurred from the stomach thirty-eight
times, from the mammary glands twenty-five times, from the
lungs twenty-four times, and from the nasal mucous membrane
eighteen times. In all the cases menstruation had long been in
abeyance.
Regarding vicarious epistaxis, especially exact observations have
been published, showing the mutual relationship between the genital
and the nasal mucous membrane. A series of cases has been recorded
by Fliess. In one of these a remarkably well-developed girl
of fourteen, who complained at three-weekly intervals of molimina,
in the form of languor, headache, and sacrache, after an interval of
four weeks epistaxis occurred instead of the expected menstruation;
three weeks later came another attack of epistaxis; and finally, after
an interval of seven weeks, came the first menstruation, which henceforward
recurred every three weeks. In another case, that of a
girl aged fifteen, menstruation appeared once; four weeks later came
an attack of epistaxis instead of menstruation, and these attacks of
epistaxis were continually repeated, at intervals of twenty-nine days,
166in place of menstruation, until finally pregnancy occurred. During
pregnancy the epistaxis ceased, to recur however six weeks after
parturition; the attacks continued for eight monthly periods, when
they ceased finally at the commencement of the second pregnancy.
Other similar cases are known in which epistaxis recurred with
all the regularity of the menstruation it replaced during pregnancy
and ceased at parturition. Analogous cases occur in which epistaxis
has persisted during pregnancy, during the puerperium, and at the
climacteric period, replacing the physiologically suppressed menstrual
flow. Similarly Liégois has observed vicarious hæmoptysis
during pregnancy. According to Baumgarten, in vicarious epistaxis
the bleeding almost always proceeds from the region of the cartilaginous
septum, and may become very violent; vicarious hæmorrhage
from the larynx proceeds from the true and false vocal cords.
Tracheal hæmorrhage is a much rarer occurrence.
Analogous to these cases are those in which the vicarious hæmorrhages
occur after removal of the ovaries. Thus Tauffer in one case
saw epistaxis replace menstruation after this operation. Schmalfuss
reports a case in which a woman suffering from valvular disease
of the heart, was said after oöphorectomy to have had almost
daily attacks of hæmoptysis and epistaxis. Glaevecke found in the
post-operative history of forty-four cases of oöphorectomy that two
patients suffered from vicarious hæmorrhages. The last-quoted
author is of opinion that the suppression of menstruation resulting
from oöphorectomy rarely leads to vicarious hæmorrhages, and that
even when these do occur they are so inconsiderable in amount as
to have no practical significance.
Quain records the case of a woman aged thirty-three, in whom
uterus and ovaries were absent, and in whom for two years epistaxis
recurred every month with considerable regularity.
In cases in which menstruation is in abeyance, we sometimes witness,
instead of vicarious hæmorrhages, the occurrence of non-sanguineous
vicarious discharges from various mucous membranes.
Thus, vicarious leucorrhœa is seen, especially in chlorotic patients,
in whom, from the time of the menarche onward, such a discharge
may occur every month, instead of the delayed menstruation. Similarly,
vicarious diarrhœa and vicarious salivation have been observed.
The Sexual Impulse.
By the term sexual impulse, we understand the impulse shared by
women and by men towards intimate physical contact and sexual intercourse
with individuals of the opposite sex. In the child this
impulse slumbers, to awaken at the menarche with the onset of puberty,
167to increase slowly at first, and then more rapidly, after the
manner of an avalanche, until it becomes a powerful passion, dominant
throughout the active sexual life of the woman, and it may
even continue far beyond this period. The proper aim for whose
attainment the sexual impulse in woman strives is by no means
(as is asserted in some quarters) the fulfilment of “the impulse
toward motherhood,” but is merely the complete satisfaction of
sensual passion by intercourse with the male. Still, the sexual impulse
is often satisfied by the minor degrees of sexual gratification in
the form of the mutual contact, so agreeable to the sense of touch,
of portions of the body, and even by the play of imagination and
illusion under the dominion of love. Finally, also, love amounts
to what Buffon, the celebrated naturalist, expressed with coarse
incisiveness in the phrase, “L’amour c’est le frôlement de deux
intestins.”
In the sexually mature woman, the sexual impulse always exists,
though its strength varies in accordance with individual inheritance,
with physical and mental condition, and with external circumstances,
and though its manifestation may be repressed by force of will.
The sensation of the sexual impulse in a maiden during the years
of development is described by Goethe in a masterly manner in the
verses.[33]
“Meine Ruh ist hin
Mein Herz ist schwer,
Ich finde sie nimmer
Und nimmermehr.
Mein Busen drängt
Sich nach ihm hin,
Ach, dürft ich ihn fassen
Und halten ihn
Und küssen ihn,
So wie ich wollt,
An seinen Küssen
Vergehen sollt.”
A resemblance to heat or rut in animals, who exhibit the sexual
impulse only at definite periods, those at which the ovules ripen,
is manifested in females of the human species only in so far as there
168is during menstruation a more intense sexual sensibility; but the
limitation of the sexual impulse to definite periods, and its close
association with reproduction, are not found in women. Education
and morality impose artificial limitations on the sexual impulse
in women, whilst nature endows this impulse with a coercive
power, a fact recognized by thinkers of all times and all peoples.
Thus, Buddha wrote: “The sexual impulse is stronger than the
ankus with which the wild elephant is controlled, it is hotter than
flame, it is like unto an arrow driven into the spirit of man.” In
a similar sense Luther writes: “He who wishes to restrain the
impulse of nature and not to allow it free play, as nature will and
must, what does he do but this, to insist that nature shall not be
nature, that fire shall not burn, that water shall not wet, that man
shall neither eat, drink, nor sleep.” Schopenhaur describes the
sexual impulse as “the completest outward manifestation of the
will to live, the concentration, that is to say, of all wills. * * *
The affirmation of the will to live concentrates itself in the act of
generation, and this act is its most determined expression.” Mainländer
in his Philosophy of Deliverance makes the following statement:
“In the sexual impulse lies the centre of gravity of human
life. To nothing does man devote a more earnest attention than to
the business of generation, and in the pursuit of no other aim does
he concentrate the intensity of his will in so striking a manner as
in the performance of the act of generation.” Debay similarly
insists on the strength of the sexual impulse, saying: “The union
of the sexes is one of the great laws of nature; to that law men
and women are subordinated as completely as all other creatures,
they cannot escape its operation.”
According to the general opinion, the sexual impulse is not so
strongly developed in women as it is in men. Hegar, Litzmann,
Lombroso, P. Müller, and many others, assume that the sexual sensibility
of women is less than that of men; Fürbringer is inclined
to attribute the characteristic of sexual frigidity to the great majority
of German wives. I do not believe that this view, of the
slight intensity of the sexual impulse in women in general, is well
grounded, and can admit only this much, that in adolescent girls
who are inexperienced in sexual matters, the sexual impulse is less
powerful than in youths of the same age who have undergone
sexual enlightenment. From the moment when the woman also has
been fully enlightened as to sexual affairs, and has actually experienced
sexual excitement, her impulse toward intimate physical
contact and toward copulation is just as powerful as that of men.
According, however, to the dominant artificial conditions, man assumes
it as his right to give free rein to his sexual desires and
169to gratify them without regard to consequences, whereas woman,
narrowly confined within the boundaries imposed by law and convention,
cannot so readily yield to her inclination in the direction
of physical love, and must forcibly control that inclination. Moreover,
a powerful check on the free indulgence of the sexual impulse
is imposed on woman by the consequences of such indulgence,
consequences which exist for woman only.
I may further indicate as differential characteristics, that in woman
the sexual impulse is more accessible to voluntary control than it
is in man, the ardor of female sexual passion is more readily diminished
than that of the male; and again that in the female the gratification
of the sexual impulse is less narrowly restricted than in the
male. Excessive sexual gratification on the one hand and suppression
of sexual desire on the other are, generally speaking, less harmful
to the female organism than to the male. In these differentiæ is
to be found, in my opinion, the influence which determines the type
of sexuality in the respective sexes.
The following account is given by Havelock Ellis of the differential
characters of the sexual impulse in the female: “In courtship, woman
plays a more passive part than man; in woman the physiological
mechanism of the sexual processes is more complicated, and the orgasm
develops more deliberately; the sexual impulse in woman needs
more frequently to be actively stimulated; the culmination of sexual
activity is attained later in the life of woman than in the life of man,
the strength of sexual desire in woman becomes greater after she has
entered upon regular sexual intercourse, women bear sexual excesses
better than men; the sexual sphere is larger and more widely diffused
in women than it is in men; finally, in woman the sexual impulse
exhibits a distinct tendency to periodic exacerbations, and it
is in any case much more variable than in man.” The same author,
who has published several notable biological studies on subjects
connected with sex, maintains that the source of erotic pleasure in
the case of the male lies in activity, but in the female in the passive
state, in the experience of compulsion, and he holds that sexual
subordination is a necessary element in the sexual enjoyment of
women.
Hegar maintains that under the term sexual impulse two distinct
conceptions are confounded: First, the impulse toward copulation,
the desire of carnal union with a member of the opposite sex;
secondly, the impulse toward reproduction, the desire for children.
At the same time, this author admits that it is questionable if we
can properly speak of an impulse toward reproduction, when reproduction
is merely a consequence of copulation; in the case of civilized
man, at any rate, so much reflection is connected with the idea of
170reproduction that it can hardly be proper to speak of anything of
the nature of an impulse. In the case of woman, the expression is
less unsuitable, since in woman special organs exist for the maintenance
of the ovum after fertilization, and these organs may perhaps
lead to the production of this peculiar form of mental activity.
According to Darwin, a comparatively less intensity of sexual desire
is common to the females of all species of the animal kingdom.
The female demands a prolonged courtship, and often endeavors
for a considerable time to elude the male. In the lowest classes of
the animal kingdom the female leads a separate existence as soon as
she has been fertilized by the male, the sexual functions being thus
subordinated to the maternal. Among birds at the pairing season
the male is always the more passionate and active of the two, whilst
the female commonly remains passive and occupies herself in building
the nest. Among mammals, it is difficult to determine whether
sexual feeling is stronger in the female or in the male; but it is
certain that sexual relations are seldom long lasting, they continue
in most cases only during the period of heat or rut, and at most
only till the birth of the young.
From these phenomena witnessed in the animal kingdom, many
naturalists have concluded that in females of the human species also,
sexual sensibility and the intensity of the sexual impulse are less
than in the males, and even that the sexual sense in general is but
little developed in the female sex, or sometimes entirely wanting.
The complicated apparatus which the primary and secondary sexual
characters of the female combine to make up, exists, according to
this view, not for the gratification of the sexual impulse, but for the
fulfilment of the function of motherhood. “Love in women,” says
Lombroso, “is in its fundamental nature no more than a secondary
character of motherhood, and all the feelings of affection that bind
woman to man arise, not from sexual impulses, but from the instincts,
acquired by adaptation, of subordination and self-surrender.”
Mantegazza lays stress on the fact that in the female, sexual desire
is very rarely accompanied by pains analogous to those which
occur in man, in whom sexual excitement manifests itself in painful
tension of the testicle and the seminal vesicles, or in spasmodic,
long-continued priapism.
Sergi writes to Lombroso: “The normal woman loves to be flattered
and wooed by man, but yields herself to his sexual desires only
like an animal at the sacrifice. It is well known how much pains
must be taken, how many caresses must be expended, before a woman
will yield with pleasure to a man’s desires, and will share his sexual
passion. Without the employment of these means, a woman remains
cold and gives as little satisfaction as she feels. There are girls
171who are quite obtuse to the joys of love, and either resist energetically
a man’s approaches, or yield to him passively, without ardor and
without enthusiasm. It is well known, also, that among the lower
races of mankind, means are employed to stimulate the sexual sensibility
in women, means that seem to us to amount to torture; and
that the male, with the same end in view, undergoes the most painful
operations, from which it is apparent that the slight sexual
sensibility of women in these lower grades of civilization is fully
recognized.” And again: “If a normal woman marries for love,
she hides that love deep in her heart, and even on the wedding-day
exhibits no great sexual excitement; she often complains later that
in her husband the love-fervor of the first days still continues; the
very moderate sexual needs of the wife form a natural and most
valuable check to the much more powerful passion of the male.”
Saint Prospêre expresses himself to a similar effect: “Women
do not fall in consequence of the excessive power of the senses—in
this domain they are overlords, in striking contrast to men, whose
weakest side is here. It is not by means of the senses that a woman
is to be overcome; her weakness lies elsewhere—in her heart, in
her vanity.” And de Lambert wrote the epigram, “Women play
with love, and yield themselves to love, but they do not abandon
themselves to love.”
Well known also is the saying of Dante:
“We know how speedily in women the fire of love is consumed
Unless eye and hand continually supply it with fresh fuel.”
On the other hand, it is asserted in the laws of the Hindus that
sexual desire in women can as little be satisfied or fed full as a devouring
fire can be fed full of combustible materials, or as the ocean
can be overfilled by the rivers that pour their waters into it.
Lombroso finds a proof of the sexual indifference of women and
of the greater sexual needs of man, in the existence of prostitution,
with which can be contrasted the existence only among the degenerate
classes (both rich and poor) of a small group of male prostitutes
(alfons, souteneurs). This author also refers to the rarity and
uniformity in women of the sexual psychoses so frequent in men,
as indications of the minor intensity of sexual desire in the former;
and he refers also to a series of facts, as for instance, to the occurrence
of platonic love, which, though indeed often hypocritical, has
a real existence more often in the female sex than in the male; to
the long-enduring chastity of girls, and to vows of chastity,
which are rarely made except by females; moreover, the ready adaptation
of women to polygamy, as well as their scrupulous observance
of monogamy, which latter for the male is nominal rather than
172actual. If in general the opposite view concerning women prevails,
this is ascribed by Lombroso to the fact, that love is the most important
circumstance in a woman’s life. The reason therefore, however,
is to be found, not in the erotic sphere, but in the desire for the
satisfaction of the maternal instinct, and in a woman’s need for protection.
A celebrated accoucheur, Giordano, has remarked: “Man
loves woman for the sake of the vulva; what woman loves in man is
the husband and the father. Comprehensively we may express the
matter by saying that woman has less eroticism and more sexuality.”
As a rule, remarks Erb, it is believed that the sexual impulse is
less intense in women than in men. This is true enough, he writes,
as regards youthful and virgin individuals, who have not yet come
into intimate contact with men, and in whom sexual desire and
sensibility have not yet been directly excited; later, however, when
sexual intercourse has been begun, a change usually takes place, and
the sexual needs become active in women also, and demand satisfaction.
It is well known that not a few women experience powerful
and uncontrolled sensual inclinations, just like those of men. On
the other hand, we must insist that quite a large number of women
possess the so-called naturae frigidae, and have no sensual inclination
to sexual intercourse, to which they are either indifferent, or in
some cases strongly averse, even regarding it with horror. This lack
of the sexual sense in women, is especially common in hysterical subjects,
and Erb reports that he has encountered quite a large number
of cases of this character. Whether in quite healthy women with
normal sexual impulse, complete abstinence from sexual intercourse,
too often compulsory but sometimes voluntarily undertaken, is harmful
in its consequences—this, says Erb, is a question very difficult
to answer. Many such unfortunate women have assured him that
they suffered severely in consequence of their enforced continence;
the majority of these became neurasthenic or hysterical. The complication
of purely physical influences with mental influences, increases
the difficulty of the problem. Neurologists have observed
women on whom continence was forced either during marriage or
after its dissolution, who thereupon fell into a state of severe nervous
exhaustion or nervous excitement, or suffered from threatening
or even actually developed psychoses. That sexual abstinence is
“absolutely harmless,” as moralists and many physicians would so
gladly believe, appears to Erb a quite unwarrantable assumption.
“In the processes of reproduction,” continues Erb in his discussion
of this subject, “woman is the principal sufferer. With inhuman
cruelty, nature has condemned woman to a far more difficult rôle
than man in the intercourse of the sexes and in the preservation of
the species; she is overpowered and forced by man, she is compelled
173to make the most severe sacrifices for the sake of the new
generation, first when it is germinating within her womb, and later
when it is entrusted to her care; and only too frequently she fails to
find the respect and protection due to her for the performance of
these functions! Compared with the sacrifices made by woman, the
temporary continence which is all that is demanded from man will
be admitted to be a small matter! It is fortunate that as a rule the
young woman who has never come into intimate contact with the
male, appears to be endowed by nature with a relatively weak sexual
impulse! This unequal and unjust distribution of the male and
female rôles on the part of nature may be regretted, but it cannot
be altered.”
The modern advocates of the rights of women, who demand that
in the sexual sphere also, woman should receive emancipation, oppose
the view that in the male the sexual impulse is stronger than in
the female, and also the view that whilst in the male the impulse is
simply one toward sexual congress, in the female the determining
motive to intercourse is furnished by the desire for motherhood.
They complain of “the perverse repression in woman of the sexual
impulse and its physiological gratification,” since sexual energy and
sexual sensibility are equal in intensity and identical in quality in the
female and in the male. Thus, Johanna Elberskirchen writes
(Die Sexualempfindung bei Weib und Mann—Sexual Sensation
in Woman and Man): “Body and soul, the whole being is subordinated
to a single powerful feeling and impulse, a single will flows
through nerves and blood, forcing and driving the female toward
the male with irresistible power; the yearning, the longing for the
relief of sexual tension, the craving for the euphoria and fleshly
delight that dominate the whole personality. And this elementary
sexual longing it is that clouds the woman’s brain, that drives her
into the man’s arms, that leads her to forget all the shame threatening
her and her child, that brings her to sexual union—not the
longing for a child, not the so-called impulse to motherhood.” And
again: “Woman yearns for love, all her love-organs cry out for
love, soul and body * * *. We do not long only for the rude
sexual act. We spiritualise it—at least some of us do so; at any
rate we individualize it. It is one particular man whom we desire,
he alone can still our longing, our bodily and mental hunger for
love. He satisfies us with all his love-affinities.” Naturally, also, the
consequence is deduced, “a free course must be given to sexual
sensation in women, and to the satisfaction of sexual desire, within
physiological limits, within the bounds of physiological necessity.”
Löwenfeld asserts that in the life of woman the sexual functions
play a comparatively much greater part than in the life of man,
174woman’s thoughts and feelings are, that is to say, much more powerfully
influenced by sexual matters than those of men; but none the
less he is of opinion that in the normal woman the desire for sexual
satisfaction is on the average less keen than in the normal man. Distinctly
greater in woman is the erotic element only, the need to love
and to be loved after an ideal manner, which is excited by the reproductive
glands just as much as is the simple sensual desire. Very
frequently, manifestations of this ideal need are erroneously attributed
to the sensual impulse, yet this latter may be entirely absent
in cases in which the erotic element is strongly developed. According
to Löwenfeld, the sexual impulse is altogether wanting in young
girls before the time of puberty, and in elderly women (in the case
of the latter we consider this assertion most questionable); this lack
of the sexual impulse persists in girls for an indeterminate time even
after puberty, as long as they remain free from all experience of
sexual stimulation. In this respect they offer a notable contrast to
males of the same age. In normal girls, according to the same author,
erotic dreams and similar occurrences are entirely wanting, and
specific sexual sensations therefore remain absolutely unknown to
them; hence it follows that the sexual impulse cannot, properly speaking,
arise in such individuals, and in so far as they experience any
desire for sexual intercourse it can only take the form of a craving
for some enjoyment, the nature of which is entirely unknown. The
absolute lack of the sexual impulse (complete frigidity) persists,
according to Löwenfeld, in a not inconsiderable proportion of women
even after their introduction to sexual intercourse—Effertz estimates
that such complete frigidity is permanent in 10 per cent. of all
women—and in a still greater proportion of women the sensual
impulse never exceeds a certain minimal intensity (partial frigidity).
It is probable that in the higher classes of society, inherited predisposition,
education, and perhaps also higher intelligence, combine
to diminish the intensity of the sexual impulse. In contrast with
these women of frigid temperament, however, we meet with women,
certainly in very limited numbers, whose sexual passions are extremely
powerful, and whose needs no man can satisfy.
Hegar, who considers that the sexual impulse in women is seldom
very powerful, draws the following conclusions in respect of the
influence of sexual gratification, on the one hand, or of continence,
on the other, on the duration of life and on physical and mental
health: “As far as comparisons between married women and women
vowed to celibacy (nuns and members of other celibate religious
orders) justify any conclusion, sexual activity and inactivity, respectively,
would appear to have little influence on the duration of
life. Comparisons between married and single women show,
175indeed, that the gratification of the sexual impulse and the processes
of reproduction are distinctly injurious when experienced before the
attainment of complete sexual maturity. In married women up to
the age of thirty, in some countries even up to the age of forty, the
mortality is greater than in unmarried women. The notably smaller
mortality of married women, as compared with unmarried, after the
age of forty, is usually explained as the result of the complete fulfilment
of the genital functions. It may, however, find a truer
explanation in the selection effected by marriage, especially when
we take into consideration that from the women thus selected the
weaker individuals have been previously weeded out by the processes
of reproduction:
“The lesser mortality of married men from the age of twenty
upwards is to be explained by the selection of the fit which occurs
in marriage, by the smaller proportion of marriages among men
engaged in hazardous occupations, and by the deterioration in the
quality of the unmarried which results from emigration. Still the
directly favorable influence of marriage is undeniable, and, no doubt,
the ethical factors of this institution have a beneficial effect, whereas
the gratification of the sexual impulse hardly enters into the account.
“Suicide is certainly very little dependent upon repression of the
sexual impulse, since all the motives arising out of the affairs of
love play together but a small part among the causes of suicide.
“The beneficial influence of marriage in the prevention of insanity
is in part apparent merely, since, in the selection exercised by marriage,
those predisposed to mental disorder, and those in whom such
disorder has already manifested itself, are, for the most part, already
excluded. Still, as regards the male sex at any rate, the beneficial
influence of marriage is undeniable, and consists principally in the
favorable ethical factors of this state. In women, on the other
hand, the advantage of marriage is doubtful, since the nerve centres
and the nervous system as a whole are strongly affected by the processes
of reproduction.
“Satyriasis, nymphomania, and hysteria are in no way dependent
upon the repression of the sexual impulse.
“Criminality in the married is comparatively less common than
in the unmarried. In criminal assaults on young persons, repressed
sexual impulse plays a part.
“Chlorosis is not in any way dependent on repression of the
sexual impulse. A disease apparently analogous to chlorosis, occurring
in unmarried women from twenty to thirty years of age, is
dependent rather on mental causes, and is relieved by other
means than marriage, especially by suitable occupation. Marriage
and gestation are distinctly injurious in cases of true chlorosis.
176“The satisfaction of the sexual impulse, and still more gestation,
favor in women the origin and growth of tumors, give rise
often to mechanical disturbances, and open the way for the invasion
of toxic pathogenic germs.
“Osteomalacia occurs only in parous women.”
Moll divides the sexual impulse into two components: The impulse
toward intimate contact (in a sense both physical and mental) with
a person of the opposite sex, which he calls the contrectation-impulse
(Kontrektationstrieb); and the impulse to bring about a change in
the genital organs, which he calls the detumescence-impulse
(Detumeszenztrieb). The former impulse induces intimate physical
and mental contact between the two persons concerned, the latter
impulse induces the local processes of copulation. In women, detumescence
results from the passing off of local swelling and the release
of nervous tension in the genital organs, with the discharge of indifferent
glandular secretions, notably the secretion of Bartholin’s
glands, and perhaps also the secretion of the uterine glands. The
intensity of the detumescence-impulse in women varies greatly in
different individuals, these variations being more extensive than
those occurring in the male. In some women the impulse toward
intimate contact, the contrectation-impulse, is normal, though the
detumescence-impulse is wholly wanting (vide Dyspareunia).
Runge defines the sexual impulse as the impulse which brings the
sexes together. This impulse is subservient to an instinct, namely
the instinct of reproduction; that is to say, the sexual impulse induces
the individual to perform actions which subserve the purpose
of reproduction without the agent’s being directly or chiefly concerned
with this purpose.
The sexual impulse, as sensation, perception, and impulse, is,
according to von Krafft-Ebing, a function of the cerebral cortex;
a centre for the sexual sense has not as yet, however, been localized.
The close relations which obtain between the sexual life and the
sense of smell lead to the supposition that the sexual and the olfactory
spheres of the cerebral cortex are in close proximity one with
the other. The development of the sexual life has its beginnings
in the organic sensations of the developing reproductive glands.
A mutual dependence now arises between the cerebral cortex as
place of origin of sensations and perceptions, and the organs of
generation. By anatomico-physiological processes these now give
rise to sexual perceptions, representations, and impulses. The cerebral
cortex, by apperceived or reproduced sensuous perceptions,
influences the organs of generation. This influence is effected by
the intermediation of the centres of vascular innervation and ejaculation,
which are situated in the lumbar enlargement of the spinal
177cord, and are certainly in close proximity one with the other. Both
are reflex centres.
The psycho-physiological process embraced in the conception of
the sexual impulse is according to von Krafft-Ebing constituted in
the following manner:
I. Of the central or peripherally aroused perceptions.
II. Of the pleasurable sensations associated with these.
Hence arises the impulse to sexual satisfaction (libido sexualis).
This impulse becomes stronger in proportion as cerebral excitement,
consequent on appropriate perceptions and the working of the imagination,
strengthens the intensity of these pleasurable sensations. If
the conditions are favorable to the performance of the sexual act by
means of which satisfaction is attained, the continually increasing
impulse finds expression in action; in other circumstances, inhibitory
perceptions intervene, sexual excitement diminishes, the activity of
the centre for erection is inhibited, and the sexual act itself is prevented.
In the case of civilized humanity the ready action of such
perceptions for the inhibition of the sexual impulse is necessary
and decisive. On the strength of the impulsive perceptions the constitution
and various organic processes have an important influence;
on the strength of the inhibitory perceptions, education and the
cultivation of self-control are powerfully operative.
In addition to mental influences, all forms of local irritation of
the sensory nerves of the female genital organs and adjacent parts,
by internal processes or external friction, serve to increase the
strength of the sexual impulse. Among internal processes which
stimulate the erectile centre by centripetal impulses must be included,
the stimulus of the enlarged graafian follicle, stasis in various
vascular areas of the genital organs in consequence of a sedentary
mode of life, abdominal plethora from excessive consumption of
food and stimulating drinks, and habitual constipation. External
friction may be in the form of intentional manipulation, but it may
be due to certain bodily attitudes or to the arrangement of the
clothing.
In normally constituted individuals, the sexual impulse is by no
means constant in its intensity. Apart from the temporary indifference
resulting from sexual gratification, and apart from the decline
in the impulse that occurs after prolonged continence, ensuing
after a certain reactionary intensity of desire has been happily overcome,
the mode of life has a very great influence. The town-dweller,
who is continually reminded of sexual matters, and continually
solicited to sexual intercourse, is in any case more subject than the
countryman to sexual excitement. A sedentary and sheltered mode
of life, a chiefly animal diet, the free use of alcohol and of spices,
178and the like, have a stimulating action on the sexual life. In the
female, the sexual impulse is stronger just after menstruation. In
neuropathic women this increase of excitement may occur to a
pathological degree. Not infrequently also in the climacteric period,
women are subject to sexual excitement due to pruritus, especially in
those neuropathically predisposed. Magnan reports the case of a
lady who was subject to matutinal accesses of intense erethismus
genitalis. The same author writes of a young lady who since puberty
had been subject to continually increasing sexual impulse,
which she gratified by masturbation. Gradually it came to pass
that the sight of a good-looking man produced violent sexual excitement,
and on these occasions, since she felt herself unable to
answer for her own conduct, she used to lock herself up in her bedroom
till the storm had passed away. Ultimately she surrendered
herself to any available man in order to obtain rest from her torturing
desires, but neither intercourse nor onanism gave her relief,
so that she was finally sent to an asylum.
As regards pathological increase of the sexual impulse, hyperæsthesia
sexualis, the constitution of the individual is, according to
von Krafft-Ebing (Psychopathia Sexualis), of great importance. He
writes: “With a neuropathic constitution, a pathological increase
of sexual desire is often associated, and such individuals bear for
the greater part of their life the heavy burden of this constitutionally
anomalous sexual impulse. The intensity of the sexual
impulse may be such as to amount to an organic compulsion, and
the freedom of the will may thus be seriously imperilled. Non-satisfaction
of this desire may induce a true sexual heat (like that
of lower animals), or a mental state characterized by sensations
of anxiety, in which the individual yields to the impulse, and his
responsibility for his action is most questionable. Should the person
so affected not give way to his desire, he runs the danger, by this
enforced abstinence, of injuring his nervous system by the induction
of neurasthenia, or of seriously aggravating neurasthenia that already
exists.
“Excessive sexual desire may arise either from peripheral or from
central causes. The former variety is less common. Such cases as
do occur, may arise from pruritus of the genitals, from eczema, or
from substances which by their remote local action stimulate sexual
desire, such for instance as cantharides.
“Sexual excitement of central origin is common in those suffering
from congenital neuropathic predisposition, in hysterical subjects,
and in states of mental exaltation. In such cases, when the cerebral
cortex, including the psychosexual centre, is in a state of hyperæsthesia
(abnormal excitability of the imagination, facilitated association
179of ideas), not only optical and tactile sensations, but also
auditory and olfactory impressions, will arouse lascivious perceptions.
“Sexual hyperæsthesia may be continuous, with exacerbations,
or intermittent, and even periodic. In the last case, according to
von Krafft-Ebing, it is either an independent cerebral neurosis, or
else a partial manifestation of a general condition of mental excitement
(mania, dementia paralytica, dementia senilis, etc.).”
Erotogenic zones, the stimulation of which leads to an increase
in the intensity of the sexual impulse and of sexual sensibility, are
in woman first of all and principally the clitoris, which indeed is
said to be the only zone of this nature in the virgin state (an
opinion held by von Krafft-Ebing and others, but certainly most
improbable); next to this comes the whole of the external genitals,
and especially the parts covered with hair; also the vagina by friction
and inter coitum; finally the nipple and its areola when stimulated
by titillation—an increase of the excitability of this region appears
to result from suckling.
According to Hensen, the direct stimulation of the sexual impulse
proceeds by way of the dorsal nerve of the (penis or) clitoris; he
assumes, however, that certain states of the reproductive glands are
able to induce an increase in the irritability of the centres connected
with the aforesaid nerves. In women it certainly appears
that particular states of the ovary have a stimulating or inhibiting
influence respectively on sexual excitement, so that we might ascribe
to the ovaries the rôle of a regulator of the sexual impulse. The
processes that occur in the ovary at the time of the ripening and
rupture of the graafian follicle, and the resulting tension of the follicular
wall, induce by stimulation of the ovarian nerves an increased
sensibility of the central zones, and produce in a menstruating female
a condition of increased sexual excitability, so that slight stimuli will
give rise to a powerful orgasm more readily than would otherwise
be the case, when the reflex irritability of the centre is less pronounced
and the sexual impulse is consequently less intense. Still
more than during these ordinary menstrual processes may this
stimulation be effective at the time of the menarche, when the
changes in the ovary occur for the first time and with the greatest
intensity, so that at this time the individual may be especially susceptible
to sexual stimulation.
At such times of sexual excitement, very slight external peripheral
stimuli, in the form either of tactile stimulation of the sensory
nerves of the skin and the external genital organs, or of stimulation
of the imaginative and perceptive faculties of the brain, suffice
to induce a powerful increase of the sexual impulse; whereas at
180other times, at which no particular sexual excitement exists, much
stronger stimuli are needed to produce such an effect. Thus the
sexual impulse in women is more readily and more powerfully increased
in proportion as the central organ is in a condition of temporarily
enhanced excitability in consequence of the condition of
the ovaries.
The gratification of this impulse, the act of copulation, produces
the specific sensation of sexual pleasure; in the female this is
effected chiefly by friction of the glans clitoridis, the organ when
erect projecting downwards at a right angle, and pressing upon
the intromitted penis—the friction of the glans produces powerful
mechanical stimulation of the numerous plexuses of sensory nerve
fibres, which terminate in the genital corpuscles of Krause. In
woman, then, we find in the ovary the place of origin and the means
of regulation of the sexual impulse, and in the clitoris we find the
seat of the specific sensation of sexual pleasure.
In the poorer classes of society, an increase of the sexual impulse
occurs in women chiefly in consequence of bad example and of unfavorable
domestic conditions, such as lead to persons of opposite
sexes sleeping in the same bed, and also in consequence of the
abuse of alcohol. In the well-to-do classes, it is the perusal of
modern equivocal romances, visits to theatres, balls, and evening
parties, and, speaking generally, idleness combined with luxurious
living, that serve to stimulate the sexual impulse in woman.
A certain dependence of the sexual impulse upon seasonal variations
appears to exist also in the human species. At any rate in
certain months of the year, a definite increase in the number of
conceptions continues to recur, which indicates that during these
months a larger number of sexually mature individuals is engaged
in the discharge of sexual functions. Rosenstadt regards this as the
manifestation of a “physiological custom,” immanent in the physical
constitution of civilized man, and inherited by him from his animal
ancestors. He explains it in the following terms: “Primitive man
inherited from his mammalian forefathers the peculiarity of reproducing
his kind only during a certain definite period, the period
of heat or rut. After humanity had entered upon this period, copulation
was effected en masse, as was easy in view of the primitive
community of sexual intercourse before the origin of marriage. In
the course of his progress toward civilization, however, man began
to reproduce his kind indifferently throughout the entire year; but
the original “physiological custom,” in accordance with which
reproduction occurred at definite seasons only, did not disappear,
and persists, indeed, to a certain extent even to the present day as a
survival of earlier mammalian life, and manifests itself in the annual
recurrence in certain months of an increase in the number of conceptions.
181The analogy in structure and function between the genital
organs of the human species and those of other mammals (the
female anthropoid apes do not merely exhibit from time to time a
period of heat, but are subject to a more or less regular menstruation),
which for the most part reproduce their kind only at certain
definite periods, leads to the conclusion that in the human species
also the sexual impulse may originally have awakened only at a
particular season of the year, and that the persistence of this physiological
custom in man, in spite of the fact that sexual intercourse
occurs all through the year, and notwithstanding that the conditions
necessary to awaken the sexual impulse are actually perennial, must
be ascribed to inheritance.”
This view, which is maintained also by other gynecologists, finds
support in Kulischer’s assumption, based upon ethnological investigations,
according to which coupling in primitive man took place
only at certain seasons, namely, at spring and at harvest-time. In
support of this view, which was held also by von Hellwald, Kulischer
refers to a number of actual and symbolical practices among different
races, which make the assumption extremely probable.
Sexual desire in women, the sexual impulse, outlasts the proper
sexual life, and manifests itself even after the cessation of menstruation,
when the possibility of conception has passed away; it appears,
therefore, to have no necessary connection with the function of
ovulation.
This is indicated by the always respectable number of women who
enter upon marriage even after the climacteric age. Thus the percentage
of brides who were more than 45 years of age was: In
Prussia, 2.58 per cent.; in England, 1.38 per cent.; in Sweden, 1.53
per cent.; in Ireland, 0.31 per cent. Of quite peculiar interest are
the figures relating to elderly women who marry men considerably
younger than themselves. Thus we learn from the tables of Routh
that in the space of 10 years in Ireland:
| Women between the ages of 46 and 55 years married |
|
| |
Men below the age of 17 in |
1 instance. |
| |
Men between the ages of 17 and 25 in |
35 instances. |
| |
Men between the ages of 26 and 35 in |
145 instances. |
| |
Men between the ages of 36 and 45 in |
227 instances. |
| |
| And women of ages greater than 55 years married |
|
| |
Men below the age of 17 in |
1 instance. |
| |
Men between the ages of 17 and 25 in |
3 instances. |
| |
Men between the ages of 26 and 35 in |
12 instances. |
| |
Men between the ages of 36 and 45 in |
15 instances. |
| |
Men between the ages of 46 and 55 in |
52 instances. |
In England during the year 1855 the age of the bride exceeded the
climacteric age in 778 instances. The brides were:
| From 46 to 50 years of age in |
135 instances. |
| From 51 to 55 years of age in |
219 instances. |
| 182From 56 to 60 years of age in |
89 instances. |
| From 61 to 65 years of age in |
22 instances. |
| From 66 to 70 years of age in |
7 instances. |
| From 71 to 75 years of age in |
3 instances. |
| From 76 to 80 years of age in |
3 instances. |
In Bohemia in the year 1872 the oldest bride numbered no less
than—86 years.
Börner reports cases in which the sexual impulse remained in full
activity after the change of life, and in some cases was greatly increased
in intensity—these latter individuals being in a condition
of real torment, which induced them to masturbate to obtain relief.
The sexual impulse may be present in cases in which the ovaries
are entirely wanting. Thus, Hauff reports the case of a young girl
who had no ovaries, but was nevertheless excessively addicted to
masturbation. Gläveke speaks of a puella publica in whom the
uterus and the ovaries were entirely absent, but who asserted that
she experienced during coitus active sexual sensation. Both
Kussmaul and Puech report similar experiences in cases of absence
or arrested development of the uterus.
As regards the effect on the sexual impulse of the operation of
oöphorectomy, most authors state that no change occurs; still, there
remain many who express the opposite opinion. From the collective
summary of cases bearing on this question made by Gläveke,
it appears that after extirpation of the ovaries the sexual impulse
remains unchanged in the great majority of cases, or at most is but
slightly diminished in intensity. Hegar states that he has often
witnessed a diminution of the sexual impulse after oöphorectomy,
but that this decline is by no means constant, indeed he states that
one of his patients assured him that in her case no decline in the
intensity of the sexual impulse had followed the operation. Similarly
variable reports were the experience of Schmalfuss. In one case
he found there was but little sexual inclination; in one case, disinclination;
in one case disinclination at first, followed by a return
of inclination. Bruntzel reports that in four patients subjected to
oöphorectomy, in two cases the sexual impulse persisted, but in the
remaining two it was extinguished. Köberle is of opinion that
sexual inclination diminishes as a result of this operation. Peaslee,
on the contrary, asserts that the patients remain striking examples
of womanhood, in whom all the qualities peculiar to their sex are
preserved. Péan observed as a rule no difference in the sexual
impulse to result from this operation, but he considers that the
patients are apt to describe in exaggerated terms the amount of
sexual feeling that remains to them. In one case, Spencer Wells
observed after oöphorectomy an increase in sexual excitability;
183Tissier had the same experience, and this author believes that in
these cases the sexual impulse is generally preserved. On the other
hand, Bailly observed a case, in which both ovaries were removed
on account of new growths, where the sexual impulse at first became
excessive, and then completely disappeared. Anger and
Goodell speak in the same sense.
I am myself acquainted with a woman twenty-six years of age
who in girlhood underwent oöphorectomy on account of extremely
severe nervous troubles associated with menstruation; she had not
experienced in consequence any loss of the sexual impulse; she
married a man belonging to the upper strata of society, and consulted
me four years later to learn if she could by any means be
rendered capable of bearing a child. Two other cases have come
within my personal experience in which young women married after
extirpation of the ovaries, and in whom sexual desire and sexual
sensation were all that could be wished.
In twenty-seven women who had undergone the operation of
oöphorectomy, Gläveke made inquiries regarding the three following
points: First, whether the sexual impulse had been affected by the
operation; secondly, whether during intercourse sexual pleasure was
experienced to the same degree as formerly; and thirdly, whether
during intercourse any kind of difference was observed as compared
with pre-operative experience. He obtained the following results:
| Sexual inclination was |
|
| |
Unaffected in 6 cases |
22 per cent. |
| |
Diminished in 10 cases |
37 per cent. |
| |
Extinguished in 11 cases |
41 per cent. |
| Sexual pleasure during coitus was |
|
| |
Unaffected in 8 cases |
31 per cent. |
| |
Diminished in 10 cases |
38 per cent. |
| |
Extinguished in 8 cases |
31 per cent. |
In a considerable number of cases the sexual impulse was thus
found by Gläveke, not indeed to be entirely extinguished, but still
notably diminished. In another set of cases, the sexual impulse
was entirely extinguished, but only in one case was there actual
aversion to coitus. The women readily permitted intercourse when
their husbands desired it, but remained themselves quite indifferent.
The greater number of these women stated that the specific sensation
of pleasure during coitus was markedly weakened, but not entirely
lost; in a small proportion, this sensation was completely extinguished.
In the case of seven women who complained that coitus
was very painful, Gläveke found that the calibre of the vagina was
much diminished. In these cases, the sensation of pleasure during
coitus was either greatly diminished or completely extinguished.
The women permitted intercourse very unwillingly, their unwillingness
184arising, not from any actual aversion, but because they dreaded
the pain which coitus produced. An extremely hysterical woman,
affected with severe prolapse of the uterus, stated that every attempt
at intercourse was frustrated by violent hysterical convulsions.
The sexual impulse appears always to suffer first and most severely,
and only after this is the sensation of pleasure during coitus affected.
In a few women only, according to the experience of this
author, was the sexual impulse quite unaffected by the removal of
the ovaries.
Amputation of the clitoris appears notably to diminish both the
sexual impulse and the sensation of sexual pleasure, but the results
of clitoridectomy for the cure of masturbation are by no means always
favorable. In the women of the Russian sect of the Skopstki,
the clitoris, the nymphæ, and a part of the labia majora are removed,
in order to destroy sexual desire. According to von Krafft-Ebing it
is probable that in the virgin the clitoris is the only erotogenic zone,
that is to say, that only by the stimulation of the clitoris can erection,
the orgasm, and the sensation of ejaculation be induced. It
is probable that the vagina becomes erotogenic only as a result of
coitus; thenceforward, however, the erotogenic significance of the
clitoris is notably lessened, and in multiparæ may entirely disappear.
Nymphomania, Anæsthesia and Psychopathia Sexualis.
The sexual impulse in women is subject to morbid changes, both
in the way of increase and of diminution, exhibiting abnormal violent
increase (nymphomania), or declining to the state of complete
frigidity and sexual indifference, or, finally, manifesting itself
in some perverse manner (psychopathia sexualis).
Psychopathically increased sexual impulse in woman is known
as nymphomania or uteromania. In such women there is a dominant
state of psychical hyperæthesia, principally in the genital sphere.
The most indifferent perceptions give rise to erotic sensations and
to lascivious impulses. All sensory perceptions obtain a sexual content,
and induce stimulation of the cerebral cortex. All sensation and
all activity in such unhappy beings ultimately concentrates itself in
the act of copulation, or in some other form of sexual gratification,
the greatest perversities of sexual practice frequently arising,
masturbation, tribadism, and, for the most part, prostitution, even
in the case of married women.
The nymphomaniacal woman, says von Krafft-Ebing, endeavors
to allure men by means of exposure of the genital organs or indecent
gestures; the sight of man produces intense sexual excitement, which
is gratified by masturbation or by stimulatory movements of the
pelvis. According to this author, nymphomania is not very infrequent
185at the climacteric period; it may even occur in old age. Abstinence
in association with simultaneous excitement of the sexual
sphere by mental or by peripheral stimuli (pruritus pudendi, oxyuris,
etc.), may induce these states, probably, however, only in those
hereditarily predisposed.
The history of antiquity contains records of the corrupt practices
of nymphomaniacal empresses. Thus, Messalina furnishes a well-known
historical example of the abnormal violence of a pathologically
intensified sexual impulse in woman. She was given the agnomen
of invicta, having received the embraces of fourteen athletes.
Pliny says of her, die ac nocte superavit quinto et vicessimo concubitu;
and Juvenal writes of her the verses,
... tamen ultima cellam
Clausit, adhuc ardens rigidæ tintigine vulvæ
Et resupina jacens multorum absorbuit ictus
Et lassata viris, necdum satiata, recessit.
In corrupt Rome, Messalina was not the only woman necdum
satiata, ever insatiable; we need only refer to the orgies of an Aggripina,
a Livia, a Mallonia, or a Poppæa; and Seneca hurls against
the women of his day the reproach, adeo perversum commentæ genus
impudicitiæ viros ineunt. And of Cleopatra, the beautiful Egyptian
queen, Marcus Antonius writes in a letter to his physician, Soranus,
that she had such violent sexual desire as to lead to her having
connection in a brothel with 106 men.
Through the report of Herodotus it is well known that the pyramid
of Cheops was built by the numerous lovers of the daughter of
this king, who raised this enormous monument in recognition of
the innumerable times she had yielded herself to their desires. On
record also are the sexual excesses of the Roman ladies at the festival
of Saturn, the festival of the Bona Dea, and the festival of Priapus;
indeed, many of these women allowed themselves to be debauched
in the temples (Ploss and Bartels).
But returning to the present day, both gynecologists and alienists
record numerous cases of great pathological increase in the intensity
of the sexual impulse in women. According to Lombroso,
such continued ardency of sexual desire occurs chiefly in women
with an inherited tendency to crime and to prostitution, whose
natures exhibit a commingling of lasciviousness with barbarism.
He gives examples of such women, one of whom surrendered herself
to her husband’s laborers; another had as her lovers all the
desperadoes of Texas; a third had intercourse with all the herdsmen
of her village; a fourth, though her husband occupied a good
social position, led the life of a prostitute; a fifth, a cultured and
186intelligent woman, entertained a common bricklayer, and wrote
to him letters full of shameless declarations of her sexual passion;
further he writes of a series of criminals, in whom, indeed, increased
sexual desire is a common phenomenon; one of these, a thief, experienced
sexual excitement at a mere glance at a good-looking man;
a murderess, in whom lascivious feeling induced masturbation whenever
she saw a man, and who made experiments in sexual intercourse
with dogs; another, who often took to bed with her, in addition
to her son, three or four men selected at random from the
streets; and many others. Jolly reports the case of a widow, a
celebrated lionne of the demi-monde, who kept in her desk, side by
side with devotional literature, a number of lascivious books and
preparations of cantharides, and entertained quite a number of
powerfully-built lovers drawn from the lowest canaille.
In hysterical women the sexual impulse is frequently excessive,
and may increase to such a degree as to produce hallucinations of
coitus; sometimes, on the other hand, the impulse is extinguished,
or psychopathically metamorphosed, passing in a most paradoxical
manner from sexual frigidity to lascivious reflections and continuous
occupation with sexual affairs; not uncommon in such women are
false accusations of indecent assaults of which they assert themselves
the victims.
Lombroso gives several examples of the increase of the sexual
impulse in hysterical women: “A hysterical girl visited a physician,
and said to him: ‘I am still a virgin, take me;’ she submitted him
to the utmost extremity of provocation, and asserted afterward that
she had been violated. Another hysterical subject, a rich young
lady, met a workman in the street, offered herself to him, was accepted,
and when she returned home related the affair with laughter.
A third sought men from the street in order to find one suffering
from syphilis, her object being to infect her own husband with the
disease.”
According to the observations of Schüle, young married, hysterical
women not infrequently run away with a waiter during the
honeymoon journey. This author also points out that in women
moral insanity is especially apt to manifest itself during the first
years of married life. Many advocate a far-reaching libertinism,
and threaten to enter a brothel. In these forms we observe, in
addition to ill-temper and malignity, especially obscenity and
tribadism.
Such a case, observed by Giraud and quoted by von Krafft-Ebing,
is the following: Marianne L., of Bordeaux, during the night,
while her master was sleeping soundly under the influence of narcotics
she had administered, was in the habit of giving up her
187master’s children to her lover for his sexual gratification, and made
them witnesses of the most immoral scenes. It appeared that L.
was hysterical, suffering from hemianæsthesia and convulsive
seizures, and that before her illness she had been a sensible and
trustworthy individual. After the illness, however, she prostituted
herself in the most shameless manner and completely lost her moral
sense.
Galen relates of his own mother that she suffered from nymphomania,
and that in the attacks she bit her female slaves like a wild
animal.
As a negative aspect of the sexual impulse in woman we must
regard the absence of the impulse, or anæsthesia sexualis, and also
the deficiency of the sensation of pleasure during the act of copulation,
or dyspareunia.
Of dyspareunia we shall speak more at length later, in connection
with the pathology of copulation. As regards the entire lack of
the sexual impulse, however, in women whose genital organs are
normally developed and normal in the performance of their functions,
and whose cerebral condition is also normal, we must consider such
lack an extremely rare condition, if indeed it ever occurs. It is
only in cases in which the female genital organs are wanting,
wholly or to a considerable extent, or in which there are important
cerebral disturbances or states of mental degeneration, that the
sexual impulse is wanting.
Normally, in the young, sexually unspoiled girl, the sexual instinct[34]
slumbers in the cerebral cortex, but becomes active, as sensation,
perception, and impulse, as soon as the cerebral centre has
been aroused by mental impressions or by physical peripheral stimulation
of the genital organs and their environment. Among stimuli
of the latter class must be reckoned the menstrual stimulus, set
on foot by the developmental processes of puberty. These stimuli
arouse in the cerebral cortex sensations and perceptions which, rising
to specific sexual feelings, produce an impulse to increase the intensity
of these feelings by purposive action; thus is awakened the
sexual impulse, the strength of which is extremely variable.
Only when the cerebral cortex, as the place of origin of sensations
188and perceptions, fails to perform its functions in the manner
just described, or when the anatomico-physiological processes in
the genital organs which normally act as peripheral stimuli fail to
occur, or when there is a failure in the conducting tracts, are sexual
perceptions and impulses lacking. Such anomalies may be congenital.
A milder form is that, likewise congenital, in which a
woman has a sexually “cold nature;” in these cases the sexual impulse
is not completely wanting, but it is so slight in intensity that
it can be awakened only by very powerful stimuli, and in her normal
state the woman so affected is quite free from any wish for sexual
gratification.
Such congenital subnormal intensity or entire lack of the sexual
impulse may be due to very various causes. According to von
Krafft-Ebing, these causes may be organic or functional, mental or
physical, and central or peripheral. The declining intensity of the
sexual impulse with the advance of years, and the temporary disappearance
of that impulse after the sexual act, are both physiological
occurrences. Education and mode of life have a marked influence
on the intensity of the vita sexualis. Strenuous mental activity,
earnest study, severe physical exertion, mental depression, and sexual
continence, notably diminish the excitability of the sexual impulse.
At first, indeed, abstinence leads to an increase in the intensity of
the impulse, but sooner or later the functional activity of the organs
of generation declines, and therewith also the intensity of the sexual
impulse. As peripheral causes of diminution or disappearance of the
sexual impulse, von Krafft-Ebing mentions oöphorectomy, degeneration
of the reproductive glands, marasmus, sexual excess, whether in
the form of coitus or of masturbation, and alcoholism. In like manner
is to be interpreted the disappearance of the sexual impulse in
general disorders of nutrition (diabetes, morphinism, etc.).
A decline in the intensity of the sexual impulse in consequence of
degeneration of the conducting tracts, is found, according to von
Krafft-Ebing, in diseases of the brain and the spinal cord. Central
affection of the sexual impulse may be due to organic disease of the
cerebral cortex (dementia paralytica, general paralysis of the insane,
in the later stages), or it may be due to functional disorder, such
as hysteria, or to mental diseases (melancholia or hypochondriasis).
Finally, in some instances, the sexual impulse in women manifests
itself, not in the normal manner with copulation with the male as its
goal, but in a form demanding some abnormal kind of gratification
(psychopathia sexualis), whether it be because sexual intercourse
with the male affords the woman no enjoyment, or simply because
no opportunity exists for such intercourse.
Masturbation is very frequent; the habit having been acquired
189from bad example by the girl during the menarche, it is sometimes
continued by the wife during married life. In these cases we often
find distinct changes in the genital organs, such as hypertrophy of
the clitoris, enlargement and bluish discoloration of the nymphæ,
retroversion of the uterus, tenderness and displacement of the ovaries,
considerable vaginal discharge, and sometimes menorrhagia.
Kussmaul draws attention to the connection between masturbation
and nymphomania, on the one hand, and imperfect development of
the uterus and the other genital organs, on the other. Campbell
records the case of a woman addicted to masturbation, who had
never menstruated, and who, in addition to imperfectly developed
genital organs, had a dermoid cyst of the ovary. In a young woman
who indulged in masturbation, Aran found that the uterus and its
annexa were imperfectly developed. Vaddington also describes a
case of abnormal sexual impulse which was associated with absence
of the uterus.
Troggler reports the case of a woman twenty years of age, who
had been six months married to a healthy, potent man, was herself
healthy and blooming, with a good family history, and had never
suffered from any severe illness. At the age of thirteen she had
learned to masturbate, effecting this by stimulation of the clitoris.
Now she found no gratification in coitus, so that she continued to
masturbate, and during coitus obtained satisfaction by manual friction
of the clitoris. Examination showed that the clitoris was strikingly
large, the vagina flaccid, and that there was some vaginal discharge;
in other respects the genital organs were normal.
Not infrequent, it may be in those whose mental condition is in
other respects fairly normal or it may be in psychopathic subjects,
is the existence of contrary sexual sensation, or sexual inversion, a
condition which has been described by Casper, Westphal, von
Krafft-Ebing, and Moll, and has indeed been well known since the
days of antiquity. In the case of a considerable number of notable
women, homosexual practices have been recorded. According to
the observations of Coffignon, in Paris the homosexual instinct,
when occurring in other women than prostitutes, is found chiefly
among the ladies of the aristocracy.
Of homosexually inclined women, some engage in the practice of
tribadism, familiar to the ancient world, and recorded by Martial in
a satire, in which sexual gratification is obtained by mutual friction
of the genital organs, or by penetration of one woman’s clitoris into
the vagina of the other; whilst some indulge in the amor lesbicus,
in which gratification is obtained lambendo linguâ genitalia, a very
ancient practice indeed, transported from Phœnicia to Greece (where
in especial it was indulged in by the women of Lesbos), and later
190from Syria to Italy, where it was widely diffused among the Romans
of the imperial age. Sappho, celebrated as the tenth muse, is supposed
to have been addicted to the practice of Lesbian love.
All such homosexual (female) individuals are, then, endowed with
the perverse instinct toward sexual connection with women instead of
with men. In such cases, the genitals are usually quite normal;
sometimes, however, the woman thus affected is markedly of a male
type, being called by von Krafft-Ebing a gynandrist, the affection
itself being termed gynandry; when the woman concerned not only
possesses a homosexual impulse, but also in other respects exhibits
tendencies properly characteristic of the male sex, she is called virago,
and the affection is termed viraginity.
I had under my care such a woman, belonging to the upper circles
of society, who had been married sixteen years before, had
lived a married life for six years (during which she remained barren),
and had then separated from her husband. She was of a
very masculine disposition, smoked, gamed, drank like a student,
and preferred to wear men’s clothing, and she bestowed her affections
on a female companion. Examination of the genital organs
disclosed no abnormality beyond a slight vaginal catarrh. Menstruation
was regular, and the general appearance showed no departure,
with the exception of a slight moustache that shaded the upper lip,
from that of a normal feminine beauty.
Mantegazza is of opinion that in the case of many unhappy marriages,
in which the source of the unhappiness is obscure, the trouble
is to be found in the homosexual inclination of the wife. Martineau
and Moll report that married women who are homosexually inclined,
indulge in sexual intercourse with other women behind their
husbands’ back. Duhousset, at a meeting of the Anthropological
Society at Paris in 1877, related the almost incredible case of a
married homosexual woman who, in intercourse with another
woman, transferred to the latter her husband’s semen, so as to
induce pregnancy.
Many writers on forensic medicine, Tardieu, Pfaff, Schauenstein,
Wald, and Mantegazza, for instance, have recorded that in numerous
circles of European society women practice masturbation and
tribadism (sodomy, so called) with dogs and monkeys; and Plutarch’s
statement is well known regarding Egyptian women and the
sacred goat, Mendes, that the women who were locked in with this
animal practiced sodomy therewith; and again it is asserted that
the serpents in the temple of Æsculapius and also in private houses
were employed in the practice of sodomy.
Von Maschka records a case which came before the courts a few
years ago in Prague, in which a woman forty-four years old confessed
191that “in consequence of the very ardent temperament she
possessed, she had, perhaps, as often as six times indulged herself
with her house dog, which jumped between her legs and licked her;
that she took the animal between her bare legs, stroked its belly
until its penis became erect; then, supporting herself on the back
of a chair, she pressed the animal against herself, introduced its
penis between her labia majora, and let it continue its movements
until its semen had been ejaculated.” Examination of the genital
organs of this woman disclosed no abnormality.
Schauenstein reports the case of a girl who carried out unchaste
practices with a little dog to an utterly immoderate extent, so that
after the lapse of some years she died in an asylum. In a case recorded
by Wald, a maid servant was observed in lewd practices with
a poodle; she supported herself on elbows and knees, while the dog
copulated with her from behind.
A woman about thirty years of age, who had lived with her husband
in sterile marriage for nine years, complained to me that she
had not for a long time had sexual intercourse, since during copulation
she not only experienced no sexual pleasure, but actually felt
a loathing to the act; on the other hand, she was subject to an uncontrollable
impulse to handle the genital organs of children, both
of the male and of the female sex, and this performance gave her
sexual gratification; during the menstrual period, this impulse overpowered
her will. Local examination in this patient showed that the
uterus was enlarged and retroflexed, and that there was anæsthesia
of the vagina.
Anjel reports the following case of periodic psychopathia sexualis,
associated with menstruation. A lady of quiet disposition, near the
climacteric. Serious congenital predisposition. During youth suffered
from attacks of minor epilepsy. Married, but childless. Several
years ago, after violent emotional disturbance, she had a
hystero-epileptic seizure, followed by post-epileptic mania lasting
several weeks. Thereafter, insomnia for several months. As a
sequel, continually recurrent menstrual insomnia, accompanied by an
impulse to embrace boys under ten years of age, to kiss them, and to
handle their genital organs. Impulse toward coitus, to close sexual
contact with a grown man, non-existent at this time. The patient
often speaks openly of her morbid impulse, and begs that she may
be supervised, as she feels unable to answer for her own conduct.
In the intervals, however, she carefully avoids all reference to the
matter, is strictly decent in her conduct, and in no way sexually
ardent.
Tribadism is frequently mentioned by the writers of classical
antiquity, especially by those of Greece, where the cult of naked
192beauty encouraged sexual excitement of this character. This form
of unchastity was common among the flute-playing girls of Greece,
and at the secret festivals of such associates Aphrodite Peribasia was
invoked. Lucian, in his dialogues of hetairai, depicts the intensely
passionate nature of these homosexual unions between girls. Lombroso
reproduces Juvenal’s description of such a love-feast. “When
the flute calls to the dance, the mænads, inflamed with wine and
beer, loosen their long tresses, they sigh languishingly and eagerly,
and an ardent desire draws them one to another, the desire and the
passion of the dance gives their voices an alluring sound; nothing
now can serve to bridle their unrestrained desires. Lacasella swings
her wreath, which she has won in the contest of lascivious gestures
and movements, but even she must give way before Medullina with
her ardent postures. About these games there is no trace of unreality,
and the most rigid Spartan, hardened from the very cradle,
even old Nestor himself, notwithstanding his hernia, could not fail
to be stimulated by such an inflammatory spectacle.”
In the present day, also, the practice of tribadism is more widely
diffused than people in general imagine. I have often encountered
instances of it in ladies of good position, who were past their first
youth, who would not or could not marry, and who undertook
extensive and long-enduring journeys with a female “companion,”
of similar age, or perhaps a little younger. Their erotic needs, which
could not be gratified in normal fashion, led to this sexual perversion—a
tendency observable especially in persons with neuropathic
predisposition, or with a liability to hysteria or to epilepsy.
Sometimes such girls, even before puberty, show an inclination to
wear boys’ clothes, to avoid all feminine manual occupations, and
to examine and to handle the genital organs of their playmates.
Even after puberty, such tribadists like to make a parade of masculine
attitudes, they have their hair cut short, wear clothes of a
masculine cut, smoke a great deal, and show in their conversation,
and still more in their letters, great exaltation of the passions. It
not infrequently happens that an elderly lady who has lived well in
her day, and from youth upward has had much intercourse with
men, comes at last to lament her worthlessness to men, and from
this proceeds to the idea of obtaining sexual enjoyment by means
of tribadism. The tribadistic union sometimes lasts for several
years, but in most cases the alliances are quickly and frequently
changed.
According to Taxil, tribadism is fairly common among the married
women of Paris, and in upper-class women is extremely prevalent.
This author describes with what industry and perseverance
many elderly tribadists endeavor to win for themselves and to seduce
193young girls, just as old women often work hard to gain money
for the enjoyment of the favored person.
In these unions, according to the descriptions of Lombroso, very
remarkable phenomena occur. A particular jargon arises with tender
designations for this or that bodily beauty; a violent jealousy
develops, and a newly united pair keep together as much as possible
for fear of losing one another’s affection; the “friends” tread
always in one another’s footsteps. This author rightly points out
that the very numerous romances describing relations of this kind
prove the diffusion of this vice in “high life.” Novels of this class
are referred to by Mantegazza in his book, “Woman as Criminal and
Prostitute.” He mentions: Diderot, “La Religieuse;” Balzac, “La
Fille aux Yeux d’Or;” Gautier, “Mademoiselle de Maupin;”
Feydeau, “Le Comtesse de Cholis;” Flaubert, “Salammbô;” Bélot,
“Mademoiselle Giraud ma Femme;” Willbraud, “Fridolins Heimliche
Ehe;” Graf Stadion, “Brick and Brack;” Sacher-Masoch,
“Venus im Pelz.” Zola, also, in “Nana” and “La Curée,” and
Butti in “L’Antona,” make some reference to this matter.
Sauval relates of the dissolute life at the court of the French
king, Francis I, that the women learned also to play the part of
men; a princess had a hermaphrodite maid-of-honor, and the court
and all Paris gossiped about the Lesbian-loving ladies, whose husbands
were delighted, since they were thus quite freed from jealousy,
and prized their wives above all on this account. Such a mode of
life was so pleasing to many ladies that they refused to marry, and
refused also to allow their “friends” to marry.
Tribadism is very common among prostitutes. According to
Parent-Duchatelet, tribadism begins only after prostitution has long
been practised, between the twenty-fifth and the thirtieth year of
life; generally there is a notable difference in age and also in beauty
between the two women forming a tribadistic alliance, and as a rule
the younger and prettier of the pair is the more passionately sensitive
and the more constant. Parent-Duchatelet endeavours to explain
the origin of tribadism by referring to the manner in which in
brothels and reformatories the women are closely packed together,
to the enforced abstinence from normal sexual intercourse (in
prisons and reformatories), to the loathing for men sometimes felt
by prostitutes, and to the opportunities for mutual observation of
the most intimate nudities. Even women who at first object to it
most vehemently, commonly give way to this vice after eighteen or
twenty months.
Among 103 prostitutes examined by Lombroso, he found tribadism
to be practiced by five. He considers the principal cause of tribadism
to be in the lascivious search for new and unnatural pleasures, and
194quotes in illustration the characteristic remark of Catharine II, herself
a tribadist, “Why did not nature endow us with a sixth sense?”
Female criminals who seduce others to the practice of tribadism
have usually themselves acquired the vice during a long term of
imprisonment—it is, in fact, the long-sentence criminals, women
with a congenital inclination toward crime, that incline also to unnatural
vice. The influence of environment is, according to Lombroso,
indicated by the fact that the most confirmed criminals, in
prisons for women, corrupt in this manner so many of the inmates
who are merely “criminaloids,” and corrupt even the wardresses.
Further, he is led to conclude, the confinement in close association
of so many extremely sensual and prostituted women, leads to the
origin of a kind of ferment of new lascivious desires, and causes an
increase of one form of degeneracy by means of another. Prostitutes
often see one another naked, sleep two or three together in
the same bed; similar things occur in boarding-schools. In asylums
also we may observe that the admission of a tribadist will result in
the infection of all the inmates with this vice.
According to Moll’s estimate, 25 per cent. of the prostitutes of
Berlin practice tribadism. According to the experience of this
author, in cases in which tribadists live in concubinage, one of them
is always a prostitute; the active and the passive rôle are always
played by the same respective members of the alliance; the active
member is called “papa” or “uncle,” is usually a prostitute, and,
like the man in the married state, possesses great comparative freedom
in sexual matters, whilst the passive member, the “mother,”
is not allowed to form any sexual relations outside the concubinage.
According to Ricardi, many frigid prostitutes practice with pleasure
clitoris-masturbation, cunnilictio, and, especially, sapphism, preferring
these perversions to the normal sexual act. Moreover,
among prostitutes and female criminals there is no lack of lovers
of martyrization, of flagellation, even to the drawing of blood, of
tyrannical treatment, and of the initiation of children into the
mysteries of sex.
[For a detailed account of Sadism and Masochism, see von
Krafft-Ebing’s “Psychopathia Sexualis.” These particular perversions,
common in men, are rare in women; hence but passing allusion
is made to them in the present work.]
Lombroso records on account of its rarity a case of masochism
observed by him in a woman thirty-five years of age, who liked being
whipped.
Moraglia reports a remarkable instance of sexual perversion in a
girl of eighteen, who preferred to coitus, masturbation associated
with the stimulating influence of the odor of male urine; this peculiar
form of irritability was so powerful as to drive the girl to masturbation
195in public urinals, notwithstanding the risk of arrest, which
indeed often occurred.
According to Carlier, there are four or five brothels in Paris
which are not infrequently visited by rich ladies in search of tribadistic
enjoyments, and ladies of “high life” assemble there for
communal orgies; it is noteworthy that prostitutes surrender themselves
for such purposes to these women who are outside their own
circle with great reluctance, and only for a very high fee.
Speaking generally, however, sexual perversion is rarer and
less intense in women than in men. This fact is explained by
Lombroso on the ground that the erotic element in women’s nature
is less active, and that women are less often affected by epilepsy,
the principal source of these anomalies. In cases in which the
genital organs are healthy we must, with Westphal, conclude, with
reference to contrary sexual sensation, that the abnormal sexual
feelings have a cortical origin.
From von Maschka’s elaborate account of unnatural offences, in
his Handbook of Forensic Medicine, we abstract the following passage
relating to the female sex: “Lascivious procedures liable
under certain circumstances to legal punishment may consist:
1. In handling or other manipulation of the genitals, without actual
intercourse. If the genital organs of a female have merely been
gently handled, without any more violent manipulations, we shall
not, as a rule, either in the case of children or of adults, find any
local changes as a result; contrariwise, if the handling has been
rough and brutal, if the fingers have been forcibly thrust within
the vulval cleft, or if the pudendum has been pulled and rent, we
may expect to find excoriations, redness, swelling, laceration of the
hymen, or even of the vagina and the perineum. 2. In licking the
female genitals (cunnilingere). An analogous process also effected
by members of the female sex, whether children or adults, is
irrumare, id est, penem in os arrigere; fellare, id est, vel labiis vel
lingua perfricandi atque exsugendi officium penis præstare. 3. In
introduction of the membrum virile into the rectum, either of children
or of adults, pæderasty.” That this form of sexual gratification
is not infrequently practiced upon women has been pointed out
especially by Parent-Duchatelet, and is asserted by von Maschka
from personal knowledge of cases in which it has occurred.
Tribadism and Lesbian love, unnatural vice practiced by two
individuals of the female sex, occur, according to von Maschka’s
description in the following manner: a.) By masturbation, either
one person gratifying the other by manipulation, or mutual masturbation.
In a case of this kind recorded by Tardieu, a wife still
young repeatedly, and by day as well as by night, introduced her
196finger deeply into the vagina or the rectum of her little girl, moving
it about there sometimes for as long as an hour. According to the
child’s account, the mother herself at these times was in a condition
of excitement, no doubt sexual, which she gratified in this
manner. In another case, several older girls engaged with their
own fingers and tongues in lascivious practices with the genital
organs of a little girl of seven. According to Krausold, among
female prisoners such “forbidden friendships” are extremely common,
formed for the purpose of mutual masturbation, and in connection
with which the bitterest jealousy and the most ardent love
are exhibited. b.) With the assistance of an enlarged clitoris,
with which one woman performs the sexual act by introducing the
organ within the vagina of another. In France in the nineteenth
century a woman is said to have lived whose genital organs were
so formed that, on the one hand, as a woman she played the passive
part in intercourse with men, and, on the other hand, was able to
give sexual gratification to women by assuming the active part of
the male. c.) By the employment of an artificial membrum virile.
This mode of obtaining satisfaction of sexual desire was known
already to the ancients, and such a priapus was by the Greeks termed
ὸλισθος. The fact that such articles are manufactured and sold,
affords sufficient proof that their use is not unknown in our own
day. Von Maschka describes such priapi as being made of india
rubber, of the size and shape of an erect penis, perforated longitudinally
and fitted at the lower end with a testicle-like attachment,
to be filled with warm water or milk, so that by squeezing it an
ejaculation can be counterfeited. This priapus is also so constructed
that it can be attached to the body by means of a girdle and can
thus be employed for the gratification of another individual.
We have already referred to sodomy, unnatural intercourse with
the lower animals. Von Maschka gives several instances of this,
which we have previously mentioned, and states also that some
years before, during his stay in Paris, a female was accustomed to
hold a secret exhibition, the entry to which cost ten francs, and at
which she had sexual intercourse with a bulldog trained for the
purpose.
According to Lombroso, even at the present day, the inmates of
licensed brothels frequently hold exhibitions, for admission to which
a fee is charged, of tribadistic couples in poses plastiques, and of
another prostitute in coitus caninus.
In his widely-celebrated work on Psychopathia Sexualis, von
Krafft-Ebing discusses these morbid sexual processes in women.
We select certain data from his exposition. Regarding the congenital
morbid phenomenon of the lack of sexual feeling in women,
197as contrasted with perversion of sexual feeling, and the sexual
impulse toward an individual of the same sex (antipathic sexual
feeling), von Krafft-Ebing writes: “The woman-loving woman
feels herself sexually to be a man, she rejoices in the exhibition of
courage, of masculine sentiments, since these characteristics make
the man desirable to the woman. The female urning,[35] therefore,
likes to have her hair cut short and her clothes of a masculine cut;
and one of her greatest pleasures is when opportunity offers to
appear in male attire. Her ideals are notable feminine personalities,
distinguished by spirituality and energy; in the theatre and in the
circus, it is only the female performers that attract her interest;
and in the same way, in collections of pictures and statues, it is
only the representations of women that awaken her æsthetic sense
and her sensibility.” Von Krafft-Ebing insists that in nearly all
cases of antipathic sexual feeling in which a family history was attainable,
that history was found to exhibit instances of neuroses, psychoses,
stigmata of degeneration, etc. In hysteria, according to
this author, the sexual life is especially often abnormal; in cases
with neuropathic inheritance, one may say always: “All possible
anomalies of the sexual functions occur in such cases, with the
utmost variety and the strangest commingling, based upon hereditary
degenerative processes, and accompanied by moral imbecility
in its most perverse manifestations. * * *. Frequently, in hysterical
subjects, the sexual life is morbidly excitable. This excitement
may be intermittent (? menstrual). Shameless prostitution
may result, even in married women. In cases of a milder type, the
sexual impulse is exhibited in the form of onanism, nude perambulations
about the room, wearing of male attire, etc. In cases of
hysterical mental disorder, the morbidly excited sexual life may
manifest itself in the form of maniacal jealousy, baseless complaints
against men of indecent assault, hallucinations of coitus, etc. Sometimes
there may be frigidity, with lack of sexual pleasure, commonly
due to genital anæsthesia.”
Incest in women, dependent upon psychopathic causes, is also
alluded to by von Krafft-Ebing; it occurs in those in whom a partial
imbecility that leaves the sense of modesty undeveloped is combined
with eroticism. Thus, a case reported by Schürmayer is mentioned,
in which a mother had, or attempted, intercourse with her son,
aged five and one-half years; and again a case reported by Lafarque,
in which a girl of seventeen laid her thirteen-year-old brother on
herself for the gratification conjunctionis membrorum, while simultaneously
198masturbating her brother; Magnan’s case, an unmarried
woman twenty-nine years of age, who could hardly resist the impulse
toward copulation with her nephews as long as they were quite
young; Legrand’s cases, in one of which a girl fifteen years of
age seduced her brother to the performance of all possible sexual
excesses on her body; another, a married woman aged thirty-five,
who committed incest with her eighteen-year-old brother; and a
third, a mother aged thirty-nine, who committed incest with her son.
According to Moll, women who suffer from antipathic sexual sensation
are, in many cases, married; it appears, however, that for
the most part they have no inclination to marry. In isolated cases
there may exist a psychical hermaphroditism, the woman thus
affected having sexual inclination both towards men and towards
women. In the case of homosexual women, normal intercourse
appears not to furnish complete satisfaction. As regards fetichistic,
masochistic, and sadistic inclinations on the part of women with antipathic
sexual sensation, Moll was unable to obtain any trustworthy
information. Sometimes in women the perverse sexual impulse
appears periodically, being then often associated with the appearance
of other psychical abnormalities. In some women the perverse
impulse is especially active at the menstrual periods; whilst at other
times these subjects, even though not quite sexually normal, are
still very much quieter. Antipathic sexual sensation in women may
depend upon inherited predisposition, and may often be traced back
to a very early age. In many cases an exciting cause may be
demonstrated.
Mantegazza, who relates that homosexual practices are common
among the inmates of harems, believes that antipathic sexual feeling
is readily curable in women soon after marriage, but that later a
cure is rare.
A perverse form of sexual gratification sometimes met with in
women is flagellation. By chastisement with birches, straps, or whips
on the bare buttocks, the nerves of the sexual apparatus are stimulated,
and these organs become congested, with an effect resembling
that of onanism. Such flagellation was practiced by the wanton
ladies of ancient Rome. In the Middle Ages, hysterical women
derived great pleasure from the stimulatory effect of whippings.
It is reported of Catharine de Medici, that she had herself whipped,
and that she delighted in seeing the ladies of her court undergoing
similar treatment. In the present day many women derive intense
sexual pleasure from being birched by their lovers on bared portions
of their bodies. In Paris and other large towns there are special
places of resort for those who pursue this form of perverse sexual
gratification. Sometimes such women are only the active fouetteuses
for worn-out, perversely-feeling men.
199Among the Greeks, a woman who had remained barren during
the early years of marriage would visit the temple of Juno, in order
to receive from a priest of Pan the gift of fertility. She stripped
naked, and, while thus exposed to the flagellant priests, she received
all over the back of her body numerous blows inflicted with thongs
of a he-goat’s hide—this process being supposed to induce fertility.
The object of this form of flagellation would appear to be to induce
an increase of sexual desire.
Sexual neurasthenia is defined by Eulenburg as a neuropsychosis
of chronic course, manifesting itself chiefly in the form of excessive
irritability of the sensory and psychosensory neuron-systems, in
association with excessive tendency to exhaustion of the motor and
psychomotor neuron-systems. This exhaustion occurs especially in
relation to the genital system, in which we see exhibited the phenomena
of irritable weakness, of increased excitability combined
with increased tendency to fatigue of the genital nerve apparatus—such
chronic morbid disturbances are, according to this author, comparatively
rare in women, that is to say, the developed typical picture
of the disease does not occur in women, or occurs very rarely.
Among 168 patients suffering from sexual neurasthenia, only six
were women. Two of these latter were addicted to masturbation,
and in the anatomical sense both were still virgins; the rest were
married women, not receiving sufficient sexual gratification in their
married life, two of these were probably also addicted to masturbation,
two indulged in homosexual practices.
Onanism, according to Eulenburg, is the cause of sexual neurasthenia
in women as well as in men. If, however, among the relatively
very large number of women addicted to masturbation, there appears
to be such a very small proportion of instances of sexual neurasthenia,
this depends on the fact that from the nature of onanism in
women the physical and also as a rule the psychical consequences are
as a whole apt to be much less severe than those arising from similar
practices in men; but it depends also on the circumstances that
neuromental abnormalities of other kinds and denoted by other
names, such as dyspareunia, vaginismus, sexual hysteria, nymphomania,
feminine sadism, and tribadism, are apt to arise in consequence
of onanism. As regards onanism, so also may it be in regard
to sexual excesses and aberrations in general; they may be on the
one hand causes, but on the other symptoms and sequelæ, of sexual
neurasthenia. Early-acquired or inherited homosexual tendencies
and habits may, as Eulenburg further points out, lead to sexual
neurasthenia only, but then very easily, when such individuals have
allowed themselves, against their nature but in obedience to conventional
points of view and to the advice of the relatives, to be persuaded
into marriage. That sexual abstinence alone is competent to
induce sexual neurasthenia must be dismissed as a fable.
200
II. THE SEXUAL EPOCH OF THE MENACME.
By the term menacme I designate the culmination of the sexual
development of woman, during which the processes of reproduction,
copulation, conception, pregnancy, parturition, and lactation occur.
The processes of puberty in woman are fully completed at the age
of from eighteen to twenty years, so that from this time forward
she is fully equipped for the performance of her sexual duties. The
first act in the fulfilment of these duties is copulation, which in
civilized countries is in the great majority of women first undertaken
at the commencement of married life. The average age at marriage
in the women of this part of the world is 22; but marriages at
an earlier age are very common, and in many circles of society the
average age is as low as 20. The fullest maturity of sexual activity
in women occurs, however, in the thirty-second year of life, this
being the year in which on the average the maximum fertility is
attained.
At the menacme, the beauty and energy of women attain their
fullest evolution, her sexual characteristics their strongest development.
It is this period of life, however, that entails the greatest
dangers to beauty and health in connection with the functions of
the genital organs. Copulation, the first act of sexual intercourse
with the male, often produces in the female injuries from which she
never completely recovers. Gonorrhœal infection has been a source
of unspeakable miseries to women. Motherhood itself entails the
risk of a great number and variety of illnesses, which, as puerperal
sequelæ, affect this phase of woman’s life. The struggle for existence,
in which woman at her prime is also involved, and the fulfilment
of duties to husband and children, further lead to the production
of a series of changes, both physical and mental, in the feminine
organism, which influence all the functions.
The great characteristic of this epoch is maternity. In maternity
the fully developed woman lives and has her being, but to maternity
also she often succumbs as a sacrifice to the fulfilment of her natural
functions. Inasmuch as in this sexual phase the functions of the
genital organs are of greater importance, to the same degree is
enhanced the importance of the mutual relations between these
organs and the other organs of the female body.
201Another influence of fundamental importance in the sexually
mature woman is that of the sexual impulse, the force of which is
at times overwhelming, so that its gratification is sometimes sought
without regard for the consequences to married and family life.
The physiology and pathology of the menacme coincides with the
normal processes and pathological changes respectively of the female
genital organs consequent on their functional activity as organs
of sexual sensation and of reproduction. Woman as wife and
mother stands at the climax of her existence.
In a quite astonishing manner, however, many of the advocates of
the modern movement for the emancipation of women contest the
significance of maternity to women.
A modern authoress and supporter of women’s rights, Ellen Key,
avows that she was in error when at an earlier date she “regarded
maternity as the central point in woman’s existence.” She asserts
that it lies within the sphere of a woman’s individual rights, as of
a man’s, to reject marriage, or to accept marriage while rejecting
maternity. “The grounds for the rejection of maternity may as
well be deeply altruistic as deeply egoistic. It lies within the sphere
of individual rights to dispense with love or with maternity when
either is regarded or both are regarded from this point of view.
It is entirely within a woman’s rights to transform herself into a
member of the ‘third sex,’ the sex of the worker bee, of the neuter
ant, if she finds therein her greatest pleasure. * * * Women
exist in whom erotic feeling is totally atrophied; there are yet others
who fail to find in intercourse with the modern man that soulful
and deep erotic harmony which they rightly desire; and there are
others still more numerous who desire love, but not maternity,
which indeed they dread.”
A celebrated German authoress of the present day, Gabriele
Reuter, refers in similar terms to the justifiable fear with which
so many aspiring and hard-working women regard maternity, “the
perpetual, watchful, emotional dread of motherhood, a dread which
causes them to turn at bay. A dread, a hatred, it is, which has
grown so strong, so active, that one might almost regard it as an
obscure perverse instinct, awakened and developed and strengthened
by bitter necessity. It is as if in the innermost recesses of their
nature such women had a belief that should they pay their tribute
to sex they would loose all the energy, clearness, and brightness of
mind, by means of which they have raised themselves above the level
of their sex. And perhaps women of a certain type are justified
in this fear.”
Fortunately, however, the woman who does not prize maternity
still remains an exception. The great instinct for the preservation
202of the species, which nature has planted deeply in every human
being, still as a rule in women remains much more powerful than
the instinct of self-preservation at every one else’s expense—more
powerful than such self-sufficient egoism. And now as ever it is
the duty of humanity to educate women for maternity from her youth
upward, so that she is in every way fitted for the supreme duty of
her sexual nature, the renewal of life from generation to generation.
Against the significance and importance of maternity to woman,
the mountainous waves of the movement for the emancipation of
women dash themselves as vainly as against the solid rock. Much
justification may be found for the efforts of women in modern
civilized communities to engage in departments of activity to which
hitherto men only have been admitted; and as regards the intellectual
capacity of women we may acknowledge their competence for
the higher scientific professions; but while admitting this we must
hold firmly to the physiological standpoint and must more especially
bear in mind the sexual life of woman. Such professions only
are suitable for a woman as do not entail a restriction of the sphere
of her reproductive activity, a hindrance to her principal duty, that
of maternity, an interference with the discharge of her obligations
to husband and children, or a diminution of her domestic value and
an evasion of her responsibilities in family life. As L. von Stein
so justly remarks, the woman who spends the whole day at a desk,
in the law courts, or in a house of assembly, may be a most honorable
and most useful individual, but she is no longer a woman, she cannot
be a wife, she cannot be a mother. In the condition of our
society, the emancipation of woman is in its very nature the negation
of marriage.
We may not agree with the great misogynist, Schopenhaur, in his
depreciation of the female sex, or in his assertion that woman exists
simply and solely for the propagation of the species, and that “her
life should therefore flow more quietly, more inconspicuously, and
more gently than that of man toward its goal;” nor need we regard
as justified the severe sentence of the philosopher, E. von Hartmann,
that from the moral standpoint, “the greater number of women pass
the whole of their lives in a state of minority, and, therefore, to
the end stand in need of supervision and guidance;” but the statement
made by Friedr. Nietsche in his book Also sprach Zarathustra
deserves acceptation, “Everything in woman is a riddle, and everything
in woman has its answer: it is called pregnancy,” and again,
“For woman, man is only the means; the end is always the child.”
Unsearchable in its judgments, nature has imposed on woman alone
the consequences of the act of generation; man has the pleasure,
but not the labor and the pain. We might indeed regard as highly
203unjust the distribution of the rôles in the process of reproduction,
were it not that in a mother’s love and a mother’s joys, woman finds
a compensatory solace. The man’s part is a much easier one and
costs far less than that of woman; with the gratification of his sexual
desire, man shakes off any further responsibility, whereas the
woman’s body becomes the workshop in the wonderful act of creation
of a new human life.
Maternity, says Lombroso, is the characteristic function of the
female sex, upon which rests her whole organic and physical variability,
and this function is indeed throughout of an altruistic nature.
Although there is a certain antagonism between the sexual impulse
and maternity—according to Icard, the sexual impulse is extinguished
in women during pregnancy,—still, maternity appears to
depend upon sexual perceptions. For instance, the act of suckling
the infant often arouses voluptuous sensations, and Icard mentions
a case in which a woman permitted fertilization to occur solely on
account of the pleasure obtained by suckling. The anatomical
cause of this fact is to be found in the connections between the nipple
and the uterus by way of the sympathetic nervous system. * * *
It is likewise probable that in the happy feeling of maternity there
intermingle very gentle voluptuous sensations derived from the
genital organs. According to Bain also, very delicate sensations of
contact form an element in maternal love.
The epoch of the menacme is that in which, independently of
maternity, the sexual impulse often becomes so powerful in woman
as to be entirely dominant. The problems relating to marriage and
to the sexual position of woman, so widely discussed at the present
day, are, therefore, of especial importance in regard to women at
this period of life. The forcible repression and control of the sexual
impulse inculcated by moral and religious ordinances are now, according
to the modern leaders, both male and female, of the woman’s
movement, to be abandoned; and it is loudly asserted that every
woman has the same right as man to physical love and the happiness
it produces. Hence, free love is demanded. “Freedom in love,
freedom for love—this is what the dignity of the human race demands,”
asserts the authoress of a book recently published (Elisabeta
von Steinborn, The Sexual Position of Woman). With laws
for the regulation of marriage, this section of the women’s rights
party will have nothing to do. A truly good and honorable man,
they contend, has as little need of laws to regulate his amorous
relations as he has of laws against murder and theft. In the first
place, love, the sexual relation between man and woman, must be
free, and humanity, freed from vexations and needless control, will
then seek and find the proper path, even if at the expense of a few
204errors by the way. Only after this unrestrained sexual intercourse
has lasted for a long time, will free marriage become the rule.
“Out of this phase will develop the monogamic system willed by
God, for which, in its most ideal form, we are not yet sufficiently
ripe.” It is hardly necessary to discuss in detail the general deleterious
influence of such unlimited, unregulated free love upon the
community, upon human society as a whole, to describe the results
of free love, to attempt to realize the chaos which it would bring
about in the social relations of civilized humanity. We must rather
indicate it as desirable from the medical standpoint also, that such a
change in general domestic economy shall be aimed at as will enable
the great majority of women to share in married life and family
happiness, and thus making allowance both for human nature and
the demands of social life, to effect a true harmony between sexual
morality and sexual practice.
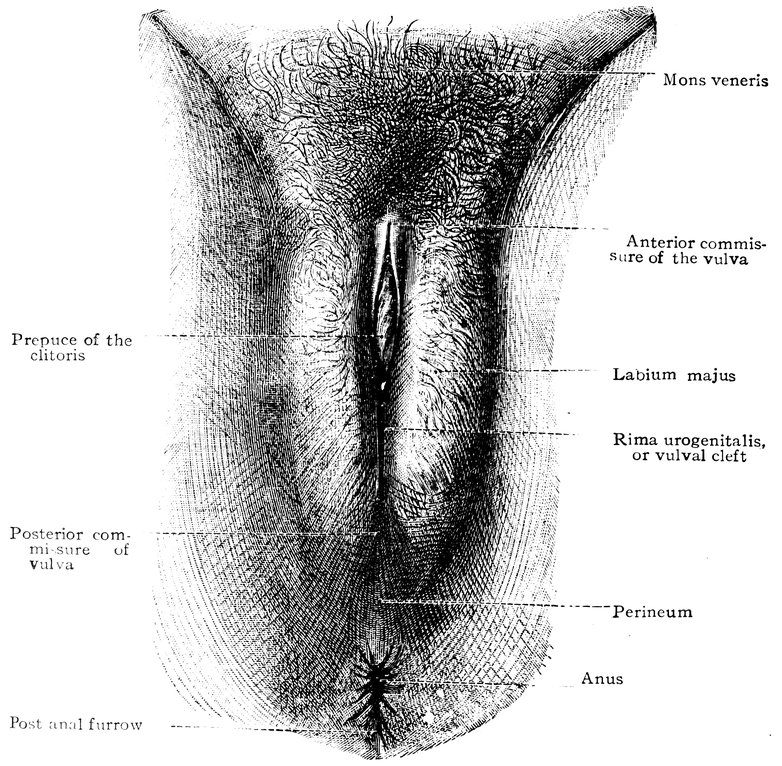
Fig. 48.—The female pudendum, or vulva, with the labia majora. The vulval cleft. Female perineum. Mons veneris, with the pubic hair. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
205We must point out that in so far as the modern woman’s movement
aims at dispensing with man and at basing the entire life of
woman upon the independent ego, that movement is in opposition
to nature and its eternal laws. A woman who thus seeks the solution
of the woman’s question in the direction of freedom and independence
is one who endeavors to avoid the burthen of womanhood.
She desires to escape, always from guardianship, often from
maternity, and usually from the restrictions, the unselfishness of
womanhood. But none the less does she remain unable to escape
from her femininity.
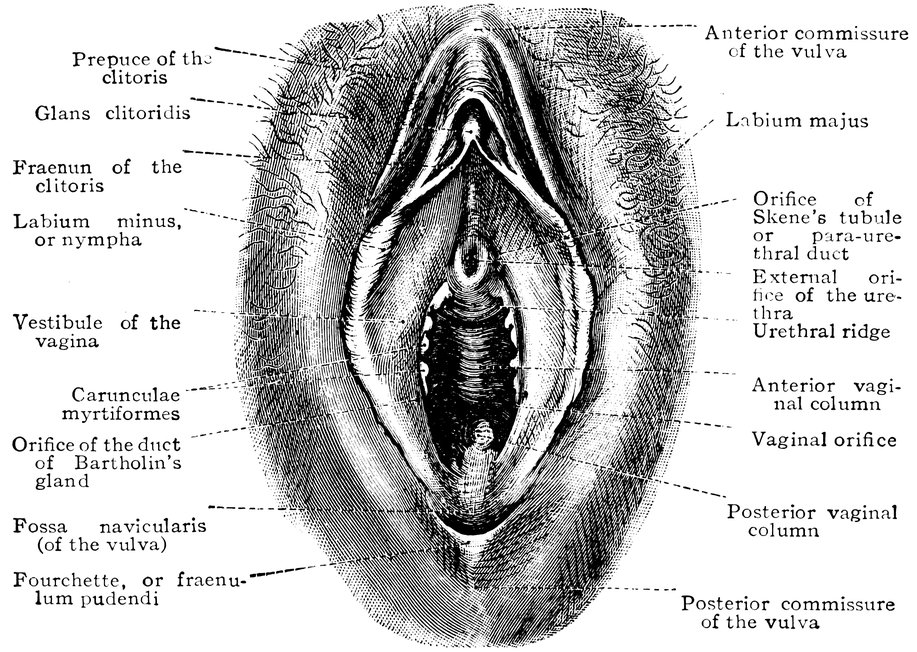
Fig. 49.—Vestibule of the vagina, with the labia minora or nymphæ, the vaginal and urethral orifices, and the glans clitoridis. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
“The true significance of woman,” insists Laura Marholm in
opposition to the modern tendency, “has at all times consisted rather
in what she is than in what she performs, and it is precisely in
the former point that the women of the present day seem so unusually
wanting. Their performances are indeed many and various,
they study and they write innumerable books, they are the directors
or principals of all possible concerns and collect funds for every
possible object, they wear doctors’ gowns, conduct agitations, and
found clubs, and they come continually more and more into publicity.
And yet their public significance is after all diminished. The
greater the influence of woman in the mass and as a numerical
206majority, the less is her influence as an individual, the smaller is the
triumph of her sex. She herself has induced man to sound the
trumpet note of the abhorrence of women. Tolstoi in The Kreuzer
Sonata, Strindberg in numerous dramas, Huysmans in En Ménage,
write in this strain; and in the works of many lesser luminaries we
encounter this mistrust of love. * * * The modern system of
education for girls, with its polyglossia and polymathy, favors a
superficial development of the understanding, and produces women
who are pretentious without being profound.”
Feminine beauty suffers during the menacme from the stress
of the demands made on the sexual activity as well as on the functional
capacity of the individual. Repeated, rapidly succeeding pregnancies
and confinements impair the beauty of the breasts and the
abdomen, the figure and the carriage. In consequence of suckling,
the breasts, hitherto firm and elastic, usually become more or less
pendent and wrinkled, sometimes also flabby and inelastic, sometimes
nodular. Diseases of the genital organs and the disorders of
the general health dependent thereon, leave disfiguring wrinkles in
the face and other traces in the whole structure of the body. Toil,
anxiety, and grief also write their horrible marks deeply on the appearance.
The mature working-class woman, through sharing in
masculine labors, through long-continued muscular exertion, and
through neglect of bodily care, frequently assumes in her features,
her carriage, her figure, and her whole appearance, a rather masculine
type.
The beauty and the youthful freshness of girls belonging to the
labouring classes seldom endure for long after the menarche, and
in cases in which the environment is one of poverty, they last through
a very short part only of the epoch of the menacme. The early appearance
of wrinkles in the face, the stiff, angular character of the
movements, the ungraceful carriage of the body, all these combine
to make a woman of five-and-twenty who groans under the burthen
of toil appear at the first glance an elderly woman, and a closer
investigation shows what damage has been wrought to the attributes
of beauty, how the breasts are flabby and flattened, the belly prominent,
the buttocks pendulous, the arms muscular.
In the well-to-do classes, again, at this period of life, when generous
diet combines with insufficient exercise, an abundant deposit
of adipose tissue may already have occurred, resulting in a great
impairment of beauty, the body and limbs being enlarged, the gait
and the carriage correspondingly altered for the worse—changes
which seem desirable only to those orientals to whom such obesity,
such exaggeration of femininity, is sexually stimulating. If, however,
this deposit of fat is not excessive, this it is which endows
207women during these years of fullest development with an imposing
appearance and buxom form. In favourable circumstances, beauty
of this type may persist to the fortieth year of life and even beyond,
and it is of such a character as to justify the proverb that
woman’s first sexual epoch is dedicated to love, her second to voluptuousness.
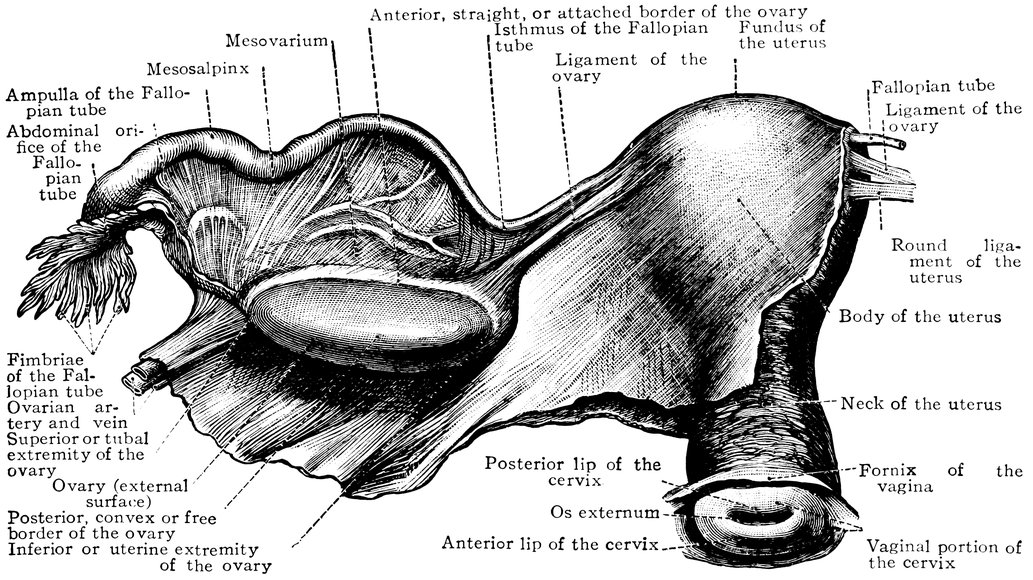
Fig. 50.—The uterus, the left Fallopian tube and the left ovary, in their connection with the broad ligament of the uterus, which has been fully unfolded. Seen from behind. From a virgin, aged nineteen years. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
“Bountiful nature,” writes Mantegazza, regarding woman at this
sexual epoch, “sends to woman an ingenious engineer, who enlarges
the hills to mountains and fills up the valleys with a soft
alluvium of fat. The commencing wrinkles disappear, being
smoothed out under the beneficial influence of this plastic material;
the slender, elastic palm-tree stems are converted into majestic columns
of Parian marble; quality is replaced by quantity, and if the eye
has lost a few provinces, the hand has gained just as many. * * *
A certain number of chosen women understand how to preserve for
as long as ten years the unstable equilibrium of the period which
separates these two ages of life. There are divine beings who with
every oscillation of their tresses or rocking of their hips, with
every undulation of their bosom, every serpentine movement of their
limbs, instil desire. * * * They constitute our most intense
208delight, and our intensest torment, they make our life a blessing or
a curse, they are the uttermost goal of human passion, of human
voluptuous desire.”
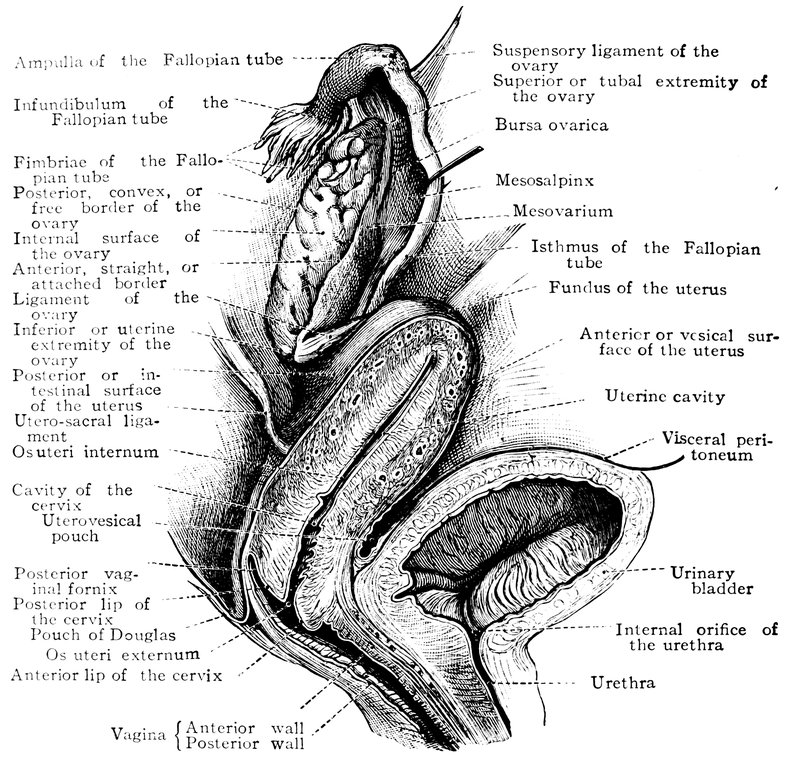
Fig. 51.—Female internal genital organs in the fully developed state. (From Toldt: Atlas of Human Anatomy.—Rebman Company, New York.)
Among the injuries to beauty effected by pregnancy, one above all
evident to the eye is the almost invariably ensuing change in the
skin, principally taking the form of a change in pigmentation, with
the appearance of spots varying in size and tint, on the face and
especially on the lips and the forehead; there is greatly increased
pigmentation also of the areola mammæ and the linea alba, and in
addition of the labia majora and minora and of the anal region. It
is not certain whether this chloasma uterinum is dependent, as Jeamin
assumes, on the discontinuance of menstruation, or, as Virchow
believes, on changes in the blood and the blood-pressure. Sometimes
also, in pregnant women, we observe on the face, chiefly on
209the nose and the cheeks, dilatations of the small cutaneous vessels,
often associated with acne nodules.
A permanent disfigurement is caused by the lineæ (vel striæ) albicantes,
white lines or streaks of varying length and resembling
scar tissue in appearance on the skin of the abdomen, the adjoining
parts of the buttocks and thighs, the lower part of the front
of the thorax, and the mammæ. They are not true scars, not
being new formations of connective tissue, being on the contrary
dependent on solutions of continuity, on relative diminution, that is
to say, of the connective tissue layer of the skin. They are formed
in consequence of the fact that the connective tissue bundles are not
able to keep pace in their superficial enlargement with the necessarily
rapid extension of the cutis, hence great meshes appear in
the former, situate in the direction of the greatest tension of the
skin. (Spietschka and Grünfeld).
Transiently during pregnancy, but in some cases permanently
also, the beauty of the lower extremities is apt to be impaired by
enlargements of the veins, the formation of varices, and sometimes
also by œdema; these conditions depend upon the hindrance to the
venous return caused by the pressure of the pregnant uterus. Thick,
vermicular, bluish strings or nodular enlargements appear in the
course of the great veins, with consequent eczema and ulceration.
In pregnant woman, eczema is common in other regions, on the
face, the hands, the forearms, and the genitals; also erythema,
urticaria, and the pustular eruption known as impetigo herpetiformis.
Parturition and lactation entail further disfigurement of the skin
through the production of various lesions, such as cracks and fissures
of the skin of the breast, dermatitis due to venous thrombosis in the
lower extremities, scarring of the breast after mastitis, etc.
In the description of the sexual life of woman in the epoch of the
menacme, we shall consider at some length copulation and conception,
the relations of fertility and sterility, the important topic of
the use of measures for the prevention of pregnancy, and the interesting
subject of the determination of sex; on the other hand,
pregnancy, parturition, and the puerperal state, since these subjects
are specially treated in the ordinary textbooks on midwifery, we
shall discuss only in so far as certain relations between these reproductive
processes and the organism as a whole and its functions,
appear to us especially worthy of note.
Anatomical Changes in the Female Genital Organs in the Period of the Menacme.
In the fully-developed woman during the period of the menacme,
the mons Veneris forms a rounded elevation which consists of very
210dense connective tissue containing large quantities of fat, while the
integument that covers it is usually coated with a thick growth of
hair. The form of this hairy covering, which by the Roman poets
was designated Hebe, by the Greeks zunaikomustax (translated by
Albrecht Dürer as Weybsbart—woman’s beard), by Galen termed
ornamentum loci, is various, and, as an external sexual character, it
deserves more accurate observation than it has hitherto received from
anatomists.
The hairy covering of the female genital organs is in adults, and
especially in brunettes, very abundant; above, it is usually sharply
limited by a transverse line across the top of the mons Veneris, and
it extends outwards only a little beyond the labia majora, whilst below
it extends only to about the middle of the sides of the perineum.
According to Bergh, however, who made an exact study of this
matter in 2,200 women of ages for the most part between fourteen
and thirty years, in some cases the shape of the patch of hair (which
is in such instances always very thick) resembles that so common in
the male, there being a pointed process, usually rather narrow,
extending upward toward the navel. This masculine form of the
pubic hair is by no means common in women; according to Lombroso
it is met with more frequently in Italian women than in those
belonging to other European nations. In most women, the thick
hairy covering of the mons Veneris is sharply limited above by the
curved line that indicates the upper margin of the eminence, whereas
in men a strip of hair usually passes up from the mons pubis to the
umbilicus. Still, exceptions are met with. Thus, in 100 women,
Schultze found five in whom the hairy covering extended up to the
navel. Sometimes other variations occur, for instance, the hair may
extend laterally into the groin, occasionally as far as the anterior
superior spine of the ilium, and across the upper part of the front
of the thigh, not infrequently in association with a thick growth of
hair along the sides of the perineum as far as the anus. Of women
with the hair growing in this fashion, not a few appeared to Bergh
to have unusually strong sexual passion.
In contradistinction to these cases in which the development of
the pubic hair is thick and even excessive, we meet with others in
which it is very scanty, and this not only in quite young individuals
(at an age from 15 to 18 years), with but slight development of the
labia, but also in older and fully developed women—for the most
part blondes.
The growth of the pubic hair is thickest and strongest near the
median line, whilst laterally the hairy covering is thinner and
weaker. The thickness is extremely variable. “In some women we
find a flattened, occasionally frizzled, turf-like covering; in others,
211a dense, elevated, luxuriant bush of hair” (Bergh). The length of
the pubic hair is variable, but as a rule it is somewhat shorter in
the female than in the male. Still, cases have been known in women
in which it reached to the knees.
The colour of the pubic hair commonly resembles that of the hair
of the head, but the pubic hair is usually the darker of the two.
Blondes with dark or black eyebrows have, according to Bergh,
usually dark or black pubic hair. The pubic hair turns grey late in
life, later as a rule than the hair of any other part, a fact known already
to Aristotle; it is rather late in life also that the pubic hair
becomes thin, and in this state it remains almost invariably up to
an advanced age, even when the scalp has become almost or quite
bald.
The pubic hair, according to the same author, is seldom straight,
being almost always curly, frizzled, or more or less rolled up into
rings or spirals, generally forming smaller or larger locks. Fairly
often, we meet with curled locks, either one pair or two, symmetrically
disposed on either side of the depression adjoining the præputium
clitoridis; these usually have an outward direction. Much
more rarely we find similar locks symmetrically attached further back
on the labia.
In the case of 1,000 adult women examined by Eggel with regard
to the colour of the pubic hair, the colour of the eyes, and the colour
of the hair of the head, there were 239 with dark eyes, 333 with dark
hair on the head, and 329 with dark pubic hair; contrariwise, 761
had light eyes, 667 light hair on the head, and 679 light pubic hair.
Obviously, then, a considerable number of women with light-coloured
eyes must have had dark pubic hair. Roth, in 1,000 North German
women examined by him, found the pubic hair blonde, but a rather
dark blonde, in a large majority of the cases; in red-haired women,
the pubic hair was in all cases bright red, in black-haired women
the pubic hair was black in two-thirds only of the cases, in nearly
a third it was brown, in two cases dark blonde; in Jewesses, in a
large majority of instances, the pubic hair is brown. The arrangement
of the pubic hair is described by Roth as very variable.
“Sometimes it is short and frizzly, sometimes a luxuriant bushy
growth; sometimes the hairs are scanty and thinly set; sometimes
they are irregularly distributed; sometimes we see only a narrow
strip of long hairs down the middle of the mons Veneris, which
is bare at the sides. In some the lateral boundaries of the pubic
hair are sharply defined, in others the hairy covering spreads beyond
the usual limits.”
Among the ancient Greeks and Romans, it was customary for
women to remove the pubic hair, a custom even now observed by all
oriental races; for this reason in ancient art the nude female body
212is depicted without pubic hair. According to Stratz, in the Chansons
de Bilitis it is said of the priestesses of Astarte: “They never
draw their hairs out, in order that the dark triangle of the goddess
shall represent on their bodies the form of a temple.”
The physiological purpose of the pubic hair is to prevent irritation
of the genital organs by the sweat that would otherwise run down
upon them, and to protect the skin from direct friction during the
act of copulation.
The labia majora in women during the menacme are usually
strongly developed, their outer surface is hairy; in parous women
we almost invariably observe small or even large lacerations of
the frænulum pudendi or fourchette, in front of the posterior
commissure of the vulva. On the inner surface also of the labia
majora, the general characters of which are those of mucous membrane
rather than of skin, fine hairs are also to be found. In multiparæ,
and even in women who have frequently had sexual intercourse,
these inner surfaces of the labia majora are not usually any
longer in mutual contact, so that the rima urogenitalis or vulval
cleft gapes more or less. In well-nourished women who have led the
“sheltered life,” the dense and fat-containing connective tissue of
the labia majora (continuous with and similar to that of the mons
Veneris) gives these structures a certain firmness and elasticity, and
the labia minora or nymphæ do not project beyond them. But when
the genital organs are not well preserved, projection of the nymphæ
occurs. In women whose genital organs are beautifully formed,
the nymphæ are of a soft, delicate consistency, and their mucous
membrane is of a pink color; but when the reproductive organs
have been subjected to excessive stimulation, the nymphæ are dry,
hard, brown in color, and they project from the vulval cleft. In
women of the Hottentot and Bosjesman races, the nymphæ attain,
as is well known, an excessive length, forming the so-called “Hottentot-apron;”
and in certain other indigenous races of Africa, the
enormous size of these organs renders resection necessary.
During this sexual epoch, in women with strong sexual passion
and having frequent sexual intercourse, the clitoris is largely developed,
and sometimes the dorsum of the organ protrudes from
between the anterior extremities of the labia majora.
The vaginal orifice gapes a little, so that the irregular carunculæ
myrtiformes are visible. In parous women, the vaginal orifice is
enlarged in such a manner that the wall of the vagina passes directly
and without limitation into the wall of the vestibule, and the external
orifice (meatus) of the urethra is situate immediately in
front of the anterior vaginal column, and thus lies within the vaginal
orifice.
213The breasts of a strong, healthy woman who has attained complete
sexual maturity are more or less firm in consistency, and
considerable in size, exceeding now Ovid’s demand concerning these
organs, ut sit quod capiat nostra tegatque manus. The normal
hemispherical form and the somewhat soft texture are subject to
many variations, these being dependent upon race, climate, and sexual
activity and also upon the kind of clothing worn. The nipple and
its encircling areola are usually of a brownish colour; but in beautiful
women they sometimes retain the pink colour characteristic of these
structures in the virgin. In parous women who have suckled their
children, the breasts are usually pendent, and often the left breast
will be found to be somewhat larger than the other; generally also
in such women the nipples are longer and thicker than normal. Not
infrequently the nipples are withdrawn into a furrow of the skin,
and become prominent only on local stimulation or as a result of
sexual excitement. Sometimes in the region of the areola, especially
in brunettes, we see a circle of small glands, which produce eminences
beneath the skin.
It is easy to understand that the breasts of such women in general
no longer have the virginal form of small hemispheres, but
have matured to a greater fulness and size. This, however, does
not diminish their beauty, for the ideal of beauty must take into
account the natural development of the body. Whereas at the present
time, under the influence of the modern negation or at any rate
undervaluation of maternity as the goal of woman’s life, it is the
tendency of a certain school of art to misprize the influence of that
state on the form of the breast, and to esteem the “flat bosom,” at
an earlier day under the influence of Rousseau’s Emile, a book in
which mothers are strongly urged to suckle their own children, the
full bosom as a beauty was the fashion in art.
Only a perverted taste can find a woman beautiful without bosom—without
“that golden chalice, from which men quaff love, and
children life” (Mantegazza),—an angular, flat being, without a
rounded form. Nothing but a morbid desire for equality with man
can induce woman herself to endeavor to conceal also the external
manifestation of her sexual characteristics, and by her clothing to
disguise, like a nun, the sexual curves of her figure.
Great deposit of fat, such as occurs from liberal feeding in conjunction
with a sedentary mode of life, or as a result of several
pregnancies, destroys the beautiful form of the breasts, which attain
an immoderate size, thus disturbing the grace and symmetry of the
feminine figure, a fact recognized already by the Romans. Hyrtl
condemns, from the point of view of anatomical beauty, the nude
female figures in the pictures of Rubens, remarking that “the goddesses
214and angels of this painter are as luxuriant in their development
as a Flemish dairy-maid;” and the buxom “goat’s-udder
breast” prized by the Arabs does not represent any nobler ideal of
beauty. Sometimes these excessively large and fat breasts hang
down in a conical form, or, as more or less flattened hemispheres,
reach right down over the gastric region; moreover, the interspace
between the two breasts seems to disappear, and they touch or rub
against one another.
According to Ploss and Bartels, the various forms of breast occurring
in different races may be classified as follows: A. According
to size: 1, very large; 2, large; 3, medium; 4, small. B. According
to consistency and firmness: 1, high; 2, semi-pendent; 3, pendent.
C. According to shape: 1, shell-shaped (disc-shaped); 2, hemispherical;
3, conical. The nipples also, according to these authors, exhibit
variations dependent upon race, being in some cases small and
flat, like a little knob, in some cases large and conical in shape, with
a broad base and a rounded extremity, and in some cases large and
cylindrical, having almost the shape of a finger-joint. The areola,
finally, is in some women quite pale in color, in some dark pink, in
some brown and even almost black from excess of pigment.
The uterus of a woman who has attained complete sexual maturity,
has undergone such alterations in its proportions that the cervix
and the body are of almost the same length. The constriction, visible
externally, indicating the separation between these two segments
of the organ, is depressed somewhat toward the external os. In
sexually active women, a widening and an increased curvature of
the region of the fundus occur, the uterine extremities of the Fallopian
tubes becoming more widely separated; at the same time the
posterior wall becomes more and more convex. The more frequently
the uterus has functioned as a reproductive organ, the more
strongly marked is the convexity of the body of that organ. The
relative lengths of the corporal and cervical portions of the uterine
cavity are now the reverse of those that obtain in the uterus of the
child; the transverse and antero-posterior diameters have greatly
increased. Transverse diameter at the fundus; virgin, 4 centimetres
(1.575″), multipara, 5.5–6.5 centimetres (2.165–2.559″): sagittal
(antero-posterior) diameter; virgin, 2 centimetres (0.787″); multipara,
3–3.5 centimetres (1.181–1.378″). (Chrobak and von Rosthorn.)
During the menacme, in consequence of the act of reproduction,
the uterus undergoes important changes in form. In a nulliparous
married woman, the uterus differs little from that of a virgin; the
cavity is somewhat more extensive, the convexity of the outer surface
a little greater, there is some increase in width in the neighborhood
215of the fundus, the plicæ palmatæ (arbor vitæ uterinum) are
confined to the cervical canal; further, under the influence of copulation
the appearance of the vagina changes, it becomes larger, and
its walls become smoother, sometimes quite smooth, from the disappearance
of the rugæ of the mucous membrane and especially of
those attached to the posterior vaginal column. Much more extensive
are the alterations in the uterus of a multipara. According to
Toldt, “the parts of the cavity representing the cornua, which are
pointed on either side as they pass toward the Fallopian tubes, become
completely included in the lower undivided portion of the
cavity, this change being effected chiefly by means of the increasing
outward curvature of the walls, so that the cavity comes to assume an
amygdaloid form; the cervical canal is also enlarged, especially the
lower part, where also the plicæ palmatæ (arbor vitæ uterinum) becomes
less distinct; the vaginal portion of the cervix is shortened,
the os uteri externum gapes, the lips of the cervix are tumid, nearly
equal in length, and usually beset with scarred depressions.” In
nulliparae, the vaginal portion of the cervix is, as in a virgin, of a
rather tough consistency, smooth on the surface, while the external
os is small, like a dimple, or transversely oval; the color of the
vaginal portion of the cervix is identical with that of the vaginal
mucous membrane in general. Through frequent copulation, however,
the form of the vaginal portion of the cervix is so far altered
inasmuch as it is more freely supplied with blood, and, therefore,
changes slightly, in consistency. In multiparæ, in consequence of
lacerations of the cervix, the os uteri externum changes to a wide
transverse fissure with tumid margins, justifying the old designation
of this orifice as os tincæ;, carp’s mouth. A large size of the
external and internal os, moderate enlargement of the cavity, rounding
of the upper angles adjacent to the uterine orifices of the Fallopian
tubes, increased convexity of the walls, and partial or complete
effacement of the plicæ palmatæ (arbor vitæ uterinum), are the
characteristics of the uterus of a multipara (Chrobak and von Rosthorn).
According to Hennig, the vaginal portion of the cervix is
longest in women who have undergone defloration, and in nulliparae;
widest in prostitutes; narrowest in childless wives; thickest in young
widows. This author gives the following measurements of the external
os, showing its variations in accordance with age and sexual
activity:
| In childhood, transversely oval |
0.46–0.56 cm. |
(0.18–0.22″) |
| In the virgin, rounded |
0.20–0.50 cm. |
(0.08–0.20″) |
| In prostitutes, transversely, oval |
0.60–2.50 cm. |
(0.24–0.98″) |
| In sterile married women, round |
0.16 cm. |
(0.06″) |
| In parous married women, transverse fissure |
1.10 cm. |
(0.43″) |
| After the menopause |
0.81 cm. |
(0.32″) |
216In the fully-developed woman, the ovaries undergo changes in size,
shape, and consistency, these changes being dependent upon the
age, the sexual functional activity, and the constitutional predispositions
of the individual. The average length of the ovary is 3–4 centimetres
(1.18–1.58″); the average width, 2–3 centimetres (0.79–1.18″);
and the average thickness 1 centimetre (0.39″). The surface
of this organ gradually assumes a ragged appearance, from the
scarred depressions caused by the great number of successive menstruations
(ovulations)—sometimes the appearance produced resembles
that of a mulberry.
In the vagina at this sexual epoch, the surface of the anterior and
posterior vaginal walls is rendered uneven and rugose by well-developed
vaginal columns (columnæ rugarum), which feel almost as hard
as cartilage, and project considerably above the general level of the
wall; the transverse ridges (rugæ) run horizontally outward from the
columns. By frequent copulation, the rugæ are partially effaced, and
the columns themselves become flatter and softer; still, except in
cases in which the genital functions are exercised to great excess,
the vagina remains tense and rugose until after several children have
been born, when it becomes soft, flaccid, and smooth. Even in women
who have been accustomed to frequent intercourse, the narrowest
portion of the vagina is still the orifice and the part of the passage
lying immediately within the orifice, which can be constricted by the
levator ani muscle; childbirth, however, brings about great and
permanent distension of these parts also. The widest and most distensible
portion of the vagina is the uppermost segment, the region
of the fornices.
A special significance must be attached to the glands of the cervix
uteri, which, according to my own observations, have the function
of providing a secretion that increases the mobility of the spermatozoa,
and this enables them more readily to find their way into the
uterus. I have endeavored, by a series of histological observations, to
determine the properties of these glands and the changes they undergo
in the different phases of sexual life. The most important
results of these researches may be stated as follows. These glands,
which are lined with columnar ciliated epithelium, are but slightly
developed before puberty, being then simple excavations; at the
time of the menarche, they become tubular; later, during the menacme,
they become long, dendriform, blind-ending glands, which
during menstruation and under the influence of sexual excitement,
furnish a secretion, variable in quantity, and in quality distinguished
especially by its alkaline reaction; further, in connection with a
number of pathological disorders of the female genital organs, these
glands undergo various changes both in their anatomical structure
and in their secretory activity. At the time of the menopause and
217after the climacteric age, these glands, which have hitherto consisted
of branched tubules, tend to undergo cystic degeneration,
leading to the formation of the vesicles known as ovula Nabothi.
After the climacteric, the existence of these cysts may be regarded
as a normal occurrence; and, sometimes arranged in grape-like
clusters, they often project so as to occupy the greater part of the
lumen of the cervical canal.
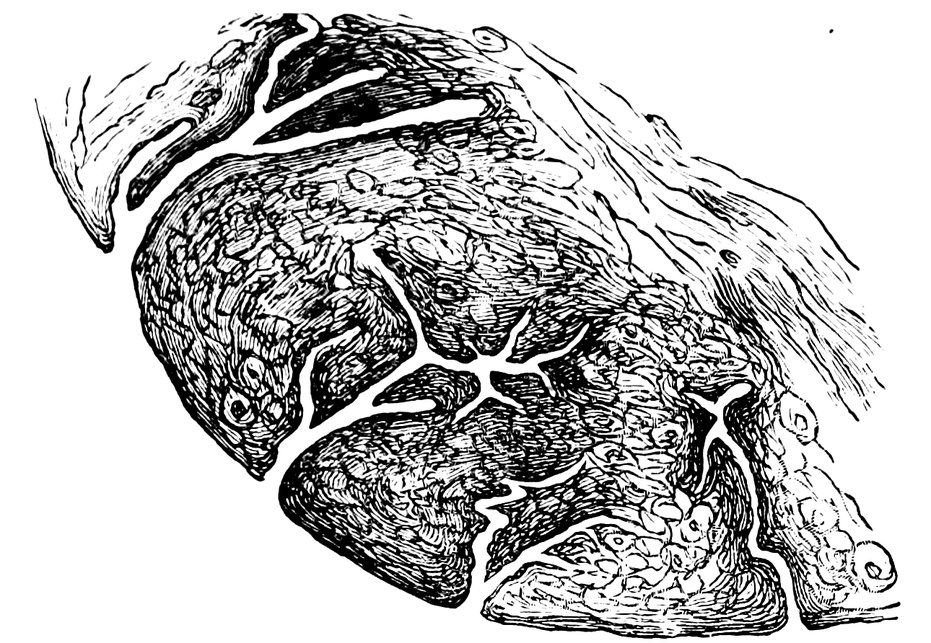
Fig. 52.—Sagittal section through the cervix uteri of a woman 26 years of age, dendriform branched glands.
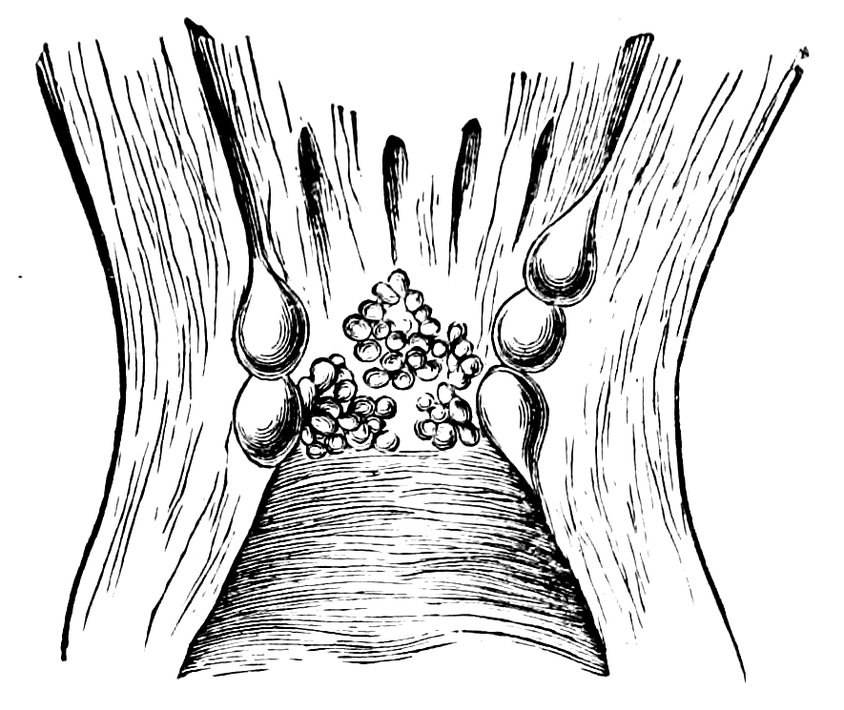
Fig. 53.—Cervix of a woman 72 years of age, with glands that have undergone cystic degeneration.
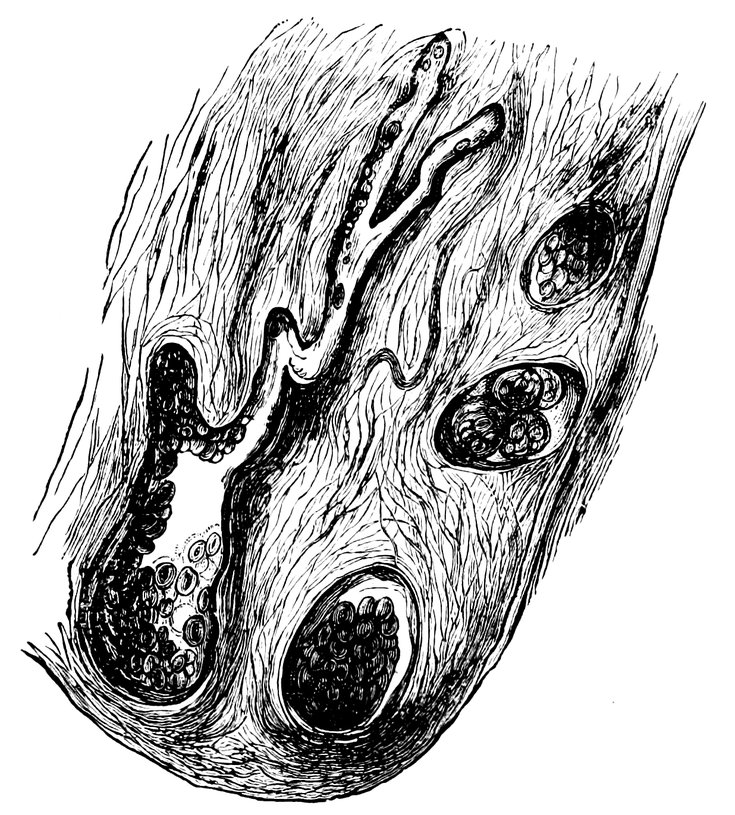
Fig. 54.—Sagittal section through the cervix uteri of a woman 65 years of age. The glands have undergone cystic degeneration.
Diseases of the uterine mucous membrane during the period of
sexual maturity often induce various pathological changes in these
cervical glands. In consequence of obstruction of their excretory
218ducts, they may undergo cystic degeneration, forming follicles filled
with mucus and epithelium, or cavities containing blood, which pass
through the substance of the cervix in every direction; or they
may give rise to the formation of slowly-growing glandular polypi
and other glandular new formations—changes the general result
of all of which is to interfere with the secretory function of the
glands.
Pathology of the Menacme.
The full evolution of the sexual life brings in its train many
dangers to a woman’s life. This appears at first sight from a comparison
of the mortality of married women during the period of
greatest sexual activity with that of single women of similar age.
Between the ages of 20 and 25 years, the mortality of married
women is in all races higher than that of unmarried women; and
the same is true between the ages of 25 and 30 years, except in
France, in which country from artificial causes maternity ceases
at a very early age. In Prussia, in the year 1880, of every 10,000
married women, between the ages named, 21 died, of every 10,000
unmarried women, only 2. In Holland, Belgium, and Bavaria, this
excess in the mortality of married women continues up to the age
of 40 years; whilst in Prussia, from the age of 30 upward, the
mortality of married women and unmarried is practically the same.
In many countries, the mortality of married women at many ages
exceeds even that of unmarried men.
This greater comparative mortality of married women is ascribed
by Hegar to the satisfaction of the sexual impulse, and this authority
believes that the dangers attendant on this function would be manifested
yet more clearly if the contrast were made, not between married
women and single, but between those habituated to sexual indulgence
and those who are continent. We, however, are of opinion, that
the satisfaction of the sexual impulse is only harmful to this extent,
that it exposes women to the consequences of venereal infection,
and also to the risk of numerous puerperal and other diseases of
the genital organs. This is proved also by the statistical results of
the investigations concerning mortality during pregnancy, parturition,
and the puerperium. According to Hegar, adding deaths resulting
from premature delivery to deaths resulting from delivery
at full term, we find the mortality of childbirth in Germany to be
about 0.6 per cent.
Whilst Bertillon and Simpson believe that the lower mortality
of married women above forty years of age as compared with unmarried
women at the same period of life is dependent upon the
advantage to the former of the fulfilment of sexual functions, Hegar,
on the contrary, gives another explanation. He writes: “At the
219age of 40, the less powerful married women have already been
weeded out. At first, owing to the selection exercised by marriage,
the quality of the unmarried women was inferior to that of the
married women; the former, however, have not been exposed to
the dangers attendant on the reproductive process, and so have
passed through the time during which the body possesses the greatest
elasticity; but in the years in which a decline in the vital powers
naturally sets in, the originally inferior quality of the unmarried
women is manifested by a comparatively higher mortality. Also we
have to take into account among the unmarried, the consequences of
extra-marital sexual intercourse and of prostitution, and further the
lack of a family, of the support furnished by husband and children.”
In addition to the far-reaching disturbances of health dependent
on sexual activity at this period of life, there are the minor domestic
troubles by which woman is depressed and by which her powers are
exhausted. The influence of these latter is admirably described by
G. von Amyntor: “How many millions of brave house-wives boil
and scrub away their vital energy, their rosy cheeks, their merry
dimples, in the performance of their household duties, until they
become wrinkled, worn-out, dried-up mummies. The ever-renewed
question, ‘what must be cooked for dinner to-day,’ the perpetually
recurring necessity for scouring and sweeping and dusting and
washing-up—these are the continual dropping which slowly but
surely wears away soul and body. * * * On the flaming altar
on which the sauce-pan simmers, youth and simplicity, beauty and
good temper, are offered up; and who can recognize in the old,
hollow-eyed cook whose back is bent with toil and trouble, the once
blooming, energetic, chastely coquettish bride adorned with her
myrtle crown?”
A great number of the diseases of the female genital organs occurring
at the epoch of the menacme need only a passing mention.
Even coitus, in cases in which there is great disproportion in size
between the penis and the vaginal orifice, or when the organ is very
rapidly introduced or the act is very roughly performed, may lead
to injury to the vulva or the vagina, a fact to which a very large
number of recorded cases bears witness.
During the acme of the sexual life of woman, disturbances of the
menstrual function are also frequent. Menstruation may cease in
consequence of intercurrent diseases or constitutional anomalies;
amenorrhœa may occur during the convalescence from acute diseases,
in obese women, in those suffering from tuberculosis, diabetes,
alcoholism, or psychoses. On the other hand, severe menorrhagia
or atypical metrorrhagia may occur, the bleeding either being due
to diseases of the uterus, such as endometritis, retroflexion of the
220uterus, or uterine myomata, or resulting from infectious diseases,
disease of the heart or kidney, or from general disturbance of the
health by chill or over-exertion. Or, again, dysmenorrhœa may arise,
either as a symptom of some local uterine disease or in consequence
of external noxious influences or weakness of the nervous system.
During the life-epoch of the menacme, moreover, disturbances of
the nutrition of the uterus are of common occurrence, as, for example,
hyperplastic processes in the mucous membrane of the cervical
canal and of the cavity of the body of the uterus. Common also
during the menacme is chronic oöphoritis, which may be due to mal-regulation
of marital intercourse (especially to coitus too soon after
childbirth), to carelessness during menstruation (dancing, skating, or
mountaineering), to incomplete coitus (congressus interruptus), and
not infrequently, to gonococcal infection; or, finally, the oöphoritis
may occur soon after the puerperium in association with subinvolution
of the uterus.
Next we may mention inflammatory diseases of the Fallopian
tubes. In the etiology of these diseases in latter-day marriage, a
dominant rôle must be assigned to the gonococcus; but they also
arise in many cases from nutritive disturbances, infection (other
than gonorrhœal), and indiscretions during menstruation. Pelvic
peritonitis owns similar causation.
In this phase of women’s life, the commonest new growths of the
uterus, myomata, also develop, most commonly between the ages
of thirty-six and forty-five, and they occur in strikingly larger proportion
in unmarried women; it is between the same ages also that
cysto-adenomata of the ovaries are of commonest occurrence.
Sexual intercourse gives frequent opportunities for the introduction
of infective germs into the vagina, and for the origination of
inflammatory affections of the mucous membrane (colpitis), the
intensity of which depends upon the species, the quantity, and the
virulence of the germs in question, on the one hand, and upon the
local and constitutional predisposition of the infected person, upon
the other. Especially grave in its consequences is gonorrhœal infection
transmitted by the male, for this virus gives rise to a great
variety of pathological processes in the female genital organs. In
the act of defloration, considerable injuries are sometimes produced,
and these readily supply a breach for the invasion of infective organisms.
The condition of passive hyperæmia that occurs in the genital
organs during pregnancy also provides a favorable soil for their
growth.
Gonorrhœal infection of young married women is so frequent and
so serious an occurrence in the sexual life of woman, that it requires
special consideration. The cases in which the man entering upon
221marriage is so unscrupulous and so brutal as to deflower his young
wife and to continue copulating with her, while suffering himself
from a quite recent and active gonorrhœa, are on the whole rare.
More common is it for the bridegroom to believe himself completely
cured of his previous claps, and he is declared cured by his physician.
The disease is, however, latent merely, the gonorrhœa has
become chronic, the discharge is so slight that it is overlooked; but
by the stimulation of the frequent acts of coition usual in the early
days of marriage, the disease is lighted up afresh, the gonococci
multiply quickly and intensely, the young wife is infected, and
suffers from an acute gonorrhœa, which may often escape observation
for a considerable period.
In a gonorrhœal marriage, one in which both husband and wife
have gonococci in their genital organs, very diverse phenomena may
be observed and very various conditions may result. On this subject
M. Runge writes: “If the husband’s gonorrhœa is not cured,
fresh, virulent cocci are repeatedly transmitted to the wife, in whom,
therefore, the disease often gets worse by distinct stages. If the
wife undergoes treatment, the effect in these circumstances will
naturally be nil, since the husband is always supplying fresh infection.
On the other hand, the wife on her side returns the gonococci
to her husband, and in this way his gonorrhœa may undergo aggravation.
If the husband is compelled, by illness, for instance, or by
absence, to abstain for a long period from intercourse with his wife,
the latter’s gonorrhœa may, in favorable circumstances, undergo
alleviation and cure. It may happen, however, that in the husband,
in consequence of sexual rest, the gonorrhœa becomes latent, and
even entirely disappears, whilst the wife still suffers from infection.
If now, after long abstinence, the husband has renewed intercourse
with his wife, he may be reinfected, and suffer from an acute attack
of gonorrhœa, though this is due to the descendants of the very
gonococci that he himself sometime before conveyed to the genital
organs of his wife—he reinfects himself, as people say. Such
cases have given rise to suspicions of unchastity on the part of the
wife, when the husband is in actual fact enjoying his own work in
a new edition. A further possibility is that both husband and wife
have become habituated to their own gonococcal interchange; that
is to say, the organisms produce no notable effect in either. But if
the wife in such a condition receives the embraces of a lover, the
latter may be infected with an acute gonorrhœa—a fact that has
long been known.”
The principal rôle in the etiology of the diseases of the female
genital organs must be assigned to pregnancy and childbirth. Anæmic
women readily suffer during pregnancy from a further decrease
222in the corpuscular richness of the blood; those affected with valvular
incompetence find their troubles much aggravated by pregnancy;
where the kidneys are in an irritable condition, pregnancy not infrequently
results in the onset of nephritis, those with disordered digestion
often suffer from increased disturbance of the functions
of the stomach and the intestinal tract; those with gall-stones are
apt to suffer from exceptionally severe attacks of biliary colic, and
acute yellow atrophy of the liver is especially apt to occur during
pregnancy. In women in whom dilatations of the veins already exist,
very great increase of the enlargement is apt to occur during pregnancy;
and in the same circumstances, trifling telangiectases increase
to extensive angiomata. Enlargements of the thyroid body
undergo rapid increase during pregnancy, so that they may attain
threatening proportions. In women in whom the abdominal walls
are flaccid, the viscera may protrude during pregnancy through the
enlarged lacunæ, giving rise to herniæ. The great relaxation of the
peritoneal and other ligamentous attachments of the great abdominal
glands, occurring during pregnancy and the puerperium results in
displacements of these organs; hepatoptosis (migrating or movable
liver), lienoptosis (splenoptosis or wandering spleen), nephroptosis
(ren mobile, floating or movable kidney), and other varieties of enteroptosis
(splanchnoptosis, visceroptosis, or Glénard’s disease). During
pregnancy, previously sound teeth are apt to become carious, and already
existing caries rapidly advances. New growths of various kinds
originate at this period, those previously present exhibit rapid increase;
and relapse after operations for the extirpation of malignant tumors is
especially apt to occur. Even the bones are unfavorably influenced.
A weakened nervous system is subject to a storm of changing
nervous troubles, in some cases so severe as to lead to the outbreak
of actual psychoses; while mental disorder already present tends,
as a rule, to be seriously aggravated during pregnancy. In the eyes,
serious disorders may occur, such as retinitis, and atrophy of the
choroid with complete amaurosis. As regards the hearing, tinnitus
aurium is not uncommon, and sometimes complete deafness occurs.
Numerous diseases of the skin are apt to occur during pregnancy;
in addition to the well-known pigmentation of the face, the areola
mammæ, and other parts, we may have herpes, eczema, or pruritus.
The serious aggravation which pregnancy is liable to induce in
many disorders previously existent, is well known, and this exacerbation
provides in some cases an indication for the induction of artificial
abortion. This necessity may arise in severe cases of renal,
cardiac, pulmonary, or hepatic disease, in progressive anæmia, severe
osteomalacia, hæmophilia, and many other acute and chronic pathological
states, since, in exceptional cases, as pregnancy advances, the
223symptoms of any one of these diseases may become so threatening,
that the patient’s life is either in immediate danger or is almost
certain to be in danger within a very short space of time—this may
occur, for instance, in diabetes, struma (goitre), or certain nervous
diseases, such as chorea, polyneuritis (multiple neuritis), or mental
disorders. Undoubtedly, in this connection, as W. A. Freund insists,
it is not the actual nature of the disease that is of decisive
importance, but rather its intensity, and its influence on the health of
the pregnant women; these circumstances, considered in relation to
the resisting powers of the patient, must be determinative in the adoption
of measures for terminating the pregnancy. An indication for
the induction of artificial abortion is generally furnished also by uncontrollable
vomiting dependent on pregnancy and endangering the
life of the patient; irreducible incarceration of a retroflexed gravid
uterus in the pouch of Douglas, or of a gravid uterus in a hernia, or
irreducible prolapse of a gravid uterus will also necessitate abortion.
W. A. Freund gives an example of a common pathological state,
usually quite free from danger, but now and again, when associated
with pregnancy, seriously endangering life and rendering the
induction of artificial abortion absolutely necessary—this is acute
struma vasculosa—(vascular enlargement of the thyroid body),
which may during the first three months of pregnancy exhibit such
rapid growth as to lead to severe orthopnœa and cyanosis and so to
imperil the patient’s life.
In cases in which laryngeal tuberculosis exists as a complication of
pulmonary tuberculosis, the former disease sometimes progresses
so rapidly in the course of pregnancy that sudden death from œdema
of the glottis is by no means rare. Freund, therefore, sees in this
complication an absolute indication for the artificial termination of
the pregnancy.
In cases of previously well-compensated valvular lesions of the
heart, disturbances of compensation not infrequently occur as a result
of pregnancy; whilst in cases in which cyanosis, dyspnœa, albuminuria,
and dropsy existed even before pregnancy, the latter
condition is likely to result in an aggravation of these symptoms to
a degree that imperils life.
Parturition, to an even greater extent than pregnancy, may induce
serious injuries to the female organism. Thus, during parturition,
lacerations of the vagina are frequent, with consequent scar-formation
and stenosis; lacerations of the perineum are also common,
causing great inconvenience, and when complete, leading to
incontinence of fæces with all its unpleasant consequences. Great
is the danger arising from septic puerperal inflammations, such as
pelvic peritonitis (perimetritis); serious are the results of puerperal
vesico-vaginal and recto-vaginal fistulæ.
224A large part in the local pathology of the female genital organs is
played by the various displacements of the uterus, either arising in
consequence of inflammatory processes in their ligaments, or dependent
upon relaxation of these ligaments from subinvolution of
the internal generative organs, either following delivery at full
term or following abortion.
The injury which women alike of the well-to-do and of the laboring
classes suffer in consequence of numerous and frequently repeated
pregnancies, is minutely described by Hegar. “We can,” he
writes, “calculate the danger to life to which such an unfortunate
woman is exposed by the act of reproduction. If we assume the
ordinary mortality of women in childbed to be 6 per mille, then,
in a woman who within 15 years has been delivered 16 times
(whether prematurely or at full term), the danger will be 16 times
as great as that of a single delivery, and the mortality will be
6 × 16 = 96 per mille; that is to say, of 1,000 women who have all
been pregnant that number of times, 96 will die—nearly 1 in 10.
Moreover, in this calculation the increased danger consequent upon
the unusually rapid sequence of the deliveries has not been taken
into consideration. And, again, only the immediate results of the
deliveries have been taken into the account. Not infrequently women
succumb at a later date to illnesses acquired in childbed; whilst
others, in consequence of repeated pregnancies, have their powers of
resistance so greatly diminished, that they are unequal to the contest
with incidental diseases. In any case, a woman who has experienced
numerous and rapidly successive pregnancies, has sustained damages
which will endure for the rest of her life. Her tissues have
lost their elasticity, the abdominal walls are flaccid, the abdomen is
prominent, the abdominal viscera are displaced, the vessels dilated,
the reproductive organs in a state of subinvolution, and are the seat
of structural alterations. The greatest dangers arise in cases in
which the pregnancies are consequences that have to be paid for
illicit love, since in such cases syphilitic and gonorrhœal infection are
exceptionally common. These complications, indeed, are not excluded
in the case of married women, since marital infidelities occur,
and, again, a premarital but not completely cured venereal illness may
bear fruit in marriage, the latter occurrence being almost always attributable
to the husband. Syphilitic or gonorrhœal infection may
also arise in some other way than by copulation, and to this women
are more exposed than men, owing to the greater size of the genital
passage in the former.”
Very numerous are the disorders of the nervous system referable
to the sexual functional activity of woman during this epoch of her
sexual life.
225Freund, in his description of a neurasthenic symptom-complex
to which he gives the name of angst-neurosis,[36] maintains that the
cause of these attacks of anxiety[36] is very frequently to be found in
a number of injurious influences in the sphere of the sexual life.
In women, these anxiety-neuroses occur:
a) As virginal anxiety, or anxiety of adolescents. Freund has
observed a number of unequivocal instances showing that a first
encounter with the sexual problem, a rather sudden unveiling of
what has hitherto been concealed, as, for instance, the sight of some
sexual act, or something read or heard in conversation, may, in a
girl at the time of puberty, give rise to an anxiety-neurosis, which
is in a very typical manner combined with hysteria.
b) As anxiety of the newly married. Young wives who have
been without sexual feeling in their first experience of intercourse
are not infrequently attacked by an anxiety-neurosis, which, however,
disappears as soon as the sexual feeling becomes normal.
Since, indeed, the majority of young women who lack sexual feeling
in their first experience of sexual intercourse remain nevertheless
quite healthy, it is evident that some other cause must coöperate
in arousing the anxiety-neurosis.
c) As anxiety in married women whose husbands suffer from
ejaculatio praecox or from great diminution of sexual potency, or
d) Whose husbands practice coitus interruptus or coitus reservatus.
Cases in these two classes are closely associated, since it is
easy to ascertain, from the analysis of a sufficiently large number
of cases, that the really important question is, whether during coitus
the wife obtains or fails to obtain sexual satisfaction. In the latter
event, the condition requisite to arouse the anxiety-neurosis is supplied.
e) As anxiety in widows and in voluntary abstinents, not infrequently
in typical combination with impulsive ideas.
f) As anxiety in the climacteric period, during the final flare-up
of sexual passion.
Numerous anomalies of the genital organs which gave rise in the
virgin to no trouble whatever display their influence during the
menacme by unfavorably affecting the nervous system. Thus, in
cases of malformations of the external organs of generation, slight
atresia of the vagina, a rudimentary condition of the vagina, a rigid
hymen, or local changes in the vagina, it is only when sexual intercourse
begins that neuroses or hysteroneurasthenic troubles ensue.
226So also at times nervous diseases which, though the disposition to
them was present, were latent in the girl, such as epilepsy and various
mental disorders, first become apparent in consequence of sexual
intercourse.
The mechanical irritation of the nerves of the pelvis that occurs
in sexual intercourse may, even in women whose reproductive organs
are healthy, arouse sensations of weight, pressure, and bearing-down,
various painful sensations in the sacral region, over the coccyx, in
the buttocks, or in the upper part of the thighs, and also “lumbar
enlargement symptoms,”[37] viz., weakness of the lower extremities,
abnormal sensations of fatigue in the lower extremities and the
back, sometimes also disorders of micturition and defæcation.
Throughout the manifold diseases of women in or connected with
the reproductive system during the age of sexual maturity, associated
mental processes take place, which powerfully affect the nervous
system. Such processes are, melancholy and anxious thoughts concerning
the possible influence of the illness on the happiness of married
life, concerning childlessness, or concerning loss of a husband’s
sexual esteem, or again, fear that the affection will become cancerous,
fear of some necessary operative procedure, or vexation in
consequence of the limitation of her usefulness as housewife, wife,
and mother. Thus in women suffering from sexual affections, a
state of general neurasthenia, or some neurasthenic functional disturbance
of other organs, very commonly arises.
The knowledge that she is suffering from an affection of the
genital organs, makes a deep and lasting impression on the mind
of a woman who takes a serious view of her duties as a wife, and
whose thoughts and feelings are concentrated in the sexual sphere.
The result is, that minor troubles are regarded through the magnifying
lens of anxiety, and the general sensibility is increased. This
hyperæsthesia is not confined to the affected region, but manifests
itself in various other parts of the body by numerous phenomena of
a reflex character. In the first place must be mentioned severe
headaches, sacrache, sensations of pressure in the abdomen, cardiac
troubles, palpitation, stomach-ache, nausea and retching and
disorders of appetite and digestion. Capacity for work and the
enjoyment of life are destroyed by these disorders.
We have further to take into account the numerous conditions
liable to disturb the mind at this period of life. In childless women,
we have the subject of their sterility, the continued yearning to be
blessed with children, the eager search for a remedy, and not rarely
in these cases the conflict between the reproductive impulse and the
ethical principle of conjugal fidelity. In fruitful mothers, on the
227other hand, we have the anxiety lest, by too frequent child-bearing
their beauty should be impaired and the livelihood of the family endangered;
these considerations leading in many cases to the practice
of coitus reservatus, with its deleterious physical and moral consequences.
In the middle and working classes, we have the strain
of the endeavor to be a helpful companion to the husband and at
the same time to assist in the support and the education of the
children. Last but not least, we have the potent influence of local
therapeutic measures, and the fear of operative procedures, both
of which have a most agitating effect on a woman’s mind. In truth,
the menacme is a period full of stormy excitations and powerful
revolutions.
In addition to its influence on the genital organs themselves, the
sexual life of woman during the period of the menacme manifests
its powers for evil especially in relation to the digestive functions,
and to the functions of the heart and the nervous system.
When we compare the various consequences which may be induced
in the principal organic systems as a result of functional
disturbances and organic diseases of the female genital organs, we
find that in respect of the frequency of their occurrence the diseases
of the nervous system occupy the first rank; next in frequency come
the disorders of the digestive organs that arise in sympathetic association
with diseases of the female reproductive organs; whilst the
third rank in respect of frequency and importance is occupied by the
cardiac disorders that arise in connection with changes in the female
organs of generation, and take the form either of disturbances of
the heart’s functions or structural changes in the heart’s muscle.
Dyspepsia Uterina.
Although it has long been a familiar observation that pregnant
women and women suffering from diseases of the reproductive organs
suffered from various dyspeptic troubles, I was myself the
first (in the Berliner Klinische Wochenschrift, 1883) to bring together,
and to describe under the name of dyspepsia uterina, a peculiar
group of dyspeptic conditions which are dependent upon diseases
of the female reproductive organs. I dismissed from consideration
organic diseases of the stomach and intestine dependent upon
anatomical changes in these organs, even though these also might owe
a similar etiology, and described only the more frequent dyspepsias
occurring without organic change in the digestive apparatus, the origin
of which is to be explained by the fact that certain structural
changes and displacements of the uterus (to be discussed later)
arouse centripetal impulses, and that these exercise a reflex influence
on digestive activity.
228This influence, according to my observations, affects the secretory
and muscular apparatus and also the nervous elements of the digestive
tract, and I regard the following conditions as characteristic
of uterine dyspepsia, though they do not necessarily all occur simultaneously:
changes in the gastric secretion, excitement of the vomiting
centre, an inhibitory influence on intestinal peristalsis, and
hyperæsthesia of the stomach.
The symptoms of uterine dyspepsia may vary greatly in intensity,
but not infrequently become so severe as to disturb very seriously
the general health of the woman so affected. They may be enumerated
as follows: The appetite in uterine dyspepsia is variable,
but is generally good; the tongue is not usually coated to any
great extent, nor does the mucous membrane of the mouth commonly
exhibit any notable change; pain in the epigastrium is common
after meals, with acid eructations and heartburn (pyrosis);[38]
sometimes there is violent vomiting, occurring after every meal, or
in the morning on an empty stomach; in addition, constipation is
an almost constant symptom, associated with excessive development
of gases in the intestinal canal. The pain is usually dull in character,
and somewhat relieved by pressure, but it may be severe
and lancinating, and may shoot along the intercostal spaces. The
accumulation of flatus within the abdomen gives rise to various
painful sensations, distension, a sense of fulness; and its expulsion
is attended with notable relief.
As regards the composition of the gastric secretion, an increase
of acidity is sometimes noticed. Gastric digestion is retarded; experimental
evacuation of the stomach, after a simple test meal (beefsteak
and roll) showed that small quantities of undigested remnants
were to be found in the stomach as long as seven or eight hours
afterwards. The frequent eructations evacuate flatus, or else a
watery fluid with an acid reaction (pyrosis or water-brash—see
note 38). By the act of vomiting, larger or smaller masses of
the food that has been taken are evacuated; in the vomit, sarcinæ
in large numbers may frequently be detected by the microscope.
Constipation is present in nearly all cases of uterine dyspepsia; and
even in cases in which attacks of diarrhœa occur from time to time,
careful examination will show that these are generally transient,
being sequelæ of constipation due to the irritation caused by the
accumulated masses. In one case of long-standing uterine dyspepsia,
I observed, in the absence of any gastric dilatation, the well-known
229phenomenon of “peristaltic restlessness of the stomach” (tormina
ventriculi nervosa), in which the peristaltic activity of the stomach
is greatly exalted, and becomes visible to the naked eye in the form
of large and powerful undulations in the gastric region, moving from
left to right.
With these symptoms affecting the digestive organs are associated
variable nervous manifestations in different organs, such as neuralgia
of various nerves, palpitation of the heart, vertigo, headache, and
nervous asthma. The general nutrition of the body often suffers
considerably in cases of long-enduring uterine dyspepsia; excessive
emaciation and general marasmus may ensue; we see also mental
depression, melancholia, an irritable disposition, and disinclination
for every kind of work.
Very important, but very difficult, is the differential diagnosis
between uterine dyspepsia, on the one hand, and, on the other,
chronic gastric catarrh, chronic ulcer of the stomach, nervous dyspepsia,
and sometimes even carcinoma of the stomach.
As regards the distinction from chronic gastric catarrh, in this
latter disease loss of appetite and changes in the oral mucous membrane
are prominent symptoms; the vomit also usually contains much
mucus. More difficult is the differential diagnosis of chronic ulcer
of the stomach, in cases in which anæmic subjects complain of
anomalies of menstruation, associated with dyspeptic troubles and
cardialgia. In severe cases of uterine dyspepsia, the distinction from
carcinoma of the stomach may be very difficult—at any rate in
cases in which no examination of the genital organs has been made.
Obstinate dyspeptic troubles, resisting all curative measures (unless
indeed these are directed to the relief of the local disorder of the
reproductive organs), progressive anæmia, great emaciation, and
pains localized in the stomach, are all conditions common to both
of these maladies. The absence of a tumor of the stomach, careful
examination of the vomit, and examination of the genital organs,
will lead to a correct diagnosis if the case is one of uterine dyspepsia.
A superficial investigation is exceedingly likely to result in a case
of uterine dyspepsia being regarded as one of nervous dyspepsia
(von Leube); none the less, even though a very close resemblance
exists between the symptoms of the two diseases, to differentiate
them is a matter of importance. In nervous dyspepsia, the act of
digestion influences the nervous system in such a manner that, even
when the chemical processes are normal, the organism as a whole
is sympathetically affected by a reflex from the stimulation of the
nerves of the stomach, and in return reacts on the mechanical process
of digestion in a more or less violent manner. In uterine dyspepsia,
however, the relationship that obtains is exactly the reverse of this,
230inasmuch as the gastric activity is influenced by the nervous system,
by reflex impulses originating in the morbid processes in the
reproductive organs; moreover, in this form of dyspepsia, in direct
contrast with nervous dyspepsia, the chemistry of digestion is often
disordered, and, in addition, the process is not completed within the
normal period.
Oftentimes, the diagnosis of uterine dyspepsia can be made with
certainty only ex juvantibus.[39] For this disorder cannot be cured
unless the disease of the reproductive organs on which it depends is
first relieved; and, conversely, local measures for the relief of uterine
disease, will often at once remove all the dyspeptic troubles from
which the patient suffers.
My own experience has led me to conclude that it is certain
distinct local mechanical stimuli affecting the female genital organs
which, acting for a long period on the sensory nerves of the uterus
or its annexa, induce by reflex action the before-mentioned digestive
disturbances. Diseases of the vulva and the vagina, catarrhal
inflammation, colpitis and leucorrhœa, and prolapse of the vagina,
do not by themselves lead to the occurrence of uterine dyspepsia;
nor do inflammations of the uterine mucous membrane, such as
endometritis (unless associated with parenchymatous changes of the
whole uterus), chronic catarrh of the mucous membrane, erosion
and ulceration of the cervix to an inconsiderable extent, or moderate
perimetritic and parametritic exudations. On the other hand, uterine
dyspepsia frequently ensues in cases of uterine displacements,
flexions, or versions, or in cases of structural changes of the uterus
accompanied by enlargement of the organ, chronic metritis,
myomata, especially when intramural (interstitial), displacement of the
Fallopian tubes and the ovaries, chronic oöphoritis, extensive
inflammatory exudations, resulting from pelvic peritonitis, and
leading to dislocation, “compression” or distortion of the uterus and its
annexa, deep follicular or carcinomatous ulceration of the cervix, or,
finally, ovarian tumors. As the commonest condition giving rise to
dyspeptic disturbances of the kind under consideration, retroflexion
of an enlarged uterus must be mentioned.
Under the head of uterine dyspepsia, we may also classify dyspeptic
disturbances occurring at the time of puberty or of the menopause,
and in association with certain amenorrhoeic and dysmenorrhœic
conditions, and, in addition, the vomiting of pregnant women.
The vomiting of pregnant women, which must be regarded as a
reflex disturbance of the stomach, occurs, with especial severity in
first pregnancies, in the early months of pregnancy, with such
regularity that it is regarded as one of the most typical signs of pregnancy.
231Thus, in 177 pregnant women, Horwitz observed vomiting
in 147 (83 of whom were primiparæ, and 64 multiparæ), and in
29 only was this symptom wanting. In this series of cases, it most
commonly made its appearance between the tenth and eleventh week
of the pregnancy. The vomiting of pregnant women occurs most
commonly early in the morning, immediately after rising (morning
sickness), but also at other times of the day; it usually takes place
easily, without any great distress, and after it is over the patient
feels quite comfortable. It rarely continues later than the fourth
month of pregnancy.
Very serious in its effect on the general state of nutrition is the
uncontrollable vomiting that sometimes occurs in pregnant women
(hyperemesis gravidarum), lasting throughout the whole term of
pregnancy. It must be regarded as an exaggeration of the physiological
vomiting of pregnant women, in patients whose nervous
equilibrium is profoundly disturbed; but equally with the ordinary
“morning sickness” is it dependent on the reflex stimulation
of the nerves of the stomach exercised by the growing uterus. One
source of such stimulation may be found in the stretching of the
peritoneal investment of the uterus which results from the enlargement
of that organ; another, in certain displacements of the uterus;
but in addition to these local anomalies, we must assume the existence
of a peculiar predisposition on the part of the nervous system,
in virtue of which reflex irritability is increased, while the power of
reflex inhibition is diminished.
The prognosis and treatment of uterine dyspepsia depend chiefly
upon the nature of the diseases of the female genital organs that
have given rise to the disturbances of digestion, and this pathological
relationship demands above all a careful investigation. The following
instance from my own case-book may be regarded as typical
of cases of this class. Mrs. N., aged 25, married 6 years, barren,
complains of severe dyspeptic trouble. Appetite fairly good, but
after every meal severe gastralgia occurred, with heartburn and acid
eructations, and very often the food was rejected; there was also
obstinate constipation, and great distress from the accumulation of
flatus in the intestinal canal. No blood was ever seen in the vomit.
The patient was much emaciated, and was greatly depressed in
spirits. Neither in the lungs nor in the digestive organs had any
of the physicians under whose care the lady had been for the last
four years found any abnormal change to account for the stormy
manifestations. Now, at length, the gynecological examination,
which had hitherto been neglected, was undertaken. The uterus
was found to be strongly retroflexed and enlarged. Rectification of
the position of this organ was immediately followed by the disappearance
of all the stomach troubles; the vomiting ceased, some months
232later the woman became pregnant, and pregnancy and parturition
were quite normal; since then there has been no return of the
dyspepsia.
Since the appearance of my work on dyspepsia uterina, numerous
observations have in recent years been published, proving even more
clearly the causal dependence of disturbances of the gastric function
upon diseases of the female genital apparatus.
Lamy, for example, has made an elaborate study of one of the
above-mentioned symptoms of uterine dyspepsia, namely, excitement
of the vomiting centre. His conclusions are as follows:
Among the general symptoms of diseases of the uterus, dyspepsia,
in all its forms and in all degrees of intensity, occupies the first rank
in respect of frequency of occurrence. Among the accompaniments
of these reflex processes, uterine vomiting must be mentioned. It
seldom occurs as the sole symptom of disorder of the digestive
organs; but when it does occur alone, it is of great importance that
the cause of the affection should not be misunderstood. Diseases
of the uterus and periuterine affections are the conditions that most
commonly give rise to this trouble, but in a certain number of
cases it is due to physiological changes in the female genital organs.
Such changes are those associated with the functional activity of
the reproductive apparatus at the time of puberty, during menstruation,
in connection with coitus, during pregnancy, and at the change
of life, the menopause. The vomiting of pregnant women is of
the same nature, and confirms our belief in the uterine origin and
pathogenesis of vomiting at other times than during pregnancy. The
diagnosis of the true cause of uterine vomiting cannot be made
from the nature of the latter, but only from a knowledge of the conditions
in which it occurs, just as with other uterine reflexes, such
as neuralgia or cough. The vomit may consist merely of the food
last taken, or it may contain bile, without the presence of this latter
constituent indicating the existence of any disease of the liver. The
treatment of this disorder, which indeed does not threaten life, but
does seriously impair the general state of nutrition, must be local,
directed against the disease of the genital organs: Thus, in one
case of this nature, a cure was effected by oöphorectomy.
The majority of the women in whom Lamy observed this symptom
of uterine dyspepsia were chloro-anæmic individuals with an irritable
nervous system, town-dwellers, young girls in whom frequent
evening parties and dances, ill-chosen diet, and a generally
unsuitable mode of life, had led to the development of a
“virginal metritis.” The signs of the disturbance of the gastric
functions were in the first place a retardation of gastric digestion
while the appetite remained good. Moreover, the stomach was
233often distended with flatus, and this caused frequent gaseous eructations;
there was also epigastric pain, which made it difficult for
the patient to bear the pressure of the clothing, and sometimes
great pain was aroused by the slightest contact. The attacks of
vomiting, which occurred in a characteristic manner with periodical
intervals of freedom, were usually preceded for a longer or shorter
period by dyspeptic symptoms. The vomiting itself, if it occurred
immediately after a meal, was not accompanied by nausea, a feeling
of faintness, or cold sweats, but rather resembled a kind of painless
regurgitation; but when the vomiting did not occur till some
hours after food had been taken, it was painful, and the vomit was
then green-tinted owing to the admixture of bile.
The gastric troubles that occur during menstruation are regarded
by P. Müller as a further indication of the intimate connection between
the genital organs and the digestive tract. In women who
suffer from hysterical manifestations, gastric disturbances, cardialgia,
and nervous dyspepsia, are very frequently associated with menstruation.
These gastric symptoms generally make their appearance
a few days before menstruation is due, and disappear as soon as the
flow is established. In other forms, again, the digestive troubles
set in with the appearance of the flow, to disappear during the later
course of menstruation; and in yet other cases the gastric disturbance
begins even later, and ceases only when the flow comes to an
end. These symptoms may occur in women in whom the genital
organs are perfectly healthy and in whom menstruation runs a
regular course. More severe symptoms may, however, appear if
menstruation is disturbed for any reason, or if it is suppressed.
Not rarely such women, when they become pregnant, suffer, especially
during the early months, from dyspeptic symptoms; but
similar dyspepsia may occur in pregnant women who have previously
been quite healthy.
To the same category belong the cases formerly described by von
Leyden under the designation of neuralgia and hyperæsthesia of
the stomach, which he observed in young girls as a sequel of menstrual
disturbances, and more particularly of suppressio mensium.
In these circumstances, the sensibility of the stomach may become
so extreme that every time food is taken the patient suffers from
such severe pains, or from so distressing a sense of anxiety and
oppression, that she comes to eat less and less, and an extreme degree
of emaciation and marasmus results. In one such case, congenital
atrophy of the uterus was discovered on gynecological examination.
According to R. Arndt, it is especially in chloro-neurotic individuals
that the stimuli proceeding from morbid conditions of the
reproductive organs frequently induce, by reflex action, all kinds
234of disturbances of the alimentary tract, such as constipation and
flatulence, gastric uneasiness and loss of appetite, weakness of digestion,
cardialgia, and stricture of the œsophagus. Even simple
menstruation suffices to give numerous proofs of this fact, but still
more do such consequences arise from serious diseases of the reproductive
organs, such as changes in form, displacements, and inflammatory
states, and also, on the other hand, more or less pronounced
hypoplasia.
G. Braun has published three cases illustrating the connection
between neurosis of the stomach and uterine disorders. In the first
of these cases, severe digestive disturbances occurred after every
meal, with occasionally violent vomiting, in a woman, aged twenty-five
years. No changes were found in the stomach or other digestive
organs, and the symptoms obstinately resisted all direct treatment.
Gynecological examination showed extreme mobility of the uterus,
and for the relief of this a suitable pessary was introduced. The
vomiting thereupon immediately ceased, all the other digestive
troubles passed completely away, and the general state of nutrition,
which had before been so much impaired as to necessitate the use
of nutrient enemata of meat-solution, now became normal. The
second case was that of a woman aged thirty, who, since her last
confinement two years before, had continually suffered from disagreeable
gastric sensations and from vomiting, which latter had
proved quite uncontrollable. Gynecological examination disclosed
extensive laceration of the cervix with ectropium of the mucous
membrane. An operation was performed for the relief of this condition,
and the vomiting of two years standing was also thereby
cured. In the third case, that of a woman twenty-eight years old,
vomiting began three months after her confinement, and recurred
whenever the patient left the recumbent posture, in which latter
she felt quite well. On local examination, the uterus was found
to be prolapsed, the vaginal portion of the cervix moderately enlarged
and just within the vaginal orifice. Amputation of the vaginal
portion of the cervix cured the vomiting and completely restored
the patient’s health.
The frequency of gastric affections in cases of retroflexion of the
uterus is insisted on by Panecki. In eight instances he found neuroses
of the stomach consequent upon such retroflexion, and in all
cases a cure immediately followed rectification of the position of
the uterus. He urges that if after the reposition of the retroflexed
uterus the gastric troubles should still persist, a careful local examination
of the stomach is indispensable.
Eisenhart, in a woman forty-two years of age, corrected a mobile
retroflexion of the uterus, and thereupon very severe gastric symptoms
of several months’ duration soon disappeared. Graily-Hewitt,
235in an unmarried woman twenty-seven years of age, cured by reposition
of a retroflexed uterus a gastric disorder which had subsisted
for nine years; Elder and Henrik report identical results in gastric
troubles consequent on retroflexion or retroversion of the uterus.
Jaffé, in a virgin, aged twenty-three, who had been brought near
to death by gastric disorder with vomiting, found on local examination
that there was a profuse, thick, purulent discharge from the
interior of the uterus; curetting, and irrigation of the uterine cavity
with antiseptic solutions, gave immediate relief to the stomach
trouble. Similar experiences are recorded by C. van Tussenbeck and
Mendes de Leon in cases of gastric disorder consequent on endometritis
fungosa and endometritis interstitialis parenchymatosa;
and by Gottschalk, in cases consequent on sarcoma of the chorionic
villi. Lewy and Butler-Smythe have observed the relief of pernicious
vomiting by Emmet’s operation (trachelorraphy).
As regards the relations of gastro-intestinal affections to the
diseases of the reproductive organs, Theilhaber, in the cases observed
by himself, distinguishes three groups. In the first group
of cases, the gynecological abnormality was a chance accessory,
and was not the cause of the gastric trouble. In the second group,
he regards the gynecological trouble as dependent upon the affection
of the gastro-intestinal tract, believing that, in consequence of
atony of the intestine and an accumulation therein of fæces and
flatus, a retardation of the circulation occurs in the region of the
inferior vena cava, resulting in venous stasis in the uterus, and so
giving rise to metrorrhagia, dysmenorrhœa, and fluor albus. In
the third group of cases, Theilhaber believes that the uterine trouble
is the cause of the disturbances in the stomach and intestine. He,
like myself, has found in all these patients an inhibition of the intestinal
movements; but he found, on the other hand, that the gastric
secretions were more commonly normal, and that only in a small
proportion of the cases was the vomiting centre excited. Further,
in the majority of these women, the course of the digestive processes
was quite normal; and, finally, in his series of cases, endometritis
was one of the commonest causes of consecutive gastric disorders.
His observations led him to conclude that “in consequence of affections
of the uterus a large number of different symptom-complexes
of gastric trouble occur:” the pure nervous dyspepsia of
Leube, dependent on atony of the large intestine and atony of the
stomach, hyperchlorhydria and anacidity, periodic gastralgia without
anatomical cause, etc.
Cardiopathia Uterina.
I use the term cardiopathia uterina to denote the manifold cardiac
disorders which occur in women as reflex processes excited by the
236physiological functions and the pathological disorders of the genital
organs, and take the form of very various disturbances of the cardiac
function. Every phase of the sexual life of women—that in which
the reproductive organs attain complete development and menstruation
first appears (the menarche); the commencement of sexual
intercourse; pregnancy, parturition, and the puerperium; finally the
retrogressive process at the climacteric age, of which the menopause
is the outward manifestation—may give rise to the occurrence of
such cardiac troubles. In order to explain these troubles as reflex
in their nature, we must on the one hand recur to the anatomical
changes in the uterus and its annexa that take place in every one
of the above-mentioned phases of the sexual life; and on the other
hand we must take into consideration the mental processes that accompany
these anatomical changes, in order to estimate their influence
upon the motor and sensory nerves of the heart (see the sections
on the Menarche and the Menopause).
A certain predisposition to uterine cardiopathy exists in many
individuals and in many families. This predisposition may be manifested
in this way, that in women who at the time of the menarche
have suffered from cardiac disorder, similar cardiac disorder is likely
to recur at the time of the menopause, the symptoms of the recurrent
attack being in most cases identical with those that occurred
during the menarche. In the well-to-do and cultured circles of society,
uterine cardiopathy is far more frequently encountered than
among the working classes. Both unusually early and unusually
late commencement of menstruation tend to favor the occurrence of
uterine cardiopathy. The most valuable therapeutic measures that
we can employ to combat these disorders are suitable dietetic and
hygienic regulations, in association with favorable mental influences.
Diseases of the female reproductive organs, including simple
functional disturbances, are very frequently accompanied—far more
frequently than has hitherto been supposed—by cardiac disorders.
But whereas in some cases these cardiac disorders are directly dependent
upon the disease of the genital organs; in other cases no
such etiological relationship can be shown to exist, and the association
must, therefore, be regarded as fortuitous.
In cases of the former kind, the dependence of the cardiac disorder
upon the disease of the genital organs is very variable in its nature.
Reflex manifestations on the part of the nervous system may be
aroused by pathological changes in the genital organs, in a manner
similar to that discussed in other parts of this work in regard to
the cardiac troubles that are liable to occur during the menarche
and the menopause; such cardiac disorders are indeed excited especially
by changes in the ovaries, by disturbances of menstrual activity,
237by suppression of the menses—as manifestations, that is to
say, of the menstrual reflex. The cardiac disorder most commonly
takes the form of tachycardiac paroxysms, recurring periodically,
either in association with the menstrual flow, or, if this is in abeyance,
at the times at which it ought to appear. We must assume
in these cases that the local stimuli aroused by the pathological
changes in the uterus and the ovaries have a reflex influence upon
the cardiac nerves, by means of which the heart’s action is increased
in frequency, without inquiring more particularly whether the reflex
influence is effective by inhibiting the normal action of the vagus,
or by stimulating the sympathetic, or, perhaps, by a combination of
these factors. Much more rarely do we notice, in association with
disorders of the reproductive system, a reflex decrease in the frequency
of the heart’s action, this effect being explicable in the same
manner as the well-known experiment of Golz, in which, if the
abdomen of a frog be laid bare, and the intestine be struck sharply
with the handle of a scalpel, the heart will stand still in diastole with
all the phenomena of vagus inhibition.
In another group of diseases of the genital organs, the disturbances
of cardiac activity may be brought about by pressure which,
in consequence of the morbid processes in the reproductive organs,
is exercised upon individual nerves or upon an entire nerve plexus.
Tumefied and prolapsed ovaries, an enlarged and misplaced uterus,
inflammatory nodules and hyperplasias of the intrapelvic connective
tissue, contractile processes in the parametric connective tissue,[40]
tumors of the uterus whether intramural or in the interior of that
organ, ovarian tumors, prolapse of the uterus, and intrapelvic peritoneal
adhesions resulting from inflammatory processes—these are
the principal conditions liable to occasion reflex cardiac disorder;
but certain tissue changes, such as endometritis, erosions (chronic
cervical catarrh), and ulcerations of the genital passages, with or
without exposure of nerve-endings, are also competent to produce
the same effect. Here the sympathetic nervous system constitutes
the channel by means of which the stimuli affecting the nerves of
the genital organs are conveyed to the central nervous system, and
by means of which also the reflex manifestations of this stimulation
are produced, taking the form, partly of disorder of the cardiac
action, of palpitation of the heart and paroxysmal tachycardia, and
partly of pains in the cardiac region and disturbances along the
course of the great vessels.
Further, in cases of long-continued disease of the female genital
238organs associated with severe hæmorrhage and in some cases fluor
albus, nutrition in general and hæmotopoiesis may be seriously affected,
and disturbances of cardiac activity may result, as, for instance,
is frequently witnessed in chloro-anæmic states. In such
cases we have palpitation of the heart, both subjective and objective,
a weak and compressible pulse, often irregularity of the heart’s
action, singularly clear heart sounds, often, however, systolic murmurs
at various orifices, increased frequency of heart and respiration
to a disproportionate degree on slight exertion, strong pulsation
of the carotids, and slight œdema of the ankles.
Often, however, the disturbance of cardiac activity is dependent
also upon degenerative processes in the myocardium, upon fatty
degeneration and the consequent dilatation of the cavities, this degeneration
being a consequence of the growth of a uterine tumor
and especially of uterine myomata, or resulting from some constitutional
disorder which is itself dependent upon the affection of the
genital organs. In such cases the signs of degeneration of the
heart are very striking: weakening of the cardiac impulse, notable
faintness of the sounds of the heart, occasionally reduplication of the
second sound, a galloping rhythm, while percussion shows the existence
of considerable dilatation of the left, and still more frequently
of the right ventricle; in many cases also we have angina pectoris,
passive hyperæmia of the lungs, the mucous membranes, and the
extremities; and sudden death sometimes ensues.
No less important are the mental influences exercised by diseases
of the genital organs in which operation is proposed or actually performed,
also by long-lasting diseases of the reproductive organs and
by the disturbances these diseases produce in the reproductive functions,
more especially in relation to copulation and the actual process
of reproduction. In this way cardiac neuroses of various kinds may
be induced.
Finally, cases have come under my notice in which the cardiac
trouble was not the direct result of the disease of the genital organs,
but was a consequence of the therapeutic measures employed for
the relief of the latter; and in this connection I must regard as especially
blameworthy, in addition to intra-uterine manipulations, such
as sounding and cauterization, the modern practice of gynecological
massage.
Not all diseases, however, of the female reproductive apparatus,
tend in a similar manner and with equal frequency to give rise to
consecutive cardiac disorders. According to my own observations,
the diseases of the vulva and the vagina, catarrhal inflammation,
colpitis (vaginitis), leucorrhœa, and prolapse of the vagina
(cystocele and rectocele), are those which most rarely induce cardiopathy;
239unless, indeed, the diseases just enumerated have led to the
occurrence of vaginismus, for in this latter condition cardiac trouble
not uncommonly ensues. More commonly than by vulval and vaginal
diseases, cardiac troubles are induced by inflammation of the
uterine mucous membrane, as by chronic endometritis, by erosion
and “ulceration” of the cervix (chronic cervical catarrh); they
also sometimes occur in connection with perimetritic and parametritic
exudations. Most frequently of all, and most severely, cardiac disorders
are aroused by displacements of the uterus, flexions or
versions; by structural changes of the uterus accompanied by enlargement
of that organ, such as chronic metritis and the growth of
myomata (especially intramural); by prolapse, enlargement, and
tumor of the ovary; by intrapelvic exudations which when extensive
give rise to displacement or compression of the uterus or its annexa.
In cases of carcinomatous or other malignant new growths affecting
the reproductive organs, I have in comparison very rarely
observed the occurrence of reflex cardiac disorders.
Disturbances of menstrual activity, amenorrhœa, menorrhagia, and
dysmenorrhœa, owning the most varied causes, very frequently give
rise to cardiac trouble, a point on which we have already insisted.
(See page 142, et seq.)
Very violent forms of cardiac neurosis have been observed by
me in women suffering from chronic disorder of the reproductive
organs, who have consulted one gynecologist after another and have
been subjected to many different methods of local treatment; also
in women who have for a long time suffered from some gynecological
ailment hitherto believed to be trifling, but who have at length suddenly
been informed that some severe operative procedure has become
necessary. In such cases the cardiac trouble took a paroxysmal
form, the intervals being usually considerable, several weeks or
months in duration, and the general system was as a rule seriously
involved in the attacks. These latter began with severe cardialgia,
radiating from the cardiac region outward along the intercostal
spaces, upward to the shoulder and along the left arm, sometimes
indeed extending into both arms. At the same time the heart’s
action was greatly increased in frequency, there being sometimes
more than 200 beats per minute, the pulse was soft, small, difficult
to count, the respiration greatly increased in frequency, sometimes
very shallow, with respiratory anxiety, and exceptionally severe
general excitement and sense of impending death. In some cases
also I observed spasm of various groups of muscles, dizziness (with
a sense that the objects of vision were flickering), aphasia, and
mental stupor. The paroxysms lasted for some time, two or three
hours, as a rule, and gradually passed away. Their character was
240that of the cardiac disorder variously described under the names
of pseudo-angina and angina pectoris hysteria.
Such attacks as these are followed by a sense of severe general
depression and want of energy, and by a decline in body-weight.
They are distinguished from true angina pectoris by the absence of
any signs of arteriosclerosis or of degeneration of the myocardium.
They may be regarded as cardiac disorder of duplex causation, being
partly dependent on the disease of the genital organs, which gives
rise to a number of local afferent stimuli, and partly dependent on
mental influences which have a depressant, paralyzing influence on
the cardiac nerves; it is possible also that spasmodic contraction of
the walls of the coronary arteries or of the myocardium itself is
induced as a reflex effect of the local disorder of the reproductive
organs.
With regard to uterine myoma as the exciting cause of cardiac
degeneration, very numerous observations and experiments have
recently been made, and the reality of the occurrence is no longer
open to dispute, even if its significance is subject to various interpretations,
whilst no satisfactory explanation has yet been forthcoming.
L. Landau writes concerning the disturbances induced in the
circulatory apparatus by the growth of myomata in the uterus:
“The formation of varices, the occurrence of thrombosis, and,
finally, the onset of degeneration of the myocardium, are very common.
Should the last-named process result—and it is truly alarming
to observe the frequency with which cardiac affections are associated
with uterine myomata,—then, by a vicious circle, the
uterine hæmorrhages become continually more profuse, in consequence
of increasing passive hyperæmia dependent upon diminishing
power of the cardiac pump. Venous congestion in the province of
the inferior vena cava results in ascites, and sometimes in general
œdema; and even in cases in which no increase of the uterine hæmorrhages
is observed, the patient may succumb in consequence of secondary
disease of the heart. * * * In the great majority of
cases, the myoma and the uterine hæmorrhages that result from its
growth are the primary cause of the morbus cordis. Naturally in
cases which come under observation only when both uterine and
cardiac disease are already present, it is difficult to determine with
certainty the true causal connection. When, however, a number of
patients suffering from uterine myomata are observed, in whom at
first the heart was found to be healthy, and subsequently to have
become affected; and when, on the other hand, we see patients affected
with myoma uteri in whom operation is undertaken notwithstanding
the existence of cardiac disease, and in whom, after the
241operation has been successfully performed, the cardiac murmurs
disappear as well also as the other signs of heart disease, when dilatation
can no longer be detected, when the pulse-frequency declines
to normal, whilst a previously feeble and compressible pulse gains
in tension and power—then it is impossible to doubt that the heart
disease was secondary, and was etiologically dependent upon the
primary myoma and the uterine hæmorrhages.”
Lehmann and P. Strassmann examined the material of the Charité-Policlinik
at Berlin in order to throw light on the relation between
uterine myomata and diseases of the heart, a connection already
proved to exist alike by recent pathologico-anatomical researches,
by clinical experience of the results of operations (death from
shock), and, finally, by the subjective troubles of the patients (palpitation,
venous congestion, giddiness, and syncope). Examining 71
women suffering from myoma uteri, Lehmann and Strassmann found
in 29 (41%) that some abnormality existed in the cardio-vascular
system, such abnormalities being extremely variable in character,
as for instance: hypertrophy or dilatation of the heart, irregularity
of the cardiac action, passive hyperaemias, œdema, albuminuria, angina
pectoris, and cardiac asthma. The next point was to determine
the mutual relations between the heart disease and the development
of the uterine myoma. Hitherto it has been assumed that the latter
is the primary disease, and such a sequence is certainly the commoner,
more especially in cases in which hæmorrhage has been profuse, with
consecutive anæmia and fatty degeneration of the heart. In these
cases, a certain time after the commencement of the severe hæmorrhages,
cardiac troubles make their appearance; such troubles are
beyond question secondary, and they disappear as soon as the
hæmorrhage has been controlled. In other patients, however, we
obtain a history of the appearance of cardiac disorder at a date prior
to that when any symptoms occurred indicating the growth of a
myoma; in these cases, therefore, the heart disease has developed independently
of the uterine disease, and has run a parallel course to
the latter; perhaps, indeed, by leading to venous congestion or to
rapid changes in blood-pressure, the heart disease may have favored
the growth of the commencing or fully developed tumor. In some
of the patients, operative measures were followed by rapid recovery
from the cardiac disorder (cases of simple anæmia); in a second
group of cases, however, the heart disease was uninfluenced by
operation (cases of irreparable anæmia, and cases of heart disease
independent of the myomata); and, finally, a considerable number
of patients remained, constituting a third group, in whom, notwithstanding
the removal of the tumor by operation, the heart disease
continued to grow worse (cases of progressive heart disease independent
of the myomata, especially cases of arteriosclerosis).
242Among 120 women of ages between 17 and 48, in whom I found
very various functional disorders of or pathological changes in the
genital organs, and in whom I made a particular investigation concerning
the presence or absence of heart disease and examined the
heart carefully, I was able to detect the presence of cardiac troubles
in 38 instances. Thus, heart trouble was found to exist in 32.7 per
cent. of women suffering from disease of the reproductive organs.
In these 38 persons suffering from cardiac disorder, I found:
| Nervous Tachycardia in 21 instances, that is, in about |
55.2 per cent. of the cases. |
| Hypertrophy of the Heart in 4 instances, that is, in about |
10.4 per cent. of the cases. |
| Pseudo-Angina Pectoris in 3 instances, that is, in about |
7.8 per cent. of the cases. |
| Asthenia Cordis in 7 instances, that is, in about |
18.4 per cent. of the cases. |
| Mitral Incompetence in 1 instance, that is, in about |
2.6 per cent. of the cases. |
| Fatty Heart in 2 instances, that is, in about |
5.2 per cent. of the cases. |
As regards the varieties of functional and organic disease of the
genitals met with in the 120 cases, and the number of instances complicated
with heart trouble in each variety, I found:
| Chronic Metritis in 32 patients, complicated with cardiac disorder in |
13 instances. |
| Chronic Oöphoritis in 10 patients, complicated with cardiac disorder in |
4 instances. |
| Parametric Exudations in 14 patients, complicated with cardiac disorder in |
6 instances. |
| Chronic Endometritis in 16 patients, complicated with cardiac disorder in |
2 instances. |
| Flexions and Versions of the Uterus in 26 patients, complicated with cardiac disorder in |
9 instances. |
| Stenosis of the Cervix in 6 patients, complicated with cardiac disorder in |
0 instances. |
| Tumors of the Uterus and its Annexa in 8 patients, complicated with cardiac disorder in |
4 instances. |
| Infantile Uterus in 3 patients, complicated with cardiac disorder in |
0 instances. |
| Colpitis (Vaginitis) in 5 patients, complicated with cardiac disorder in |
0 instances. |
From these figures we obtain the following percentages, showing
the frequency with which heart trouble occurred as a complication
of the respective diseases of the genital organs:
| In Chronic Metritis, cardiac disorder was found in |
40.6 per cent. of the cases. |
| In Chronic Oöphoritis, cardiac disorder was found in |
40 per cent. of the cases. |
| In Parametric Exudations, cardiac disorder was found in |
42.8 per cent. of the cases. |
| In Chronic Endometritis, cardiac disorder was found in |
12.5 per cent. of the cases. |
| In Versions and Flexions of the Uterus, cardiac disorder was found in |
34.6 per cent. of the cases. |
| In Tumors of the Uterus and its Annexa, cardiac disorder was found in |
50 per cent. of the cases. |
243To summarize the result of my observations regarding the cardiac
disorders secondary to diseases of the female genital organs:
1. Tachycardial paroxysms in cases of amenorrhœa were premenstrual
in rhythm, the paroxysms occurred, that is to say, some
days before the due date of the suppressed flow.
2. In cases of dysmenorrhœa, I observed heart trouble with severe
dyspnœa and feelings of anxiety, also in some cases symptoms of
cardiac asthenia; these symptoms were perhaps dependent upon
acute dilatation of the heart. The heart trouble associated with profuse
menorrhagia exhibited similar characters.
3. Attacks of pseudo-angina pectoris occurred in women in whom
local treatment for disease of the genital organs had been carried
out for a long time, and in cases in which operative measures were
in contemplation.
4. Paroxysms of tachycardia and cardiac distress were observed
in connexion with displacements of the uterus, and especially in
cases of retroflexion; also in association with oöphoritis and with
parametric exudations.
5. Cases of degeneration of the myocardium, sometimes running a
rapidly fatal course, were found to be consecutive to tumors of the
uterus and its annexa, especially to myomata of the uterus.
Nervous Diseases Secondary to Diseases of the Genital Organs.
In earlier chapters of this work we have frequently referred to
the reflex influence exercised upon the nervous system in general,
alike by the normal functions and the pathological states of the
female genital organs. We must now briefly explain the more intimate
connection between nervous diseases and diseases of the genital
organs, the causal dependence of local nervous disturbances and of
general neuroses upon diseases of the reproductive organs.
The origination of a local nervous disease by a primary disease of
the genital organs is dependent upon a simple mechanical process,
which is explained by Windscheid in the following terms: “In this
connection, the two principal mechanical factors are pressure and
traction. Pressure may affect individual nerves or an entire nerve
plexus, and may be exercised by a tumour, an exudation or a misplaced
organ (Hegar); further causes of pressure are furnished by
inflammatory nodules, by connective tissue hyperplasias, and, according
to Freund, by contractile processes in the organs themselves
and in the ligaments. Traction on the nerves results from
displacements, as from prolapse of the uterus or the ovaries, and,
according to Hegar, from traction on the pedicle of small tumours.
A combination of pressure and traction occurs especially in affections
244of the abdominal attachments of the uterus, also where there is
scarring of the neck of the uterus and of the vaginal fornices.
Great importance, also, in relation to the production of local nervous
disorders, must be attributed to the laying bare of nerve-terminals
by catarrhal and other inflammatory processes. Abnormal mobility
of the genital organs as a partial manifestation of enteroptosis
must also be mentioned as a cause of mechanical stimulation of the
nerves. Finally, in this connection, must be considered the paresis
of the abdominal walls that follows frequent and severe confinements.”
The symptoms of the local nervous disorders to which these
mechanical stimuli may give rise, are very various, but may, according
to Hegar, be comprised under the general designation of
lumbar enlargement symptoms (Lendenmarksymptome), inasmuch
as the local stimulation of the intrapelvic nerves, affects the nerve-centres
of the lumbar enlargement of the spinal cord. Among the
symptoms, severe pains are prominent, either continuous or intermittent,
within the pelvis and in the sacral region, accompanied
by a sense of weight and pressure in the abdomen, or by dragging
pain in the region of the hips, in the gluteal region, in the outer
and back parts of the thighs, in the inner surface of the leg, in the
calf, in the dorsum of the foot, the sole of the foot, and the heel; or
by coccydynia (pain over the coccyx and the lower extremity of the
sacrum), or hyperæsthesia and anæsthesia of the external genitals in
the region of the vaginal orifice, or, finally, by disorder of the processes
of micturition and defæcation. In some of these cases, the
weakness of the lower extremities is so severe that a paralytic condition
is simulated. Actual paralysis may however occur, in consequence
of the extension of peritoneal inflammation to the nerve-plexuses
of the pelvis, leading to the occurrence of neuritis.
The development of a general neurosis in consequence of disease
of the genital organs, either as a complication dependent upon the
nervous stimulation excited by the primary disease, or as a reflex
consequence of this disease, implies, as Windscheid strongly maintains,
the existence prior to the occurrence of the disease of the
genital organs of diminished power of resistance on the part of
the nervous system. This neuropathic constitution may be the result
of inheritance, and, according to Engelhardt, was so in 40 per
cent. of his cases of women suffering from nervous disease secondary
to the disease of the genital organs; or it may be acquired.
Given this weakness of the nervous system, a local disturbance of the
genital organs may act as the ultimate exciting cause of the onset
of the neurosis in one of two different ways (Windscheid). “1. The
stimulus which the nerves of the affected genital organ (or those
245of some adjacent area, affected by direct extension) have received,
proceeds upward from segment to segment of the spinal cord, and
ultimately passes to the highest centres. 2. Or, on the other hand,
the local nerves are not directly involved in the morbid process in
the genital organs, but this latter acts as a source of reflex disturbance,
a disturbance which must also pass through nervous channels.
To this latter class of cases belong the instances, comparatively so
frequent, in which, for example, a trifling retroflexion of the uterus
must be regarded as the exciting cause of the neurosis.” The commonest
neurosis of those that may be excited by local disease of the
genital organs is undoubtedly hysteria, next in frequency come
chorea and epileptic seizures.
Schauta draws attention to the important fact that hereditarily
predisposed, neurasthenic individuals bear very badly repeated
gynecological examinations and long-continued local treatment, inasmuch
as, in such persons, a notable increase in the severity of the
nervous affection may result, and even the outbreak of actual mental
disorder; and he further points out that in hereditarily predisposed
individuals, psychoses not infrequently occur in consequence of the
performance of gynecological operations.
The processes of pregnancy make a deep impression on woman’s
entire nervous system, and more especially on her mental functions.
This is especially noticeable in the case of primiparæ. The fact is
easily understood, for a woman is filled with expectation and anxiety
concerning the unknown event, the complete revolution in her
organization, the powerful impressions on her physical ego, the
formation of a new being within her womb. How many joyful
hopes, how many distressing fears, are connected with that which
is about to take place, with the act of creation within her bosom;
what changeful glimpses into the future, on the one hand the gladness,
on the other the terror, of motherhood; often, also, the anxious
doubts as to the probable sex of the newcomer. Consider, too, the
stormy sensations experienced by a woman who, unmarried, has
become pregnant contrary to her desires and expectations, especially
one in a poverty-stricken condition—consider the agonizing
thoughts in such a case regarding the consequences of giving birth
to a child. It is only to be expected that in pregnant women in
general there will almost always be increased irritability of the
nervous system combined with a tendency to the rapid variation
of emotional states. Neumann found, in almost all the pregnant
women he examined in respect to the point, that there was an increase
of the knee-jerks, as a manifestation of the general increase
of nervous irritability. Nor does this change depend upon mental
influences exclusively; there are other factors, such as the reflex
246processes aroused by the enlargement of the uterus, and also the
changes in the composition of the blood which occur during pregnancy,
and cannot fail to have an influence on the nutrition of the
brain. Finally, also, the deposit of carbonate of lime on the inner
surfaces of the cranial bones (the parietal and frontal bones)
which occurs during pregnancy, may be regarded as having some
casual connection with the changes in the nervous system; and,
again many authors assume that the cerebral circulation is influenced
by the formation of the placental circulation.
The pathological consequences of pregnancy, as far as they affect
the nervous system, take the form of neuralgia and of peripheral
neuritis of various nerves, of chorea, of disturbances of the sense
organs, and of actual psychoses.
Peripheral neuritis in pregnant women affects chiefly the lower
extremities, but has been observed in the arms also; it is characterized
by muscular wasting with reaction of degeneration, by
trophic disturbances, and by disorders of sensation. A cure may
ensue even during the pregnancy, but in other cases the illness persists
until after parturition and on into the puerperium. To the same
cause Windscheid assigns the paræsthesias of pregnancy, burning,
prickling, and numb sensations of the finger-tips, less commonly
of the toe-tips; these sensations are continuous, not paroxysmal, and
cause very great suffering.
Pregnancy favors the occurrence of chorea, a circumstance explicable
by the increased irritability of certain nerve centres characteristic
of the pregnant woman. The chorea of pregnancy occurs
for the most part in primiparæ, it is commoner in young than in
older pregnant women, and appears especially in the early months
of pregnancy. In the majority of cases the disease undergoes
spontaneous cure before the end of the pregnancy, but cases with
a fatal termination have been observed.
On the other hand, a curative influence in previously subsisting
hysteria has been assigned to pregnancy. This in fact only occurs
in cases in which the hysterical manifestations have been evoked
by influences which are counteracted or removed by the occurrence
of pregnancy, such, for instance, as intense longing to bear a child,
dissatisfaction with the existing circumstances of married life, etc.
Conversely, it is by no means unusual to observe that, in patients
who have previously suffered from hysteria, the attacks become more
frequent during pregnancy, and that other nervous disturbances associated
with the hysteria become more prominent; hysterical paralysis,
even, may appear. Very variable also is the influence of
pregnancy in epileptics. Most commonly, indeed, a certain quiescence
sets in, the attacks becoming less frequent and less severe;
247but the reverse of this is at times observed. In the domain of
the sense organs we observe amblyopia and hemianopia, deafness,
and tinnitus aurium, and disorders of taste; all these appear as pure
nervous disturbances without known anatomical basis (Windscheid).
Finally, among neuroses, tetany may be mentioned. In women,
this disease occurs almost exclusively during pregnancy and the
puerperal state, in the form of paroxysmal spasm, affecting chiefly
the extremities, and especially the hands; the spasm is bilateral,
tonic in character, and painful. The tetany of pregnancy usually
runs a favourable course.
The slighter forms of mental disorder consist of perversions of
taste and smell. Of actual psychoses occurring during pregnancy,
the commonest forms are melancholia and mania. The former condition,
which, according to Ripping, occurs in 84.4 per cent. of the
cases, is usually very severe, and is characterized by a peculiar
dreamy condition; it often leads to suicide, or to infanticide immediately
after parturition. The psychoses of pregnancy are seen
with greater frequency in the second half of pregnancy, they occur
especially in primiparæ, and are also commoner in unmarried women.
The prognosis is on the whole an unfavorable one; sometimes, indeed,
the mental disorder terminates with the pregnancy, but in
other cases it continues during the puerperium. Mental alienation
occurring in the early months of pregnancy is apt to be less severe
and to permit of a more favorable prognosis, than that which makes
its appearance during the later months or at the end of the pregnancy.
In 32 cases of insanity of pregnancy recorded by Ripping, 8 cases
occurred in the first pregnancy, 5 in the second, 6 in the third, 3 in
the fourth, 4 in the fifth, 1 in the sixth, 1 in the seventh, 3 in the
eighth, 1 in the tenth. Of these women
3 became affected in the 1st month
[41] of pregnancy.
4 became affected in the 2d month of pregnancy.
1 became affected in the 3d month of pregnancy.
2 became affected in the 4th month of pregnancy.
1 became affected in the 5th month of pregnancy.
0 became affected in the 6th month of pregnancy.
5 became affected in the 7th month of pregnancy.
5 became affected in the 8th month of pregnancy.
5 became affected in the 9th month of pregnancy.
6 became affected in the 10th month of pregnancy.
The neuralgias of pregnancy affect the most diverse nerve tracts,
and may occur either spontaneously, without any discernible local
exciting cause, or in consequence of the pressure exercised by the
248enlarging uterus. To the former class of cases belong severe trigeminal
neuralgia, the familiar toothache affecting quite sound
teeth at the very beginning of pregnancy, intercostal neuralgia, and
paroxysms of mastodynia. The pressure neuralgias affect chiefly
the domain of the great sciatic nerve, manifesting themselves by
the occurrence of pain down the back of the thigh, in the calf, and
on the dorsum of the foot, sometimes associated with formication
and other kinds of paræsthesia.
Parturition, by its powerful effect on the emotional nature in
combination with intense physical suffering, may give rise to numerous
nervous disturbances. The chief of these are, neuralgia, occasioned
by the pressure of the fœtal head as it passes through the
pelvis of the mother, paræsthesias, convulsions, maniacal paroxysms,
transitory mental alienation, cerebral hæmorrhages, and eclampsia.
The nervous disturbances dependent upon the processes of the
puerperium are numerous and severe. According to Windscheid,
four types of affection of the motor nerves may arise at this period.
1. Pressure-paralysis may occur in cases of generally contracted
pelvis, or even in the absence of such contraction in cases of prolonged
labor, from the pressure exercised by the child’s head upon the
intrapelvic nerves, and above all on the great sciatic nerve; pressure-paralysis
may also result from obstetric operations, and especially
from forceps delivery. The symptoms of pressure-paralysis consist
chiefly of paralysis of the extensors of the feet and the toes; sensory
symptoms are usually wanting. 2. Inflammatory infective paralyses,
due to the extension to adjacent nerves of puerperal inflammation of
the pelvic connective tissue. 3. Acute multiple neuritis, occurring
either during the latter half of pregnancy or a few days after delivery,
and affecting not only the nerves of the lower extremities, but
those of remote regions, even the cranial nerves. 4. The rare puerperal
hemiplegia due to cerebral hæmorrhage, occurring usually
at the time the patient leaves her bed after delivery; puerperal
hemiplegia may also arise from embolism consecutive to endocarditis,
which may itself have originated before the termination of the
pregnancy.
Other puerperal diseases of the nervous system requiring mention
are, on the one hand, tetany, occurring during lactation, and permitting
of a favorable prognosis, and on the other, the infective
puerperal tetanus, the prognosis of which is exceedingly unfavorable.
Finally, the puerperal state has to be considered as a factor in determining
the onset of psychoses.
The puerperal psychoses are for the most part dependent upon
the great loss of blood occurring during delivery, leading to anæmia
and increased irritability of the brain, in association also with the
249circulatory disturbances that arise in the central nervous organs
in consequence of the sudden emptying of the abdomen by the
act of childbirth; but additional causes of mental disorders are to be
found in the changes in the composition of the blood that occur during
pregnancy, and the influence of these changes upon the nutrition
of the brain. Inherited predisposition plays its usual part in these
cases; and accessory factors in producing mental disturbance during
the puerperal state are to be found in puerperal infection, eclampsia,
osteomalacia, and emotional shock.
Thus, for example, among 49 cases of puerperal psychoses, Hansen
found that in 42 instances there was puerperal infection; and
among 200 cases of puerperal eclampsia, Olshausen found 11 patients
suffering from mental disorder. The principal forms of insanity
occurring at the puerperium are mania and melancholia, next in
frequency come monomania (Ger. Verrücktheit), dementia (Ger.
Blödsinn), alternating or circular insanity (folie circulaire),
hallucinatory paranoia (chronic delusional insanity with hallucinations),
and hysterical mental disorder.
According to Windscheid, the commonest cases are those which are
purely puerperal, the rarest those in which the insanity of pregnancy
continues during the puerperal state; the age at which puerperal
psychoses most commonly occur varies between 31 and 35 years, the
average age being 29.1; multiparæ are more often affected than
primiparæ; the outbreak of mental disorder most commonly occurs
within a week after the birth of the child; there is nothing specific
about the various forms of puerperal insanity, which are identical
with the respective varieties owning another etiology. According
to this author, before an attack of puerperal mania, prodromal
symptoms usually occur, such as headache, dizziness (Ger. Augenflimmern),
feelings of anxiety, insomnia, followed by various congestive
symptoms, and either by great restlessness or by great
apathy, and very often by indifference to the infant; to these symptoms
succeeds the period of motor excitability, characterized by
great bodily restlessness and by continued talkativeness; the culmination
takes the form of a maniacal outburst, in which infanticide
even may occur; the delirium runs mostly in erotic and religious
channels. Puerperal melancholia also exhibits the usual clinical
picture of this form of mental disorder; after prodromal headache,
stupor sets in, often associated with attacks of anxiety and with
hallucinations of sense, and always characterized by great loss of
appetite and by a suicidal tendency.
In relation to the puerperal psychoses, it appears that the first
menstruation after the birth of the child has, like the very first
appearance of the menstrual flow during the menarche, a tendency
250to favor the onset of mental disorder. According to Marcé, this
first post-puerperal menstruation has a very definite significance in
the causation of psychoses. Among forty-four cases of puerperal
psychoses, there were eleven instances in which the mental disorder
made its appearance six weeks after childbirth, exactly at the
moment, that is to say, in which, had the mothers not given suck to
their children, menstruation ought to have reappeared. In those
who did not nurse their infants, and in whom menstruation recommenced
at the due date, the psychosis usually began on the first day
of menstruation, less often on the fourth or fifth day. In some
instances the psychosis appeared at the time at which menstruation
might have been expected to occur, but when the flow was still
in abeyance. And in some women who suckled their children for
a time and then weaned them, the psychosis made its appearance at
the time of the first recurrence of menstruation.
Among diseases of the sense-organs occurring during the menacme,
ocular lesions are by no means rare as sequels of pathological
changes in the genital organs. Thus, in cases of displacements of
the uterus, especially prolapse, retroflexion, and retroversion, we
sometimes see retinal hyperæsthesia and reflex amblyopia, photophobia
and lachrymation, and accommodative or muscular
asthenopia. Inflammation of the pelvic connective tissue, perimetritic
and parametritic exudations, and especially parametritis
atrophicans, may give rise to functional disorders of the eye, reflex
hyperæmia of the trigeminal and optic nerves, various painful sensations,
and photophobia. Severe metrorrhagia may also cause disturbances
of vision, either by inducing local anæmia and consequent
functional failure of the nervous apparatus, or by leading to serious
infiltration of the optic nerve which manifests itself also in the
retina in the form of a transudation. In cases alike of congenital
and of acquired atrophy of the uterus, and frequently, therefore, in
sterile women, optic nerve atrophy may occur.
Competence for Marriage of Women Suffering from Disease.
In this section we must consider the competence for marriage of
women suffering from heart disease, of those suffering from hereditary
tendency to mental disorders and neurasthenic states, and,
finally, of those affected with tuberculosis.
Every doctor is confronted during the practice of his profession
by the problem whether a young woman known to suffer from heart
disease is justified in entering upon marriage and in exposing herself
to the dangers entailed on her diseased heart by copulation,
pregnancy, parturition, and the puerperium. The solution of this
problem is as important as it is difficult. On the one hand, it determines
251the whole future course of a human life which is still
ascending the upward path of its vital career, and a negative decision
often annuls in a moment the young woman’s ideals and
hopes; on the other hand, an affirmative decision involves the responsibility
for the consequences of marriage, often grave in these
cases.
The consequences are in fact apt to be very serious indeed. The
normal act of intercourse, in a young and sensitive woman, has
already an exciting influence on the nerve apparatus by which the
movements of the heart are controlled. The frequency of the
heart’s action is greatly increased, the cardiac impulse becomes much
stronger, there is marked pulsation of the peripheral arteries, the
conjunctiva is injected, the respiration more frequent. These manifestations,
which normally are quite transient, attain a greater intensity
and exhibit a longer duration in persons affected with heart
disease. In some instances, violent tachycardial paroxysms occur,
with considerable dyspnœa, pains in the cardiac region, headache,
and even syncopal attacks.
Pregnancy, in consequence of the extensive changes undergone not
only by the reproductive apparatus but also by the general system, and
further in consequence of the vital needs of the developing embryo,
involves extensive claims upon the cardiac activity. It is easy to
understand that the diseased heart must be taxed more severely
than the healthy heart by the extension of existing vascular areas,
the addition of new vascular areas, and the increase in the quantity
of the blood, during pregnancy; and it is not surprising if the overtaxed
organ threatens sometimes to give way under the strain.
Thus, during pregnancy in women affected with morbus cordis, we
observe numerous troubles in the way of disturbances of cardiac
activity and passive congestion of various organs, culminating at
times in abortion.
Parturition and the puerperium, moreover, bring several factors
into play which tend to affect unfavorably even a heart that is quite
normal; and in cases in which there is disease either of the heart or
of the great vessels, these factors may lead to the occurrence of most
alarming symptoms. In this connection we may refer to endocarditis,
to fatty degeneration of the myocardium, and to the rupture
of atheromatous arteries.
From the time of Galen onwards all medical writers have agreed
that the heart is unfavorably influenced by pregnancy and its consequences—but
from this incontestable proposition to deduce the
general conclusion that young women affected with heart disease
must be forbidden to marry is in my opinion too great a jump, and
altogether too sweeping a statement. The apophthegm of Peters, an
252author to whom we are certainly indebted for some of our knowledge
of the accidents gravido-cardiaques, that in the case of women
suffering from morbus cordis the rule must be enforced, fille pas de
mariage, femme pas de grossesse, mère pas d’allaitement, has a fine
air of apodictic brevity, but is entirely devoid of justification. No
such rigid prohibition is advanced by recent writers on heart disease,
such as Huchard, von Leyden, and Rosenbach; not, at least, without
qualifications.
The question as to the permissibility of marriage to girls and
women affected with heart disease cannot, in fact, be answered
by any general proposition; and each case demands separate inquiry
and a careful balancing of individual considerations. I have known
cases in which the marriage of young girls suffering from morbus
cordis was equivalent to a sentence of death, the execution of which
was delayed for a few months only. On the other hand, I have known
many women belonging to the upper classes and suffering from cardiac
defects to pass through numerous pregnancies and to give birth
to a number of children with no more than trifling disturbances of
compensation. I am acquainted with a lady who when a young
girl was urgently advised against marriage, on account of extensive
aortic valvular incompetency, by two celebrated physicians. The
advice was disregarded, and this lady is now the mother of four
children, the eldest of whom is twenty-two years of age, and her
general condition is in no way worse than it was before her marriage.
The dangers of marriage in women suffering from morbus
cordis are in my opinion generally overrated.
The degree to which a woman affected with heart disease will be
injured by married life, will depend on the nature of the cardiac
affection, on the time it has already existed, on the adequacy of
compensation or the intensity of existing disturbances of compensation,
on the general state of nutrition of the patient, on the more or
less favorable social position, and on the manner in which sexual intercourse
is regulated.
My own opinions in respect of this question may be summed up
as follows: A woman who has comparatively recently (within a
few years) acquired a valvular defect, and in whom the disease has
run such a course that, in consequence of dilatation of certain
chambers of the heart and of hypertrophy of those segments of the
myocardium on which increased work has been thrown, and thus
in consequence of adaptation of the cardio-vascular apparatus to
the new conditions, the circulation and distribution of the blood
take place in a manner closely resembling that in which these functions
are effected in a normal, healthy individual—in a word, a
woman in whom the valvular disease appears to be adequately compensated,—if,
253in addition, the patient is well nourished, if the
hæmatopoietic function has not undergone any notable disturbance,
if the muscular system is powerful and the nervous system possesses
sufficient power of resistance—then marriage may be permitted
without hesitation. In the case of such a girl or woman, we can
confidently assume that the adequate compensation of the valvular
disease will enable the heart to meet with success the claims made
upon its reserve energies by sexual intercourse, by pregnancy, and
by parturition, and that these processes will not involve any excessive
danger to life.
A woman with valvular heart disease, even when that disease is
well compensated, will indeed during pregnancy and still more during
parturition and the early days of the puerperium, be liable to
suffer from various manifestations of cardiac disorder. The action
of her heart will be subject to paroxysmal increase in frequency and
force, sometimes also there may be transient attacks of cardiac
asthenia; at the same time the breathing will become more frequent
and deeper, and occasionally, even, there may be severe dyspnœa.
Perhaps also symptoms of venous congestion may manifest themselves,
digestive disturbances, sense of pressure in the head, swelling
of the feet, œdema of the abdominal wall, even slight albuminuria.
Just after childbirth, moreover, an abnormally intense depression of
the circulation with infrequency of the heart’s action will be liable to
ensue. In the great majority of cases, however, in which the conditions
detailed above are fulfilled, the disturbances of compensation
occasioned by pregnancy and the puerperal state will not seriously
threaten life; and as soon as the puerperal period has been safely
passed through, the heart will again be competent for its duties and
will do its work as well as before.
These statements apply, not only to cases of well-compensated
valvular disease, especially mitral insufficiency, mitral stenosis, and
aortic insufficiency, but also to cases in which the heart has made a
good recovery after an attack of pericarditis, and to cases of moderately
extensive disease of the myocardium consequent on acute
articular rheumatism or the acute infections.
As indispensable conditions for such a favorable prognosis, we
naturally assume that the pregnant woman is in a position to command
the extreme bodily care that in her condition is doubly needful,
that she is able to avoid all severe physical exertion, and that
she will be subjected to continuous medical supervision in respect of
the adoption of suitable dietetic and hygienic measures.
Such a favorable prospect as regards marriage in cases of well-compensated
heart disease will, however, be clouded in the case of
women who are either very anæmic or predisposed to nervous disorders;
nor is the prognosis favorable as regards women in whom
the heart disease is either congenital, or acquired in early youth, or
254as regards women contemplating marriage when already well up in
years.
For in very anæmic women, even when the heart is quite sound,
frequently recurring attacks of tachycardia often occur during pregnancy,
in the absence of any obvious exciting cause; œdema of the
lower extremities, and the formation of extensive varices, are also
common. Increased nervous reflex irritability has also an unfavorable
influence upon cardiac innervation. In cases, again, in which
the heart disease is of long standing, the functional capacity of the
heart is so notably depressed that the organ is likely to prove incompetent
to meet the increased demands made upon it by the
processes of pregnancy. Finally, in elderly women, superadded to
the valvular defects, we have the dangers dependent upon the already
beginning arteriosclerotic changes in the bloodvessels. In all such
cases, therefore, it will be the duty of the physician to advise his
patient not to marry; and in any case to impress upon her mind the
extreme probability, amounting almost to certainty, of serious aggravation
of the heart disease by marriage, with permanent impairment
of the general health.
In cases of valvular disease accompanied by serious disturbances
of compensation, and in cases of notable degeneration of the myocardium
in which pronounced symptoms of cardiac muscular insufficiency
have made their appearance, marriage must be absolutely
forbidden, as directly imperilling life. When even moderate bodily
exertion suffices to cause palpitation, increased frequency of the
pulse, and shortness of breath, when extensive œdema of the lower
extremities is present and fails to disappear even after the patient
has been strictly confined to bed, when the pulse very readily becomes
irregular both in rhythm and force, whilst the urine is often scanty
and contains variable quantities of albumin, when conditions of
cardiac asthenia readily arise, characterized by a small, irregular
pulse, coldness of the extremities, cyanotic tint, nausea, respiratory
need,[42] and syncopal attacks—in all such cases, whether the symptoms
just described are dependent upon valvular defects, upon pathological
changes in the arteries, or upon diseases of the myocardium,
in all alike the occurrence of pregnancy is a true disaster, which in
the vast majority of cases causes a great and enduring aggravation
of the disease, and frequently enough costs the patient her life.
Even in such cases as were previously described, in which, the
heart disease not being severe, the patient was told that marriage
was permissible, it is the duty of the physician to lay down certain
rigid rules regarding sexual activity.
Women suffering from heart disease should not have sexual intercourse
255frequently, because, if the peripheral nervous stimulation
of the genital organs is excessive in consequence of too frequent
acts of coitus, cardiac activity is likely to be influenced powerfully
in a reflex manner, leading to the occurrence of attacks of cardiac
asthenia. Again, sexual intercourse must always be effected in
such a manner that the act attains its physiological conclusion, and
that in the woman as well as in the man the orgasm has its normal
outcome, that is to say that at the conclusion of the act the woman’s
cervical glands are evacuated with the accompaniment of the sense
of ejaculation. The congressus interruptus, which precisely in these
cases in which the wife suffers from heart disease is so frequently
practiced by the husband with a view to preventing conception, must
be strictly forbidden, since this mode of intercourse tends to give
rise to various forms of reflex cardiac disturbance, most commonly
to paroxysms in which the cardiac action becomes unduly frequent,
in association with diminution of vascular tone, vasomotor disturbances,
and states of mental depression; and where organic heart
disease already exists, these reflex functional disturbances involve
various dangers.
The physician is further justified in advising that a woman with
organic heart disease should not give birth to more than one or
two children. This advice is the more needful for the reason that
with each successive pregnancy the functional capacity of the
woman’s diseased heart diminishes according to a geometrical ratio,
and to a corresponding degree the danger to life increases. These
are cases in which in my opinion it is the physician’s duty to concern
himself with the subject—in general so equivocal—of the
use of preventive measures, and, having regard for the preservation
of a woman’s life, and uninfluenced by any false delicacy, but with
moral earnestness, to inform his patient with respect to the needful
prophylactic measures. The artificial termination of pregnancy,
which unquestionably is often justified in women suffering from
heart disease, but which unfortunately is apt to have very unfavorable
results, will rarely need to be discussed if by the proper employment
of preventive measures care is taken that pregnancy does
not recur too frequently.
To enable us to answer the question whether, in the case of neurasthenic
and hysterical young women, and in those hereditarily predisposed
to the occurrence of mental disorders, the physician shall
advise for or against marriage, attention must in the first instance
be directed to the established facts relating to the favorable or unfavorable
influence, as the case may be, of sexual intercourse and
its consequences (pregnancy and childbirth) upon existing nervous
disorders and upon the predisposition to their occurrence.
256Without regarding as fully justified the opinion that in the female
sex sexual abstinence has in all circumstances an unfavorable influence
upon the nervous system or even that such abstinence is to
be regarded as the principal cause of nervous and hysterical troubles,
we must consider it fully proved that in a number of the commonest
varieties of nervous disease occurring in neurasthenically predisposed
subjects, such as neurasthenia, hysteria and neurosis of anxiety[43],
the lack of sexual satisfaction aggravates these troubles, whilst
suitably regulated sexual intercourse has an actively beneficial effect.
Not, indeed, that it is an infallible means, but none the less the
effects are often striking, as I have frequently had occasion to
observe, both in young women so affected entering upon marriage
for the first time, and also in young widows who have remarried.
Especially is this true of women in whom the sexual impulse is exceedingly
powerful, and even pathologically increased to the extent of
marked sexual hyperæsthesia; likewise also in women whose social
circumstances and manner of life induce increased sexual appetite.
Be it understood, I refer here to regular and moderate sexual intercourse,
and not to sexual excesses, which latter, by inducing nervous
exhaustion, may have a distinctly deleterious effect. In many cases,
however, we observe in women suffering from sexual neurasthenia,
that sexual intercourse, even when practiced at long intervals, gives
rise to nervous prostration with deep emotional depression and long-lasting
aggravation of the existing nervous disorder. This statement
applies with especial force to very hysterical epileptic girls
with hereditary predisposition to mental disorder.
From the fact that among persons hereditarily predisposed to
mental disorder, the unmarried are on the average more often
affected with insanity than the married, the inference has been drawn
that marriage may be recommended to such persons as a measure
likely to counteract their hereditary tendency to insanity. The argument,
however, lacks validity, more especially as regards women;
among whom, moreover, from the age of sixteen to the age of
thirty, insanity is proportionately more prevalent among the married,
though above the age of thirty it is more prevalent among the
unmarried.
In the great majority of neurasthenic women, normal sexual intercourse,
practiced in moderation, has, according to Löwenfeld, no deleterious
effect; often, indeed, as a consequence of unaccustomed abstinence,
an aggravation of existing nervous troubles may be observed.
But, as this author maintains, nervous exhaustion may result in the
complete disappearance of the orgasm during sexual intercourse, or
in great difficulty in its production; this circumstance suffices for the
257most part to explain the fact that in women suffering from great
depression of the nervous functions, the fulfilment of their sexual
duties has sometimes an unfavorable influence on their general
condition. As regards hysteria, it cannot be denied, that in many
hysterical women marriage results in a favorable change in the
general condition; we must, however, be careful not to overrate
the significance of such observations. As a rule all that actually
takes place is a diminution in the intensity or even a disappearance
of certain morbid manifestations previously present, without, however,
an eradication of the hysterical temperament.
In epileptic young women, the first experience of sexual intercourse
may precipitate a fit. Cases are indeed on record in which,
in hereditarily predisposed girls, the first coitus was the exciting
cause of the first epileptic fit, the fits recurring every time sexual
intercourse was repeated.
It is a comparatively frequent occurrence in psychopathically predisposed
girls for severe mental disturbances to make their appearance
during the honeymoon, after the first experience of sexual
intercourse; when this occurs, it is doubtless to be accounted for by
the combined influence upon the mind of all the changes in the circumstances
of life which have resulted from the marriage. In the
case of two newly married women, one of whom had well-marked
hereditary predisposition, whilst in the other there was no known
family history of mental disorder, Löwenfeld observed shortly after
marriage the onset of severe melancholia, with refusal of food. The
delicate, nervous temperament of these two women, on the one hand,
and, on the other, possibly, a somewhat too eager and passionate
attitude on the part of their respective husbands, led their first
experience of sexual intercourse to result in a nervous impression
of the nature of shock, which their nervous system was too weak
to resist.
Frequently recurring pregnancy and childbirth may, according to
Krönig, act as the predisposing cause in the production of neurasthenia.
In regard to hysteria also we must admit that the onset
of some disease of the organs of generation frequently leads previously
latent hysteria to manifest itself openly, and further we have
to recognize that diseases of the reproductive system often
give the clinical picture of hysteria a quite distinctive coloration;
the physiological course of the functions of the generative organs is
also competent to produce both of these effects. Krönig, however,
rejects the view that the lack of sexual intercourse has an unfavorable
influence upon the nervous system in women, and gives rise to
hysterical and neurasthenic disorders. The favorable influence
which marriage is often observed to exercise upon the course of
nervous disorders is explicable with reference to psychical considerations
258of a very different nature. Sexual abuses, masturbation, and
the use of preventive measures, give rise in women far less often
than in men to neurasthenic and hysterical conditions.
Féré asserts that in certain neurasthenic patients sexual intercourse
induces a general blunting of the senses, and especially of
hearing and sight. Actual amaurosis of short duration may even
be observed; also cutaneous anæsthesias, paralytic conditions of the
extremities taking the form either of hemiplegia or paraplegia, convulsive
attacks, and somnolent paroxysms.
Delasiauve observed that epileptic patients, who during residence
in an asylum had remained almost entirely free from fits, after returning
home and resuming sexual intercourse, even in strict moderation,
suffered from a recrudescence of the convulsive seizures; when
intercourse was excessive, the relapse was naturally even more
severe.
In two instances, in women who in a single night had practiced
intercourse to very great excess, Hammond observed paralysis of
both legs to ensue; he saw also in numerous cases spinal irritation
and other nervous disturbances as a consequence of sexual excesses.
Von Krafft-Ebing points out, with reference to the prophylactic
influence of marriage in respect of mental disorder, that in men
early marriage diminishes the danger of the occurrence of such
disorder, whereas in women marriage is undesirable before the attainment
of complete physical maturity.
With regard to marriage in the case of persons suffering from
nervous diseases, Ribbing lays down the rule that when such diseases
have been severe and have occurred in numerous members of a
family, whilst a few only in the family have remained healthy,
when, moreover, the illness has been accustomed to make its first
appearance only after the attainment of maturity, no indications of
its onset being noticeable in childhood or youth—one belonging to
a family thus afflicted should be advised not to marry. Where,
however, the hereditary tendency is to a disease likely to manifest
itself in childhood or youth, a member of such a family who has
been fortunate enough to pass through the years of development
without exhibiting any pronounced disturbance of the nervous system,
may be permitted to marry if certain precautions are observed.
A woman with a tendency to alcoholism should in no circumstances
be allowed to marry. In the cases, fortunately rare, in which the
drink-craving exists in women, marriage is even more undesirable
than it is in the case of men similarly afflicted, for the female
drunkard is in a position in which she can mishandle and neglect
her children throughout the entire day; and, moreover, this affection
appears to be even more obstinately incurable in women than it is
in men.
259Löwenfeld very rightly insists that in deciding on the advisability
of marriage in the case of neurasthenic and hysterical girls the
anticipated influence of sexual intercourse must not be the sole
determinant. “Regulated sexual intercourse, such as is rendered
possible by marriage, has often a favorable influence on previously
existing states of nervous weakness. But we should go too far
if we were to attribute the beneficial effect of married life on such
conditions solely to sexual intercourse. This latter is but one factor
among several, the others being no less important. These others
are: The pleasures of an orderly domestic activity; the withdrawal
of the patient’s attention from her own condition, partly by domestic
duties and difficulties, and partly by the novelty of marital companionship;
the gratification, especially strong in women, at having
obtained a support in life; and, finally, the joyful expectation of
motherhood. These factors, however, are not present in every marriage.
When their presence cannot reasonably be anticipated, when,
in consequence of insufficient means, the marriage is likely to entail
increasing troubles, or when, owing to the want of suitability of
temperament, annoyances and quarrels are likely to occur, we must
throw the weight of our advice into the scale against the proposed
marriage, since the advantages of regulated sexual intercourse are
not likely to outweigh the disadvantages just detailed. Even when
means are ample and the characters of the couple contemplating
marriage are unquestionably harmonious, we must nevertheless
(temporarily, at any rate) advise against marriage, we must, that
is to say, advise the postponement of marriage, if the bride is suffering
from severe hysterical or neurasthenic states. Where, further,
such neurasthenic or hysterical troubles occur in a woman with
pronounced hereditary predisposition to nervous disease, we must,
both for the sake of the possible progeny and on account of the
uncertain influence of married life on the health of the patient,
absolutely and unconditionally prohibit marriage. In cases also in
which severe hereditary predisposition to mental disorder exists
(especially when derived from both parents), and in addition stigmata
of psychopathic degeneration are actually apparent in the
patient, or she has already suffered from the development of a
psychosis, we must decisively object to the patient’s marriage.”
As regards the marriage of young women suffering from tuberculosis,
we must take into consideration a fact that medical experience
has conclusively established, namely, that the processes of
generation have an unfavorable influence upon pulmonary phthisis.
Girls with an inherited predisposition to tubercular disease, sometimes
first manifest the symptoms of pulmonary tuberculosis at the
time of the menarche. In cases of developed tuberculosis, copulation
260and the excitement of the vascular system associated therewith have
a more or less unfavorable influence—and all the more inasmuch
as, in accordance with the saying omnis phthisicus salax, women
affected with tuberculosis often exhibit a very lively sexual impulse,
an almost insatiable sexual appetite. Sexual excesses are,
moreover, very likely to lead to the occurrence of hæmoptysis.
In former days it was believed that conception and pregnancy,
when occurring in women suffering from tuberculosis, had a restraining
influence on the progress of the pulmonary disease, a view
which found expression in the assertion of Baumes and Rosières de
la Chassagne that of two women affected with tuberculosis to the
same degree of severity, one who became pregnant would always
outlive the other who failed to become so. Careful and sufficient
observations on the part of physicians and gynecologists have, however,
shown that this view was fallacious, and, on the contrary, that
during pregnancy tuberculosis advances with more rapid strides,
that pregnancy, and lying-in accelerate the fatal event (Grisolle,
Lebert), that tuberculosis acquired shortly before pregnancy or in
the course of that condition, progresses with exceptional rapidity
(Larcher), and that the lying-in period is especially perilous to these
patients (A. Hanau). In some cases of consumption it is the first
pregnancy that is the most perilous, but in other cases a later pregnancy
proves more destructive.
Ribbing goes even further, insisting that neither man nor woman
affected with pulmonary consumption should marry. “If, indeed,”
he writes, “consumptives desire to enter upon marriage, merely with
the aim of being faithful to one another and assisting one another
for the short time that remains to them, I should offer no opposition.
But there must be a complete mutual understanding of the facts
of the case, and an unalterable determination on the part of both to
carry out the resolutions made prior to marriage, for failing this
the consequences will be most disastrous. In most cases, however,
the course adopted by Bulwer’s Pilgrims of the Rhine is to be preferred,
the lovers contenting themselves with the condition of a
betrothed pair, and in that state awaiting the approach of death—or,
if exceptionally fortunate, proceeding to marriage only after
restoration to health.”
It would certainly appear that in the case of girls suffering from
pronounced phthisis, we are justified in advising against marriage,
on account of the great danger which this state entails of a rapid
advance in the pulmonary disease.
Based upon the observations of Schauta and Fellner, the latter author
advances the rule that in the case of a woman suffering from
disease, marriage should be forbidden only when the mortality from
261the disease in question is not less than 10 per cent. In this category
we must include severe cases only of pulmonary tuberculosis; whilst
cases of laryngeal tuberculosis will, according to this rule, be absolutely
unfitted for marriage. Among heart-affections contra-indicating
marriage, he includes mitral stenosis, other valvular affections
in which there is serious disturbance of compensation, and
myocarditis; he considers marriage inadmissible also in cases of
chronic nephritis, and, among surgical affections, in cases of malignant
tumour. In cases in which during a previous pregnancy the
patient has been affected by one of the following diseases, viz.,
severe chorea, mental disorders, severe epilepsy, pulmonary tuberculosis
which progressed much during the pregnancy, morbus cordis
with considerable disturbance of compensation, severe heart trouble
due to Graves’ disease—in all such cases, a repetition of pregnancy
should be avoided.
Hygiene During the Menacme.
During the sexual epoch of the menacme a woman’s principal
hygienic need is marriage completely satisfactory alike to body and
to mind. It cannot be denied that sufficient sexual gratification,
regular, of course, and free from all excess, such as is usually experienced
in married life, is very advantageous to the health of a
woman who has attained sexual maturity—even though we admit
that the drawbacks of sexual abstinence, regarded as a cause of
disease of the female genital organs and the nervous system have
been as a rule greatly exaggerated.
The inability to marry always makes a deep impression on the
mental life of woman, and in many cases also gives rise to burning
desire and tormenting yearning of an erotic nature. The unmarried
miss life’s true goal and fail to enjoy the natural exercise of their
functional capacities; alike in the cultured lady and in the poor
working woman who has failed to marry, the thoughts and feelings
return again and again to her own condition in a self-tormenting
manner.
The physical and mental disadvantages entailed by sexual gratification
when obtained by an unmarried woman, one who, according
to modern phraseology, “wishes to secure her natural share of the
joys of love,” and who regards voluntary chastity as “a sacrifice to
meaningless prejudices”—need not be more particularly described.
Free love, moreover, is the most important disseminator of
gonorrhœal infection. “In any future commonwealth,” says Runge,
“in which marriage is abandoned in favour of the general practice of
free love, the human race will be overwhelmed by gonococci in a
manner now hardly conceivable, and the reproductive capacity in
262both sexes will be diminished by the results of gonorrhœa to a very
serious extent.”
Frequently enough, also, free love leads to prostitution, which at
the present day is so widely prevalent. Various reasons have been
suggested to account for the increase of prostitution. Among these
are: The growth of modern industry, with the consequent aggregation
of the population in large towns; the decline in the marriage rate;
the postponement of marriage; universal military service; the freer
mutual companionship of the sexes; and many others. At any rate,
the fact would appear to be established, that in the case of woman
the determining cause of prostitution is hunger rather than the
sexual impulse. The worst paid classes of workwomen are shown
by official statistics to furnish the largest number of recruits to the
ranks of prostitutes; and it is during times of deficient employment
that the number of women practicing occasional prostitution increases.
Thus, material need is the most important of the causes
of prostitution.
This remains true even though the doctrine of Lombroso and
Tarnowsky should find fuller justification, the doctrine that the
practice of prostitution by women is the natural expression of a
congenital morbid predisposition, “which impels them, in defiance
of their direct advantage, of reason, and of all counter-advice, to
adopt this accursed mode of life.” Prostitution, in this view, is to
be regarded as the inevitable outcome of congenital moral insanity.
This is certainly true of a small proportion of prostitutes, but is as
certainly false of the great majority, in whom unfavorable, difficult
conditions of life form the determining cause. A certain inherited
or acquired mental disposition may, indeed, be assumed to exist
in these cases also—an unstable moral equilibrium, an insufficient
development of the force of the will and of the power of resistance.
The hygienic requirement of married life for woman during the
menacme is undoubtedly sometimes hard to fulfil in our day, when
the more elaborate and expensive standard of life has increased the
difficulty of supporting a family; but from the medical point of
view it is necessary to insist forcibly on this categorical imperative,
in opposition to the view advanced by the modern women’s rights’
party, that “love is moral also in the absence of legal marriage”
(Ellen Key); in opposition to the yet more extreme opinion of
George Sand and of Almquist, who, regardless of consequences,
declare marriage to be immoral; and, finally, in opposition to the
advocates of “free love,” who wish woman to be as free as man
in sexual relations.
Much as we may wish that man and wife should be in complete
harmony in marriage, and that they should feel themselves to be
263firmly united alike by mutual love and by a reciprocal sense of duty,
none the less we must consider the modern maiden ripe for marriage
as unjustified in demanding, before undertaking marriage, “perfect
love as typifying the inner yearning of two beings to become one;”
and we must regard the latter-day woman as extravagant in insisting
that the man shall enter upon marriage in a condition as virgin
as that of his contemplated wife. “Perfect love” is as rare and as
little to be expected as perfect beauty; and the sexual life of man
differs entirely in nature and in the course of its development from
the sexual activity of women.
Doubtless they spring deep from the soul of woman, the demands
expressed by the writer of the book “Vera” and by her numerous
imitators, the apostles of “Veraism,”—the demands of the maiden
entering upon marriage that her husband shall be as chaste and
sexually as unspotted as herself. Difficult of fulfilment as they
are, if fulfilment is even possible, these demands must none the less
be regarded as characteristic of the sexual life of modern womanhood.
“Is man’s sexual honor,” exclaims Vera, “then altogether
different from that of woman? Is not the alleged necessity for
sexual gratification in youth either a well-organized fraud or an
enormous error on the part of physicians? Is it possible that chastity
can entail diseases as terrible, as destructive to life and happiness as
those that result from unchastity? And is it not a crying sin, even
if some of these fears are justified, to ruin both mentally and
physically the whole race of women? * * * Man demands from
the girl of his choice, not chastity alone, but an absolutely unblemished
character. And rightly so. But the wife must share her
husband with street-walkers? She must bear the pangs of maternity,
while fortified by the terrible knowledge that the father of her
children has wasted his youthful virility in purchased embraces, that
he has not recoiled from impurity, that he has exposed himself to the
risk of infection with the most horrible diseases, that he has squandered
his virginity in the most bestial sensuality? * * * We
girls must also be granted the right to demand from the man of our
choice the same purity, the same unspottedness by sensuality, that
he so rigorously demands from ourselves! We must no longer content
ourselves with the remnants that are left for us by others! We
must no longer be satisfied with man’s moral inferiority! Then
there will be more happiness, more love, more health and joy of
life!”
These accusations and demands so boldly made are not to be disposed
of by mere mockery. With deep sorrow we must admit the
absolute truth of the charge that too many men clamber out of
the abyss of debauchery to a blighted marriage. But the demand
264for equal moral rights, for the abandonment of the hitherto prevalent
bisexual ethical standards, is in vain conflict with actuality, with
the defensive instincts of young men, with the difficulties entailed
by the struggle for existence, with the increasing pretensions (to
sexual freedom) of women themselves; but above all is it in conflict
with the thousand-year-old notions of sexual honor in the male
and the female respectively, and with the undeniable fact that the
mature man is capable of elevating himself out of the base intoxication
of the senses characteristic of youth, to attain the noblest and
most intimate married love, whereas the girl who has once descended
into such an abyss sinks therein and is beyond the possibility of
rescue. Thus early marriage with equal purity of husband and wife
remains a postulate which the present can hardly be expected to
satisfy, and one whose fulfilment must be left to the future.
In consequence of modern writings and discussions concerning the
erotic problem, there has arisen a hypersensibility on the part of
women in respect of the conditions in which they pass their married
life, leading them to demand greater independence, a greater expansion
of their own individuality; this tendency must, however, be
resisted, if the marriage is to be a happy one, with mutual comfort
and reciprocal consideration, one suitable, not for exceptional beings
in an ideal state, but for men and women as they really are. In such
a marriage, affection and a sense of duty will strengthen love and
preserve fidelity. A prudent, clever woman will always understand
how, notwithstanding all necessary self-surrender, to preserve the
freedom of her own individuality and the esteem of her husband.
Marriages based upon true inclination usually result in the birth
of stronger and more beautiful children than marriages in which
the money-bags were the sole or the principal determining cause.
In England, where people commonly marry when still quite young,
beautiful and healthy children are more often seen than in France,
where marriages of expediency form the great majority. According
to Bertillon, of 1,000 young men from 20 to 25 years of age, in
England 120 marry, but in France less than half that number, viz., 57
only. And 100 wives between the ages of 15 and 40 give birth
annually, in England to 39 children, in France to 26 only, a number
less by one-third.
In deciding upon marriage, hereditary influences deserve careful
consideration in respect alike of the family of the prospective husband
and that of the prospective wife. For it is well established that
the law of inheritance relates not only to the peculiarities of external
configuration, to the features, the stature, the tint of the skin,
but also that children inherit from their parents their mode of
bodily development, the functional activity of their organs, the duration
265of their life, their predisposition to disease, and even their intellectual
and moral qualities. As regards hereditary predisposition
to disease, the most important are, as is well known, the predisposition
to tuberculosis, that to malignant tumors, and that to mental
disorders.
Great disparity in the respective ages of prospective husband and
wife entail various kinds of unsuitability for marriage. An elderly
man who marries a young girl, even if he still possesses a certain
amount of virility, is unlikely to procreate healthy and powerful
children; and these latter for the most part will be weakly, scrofulous
cachectic, endowed with deficient powers of resistance, and often
badly equipped from the intellectual standpoint. Similar considerations
prevail in respect of marriages in which the husband has been
exhausted by earlier sexual excesses, so that he retains no more
than remnants of virility, whilst his semen is of doubtful fertilizing
power. D. Richard relates that Louis XIV asked his physician why
it was that the children he (the king) had by his wife were delicate
and deformed, whilst those he had by his mistresses were beautiful
and powerful. “Sire,” was the answer, “c’est parce que vous ne
donnez à la reine que les rincures.”
Plato maintains that before every marriage the man and the
woman should both undergo official examination to determine their
fitness or unfitness for the married state, the man being absolutely
nude, and the woman stripped to the waist, for the examination.
This author goes so far as to regard it as “a form of homicide for
a man to embrace a woman when he is incapable of fertilizing her.”
How rarely it happens in our day, however, that the physician, the
official with the requisite knowledge to fulfil Plato’s requirements,
is asked for his opinion regarding the desirability of a contemplated
marriage! The only occasion on which this is likely to occur is
when a man intending to marry wishes to be assured that he is completely
cured from an earlier infection with syphilis, and, therefore,
runs no risk of transmitting the disease to his wife or to
possible offspring. But it never occurs to the parents of a girl about
to marry to ask the physician whether she is physically suitable for
marriage.
In deciding on marriage, however, care should before all be taken
to determine that the girl has attained complete physical and especially
complete sexual development. The age at which woman attains
complete sexual maturity is in our climate and race coincident
on the average with the twentieth year of life.
For the hygiene of marriage it is necessary that the bride should
not be extremely youthful. Notwithstanding the fact that the legal
codes of civilized countries nowhere demand for girls a greater age
266than fifteen years before permitting marriage, this limit is, generally
speaking, fixed far too low. Before becoming a wife, the girl should
not merely have attained complete physical development, with her
reproductive organs in a state of maturity, but she must also be
developed intellectually to such an extent that she is fully capable
of understanding the nature and significance of marriage. At the
age at which marriage is legally permissible, a girl is still far from
having attained physical and mental ripeness for marriage, reproduction,
and maternity.
Especially with reference to the last consideration is it inadvisable
that in our climates a girl should marry earlier than from 18 to 20
years of age, and preferably even she should first attain the age of
from 20 to 22. In that case her happiness as a mother will be more
secure, and there will be a greater probability of her producing a
healthy progeny. In the East, indeed, quite different views prevail.
According to the laws of Manus, a girl might marry on attaining
the age of eight years; if within three years thereafter her father
failed to provide her with a husband, she might choose one for
herself. Among the Hindus it is regarded as a disgrace to the
parents if a girl does not marry quite young, indeed before the first
appearance of menstruation. Atri and Kasypa state that if a
girl begins to menstruate before she leaves her father’s house, the
latter must be punished as if he had destroyed a fœtus, while the
daughter herself loses caste. Marriage delayed till after the appearance
of menstruation being regarded as sinful, girls are married
while still children, in order to prevent the loss of mature ova, which
is regarded as equivalent to infanticide. Very early marriage has
thus in India been legally ordained for thousands of years. The
Hindus, who even now regard every menstruation which has not
been preceded by coitus in the light of infanticide, marry their
daughters before the age of puberty.
According to oriental tradition, Mahomet married Khadijah when
five years of age, and cohabited with her three years later. In the
Bible, numerous similar examples are recorded. Among many
savage tribes, as, for instance, among some of the aborigines of
India, and among the indigens of Australia, copulation is usually
effected before girls reach the age of puberty; in India, indeed,
according to Ploss and Bartels (Das Weib in der Natur und Völkerkunde),
marriage with immature girls is a widely diffused
custom, and in Australia a child of ten or eleven is often found to
be the wife of a man of fifty or the concubine of a sailor. In general,
according to these authors, we find that the age of nubility in girls
is lower in proportion to the lowness of the stage of civilization
attained by the race or people to which they belong. Among the
267ancient Romans, girls were commonly married between the ages of
thirteen and sixteen years.
In the Talmud, Rabbi Joshua gives the following advice regarding
early marriage in Jewish girls: “If your daughter has attained
puberty and is twelve years and six months old, she must be married
at any cost. If no other means are available, manumit one of your
slaves, and give her to the freedman to wife.”
Experience proves, however, that in our climate, at any rate, girls
who marry at a very early age are inferior in fertility to those who
refrain from marriage until the genital organs have attained complete
maturity; and statistics show that those women who marry
before attaining the age of twenty must wait longer for their first
pregnancy than those who marry between the ages of twenty and
twenty-four. At the higher age also, women bear parturition and
its consequences more easily than those who marry very young.
A similar influence in marriage to that resulting from undue juvenility
is exercised by its opposite, marriage when a woman is
already elderly; in this case fertility is limited, and health also is
especially apt to suffer. When the indications of the climacteric
are clearly apparent, marriage is contra-indicated, not only on account
of the impossibility of fertilization, but also in respect of
its general unsuitability in the closing stage of the sexual life.
Not only is the absolute age of the woman of importance in deciding
on the advisability of marriage, but the relative ages of the
proposed husband and wife must also be taken into account, first
of all in respect of the wife’s possible fertility, and secondly in respect
of her general health. The most suitable arrangement is that
in which there is no marked difference in age. The husband may
be, and indeed in existing social circumstances almost necessarily is,
somewhat older than his wife, as much perhaps as eight or ten
years. But a very great disparity of age (in either direction) is a
serious error. If a very young girl marries an elderly man, or a
developed matron marries a young man, the true purpose of marriage
is unfulfilled, the eternal laws of nature and all ethical principles
are infringed. In the breeding of animals, the fundamental principle
has long prevailed that the animals chosen for coupling should
be well suited each to the other and should be in perfect physical
condition; and breeders are also familiar both with the favorable
influence of good nourishment and with the advantage of the opportune
crossing of distinct varieties. The same principles are
equally applicable to the human race, neglected as they commonly
are in practice.
With regard to the marriage of near kin, we can only remark
that the marriage of those closely related by blood should as far
268as possible be avoided, and that such a marriage must be absolutely
prohibited when in both families there is a history of tuberculosis,
mental disorders, diabetes, and the like. When first cousins contemplate
marriage, it is indispensable, not only that both individuals
should be in perfect health, but also that on neither side there should
be any serious family history of transmissible disease or transmissible
morbid tendency; and, further, it is absolutely necessary that no
such marriage of near kin should have taken place in the proximate
ancestry of the cousins, i. e., their cousinship must not be a double one,
derived both from the paternal side and the maternal. It is indeed
to be recommended, with a view to the production of a healthy and
powerful posterity, that marriage should bring about a crossing of
healthy individuals proceeding from different families, different
places, and different constitutional types. An instance of the advantage
to be found in this practice is pointed out by Ribbing, who
shows that the most powerful aristocracy in Europe, that of England,
by the gradual creation of new peers, on the one hand, and
by the gradual decline of younger sons and their descendants into
the middle class, on the other, has undergone a continual crossing
with less exalted but originally sounder stocks; in this way its vigor
and fertility have been maintained, in contrast to the nobility of
many continental states, which has so largely perished, in consequence
of its exclusiveness in the matter of marriage.
“In this connection,” continues Ribbing, “we must bear in mind,
that blood-relationship is not the only matter that has to be considered;
in the interest alike of the family, and of society, it is necessary
to demand that certain degrees of relationship by marriage
alone, should fall within the ‘prohibited degrees’ of love and
marriage. There are certain groups related by marriage and held
together by the bond of affection, from which foster-parents and
guardians may most suitably be selected to fulfil the duties as regards
education and training of children who have been orphaned in
early years. For such a purpose none seem better adapted than the
brothers and sisters of the deceased parents; but the upbringing of
the children can be confidently entrusted to the former only if the
relationship between the older and the younger branches of the
family is one regarded by law, and still more by morality and
custom, as one precluding the possibility of the occurrence of sexual
love and marriage.”
Möbius, writing on “The Ennobling of the Human Race by Selection
in Marriage,” observes: “The most important aim of
natural development is the perfection of humanity. The qualities
of the coming generation depend for the most part upon the qualities
of the parents. Marriage from affection ensures the fulfilment of
269nature’s aims with more security than marriage from reason; since
what we have to think of is not the happiness of the married pair
but the quality of their children. Of great importance, also, to the
development of the human race are the conditions during the commencement
of life, and the mode of education. The improvement of
the race has not hitherto been the conscious aim of the generality of
people. The law does not as yet, as it should, take into account
the advantage of posterity. Capital punishment is fully justified
and purposive. Criminals should not be allowed to marry. The
perpetuation of disease by inheritance should be checked by the utmost
powers of the state. Any one marrying while suffering from
any venereal disease still in an infective condition should be punished.
The marriage of persons suffering from tuberculosis should
be prohibited. For the prevention of disease is more important than
its cure. The most important factor in preventive medicine is an
improvement in the conditions of life. The human ideal should be,
goodness of heart in association with physical and mental health.
Goodness, beauty, and strength should be simultaneously pursued.
Since, however, man is made by birth far more than by education,
selection in marriage is of fundamental importance. In the choice
of a partner, attention is rightly paid to beauty, since beauty and
health are fundamentally identical; moreover, a human being endowed
with beauty is usually also more moral than one devoid of
that attribute. Equality of birth is as a rule desirable in marriage;
but not the family only is to be considered in determining the existence
of such equality, individual characteristics must likewise be
taken into account. Whether the crossing of races is desirable is
not yet certainly determined.”
From the hygienic standpoint it is necessary that in marriage
also the frequency and the manner of sexual intercourse should be
regulated.
Wise men and lawgivers of all the nations of antiquity have insisted
upon the necessity of certain intervals between the acts of
intercourse. Thus, Mahomet prescribed 8 days, Zoroaster 9 days,
Solon 10 days, Socrates also 10 days. Moses forbade intercourse
during menstruation and for a week after the cessation of the flow.
Luther prescribed intercourse “twice a week.”
Birds and many mammals are competent to perform intercourse
at exceedingly short intervals. A well-bred cock will repeat this
act 50 times daily; a sparrow, 20 times in an hour; a bull, 3 to 4
times in an hour. In the human species, however, too rapid repetition
of intercourse is deleterious not only to the male, but to the
female also, though the latter certainly suffers in less degree. For
in this act the female plays a more passive part, and for this reason
270can repeat it with impunity more frequently than the male, who
loses semen at each repetition. It is not possible, however, to lay
down precise rules as to the permissible frequency of intercourse
in either sex; the matter must depend upon physical needs. Moderate
and regular indulgence in sexual intercourse is unquestionably
advantageous to women both physically and mentally, regulating all
the functions of the body, and tending to produce a contented and
cheerful frame of mind.
During menstruation, a woman should refrain from intercourse.
By the Mosaic law the death punishment was allotted both to the
man and to the woman who indulged in coitus while the latter was
menstruating. As a matter of fact, considerations alike of hygienic
cleanliness and of sanitary precaution prohibit the performance of
coitus during this period. Severe menorrhagia, perimetritic irritation,
and parametritic inflammations, have been observed to follow
such indiscretions. On the other hand, it is more than doubtful
whether, in the event of pregnancy resulting from intercourse performed
during menstruation (and conception is especially apt to
occur at this time), the child is likely, as earlier authors maintained,
to be unfavorably affected, and to suffer from cachexia, scrofula,
or rickets.
After the act of intercourse, a woman should rest; and indeed
sleep for some hours is especially to be recommended. A vaginal
douche should not be administered until several hours have elapsed,
otherwise there will be a risk of preventing fertilization of the
ovum. The water employed for vaginal irrigation should never be
quite cold; a temperature of 79°–82° F. (26°–28° C.) is best.
All measures for the purpose of artificially increasing sexual desire,
such as alcoholic beverages (especially champagne), and certain
drugs (especially cantharides), are even more harmful to women
than they are to men. The woman who conceives while in a state
of intoxication commits a great sin against the coming generation.[44]
Just as harmful, however, are the anaphrodisiacs sometimes employed
to diminish the intensity of sexual desire when this cannot be
gratified. When affected with intense sexual excitement, a woman
is much more unfavorably situated than a man, since man claims
the right to indulge in sexual intercourse whenever he feels disposed,
271and has, moreover, ample opportunity for sexual gratification. A
woman, however, properly endowed with self-respect, will understand
how to bridle her senses. Bodily exercise, moderate, unstimulating
diet, intellectual occupation with serious matters, the avoidance
of equivocal literature and of sensual dramatic representations,
cold bathing, and the use of a hard mattress and light bed-clothing—these
means will coöperate powerfully toward the prevention
of excessive sexual desire. Horace already remarked:
“Otia si tolles, periere Cupidinis arcus.”
The wife should know how to bridle, not her own desires only,
but also those of her husband. She must not demand too much
during the intoxication of youthful vigor; she must prevent the complete
combustion of the flames of masculine passion, and must keep
sparks glowing in the ashes. Economy during the sexual prime
preserves sexual power, enables a man to continue intercourse to a
ripe age, and avoids premature exhaustion and satiety. When the
husband is drawing near the end of his sixth decade, the wife must
accustom herself to see in him rather the father of her children
than her own husband, and must reduce her sexual demands to that
measure which will not be injurious to his health. Demosthenes,
writing of the sexual life of the Athenians of his time, said: “In
order to obtain legitimate offspring and to provide a faithful
guardian of our household, we marry a wife; for our service and
for the performance of daily household duties, we keep concubines;
for the joys of love, we seek the hetairai.” The task is extremely
difficult, but a clever and virtuous modern wife must endeavor to
combine in her single personality the sensual attractiveness of an
Aspasia, the chastity of a Lucrece, and the intellectual greatness of
a Cornelia; she must bear in mind the epigram of Bacon, “A wife
must be a young man’s mistress, a middle-aged man’s companion,
an old man’s nurse.”
In the act of intercourse the woman must always play the more
passive part; she must be desired, rather than desire. Woman’s
modesty increases man’s desire. By this coquetry, permissible because
natural, the woman can bind the man to herself, and can
give the lie to the assertion that marriage is the grave of love.
Partial concealment of her desire on the part of the woman is more
stimulating to the man than an open manifestation of the sexual
impulse; and a certain amount of modest reluctance is more alluring
to him than a plain invitation. Plenty of room must be left for
the play of fancy and imagination. Schiller makes Fiesco say to
the Countess Julia, as he covers up her bosom, “The senses must
be blind letter-carriers only, and must not be aware of that which
nature and the imagination communicate each to the other. The
best of news is stale as soon as it has become the talk of the town.”
272For this reason, also, it is more suitable that intercourse should
take place, not by day, consequent on the brutal prompting of
vision, but by night only, beneath the protecting veil of darkness.
A night’s rest, moreover, will serve to restore the exhausted nerves,
and to replace the expended secretions. Less advisable is coitus in
the morning, on awaking from sleep, since the labors of the day must
immediately thereafter be undertaken. Partially impotent men only,
who wake up with an erected penis, endeavour to avail themselves
without delay of this favorable opportunity, bearing in mind the
French proverb, “On aime quand on peut, et non pas quand on
veut.”
The French custom, in accordance with which the married pair
sleep together in a double-bed is undesirable on several hygienic
grounds, and, in the first place, for the reason that this continuous
nocturnal proximity is likely to give rise to the habit of indulging
in excessively frequent acts of intercourse. The best and most affectionate
of men has neither disposition nor capacity to play the
part of Romeo every night, and thus the value and enjoyment of
marital duties becomes lessened. The fulfilment of his desires should
not be rendered quite so easy to the husband; he should always appear
the lover, one who seeks a woman’s favours because he longs
for her; he should not be the master, exacting an unquestioned right.
For this reason, separate beds are advisable for the married pair,
and, when possible, even separate bedrooms.
Among the ancients, Lycurgus, the Spartan law-giver, regarded
maternity as woman’s principal attribute, and considered the sexual
impulse to be the means merely by which healthy citizens were provided
for the state. In accordance with this view, the sanctity of
marriage was violated, and every powerful, handsome, and valiant
Spartan had the right to request the privilege of intercourse with the
wife of another, in order to enrich that other’s family with his seed.
Elderly, impotent men conducted well-formed young men into the
arms of their own wives. The girls, like the young men, went
through a course of gymnastic exercises, in order to harden their
bodies, and to fit them for the bearing of strong and healthy children.
No man might marry before attaining the age of thirty, no
woman before attaining the age of twenty. Girls ripe for marriage
were assembled in a dark place, and there the young men chose
their brides, as chance might direct. The young men were allowed
to visit their wives by night only, and secretly, in order that
the vigor of the sexual impulse might be increased and maintained.
Among the Spartans, it happened quite frequently, that a man
whose wife had remained childless, and who believed himself to be
273at fault in the matter, would beg one of his fellow-countrymen, or
even a foreigner, to come to his assistance. It was enacted by one
of Solon’s laws, to prevent a man from neglecting his marital duties,
that he should have intercourse with his wife not less than three
times monthly. According to another of Solon’s laws, an Athenian
heiress might call upon her nearest relative for the gratification of
her sexual desires.
The bluntest contrast to this Spartan simplicity is furnished by
the unbridled lasciviousness that prevailed in Rome under the
Cæsars, when women’s sole desire was sexual enjoyment, while
maternity was a state to be avoided. To such an extreme was this
carried, that the Roman ladies of that day preferred to marry
eunuchs, and further, as Pliny reports, hermaphrodites were in great
request. Juvenal writes: “There are women who prize the infertile
embraces of base eunuchs; thus they are able to dispense with the
use of abortifacients.”
The hygiene of the nuptial night deserves from the physician
more attention than it has hitherto generally received. He should
warn and enlighten the young husband, in order that the brutality
with which the act of defloration is apt to be performed may be
lessened, and further in order that mistakes in this connection, resulting
from ignorance and likely to have serious consequences, may
be avoided. It is well known that lacerations of the hymen and its
environment, and even serious injuries of the genital organs, may
result from maladroit attempts at penetration. The physician will
admonish the husband in the words of Michelet: “Bear in mind in
this hour that thou art an enemy, a tender, considerate, and gentle
enemy!”
The young woman entering upon marriage should receive instruction
from her mother regarding all the sexual processes of copulation,
instruction at once earnest and complete. By such enlightenment,
the young bride will be spared much suffering, and a sudden
disillusionment which might seriously affect the whole of her future
life will be avoided; complete ignorance, on the other hand may
lead, not merely to needless mental and physical suffering, but to
the most tragic consequences on the bridal night. In one case known
to me, the young wife, who before marriage was utterly ignorant
of the nature of physical love, was so completely overwhelmed in
her ideals by the somewhat energetic procedure of the bridegroom as
soon as he found himself alone with his wife, that she fled from
her new home then and there in the night, and by no persuasions
could be induced to return.
In that decisive moment in which the maiden loses her virginity,
she must find in her husband, not the brutal man who forcibly takes
274possession of her body, but the chosen man of all, to whom her love
can refuse nothing.
“Delicate foresight and restraint,” writes Ribbing, “are needful
above all at the commencement of married life. The young wife,
coming to the bridal bed a pure virgin, is not, like her husband,
fully prepared for what is to take place. In all cases she is somewhat
fearful of the new experience. The first act of intercourse
involves for her a certain amount of pain, and this pain is not solely
physical. * * * Moreover, we must remember that the entire
change in her mode of life makes a deep impression upon a woman’s
mind; time and quiet are needed before she can find herself at
home in the novel surroundings, before she can adapt to the changed
circumstances her moral and religious convictions, and before she
can ‘think true love acted simple modesty’ (Romeo and Juliet, III,
2.16). Impatient husbands, through want of knowledge and lack
of consideration during the honeymoon, have often ruined the happiness
of subsequent married life.”
It happens often, unfortunately, that the wife has reason to complain
of the reckless manner in which her husband has used, or
misused, his sexual powers. Frequently enough, on the bridal night,
the man proceeds with such violence in his assault on the virgin
reproductive organs of his newly-wedded wife, that we must actually
speak of him as ravishing an ignorant and timid girl. Later, when
the stimulus of novelty has passed away, the husband often performs
intercourse in a manner more calculated to awaken his wife’s sexual
desires, but in seeking his own lordly gratification and obtaining it
he is still apt to leave out of the reckoning the need for effecting
coitus in such a way as will give complete satisfaction also to his
wife.
The wedding journey likewise deserves consideration from the
hygienic standpoint. Much is to be said in favor of such a journey,
inasmuch as it endows the necessarily somewhat brutal first act of
intercourse with an aspect of romance. The removal to a foreign
country, to a strange environment, will spare the chaste maiden
much shame and vexation. On the journey, moreover, the young
couple are much in each other’s company, and the process of mutual
adaptation is agreeably favored. And yet this modern custom of
making a wedding journey entails certain serious disadvantages.
The young woman leaves her home and her nearest relatives, and
is in a moment involved in the excitement of travel, an excitement
liable to increase to the degree of morbid anxiety. The fatigues
of railway-travel, of wandering about strange towns, of visits to
museums and picture-galleries, are apt to cause general loss of
nervous tone, and also local hyperæmia of the genital organs. In
275addition, false modesty and the prescribed arrangements for the
journey may lead the onset of menstruation to be ignored and the
customary rest at this period to be dispensed with. Still more,
the possibility of the occurrence of conception and of the commencement
of pregnancy is usually left altogether out of the account.
Many an attack of menorrhagia, of perimetritis, and of endometritis,
many a miscarriage, and many instances of protracted sterility, are
dependent upon the hygienic mistakes of the wedding journey, and
less, indeed, upon the abuses arising out of the intoxication of passion,
than upon the fatigues of excessive travel both by day and by
night. The bride who on her wedding-day was young, healthy, and
full of vitality, not infrequently returns from the wedding journey
a sickly and debilitated woman.
With regard to wedding journeys in relation to the causation of
chronic metritis, Scanzoni has expressed an authoritative opinion.
“After many weeks of unsatisfied sexual desire, the young married
pair, now freed from all restraint, give themselves up to
the joys of love; the intense sexual excitement causes great stimulation
and hyperæmia of the female sexual organs; in addition, the
noxious influences of travel make themselves felt, and also hygienic
indiscretions are perpetrated, dependent upon the young wife’s
modesty; it is, therefore, by no means to be wondered at that, having
left home a perfectly healthy woman, she returns from her wedding
journey with the germs of an illness from which she never fully
recovers, and which is the source of unending suffering, and more
particularly of a sterile marriage.”
Sexual hygiene demands a certain moderation in the enjoyment of
physical love, and also a certain constancy, such as may be expected
in a happy marriage.
It is not possible to lay down a general rule with regard to the
frequency of sexual intercourse, notwithstanding the earnestness
with which religious zealots, physicians, and moral teachers have
in all ages endeavored to determine how often it was proper for
a man to cohabit with his wife. The rules that have been prescribed
by the various authorities had in view, for the most part, the protection
of the wife from excessive demands on the part of her husband;
sometimes, however, by the establishment of a minimum
period, a certain amount of sexual gratification was secured to the
wife; finally, also, the generation of a healthy posterity had to be
taken into consideration. Ribbing, however, justly observes: “Sexual
intercourse results from a natural impulse, and he whose senses
are unimpaired, and who has learned, at the same time, amid the
tumult of his sensations, to preserve proper consideration for his
wife—such a man runs little danger of making any mistake. In
276opposition to the opinion of many, I regard it as entirely right and
reasonable that husband and wife should have intercourse whenever
physically and mentally impelled to that act. Nor do I see any
reason why, during the first period in which they are able to enjoy
without intermission the pleasures of sexual intercourse, they should,
in accordance with any theory whatever, impose on themselves
further restraints than those demanded by care for their physical
and mental health. The touchstone of marital hygiene is this, that
on the day following intercourse both husband and wife should feel
perfectly fresh, vigorous, and lively, alike in body and mind—even
more so, perhaps, than on other days. In the absence of such feelings,
we may feel assured of the occurrence of sexual excesses.”
The same author quotes a saying of Pomeroy’s: “We may quaff
the nectar as freely as we will—nature herself mixes the draught
and holds the goblet to our lips; if, however, we drink too much,
she first dilutes the draught with water, later adds gall, and ultimately
perhaps deadly poison.”
The occupation, trade, or profession, and the nutritive condition
and physical constitution of the married pair, have an important
bearing on the frequency with which, without detriment to health,
cohabitation is permissible. The rules of the Hebrew Talmud already
take these circumstances into account, ordering as they do
that young and powerful men not engaged in any regular occupation
shall have intercourse with their wives daily; manual labourers,
on the other hand, once a week only; whilst brain-workers, finally,
or those whose work is extremely arduous, should allow an interval
of one or more months to elapse between the acts of intercourse.
Acton also prescribes that in the case of brain-workers and of those
manual workers whose labours are exhausting, intercourse must not
occur more frequently than once every week or ten days.
The married couple should understand how to impose on themselves
a certain restraint in the matter of marital intercourse, without,
however, going so far as on altogether trifling grounds to
refuse the husband access to his wife. In this respect also, the
opinions that have recently come to prevail concerning the rights
of women have had an influence. W. Acton relates a case that
came under his observation in which the wife refused to allow her
husband any voice in determining when and how often intercourse
should take place; the wife, she maintained without hesitation, since
she had to bear the consequences of intercourse, was fully justified,
whenever she thought fit, in refusing her husband’s embraces.
The dangers to the sexual life of woman which are involved by
the modern woman’s rights agitation are seen already in the changes
which the emancipation of women in North America has produced
277in the functions of woman as wife and mother. In that part of the
world, everything possible has been done “to transform” (to quote
the words of a brilliant journalist) “the doll into an independent
existence, to enable the helpless woman to earn her own subsistence,
and the result of these endeavors has been most striking.
The American woman has obtained the right to enter every
profession and to follow every kind of occupation which have
hitherto been reserved for men; she is physician, lawyer, merchant,
professor; her boudoir has become an office, often connected with
the stock exchange by a private wire. Legally, also, she now possesses
the same rights as man; in many States she has both the
suffrage and the right of entering the house of representatives; she
has fully emancipated herself from her former condition of tutelage,
and in her shrillest tones can cry to heaven ‘I am free, I am independent,
I am emancipated, I am myself!’ And observe, as the
result of all these attempts at the conversion of woman into man,
that in the matter of marriage also she acts as if she were no longer
woman. The American woman no longer marries; perhaps, indeed,
because she no longer has the capacity. So long and so eagerly has
she given herself up to masculine occupations, that her inward
feminine nature has also perhaps undergone transformation, so
that she has become affected with a kind of neutral lack of desire.
Unquestionably, the desire for marriage on the part of this modern
‘emancipated’ woman has vanished in the most alarming manner,
there is a notable fall in the birth-rate, and the indigenous (white)
population actually threatens to disappear.”
The wife acts wisely, not on hygienic grounds alone, in not
always acceding at once and unconditionally to her husband’s demand
for the repetition of intercourse. Her modest reluctance enhances
her desirability in the eyes of her amorous husband. Thus,
Shakespeare makes Posthumus exclaim (Cymbeline, Act II., Sc. 5,
l. 9):
“Me of my lawful pleasure she restrained
And prey’d me oft forbearance; did it with
A pudency so rosy the sweet view on’t
Might well have warmed Old Saturn.”
Especially justified is such refusal when coitus has been already once
or twice performed, or when the consumption of alcoholic beverages
has made the husband unduly lustful. On the other hand, the refusal
of intercourse when demanded by the husband should never
depend upon baseless feminine caprice, or upon the now so frequently
asserted “rights of women.”
Experience has long ago established as a fact that unduly frequent
satisfaction of the sexual impulse entails serious consequences
to the health of the individual. And in the case of the wife these
278consequences may be especially disastrous when intercourse is indulged
in recklessly during menstruation, during all stages of pregnancy,
and even during the puerperium. “Incontinence during
menstruation leads to serious circulatory disturbances and to the
consequences of these disturbances; during pregnancy it is likely
to give rise to miscarriage; during the puerperium, to congestions
and inflammations. Should conception occur as a result of intercourse
during the lying-in period (and this may happen very shortly
after childbirth), abortion, and even more serious consequences, are
likely to ensue. By intercourse during lactation, the premature
recurrence of the menstrual flow is induced, and the gradual reversion
of the reproductive apparatus to the condition in which it
was before pregnancy (the process of involution) is hindered; moreover,
the secretion of milk is diminished or even entirely suppressed.”
In these terms Hegar depicts the consequences of premature resumption
of marital intercourse, taking perhaps a somewhat extreme view
of the matter.
Nevertheless, this author is undoubtedly right in declaring that
one of the principal disadvantages to a woman of excessively frequent
sexual intercourse is that pregnancy occurs too often. It
is astonishing to observe the number of full-term deliveries and
miscarriages that a woman will experience within a comparatively
short period of time, as is seen too frequently among the labouring
classes and more especially among factory workers. “If we assume
the ordinary mortality of childbed to be 6 per mille, a woman who
in the course of 15 years undergoes labour (at full term or prematurely)
16 times, runs a risk of death to be expressed by the
ratio of 6 × 16 = 96 per mille; that is to say, on the average, of
1,000 women who become pregnant as often as this, nearly 1 in 10
will die in childbed.”
Young men who have previously suffered from gonorrhœa and
who wish to marry, must, unless they wish to cause unspeakable
misery, undergo an exact and thorough examination; not only must
the physician inquire as to the presence of certain symptoms, such
as smarting during micturition, adhesion of the lips of the urethral
meatus, “clap-threads” in the urine, etc., but during a considerable
period of time repeated microscopical examinations of the urine must
be undertaken, and the filaments, if present, must be examined for
gonococci. The physician will also have to determine whether any
vestiges remain of epididymitis, and whether the quality of the
semen has been impaired by the attack of gonorrhœa. Unfortunately,
it is not yet within our power absolutely to forbid marriage
to a man exhibiting all the symptoms of chronic gonorrhœa; but it
is the duty of the physician to explain to such a man the scientific
279views regarding this matter that now prevail, in order to furnish
him with the grounds for a decision.
It is not possible, when discussing the hygiene of married life,
to preserve silence respecting the extremely pressing question of
the use of measures for the prevention of conception, for in recent
years their use has become extraordinarily general, chiefly, indeed,
in the upper and middle classes of society, but to some extent also
among the working-class population. Although we devote a special
chapter to this topic, we must here express the opinion that, except
in certain instances in which their employment can be justified on
carefully weighed and well-established medical grounds, the use of
any mechanical or chemical means for the prevention of conception
must be discountenanced as injurious to health. The wife who
wishes to preserve her psychical purity and moral chastity, which is
not only possible in marriage but also greatly to be desired, must
not concern herself much with the technique of the sexual life, but
must give herself up to sexual enjoyment only as the result of a
delicate and immediate bodily and mental desire. Not only for
reasons of national economy regarding the means of providing for
the family, but also for well-grounded personal reasons regarding
the wife’s health, must the latter be spared an unduly rapid succession
of pregnancies and confinements. And this should be effected
by a certain degree of continence and by the observation of extensive
periods of sexual quiescence.
To preserve a woman’s health during the acme of her sexual
activity, a careful general hygiene is an important requisite. The
dwelling should be dry and roomy; above all the bedroom should
not be too small, neither damp nor dark, and it should be well ventilated.
The wife’s occupations should be so arranged as to afford a
suitable alternation of activity and repose, and there should be as little
night work as possible. Certain occupations are especially potent in
the causation of the diseases peculiar to women, principally, for the
reason that they do not permit of the requisite repose during menstruation.
Thus, washerwomen, vocalists, and sewing-machine operatives,
suffer with especial frequency from diseases of the genital
organs.
Great care in the cleansing of the genital organs is indispensable
in the case of women; the vulva and its environment should be frequently
and carefully washed; and an occasional vaginal injection
is advantageous. As regards the last-named measure, however, we
must point out that it is possible to err by excess as well as by
defect, and that a daily vaginal douche can by no means be regarded
as a necessary part of the hygiene of the reproductive organs. For
recent researches have shown, on the one hand, that the vagina constitutes
280a natural mechanism for the destruction of pathogenic organisms,
and on the other hand, that complete disinfection of the vagina
is extremely difficult to effect. Inflammations of the vulva, which
are somewhat frequent in consequence of excessive perspiration and
undue discharge from the genital canal, demand careful cleansing
with soap and water and the use of a soft brush. The addition to
the water of lysol (in the proportion of ¼ to ½ per cent.) is
advantageous. A general bath or a local sitz bath, the water being
moderately warm (95°–99° F.; 35°–37° C.), may be recommended
on grounds of beauty as well as of health, and should be taken at
least once a week.
The regular use of lukewarm sitz baths is a most valuable hygienic
measure for the prevention of various general or local disturbances
consequent upon increased flow of blood to the genital organs.
These local baths are best taken at a temperature of 95° F. (35° C.),
and should last twenty minutes; they should be taken just before
going to bed, and while sitting in the hip bath the skin of the abdomen
and of the lower part of the back should be rubbed with the
hand encased in a friction-glove. The bather on leaving the bath
should get straight into bed, and should dry herself beneath the bedclothes,
rubbing the skin till it glows. Such sitz baths serve also to
keep the external genitals clean, and to guard against infection. For
vaginal douching, water sterilized by boiling should be employed,
and where any catarrh of the vaginal mucous membrane is present,
some alum, permanganate of potassium, or boric acid may be added
with advantage; the pressure of water, when a vaginal douche is
given, should never be high, the reservoir of the irrigator being
raised not more than twenty inches above the outlet of the nozzle;
as a rule the water should be lukewarm; the patient should be in
the recumbent posture. The reservoir of the irrigator and the
intra-vaginal nozzle are most suitably made of glass, to insure
cleanliness; the nozzle should not be thrust too far in, two inches
being quite sufficient. After the use of the douche, the woman
should remain ten or fifteen minutes in the recumbent posture.
In addition to the hygienic employment of such full baths and
local baths, a number of mineral baths have important therapeutic
applications in cases of disease of the female genital organs, the
traditional value of such baths having been scientifically endorsed by
the modern science of balneo-therapeutics. By means of suitably
selected mineral water baths, a powerful derivative stimulus may be
given to the skin, and the affected reproductive organs may thus be
beneficially influenced. Further, in acute inflammatory conditions
or hyperæmia of the uterus or its annexa, these baths have an antiphlogistic
influence; on the other hand, when intrapelvic exudations
281have formed, the baths promote the absorption of these inflammatory
products; again, in congestive states of the female
genital organs, with relaxation, thickening, and hypersecretion of
the genital mucous membrane, the baths have an astringent and
tonic influence on the tissues; finally, they have a favorable effect
on the innervation and nutrition, not only of the reproductive apparatus,
but of the entire organism. It is easy to understand why
women during the menacme are frequent visitors to spas.
At this period of life, and especially in women who lead luxurious
“society” lives, the thoughts tend strongly in the sexual direction;
to avoid this, and to prevent the ever more and more frequent
breaches of marital fidelity, the best means are the practice of vigorous
bodily exercises, and active employment, either in household affairs
or in intellectual occupations. Cold sponging of the body or
cold full baths will also be found an excellent measure for the prevention
of sexual excess. In such cases also the diet should be
limited, strong and stimulating food should be avoided, but little
butcher’s meat should be taken, whilst green vegetables and raw
and cooked fruits should be liberally consumed; at the same time,
all alcoholic beverages must be rigidly prohibited. Moreover, care
must be taken that during the night there should be no undue physical
stimulation in consequence of excessively warm and soft bedding;
hair mattresses are to be preferred to feather beds, with light down
quilts for a covering. Finally, no stimulation of an erotic character
should be offered to the imagination, and for this reason equivocal
literature and lascivious dramatic representations must be avoided.
By a sufficiency of occupation, regular, interesting, and demanding
a considerable expenditure of physical energy, a woman may be
enabled to a great extent to escape the inconvenience and distress
attendant on entire or partial lack of gratification of the sexual
impulse.
It cannot be disputed that a certain and moderate amount of
sexual gratification is requisite for the perfect maintenance of physical
health in woman, and that the absence of this gratification, or
the gratification of the impulse in an abnormal or incomplete manner,
entails disturbance of alike the mental and the physical equilibrium;
but, on the other hand, the deleterious consequences of
sexual abstinence have been greatly exaggerated by many writers—both
by physicians and social economists. Owing to the fact that
to the cultivated woman sexual gratification is possible only in the
married state, whilst social conditions render marriage impossible
to many women greatly in need of such gratification; in consequence,
also, of the modern and ever more widely diffused practice by husbands
of coitus interruptus altogether regardless of the woman’s
need for complete sexual gratification—there arise in women numerous
282local disorders and nervous disturbances, hysteria and even
insanity being results by no means infrequent. The significance
of ungratified sexual impulse in the pathogenesis of nervous disorders
has been established by von Krafft-Ebing, who points out
that in unmarried women insanity most frequently occurs between
the ages of twenty-five and thirty-five years, during the decade,
that is to say, in which youthful bloom and the hopes of marriage
simultaneously disappear; whereas in the male sex the greatest incidence
of insanity is between the ages of thirty-five and fifty years,
the period of life in which the struggle for existence is fiercest.
Hegar, on the other hand, is a firm opponent of the view that
the favourable influence of marriage is overrated. According to
this author, the favourable effect of marriage in respect of mental
disorders is to be found, not in the gratification of the sexual impulse,
but in the ethical factors of marriage. Statistics show that
even in the favourable circumstances of marriage, sexual gratification
has in women an unfavourable influence, inasmuch as the proportion
of sufferers from mental disorders is higher among married women
than it is among married men. A study of the mental disorders
which in women are especially associated with the process of reproduction
(puerperal mania) confirms this impression. Hegar
insists that he has never seen nymphomania arise in women in consequence
of forcible repression of the sexual impulse; but that he
has not infrequently seen this disorder result from unnatural excesses
or from long-continued sexual irritation, especially in hereditarily
predisposed persons. Such unnatural stimulation of the female
is not infrequently practiced by the male—by the lover and even
by the husband—it may be because he himself derives pleasure
from such perverted practices, and wishes to obtain sexual
gratification without the risk of impregnation, or because he
is himself incompetent for normal complete intercourse. Hegar
is further of opinion that in the causation of hysteria and also
in that of chlorosis the repression of the sexual impulse plays
a quite subordinate rôle. And he regards as pure fable the belief
that continence in women is liable to lead to the formation
of mammary, uterine, or ovarian tumors. He would more
readily incline to the contrary opinion; the reproductive process
being in this respect distinctly disadvantageous to the female
sex. The unfavorable influence of the reproductive process is
shown most clearly in the case of carcinoma of the uterus; the
majority of the patients suffering from this disease are either married
or widowed, and many of them have given birth to a large
number of children. “Gratification of the sexual impulse, and more
particularly the reproductive process, give rise in women to the
283formation and growth of tumors, cause numerous mechanical disturbances,
and open the way to infection with various pathogenic
organisms.”
Hegar considers that there is hygienic justification for the limitation
of the number of children to which a woman gives birth.
The most suitable age for motherhood lies in his opinion between
the ages of twenty and forty years. Childbirth in women younger
or older than this entails too much danger both to mother and child.
At least two and a half years ought to elapse between two successive
births; and these figures give us eight as the maximum family.
If we assume that the duration of pregnancy is nine months, and
that of lactation nine to twelve months (or in cases in which the
mother does not nurse her own infant, that a like period must be
devoted to the careful supervision of the wet-nurse or of the methods
of artificial feeding), we cannot consider it unreasonable to devote
a further period of from six to nine months to the complete reestablishment
of the woman’s health. “Moreover, woman does not
exist solely for the purpose of subserving during two decades of
her life the processes of reproduction. And to permit the maximum
number of children to be as great as eight, we must presuppose
that the woman is in perfect health, and that she lives in a perfectly
healthy environment. Any illness or infirmity which renders the
duties of housekeeping and the rearing of the existing family unduly
difficult, indicates the need for a further limitation of child-bearing.
And if the reproductive function is to be rationally controlled, we
must above all attend to the age and the health of the parents.
Occupation, habitation, and general environment have also to be
considered. The correct ideal is indeed not difficult to discover.”
Hegar concludes that strict moderation and even absolute continence
in sexual matters are often, and for long periods of time,
a pressing duty. “The numerous and various disasters which are
brought upon the world by unbridled and unregulated sexual
passion can be prevented only by enlightenment, moderation, and
continence. If marriage were postponed until the attainment of
complete physical maturity, in women till the age of 20, in men till
the age of 25, while at the same time procreation were no longer
undertaken by women above the age of 40 or by men above the
age of 45 to 50 years; if, again, between successive pregnancies
a sufficient pause for the woman’s recuperation were insisted upon,
and intercurrent illnesses and states of debility were taken into
account; and if, finally, sickly individuals, those hereditarily predisposed
to disease, and those in any way below par either mentally
or physically, were more than heretofore prevented from marrying;
then the increase of population, which in Germany is unquestionably
284too rapid, would to some extent be checked. Thoroughgoing
regulation of the reproductive process will not, however, be thus
attained without the adoption of a method of selection too rigorous
for present-day notions; and for a further advance we must in
the meantime depend upon moderation and continence.” As regards
the modern demand of the “right to love,” the same experienced
gynecologist writes: “Whoever preaches to mankind the doctrine
that ‘a man sins against his own personality if he neglects to exercise
every limb he possesses, and if he denies himself the gratification
of every natural impulse,’ or the doctrine that ‘it is the duty of
every human being to gratify all his natural impulses, since these
are most intimately inter-connected with his personality—are indeed
his personality itself;’ such a preacher does harm to his kind. Such
rights and such duties are chimerical for this reason if for no other,
because two persons are necessary in the case of sexual gratification,
and sometimes—though not as often as might be wished—Hans
fails to find his Grete, without any consequent loss to society at
large.”
An especially important chapter in the history of woman at this
period of life relates to the dietetics of pregnancy and parturition,
and to the regulations to be observed for the maintenance of
health at this time and in connection with the processes of pregnancy,
parturition, puerperal involution of the uterus, and lactation.
This subject cannot now however be considered at length, and for
our present purposes it is sufficient to point out how important
it is alike for mother and child, alike for family and society, that
the ever more and more widely and generally diffused practice of the
artificial feeding of infants should be abandoned, and that there
should be a return to the natural method according to which each
mother nurses her own infant. The prevailing custom costs every
year thousands of mothers their health, and thousands of children
their lives.
Copulation and Conception.
Copulation.
The reproduction of the species is effected by means of an act of
copulation on the part of a male and a female individual, both
of whom must have attained complete sexual development. In
all the sequence of reproductive processes it is copulation alone
that is a voluntary act, all the other processes being independent
of the will and even of consciousness.
A characteristic difference between man and the lower animals
lies in the fact that in the human species sexual pleasure and the
act of copulation may occur at any season of the year; and a
285further characteristic difference may perhaps be found in the fact
that in the great majority of individuals of the human species the
psychical process of “love” plays a determinative part. Voltaire
pointed out that to man alone among animals are known the embrace
and the joy of the kiss.
The significance of the kiss is depicted by Grillparzer in the following
verses:
Auf die Hände küsst die Achtung,
Auf die Wangen Wohlgefallen,
Seelige Liebe auf den Mund.
Auf den Nacken das Verlangen;
Uberall sonsthin Raserei.[45]
In this act of conjugation between two individuals of the same
species, differentiated each from the other by the characteristics of
sex, the active, provocative rôle is allotted to the male, the passive,
receptive rôle, to the female. The modest and coy reluctance characteristic
alike of the maiden and of the wife, promote an increase
of sexual excitement in the opposite sex, and this not only in a
man of purely sensual character, whose vanity is stimulated by his
being the chosen one among many—a circumstance which, in view
of the great dependence of the sexual act upon psychical processes
and imaginative influences, is by no means devoid of importance.
The woman’s coy reluctance must be overcome by means of a
tender strategy before she is willing to grant the final possession of
her body; and the act of copulation forms at the same time the conclusion
of the physical and mental yearnings of the lover, and the
commencement of the new-coming being. There is thus a physiological
reason for the advice given by the celebrated surgeon, Ambroise
Paré, that a man, before completing coitus, should employ
some of the delicate and sensually stimulating manipulations of the
earlier stages of courtship, for, he writes, “aucunes femmes ne
sont pas si promptes à ce jeu que les hommes.”
The potency for intercourse of the sexually mature man, his
capacity for the introduction of the erect penis during the act of
copulation, is dependent on the fact that sexual excitement gives
rise to a sufficient stimulus which, acting on the erection centre
(and presuming that the centre and its afferent and efferent tracts
are normal), leads to an increased flow of arterial blood to the penis
286and a diminished outflow through the veins of that organ, and
consequently to its erection. The cerebrum is the organ in which
the sensation of libido sexualis, of sexual excitement, has its seat;
with this higher centre is connected by means of intercentral nerve
tracts a lower, mechanical, reflex centre, situated in the lumbar enlargement
of the spinal cord, and presiding over the performance
of the act of copulation; it is moreover probable that nerve fibres
proceed from the spinal cord direct to the blood vessels of the
erectile tissue, by means of which the calibre of these vessels can
be lessened or their extensibility diminished. The relation of the
erector nerves (nervi erigentes) to the penis is by many physiologists
compared to the relation of the vagus nerve to the heart. In the
quiescent state the small arteries of the penis and perhaps also the
cavernous spaces of that organ are in a state of mean contraction,
so that they offer a considerable resistance to the passage of the
blood current. When now the nervi erigentes are excited to activity,
the hitherto tonically contracted vessels of the penis undergo, according
to the school of physiologists just mentioned, relaxation, so
that they dilate under the pressure of the blood within their walls,
and, the previous resistance to the flow being now removed, the
blood pours freely into the cavernous spaces of the penis, and
distends these to the uttermost. In this manner erection is effected,
rendering possible the insertion of the penis into the genital passage
of the female; with the culmination of the sexual act, the semen is
ejaculated, the muscles of the prostate and the membranous portion
of the urethra together with the ischiocavernosus and bulbocavernosus
muscles, all acting strongly and simultaneously.
By the contraction of the muscular apparatus just described, the
penis is constricted in the neighborhood of the pubic symphysis,
and this further hinders the outflow of the blood from the corpora
cavernosa, increasing the intensity of the state of erection of the
penis. Should the relaxation of the corpora cavernosa, dependent
upon the stimulation of the nervi erigentes, be incomplete, it is not
possible for sufficient blood to pass into the cavernous spaces to
exercise considerable pressure upon the efferent veins, and thus
complete erection fails to occur. If, again, the contraction of the
muscular apparatus at the root of the penis is insufficiently vigorous,
complete erection likewise fails to occur; the organ becomes semi-erect
only, or erect for a period too short to permit of the completion
of intercourse.
Since, physiologically speaking, conception is the purpose with
which copulation is effected, the ejaculation of the semen must
be regarded as the principal object of that act; now in normal
conditions, ejaculation takes place only when the penis is fully erect.
287Associated with the erection of the corpora cavernosa is a swelling
of the caput gallinaginis, whereby the orifices of the ejaculatory
ducts are directed forwards toward the membranous portion of the
urethra, and at the same time the backward passage to the bladder
is cut off. By this mechanism, the urethra, which usually serves
as the canal for the outflow of urine, is made for the time being
solely subservient to the purposes of the sexual act. That the outlet
from the bladder is obstructed by the swollen caput gallinaginis
when the penis is erect, is shown by the familiar fact that a man
whose penis is erect cannot pass water, although the way is freely
open for the ejaculation of the semen.
Before ejaculation begins, the urethral glands already begin to
secrete; and when erection is powerful and prolonged, this secretion
often makes its appearance at the urethral orifice in the form
of drops of a clear somewhat tenacious fluid. Ultzmann considers
that the function of this secretion is probably to moisten the walls
of the urethra, over which the acid urinary secretion is continually
flowing, with a protective alkaline fluid, and thus to prepare the
canal for the passage of the semen. An analogy may be found in
the secretion of the cervical glands of the uterus in the female, for
this secretion has been found to enhance the activity of the movements
of the spermatozoa. If now during copulation the moment
of ejaculation begins, the male experiences at the same time a sense
of voluptuous pleasure and a feeling of muscular spasm in the
perineal region, and this indicates the commencing evacuation of
the contents of the seminal vesicles through the ejaculatory ducts.
Simultaneously, the secretion of the prostate is poured into the
urethra. The semen now gradually passes out through the narrow
ejaculatory ducts, and, since in consequence of the swelling of the
caput gallinaginis, it cannot pass backwards towards the bladder,
it runs forwards, and accumulates in the bulb of the urethra, the
physiological excavation of that tube. As soon as a considerable
quantity of the semen has collected in this situation, so that the
bulb of the urethra becomes distended, reflex contractions of the
bulbocavernosus muscles ensue, by means of which the seminal
fluid is forced out of the urethral orifice. In cases in which this
muscular apparatus does not function properly, as in the paralytic
form of impotence, the semen during ejaculation is not ejected in a
forcible jet, but rather flows slowly, as from a lax tube partially
filled with fluid, from the urethral orifice.
We are indebted to Roubaud for a classical description of the
phenomena of copulation, and this description is here appended.
It runs as follows: “As soon as the penis enters the vaginal vestibule,
it first of all pushes against the glans clitoridis, which yields
288and bends before it. After this preliminary stimulation of the two
chief centres of sexual sensibility, the glans penis glides over the
inner surfaces of the two vaginal bulbs; the collum and the body
of the penis are then grasped between the projecting surfaces of
the vaginal bulbs, but the glans penis itself, which has passed
further onward, is now in contact with the fine and delicate surface
of the vaginal mucous membrane, which membrane itself, owing to
the presence of erectile tissue between its layers, is now in an elastic,
resilient condition. This elasticity, which enables the vagina to adapt
itself to the size of the penis, increases at once the turgescence and
the sensibility of the clitoris, inasmuch as the blood that is driven
out of the vessels of the vaginal wall passes thence to those of the
vaginal bulbs and the clitoris. On the other hand, the turgescence
and the sensitiveness of the glans penis itself are heightened by
compression of that organ, in consequence of the ever increasing
fulness of the vessels of the vaginal mucous membrane and the two
vaginal bulbs.
“At the same time the clitoris is pressed downward by the anterior
portion of the compressor muscle, so that it is brought into
contact with the dorsal surface of the glans and of the body of the
penis; in this way a reciprocal friction between these two organs
takes place, repeated at each copulatory movement made by the two
parties to the action, until at length the voluptuous sensation rises
to its highest intensity and culminates in the sexual orgasm, marked
in the male by the ejaculation of the seminal fluid, and in the female
by the aspiration of that fluid into the gaping external orifice of the
cervical canal; so true, indeed, is this, that it is a difficult matter
to give a picture at once accurate and complete of the phenomena
attending the normal act of copulation. Whilst in one individual
the sense of sexual pleasure amounts to no more than a barely
perceptible titillation, in another that sense reaches the acme of
both mental and physical exaltation.
“Between these two extremes we meet with innumerable states of
transition. In cases of intense exaltation, various pathological
symptoms make themselves manifest, such as quickening of the
general circulation, and violent pulsation of the arteries; the venous
blood, being retained in the larger vessels by general muscular contractions,
leads to an increased warmth of the body; and further,
this venous stagnation, which is still more marked in the brain in
consequence of the contraction of the cervical muscles and the backward
flexion of the neck, may cause cerebral congestion, during
which the consciousness and all mental manifestations are momentarily
in abeyance. The eyes, reddened by injection of the conjunctiva,
become fixed, and the expression becomes vacant; lids close conclusively,
289to exclude the light. In some, the breathing becomes
panting and labouring; but in others, it is temporarily suspended, in
consequence of laryngeal spasm, and the air, after being pent up for
a time in the lungs, is finally forcibly expelled, and they utter incoherent
and incomprehensible words.”
The impulses proceeding from the congested nerve-centres are
confused. There is an indescribable disorder both of motion and
of sensation, the extremities are affected with convulsive twitchings,
and may be either moved in various directions or extended straight
and stiff; the jaws are pressed together so that the teeth grind
against each other; and certain individuals are affected by erotic
delirium to such as an extent that they will seize the unguarded
shoulder, for instance, of their partner in the sexual act, and bite
it till the blood flows.
A period of exhaustion follows, which is the more intense in proportion
to the intensity of the preceding excitement. The sudden
fatigue, the general sense of weakness, and the inclination to sleep,
which habitually affect the male after the act of intercourse, are
in part to be ascribed to the loss of semen; for in the female, however
energetic the part she may have played in the sexual act, a
mere transient fatigue is observed, much less in degree than that
which affects the male, and permitting far sooner of a repetition of
the act. “Triste est omne animal post coitum, praeter mulierem
gallumque,” wrote Galen, and the axiom is essentially true, at any
rate so far as the human species is concerned.
The question has been mooted, and many earnest inquirers have
devoted much thought thereto, whether in this moment of most
intense sexual gratification it is the male or the female that experiences
the greatest amount of pleasure. As in the case of all
questions the data for the solution of which are at once very various
and very variable, so in this case also, very different opinions have
been put forward. “In fact,” writes Roubaud, “when we take into
consideration all the circumstances by which the intensity of sexual
sensation is influenced, it may well be doubted if it is at all possible
to find an a priori solution for the problem. When we take into
consideration the influence exercised by temperament, constitution,
and a large number of conditions both general and special, on
sexual sensibility, we cannot fail to be convinced that this problem,
in consequence of all the complicated characteristics it presents, is
actually insoluble.”
In regard to the pleasure experienced in the act of intercourse,
a remarkable distinction is drawn by Gutceit. The male, in every
case and with every woman, experiences the full degree of pleasure;
and even though from the mental point of view this pleasure may
be enhanced by inclination, attraction, and mutual love, from the
290physical point of view there is no difference between different acts
of intercourse, so that the cynical old Roman was right when he
wrote. “Sublata lucerna nullum discrimen inter foeminas.” But
in the case of the female it is very different. Her first experience
of sexual relations is a very painful one, and this pain prevents all
enjoyment as long as it continues, as it does in many women for
one, two, or even four weeks. And when this period is once over,
not more than two women in every ten experience the pleasure
of sexual intercourse in its full intensity. Of the remaining eight,
four have indeed an agreeable sensation during the rubbing movements
of the sexual act, but it is a long time before they experience
a sensation analogous in its intensity to that which in man accompanies
the act of ejaculation. In some women it may be six months
after marriage before the true sexual orgasm is experienced, in
others it may be a year, or even several years; in a considerable
number this does not happen until after they have given birth to
several children. As a result of numerous observations on this
point, Gutceit asserts that in women sexual pleasure is experienced
only in intercourse with a man who is beloved, or against whom, at
least, no repulsion is felt; and that no pleasure is felt by a woman
in intercourse with a man towards whom she feels an actual dislike.
Further, he maintains, that a woman, loving another man, and
feeling pleasure in intercourse with him, has on the other hand no
voluptuous sensations during intercourse with her husband, whose
embraces she permits only from a sense of duty. Thus in the male,
intercourse is always pleasurable, while in the female, pleasure is
experienced only when certain conditions are fulfilled.
Contact with the male genital organs stimulates in the female
the sensory nerves of the vulva, the vestibule, and the vagina; the
nervous stimulus is transmitted to the cerebral cortex, where it
gives rise to the sensation of sexual pleasure, and causes, through
the intermediation of the genito-spinal centre, a number of reflex
actions. As sensory nerve terminals of such reflex arcs, the final
ramifications of the pudic branch of the sciatic plexus play the most
important part; in the clitoris these nerves are beset with a peculiar
kind of end-bulbs, the genital corpuscles discovered by W. Krause;
from their structure these corpuscles seem admirably adapted to
respond to the very slightest stimulation, producing voluptuous
sensations and perceptions, and giving rise to various reflex manifestations.
The first part of the path of the afferent impulses by
which sexual pleasure is aroused is constituted by the dorsal
nerves of the clitoris. The reflex changes consequent upon sexual
excitement begin already in the vestibule, inasmuch as the secretion
of Bartholin’s glands, which are compressed by the action of the
291constrictor cunni muscle, is expelled during coitus, the secretion,
owing to the situation of the orifices of Bartholin’s ducts, passing
over the external genitals. The clitoris becomes erect; the blood in
the bulbs of the vestibule, the venous plexus situated around the
margin of the vestibule along the boundary between the labia majora
and the labia minora, is pressed into the glans clitoridis, the
erection and sensibility of this structure being proportionately
heightened. By the action of the constrictor cunni and ischiocavernosus
muscles, the clitoris, the distal extremity of which is bent
downwards at a right angle, is drawn down and pressed against the
penis.
At the entrance of the vagina is the sphincter vaginæ muscle,
whose action is reinforced by muscular fibres running in the middle
coat of the vagina itself. It is probable that the muscular activity
of the vagina and the uterus facilitates the entrance of the semen
into the cavity of the uterus.
Dorsal decubitus is rightly regarded as the most correct position,
physiologically speaking, for the woman to assume during coitus.
That from the earliest times and in the most diverse races, this
position has been customary, is shown by numerous antique paintings
and statues, and by the reports of those who have studied
the customs of savage races. Various other positions are, however,
occasionally assumed; thus, Ploss and Bartels report, that
among the Soudanese, coitus is practiced in the erect posture, with
the man standing behind the woman; that among the Inuits
(Eskimo), the act is performed in the manner usual among quadrupeds;
that among the Swahelis in Zanzibar, and among the indigens
of Kamschatka, the lateral posture is customary; and that
among the Australian blacks, coitus is usually effected in the crouching
posture, both parties squatting on their hams. The same
writers remind us, that in the old calendars of the fifteenth, sixteenth,
seventeenth, and eighteenth centuries, definite commands
and prohibitions for the conduct of marital intercourse are to be
found, and that lucky and unlucky days, respectively, are specified
for the performance of the act. These recommendations would
appear to be relics of antiquity, for in the Sanscrit work Kokkogam,
under the heading “Sexual Intercourse According to the
Days of the Month,” exact instructions are given for the proper
performance of coitus.
In the Kamasutra (the Indian ars amatoria, a work only in
recent days rendered accessible to European readers in the translation
of R. Schmidt), several chapters are devoted to the detailed
description of the various methods of copulation, and rules are
given for the carnal union of man and wife. But, as the Indian
292author justly remarks, “Rules are of value only for the control of
moderate desire; when the wheel of passion has once begun to roll,
to prescribe a course is no longer of any avail.” In this work,
sixty-four varieties of erotic enjoyment are enumerated, and we
find an explicatio coitus secundum mensuram, tempus, naturam, de
modis inter coitum procumbendi, de minis coitibus, de coitu inverso,
de viri inter coitum consuetudinibus.
At times, in order that coitus may be effective, some other
position than the natural one is indispensable. Such a necessity
has been recognized even by theologians, by whom any divergence
from nature in this matter has usually been regarded as sinful. For
instance, in the work of Craisson, De Rebus Venereis ad Usum
Confessariorum, we read: “Situs naturalis est ut mulier sit succuba
et vir incubus, hic enim modus aptior est effusionis seminis virilis
et receptioni in vas femineum ad prolem procreandum. Unde si
coitus aliter fiat, nempe sedendo, stando, de latere, vel praepostere
(more pecudum), vel si vir sit succubus et mulier incuba, innaturalis
est.... Sed tamen minime peccant conjuges si ex justa causa
situm mutent, nempe ob aegritudinem, vel viri pinquetudinem, vel
ob periculum abortus; quandoque ait St. Thomas, sine peccato esse
potest quando dispositio corporis alium modum non patitur.”
In certain pathological states, as for the prevention of sterility,
an abnormal posture during coitus may advantageously be recommended,
in order to favour the entrance of the semen into the
cervical canal, and to allow the semen to stay longer in the vagina
before it flows out. An old and often efficacious means for this
purpose is the performance of coitus with the woman in the knee-elbow
posture. In order to favour the entrance of the semen into
the deeper portion of the genital tract, Hegar and Kaltenbach
recommend that after coitus the woman should remain for some
time in the knee-elbow posture, while the man from time to time
gently presses up the anterior abdominal wall, and then abruptly
relaxes the pressure.—In the Talmud, coitus was regarded as unfruitful
if performed when the woman was in the erect posture.
Casper reports the case of a woman with severe scoliosis, who had
long remained sterile, and who only conceived (and was subsequently
happily delivered) after performing coitus in the abdominal
decubitus.
Guéneau de Mussy suggests the following, very characteristic,
method of ensuring fertilization, one which also certainly dates
from great antiquity: “Sed haud illicitum mihi visum est, si post
diversa tentamina diutius uxor infecunda manserit, ipsum maritum
digitum post coitum in vaginam immittere, et ita receptum semen
uteri osteo admovere. Et cum ostiolo uteri haeret, ut in pervium
293canalem spermatozoidum motibus faventibus, prodeat, sperare non
absurdum.” Eustache reports a case, the wife of a physician, in
which this manoeuvre was effective in ensuring conception.
A similar procedure has been employed with success by Kehrer,
in a case of enfeebled potency on the part of the male, leading to
premature ejaculation. A speculum was introduced into the
vagina, and through this instrument the semen, ejaculated in consequence
of sexual excitement, was introduced into the vaginal fornix;
conception ensued. In an analogous manner, A. Peyer recommended,
in a case of partial impotence, in which special manipulations were
needed to bring about ejaculation, that conception should be
favoured in the following manner: Erection having been effected
by ordinary sexual contact, the manipulations needed to produce
ejaculation were carried out, and the penis was intromitted into the
vagina the moment before ejaculation occurred. This has been
done with fruitful results. Englisch reports the case of a hypospadiac
who, in order to render coitus effective, used a condom in
the anterior extremity of which he made an aperture. In this
way he became the father of three children.
In very obese men with extremely protuberant abdomens, we
may recommend for the furtherance of conception that they should
have intercourse with their wives a parte posteriori; and the same
recommendation may be made in cases in which the wife herself is
extremely obese. In Australia, it is said that among the indigens,
coitus is usually practiced a posteriori; and there is a saying in the
Talmud to the effect that sexual intercourse performed in the
ordinary manner does not lead to the conception of infants so good,
wise, talented, and promising as those whose conception is the
result of coitus a posteriori. Mohammed, on the other hand, declares,
“Your wives are your tillage, go therefore unto it in whatsoever
manner ye will.”
In cases of retroflexion of the uterus, with a markedly forward
direction of the vaginal portion of the cervix, I have recommended
to the husband that he should perform coitus with his wife in the
upright sitting posture. In this posture the fundus uteri passes
downwards and forwards, whilst the vaginal portion of the cervix
passes upwards and backwards.
In cases of retroversion of the uterus with the formation of a
cul-de-sac in the posterior vaginal fornix, Pajot recommends, with
the aim of temporarily restoring the uterus to a position in which
the occurrence of conception is favored, that for three or four days
prior to coitus the patient should retain the fæces, eating the while
freely of eggs and rice, and taking a small opium pill every evening;
in cases of anteversion, the patient should retain her urine for
294a considerable time—five or six hours—before coitus; and in
cases of lateral version he recommends that the patient should have
intercourse while lying on that side towards which the vaginal portion
of the cervix is directed.
Edis recommends that in cases in which there is sterility dependent
upon backward displacements of the uterus, that the organ
should be replaced while the patient is in the genu-pectoral posture,
and a pessary inserted; coitus should then be effected without the
patient’s changing her posture.
In the human species as compared with the lower animals, there
has been a notable diminution in the frequency of the separate acts
of intercourse, a diminution dependent upon the higher vital aims
of the former. Burdach formulates as a physiological law that the
frequency of sexual intercourse is inversely related to the duration
of the act.
Amongst all civilized races, sexual intercourse ceases during menstruation,
since in the normal man there is aversion to intercourse
with a menstruating female.
By the Mosaic law, intercourse with a woman during menstruation
and for seven days after the cessation of the flow, was forbidden
under pain of death. The Talmud further ordains that a purifying
bath shall be taken by the woman a week after menstruation. By
intercourse itself, moreover, both man and woman were rendered
unclean to the evening; and, according to the Mosaic law, both must
bathe after the act of coitus. In the Koran, also, intercourse is forbidden
during menstruation, and until the woman has been purified
with water. The law’s of Islam demand from a man who marries
a virgin that he shall have intercourse with her the first seven nights
in succession; whilst he who marries a wife no longer virgin, needs
to visit her only the first three nights in succession. Subsequently,
during married life, the Mohammedan shall have intercourse with
his wife regularly once a week. Amongst many savage races, intercourse
is forbidden with a woman during pregnancy, the puerperium,
and lactation.
The first act of intercourse is difficult and painful to the virgin.
At times the rupture of the hymen is exceedingly difficult. Even
after this, it is some time before genuine pleasure is experienced
in sexual intercourse.
To the female, intercourse is harmful when performed with undue
frequency, or during menstruation, or indiscriminately throughout
pregnancy, or during the puerperium, or incompletely or in an
unnatural manner, or finally when performed in an unsuitable bodily
attitude.
“Unduly frequent performance of the act of coitus,” writes
Hegar, “which is liable to occur either in marital or in illicit intercourse,
295gives rise to anæmia, defective nutrition, muscular weakness,
intellectual and nervous exhaustion. Young and healthy individuals
recuperate rapidly after excesses of brief duration, as is
often seen in young married pairs. Sickly and elderly persons, on
the other hand, are much more severely affected by sexual excess,
and recover therefrom but slowly if at all. Long continued sexual
excesses ultimately wear out even the strongest.”
Intercourse effected by force, or with a girl of immature age, is
distinguished as rape, a punishable offence both in Germany and in
Austria. The offence is defined as extra-marital intercourse with a
female under the age of fourteen years, with or without the latter’s
consent; or extra-marital intercourse with a female of any age
against her will or deprived of the power of resistance—either by
the use of actual force, by the employment of threats, or by loss of
consciousness. With regard to the last specification, the law regards
as rape intercourse with a woman unable to resist through
loss of consciousness, whether that loss of consciousness is or is not
produced by the direct action of the violator.
In the female, the act of intercourse, alike physically, in its natural
consequences, and mentally, is at once more difficult and of more
enduring results than in the male. A writer of the new school,
who according to his own admission has no other interest than the
study of the sexual life, writes of himself: “I have often enough had
intercourse with members of the other sex, in a few cases, indeed,
out of pure inclination; but in all cases alike the aim and the result
were the same—as soon as I had gained my end, the affair was
finished. Passion, a bestial act, exhaustion, commonly a feeling of
loathing; in the best possible case a fugitive but not an agreeable
memory; voilà tout.” To women, such a description, happily, is
applicable only in the most exceptional cases.
With the completion of coitus, the voluntary and conscious action
of the two parties to the act is at an end; the subsequent stages of
the function of generation are independent alike of consciousness
and will.
When complete intromission of the penis has been effected, and
ejaculation takes place, the semen is usually deposited at the os
uteri or in the immediate neighborhood of that orifice. During
the act of ejaculation, a peristaltic contraction of the vagina occurs,
by means of which the semen at the os uteri is subjected to a moderate
degree of pressure; the contraction and the pressure may
perhaps persist for some little time after the completion of the
coitus. In rabbits on heat, such contractions of the vagina, by
means of which the semen was forced under pressure into the interior
of the uterus, have been actually observed.
During coitus, the uterine muscle is also active. During strong
296sexual excitement, the uterus descends in the pelvis, the downward
movement being increased by the pressure on the woman’s abdomen.
The os uteri externum is drawn open, and the aperture, hitherto
flattened, now becomes rounded. At the same time, the secretion of
the cervical glands is expelled, and small quantities of semen are
sucked into the cervical canal. The plicae palmatae offer a certain
hindrance to the entrance of the semen; but the surface of the interior
of the canal is rendered much smoother by the free secretion
of mucus by the cervical glands. Further, it appears highly probable
that during the excitement of coitus, the mouths of the Fallopian
tubes, ordinarily more or less tightly closed, become widely opened,
so that the entrance of the spermatozoa is favored.
The muscular movements of the uterus were observed by J. Beck
in a woman suffering from prolapse. During sexual excitement, the
os uteri opened and closed rapidly five or six times in succession,
remaining at last firmly closed. Further, in bitches on heat, Basch
and Hoffmann observed the vaginal portion of the cervix to descend
in the vagina, the os uteri opened, mucus was extruded, and the
os was then retracted.
Hohl, Litzmann, and others have reported, that in women endowed
with great nervous susceptibility, friction of the vaginal
portion of the cervix with the finger arouses sexual sensation, with
rounding of the os uteri externum, descent of the uterus, and hardening
of the vaginal portion; this latter is regarded by Graily
Hewitt and by Wernich as a necessary accompaniment of copulation.
Henle believes that the hardening and protrusion of the vaginal
portion of the cervix are due to a change in the tension of the
delicate vessels of this structure, which have an exceptionally thick
muscular coat; Rouget compares the mechanism with that by which
erection of the penis is produced. These authors consider that
sexual excitement is indispensable for the erection of the vaginal
portion of the cervix.
Thus, Hohl writes: “Numerous observations have shown that in
females endowed with a considerable degree of nervous susceptibility,
and especially in nulliparae, during examination and during
any increasing irritation, not only is there an increased secretion
of the vaginal mucus, but also a momentary descent of the uterus
and an opening of the os uteri externum, so that this orifice has
the appearance for the instant of the open mouth of a tube.” Litzmann
reports that during the vaginal examination of a young, extremely
erethistic woman, the uterus suddenly assumed a more
vertical position, and came lower down in the pelvis; at the
same time, the lips of the cervix became equal in length, the os
uteri externum became rounded, soft, and penetrable by the finger;
297whilst the breathing and the voice indicated the occurrence of intense
sexual excitement. Rouget assumes that the body and the
fundus of the uterus constitute an erectile organ, which however
possesses capability for erection only during the period of ovulation;
Hewitt, on the other hand, considers it extremely probable that the
erection may occur at any time during sexual intercourse, whether
ovulation is proceeding or not. A. Wernich considers, basing his
views in part on personal observations, that erection of the lower
segment of the uterus occurs, like erection of the penis, whenever a
moderate degree of sexual excitement is experienced; in women,
however, he believes that erection is seldom extreme, and that it
declines with the other symptoms of sexual excitement, viz., flushing
of the face, moisture and glistening of the eyes, peculiar groaning
expiration, etc. Whereas during ovulation, erection is merely
a necessary concomitant of the other menstrual processes; during
coitus, erection not only occurs much more powerfully, but it is
also an important—perhaps the most important—contributory
factor in effecting fertilization.
It is no longer possible to accept the view of earlier physiologists
that the purpose of this erection of the lower segment of the
uterus is “to constitute with the penis a continuous canal between
the male and the female genital organs.” Contact between the
glans penis and the os uteri externum is not indeed an occurrence
of extreme rarity; but, on the other hand, it is in no sense a constant
nor even a frequent incident of sexual intercourse. It is ejaculation,
especially, which is subserved by the erection of the vaginal
portion of the cervix. In the female, ejaculation occurs at the moment
of the most intense sexual pleasure, and is marked by the
evacuation from the os uteri externum of a moderate quantity of
mucous fluid with an alkaline reaction. In some cases, in which a
chronic discharge of this cervical mucus occurs, it forms an
elongated coagulum of delicate vitreous jelly, the “mucus-string”
of Kristeller. The last-mentioned author is of opinion that the
spermatozoa slowly, but by active movements, find their way along
this string into the cavity of the uterus. This assumption, however,
is met by C. Mayer and Marion Sims with the objection, that
Kristeller’s observations were for the most part carried out on
women who were out of health, and that a gelatinous secretion of
this character obstructs the orifice of the cervical canal, and hinders
the occurrence of conception. From the erection of the portio
vaginalis during sexual excitement, and its sudden relaxation post
cohabitationem, Wernich deduces the occurrence of a process of
aspiration, by which the semen is drawn up through the cervical
canal into the cavity of the uterus; a process which has been seen
298in actual occurrence in vivisected animals. It is said that to many
women this feeling of a process of suction is so well known, that
thereon, in association with the consequent almost complete absence
of mucus and seminal fluid from the vagina, they are accustomed
to base a belief that conception will occur. It is said that
this aspiratory activity on the part of the uterus may be perceived
during coitus by the male also (?). It is assumed by Grohe that
the wave motion of the cilia of the epithelium lining the cervical
canal, is of importance in promoting the ascent of the spermatozoa;
it may be that the vibration of the cilia exercises a motile stimulus
on the spermatozoa, it may be that the continually repeated stroke
of the cilia serves to prevent the permanent agglutination of the
spermatozoa into groups.
According to Sims, the aspiratory action of the uterus is effected
in the following manner: By the contraction of the constrictor
vaginae superior muscle, the cervix is pressed downwards against
the glans penis, and by this pressure its contents are evacuated; the
parts then relax, the uterus suddenly returns to its normal state, and
thus the seminal fluid with which the vagina is filled is drawn into
the interior of the cervical canal.
Eichstadt also attributes to the uterus an aspiratory force, dependent
upon coitus, and competent to force into the interior of the
uterus the semen ejaculated into the os uteri. The changes in the
uterus which are the necessary antecedents of this aspiration,
namely, an engorgement with blood whereby the flattened form of
the uterus gives place to a more rounded form, and the cavity of
the organ is increased in capacity, take place, in the opinion of this
author, only when during intercourse the woman has attained the
acme of sexual gratification, by which alone can the aforesaid
change in the uterus be brought about. E. Martin and Chrobak
have also directed attention to the fact, that some importance in
this connexion must be attached to the facultative enlargement in
the size of the os uteri externum.
Lott, by his researches into the behaviour of the cervix uteri in
relation to the act of conception, is led to the conclusion that the
locomotive capacity of the spermatozoa forms the principal factor
in effecting a fertilizing contact between the spermatozoa and the
ovum. This locomotive capacity may be increased or diminished
by a number of conditions, among which the principal are: the
activity of the cervix uteri (the ciliated epithelium); the character
of the secretions; and the position, shape, and size of the cervix.
299Thus, this author concludes, the part played in conception by the
normal cervical canal is a purely passive one, with the sole exception
of the activity of the ciliated epithelium—and the influence of this
factor must be regarded as extremely doubtful. That during
ejaculation the external orifice of the male urethra and the os uteri
externum are in close apposition, is denied by Lott, who adduces in
support of his views data derived from comparative investigations
on various animals. In the dog, the configuration of the genital
organs is such that it is impossible to suppose that any apposition
can occur; the same is the case with the sheep; and still more so
with the rabbit, who possesses two quite distinct portions vaginales,
projecting freely into the vagina. In the human species also,
the character of the walls of the cervical canal, where in the normal
state the plicae palmatae may almost be said to interlock, separated
only by a thin stratum of mucus, offers a hindrance to the entrance
of the ejaculated semen by the direct force of ejaculation itself.
As regards the independent motile powers of the spermatozoa, the
researches of Lott showed that not only can they overcome strong
capillary currents, and can traverse the width of a coverglass
(18mm.—about ¾ in.) in about five minutes; but further that they
are capable of migration through the finest interstices (those of an
animal membrane) provided that the fluid with which the membrane
is moistened is one favourable to their vital activity.
Kehrer, who in general supports the view that the modus coeundi
and an active attitude on the part of the female have an important
influence on the occurrence of conception, assumes that independent
contractions of the cervix occur, whereby is expelled the delicate
plug of mucus that fills the cervical canal and offers an obstacle
to the passage of the spermatozoa. He believes that the duration
of the act of intercourse, the mechanical relations between the penis
and the vagina, the activity of the uterine muscle, the secretory
activity of the utero-vaginal mucosa during the act, and the posture
of the female post coitum, are all important factors in the occurrence
of conception. Thus, he believes that if during intercourse
there is a failure of the uterine contractions, which should expel
the plug of cervical mucus, the semen flows away without effecting
fertilization; if an unsuitable posture is assumed during intercourse
the woman remains sterile, but can be fertilized without difficulty
by coitus effected in the proper manner.
Haussmann has shown, that in the same woman, and in similar
conditions, spermatozoa will on one occasion be found in the cervical
300canal, and on another occasion will not be found there; and
he has further shown, that in some women we fail to find spermatozoa
in the cervical canal in circumstances in which, in other
women, we regularly find them in that situation.
Far as we may be from a complete knowledge of the conditions
upon which conception depends, this at least is certain, that the
passage of spermatozoa through the os uteri externum is a sine
qua non of fertilization. Indeed, it would seem that we must accept
as true the assumption of Meyerhofer, that fertilization is
possible only if the semen passes at once into the cervical canal,
mingles, that is, at once with the alkaline cervical mucus—unless,
indeed, the coitus takes place during the catamenial flow, when
the blood has neutralized the acid reaction in the vagina, or takes
place when some morbid condition has had the same result. The
theory of Johann Müller, regarding the piston-like action of the
penis during coitus, by which the semen is actually forced through
the cervix, must be rejected; equally unsound is Holst’s assumption
that during intercourse the semen is ejaculated through the enlarged
cervical canal directly into the cavity of the uterus. It would appear,
however, to be a necessary condition of fertilization, that the
semen should be ejaculated into the uppermost segment of the
vagina, so that the fluid comes into actual contact with the os uteri
externum; it may be that the alleged aspiratory force of the uterus
then comes into play, by means of which the semen is sucked into
the cavity of that organ; it may be, on the other hand, that Beigel
is right in his theory of the existence of a receptaculum seminis,
formed by the anterior and posterior lips of the cervix uteri and
the uppermost segment of the vagina—in this space, he supposes,
a part of the semen is retained in contact with the orifice of the
cervical canal.
It is, also, exceedingly probable that during coitus a reflex nervous
mechanism becomes active, by means of which the uterine
orifices of the Fallopian tubes are opened, the vaginal portion of
the cervix descends in the vagina, the os uteri externum enlarges,
the orifice becoming rounded where before it was flattened, and
finally small quantities of semen may be aspirated into the cavity of
the uterus.
I further regard it as important in promoting conception, that
simultaneously with the changes above described, the reflex nervous
stimulation should lead to the secretion by the cervical glands
of a gelatinous material, alkaline in reaction, and therefore adapted
301to increase the locomotive powers of the spermatozoa, so that these
latter, aided by the activity of the ciliated epithelium lining the
cervical canal, will gain the interior of the cavity of the uterus, and
thence pass onwards to the Fallopian tubes. The significance of the
glands in the mucous membrane lining the cervical canal has hitherto
been underestimated in this connexion.
Whereas in the primitive state of mankind, among savage races
at the present day, as among our own prehistoric ancestry, nakedness
is the rule, so also intercourse in these circumstances is effected
altogether without any regulation by law or custom, on the
mere prompting of unbridled natural passion, and, moreover, there
is the fullest promiscuity in sexual relations; but civilization has led
man to impose restraints upon sexual intercourse, and has introduced
marriage as a sacred institution. Among certain primitive
peoples, however, among whom the wives are common to all the
men, transitory pairings nevertheless occur, especially when a
woman becomes pregnant; to cease, however, during the period of
lactation. “This is the origin of marriage, which has evolved
from rape and prostitution, as law has evolved from crime”
(Lombroso). This author makes an interesting observation when
describing the entire freedom of sexual intercourse that obtains
among the Red Indians of North America, to the effect that “often,
times of general promiscuity occur, as with rutting animals, generally
in the warm season of the year, when nutriment is abundant;
it is difficult to indicate any distinction between the tumultuous
orgies of the baboon, and those of the Australian Blackfellows,
among whom the sexes keep apart during the greater part of the
year, to intermingle like rutting beasts during the season of the
yam-harvest.”
The paths of civilization, from the complete promiscuity of sexual
intercourse to the lofty ideal of life-long monogamic union, has not
been a straightforward one, but has been marked by various aberrations
of sexual relationship; hetairism, prostitution, polyandry, incest,
rape, the jus primae noctis, etc. The anthropologist is able
to trace the successive stages of the development of the institution
of monogamic marriage; the community of wives within the clan;
free sale of wives and daughters; bestowal of a man’s wife or concubine
for the honour of a guest; ritual prostitution for the honour
of the gods and at numerous religious festivals; æsthetic and literary
hetairism, with bestowal of favours according to free inclination;
community of wives among all males of the same family; the
302claim of the wife to as many as five or six husbands; the right of
brothers to their sisters; the defloration of virgins by the priests in
heathen temples; the temporary possession of the wife by the chief
of the community, prior to her possession by her permanent husband;
defloration of the bride by the bonze before her marriage;
the feudal right of the mediæval seigneur to the prima nox of the
bride of his retainer.
In the lower stages of civilization, copulation appears so natural
an action that it is performed in public entirely without shame.
Thus, Cook, in his first voyage, describes having seen an indigen
engage in sexual intercourse with a girl of eleven years, under the
very eyes of the queen, with whom Cook was then having audience;
the sexual act was, according to Cook, the favourite topic of conversation
between the sexes. Herodotus reports that many peoples
of antiquity had no regard for privacy in sexual intercourse, but
that, like the lower animals, they had connexion in any company.
In the Bible, also, it is recorded that sexual intercourse was practised
in public: “So they spread Absalom a tent upon the top of
the house; and Absalom went in unto his father’s concubines in the
sight of all Israel.” (II. Samuel, XVI. 22.) According to
Athenaeus, the Etruscans, at their public banquets, were equally unrestrained.
Plutarch reports that among the Spartans the maidens
and the young men went about naked together. Even, indeed, after
the sense of modesty had begun to develop, it was long before any
secret was made about the act of intercourse. In classical antiquity,
it was very frequently the subject of pictorial and plastic representation.
Even in more recent days, there have been artists who have not
hesitated to depict the sexual act: thus we have the Venus with a
Faun by Caracci; the Jupiter and Io of Correggio; the Leda and the
Swan of Tintoretto; and similar pictures by Luca Giordano, Rubens,
Titian, and Franceschini.
Even in the early centuries of the Christian era, the sect of the
Adamites practised intercourse openly in the light of day, on the
ground that that which was right in the dark, could not be wrong
in the light. The same is reported of the sect of Turlupins, in
France in the fourteenth century. We cannot refrain from quoting
at length from Lombroso and Ferrero a passage relating to the
evolution of sexual manners in the female sex (Woman as Criminal
and Prostitute): “In the lowest stages of development, the feeling
of modesty is entirely wanting; limitless freedom in sexual
intercourse is the general rule; and even where no system of
303promiscuity prevails, marriage rather fosters than discourages prostitution,
especially in countries in which husbands are accustomed
to expose their wives for sale. This fact may be brought into relation
with the well known lasciviousness of apes and other animals
high in the scale, showing that sexual excitability increases pari
passu with intelligence, so that to man it is as impossible as to an
ape to satisfy his sexual needs with a single female. Whilst among
the apes, a single male possesses a number of wives, we find in the
gregarious life of primitive man that community of wives has taken
the place of polygamy, which institution, however, reappears in a
higher stage of culture for the benefit of the more powerful masculine
natures.
“To the dominion of prostitution as a normal institution succeeds
the period in which it persists as a variously metamorphosed survival:
it may be as the duty of the wife to surrender her person to
any other male of the same family; or the woman may have to
bestow her favors on a religious or political chief, as in the institution
of temple-prostitution, where the wife must give herself, it may
be to any one and at any time, or it may be to defined persons only
and at stated festivals. Frequently we meet with another development
of prostitution, finding that while the wife must remain chaste,
the unmarried woman is allowed unrestricted intercourse; or, again,
the wife at certain definite periods may dispense with fidelity to her
husband, and return to the primitive condition of promiscuity. In
certain instances prostitution is combined with the duties of hospitality,
and marriage, though approximating to the monogamic
ideal, must tolerate the intrusion of the guest into the marriage
bed.”
“In a third period, prostitution no longer fills the place of a
traditional survival, but is a morbid manifestation confined to a certain
class of the community. But bridging this transition of prostitution
from a normal to a morbid manifestation, we have the
remarkable phenomenon of æsthetic prostitution. Thus, in India
and in Japan, an agreeable class of prostitutes practices the arts of
singing and dancing, and forms a privileged caste; similarly, in the
most flourishing period of Grecian culture, the leading men of the
time formed a social circle around the hetairæ, from whom they
derived a fruitful stimulus to intellectual and political activity. In
this respect, history repeated itself in Italy in the sixteenth century.
Alike in classical Greece and in mediæval Italy, this æsthetic prostitution
fanned the flames of a period of intense spiritual activity—for
304in individuals as in races, intellectual quickening is ever accompanied
by erotic excitability.”
The unbridled passion of the primitive races of mankind, the
coercive love of beauty felt by the ancient Greeks, the swelling flood
of erotism of the great mass of people of all times, is gradually
guided into the quiet channel of the marriage bed; and even though
monogamic marriage is incapable of fully providing for all manifestations
of sexual passion, still, from the medical point of view,
we must maintain that marriage is for women the most hygienic
and the most proper means of gratification of the sexual impulse.
Conception.
The union between ovum and spermatozoön, whereby fertilization
is effected, appears to occur in the human species as a rule in the
outer third of the Fallopian tube, the ampulla of this structure
(receptaculum seminis in Henle’s terminology) serving to store the
semen for a considerable period; in the lower animals, the usual
occurrence of fertilization in this region has been established by
direct observation. The open mouth of the tube receives the mature
ovum, guided thither from the ovary by appropriate movements
of the ovarian fimbriae; these movements have been seen in active
occurrence in the guinea pig by Hensen. Once within the tube, the
onward movement of the ovum is effected by the cilia of the epithelium
lining of the canal.
His has formulated the theory that in the human species fertilization
is possible only in the uppermost segment of the tube; an assumption
that is probable enough, but cannot be regarded as
definitely established. An analogy certainly exists among the lower
divisions of the animal kingdom, for Coste, His, and Ohlschläger
have proved that an ovum which passes through the Fallopian tube
without being fertilized, undergoes notable alterations. Further,
Coste has shown, in the case of the ovum of the domestic fowl, that
this is no longer capable of being fertilized after it has passed
through the upper segment of the oviduct. Other authorities, however,
namely Löwenthal, Mayrhofer, and Wyder, oppose the extension
of this rule to the human species. Löwenthal assumes that in
the human female, fertilization ordinarily occurs in the cavity of
the uterus, in the wall of which the unfertilized ovum has already
embedded itself; and he supports his contention by the statement
that spermatozoa are not to be found in the Fallopian tubes or on
the surface of the ovaries. Mayrhofer and Wyder point out that
305the movement of the cilia of the ciliated epithelium is in the interior
of the uterus in an upward direction, but in the Fallopian tubes is
downwards in the direction of the uterus.
The contention of Löwenthal was disproved by Birch and Hirschfeld,
who, in a prostitute dying during the act of intercourse, found,
fifteen hours after death, living spermatozoa in the Fallopian tubes.
On the other hand, more recent investigations, those, for instance,
of Hofmeier, Mandl, and Bonn, have confirmed the data given
above with regard to the direction of the ciliary movement in the
interior of the genital passages. Moreover, O. Becker has shown
that the ciliated epithelium of the tubes extends over the fimbriae
and even on to the adjoining pavement epithelium of the peritoneum;
and he believes that the ciliary movement of this region
keeps up a constant current, the purpose of which is to sweep the
ovum into the ostium of the tube, and thence down towards the
uterus. Lode has adduced positive experimental evidence of the
occurrence of such a movement of translation.
The general result of anatomical investigation is, that the conjugation
of the ovum with the spermatozoön takes places in the ampulla
of the Fallopian tube; but it is established that fertilization
may also take place lower down in the tubes, or in the uterine cavity,
or even on the surface of the ovary, i. e., in the abdominal cavity.
The fertilization of the mature ovum—maturation having occurred
within the ovarian follicle before its rupture—has been
shown by numerous researches on the ova of other animals to consist
in the fusion of the male and the female nuclear substance; and
it appears that of the enormous number of spermatozoa, estimated
by Lode at 226 million at a single ejaculation, that enter the female
genital passage, but a single one penetrates the ovum. Towards
the head of this spermatozoön there extends from the surface of
the ovum a process, flat at first, but becoming more and more
prominent, until it surrounds the head, and fuses with it. The
motile tail of the spermatozoön disappears, whilst the head, which
has now passed through the vitelline membrane and entered the
ovum, assumes the appearance of a nucleus, and is called the male
pro-nucleus. The original nucleus of the ovum has previously prepared
itself for fertilization by the extrusion through the vitelline
membrane of portions of its substance (known as polar globules),
and now constitutes the female pro-nucleus. Towards this latter,
situated somewhere near the centre of the cell, the male pro-nucleus
continues to move, the vitelline granules meanwhile being disposed
306round about it in radiating lines, forming a star-shaped figure.
Having come into contact, the two pronuclei fuse completely to
form a new nucleus, the nucleus of the now fertilized egg-cell.
The result of fertilization is the formation of the first segmentation-sphere,
from which, by further subdivision, the new individual is
formed. Thus is effected that which Hippocrates describes in the
words: “The seed possessed both by man and by woman, flow together
from all parts of the body; the fruit is formed by the mingling
of the two seeds.”
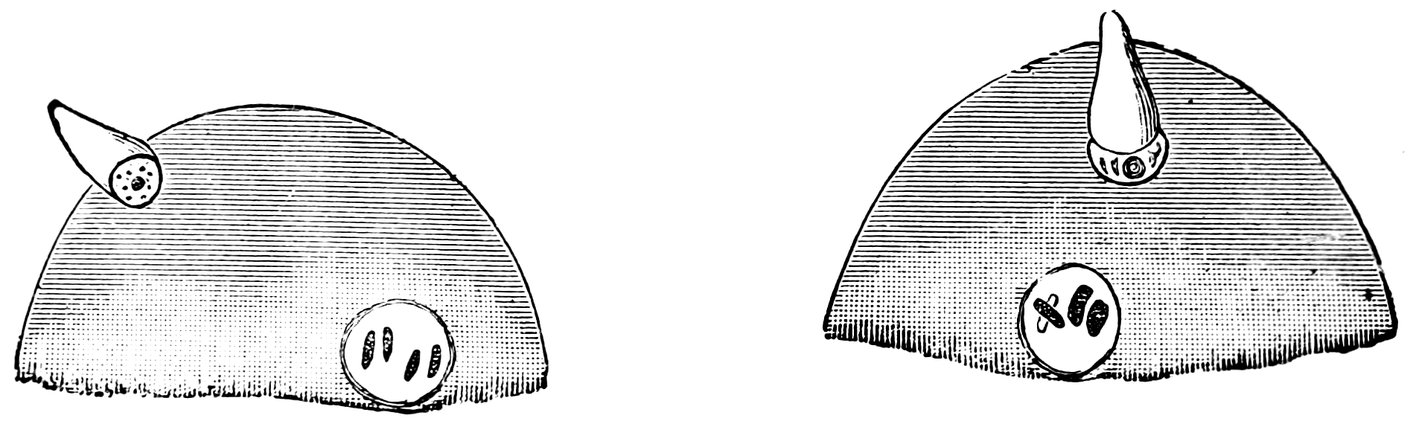
Fig. 55A.—First Stage. Fig. 55B.—Second Stage.
Entrance of a spermatozoon into the ovum of ascaris megalocephala. After preparations by M. Nussbaum. (Half of the ova only are depicted.)
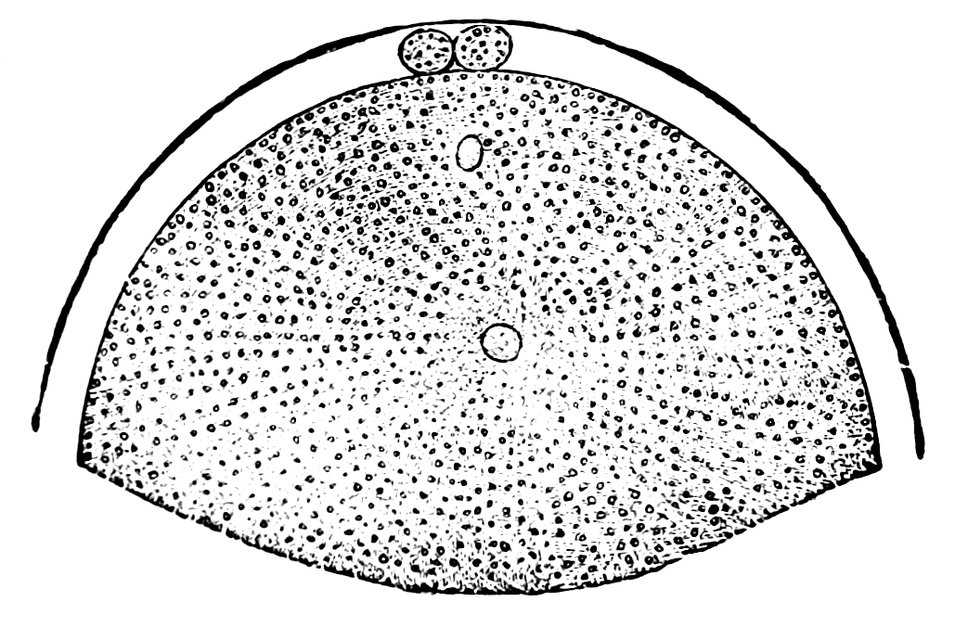
Fig. 56.—Ovum of Asterakanthion ten minutes after fertilization.
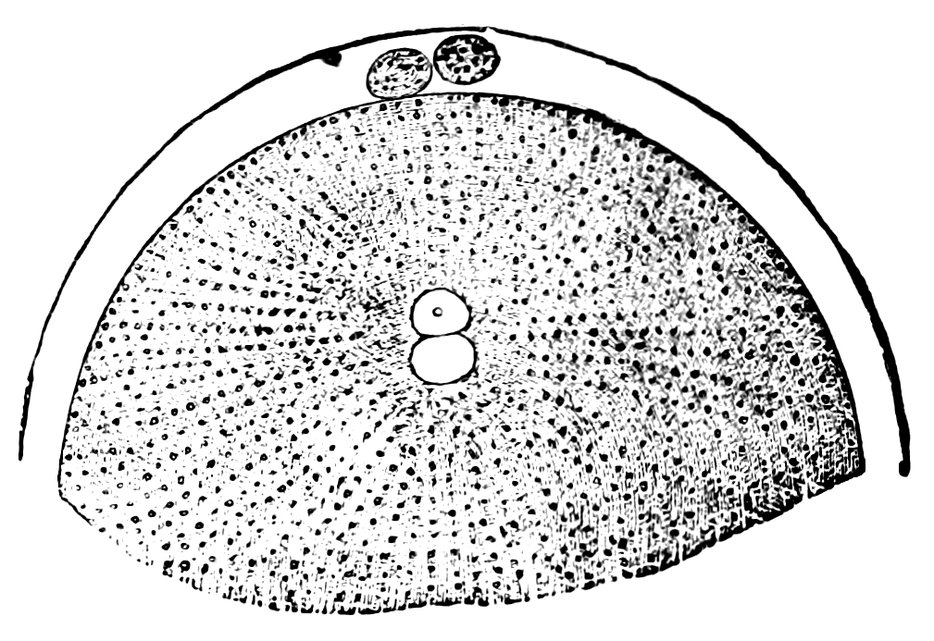
Fig. 57.—Fusion of male pro-nucleus and female pro-nucleus to form the segmentation nucleus of the fertilized ovum.
The most favourable period for the occurrence of fertilization
appears to be when intercourse takes places from eight to ten days
after the termination of the menstrual flow. In 248 instances in
which the date of the fruitful coitus was exactly known, it was
ascertained by Hasler that in 82½ per cent. of all cases, conception
was effected in the fourteen days succeeding the menstrual period.
In general it may be stated that the theory of the periodicity of
ovulation and of the causal relation of this process to menstruation,
has not been shaken by the result of researches recently undertaken
307by opponents of that theory; hence it appears that the fertilized
ovum is the ovum of the last completed menstruation.
Already in the writings of the old Indian physician Susruta, we
find expression of the view that the period that immediately succeeds
the cessation of the menstrual flow is one most favourable to
conception. “The time of generation,” he says, “is the twelfth
night after the commencement of menstruation.” In the Jewish
Talmud, the day before the onset of menstruation, and the days immediately
succeeding the cessation of the flow, are indicated as
those most favourable to the occurrence of conception; moreover,
in the Talmud, notwithstanding the fact that intercourse during
menstruation is prohibited on pain of death, and that coitus is not
regarded as permissible until the lapse of twelve clear days after
the cessation of the flow, nevertheless the assertion is made that
intercourse during menstruation may lead to conception.
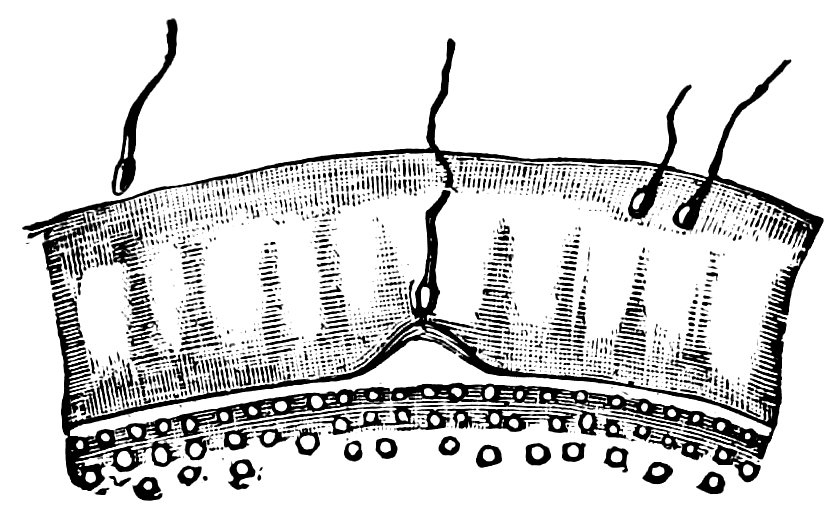
Fig. 58. —Passage of spermatozoon through the zona pellucida of the ovum of asterakanthion.
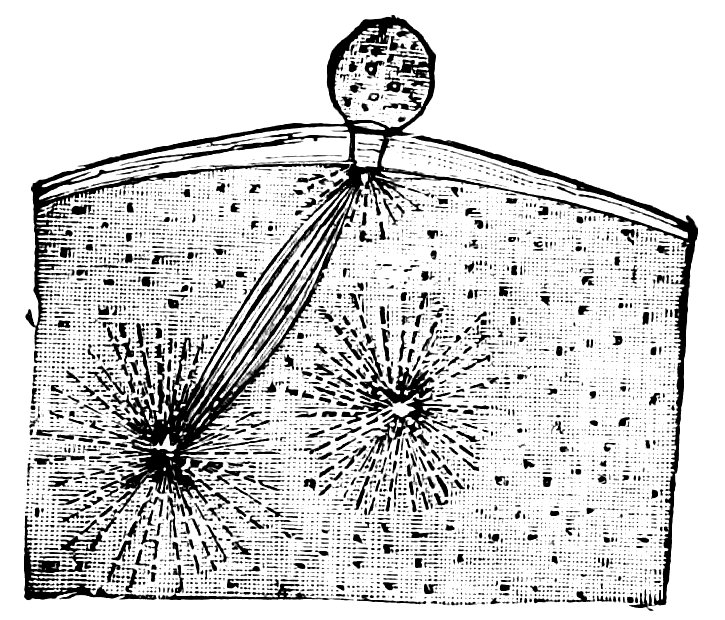
Fig. 59.—Ovum of scorpæna scrofa thirty-five minutes after fertilization.
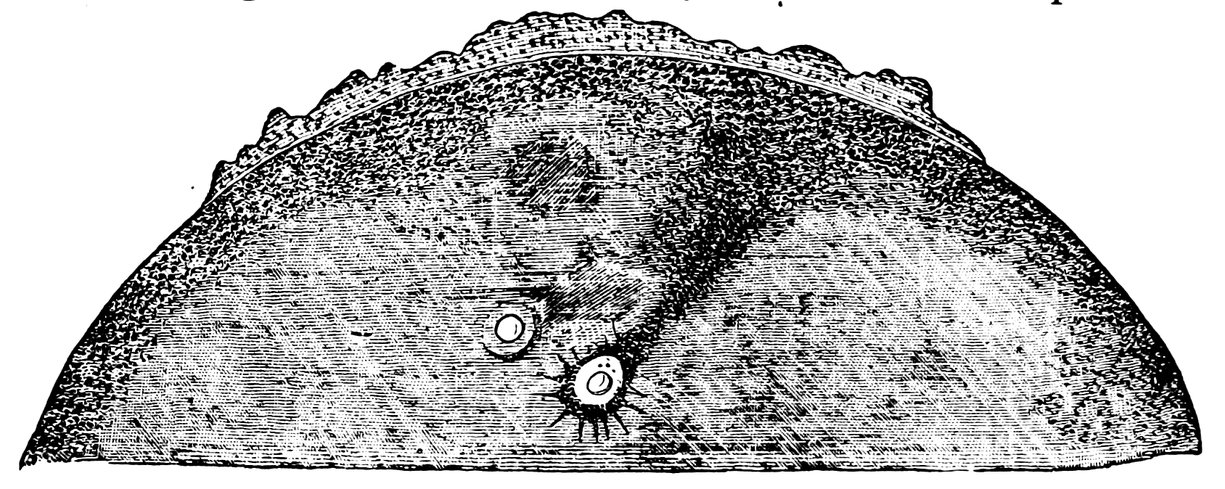
Fig. 60.—Male pro-nucleus and female pro-nucleus in fertilized ovum of frog, prior to the formation of the segmentation nucleus.
Hippocrates writes: Hae nempe post menstruam purgationem
utero concipat. Aristotle says: Plerasque post mensum fluxum
nonnullas vero fluentibus adhuc menstruis. Galen writes: Hoc
autem conceptionis tempus est vel incipientibus vel cessantibus
menstruis.
308Soranus writes to a similar effect: Just as the soil is suitable only
at certain seasons for the reception of the seed, so also in the
human race intercourse does not always take place at a time suited
for the reception of the semen. To be effective, coitus must occur
at the proper time.... The act of intercourse that is to lead
to conception may best occur either just before or just after the
menstrual flow, when, moreover, there is strong desire for the
sexual embrace, and neither when the body is fasting, nor when it
is full of drink and undigested food. The time before menstruation
is, however, unsuitable, for then the womb is heavy from the
flow of blood, and two conflicting tendencies will come into operation,
one for the absorption of material and the other for its outflow.
During menstruation, again, conception is unlikely to occur,
for then the semen is wetted and washed away by the flowing blood.
The sole proper time is that immediately after the flow, when the
womb has freed itself from its humours, and warmth and moisture
stand in harmonious relationship.
Among many of the castes of Hindustan, it is a religious ordinance
that on the fourth day of menstruation a man shall have intercourse
with his wife, “since this day is that on which conception is most
likely to occur.” Indian physicians advise, in order to bring about
conception, “that coitus be effected always as soon as the menstrual
flow has ceased, at the end of the day, and when the lotus has
closed.” In Japan, medical opinion is to the effect that a woman
is capable of conceiving during the first ten days after menstruation,
but not later (Ploss and Bartels).
The view that the first days of the intermenstrual interval are
those most favourable to the occurrence of conception, is further
confirmed by the statistical data collected by Löwenfeld, Ahlfeld,
Hecker, and Veit; and it appears that as the date of the next menstruation
is approached, there is a continual decline in the frequency
of conception; just before the flow, conception hardly ever occurs.
Hensen, from the records of 248 conceptions in which the date of
the fruitful intercourse was exactly known, draws the following conclusions:
1. The greatest number of conceptions follow coitus effected
during the first days after the cessation of the menstrual flow.
2. When coitus is effected during menstruation, the probability
of conception increases day by day as the end of the flow is approached.
3. The number of conceptions following coitus effected shortly
before menstruation is minimal.
3094. However, there is no single day either of the menstrual flow
or of the intermenstrual interval, on which the possibility of the
occurrence of conception can be excluded.
Feokstitow has drawn up from statistical data an ideal “conception-curve,”
which teaches that conception most readily ensues upon
coitus effected soon after the end of the menstrual flow, in the first
week, that is to say, of the intermenstrual interval; moreover, the
curve shows that the highest percentage of conceptions occurs on
the very first day after the cessation of the flow, and that after
this day the percentage of conceptions declines. The percentage
frequency of conceptions from coitus effected on the last day of
menstruation, and on the first, ninth, eleventh, and twenty-third
days, respectively, of the intermenstrual interval, is expressed by
the ratio 48 : 62 : 13 : 9 : 1; and between the points given, the course
of the curve is almost rectilinear. The probability of the occurrence
of conception on the twenty-third day of the interval (on
which day the curve reaches its lowest point), is one-sixty-second
of the maximum probability.
The proper performance of coitus depends upon the potentia
coeundi of the male; the attainment of conception depends upon his
potentia generandi. The potentia generandi demands from the man
the functional competence of the testicles, the perviousness of the
seminal passages (namely, of the vasa deferentia and the urethra),
the secretion of a normal semen, and, finally, a proper formation of
the penis, whereby during ejaculation the semen may be deposited
in sufficient proximity to the os uteri externum.
Normal semen is a whitish, semi-transparent fluid, of the consistency
of thin cream. It contains aggregations of a nearly
spherical shape, consisting of a vitreous, transparent, colourless or
light yellow, gelatinous, elastic substance. Under the microscope
this substance has a hyaline appearance, and exhibits in its interior
innumerable clear spaces of varying size, which are apparently filled
with a clear fluid. Not infrequently, these spaces are extremely narrow
and therewith greatly elongated and disposed in parallels, so
that the whole substance thus obtains a striated appearance. When
treated with water, this material becomes whitish and non-transparent,
and assumes under the microscope a finely granular aspect.
When allowed to stand without agitation for twenty-four hours,
this substance dissolves and becomes so intimately mingled with the
seminal fluid that it can no longer be clearly differentiated therefrom.
In all probability it is merely a secretory product of the
seminal vesicles.
310The truly fluid portion of the semen contains the following
morphological elements:
1. Microscopic aggregations of hyaline substance, variously
shaped.
2. Very numerous granules, small and extremely pale, albuminous
in their nature, and disappearing on treatment with acetic acid.
3. A small number of rounded or oval cells, about the size of
leucocytes, containing one, or sometimes two small round nuclei.
4. Prostatic calculi. These are an inconstant constituent, but
are very frequently met with after repeated coitus. According to
some observers they are derived also from the bladder and urethra.
They are distinguished by their yellowish colour, their irregular
form (sometimes triangular, sometimes rounded or oval), and by
their characteristic structure. They are composed of a substance
arranged in concentric laminæ, which in the centre has a granulated
appearance; they often exhibit one or more oval nuclei.
5. Spermatozoa in countless numbers.
In exceptional cases we find as additional morphological elements,
especially in elderly people, scattered erythrocytes, cylinder-epithelium
cells, and masses or granules of yellow pigment.
The spermatozoa are about fifty micromillimetres in length. Two
parts may be distinguished in each, a head and a tail. The head,
four or five micromillimetres in length, is flattened, and differs in
apparent shape—though generally more or less pear-shaped—according
as to whether it is seen sideways or on the flat.
The tail, which is about forty-five micromillimetres in length, narrows
from before backwards. The fine posterior extremity is said
to contain the contractile element, so that it is upon this portion
that the familiar movements of the spermatozoa depend (Fig. 61).
The spermatozoa are made up of a substance very rich in
sodium chloride, and strongly resistent to reagents and to putrefaction.
In consequence of their richness in mineral constituents, the
ash, when they are calcined, retains their original form.
The movements of the spermatozoa can be properly observed only
in fresh, pure semen (Fig. 62).
If freshly ejaculated semen is treated with water, the movements
of the spermatozoa very shortly cease, and their tails become rolled
up in a spiral form.
311
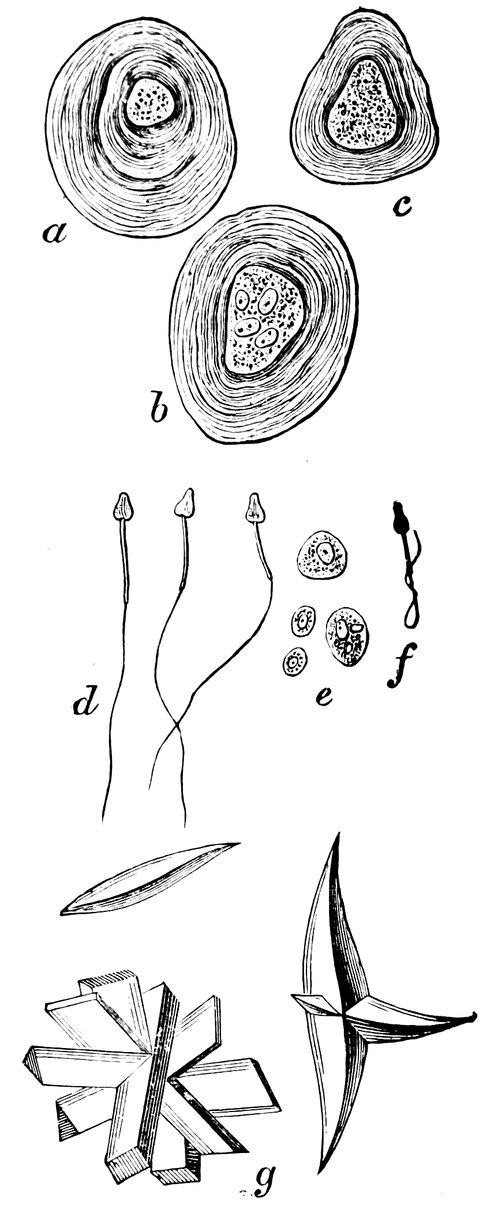
Fig. 61.—a. b. c. Prostatic calculi from normal semen. d. Spermatozoa. e. Large and small cells, some containing granules, as morphological elements of semen. f. Spermatozoon distorted by imbibition of water. g. Crystals. (After Bizzozero.)
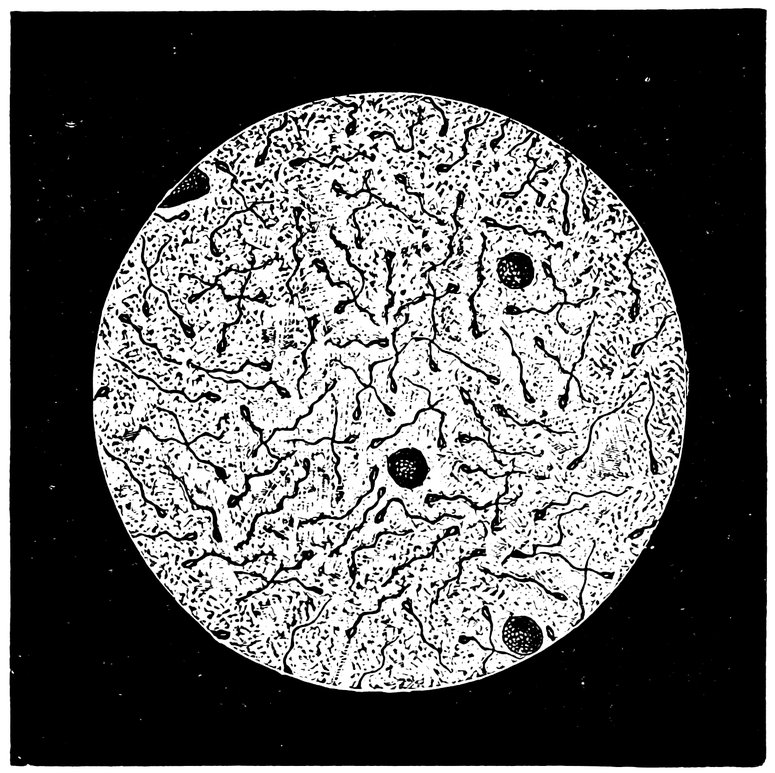
If semen is left undisturbed for twenty-four hours or longer, the
vitreous substance dissolves in the surrounding fluid, and this latter
separates into two layers, an upper which is thinner, and a lower,
which is thicker and non-transparent. In the former, the morphological
elements are found but sparingly, whilst in the latter, they
are plentiful. In addition to the elements already described, we
find often two varieties of crystals. One of these varieties, which
appears only when decomposition is far advanced, consists of ammonium
magnesium phosphate. The other variety has a chemical
composition not yet determined. These crystals belong to the monoclinic
system, forming prisms or pyramids, often with curved surfaces;
they are colourless or light yellow; they lie superimposed,
312often forming beautiful star-shaped figures. They are soluble in
mineral and vegetable acids, and in ammonia, but are insoluble in
alcohol, ether, and chloroform; they are remarkably resistent to the
solvent powers of cold water, but not so to those of boiling water.
Shreiner has proved that these crystals consist of a phosphate of a
base which is represented by the formula C2. H5. N. According to
Fürbringer, these crystals are produced as a result of the action of
the semen upon the prostatic secretion.
The quantity of semen ejaculated during coitus is very variable,
depending upon the age and size of the individual and the formation
of his testicles, upon his individual sexual capacity, and upon the
question whether antecedently there has been sexual excess on the
one hand or long continued continence on the other. In general,
the quantity of semen ejaculated at one time varies between 0.75
and 6 c.c. (10 to 100 minims).
If healthy, normal semen, with adequate fertilizing potency, is
properly preserved from cold and light, we may, even after the
lapse of twenty-four hours, find under the microscope spermatozoa
still engaged in active movement. Ultzmann employs for the description
of a drop of fresh semen, the comparison that it is full of
movement, “like a stirred up ant-heap.” Influenced by the whiplike
lashings of the tail, the spermatozoön moves steadily forwards,
finding its way through the narrowest passages on the microscopic
field without striking any of the cellular structures that may lie in
its path. The longer the semen remains under observation, the less
active are these movements of the spermatozoa, for after ejaculation
they gradually die, exhibiting after death an extended, or at
most a slightly curved tail; those spermatozoa, on the other hand,
that were dead before ejaculation, have the tail spirally twisted,
rolled up, or acutely bent. In the case of spermatozoa which have
been destroyed by the action of some other deleterious secretion, as
by urine or by acid vaginal secretion, such a condition of the tail
is very commonly seen. When the semen is treated with water, the
movements of the spermatozoa soon cease, and the ends of their
tails frequently roll up to form loops. By the addition, however,
of concentrated solutions of neutral salts, of albumen, of urea, etc.,
it is possible to reanimate these motionless spermatozoa, so that
they once more are seen to perform active movements. Moderately
concentrated animal secretions of an alkaline reaction are favourable
to the motor activity of the spermatozoa, whilst on the other hand
dilute and acid secretions, such as urine, acid mucus (including the
313acid vaginal mucus), and catarrhal secretions, even when alkaline
in reaction, have a depressant influence on this activity. Caustic
potash and caustic soda stimulate the movements of the spermatozoa.
When they are cooled down to a temperature below 15° C.
(59° F.), the movements cease entirely. Salts of the heavy metals,
and mineral acids in solution, also bring their movements to a pause.
Frequent repetition of coitus causes a diminution in the number and
in the motor activity of the spermatozoa.
Semen which contains no spermatozoa, or in which the spermatozoa
are motionless, is absolutely devoid of fertilizing power; in
the case of such semen, it makes no difference whatever that the
external genitals of the man generating it are strongly formed, that
his testicles are of normal size, and that erection and ejaculation
take place promptly. Of very little value, though not absolutely
sterile, is semen containing very few living spermatozoa, or, among
very numerous motionless spermatozoa, containing a few only that
are engaged in active movement. Suspect, is semen which does
not possess the normal light greyish white tint, but is brownish-red,
brownish-yellow, yellow, or violet; these variations in colour indicating
an admixture with the semen of varying quantities of blood
or pus, in consequence of disease of the urethra, the prostate, the
seminal vesicles, or some other part of the uropoietic system; such
admixtures seriously impair the quality of the semen. An unfavourable
judgment must also be passed on semen which, at each successive
ejaculation, is voided in very small quantities only—from
half a drachm to a drachm. When thus scanty, semen is often
found to contain an exceptionally large proportion of dead spermatozoa.
We may regard very favourably semen which is voided in
quantities considerably in excess of the average; sometimes, when
there is a veritable polyspermia, there may be an ounce or upwards,
more than three times as much as normal—provided, of course,
that this semen so richly voided is of a satisfactory quality, and
contains an ample proportion of active spermatozoa. The most
valuable characteristic in semen is exhibited when the spermatozoa
it contains are not only very numerous and vigorously active, but
when they are also very long-lived, when, that is to say, they retain
the power of active movement sometimes for as long as three days.
A decisive opinion as to the quality of a man’s semen can be given
only as the result of precise and repeated microscopic examinations,
and the medical man must be most careful, when in his first examination
he has not been able to detect the presence of any living
314spermatozoa, to abstain from giving, on that account alone, an adverse
decision—from pronouncing sentence of death on the man’s
reproductive potency.
It has not hitherto been accurately determined how long spermatozoa
can continue to live in the interior of the uterus, although the
point is of great importance, not only in relation to conception, but
also in regard to the theory of menstruation. Percy has published
a case in which, eight and a half days after the last coitus, he saw
living spermatozoa emerge from the os uteri externum. Sims bases
upon his own researches the decisive opinion that in the vaginal
mucus, spermatozoa can never survive longer than twelve hours,
but states that in the mucus of the cervical canal they can live much
longer. If thirty-six to forty hours after coitus, we examine the
cervical mucus under the microscope, we commonly find living and
dead spermatozoa in about equal numbers. Many of the living ones
will survive their removal from the cervix for as much as six hours
longer.
Of especial interest are the conditions which are liable to deprive
a man of the power to produce fertilizing semen. In the first place
must be mentioned congenital absence of both testicles—a condition
which, in otherwise normally formed male individuals, is one
of extreme rarity. Congenital absence of one testicle is less rare,
and is usually accompanied by absence also of the epidydimis, vas
deferens, and seminal vesicle of the same side. The potentia gestandi
of a monorchid depends upon the proper development of his
single testicle, and the functional capacity of this organ must be ascertained
by a careful microscopic examination of his semen. Much
more frequent than absence of the testicle, though still sufficiently
rare, is the condition of cryptorchism, non-descent of one or both
testicles, a state not necessarily associated with functional incapacity
of the organ. Most commonly, however, an undescended testis is
an imperfectly developed testis, and in the very great majority of
cases the ejaculated fluid contains no spermatozoa.
A further cause of the lack of potent semen is atrophy of the
testicles with notable diminution in the size of the glands, and more
or less complete disappearance of the seminiferous tubules and their
cellular contents. This state is rarely congenital, being nearly always
acquired: in consequence of inflammatory conditions affecting
the testicle proper or the epididymis (syphilitic inflammation,
especially, is apt to lead to overgrowth of the interstitial connective
tissue and to gradual destruction by pressure of the seminal tubules)[46];
315or in consequence of the pressure of a hernia, a varicocele,
a hydrocele, or a tubercular, carcinomatous, or other new growth;
or in consequence of constitutional disorders, especially long-lasting,
severe, and exhausting diseases, such as diphtheria, diabetes,
or chronic alcoholism; in consequence of diseases affecting that
portion of the central nervous system from which the nerves supplying
the genital organs arise; in consequence of degenerative
changes resulting from sexual excesses; or, finally, in consequence
of senile changes, such as fatty changes in the cells of the seminiferous
tubules. Certain drugs also, digitalis, salicylic acid, mercury,
iodide of potassium, arsenic, and morphine, have an unfavourable
influence alike on the quality of the testicular secretion and on the
potency of the individual. Von Gyurkovechky reports that in
Bosnia a plant locally known as “neven” is employed among the
peasantry for the temporary suppression of sexual potency, wives
giving it to their husbands when the latter are about to leave them
and go upon a journey, and sprinkling the leaves of the plant
among the underclothing.
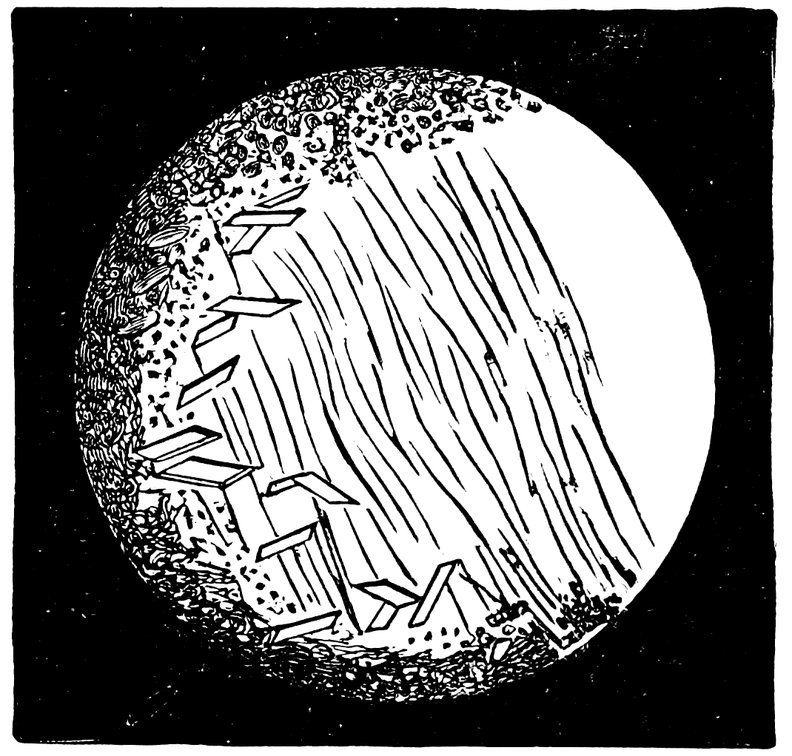
Fig. 63—Semen consisting chiefly of sperm-crystals, cylindrical epithelium and small granules exhibiting molecular movement—but containing no spermatozoa.
By the name of azoospermia is denoted a condition whose existence
can be determined only by microscopic examination.
316The subject of this affection has normal potentia coeundi, the
semen is ejaculated in quite normal fashion, and it is its constitution
only that is faulty. In appearance it is extremely fluid, and is
somewhat cloudy; its sediment contains molecular detritus and
spermatic crystals, but no spermatozoa (Fig. 63). If the medical
man makes it his rule, in all cases in which he is consulted on account
of sterility, in deciding how far this sterility is dependent on
the condition of the husband, not to confine himself solely to the
customary questions, whether intercourse is regularly practised,
whether before or after menstruation, etc.—but if in every case he
makes a careful examination of the semen under the microscope, he
will be astonished to learn the comparative frequency with which
he will note the complete or nearly complete absence of spermatozoa.
This condition of azoospermia may be permanent or
transitory.
To Kehrer belongs the credit of having pointed out that sterility
is less often due to impotence or to aspermatism than to azoospermia—a
condition often unsuspected by husband and wife, and
one to be diagnosed by the physician only after repeated microscopic
examinations of the semen. For this reason, indeed, its
existence is often overlooked. Kehrer believes himself to be justified
in asserting that one-fourth of all cases of sterility (if not
indeed more) must be referred to conditions affecting the husband,
and most often to azoospermia; hence he concludes, that the husband
must still more often be regarded as the one to blame for the
occurrence of sterility, when the cases are borne in mind in which
a man marries with an imperfectly healed gonorrhœa, and infects
his wife, giving rise to a chronic tubo-uterine blennorrhœa, and ultimately
to sealing up of the tubes and to sterility.
Complete absence or marked scarcity of spermatozoa in the
semen may occur also without any change in the testicle that can
be detected by an external examination, as a consequence of contusions
of the testicle, or of gonorrhœal inflammation of the epididymis
or vas deferens; further as a sequel of severe general diseases,
long-continued physical exertion, or great sexual excess.
In some cases, a microscopical examination reveals, not azoospermia,
but oligozoöspermia, that is to say, the number of living
spermatozoa in the semen is remarkably small. Or, again, the
anomaly may be of this character that the spermatozoa are smaller
than normal, that they are motionless, and that their tails are broken
off—such are the peculiarities, as a rule, of the semen of old men.
317A less common condition than azoospermia, but one the pathological
importance of which is equally great, is aspermatism, in
which the man, neither during coitus, nor in any other form of
sexual excitement, is able to ejaculate any semen. This condition
may be congenital or acquired; it may be permanent, or transitory
(lasting a few weeks or months). In these cases we have to do
with organic changes in the testicles, diseases of the prostate,
gonorrhœal processes, or nervous disturbances resulting in a loss
of irritability in the reflex centre for ejaculation. Aspermatism in
the narrower sense of the term, a condition, that is to say, in which
there is total suspension of the activity of all the three glands which
combine to secrete the composite fluid known as semen, namely, of
the testicle, the prostate, and the seminal vesicles—is, according
to Fürbringer, probably non-existent. The pathological state underlying
aspermatism would rather appear to be, not a failure to
secrete semen, but a failure to ejaculate it.
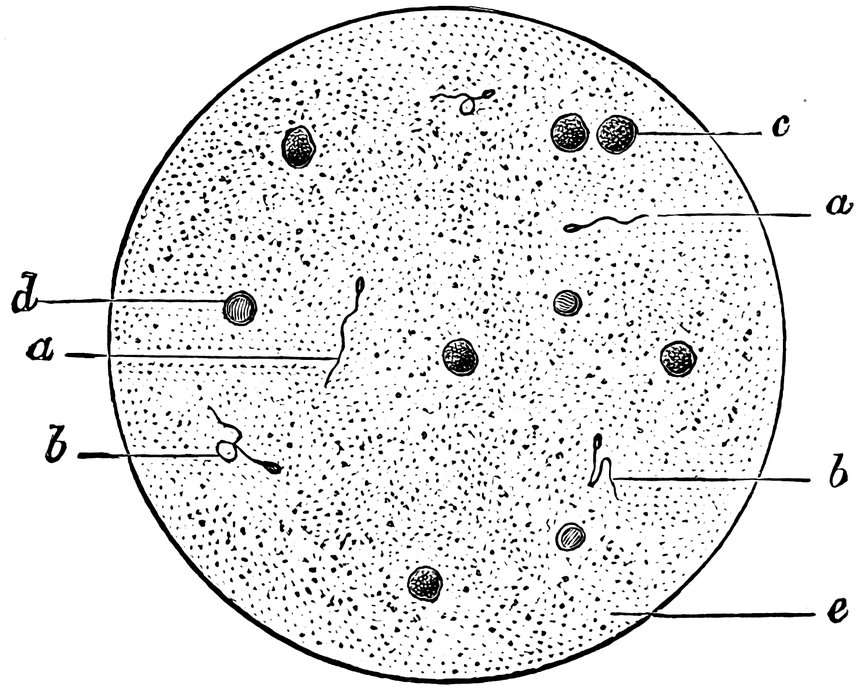
Fig. 64.—Oligozoöspermia. a. Living spermatozoa, b. Dead spermatozoa, c. Pus corpuscles, d. Erythrocyte, e. Seminal granules.
Last of all, we have to speak of conception without copulation,
of artificial fertilization. In consequence of the mechanical hindrances
which in many cases prevent the entrance of the semen into
the interior of the uterus, the idea has arisen to introduce the semen
by means of instruments directly into the cervical canal, dispensing
with the natural act of copulation. Experience long ago gained in
artificial pisciculture, no doubt gave rise to this idea. Spallanzani
and Rossi by means of a syringe injected the semen of a dog into
the vagina of a bitch, the procedure resulting in impregnation.
318Girault appears to have been the first,[47] in the year 1838, to introduce
semen artificially into the human uterus, if we leave out of consideration
the experiment of Léseurs, who introduced a tampon
moistened with semen into the interior of the vagina. The procedure
employed by Girault is thus described: The patient having
been placed in the position usually employed for gynecological examination,
a canula resembling a male catheter with the eye in its
point, and with a funnel-shaped enlargement at the opposite extremity,
is introduced into the uterus, this instrument having first
been prepared by moistening its interior with mucilage and filling
it with semen; by insufflation, the semen is now expelled into the
uterine cavity. It is stated that neither uterine colic nor any other
dangerous symptom has ever been brought on by this procedure.
The experiments were made at various periods between the year
1838 and the year 1861; they were ten in number, and of these eight
proved successful, two unsuccessful. In the ten cases, the total
number of insufflations made was twenty-one—the minimum number
in any single case being one, the maximum five. In one case,
the insufflation was effected immediately after the cessation of menstruation;
in the majority, from one to four days after the cessation
of menstruation; in one case twelve days, in one case twenty-three
days, after the cessation of the flow. Gautier, instead of insufflations,
has employed injections of semen, using two injections in
each case, one just before menstruation was expected, the other a
day or two after the cessation of the flow. Marion Sims endeavoured
in twenty-seven cases to bring about conception by the
injection of semen into the uterus; in one of these cases only was
the desired result obtained. In this latter instance the patient was
twenty-eight years of age, had been married for nine years, but had
remained barren. Throughout her menstrual life, she had suffered
more or less from dysmenorrhœa, often accompanied by severe constitutional
disturbance, such as syncope, vomiting, and headache.
Local examination disclosed the existence of retroversion of the
uterus with hypertrophy of the posterior wall, an indurated, conical
cervix, with stricture of the cervical canal, especially in the region
of the os uteri internum. In addition to all these mechanical obstacles
to conception, it was found that the semen was never retained
in the vagina after coitus. Sims examined the patient immediately
319after coitus had taken place, but never found a single drop of semen
in the vagina, notwithstanding the fact that this fluid had been
ejaculated in abundance. Sim’s first care was to bring about reposition
of the uterus, and to keep the organ in its proper place by the
insertion of a suitable pessary. Injections of semen were then undertaken,
and were continued throughout a period of nearly twelve
months. In two instances, the injection was effected immediately
before the onset of the menstrual flow; in eight instances it was
effected at varying times (two to seven days) after the cessation
of the flow. At first, three drops of semen were injected, but later
only half a drop. The semen (first ejaculated into the vagina during
normal intercourse) was injected by means of a glass syringe,
which was kept in a vessel of warm water at a temperature of 98° F.
Since during the removal of the instrument from the water and its insertion
into the vagina, some fall in temperature necessarily occurred
in the vagina, Sims allowed the syringe to remain for some minutes
in the vagina before he drew the semen into it, in order that he might
feel assured that syringe and vagina had regained the temperature
most adapted to the vital activity of the spermatozoa. The
nozzle of the syringe was then carefully introduced into the cervical
canal, and half a drop of semen was slowly injected into the uterine
cavity. For two or three hours after the operation, the patient remained
lying quiet in bed. After the tenth experiment, conception
ensued—the first recorded case of artificial fertilization in the
human species.
With right, however, this case of Sim’s was not regarded as conclusive,
since both before and after the injection, ordinary coitus
had been effected, and it is therefore impossible to determine
whether the fertilizing spermatozoön was one of those introduced
by means of the syringe, or in the antecedent or subsequent coitus—more
especially in view of the fact that by the insertion of a pessary
Sims had, previously to undertaking the injections, restored the
uterus to a position more suited to the occurrence of conception in
the natural manner.
In a case which a priori seemed exceedingly well adapted for
the performance of artificial fertilization, one of marked hypospadias
in a man whose semen was abundant and contained a large number
of vigorously moving spermatozoa, I saw this experiment fail, in
spite of all possible care in its performance. In fact, not a single
conclusive instance of successful artificial fertilization in the human
species is known to me, though I have seen reports of numerous
320disagreeable and even dangerous results of attempts to effect it.
Both parametritis and perimetritis have occurred in such cases; and
semen, being a material in a state of most intense molecular movement,
may be regarded as extremely liable to noxious transformations.
Sim’s procedure has been modified by other gynecologists. Thus,
Courty’s plan was that during coitus the semen should be collected
in a condom, fitting not too closely, from which receptacle it was
drawn up into a syringe and carefully injected into the cervical
canal. Pajot’s plan was that the semen should be ejaculated into
the vagina in natural coitus, and should thence be pressed into the
uterine cavity by means of a piston-like instrument introduced into
the vagina.
In London, Harley frequently made the experiment of injecting
semen into the uterine cavity, but in all cases without any result.
P. Muller, in two cases, on account of extreme anteflexion of the
uterus, performed this experiment. Though the general conditions
were in both cases extremely favourable, in neither instance was
there any result. It must, however, be mentioned that in one of
his cases only had there been any preliminary examination of the
semen under the microscope.
Fritsch reports a case in which gonorrhœal secretion was injected
in place of semen. Peritonitis, which for a month endangered life,
was the result.
In Paris, Lutaud has earnestly advocated artificial impregnation
in cases of sterility in which all other means have failed. It is
obvious that it would be useless to employ this measure after the
menopause, or in women in whom menstrual activity has ceased
prematurely, with simultaneous disappearance of all menstrual
molimina. Equally useless would it be in uterine atrophy and in
cases of irremediable malformation of the female genitals. Further
contra-indications, according to Lutaud, are offered by chronic pelvic
peritonitis, since here, on account of the obliteration of the lumen
of the Fallopian tubes, the operation is foredoomed to failure.
Chronic inflammatory states of the uterus and its mucous membrane,
will also render the attempt useless. Moreover, it is a condition
indispensable to success that the semen to be employed shall
have been examined microscopically, and shall have been found to
be thoroughly healthy. The operation has the greatest prospect of
success when undertaken from three to two days before the due
date of menstruation. The method employed is that of Sims. If
321after the first attempt, the due menstruation should begin, the injection
should be repeated a week after the flow has ceased; the
attempt should not, however, be repeated more than about six times
in all, since the probability of success rapidly diminishes with each
successive endeavour. Before the operation is undertaken, the permeability
of the cervical canal must be ascertained. Further, in
order that the spermatozoa shall be placed in conditions in which
they have the best possible chance of survival, a weak alkaline solution,
such as 1 per cent. of potassium bicarbonate, should as a preliminary
measure be injected into the vagina.
Lutaud thus describes the procedure he employs. Immediately
after the woman has had intercourse with her husband, a Fergusson’s
speculum is introduced into the vagina, the patient remaining
in the dorsal decubitus. As the speculum passes in, its margin
scrapes the surface of the vagina, and by this means the semen is
collected in the vicinity of the cervix. The semen is then drawn
up into a Pravaz syringe or an analogous instrument, such as a
uterine catheter armed at one end with a rubber ball. The fluid is
then carefully injected into the cervical canal, or preferably into
the uterine cavity, great care being taken not to injure the mucous
membrane in any way, since the slightest bleeding may nullify the
whole procedure. Finally, a small tampon of absorbent cotton-wool
is inserted into the os uteri externum. For some hours the woman
must remain quiet in bed; the tampon is not removed for ten hours.
As regards results, Lutaud informs us that he has in this way treated
twenty-six cases. In twenty-two of these, failure was complete; in
one case, success was partial—the patient was impregnated, but
abortion occurred two weeks later; in another case, abortion occurred
after three months pregnancy; finally, in two cases, success
was complete.
Indications for the employment of artificial impregnation are:
first, the existence of stenosis in the upper part of the cervical canal,
especially
stenosis from flexion, provided, of course, that other measures are
contra-indicated or have been fruitlessly employed; secondly, a deleterious
character of the secretion of the cervical canal; thirdly, extreme
cases of hypospadias in the male. Haussmann recommends
the employment of artificial impregnation in cases in which the
spermatozoa are found to enter the cervical canal, but fail to pass
through the os uteri internum. Whilst artificial impregnation is
theoretically a sound measure, yet in the practice the indications for
322its performance are by no means easy to establish. For, in cases
in which there is some mechanical hindrance to the contact of the
spermatozoön with the ovum (and it is for such cases only that this
method of artificial fertilization can properly be employed), it is
often extremely difficult, and may even be quite impossible, to exclude
the possibility of there being some failure in ovulation itself,
or in the maturation of the ova; or, again, sterility may depend,
not on the fact that no ova are fertilized, but on the fact that when
fertilized they always fail, for some reason, to find a resting place
in the uterus; in a word, in any case in which sterility appears to
be due to mechanical obstacles to conception, it may in reality be
due to some other disease which has escaped recognition, some
organic disease of the uterus, the tubes, the ovaries, of the periuterine
tissues.
Finally, it must be remembered that the manipulation is far from
easy in its performance. Above all, the semen must be subjected to
a most rigorous microscopical examination in respect of its fertilizing
capacity. But this examination cannot be made in the case of
the semen that is actually used for the attempt at artificial fertilization;
it can only be done with an earlier specimen from the same
man. If the semen contains no living spermatozoa, or very few
only and these sluggish in their movements, still more if it contains
pus corpuscles or gonococci, all idea of its employment for
artificial fertilization must be rejected.
The method employed by Sims, in which the semen is drawn into
a syringe inserted into the vagina post coitum, is one which I am
not able to recommend, since in this way together with the semen
some vaginal mucus is drawn up, thus, instead of pure semen, we
inject into the vagina semen mixed with various impurities, and
more especially with an acid secretion known to be unfavourable
to the life of the spermatozoa—a circumstance that will doubtless
explain many of the failures that have hitherto taken place. It is
certainly better that the semen of the husband should be collected
in a rubber condom. The preservation of the material to be injected
at a suitable temperature (the normal body-temperature), is
by no means easy. The syringe, an ordinary Braun’s uterine
syringe, is first disinfected, and then lies ready in water of the
proper temperature. The semen is rapidly drawn up into the
syringe, the nozzle of which is then passed down to the fundus
uteri. Quite a small quantity of semen will suffice. After the
manipulation, which should of course be undertaken at the time most
323favourable to conception, just after menstruation, the woman should
lie quiet in bed for some hours.
In considering the probability of a successful issue to any such
attempt to secure artificial fertilization, we cannot leave out of consideration
the likelihood that that result may be prejudiced by the
lack of all normal sexual feeling on the part of the wife; concerning
the significance of such feeling in relation to the sexual act, we have
however as yet no certain knowledge.
That this procedure of artificial fertilization is extremely disagreeable
to all concerned therein, the physician not excepted, and
that various moral and social considerations can be alleged against
it, is incontestable. It is indeed recorded that in Bordeaux a legal
penalty was inflicted on a medical man who undertook to bring
about artificial fertilization. The Society of Medical Jurists debated
this matter, and came to the conclusion that, whilst a medical man
was not justified in recommending the practice, neither was he
justified in refusing to undertake it when requested by his patients.
In Paris, a candidate for the degree of Doctor of Medicine made
artificial fecundation the subject of his thesis, and maintained that
its practice, when effected with all proper social precautions and according
to scientific principles, was possible, reasonable, useful, and
moral, and that in many instances it should be recommended by the
physician. After a long and stormy debate, the Faculty of Medicine
determined to reject the thesis and to destroy all specimens of
it already printed, on the ground that “they feared, if they gave
their sanction to the practice, that a number of more or less unscrupulous
physicians would make that sanction the basis of improper
practices, dangerous alike to the family and to the state,
since the operative method under consideration was one likely to
be eagerly exploited by the whole tribe of medical charlatans.” This
weighty pronouncement would appear to be sufficient ground for rejecting
artificial fecundation as a matter of routine practice; still,
very exceptional cases may be encountered in which it may be seized
as an ultimum refugium.
Pathology of Copulation.
The act of copulation may be interfered with or entirely prevented
by pathological conditions affecting the genital canal of the woman,
and also by disturbances of the nervous system—naturally also by
any abnormality affecting the performance of the male partner in
the act.
324Abnormality of the hymen, such as excessive strength and rigidity,
rendering the organ unduly persistent, is a not infrequent hindrance
to intercourse, one that sometimes is not overcome even after
years of married life; to such a state of affairs ignorance on the part
of the married pair in respect to the proper method of intercourse,
lack of sufficient sexual power on the part of the male, or inflammation
of the fossa navicularis brought on by maladroit attempts
at penetration, may contribute, likewise undue passivity on the part
of the female partner.
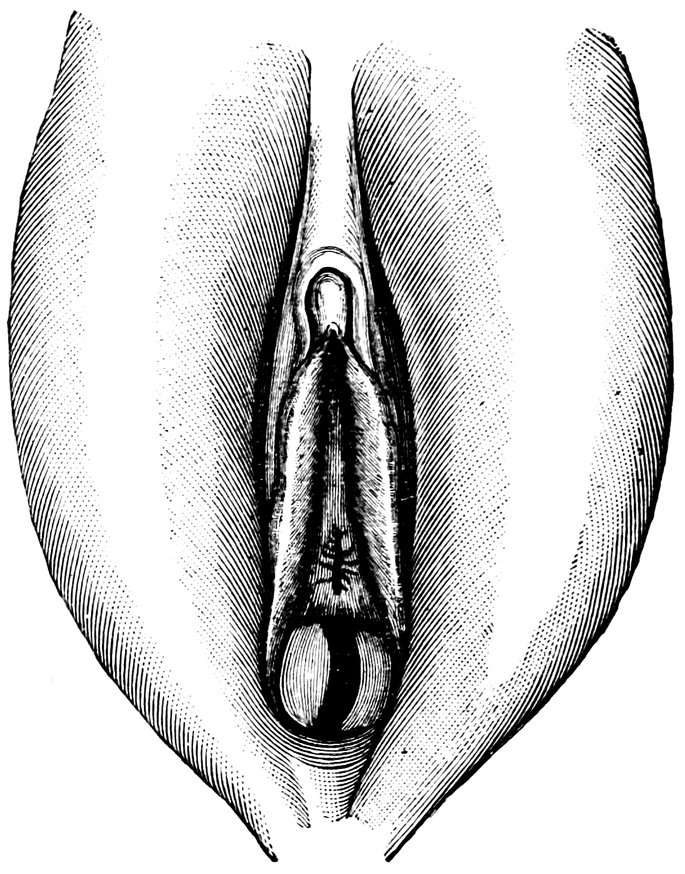
Fig. 65.—Septate Hymen, the septum having a tendinous consistency.
A notable and sometimes an insuperable obstacle (of which it has
been written, nec Hannibal quidem has portas perfringere valuisset)
is constituted by that abnormality of the hymen in which the aperture
in that membrane is guarded by a sagittally placed or sometimes
oblique septum, dense and almost tendinous in structure. In a
woman of twenty-four years, who for two years had lived in sterile
wedlock, I found such a tendinous hymen septum. She had menstruated
regularly since the age of seventeen years, but always painfully.
She complained that her husband was “very weak,” inasmuch
as on her bridal night he was unable to succeed in completing
intercourse, and since then whenever he attempted intercourse,
premature ejaculation resulted, before penetration of the penis
had been effected. In consequence of this repeated ineffectual
sexual excitement, she had herself become very nervous.
On local examination, I found an elongated oval hymen, not completely
325covering the vaginal orifice, rather strong and thick, and
divided in two halves by a median sagittal septum, of a densely
tendinous consistency. On either side of the septum, the vaginal
orifice would admit no more than the head of an ordinary uterine
sound. I divided this septum, and was informed later that the
woman had become pregnant as a result of the first subsequent act
of intercourse (Fig. 65).
A remarkable case of abnormality of the hymen is recorded by
Heitzmann, having been observed by him in a woman aged twenty-seven
years. In this instance, the hymen was represented by a swelling,
smooth on the surface and separated from the nymphæ by a
deep furrow. Behind this swelling, between it and the posterior
commissure, there was a deep depression, into which the finger
could be passed to a depth of an inch and a half or more. Anteriorly,
the very firm and fleshy prominence was bounded by a ridge, from
the middle of which to the urethral orifice ran a short but strong
and tense septum. Right and left of this septum were small apertures,
with difficulty admitting the point of a probe. Between the
anterior extremity of the septum and the urethral orifice was a
nodular representative of the swelling normally present in this situation.
Surrounding the urethral orifice were two or three additional
small nodules. The two lateral margins of the hymen were prolonged
around the urethral orifice, and united in front thereof to
form a raphe, which could be traced as far as the base of the clitoris.
The young woman had been married for some months, and asserted
that she had repeatedly had intercourse. With such a condition of
the female genitals, penetration of the penis into the vagina was
however quite impossible. During coitus, the penis must have been
inserted into the aforesaid depression behind the swelling, which
was sufficiently extensible for the purpose.
A less serious hindrance to intercourse, but one more frequently
encountered, is a partial persistence of the septum of the hymeneal
orifice, in such a manner that there is a projecting tongue of membrane
from the anterior and posterior margins of the orifice,
partially blocking this latter; or there may be a single median projection
only, either in front or behind. Such processes may be remarkable
alike for their size and their shape. Liman describes a
cordiform hymeneal orifice, constituted by an anterior or posterior
protection of the kind here described.
In cases of imperforate hymen in which the occlusion of the
vagina is not complete, impregnation may in rare instances occur,
326even though proper intromission of the penis is quite impossible.
Cases of this kind have been observed by Scanzoni, Horton, K.
Braun, Leopold, Brill, Breisky, and others.
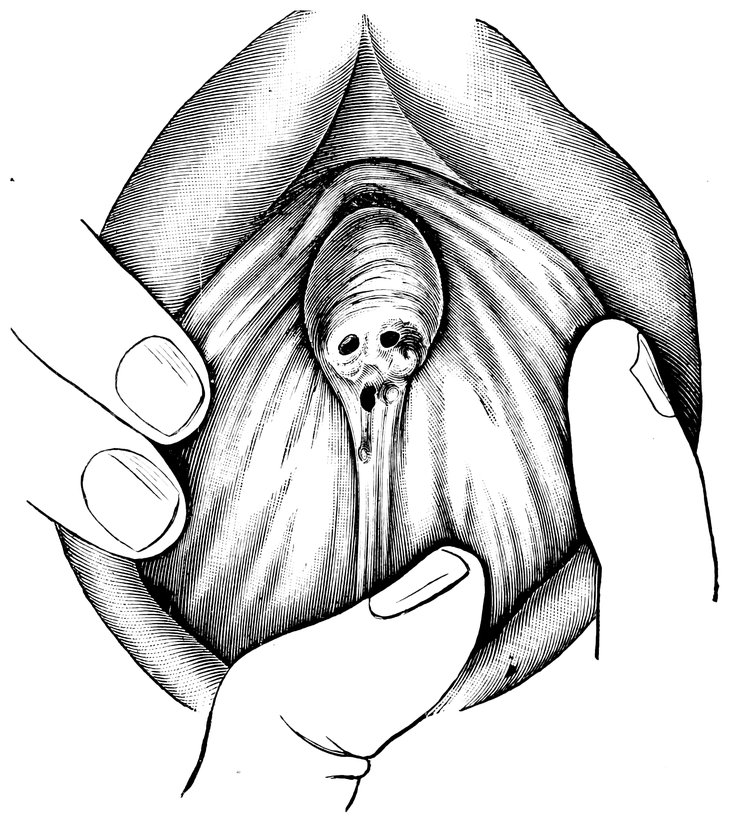
In most of these cases there was a thick, dense, “imperforate,”
or rather persistent hymen, with an orifice no larger than the head
of an ordinary probe, notwithstanding which pregnancy had occurred.
The cases reported by Brill were of a different character,
being those of two young unmarried Russian girls, with normal
undestroyed hymens, who were found to be pregnant. According
to Brill, such cases are by no means uncommon among the peasantry
of Little Russia, where the barbarous practice prevails of adolescent
girls and boys sleeping together. In these circumstances, sexual intercourse
takes place, but, from fear of consequences, it is often
incomplete. Hence, in occasional cases, results pregnancy in a
young girl with intact hymen.
In the first complete act of intercourse, the defloration of the
virgin, the hymen is as a rule torn in several directions, and in
consequence there is usually moderate bleeding. The lacerations of
327the hymen soon skin over. When the initial coitus is effected maladroitly
or roughly, more extensive lacerations are apt to occur, and
the injury may not be limited to the hymen, but may extend longitudinally
along the vaginal wall, and even involve the posterior
vaginal fornix. Or, again, without any such extensive laceration,
there may result very profuse bleeding, in consequence of abnormally
profuse vascularization of the hymen. Cases are also recorded
in which (presumably not from normal coitus alone, but
from other, unacknowledged manipulations), whilst the hymen has
been left intact, false passages have been made, leading to the formation
of fistulæ, with subsequent death from haemorrhage or
sepsis.
Apart from impotence in the male, the hymen may remain intact
when it is not touched at all during coitus. Inexperience, as Veit
remarks, will in this matter lead to results almost incredible. This
author has been informed by such inexperienced married couples,
that in attempts at intercourse “the penis of the man is introduced
between the thighs of the woman, which are closely pressed together,
the man having his legs on either side. Naturally, in this
method of intercourse, the hymen escapes destruction. In such attempts
at coitus, things are done which can hardly be compared with
the normal act of copulation.”
In isolated instances, the introduction of the penis is prevented by
congenital or acquired defects in the formation of the external
genitals. Adhesion between the labia majora and the labia minora
is sometimes met with a congenital deformity, which may or may
not be associated with atresia of the urethral orifice; in some cases
the adhesion is dependent merely upon a superficial epithelial continuity,
but in others the labia are firmly adherent throughout.
Less rare are acquired adhesions, the result of accident, between
the labia majora and the labia minora, leading to atresia of the
vulva, and thus making copulation impossible.
Intromission of the penis may be rendered quite impossible by
excessive size of the labia majora, consequent upon elephantiasis,
in which disease there is enormous hypertrophy of the subcutaneous
connective tissue. New growths may have the same result, fibroids,
for instance, lipomata, and cysts, which may attain a remarkable
size in the cellular tissue of the labia, the mons veneris, and the
perineum, and also in the nymphæ and in the cellular tissue between
the clitoris and the urethral orifice. In a very obese woman
twenty-eight years of age I saw a lipoma attached to the right
328labium majus. In the course of six years it had grown to such an
enormous size, that it extended downwards over the thigh, blocked
the entrance to the vagina, and made coitus absolutely impossible
(Fig. 67). Various forms of labial hernia are also competent to
occlude the vaginal orifice.
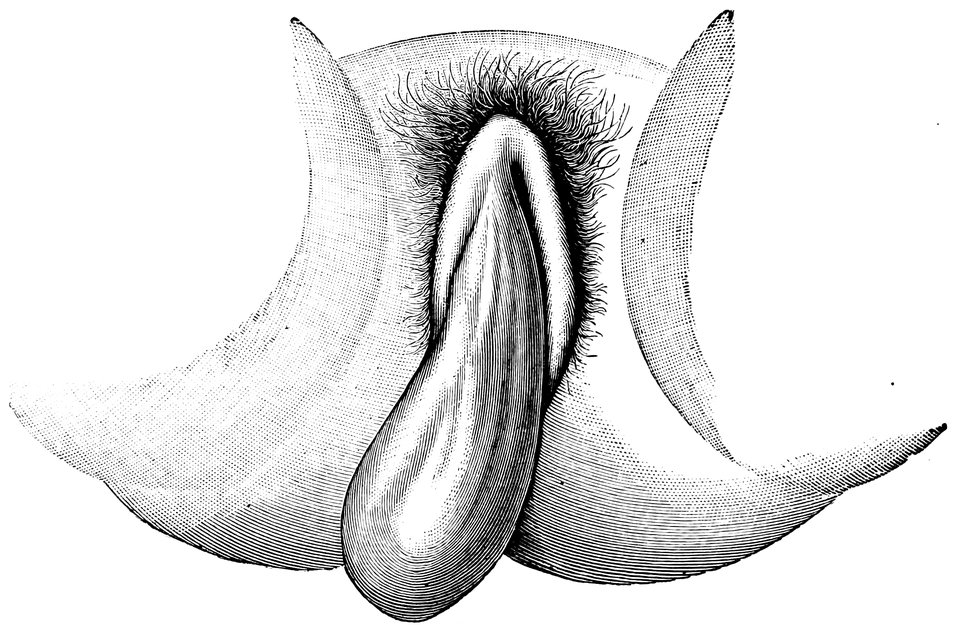
Fig. 67.—Lipoma of the right labium majus, occluding the vaginal inlet.
Hypertrophy of the nymphæ, which, as the so-called Hottentot
Apron has to be regarded as a racial peculiarity, is known also in
Europe as a pathological condition which may at times constitute a
hindrance to sexual intercourse (Fig. 68). According to Otto there
are three fundamental forms of the Hottentot apron, viz., excessive
enlargement of the nymphæ, overgrowth of the labia majora, and,
lastly, the formation of a peculiar lobe of flesh and skin, attached
to the mons veneris by a pedicle, containing the clitoris, and covering
the genital fissure as with a valve. Hypertrophy of the nymphæ
is said to be common also in Turkish and in Persian women. Owing
to the obstacle to intercourse presented by hypertrophied
nymphæ, it is among certain races an established custom to amputate
clitoris and nymphæ together. Virey writes: “The Portuguese
Jesuit missionaries to Abyssinia in the sixteenth century, endeavoured
to abolish this practice of the circumcision of women,
which they regarded as a relic of Mohammedanism; the uncircumcised
maidens, however, could find no husbands, owing to the inconvenient
length of their nymphæ. The pope sent surgeons
329to the country, to enquire into the matter, and their reports were in
such sense that circumcision was permitted as necessary.” Davis
reports observations made by Sonini on the female indigens of
lower Egypt, in whom the vulva hangs down in the form of a loose,
flabby mass of flesh, of striking length and thickness, completely
covering the genital fissure. He believes that the circumcision that
was practised on the women of ancient Egypt consisted in the removal
of this hypertrophied vulva.
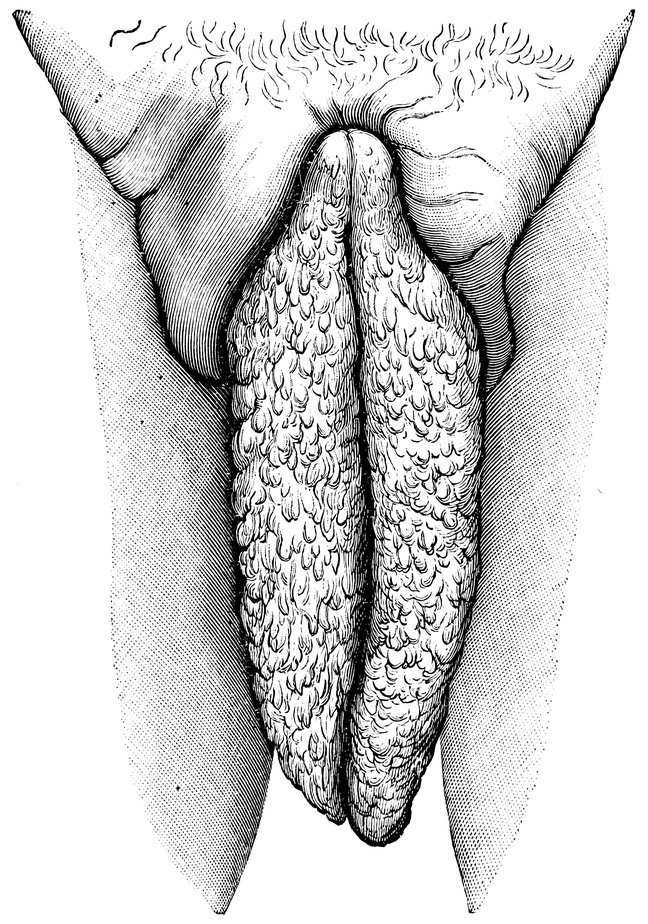
Fig. 68.—“Hottentot apron” in an adult woman, hanging down between the thighs. (After Zweifel.)
Courty saw a case in which the remarkable length of the labia
minora, which when an attempt was made to introduce the penis,
covered the vaginal orifice, had rendered coitus ineffective, and had
330caused sterility for five years. Resection of the labia minora was
followed by successful intercourse and conception.
The lipomatous form, especially, of elephantiasis vulvae often
attains a gigantic size. Growths of this nature, of the size of a
child’s head, weighing six or seven kilo (thirteen to fifteen pounds),
and reaching down to below the knee, are by no means rare. I
have known several cases in which an excessive accumulation of
fat in the vulva associated with pendulous belly has constituted a
mechanical obstacle to the completion of sexual intercourse.
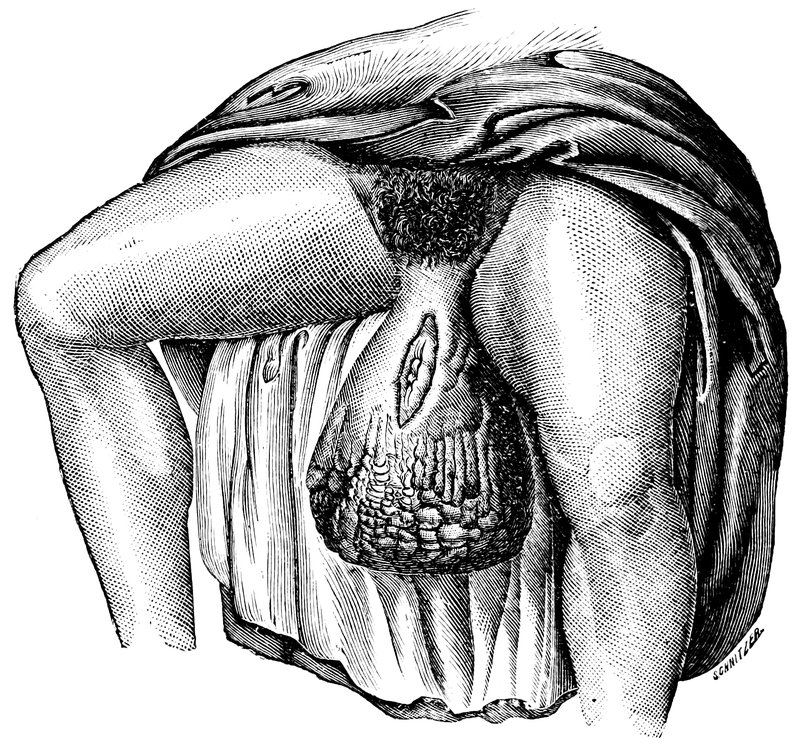
Fig. 69.—Elephantiasis of the labia majora
Hypertrophy of the clitoris may constitute an obstacle to coitus.
In exceptional cases, this organ is as large as the male penis, and
hangs down over the genital fissure like a valve. Hyrtl relates that
in certain African races, this congenital enlargement of the clitoris
is so enormous, that the organ, made fast to the perineum with
rings, serves for the protection of virginity. Schönfeld describes
the case of a woman aged twenty-eight years, in whom the vaginal
orifice was almost completely occluded by a dry and firm growth,
with a granulated surface. Close observation proved this growth
to be produced by a hypertrophied and degenerated clitoris, which
had attained the size of a child’s head. Elephantiasis of the clitoris
331is especially inconvenient in consequence of the hindrance which the
enlarged organ offers to sexual intercourse. Bainbridge describes
a case of tumour of the clitoris measuring 8 cm. (3.2 in.) in length
and 5 cm. (2 in.) in width. The following remarkable case is recorded
by Oesterlen: A young man wished to break off his engagement
on the ground that his intended wife was a hermaphrodite.
Examination, however, disclosed the existence of a strong intact
hymen, a very large clitoris, and pregnancy of the twentieth week.
Injuries of the vagina resulting from coitus are, generally speaking,
rare. The usual cause of such injuries is disproportion in size
between the erect penis and the calibre of the vagina, or else brutal
violence in the performance of coitus; sometimes, however, it is dependent
on the pathological state of the female genital organs, which
have undergone senile atrophy.
To the first group belongs the case reported by Albert, in which
a girl of eleven years was found to have a laceration of the vagina
communicating with the peritoneal cavity, the injury resulting from
coitus. To the second group belongs the case reported by Böhm,
of lacerations of the vaginal mucous membrane resulting from
forcible coitus in elderly women. E. Frank reports a case of injury
due to violent coitus in a woman in whom the vagina was already
greatly stretched by retroflexion; and another case in which injury
occurred during intercourse in a woman with vagina duplex—in
this case, not only was the hymen of the right vagina torn, but also
the septum between the two vaginae.
By no means extremely rare are injuries to the vagina in the
act of defloration, causing severe hemorrhage. Martin records a
fatal case of this nature. Maschka and Hofmann, the authorities
on Forensic Medicine, deny that vaginal laceration is the result of
simple coitus, and Hofmann maintains that such serious injury can
occur only from digital manipulations; in fact, these writers believe
that the penis alone cannot be employed with sufficient force to
cause laceration. Barthel and Anderson, however, saw vaginal
lacerations in nulliparous women; and Zeis records a case of vaginal
laceration in a woman twenty-five years of age, with whom, six
weeks after parturition, her husband, then in a state of intoxication,
had had intercourse in the position à la vache.
Anomalies of the vagina, absence, stricture, duplication, and abnormal
apertures, also diseases of the vaginal tissues, may induce
incapacity for sexual intercourse. In frequency as in significance,
among these disorders, absence of the vagina and stenosis and atresia
332of the canal, stand in the first rank. Congenital atresia may be
complete or only partial, according as the two ducts of Müller from
the fusion of which the tube is formed, remain totally or only partially
solid—or, having duly canalized, subsequently, by a foetal
inflammatory process, become transformed into a thick, more or less
solid cord. If the obliteration of the vagina is at the lower extremity
of the canal, coitus is impossible, unless, as sometimes happens,
by frequent attempts at intercourse, the short blind sac representing
the lower end of the vagina has been stretched upwards in the form
of a pouch. When the obliteration of the ducts of Müller is complete,
we have total atresia of the vagina, in which case the uterus is also
as a rule wanting, or is but imperfectly represented. In some cases,
from the ducts of Müller, instead of the normal vagina, there is
formed a tract of membrane of varying density and width, through
which passes a small canal for the passage of the menstrual discharge;
this condition is known as atresia vaginalis membranacea.
When, notwithstanding malformation of the external genital
organs and partial absence of the vagina, there is no defect in the
internal genital organs, conceptions may sometimes be effected
through some abnormal channel, as for instance through a communication
established per anum; or, again, some operative procedure
may bring relief. Rossi reports a case of congenital absence of the
external genital organs, in which an incision was made in the region
of the absent vagina, and an artificial vagina was thus constructed;
copulation was in this way rendered possible, and conception ensued.
In this connection, we may turn with interest to the essay by Louis,
entitled Deficiente Vagina, Possuntne per Rectum Concipere Mulieres?
Here we are told of a case in which vulva and vagina were
absent, and there was a monthly discharge of blood per anum; the
woman’s lover employed this passage also ad immissionem penis,
and the woman became pregnant. Pope Benedict XIV expressly
allowed to women suffering from imperforatio vaginae the practice
of coitus parte posteriori.
Further, in cases of atresia vaginae in which the genital canal
terminates in the urethra, conception can result from urethral coitus,
as is proved by cases recorded by K. von Braun, Weinbaum, and
Wyder. In Weinbaum’s case, the obliteration of the vagina was
complete, neither eye nor finger could detect the slightest aperture;
the woman having become pregnant after coitus per urethram, delivery
was effected by Caesarian section. In Wyder’s case, the vaginal
orifice was closed, with the exception of a minute aperture, by
333means of dense fibrous tissue; the woman was in labour and the
head of the child was in the pelvis. Under anæsthesia, the septum,
which was nearly an inch thick, was divided, the opening was enlarged,
and the child was extracted by forceps. An investigation
disclosed that the husband had always had intercourse by introducing
his penis into the dilated urethra; it was evident that the semen
had passed through the urethra into the bladder, and thence had
found its way through a vesico-vaginal fistula into the vagina and
uterus.
Acquired obliteration and stricture of the vagina from the contraction
of scar tissue, in consequence of deep ulceration, especially
when croupous or diphtheritic in nature, following typhus or typhoid,
pyaemia, puerperal sepsis, and the acute exanthemata
(especially variola)—may likewise serve as obstacles to coitus.
Syphilitic affections also, through contraction of exudations, the adhesion
of ulcerated opposing surfaces, condylomata, etc., may give
rise to stricture or obliteration of the vagina. The same conditions
may be induced by trauma, as by wounds, by attempts at rape, or
by the use of caustic acids and alkalis.
Thus, Ahlfeld saw severe stricture of the vagina as a sequel of
the excision of four large condylomata. Hennig the same, after
variola, and again in lunatics who had introduced caustic fluids into
the vagina. By L. Mayer, atresia vaginae was seen as a sequel
of typhoid; by Weiss as a sequel of diphtheria; by Martin from
the action of irritant secretions in cases of uterine tumour; by
Billroth as a result of continued irrigation of the vagina with alkaline
urine after lithotomy or urethrotomy, and in cases of vesico-vaginal
fistula. Ulcerative processes set up by the long continued
action of a vaginal tampon, a pessary, or some other foreign body,
have been noted as leading to consecutive obliteration of the vagina.
Such stenosis, when partial only, may prevent complete coitus,
and yet allow conception to occur. Cases illustrating this fact have
been numerously recorded. Thus, van Swieten already reported the
case of a girl aged sixteen years, whose vagina was strictured to
such an extent that the passage would barely admit a crow-quill;
nevertheless she became pregnant, and was successfully delivered.
Similar cases are mentioned by von Scanzoni, Kennedy, Devilliers,
Varge, Moreau, and Plenk.
Serious obstacles to coitus, of a nature analogous to acquired
stenosis of the vagina, are constituted by the irregular ligamentous
bridges which sometimes arise in the vagina from the adhesion of a
334strip torn from the mucous membrane on one side of the vagina to
the other side of that tube—or, again, a portion of a lacerated
cervix may adhere to the wall of the vagina. An interesting case
of this nature came under my own observation. It was a woman
aged thirty-two years, who had twice had difficult deliveries, the
last time nine years before. Since then she had been barren. On
local examination I found in the vagina a fleshy bridge, about 4 cm.
(1.6 in.) wide and 6 cm. (2.4 in.) long, extending from the left
side of the portio vaginalis to the right wall of the vagina; this
mass of tissue was so placed that the intromitted penis must necessarily
have slipped past it into a blind sac, such as the French name
une poche copulatrice. Similar membranes in the vagina have been
described by Breisky, Murphy, and Thomson.
Various tumours may narrow or even completely close the vaginal
passage, myoma, sarcoma, carcinoma, and especially the polypoid
form of fibromyoma, which may even project without the vaginal
orifice. And even when tumours of or in the vagina do not actually
hinder coitus by the space they occupy, they may affect that operation
by bleeding whenever it is undertaken, a manifestation extremely
alarming to young married persons.
The vagina may also be partially occupied, and coitus may be
impeded, by elongation of the hypertrophied cervix uteri, by inversion
or prolapse of the uterus, by cystocele or rectocele, and by
uterine polypi. Horwitz records the case of a woman aged twenty-two
years in whom impotentia coeundi was dependent upon the
occlusion of the vaginal orifice by a rounded, strongly projecting
body, which proved on closer examination to be a hypertrophied
vaginal bulb.
Tumours of the rectum and other intrapelvic growths may encroach
upon the vaginal passage and impede coitus. Closure of the
vagina has been brought about even by abnormal size and abnormal
toughness of the perineum.
Finally, in extreme degrees of pelvic contraction, the vagina may
be so much narrowed as to interfere with coitus. Von Hofmann
records a case of this nature: In a woman thirty years of age,
affected with kypho-scoliosis, who suffered extreme pain whenever
her husband attempted sexual intercourse, the pelvis was twisted
and narrowed to such an extent that the conjugate measured barely
one inch, and the vagina was so small as barely to admit the finger.
Duplication of the vagina will constitute an obstacle to coitus
when both halves of the passage are too narrow to allow of intromission
335of the penis. Difficulty in intercourse will also be caused
by abnormal termination of the vagina, as by its termination in the
rectum, likewise by severe perineal laceration which has converted
the lower parts of the vagina and rectum into a cloaca, likewise by
recto-vaginal and vesico-vaginal fistulæ; in the case of all these
latter states a feeling of disgust is apt to be aroused in the male
which may effectually check sexual desire. Still, coitus, and even
conception, are quite possible in these conditions. Kroner, among
sixty cases of vaginal fistula, observed six in which conception took
place while the fistula was actually open.
Apart from all local pathological conditions, coitus may be interfered
with by general nervous disturbances, manifesting themselves
locally, and depriving the woman so affected of potentia coeundi.
First among such states must be mentioned vaginismus, a condition
so important as to demand discussion in a separate chapter.
An important and by no means rare obstacle to the completion
of intercourse, affecting the male partner in the act, is partial or complete
incapacity for erection of the penis. Even excessive smallness
of the penis may render coitus inadequate; still more so, however,
organic diseases of the membrum, such as obliteration of the corpora
cavernosa, or of some of the trabecular channels of these
bodies, nodular formations resulting from injury, or cavernitis from
gonorrhoea. In such cases, erection is extremely irregular, and
the erect penis is sharply bent (chordee) instead of being straight,
a condition which renders intromission mechanically difficult if not
impossible. A similar effect is produced by ossification of some part
of the tunica albuginea of the corpora cavernosa—the so-called
penis bone. Mechanical obstacles to coitus are also offered by inguinal
and scrotal hernias; and by excessive obesity, where the
increase in thickness of the panniculus adiposus of the abdominal
wall and the mons pubis, whilst the penis itself remains as slender
as before, causes the organ almost to disappear from view.
Psychical impotence in the male is much more frequently observed
than organic impotence. We meet with this condition especially in
neurasthenically predisposed individuals, or in men who have been
given to excessive venery or have masturbated excessively in youth,
and who, when entering upon married life, fear they will be unable
to satisfy the legitimate desires of their wives; or in newly married
men who have suffered often from gonorrhoeal inflammations, such
as prostatitis, vesical catarrh, and epididymitis. The fear and anxiety
from which such persons suffer has an inhibitory influence upon
336the erection of the penis. In some instances, this inhibitory influence
is partial only, and the man thus affected, while perfectly competent
in intercourse with a prostitute, who employs means of sexual
stimulation to which he has become accustomed, is unable to complete
intercourse with his wife, who is ignorant and innocent, and
assumes a purely passive role; or it may be that erection is not sufficiently
powerful to bring about rupture of the hymen, and thus to
overcome the difficulties primae noctis.
As regards gonorrhoeal infection, it appears that in men who in
other respects are perfectly competent, this disease has an inhibitory
influence upon the nervous mechanism concerned in producing
erection of the penis.
Psychical impotence is usually transitory, but it may endure for
a very long time; and it may be many months before the husband,
whose nervousness has led to failure in the decisive moment at the
outset of married life, is able to command an erection sufficiently
powerful to bring about the defloration of his wife. Occasionally
such psychical impotence is not absolute but relative, it relates, that
is to say, to one particular woman—unfortunately, as a rule, a
man’s own lawful wife,—whilst coitus with another woman, even
in default of any measures for artificial sexual stimulation, is easily
effected. This fatal misfortune is especially liable to occur in cases
in which a man fully experienced in sexual matters marries a woman
whom he dislikes or for whom he has no regard; the marriage being
determined by material considerations. From such women I have
heard the painful confession that the husband, a man renowned for
his gallantries, played a very poor part in the bridal bed.
The impotence of irritable weakness is characterized by premature,
and therefore fruitless ejaculation. A man thus affected
has a powerful erection of the penis, preparatory to coitus, but at
the moment of contact with the female genital organs, before there
has been time for penetration to occur, ejaculation takes place, and
is immediately followed by relaxation of the penis. Such irritative
impotence is often met with in young men at the outset of their
sexual career, in beginners, whose sexual passion is very readily excited,
whose imagination shoots forward to the goal, and who are
unable to restrain themselves. This form of impotence can also be
cured by wisely chosen measures.
The paralytic form of impotence, on the other hand, is characterized
by the entire absence of erections of the penis, both overnight
in bed, and during the early morning hours; the penis always remains
337flaccid, or at most becomes semi-erect only, insufficiently rigid
for penetration. Ejaculation is much retarded or altogether
wanting.
Impotentia coeundi in the male may be complete, in cases in
which the erection-apparatus is entirely inactive, and in which even
an attempt at intercourse is out of the question; or, and this is
more frequently met with, it may be partial only, and manifests
itself in various degrees of imperfection in the performance of
coitus.
This latter form may often escape the woman’s notice. Whilst
complete impotentia coeundi, in which intromission of the penis is
impossible, is a state about which neither husband and wife can fail
to be fully informed, cases of partial impotence, with semi-erection
of the penis or premature ejaculation, are often glozed over by the
husband, ignored by the wife, and underestimated by the physician—and
yet such incomplete intercourse entails a series of ill-consequences
alike upon the genital organs and upon the nervous system
of the wife. Erection is incomplete, and thus the penis passes into
the vestibule only, and not deep into the vagina; even if penetration
is more thorough, the venous return of the blood from the corpora
cavernosa is not checked sufficiently to distend the penis to its full
size, and to bring it into close contact with the vaginal walls; or
ejaculation occurs prematurely, before the sexual organism of the
wife has attained that supreme degree which is needful alike for
the attainment of sexual gratification and for the occurrence of
conception.
Vaginismus.
Vaginismus is a disordered state, characterized by hyperaesthesia
of the hymen and of the entrance to the vagina, so extreme that,
even though the organs may be entirely free from any anatomical
abnormality, coitus is prevented, whenever attempted, by violent,
involuntary spasmodic contractions of the constrictor cunni and the
other muscles of the urogenital and anal region.
The centripetal paths of the reflex spasm characteristic of
vaginismus, run through the branches of the inferior hypogastric
plexus, and especially through the utero-vaginal plexus. The
spinal nerves connected with this part of the sympathetic are the
2d, 3d, and 4th sacral. The plexuses are constituted by fibres in
part from sympathic and in part from the 2d, 3d, and 4th sacral
nerves. Through the same nerves passes the centripetal motor tract
338for the transversus perinei muscle, and for the sphincter and levator
ani muscles. According to Eulenburg, the centre for this reflex is
to be found at the level of the first sacral nerve; when the disturbance
irradiates more widely, the lumbar and sacral plexuses as
a whole are involved. The constrictor cunni (sphincter vaginæ or
bulbocavernosus muscle) is supplied by the perineal branch of the
pudic nerve. The symptom-complex of vaginismus consists of
violent spastic contraction, for a term varying greatly in duration,
of the constrictor cunni (bulbocavernosus), sphincter ani, levator
ani, and transversus perinei muscles, the spasm spreading, in severe
cases, to other muscles in the neighbourhood, and especially to the
adductor muscles of the thigh; the spasm comes on when any attempt
at intercourse is made, and even when the genitals are merely
touched.
In young married couples especially, vaginismus is an extremely
distressing condition, and one that entails very serious consequences,
inasmuch as the pains and reflex spasms which result from any
attempt at coitus, and even from the mere approximation of the
penis to the female genital organs, render sexual intercourse absolutely
impossible. The cause of this pathological manifestation is
in part to be found in unskilful attempts at intercourse, which have
stimulated the female genital organs at some improper region. It
may be that the young husband is not fully instructed in sexual
matters, and does not really know how coitus ought to be effected;
in other cases there is some abnormality of the hymen, which has
rendered the rupture of that membrane extremely difficult; in some
cases there is partial impotence in the male, whose penis becomes
semi-erect only, so that ever-renewed attempts at intercourse are
followed by ever-renewed failure. Any of these causes may suffice,
in susceptible women, to originate vaginismus. The sufferer in these
cases will usually be found on enquiry to be hereditarily predisposed
to nervous disorder, and to be extremely sensitive to pain. By the
fruitless efforts of her ignorant or partially impotent husband, she is
sensually excited without ever being satisfied; the injured nervous
system responds by these local spasms, whilst ultimately, in some of
these cases, an actual psychosis ensues.
In a certain number of cases, however, the husband is in no way
responsible for the origin of vaginismus, which may depend on
pathological states of the female external genitals, leading to
hyperaesthesia; or, again, on primary hyperaesthesia of the pudic
nerve and its branches; or, finally, on general neurasthenia and
339hysteria, on excessive sensibility and lack of self-control on the
part of a young girl, who has entered upon married life under the
dominion of extravagant ideas. Vaginismus dependent upon general
neurasthenia especially in cases in which there is no strong
affection for the husband to give the spur to desire, and to enable
the woman to bear with fortitude the pangs which form the necessary
introduction to the joys of wedded life. It must not be forgotten,
as throwing light on the origin of vaginismus, that in the
digital vaginal examination of a virgin or even of a young wife,
unless extreme care is taken, pain and painful muscular spasms are
liable to be evoked.
The local pathological conditions of the female genital organs
that are most often met with in cases of vaginismus are: a very
rigid state of the hymen; inflammation and excoriation of the hymen
and its surroundings; fissures at the vaginal orifice; inflammatory
affections of the vaginal follicles; inflammation of the carunculæ
myrtiformes; a peculiar formation of the vulva, which extends
forwards over the pubic symphysis, whereby the urethral orifice
and the hymeneal aperture come to lie upon the pubic symphysis
or the subpubic ligament; vulvitis; herpes or eczema of the vulva;
colpitis; urethritis; fissure of the anus; papillary growths; pruritus
papules; urethral caruncle; inflammation of Bartholin’s glands; at
times gonorrhoeal infection.
A case came under my own observation in which a newly married
woman suffered from vaginismus. The husband believed the
cause of the trouble was his own partial impotence, consequent
upon youthful venereal excesses, and yielded to the desire of his
wife and her relatives that a divorce should be obtained. A year
later, the woman remarried, when, to her horror, the symptoms returned
in full force. Now for the first time she consulted me, and
on local examination I could detect no abnormality whatever. The
vaginismus was in this instance a pure neurosis, the only possible
cause of which was to be found in bygone overstimulation of the
vaginal orifice, the wife admitting previous onanistic excesses. In
another case known to me, vaginismus in the wife made the husband
an involuntary sodomite. The movements of the wife when
the spasm came on led to the introduction of the penis per anum,
and coitus had repeatedly been effected by this abnormal route,
when the fact first became apparent as the result of a local
examination.
Le Fort reports the case of a young Russian wedded pair who
340were spending their honeymoon in Paris. The husband took so
much to heart his inability to fulfil his marital obligations in consequence
of the vaginismus from which his wife suffered, that he
shot himself through the heart. The distressing situation of a
husband whose wife suffers from vaginismus, rendering coitus impossible,
is depicted in the well-known French romance, “Mademoiselle
Giraud, Ma Femme.” From a false shame, women often
continue to suffer from vaginismus for months and even years,
without a single effective coitus having ever taken place; it is only
the consequent sterility which at last leads to medical advice being
sought. The physician then usually ascertains that the hymen is
still intact, or at least incompletely destroyed, that on this membrane
and on various parts of the vulva there are erosions, and
that the whole of the external genitals outside the hymen are in a
state of inflammation more or less acute. In other cases, however,
neither excoriations, erosions, nor inflammation can be detected, and
the existence of vaginismus can be proved only by the pain and
the muscular spasm set up by contact with the vagina. Often, indeed,
the cause of this most distressing affection cannot be discovered.
Introduction of the penis may be rendered impossible by spasm
of the constrictor cunni (bulbocavernosus) muscle, but equally so
by spasm of the transversus perinei or the levator ani muscle.
Sometimes the spasm affects all three muscular groups; in which
case the narrowing of the vagina is extreme, and extends for some
way up into the canal. When the levator ani alone is affected by
the spasm, the penis can, indeed, be introduced into the vagina, to
encounter a powerful obstacle in the interior of that canal; and
it may happen, when the spasm comes on and affects the levator
ani only after complete intromission of the penis, that the glans is
retained in the vaginal fornix by the active contraction of the pelvic
floor.
More or less credible instances of penis captivus thus brought
about are on record. The following history is by Davis: A gentleman
entering his stable found therein his coachman and a servant-maid
in a most compromising position. All endeavours of the pair
thus surprised to separate proved ineffectual, and their attempts to
draw apart caused them intense pain. Davis was sent for, and
ordered an iced douche, which, however, failed to liberate the imprisoned
penis. Release was impossible until the woman had been
placed under chloroform. The swollen and livid penis exhibited
341two strangulation-furrows, a proof that two distinct areas of the
levator ani muscle had been spasmodically contracted.
Hildebrand records three cases observed by himself in which there
was spasm of the upper part only of the vagina, unaccompanied by
vaginismus (i. e., by pain). In two of these cases, the spasm was
originated by the contact of the examining finger with very painful
ulcers of the portio vaginalis; the third patient had a very sensitive
prolapsed ovary. Fritsch reports having had on one occasion to
give a woman chloroform for the release of a swollen and imprisoned
penis.
Hildebrand suggests that vaginismus may be caused by an abnormal
size of the penis, or by a condition occurring in weaklings
and alcoholic subjects, in whom the greatest swellings of the glans
penis occurs before intromission, whilst this greatest swelling is
normally deferred until towards the end of the act, when the glans
is in the vaginal fornix.
Schröder writes as follows regarding the etiology of vaginismus:
“The affection is dependent upon trauma, sustained in maladroit,
frequently repeated attempts at sexual intercourse; for this reason
it is met with, in the great majority of cases in young, newly married
women. Impotence in the male is by no means necessary for
its production, and such impotence is not even a frequent antecedent.
Abnormal narrowness of the vagina, or extreme firmness of the
hymen, is occasionally found, but neither is in any way necessary;
all that can be said in this connection of a small vaginal orifice is,
that it predisposes to vaginismus. If the husband is devoid of previous
experience in sexual matters, maladroit attempts at intercourse
are exceedingly likely to occur. The penis is thrust in the wrong
direction, pressing against either the anterior or the posterior commissure
of the vulva. Very often, moreover, the position of the
vulva, which is subject to very striking individual variations, is
concerned in the production of vaginismus. There are many women
in whom the vulva lies in part in front of the symphysis pubis, so
that the lower border of the symphysis lies below the urethral orifice.
In such cases the penis is directed too far backwards, and instead of
passing into the vaginal orifice, slips into the fossa navicularis.
The frequent repetition of such maladroit attempts at intercourse
gives rise to a gradually increasing sensitiveness of the
parts concerned, with the formation of excoriations. It now results
that, on the one hand, the woman dreads attempts at intercourse
on account of the pain to which they give rise; she shrinks away
342from the man, so that penetration of the vagina by the penis is
rendered even more difficult than it was before; and, on the other
hand, ungratified sexual desire leads to the frequent repetition of
attempts at complete intercourse (from which, moreover, if conception
should ensue, a cure of the trouble is expected). In this way,
the trauma is rendered more severe, the congestion and excoriation
of the fossa navicularis or of the urethral region are aggravated,
and the sensitiveness of the parts increases to such a degree that the
woman thus affected screams out when the vulva is merely touched.
Ultimately reflex cramps set in whenever intercourse is attempted,
and we then have the fully developed clinical picture of vaginismus.”
Winckel maintains that in most cases there are two principal
elements in the causation of vaginismus. In the first place, in consequence
of more or less pronounced anatomical changes, there is
undue sensitiveness and tenderness of the vaginal inlet and its
neighbourhood, and in exceptional cases also of the upper part of
the vagina, the uterus, and the ovaries. In the second place, the
patient manifests an increased general sensitiveness and nervous
irritability; this is in some cases primary, but in others it is entirely
the result of the repeated stimulation; and in either case it is
heightened by the effects of ungratified sexual desire.
A. Martin points out that the spasm of the muscles of the pelvic
floor, and especially of the levator ani muscle, upon which vaginismus
depends, may be due in some cases to the influence of chill,
since the same cause will lead to pathological contractions in other
muscular areas. But in such cases it is always open to question if
masturbation or some other sexual perversion is not the true cause
of the disorder. In some instances vaginismus is merely a symptom,
in extremely sensitive women, of various diseases of the reproductive
organs, and is brought on by the increased pain which
in such cases is caused by attempts at intercourse; when produced
in this way, vaginismus is usually a transient manifestation.
Veit considers that among the pathological conditions giving rise
to vaginismus, we must also enumerate diseases of the internal
pelvic organs, such as chronic metritis, displacements of the uterus,
oöphoritis, etc.; but he also attaches great importance to nervous
predisposition, consequent upon previous sexual stimulation, and
upon pre-existing inflammatory changes due to gonorrhœal infection.
A peculiar form of vaginismus is, according to Veit, sometimes
observed after the birth of the first child; happily the duration
of this is usually brief. After parturition the vulval mucous
343membrane remains for a time very tender, and when cohabitation
is resumed, often too soon, and perhaps, after the enforced abstinence,
too frequently repeated at brief intervals, fissures are readily
produced. Moreover, vaginismus which has existed prior to parturition
may, in some cases, recur after that event. An unusual
position of the vulva, undue smallness of the vaginal inlet, and
relative impotence of the man, may combine to cause such a recurrence.
Finally, vaginismus often persists throughout pregnancy,
and manifests itself during parturition. The magical effect which
chloroform has in some primiparæ, when the head is delayed at
the vulva, is explicable only by the supposition of vaginismus.
According to Arndt, vaginismus is not purely a local disorder,
but is in many cases the local manifestation of a neuropathic diathesis,
which may in some instances lead to general mental disorder.
Olshausen regards hyperæsthesia and vaginismus as different
stages of a single disease; he believes that the excessive sensitiveness
is seated chiefly in the hymen; he explains the spasm as the reflex
result of fissures and inflammatory changes. Pozzi considers that
excessive nervous irritability and an irritable state of the vulva
are the indispensable preliminaries to the occurrence of vaginismus.
Herman distinguishes between excessive smallness of the vaginal
inlet and vaginismus; he regards the latter as a nervous disorder,
characterized by hyperæsthesia of the vulva, and by spasmodic
contraction of the levator ani and adjoining muscles. Frost distinguishes
vaginodynia from vaginismus; in vaginodynia the pain
is so intense as to cause syncope, and the muscular spasm involves
the entire length of the vagina.
It is a notable fact, to which Veit has especially drawn attention,
that among the poorer classes of the population, vaginismus is
practically unknown. Among women of these classes, their sexual
needs, not having been so much lessened by “culture,” suffice
to withdraw their attention even from the pains of defloration,
which would otherwise often be very severe; whereas the sexually
neurasthenic woman of the upper classes, filled with dread at the
idea of the pain she expects to suffer, and not infrequently in a
condition of hyperexcitability or hypersensibility dependent upon
previously employed abnormal means of sexual gratification, is
unable to endure the pains of defloration even when these might be
expected to prove far from severe.
In some cases, painful contractions of the vagina, to which we
cannot properly give the name of vaginismus, arise from organic
diseases of the uterus and the uterine annexa; these painful contractions
344render copulation impossible. Von Hofmann reports the
case of a young prostitute, who found herself unable to continue
the practice of her profession owing to the severe pain she suffered
during intercourse; she died, and the post mortem examination disclosed
bilateral salpingitis, with reproductive organs in other
respects normal.
Maladroit and incomplete attempts at intercourse, and the consequent
repeated failure to obtain complete sexual gratification,
affect a woman’s nervous system to a varying degree; but apart
from this, in women who have long cohabited with men of deficient
sexual potency, we often find a remarkable condition of complete
relaxation of the genital organs, associated with great hypersecretion
of the mucous membrane, flaccidity of the muscles of the
pelvic floor, and displacements of the uterus. Moreover, the nervous
shock to which the repeated but unsatisfying attempts at intercourse
give rise, affects the spinal cord in such a manner that
symptoms of spinal irritation ensue. The patient complains of
pains in the back, the loins, and the nape of the neck; these pains
also radiate round the front of the abdomen and along the intercostal
spaces; hyperæsthetic points may be detected when the finger
is passed along the spine; there is weakness of the limbs with a
sensation of numbness; and neuralgic manifestations of varying
nature occur.
The dangers which sexual intercourse may entail upon women—over
and above the irritable conditions and inflammatory disorders
of the female reproductive organs, dependent upon impetuous
or unduly frequent coitus, or upon coitus practised during
menstruation—are principally due to gonorrhœal and syphilitic
infection transmitted by the cohabitating male.
Cardiac Troubles Due to Sexual Intercourse.
Among the troubles from which women at times suffer as a result
of sexual intercourse, certain cardiac disorders are especially
worthy of attention.
Every act of sexual intercourse in a young and sensitive woman
exercises an exciting influence on the nervous mechanism controlling
the cardiac movements, and this influence is more clearly
manifested in a degree directly proportional to the intensity of
the sexual orgasm. The heart’s action is markedly increased in
frequency, the cardiac impulse is more powerful, the large arteries
of the neck are seen to pulsate far more vigorously, the conjunctiva
345is markedly injected, the respiration is increased in frequency, the
respiratory movements are more superficial and have a panting
character.
But when, in a woman who is sexually irritable in an excessive
degree, the peripheral stimulation occurring in the act of sexual
intercourse is unusually powerful, there may result a notable increase
or modification of the reflex manifestations which normally
occur during sexual intercourse in the province of cardiac activity;
similar results ensue when there is a summation of stimuli owing
to excessive sexual intercourse, or contrariwise when the act of
intercourse is broken off just before its physiological climax and
the natural termination of the orgasm fails to occur.
The former cause is not infrequent in young wives during the
period of the honeymoon. The latter cause is in operation when
there are diseases of the female reproductive organs preventing the
physiological completion of intercourse; but especially in consequence
of the modern practice of coitus interruptus, in which the
man breaks off the act of intercourse the moment he feels that
ejaculation is imminent, without troubling himself regarding the
natural course of sexual excitement in the woman. Yet another
cause of excessive cardiac reflex manifestations in women is incomplete
potency of the male, which may either cause a premature
ejaculation of semen, or may lead to incomplete penetration of the
penis.
In all such cases, as a result of sexual intercourse, there may
arise cardiac disorders of various kinds; among these, tachycardial
paroxysms are the most frequent, occurring either inter actum,
or at a longer or shorter interval after intercourse.
In several cases of vaginismus occurring in young married women
which have come under my notice, it was observed that the attempts
at intercourse gave rise to violent involuntary spasmodic
contractions of the constrictor cunni and the other muscles of the
urogenital and anal regions, and in addition it was found that
these attempts were followed by tachycardial paroxysms with
dyspnœic manifestations, lasting for a considerable period, it might
be as long as one or two hours.
In women who had practised coitus reservatus for a prolonged
period, in fact for several years, in such a manner that, notwithstanding
the occurrence of intense voluptuous excitement, complete
sexual gratification rarely, if ever, occurred—in such women, in
whom these marital malpractices seemed to have profoundly influenced
346their psychical life, I have frequently witnessed a form of
reflex cardiac disorder which I must regard as a variety of the
multiform neurasthenia cordis vasomotoria. In such women, still
at the climax of their physical powers and of their sexual needs,
attacks of palpitation suddenly occur at irregular intervals, several
times daily or less frequently. Associated with this increased frequency
of the cardiac activity are an extremely distressing feeling
of anxiety, a sensation of faintness, headache, vertigo, a weakness
of the muscular system, and at times actual attacks of syncope.
Physically, the women are extremely depressed, irritable, inclined
to weep, unhappy, and weary of life. At the same time, digestion
is impaired, the appetite is small, and there is constipation. The
pulse is in most cases feeble, small, of low tension, easily compressible,
increased in frequency, often intermittent, sometimes
more distinctly arhythmical. The heart is found to be sound on
physical examination, nor can any abnormality be detected in the
great vessels. The lower extremities are free from œdema; the
urine does not contain albumen.
Women thus affected are sometimes believed to be suffering
from cardiac disorder, in other cases they are subjected to various
modes of gynecological treatment; until at length the physician, by
appropriate questions, becomes enlightened regarding the true
cause of the cardiac disorder, namely, coitus interruptus. If it is
possible to prohibit effectually this unwholesome practice, the cardiac
symptoms soon cease to recur.
Finally, in women at the climacteric age, cardiac troubles sometimes
ensue, which are dependent on interference with sexual intercourse
in consequence of anatomical changes in the vagina; changes
of this character frequently occur at the time of the menopause;
owing to hyperaemic or inflammatory processes, a partial or general
stricture of the vaginal passage results; in many cases this passage
becomes narrower, shorter, and almost conical in shape, whilst the
vaginal inlet is greatly diminished in size. Such a vaginal stricture,
which Hegar has also seen in younger women after an artificial
climacteric (oöphorectomy), interferes with sexual intercourse;
and the incomplete sexual gratification gives rise to a series
of nervous manifestations, and, among others, to the above described
reflex cardiac neurosis.
Whether, and in which cases, the cardiac disorders evoked as a
result of the local stimulatory influences of sexual intercourse, are
dependent on a reflex stimulation of the sympathetic nerve on the
347one hand, or upon a transient paresis of the inhibitory centre of
the heart and of the vasomotor centre on the other, cannot here
be fully discussed; just as little can we consider in what manner
the psyche is sympathetically affected by the irritative processes in
the genital organs, and its functional activity thus impaired.
Here I can do no more than briefly state that experience has
taught me that sexual intercourse is competent to originate cardiac
troubles in women.
1. In extremely sensitive, sexually very irritable women, tachycardial
paroxysms may result from sexual excesses.
2. Tachycardial paroxysms with dyspnœa occur in young women
affected with vaginismus; also in women at the climacteric with
constrictive changes in the vagina.
3. Cardiac troubles, characterized mainly by symptoms indicating
diminished vascular tone, occur in women who have long practised
coitus interruptus with incomplete gratification of their voluptuous
desires.
Dyspareunia.
In normal conditions the act of sexual intercourse is accompanied
in women, as in men, by a voluptuous sensation, and this
sensation must be regarded as a necessary link in the chain of those
processes by which gratification of the sexual impulse—the most
powerful of all our natural impulses—is obtained. The absence
of this voluptuous sensation in a woman, the state in which she
experiences during coitus no voluptuous sensations, but feels either
apathy, or positive distaste, is termed dyspareunia: in former times
it was also known as anaphrodisia. This abnormal state of sexual
sensibility, which up to the present is hardly alluded to in gynecological
textbooks, has received remarkably little attention from
the medical standpoint, and its importance has been underestimated.
Most unfortunately so, for dyspareunia is an important
symptom, exercising a powerful influence on the general health of
the woman who suffers from it, upon her social status in marriage,
and, as is easy to understand, upon her procreative capacity.
Dyspareunia must be clearly distinguished from two somewhat
similar conditions, with which at first sight it is liable to be confused,
namely, from anæsthesia sexualis, and from vaginismus. By
sexual anæsthesia we understand, as previously explained, the absence
of the sexual impulse, a symptom which, when the reproductive organs
are normal in structure and function, is either of central nervous
origin, a result of disease of the brain or spinal cord, or else is
due to general nutritive disorders such as diabetes, morphinism,
348or alcoholism. A woman affected with dyspareunia does, however,
experience the sexual impulse, it may be very actively, but sexual
intercourse brings about no gratification of her desires. In
vaginismus, on the other hand, the introduction of a foreign body,
that is to say of the membrum virile, into the vagina, gives rise to
painful reflex cramps of the sphincter vaginæ, or of the muscles
of the pelvic floor, whereby the completion of coitus is rendered
impossible: whereas in dyspareunia coitus can be effected, but gives
rise to no voluptuous sensations.
The pleasure which normally occurs in woman during sexual intercourse
is brought about in this way, that contact with and friction
by the penis stimulates the sensory nerves of the clitoris, the
vulva, the vestibule, and the vagina; this stimulus is propagated to
the cerebral cortex, where it gives rise to voluptuous sensations, and
then, by reflex stimulation of the genito-spinal centre, gives rise to
a series of reflex discharges. The pudic nerve, a branch of the
sacral plexus, supplies the female external genital organs. Some
of its branches pass in the clitoris to a peculiar form of nervous
end-organ discovered by W. Krause, Krause’s genital corpuscles:
the structure of these corpuscles appears to fit them exceptionally
well for the transmission of stimulatory waves to the nerve centres.
“When this stimulus,” says Hensen, in his work on the physiology
of reproduction, “in addition to other effects, also gives rise to a
voluptuous sensation, the cause must be sought in central nervous
connections and apparatus. Similar relations are to be found in
connection with the mechanism of nutrition, for example, in the
association of hunger, appetite, agreeable sensations of taste, the
act of mastication, and the secretion of saliva.” By means of this
stimulus, several reflex processes are originated in the reproductive
canal, the most notable of which are the erection of the clitoris,
and the ejaculation of the secretions of various glands. The cavernous
tissue of the clitoris is connected with that of the bulbus
vestibuli, and the dorsal nerve of the clitoris is one of the principal
nerves of voluptuous sensation. The venous plexus constituting
the bulb of the vestibule lies at either side along the margin of the
vestibule at the boundary between the labium majus and the labium
minus, and laterally it is covered by the constrictor cunni[48] muscle.
349During coitus the blood is driven out of this bulb into the glans
clitoridis, and thus the sensibility and the erection of the glans are
increased. The constrictor cunni and ischiocavernosus muscles
draw the clitoris, which is bent at a right angle downwards, into
contact with the penis. By means of the pressure of the constrictor
cunni, the mucous secretion of Bartholin’s glands, which
open into the vulva at the back of the labia majora, is expressed.
As additional reflex actions, dependent upon the activity of the
reflex centre in the lumbar enlargement of the spinal cord, there
ensue contractions of the vagina, peristaltic movement of the tubes,
some descent of the uterus, relaxation of the os uteri and rounding
of this orifice, and induration of the portio vaginalis, whereby the
tubal and uterine mucus and the secretion of the cervical glands
are expressed. This process of ejaculation constitutes the culminating
point of the voluptuous sensation occurring in the sexual
act; this act thus exhibits two phases, the sensation of friction, and
the sensation of ejaculation.
With regard to voluptuous sensations, and processes analogous
to pollutions, occurring in women, we append an extract from
von Krafft-Ebing.
“The occurrence of voluptuous excitement during coitus is dependent
in the women, just as in the man, upon:
“1. The peripheral influence of the intensity and duration of the
sensory stimulation (anæsthesia of the genital passage may be the
cause of the absence of voluptuous sensation). 2. The condition
of excitability of the reflex (ejaculation) centre in the lumbar
spinal cord. The activity of this centre varies within wide limits,
not merely in different individuals, but in the same individual at
different times. There are, indeed, women in whom it seems as
if this centre were always in vigorous activity. In normal women,
the irritability of the centre appears to be most marked at the
menstrual epoch, and to decline rapidly soon after menstruation.
In pathological conditions, the activity of the centre may be temporarily
in abeyance (organic inhibitory processes, such as are seen
in certain cases of hysteria with temporary frigidity); or again
the centre may be abnormally active owing to irritable weakness
(neurasthenia sexualis), in consequence of which ejaculation may,
just as in the male in similar circumstances, occur too easily. 3.
The occurrence of the voluptuous sensation in woman is unfavourably
influenced by psychical inhibitory perceptions (analogous to the
inhibitory influence of psychical processes in the male, such as, for
example, fear of incapacity to perform sexual intercourse). As
350examples of such inhibitory perceptions in women may be mentioned,
dislike of the man, physical loathing to sexual intercourse,
etc.”
Gutceit records interesting experiences, which are readily intelligible
in view of what we have already quoted. He finds that of
ten women after defloration, two only immediately experience full
sexual pleasure. Of the eight others, four only have an agreeable
sensation produced by the friction during coitus: but the sensation
of ejaculation does not make its appearance until the lapse of at
least six months, or it may be even several years, after marriage.
In the remaining four women, pleasure during sexual intercourse
may never become properly established. The women of the first
class are described by the author as being of a very ardent temperament,
and passionately attached to their husbands. In such
women, the sensation of ejaculation occurs during intercourse with
any man toward whom they are sympathetic. Women of the second
class are of a less ardent temperament, and are often comparatively
indifferent toward the man with whom they cohabit. Women of
the third class have little or no amatory feeling, and they either
hate the man with whom they are cohabiting, or at least feel
physical repulsion to the idea of intercourse with him. Gutceit
considers that meretrices usually belong to the third category. In
the practice of their trade, they make a counterfeit of voluptuous
enjoyment, and only experience real sexual gratification in intercourse
with the man of their choice.
It is of great practical interest, alike from the gynecological and
from the neuropathological standpoint, to determine the consequences
in women of ungratifying sexual intercourse. In the present
state of our experience it must be assumed that the effect of
abnormal sexual intercourse, that is of intercourse which does not
culminate in gratification produced by the sensation of ejaculation,
is deleterious. This is explained by the fact that, owing to the
absence of the muscular contraction of the genital passage, the
latter remains engorged with blood; the resultant hyperæmia passes
away very slowly, and, when frequently repeated, gives rise to
chronic tissue changes, manifesting themselves as diseases of the
reproductive organs. Injury to the nervous system ensues, partly
in consequence of these organic changes, partly also in consequence
of psychical non-gratification in the widest sense of the term. The
nervous disorders thus produced are typical forms of (sexual)
neurasthenia; and in cases in which the pathogenesis is predominantly
psychical (antipathy to the husband, etc.) hysterical types
351of disorder are especially frequent. Von Krafft-Ebing believes that
incomplete coitus, that is, coitus not culminating in the sensation
of ejaculation, is a frequent cause of hysterical disorders in women.
When once the clinical picture of neurasthenia sexualis is fully
developed, each act of intercourse (like pollutions or coitus in the
sexually neurasthenic male) gives rise to renewed troubles, which
are easily recognized as symptoms of venous stasis in the reproductive
organs (sacrache, sensations of weight and bearing-down
in the pelvis, fluor albus): in addition we observe exacerbations
of the lumbar spinal disorder, in the form of spinal irritation,
irradiating pains in the sacral plexus, etc. In this way general
neurasthenia develops. The conditions found in such cases on
gynecological examination (chronic endometritis, metritis, oöphoritis,
etc.) are produced by the same cause as the nervous symptoms,
namely, by an unhygienic mode of sexual intercourse. They
are not the cause of the neurosis, but important concomitant disorders;
and their effect in rendering the nervous disturbances more
severe must be freely admitted.
Among important causes of ungratifying coitus must be enumerated:
weak erection and ejaculatio praecox in the male, rendering
the stimulation inefficient; in addition, coitus reservatus, coitus interruptus,
and coitus condomatus. If the noxious influence is frequently
repeated, the occurrence of neurasthenia sexualis and its
consequences is greatly to be feared, and in women of neuropathic
constitution it is practically inevitable.
Unsympathetic coitus appears to act, not merely in a somatic
manner, but mainly upon the psyche, and to originate states of
hystero-neurasthenia or pure hysteria. If the influence of such unhygienic
conditions of the vita sexualis co-operates with that of
inherited or acquired sensuality, further dangers ensue: in cases
of ungratifying sexual intercourse, the danger of manustupration;
in cases of unsympathetic intercourse, the danger of psychical onanism,
or that of marital infidelity.
Although until recently the matter received but little attention,
it must now be regarded as a well-established fact, that in the
female (as in the male) the climax of voluptuous sensation in sexual
intercourse is normally characterized by a process of ejaculation,
accompanied by a voluptuous sensation of ejaculation, dependent
upon the acme of excitement of a reflex centre in the lumbar enlargement
of the spinal cord.
Just as in the male, this centre may be excited to action, not only
by local stimulation of the genital organs, but also by (psychical)
352stimuli proceeding from the brain (pollutions), so also in the
female a similar process may occur, and for this reason it is correct
to speak of “pollutions in the female.” Rosenthal appears to
have been the first writer to speak of pollutions in women. In his
clinical study of nervous diseases, Rosenthal described processes of
the nature of pollutions, originated in erotically over-stimulated
women by lascivious dreams. In one case he detected the outflow
of a “mucus-like” fluid from the apparently intact genital organs;
he believed this to proceed from the ducts of Bartholin’s glands,
and from the mucous glands surrounding the urethral orifice. Féré
reports the case of a patient who had an erogenic zone in the region
of the upper part of the sternum; pressure on this zone gave rise
to a profuse secretion of vulvo-vaginal fluid. In this connection
we may also recall the “clitoris-crises” to which tabetic women
are subject. Gutceit described the process of pollution in women
in the following words: “It is remarkable that in dreams
such women experience the sensation of ejaculation.”
The psychical preliminary is invariably constituted by lascivious
dream perceptions. It merely remains open to question whether
this process, which in the male is indisputably physiological, in the
female may be said to occur within physiological limits. The researches
published by von Krafft-Ebing more than twenty years
ago, under the title “Concerning Processes Analogous to Pollutions
Occurring in the Female,” gave negative results as far as
healthy individuals were concerned; on the other hand, the phenomenon
in question was by no means rare in nervously disordered,
and above all in sexually asthenic women. The neurosis was in
part found as a result of psychical or manual onanism in virgins
with morbidly intensified libido: in part in married women, as a
result of ungratifying coitus, as previously described: in part, also,
in married women with powerful libido and enforced abstinence
from intercourse, owing to acquired impotence or death of the
husband.
Just as in the case of the neurasthenic male, these pollutions
made the primary neurosis more severe, and relief from the nervous
trouble was not obtained until the factor of the “pollutions” had
been recognized, and made the object of special treatment. In exceptional
cases the “pollutions” appeared to be the starting point
of the entire neurosis.
It was further remarkable, again here displaying analogy with
what occurs in the male, how much stronger and more deleterious
353was the shock-effect of an inadequate process of ejaculation occurring
in a sexual dream, as compared with the far less deleterious
influence of similar incomplete ejaculation when occurring viâ
coitus. In very severe degrees of neurasthenia sexualis, just as
in the male, the waking imagination may give rise to a “pollution.”
In such cases the shock-effect on the nerve centres tends to be
excessively severe. A still higher degree of irritability of the genital
system appears to exist in cases in which excitement and orgasm of
the reproductive organs may culminate in a “pollution” by purely
spinal paths, without the intervention of the imagination. The significance
of this fact would appear to be considerable for the proper
comprehension and for the treatment of certain conditions of neurasthenia
(sexualis) in the female. The “pollution” may here
be the actual cause of the neurosis. But in any case, in the female,
the occurrence of pollutions is an extremely important symptom
as regards both diagnosis and therapeutics. It is extremely probable
that hallucinations of coitus, and the complaints made by insane
women of attempted violation during the night, are really
dependent upon such “pollutions.”
Von Krafft-Ebing reports the following characteristic case. Miss
X., thirty years of age, belonging to a family predisposed to insanity,
and herself neuropathic since early childhood, declared that
since she was six years old she had been subject to lascivious
imaginations, to which she became continually more liable as she
grew older. Ultimately, typical psychical onanism developed, and
in recent years her trouble assumed the form of sexual neurasthenia.
The patient herself suspected there was a connection between
her nervous disorder and her evil habit. The popular work by
Bock finally brought her full enlightenment, associated with severe
emotional disturbance. This latter was now increased by misfortunes
from which the family suffered. The patient then relinquished her bad
habit, but her state of health nevertheless became worse. She was
nervously extremely irritable; her sleep was insufficient, unrefreshing,
and disturbed by lascivious dreams; she suffered from
spinal irritation, anæmia, scanty and painful menstruation. Inclination
toward the opposite sex and toward marriage, hitherto but
slight, now sank to a minimum: on the other hand, the patient, in
spite of all efforts to the contrary became more and more subject
to a condition analogous to priapism in the male, a genital orgasm
by no means voluptuous in character, and often indeed actually
painful. Associated therewith, nocturnal pollutions occurred, the
354patient awaking from lascivious dreams with a voluptuous sensation
and moistness of the external genital organs. After such pollutions,
throughout the ensuing day, she felt extremely weary and
depressed and suffered from severe spinal irritation. After a time,
the nocturnal pollutions occurred without being preceded by lascivious
dreams, and ultimately analogous states were experienced in
the daytime. With much difficulty the patient now made up her
mind to seek medical advice. She was anæmic, emaciated,
emotional, and moody. The lumbar and cervical regions of the
spine were extremely sensitive to pressure. Sleep was scanty and
unrefreshing, the patient felt weary and miserable, she complained
of dragging sensation and other paralgic sensations, in the regions
supplied by the lumbar and sacral plexuses. The deep reflexes were
increased. She dreaded the onset of disease of the spinal cord, and
believed that the cause of her illness was to be found in the prolonged
indulgence in psychical onanism. The perusal of Bock’s
book had first made her understand the true nature of her misconduct.
She had never practised manual masturbation. Her principal
complaint was of an almost unceasing uneasiness and excitement
in the genital organs. She compared it to the uneasiness in
the stomach produced by hunger. In the genital organs (which on
examination appeared quite normal), she had a distressing sense
of burning heat, of pulsation, of disquiet as if there were a clockwork
mechanism working there. Very rarely now were these sensations
associated with voluptuous ideas. This sexual neurosis had
an intensely depressing constitutional effect. She had transient
relief only when the local sensations culminated in pollution; but
this, on the other hand, increased her general neuropathic troubles.
She suffered most severely during the menstrual period. She was
ordered sitz-baths at a temperature of 23° to 19° R. (84° to 75° F.),
suppositories of monobromide of camphor, 0.6 (9 grains), with extr.
belladon. 0.04 (⅗ gr.), sodium bromide 3.0 to 4.0 (45 to 60
grains), every evening; also powders containing camphor 0.1 (1½
grains), lupulin 0.05 (¾ grain), extr. secal 0.08 (1¼ grains),
twice daily. This treatment gave the patient great relief, and
secured complete ease during the daytime. Therewith returned her
greatly impaired trust in the future, and her emotional calm was
restored.
The frequent occurrence of pollutions in women, the so-called
vulvo-vaginal crises and clitoris-crises, is regarded by Eulenburg
as a striking manifestation of sexual neurasthenia in woman; in
355such cases a lascivious dream is spontaneously followed by a more
or less abundant discharge of the clear gelatino-mucous secretion
of Bartholin’s glands. In women who masturbate, and in tribadists,
a profuse and even violent secretion of these glands is produced by
touching the clitoris or the erogenic zones at the entrance to the
vagina, close to the orifices of Bartholin’s ducts.
Dyspareunia, the absence of voluptuous sensation in women
during coitus, may be referred to three fundamental causes:
1. Insufficient or completely wanting peripheral stimulation of
the sensory nerve terminals in the female reproductive canal: in
these cases the conducting tracts to the nerve centres never become
active.
2. Diminution or cessation of the excitability of the reflex centre
in the lumbar enlargement of the spinal cord: this leads to failure
of the sensation of ejaculation.
3. Inhibitory influences proceeding from the cerebral cortex
whereby voluptuous sensations and perceptions are checked.
The first-named of these etiological influences is in my experience
the commonest. Incomplete or quite inadequate stimulation of
the sensory nerves of the genital canal may be due to the maladroit
performance of copulation on the part of the male, owing to inexperience,
or it may depend on gross disproportion in size between
the reproductive organs of the man and the woman; in other cases
it may be due to disease of the reproductive organs in either sex,
influencing unfavourably the sensibility to stimulation of the nerves
of the genital canal. Awkward or incomplete performance of
coitus may thus lead to failure of voluptuous sensation, and this
may ultimately pass into permanent dyspareunia. Temporary dyspareunia
is very common in young wives during the first months
of married life, ensuing on the pains of defloration; and very gradually
gives place to normal voluptuous sensation. It may be one
or two years after marriage before the sensation of ejaculation is
first experienced. Not infrequently, dyspareunia depends on incomplete
potency in the husband, who is incompetent to arouse
voluptuous sensation in his wife. For this reason, dyspareunia is
common in young women married to elderly men; but is common
also, where (as so frequently among Russo-Polish Jews) the men
also marry very young, at an age of from sixteen to seventeen years,
and where, moreover, the husband has often before marriage impaired
his potency by masturbation: finally dyspareunia is common
when girls still undeveloped sexually are married to powerfully
built men.
356Regarding the pathological conditions of the female reproductive
organs which counteract the peripheral sensory excitants of voluptuous
sensation, we exclude from further consideration the obvious
causes, absence and atrophy of the reproductive organs, and senile
marasmus. Of prime importance as a cause of the failure of sexual
sensibility in the early period of married life must be mentioned
inflammation of the fossa navicularis, due to awkward attempts at
intercourse. Other causes of deficient sensibility are: complete or
partial persistence of the hymen, lesions of the vaginal inlet, acute
or chronic vulvitis in consequence of irritating abundant secretion,
especially as a sequel of gonorrhœal vaginitis. The last named infective
disorder is especially harmful, because Bartholin’s glands
are involved in the associated vulvitis. Even after the cure of the
vulvitis, permanent dyspareunia may remain. Perineal fissures may
result in the stimulant effect of coitus being insufficient, owing to
the slight friction possible at the vaginal inlet in these cases. Not
less serious sometimes are small, hardly discernible fissures in the
vagina. Additional causes of deficient sexual sensibility are recto-vaginal,
and vesico-vaginal fistulæ.
The second cause of dyspareunia, diminution or complete lack
of irritability of the reflex centre of the lumbar enlargement of
the spinal cord, appears to be less frequently operative. We must,
however, assume that certain nervous disorders, such as hysteria
and pathological changes in the spinal cord, are responsible in this
connection. The activity of the lumbar sexual centre appears in
women to be normally subject to variation within certain limits;
and seems usually to attain its maximum irritability during menstruation.
But normally these variations are never so great as to produce
in women complete though merely temporary dyspareunia; in
this respect offering a marked contrast to what occurs in other
animals at other times than the rutting season, and of which every
bitch not on heat furnishes an example when she refuses the sexual
advances of the dog.
As regards the third causal influence in the production of dyspareunia,
the influence of the brain, this, though important, is less
frequently in operation. Diseases of the brain, degenerative processes,
may constitute a cerebral cause for the failure of sexual
sensation. But more frequently, certain cortical perceptions, such
as dislike or hatred of the cohabiting male, an ardent passion for
some other lover, grief and trouble, exercise inhibitory influences,
which render the occurrence of voluptuous pleasure during the
sexual act difficult or quite impossible.
357A condition like dyspareunia, our knowledge of which depends
entirely upon the subjective sensations of the woman concerned, is
naturally one regarding whose existence accurate information is
difficult to obtain. Very rarely does it happen that women spontaneously
approach the physician with complaints of this condition;
indeed, in my experience, they do so only when they are
sterile, and when they assume, in accordance with the widespread
popular belief, that their sterility is connected with the absence of
voluptuous sensation during sexual intercourse. More commonly,
however, it is the husband who feels it his duty to confide to the
medical man the remarkable apathy of his wife in sexual intercourse.
But when once the medical man’s attention has been
directed to this question, and when he institutes enquiries among
his patients in a scientific, passionless manner, one making due allowance
for a woman’s modesty, as the moral importance of the
subject demands, he will be astonished at the frequency of dyspareunia,
and he will find herein the explanation of many obscure
phenomena in the life of women. On the other hand, it must never
be forgotten that a certain number of women complain of dyspareunia
without any justification whatever, in order to arouse interest
and sympathy, by representing themselves as unwilling sacrifices
on the marital altar: the experienced gynecologist will readily
detect the cases in which he is being misinformed; he can, moreover,
always check the wife’s statements by conversation with the
husband.
The constant sign of dyspareunia is the failure of ejaculation
during coitus. We have previously described the muscular contractions
which lead to ejaculation of the secretion of Bartholin’s
glands and to the expulsion of the uterine and cervical mucus,
as reflex actions evoked by the sensory stimulus dependent on
friction of the female genital organs. The voluptuous sensation of
ejaculation, associated with these muscular contractions, which the
woman whose sensibility is normal experiences as the culminating
point of her sexual “gratification,” is either quite unknown to a
woman affected by dyspareunia, or is experienced by her only in a
voluptuous dream, as a pollution, in which the sexual dream-perceptions
act as the psychical stimuli by which the reflex discharge
is originated. It has repeatedly happened to me, that on
enquiring of women suffering from dyspareunia regarding their
experience of the sensation of ejaculation, I have been informed
that such sensations are known to them only from the descriptions
of their female friends, or occasionally from dreams from which
358they have awakened with a feeling of moisture in the external genitals.
Von Krafft-Ebing refers this process to a peristaltic contraction
of the muscular fibres of the Fallopian tubes and the uterus,
“whereby the tubal and uterine mucus is expressed;” whereas, for
my part, I am of opinion, that ejaculation affects in the first place
and principally the glands of Bartholin, the secretion of which is
expressed by the contraction of the constrictor cunni muscles, and
secondarily only affects the cervical glands of the uterus.
As a second sign of dyspareunia, I recognize a remarkably rapid
outflow of the male semen from the female genital canal, immediately
after coitus (profluvium seminis). The woman thus affected
complains, when suitably questioned, that she is unable to retain
the semen, and that it flows out of the vagina immediately after
ejaculation. The cause of this remarkable phenomenon no doubt
lies in the fact, that, owing to the absence of the voluptuous sensation,
the reflex contractions of the muscles of the female genital
organs, normally accompanying this sensation during intercourse,
fail to occur. At the vaginal inlet, in normal conditions, the constrictor
cunni muscle contracts, and farther up in the vagina a
peristaltic contraction of the circularly disposed muscular fibres
of the tunica media occurs: in this way the semen ejaculated into
the vagina is for a time retained under a certain pressure. But in
the absence of these muscular contractions, as well as of the muscular
contraction of the pelvic floor, retention of the semen fails
to occur. Cattle-breeders and horse-breeders have made similar
observations regarding cows and mares, namely, that these animals
are sometimes unable to retain the semen after coitus, and it is
suggested that in these cases the animals are not properly on heat.
Experienced cattle-breeders recommend in such cases that the retention
of the semen should be promoted by douching the root of
the tail and the external genitals with cold water. It is well known
that by stimulating the peripheral sensory nerves in the neighbourhood
of the genital organs, a reflex excitement of the lumbar sexual
nerve centre is produced, as is seen, for example, in the practice
of flagellation of the buttocks, for the increase of sexual desire.
Passing to the consideration of the pathological changes to be
found in the reproductive organs of women suffering from dyspareunia,
the nature of these will for the most part be obvious in relation
to the etiology of the disorder. Most frequent, in my experience,
were chronic inflammatory states of the vulva and of the
vaginal and uterine mucous membrane, chronic metritis and parametritis.
359A very frequent appearance, and one practically characteristic
of dyspareunia when of long standing, is a marked total
relaxation of the reproductive apparatus. The uterus is extremely
mobile, usually retroverted and partially prolapsed, thin, with lax
walls, and usually an enlarged cavity; the portio vaginalis is flaccid,
and runs to a point; the vagina is roomy; there is marked hypersecretion
of the mucous membrane of the entire genital canal;
there is great flaccidity of the constrictor cunni and levator ani
muscles, and of the perineum. In several women with dyspareunia,
I found old unhealed lacerations of the perineum. In some cases,
the very small size of the clitoris is noteworthy. In one case
amenorrhœa was present with an infantile uterus. In a large proportion
of the cases I was able to detect a diminution both of the
tactile and algic sensibility of the vaginal mucous membrane. The
women were for the most part anæmic; many were extremely
obese, and of lymphatic constitution. In some cases, however, no
pathological changes whatever could be detected in the reproductive
apparatus.
Dyspareunia is a condition which affects a woman’s whole nature,
powerfully influences her mental life, and thus gives rise to greater
psychical than physical damage. The consciousness of being deprived
of the greatest joy of physical love produces great emotional
depression, even in a woman by no means sensually inclined,
and gives rise to a hypochondriacal state, at times even to melancholia.
In other cases, the idea, not infrequently suggested by
more happily situated women friends, that the woman herself is
not to blame for this condition, has a demoralizing effect upon her,
and destroys the happiness of married life. (It has been confessed
to me, in isolated cases, that the dyspareunia was relative only.)
Apart from this, the absence of sexual gratification gives rise to a
series of nervous troubles, presenting either the variable characters
of hysteria, or else the symptoms of neurasthenia. Finally, the frequently
repeated incomplete coitus, incomplete inasmuch as the
woman does not experience the sensation of ejaculation, induces
chronic hyperæmia in the female reproductive organs, passing on
into blood stasis, and ultimately into chronic inflammatory tissue
changes; in this way arise metritis, perimetritis, and parametritis,
salpingitis, oöphoritis, disorders of menstruation, menorrhagia, and
atypical uterine hæmorrhages. The possibility cannot be disproved,
that in this way new-growths of the reproductive organs may also
originate. The act of sexual intercourse, which at first may be to
360the woman a matter of comparative indifference, and in which she
plays her part merely from a sense of duty, becomes, in cases of
long-standing dyspareunia, something to which she feels a positive
dislike, and is recognized by her as the actual cause of the troubles
that ensue upon intercourse, such as sacrache, sensations of weight
and pressure in the pelvis, strangury, fluor albus, a feeling of exhaustion,
etc.
At times, perverse sexual sensation is associated with dyspareunia.
Women who find no enjoyment in normal sexual intercourse
with a male, sometimes masturbate, sometimes indulge in
amor lesbicus, etc.
Of great importance appears to me the relation between dyspareunia
and sterility in women. As already pointed out, dyspareunia
comes chiefly under medical observation in cases in which it is
associated with sterility. The husband, seeking advice concerning
his wife’s failure to conceive, complains of her frigidity in sexual
intercourse as the probable cause; or the wife comes to seek advice,
saying that she never experiences sexual gratification, and
that for this reason she has failed to become pregnant. As a matter
of actual fact, dyspareunia and sterility are associated with such
remarkable frequency, that my own experience leads me to believe
in the existence of an etiological connection between the two
conditions, at least in a certain proportion of the cases. Among
69 sterile women whom I questioned regarding dyspareunia, the latter
condition was present in 26, that is to say, in 38% of the cases.
Matthews Duncan reported that of 191 sterile women, 62 did not
experience sexual enjoyment. Sexual excitement of the woman
during copulation would certainly appear to have a definite bearing
upon the occurrence of conception, for we know that by the voluptuous
sensation reflex actions are aroused in the genital canal,
favouring the retention of semen and its passage through the os to
the interior of the uterus, and perhaps also giving rise to reflex
changes in the cervical secretion which favour the passage of the
spermatozoa into the uterine cavity.
In cases of relative dyspareunia, the influence of this condition
in producing sterility is also manifested, the unfaithful wife being
impregnated by her lover though she has remained sterile in intercourse
with the husband to whom she is indifferent. To dyspareunia
of this nature (dependent upon sexual disharmony), we
may also refer the sterility of a married pair who have for some
time lived together in unfruitful intercourse, whereas, after divorce
and the contraction of fresh unions, both the man and the woman
361prove normally fertile. Such cases have been personally known
to me; and similar instances aroused the attention of the natural
philosophers of antiquity, for instance, that of Aristotle. The importance
of voluptuous sensation in promoting conception is also
manifest from the fact that in the majority of women, after the
pains of defloration, dyspareunia usually persists for a season during
the early period of married life; and, corresponding with this, the
first conception is usually deferred for some little time after marriage,
to a period corresponding with the awakening of the sensation
of ejaculation. In this connection, Courty reports the case
of a lady who, although in blooming health, remained sterile during
the first fifteen years of her married life; she then gave birth to
a child whose father was unquestionably her lover; and after this
in succession to two other children whose progenitor was the legal
husband. This lady had never experienced voluptuous sensation
in intercourse prior to the time of her first conception. Similar
circumstances with an even clearer significance have been frequently
observed among the lower animals; and Darwin records
several striking observations of this character. Taking all the
evidence into consideration, we are compelled to regard dyspareunia
as a condition capable of causing sterility in women, although the
sequence is not an absolutely necessary or invariable one.
In order to excite voluptuous sensation during intercourse, savage
races make use of various means, some of which we here
transcribe from the work of Ploss-Bartels. In Abyssinia, and on
the Zanzibar coast, young girls receive instruction in certain rotary
muscular movements known by the name of duk-duk, which they
employ during coitus for the increase of sexual pleasure. Many
Daiaks perforate the glans penis with a silver needle from above
downwards; this needle is kept in place like a seton, until a permanent
canal is formed through the glans: in order during coitus
to stimulate the woman more powerfully, into this canal, just
before coitus, various small articles are inserted, such as little
rods of brass, ivory, silver, or bamboo, or silver instruments ending
in small bundles of bristles; these project from the surface of
the glans, and exercise a more powerful friction of the vagina,
thus increasing the sexual pleasure of the woman. Men without
such an apparatus are rejected by the women, whilst those who
have made several such canals in the glans, and can therefore insert
several instruments, are especially sought after and prized by
the women. Such an apparatus is known as an ampallang, and
362in a symbolic manner the woman indicates to a man of her choice
her desire that he should make use of one; he finds in his bowl
of rice a rolled-up leaf, enclosing a cigarette which represents the
size of the desired ampallang. Among the Alfurs of North Celebes,
in order to increase the voluptuous pleasure of the woman
during intercourse, the men bind round the corona glandis the
eyelids of a goat, beset with the eyelashes, thus forming a bristly
collar; in Java and in Sunda, before coitus, the men surround the
penis with strips of goat-skin, leaving the glans free. In China they
wind round the corona glandis torn fragments of a bird’s wing;
these also project like bristles and increase the friction. Among
the Batta of Sumatra, travelling medicine-men perform an operation
by means of which they insert, beneath the skin of the penis,
small stones, sometimes to the number of ten, at times also angular
fragments of gold or silver; these heal in beneath the skin, and
increase the stimulus of coitus for the women. Among the Malays
of Borneo the penis is perforated, and some fine brass wire with
the ends turned inwards is inserted: before coitus, the sharp ends
of the wire are drawn out so as to project from the skin.
In our own part of the world, voluptuaries make use of an india-rubber
ring beset with spines, which before coitus is passed over
the corona glandis, in order to promote sexual gratification in the
woman during intercourse. In cases of diminished potency in the
male, in order to produce sufficient sexual excitement in the female
by more powerful erection of the penis, various mechanical means
are now employed. For instance, in such a partially impotent
man, a constricting band of india-rubber may be passed over the
root of the penis, whereby the reflux of blood from the corpora
cavernosa is hindered, and a more complete and more enduring
erection is induced. Elderly men have frequently declared to me
that they were well satisfied by the employment of this simple
measure, whilst behind their backs, their wives have assured me
that the results were far from satisfactory. The apparatus described
by Roubaud for the enlargement of the penis is no longer
employed. Partially impotent men make use, however, of an instrument
known by the name of “schlitten,” made of gold, silver,
or white-metal; it consists of two delicate laminæ, united at the
base by a metal ring, and at the upper end by an india rubber ring.
This small apparatus, which must be made exactly to measure, renders
possible the introduction of the imperfectly erect penis into
the vagina; it supports the penis, and readily accommodates itself
to the change in size of the organ as it slowly becomes erect.
363
Fertility in Women.
Fertility in women is the basis of the fecundity of a nation, of
its growth, its power, and its importance. It is especially the
fertility of married women which enters here into consideration,
and forms the source of the statistical data of fertility; these are
usually obtained by drawing a ratio between the number of marriages
contracted in a given period, and the number of children
born in the same period.
The fertility of women is a function beginning at an age varying
in dependence on many conditions, and undergoing extinction at
a definite period of life. It is, in fact, associated with the duration
of the sexual life of woman, and, generally speaking, extends
from the sixteenth to the fiftieth year of life. Climate,
race, constitution, and morbid conditions, influence alike the first
appearance of menstruation and the first pregnancy; and as they
influence the duration of menstrual activity, so also do they influence
the duration of fertility.
In the Bible are recorded numerous instances of the early
commencement of fertility. At the present time also, in
warm climates we meet with many examples of early motherhood.
From the great work of Ploss-Bartels, from which we
have already frequently quoted, we extract and summarize the
following ethnographical details. Among the wives of the Bosjesman,
mothers aged ten are frequently seen; travellers in New
Zealand often saw mothers of eleven years, and mothers of the
same age among the Samoyedes and in Palestine; mothers of
twelve in British Guiana, in Jamaica, among the Schangallas, at
Shiraz in Persia, among the Copts in Egypt; mothers aged thirteen
in Cuba, among the Sioux and the Dakotas, and in New
Caledonia; mothers aged fourteen among the Negroes of Gaboon.
According to the observations of Robertson, of sixty-five Indian
women there gave birth for the first time:
| At the age of 10 years |
1 |
| At the age of 11 years |
4 |
| At the age of 12 years |
11 |
| At the age of 13 years |
11 |
| At the age of 14 years |
18 |
| At the age of 15 years |
12 |
| At the age of 16 years |
7 |
| At the age of 17 years |
1 |
Moreover, in the records of European countries, we find numerous
instances of very early motherhood. Molitor’s case, a girl nine
364years old giving birth to a vesicular mole with an embryo; von
Haller’s case, pregnancy in the ninth year of life; Carus’ case,
pregnancy at the age of eight. Caspar saw a girl in Berlin who
became pregnant at the age of twelve, and was delivered of a
living child. Rüttel saw a girl nine years of age pregnant. King
attended the confinement of a girl who at the time of her delivery
was not yet eleven years old. Taylor reports the case of a girl
twelve years and six months of age who was then in the last month
of pregnancy. Koblanck attended a girl of fourteen who was
delivered of a child weighing four and a half pounds.
In most of these cases the premature fertility is followed by a
premature cessation of fertility. And there is more or less truth
in Bruce’s statement regarding the Arab women in Africa, that
those who began to bear children at the age of eleven were seldom
still fertile at the age of twenty.
At times we may observe a remarkable extension of fertility beyond
the average age, that is, beyond the age of fifty years.
In northern Europe pregnancy at a comparatively advanced age
is by no means rare. From the official statistics of Denmark we
learn that among 10,000 women, 465 were delivered at ages between
50 and 55 years. In Sweden, of 10,000 mothers, 300 gave
birth to children when more than 50 years of age. In Ireland, the
proportion of mothers over 50 was 345 per 10,000. In England
the official figures dealing with the delivery of 483,613 women,
showed that 7,022 were between 45 and 50 years of age, and 167
over 50 years of age.
The Surgical Academy of Paris, in an authoritative statement
regarding the late age at which conception could take place, alluded
to the fact that Cornelia, of the family of the Scipios, gave birth
to Volusius Saturninus when sixty years of age, that the physician
Marsa in Venice recorded the existence of pregnancy in a woman
of sixty, that de la Motte recorded pregnancy in a woman of fifty-one,
and that he believed it to be true that another Parisian woman
had given birth to a girl at the age of sixty-three, and had herself
suckled the infant.
In an important case, however, which came before the Court of
Chancery in England, the court held that there was no definite
evidence of the possibility of pregnancy in a woman sixty years
of age; but that the greatest age at which, in England, pregnancy
had indisputably occurred, was 54.
Among 4,925 deliveries occurring in the Prague Maternity Hospital,
365Schwing reports that there were 9 women delivered for the
first time when over 40 years of age. Of these:
3 were 41 years of age.
2 were 42 years of age.
1 was 43 years of age.
2 were 44 years of age.
1 was 47 years of age.
Haller reports the cases of two women who gave birth to children,
one at the age of 63, the other at the age of 70 years. Meissner
delivered a woman of 60 years of her seventh child; Rush
attended the delivery of a woman aged 60; Dewees that of a
woman aged 61. Mende and Bernstein report cases of delivery
at the age of 60. Marion Sims saw, in the state of Alabama, a
negro woman 58 to 60 years of age, who gave birth to a child at
this age, at an interval of twenty years since her last pregnancy.
Nieden reports a case in which the first pregnancy occurred 26
years after marriage. When married, the wife was 18 years of
age, the husband 30; during their first twenty-five years of married
life there was no sign of pregnancy, but when the wife was 44
years of age, menstruation, hitherto regular, suddenly ceased; the
cause of the cessation proved to be pregnancy, and at term a
healthy girl weighing nine pounds was born; the mother was able
to nurse the child herself. Smith attended a woman aged 52 who
was delivered of twins; the youngest of her eight other children,
who were then all living, was ten years of age.
Rodzewitsch collected from the Russian literature of the years
1872 to 1881, eleven cases in which women aged 50 to 55 had given
birth to children. Talquist reports that in Finland, in the year
1883, a woman 58 years of age was delivered; whilst Ansell records
the case of an Englishwoman who became a mother when
59 years of age. John Kennedy records the case of a woman of
62 who was normally delivered at this age; she had begun to
menstruate at the age of 13, and since the age of 20 had previously
given birth to 21 children, the last five when she was 47,
49, 51, 53, and 56 years of age, respectively. Prior even reports
the case of a woman 72 years of age, who not only menstruated, but
had an abortion(!)
The ideal of fertility in women is that the first completed act of
sexual intercourse should be followed immediately by conception,
that the pregnancy should terminate after the normal lapse of
time in the birth of a child, and that the same process should be
366repeated at intervals of about ten months until the end of active
sexual life. In actual experience, however, this never occurs.
Fertilization as an immediate consequence of the first act of sexual
intercourse (which in the lower animals is regarded as the rule)
is a very rare occurrence in human beings. Moreover, in no
single marriage is the reproductive capacity of the wife utilized
to the full, up to the time of extinction of her generative faculty;
either because the potency of the male partner undergoes a gradual
decline, or, it may be, because, after a while, sexual intercourse
becomes less frequent, or because precautions against procreation
are taken.
The number of children to which during the three decades of
her sexual life, from the menarche to the menopause, a woman
might theoretically give birth, is never actually born. If we assume
that, during the period of active sexual life, a woman requires
a period of fifteen months to two years for each pregnancy,
parturition, and lactation, a woman could easily during this period
have fifteen or sixteen children, and this figure would represent
the normal product of the normal fertility of the human female.
There are indeed, women who, it may be in consequence of an
exceptionally long period of sexual activity, or through giving
birth repeatedly to twins or triplets, or because they have married
several husbands in succession, have given birth to twenty-four
children or even more. In Berlin, in the year 1901, there lived a
woman 41 years of age who had had 23 children; there were three
women, aged respectively 40, 43, and 46 years, who had had each 21
children; 246 women with families numbering 13 to 20; and 169
women each of whom had given birth to 12 children. In the
very great majority of cases, however, the fertility of the wife of
the present day is never fully developed. It is modified in various
ways by the conditions of marriage, by social circumstances, by
considerations relating to the health of husband or wife, by actual
illnesses, and by voluntary limitation of fertility. Generally speaking,
according to the investigations of Quetelet, Sadler, and Finlayson,
the fertility of women is greatest in marriages in which the
husband is as old as the wife, or a little older, but without marked
difference in age. Marriages contracted at a very early age are
less fruitful; the highest fertility is found in marriages contracted
when the husband is 23 and the wife 26 years of age.
Conception does not generally take place until sexual intercourse
has been frequently repeated. As the result of a statistical enquiry
367of my own, relating to 556 fruitful marriages, I ascertained that in
these the first delivery occurred:
Within 10 months after marriage in 156 cases.
Within 11 to 15 months after marriage in 199 cases.
Within 16 to 24 months after marriage in 115 cases.
Within 2 to 3 years after marriage in 60 cases.
More than 3 years after marriage in 26 cases.
Thus we learn that in 35.5% of the cases the first delivery occurred
within 1¼ years after marriage; in 15.6% within 10 months; and in
19.9% within 15 months after marriage; and 11.5% of the cases, the
first delivery was more than 1¼ years and less than 2 years after
marriage; in 6.0% it was between 2 and 3 years after marriage; and
in 2.6%, the first delivery did not occur until more than 3 years
after marriage.
From examination of the birth registers of Edinburgh and Glasgow,
Matthews Duncan determined the mean interval between marriage
and the birth of a living child to be seventeen months. In
the majority of cases, the first delivery does not occur until a complete
year has elapsed since marriage; in fact, in nearly two-thirds
of the instances the first delivery occurs during the second year of
married life.
The interval between two successive births is, according to
Matthews Duncan, on the average 18 to 24 months, according to
Goehlert, 24 to 26 months; the latter, however, points out that in
cases in which the child dies very soon after birth, the birth of the
next child ensues on the average in 16 to 18 months. In this connection,
we must not fail to take into consideration the influence
of lactation, inasmuch as mothers who do not suckle their children
become pregnant considerably earlier, on the average, than those
who undertake this duty. In reigning families, for instance, it is
by no means uncommon for the consort to be delivered twice
within a single year. The degree to which lactation hinders conception
is so widely known, that women often suckle their infant for a
very long period, with the definite aim of preventing the speedy recurrence
of pregnancy. A high official from the Dutch Indies informed
me that for this reason the native women were accustomed
to suckle their infants for several years, and that it was by no
means uncommon to see a small boy running about smoking a cigar,
and then hurrying to his mother in order to be suckled.
The age at which a woman contracts marriage has also to this
extent an influence upon her fertility, inasmuch as it appears that
those who marry very young are far less fertile than those who
368marry between the ages of 20 and 25 years; the latter moreover
have, on the average, a shorter time to wait for their first conception
than women who marry before the age of 20. Women who
marry after the age of 25 have to wait longer after marriage for
their first delivery; in fact the older the woman after 25, the
greater, on the average, the interval between marriage and the
first delivery.
Arranging the data already referred to, regarding 556 fruitful
women, in relation to this point of view, it appears that the first
birth ensued:
|
Within 10 months of marriage. |
10 to 15 months after marriage. |
15 months to 2 years after marriage. |
2 to 3 years after marriage. |
More than 3 years after marriage. |
| In 163 women marrying at ages 15 to 20 years |
36 |
53 |
46 |
18 |
10 |
| In 313 women marrying at ages 20 to 25 years |
98 |
113 |
56 |
32 |
14 |
| In 70 women marrying at ages 25 to 33 years |
18 |
30 |
12 |
9 |
1 |
| In 10 women marrying at ages over 33 years |
4 |
3 |
1 |
1 |
1 |
To give percentages, the first birth occurred,
|
Within 10 months of marriage. |
10 to 15 months after marriage. |
15 months to 2 years after marriage. |
2 to 3 years after marriage. |
More than 3 years after marriage. |
| Women marrying at ages 15 to 20 years, in |
22.0% |
32.5% |
28.2% |
11.0% |
8.1% |
| Women marrying at ages 20 to 25 years, in |
31.3% |
36.1% |
17.8% |
10.2% |
4.4% |
| Women marrying at ages 25 to 33 years, in |
25.7% |
42.8% |
17.1% |
12.8% |
1.4% |
| Women marrying at ages over 33 years, in |
40.0% |
30.0% |
10.0% |
10.0% |
10.0% |
369Thus whereas in women who contracted marriage between the
ages of 15 and 20 years, only 54.5% were confined for the first time
within 15 months after marriage, in women who contracted marriage
between the ages of 20 and 25 years, in 67.4% the first delivery
occurred within 15 months of marriage. And whereas in
those who married at the earlier age, the percentage of first deliveries
occurring between 15 months and 2 years after marriage
was 28.2, in those who married between the ages of 20 and 25,
the percentage of first deliveries after the stated interval was
only 17.8.
The figures compiled by Whitehead and Pfannkuch give similar
results. Of 700 women who married between the ages of 15 to
20 years, there were 306 only who gave birth to a child within the
first two years after marriage; whereas of 1,835 women who married
between the ages of 20 and 25 years, no less than 1,661 gave
birth to a child within two years after marriage—a percentage
of 43.7 in the former case, and 90.6 in the latter case. Pfannkuch,
as the result of a very large collection of figures relating to this
question, found that in women marrying before the age of 20
years, the average number of months before the first delivery was
26; whereas in women marrying after the age of 20 years, the
average number of months before the first delivery was 20.
According to Matthews Duncan
| Of Every 100 Women Who Marry |
There Become Mothers |
| In the 1st year of married life. |
In the 2d year of married life. |
| Between the ages of 15 and 20 years |
13.71 |
43.70 |
| Between the ages of 20 and 25 years |
18.48 |
90.51 |
| Between the ages of 25 and 30 years |
12.41 |
75.80 |
| Between the ages of 30 and 35 years |
11.44 |
62.93 |
| Between the ages of 35 and 40 years |
9.27 |
40.97 |
Sadler examined the relationship between the age at which marriage
was contracted and the number of offspring in the case of
the wives of English peers. He obtained the following results:
| Age at marriage. |
Births per marriage. |
| 12 to 16 years |
4.40 |
| 16 to 20 years |
4.63 |
| 20 to 24 years |
5.21 |
| 24 to 28 years |
5.43 |
370From exact statistical data of births in the Scandinavian countries
of Europe (Denmark, Sweden and Norway), Goehlert compiled
the following table, showing the percentages of fertility at
various ages:
| Ages. |
Married Women. |
Unmarried Women. |
| Denmark. |
Sweden. |
Norway. |
Denmark. |
Sweden. |
Norway. |
| Under 20 years. |
1.0 |
1.0 |
0.7 |
9.1 |
7.0 |
4.9 |
| From 20 to 25 years. |
13.9 |
12.8 |
11.9 |
43.9 |
35.1 |
37.0 |
| From 25 to 30 years. |
26.5 |
24.7 |
24.7 |
28.1 |
27.9 |
32.4 |
| From 30 to 35 years. |
26.7 |
26.1 |
25.3 |
11.4 |
16.8 |
14.9 |
| From 35 to 40 years. |
21.0 |
21.6 |
21.3 |
5.4 |
9.0 |
7.1 |
| From 40 to 45 years. |
9.9 |
12.0 |
13.0 |
2.1 |
4.2 |
3.7 |
| Over 45 years. |
1.1 |
1.8 |
3.1 |
From this table it appears that the fertility of married women
increases steadily up to the age of 35 years, but after this age it
begins to decline. What a marked influence the age at marriage
has upon fertility is shown by the comparison of the figures relating
to married women with those relating to unmarried women;
the fertility of unmarried mothers attains its maximum at the
ages of 20 to 25 years. In the countries under consideration the
average age of women at the time of marriage is 25 to 27 years.
In order to obtain a still clearer picture of the fertility of
women in relation to age, Goehlert has combined the figures relating
to the married and the unmarried, and then calculated the
percentages, with the following results:
| Ages. |
Married and Unmarried Women. |
| Denmark. |
Sweden. |
Norway. |
| Under 20 years. |
1.7 |
1.6 |
1.1 |
| From 20 to 25 years. |
16.6 |
15.1 |
14.1 |
| From 25 to 30 year |
26.6 |
25.0 |
25.3 |
| From 30 to 35 years. |
25.3 |
25.1 |
24.4 |
| From 35 to 40 years. |
19.6 |
20.4 |
20.0 |
| From 40 to 45 years. |
9.2 |
11.2 |
12.2 |
| From 45 to 50 years. |
1.0 |
1.6 |
2.9 |
| Over 50 years. |
371If, finally, we combine into a single table the figures relating to
all three of these countries, we obtain the following results:
| Under 20 years |
1.5% |
| From 20 to 25 years |
15.3% |
| From 25 to 30 years |
25.6% |
| From 30 to 35 years |
24.9% |
| From 35 to 40 years |
20.0% |
| From 40 to 45 years |
10.9% |
| Over 45 years |
1.8% |
From these figures it appears that the maximum fertility of
married women is attained, in Denmark at the age of 31, in Norway
at the age of 31.7, and in Sweden at the age of 32 years. In
the case of unmarried women, the maximum fertility is at the
ages of 24 to 26 years. In the Austrian Empire, the maximum
fertility of women is attained at about the age of 30 years; in
England it is attained between the ages of 20 and 25 years.
Divergent results as regards the fertility of married women at
different ages were obtained by Goehlert from the examination of
5,290 cases from the reigning families of Europe. In the favourable
position as regards means of subsistence occupied by the members
of these families, marriage naturally occurs, in most cases, much
earlier in life, the mean age at marriage being between 19 and 22
years—the youngest mother (in the Capet dynasty) was only
13 years of age—and for this reason the figures relating to the
younger age-classes are larger than in the previous tables. But as
a result of this, the reproductive capacity also undergoes an earlier
extinction, so that of these women, not one gave birth to a child
when she was over 50 years of age. Goehlert gives the following
table, compiled from these 5,290 instances:
| Under 20 years |
8.8% |
| From 20 to 25 years |
25.4% |
| From 25 to 30 years |
29.4% |
| From 30 to 35 years |
21.6% |
| From 35 to 40 years |
11.5% |
| Over 40 years |
3.3% |
In these cases the maximum fertility was obtained at the age
of 27.
The physiological fertility of women is much more clearly manifested
when we compare the fertility of women who have been
married a few years only, with the fertility of women in the
later years of married life. In the earlier period, the effective
fertility more nearly approaches the physiological fertility, because
at this time the various influences by means of which fertility is
372later so greatly diminished have not yet come into operation. In
this connection the following data, published by Körösi, regarding
the percentage fertility of recently married women, and that of
married women in general, will be found of interest:
|
Recently-married women. |
All married women. |
| At ages 20 to 35 years. |
32.9% |
20.6% |
| At ages 35 to 40 years. |
32.7% |
14.7% |
| At ages 40 to 45 years. |
21.4% |
5.9% |
Inasmuch as we learn from this table that in the case of women
aged 40 and upward, the newly married exhibit a fertility of four
times as great as that of married women in general, in whom
pregnancy has already become rare, we can infer the influence
upon fertility of abstinence and of artificial measures for the prevention
of conception.
On the average, the maximum fertility of woman, that is, the
maximum of effective fertility, is attained at the age of 18 to 20
years. Extreme youthfulness, and also the opposite condition,
too advanced an age, when marriage is entered on, impair a woman’s
fertility; whereas the conditions most favourable to fertility
are that, at the time of marriage, the uterus should have attained
its fullest development, and the ovaries also should be completely
mature; this is not usually the case at puberty, but rather at the
age of 20, 21, or 22 years. In Austria-Hungary, of 100 marriages
in which the wife’s age at marriage was less than 18 years, the
average offspring in the course of a single year were 36 to 38
children; in the case of 100 marriages in which the wife’s age at
marriage was 18 to 20 years, the average offspring in a year were
40; this being the maximum fertility, the number of offspring in a
year per hundred marriages (i. e., the percentage fertility), now
undergoes a regular decline as the wife’s age at marriage increases;
at an age of 25, the percentage fertility is 32; at the age of 30
years, the fertility is 24%; at the age of 35, 17%; at the age of
40 years barely 10%; at the age of 45, 7%; at ages 45 to 50,
0.1%. Thus, from the last figure, we see that of a thousand women
marrying at the age of 50 years, one only gives birth to a child.
373Men obtain their maximum fertility (i. e., procreative capacity)
at the age of 25 or 26 years; at this age their fertility amounts to
35% (that is, of 100 marriages at this age, 35 children will on the
average be born within a single year); at the age of 35 years, the
percentage fertility of men falls to 23; at the age of 45 years, it is
9½%; at 55, 2.2%; at 65, ½% (Körösi-Blaschko).
Whereas hitherto we have considered only the monogenous fertility
of married women, we must remember that the figures relating
to their biogenous fertility are also of interest—that is to say,
the changes which a woman’s fertility experiences in married life
in respect of the peculiarities of her husband; and of these peculiarities,
the easiest to make the object of statistical investigation is
the husband’s age. The age of the husband exercises an important
influence upon the fertility of the wife, as is proved by the following
figures published by Körösi:
| Age of the Father. |
Age of the Mother. |
| 25 years. |
30 years. |
35 years. |
| 25 to 30 years |
35.6% |
25.0% |
21.2% |
| 30 to 35 years |
31.2% |
23.6% |
19.9% |
| 35 to 40 years |
27.5% |
21.8% |
19.4% |
| 40 to 45 years |
|
16.7% |
14.0% |
| 45 to 50 years |
|
14.4% |
10.9% |
| 50 to 55 years |
|
|
10.9% |
Also:
| Age of the Mother. |
Age of the Father. |
| 25 years. |
35 years. |
45 years. |
55 years. |
| Under 20 years |
49.1% |
|
|
|
| 20 to 25 years |
43.0% |
31.3% |
16.0% |
|
| 25 to 30 years |
30.8% |
27.3% |
18.5% |
|
| 30 to 35 years |
33.5% |
23.7% |
14.4% |
8.1% |
| 35 to 40 years |
|
18.9% |
11.8% |
6.7% |
| 40 to 45 years |
|
6.6% |
6.1% |
3.0% |
We learn from these figures that the maximum fertility is exhibited
by a woman 18 years of age, when married to a man 25
years of age; less fertile is a woman 25 to 30 years of age married
to a man 28 years of age; still less fertile is a woman 35 years of
age married to a man 29 years of age. Neither the age of the
374mother alone, nor that of the father alone, is determinative of the
fertility of the marriage, for the fertility of young wives married
to elderly husbands is quite different from that of young wives
married to young husbands. Very various age-combinations are
possible, and each exhibits an average fertility peculiar to itself.
We can also regard the question from the standpoint of the
difference between the ages of husband and wife respectively. In
this connection, Körösi is led by his tables to the conclusion that
wives between the ages of 18 and 20 years attain their maximum
fertility when married to men 7 years older than themselves; women
of 25 years when married to men 3 years older than themselves;
women of 29 years when married to men of the same age; women
of 30 years and upward attain their maximum fertility only when
married to men younger than themselves. Men, on the contrary,
always attain their maximum fertility when married to women
younger than themselves. The age of maximum fertility differs
in the two sexes, and those marriages will be most fruitful in which
husband and wife are each of the age most favorable to fertility.
This will be the case when the age of the wife is 18 to 20 years,
and that of the husband 24 to 26 or perhaps 29 years.
In connection with the question of fertility, we have also to take
into consideration the vitality of the children born, that is, what
proportion of those born survive. According to Körösi’s interesting
papers regarding the fertility of the inhabitants of Buda-Pesth,
we learn that for every 100 marriages which have persisted
for thirty years and upward, there were born, on the average, 539
children, of whom during this period 241 died, so that the percentage
of survivals was 55.28. Parents who have lost one only
of several children must, therefore, regard themselves as exceptionally
favoured by fortune.
Social position, occupation, and religion, have, according to the
last-quoted author, a notable influence on fertility. His investigations
showed that the Roman Catholics and the Jews exhibited the
greatest fertility; among the Catholics there were 541 children,
and among the Jews 557 children, per 100 marriages. Amongst
100 Protestant families, on the other hand, only 479 children had
been born. It will be seen that the theory of the comparatively
enormous fertility of the Jewish race is not supported by these
statistics. The Jews do, however, exhibit a greater power of rearing
children, for among them the marriages of more than 30
years’ duration had 61⅔ % of the children still living; among the
Protestants 57¾% survived; and among the Catholics only 52–⅗%.
375It thus appears that the surviving offspring per 100 marriages of 30
years’ duration were, among the Catholics 278, among the Protestants
252, and among the Jews 349.
The question whether, and to what extent, the age of the parents
has an influence on the vitality of the children, is answered by
Körösi’s mortality statistics in the sense that mothers below 20
years of age give birth to a larger proportion of children deficient
in vital power. Where the mothers had married at the age of 16,
the mortality of their offspring was, among Catholics 43%, among
Jews 33%; married at 17, Catholic mortality 44%, Jewish
30%; married at 18, Catholic mortality 42%, Jewish 32%; married
at 19, Catholic mortality 41%, Jewish 29%; married at 20, Catholic
mortality 40%, Jewish 26%. Of the children whose fathers had
married at the age of 24, 32% had died; of those whose fathers had
married at 23, 37% had died; of those whose fathers had married
at 20, 42% had died; and of those whose fathers had married before
20, actually 44% had died. It thus appears that the children
alike of very young mothers and of very young fathers have a
lessened chance of survival.
Inasmuch as the fertility of the wife is a product of two factors,
her own peculiar fertility, and that of the procreating male, the
question of the fertility of women cannot be accurately treated independently
of this second consideration; hereby, however, is introduced
a multiplicity of obscure combinations, by which the value of
all the statistical data of fertility in women is seriously impaired.
These data give as the measure of fertility, the number of children
per marriage actually brought up, embracing fruitful marriages,
sterile marriages, and those not yet fruitful. In Berlin, in
Copenhagen, and in Buda-Pesth, the average thus attained was
slightly less than three births to each family, whilst the number
of children actually living averaged two per family. A more accurate
representation of fertility is obtained by ascertaining the
number of children born, and the number of children living in
relation to the duration of marriages reckoned in years, that is
beginning with marriages of one year’s duration, and proceeding
year by year to the highest recorded duration of marriage. In
this way interesting statistics have been obtained; for example, one
who has completed thirty years of married life may count on the
average that five or six children will have been born to him, but
may also reckon on having buried two or three at least of these.
(Körösi.)
376Fertility is, as many facts indicate, also dependent on nutrition.
A distinct proof, says Spencer, writing on the “Coincidence between
high Nutrition and Genesis,” that abundant nutriment increases
the number of births, and vice versa, is found among the
mammalia; compare, for instance, the litter of the dog with that
of the wolf and the fox. Whilst the dog’s litter numbers 6 to 14,
that of the wolf numbers 5 to 7, that of the fox 4 to 6. The
wild cat gives birth to 4 or 5 kittens once a year, the domesticated
cat to 5 or 6, twice or thrice annually. The most remarkable contrast,
in this respect, exists between the wild and the domesticated
breeds of swine. The wild sow gives birth once a year to a litter
of 4, 8, or 10 pigs (the number increasing in successive litters); the
domesticated sow has often as many as 17 in a single litter, whilst
in two years five litters, each numbering 10 pigs, are commonly
born.
Darwin also draws attention to the fact that animals under
domestication, being fed more abundantly and regularly than their
wild allies, procreate at shorter intervals and are markedly more
fertile than the latter. He states that the wild rabbit has four
litters annually, each numbering 4 to 8 young; whereas the tame
rabbit reproduces its kind six to seven times annually, and gives
birth to litters numbering 4 to 11. Among birds, analogous phenomena
are observed. The wild duck, for instance, lays 5 to 10
eggs in the course of the year, whereas the tame duck lays from
80 to 100; the wild grey goose lays 5 to 8 eggs, the domesticated
goose 13 to 18.
It must be added that this exceptional fertility is manifested in
animals that are quite inactive in comparison with their wild allies;
not only are they richly fed, but they get their food without working
for it. Moreover, it is easy to observe that among the domesticated
mammals the well-fed are more fertile than the ill-fed.
That in the human species also, fertility is influenced to a notable
degree by nutritive conditions, is shown by statistical investigation.
After years distinguished by an exceptionally good harvest the
number of children born is considerably greater than in normal
conditions; whereas after a famine the opposite is observed.
Malthus’s law of population states, inter alia, that the population
increases when the amount of available nutriment increases, that
is, that favourable nutritive conditions cause an increase, that unfavourable
nutritive conditions cause a decrease, of population.
Hardships and exhausting occupations diminish the fertility of
women. The remarkable fertility of the Kaffirs is referred to the
377fact that this people, possessing large herds of cattle, lead a life
comparatively free from care; it is no less true that the Boer
women, who lead a life of well-fed leisure, have very large families;
whereas the Hottentot women, poor, ill-nourished, and hard
working, seldom bear more than three children.
Generally speaking, it may be said that fertility of the soil, in
connection with an easily gained livelihood, favours also human
fertility, notwithstanding the fact that certain statistical data seem
to conflict with this proposition. Sadler, for instance, concludes that
an increase in the price of the necessaries of life does not per se
check fertility, but, indeed, rather increases it; he considers that
the apparent decline in fertility is due to the fact that the number
of marriages diminishes, owing to the rise in prices. We must,
however, point out, that an increase in price of the necessaries of
life is often associated with a rise in wages, and is therefore not
necessarily identified with deficient nutrition; when, however, such
a rise in prices leads to actual want, a limitation of fertility will
certainly result; this has been proved by Legoyt and Villermé with
regard to failure of the crops. Famine and disease lower the
number of births; a less severe deficiency of nutriment often lowers
only the quality of those born. Malthus was of opinion that the
population of a country at any time was related to the quantity of
nutriment produced or imported therein, on the one hand, and,
on the other, to the liberality with which this nutriment was distributed
to the individual. In countries where corn forms the
principal crop, we find a thicker population than in pasture lands;
and where rice is the principal crop, the population is even more
abundant than it is in corn growing countries.
Passing to the consideration of the individual nutritive elements,
we find that these also influence fertility. Above all, it has been
proved that alcohol notably diminishes the fertility of women.
Lippich states that of 100 women in Kärnten and Krain suffering
from chronic alcoholism, 28.3 were barren. In England, where the
abuse of alcoholic beverages is also very frequently observed in
women, the same phenomenon has been noted. Matthews Duncan
held that alcohol exercised a specific deleterious influence on fertility.
Moreover, in addition to the constitutional disturbances produced
by the abuse of alcohol, this beverage also exercises a well-known
pathogenetic influence upon the female reproductive organs;
with especial frequency, chronic oöphoritis may be shown to
depend on this exciting cause.
378A diet consisting mainly of fish is known to increase the sexual
impulse, and is said also to increase fertility. Further, a diet consisting
mainly of potatoes or rice is said to favour reproduction;
compare, for instance, the fertility of the Hindoos, who abstain
entirely from animal food, and of the Chinese, who live chiefly on
rice. Davy maintained that the women of races living chiefly on
fish were handsomer and more fertile than others: and Montesquieu
suggested that there was an association between the abundant
population of sea-ports and also of Japan and China, and the
large quantity of fish consumed in those places. On the other
hand, a diet consisting chiefly of meat is said to have an unfavourable
influence in this direction; in support of this view it is pointed
out that races living by the chase, and living therefore almost entirely
on meat, have very small families. This generalization is
invalidated by the fact that Englishwomen, who eat far more
meat than the women of the Latin races, are nevertheless distinguished
by their great fertility.
In his “History of Civilisation in England” Buckle writes: “The
population of a country, although influenced by many other conditions,
unquestionably rises and falls in proportion as the supply
of nutriment is abundant or the reverse.” Herbert Spencer also
states that “every increment in the supply of nutriment is followed
by an increment in fertility.”
It must not be forgotten that, in addition to the more or less
abundant supply of nutriment, there are always other influences
affecting fertility; the general mode of life, race, climatic conditions,
etc., may, in various ways, co-operate with or countervail the
influence of nutritive conditions. If, with the best possible supply
of nutriment, there is associated a luxurious and enervating mode
of life, the abuse of alcohol, severe intellectual exertion, or sexual
excesses, the general result will be a diminution in fertility. And
it is easy to understand why Cros, although perhaps with little justification,
goes so far as to regard easy circumstances as an active
cause of depopulation. “It is the poor,” he writes, “and the less
wealthy departments of France, in which we find the most children.”
In estimating fertility, however, we must never fail to take
into consideration the more extensive employment of means for the
prevention of pregnancy among the upper classes of society.
To a certain extent we can trace the influence of climate and of
season upon fertility. Heat appears to favour fertility; Haycraft’s
figures for the eight largest towns of Scotland show clearly how
the number of conceptions rises and falls pari passu with the temperature.
379Lower animals also, when brought from a colder to a
warmer neighbourhood, exhibit an earlier and more frequently
recurring “heat.” In Europe, however, the Northern races appear
more fertile than those of the south.
Of the seasons, spring is the one especially favourable to
fertility. Quetelet, who proves by numerous statistical data that
the maximum of conceptions occurs in May, attributes this fact to
a general increase in the vital forces occurring in spring, after the
cold of winter. Villermé, however, goes back to the older explanation,
that the increase in the number of conceptions in May and
June is due to social and economic conditions. The return of
spring, especially the end of spring and the beginning of summer,
a time of year in which the means of subsistence are provided in
exceptional quantity, and of especially good quality, the season also
of festivals and social reunion, when the two sexes are brought
into more intimate contact and when the majority of marriages
occur—these are the conditions associated with the season of
greatest fertility. The figures of Wappaeus also confirm the influence
of spring in favouring fertility. He found, however, that
there were two seasons of maximal fertility. The first at the end
of spring and the beginning of summer; the second in winter,
especially in December. Mid-winter is for most people a period
of domestic amusement and relaxation, one of exceptionally good
nutrition, and of social reunion; the spring increase in fertility is
a part of the awakening and increase of the reproductive forces
of nature at large, which recurs every spring-time.
Every marked and sudden change in the mode of life has an
unfavourable influence on fertility. Darwin reports that mares who
have for some time been stall-fed with dry fodder and are then
put out to grass are at first infertile after the change. Europeans
going to reside in the tropics experience a notable decline in fertility
as a result of the change of climate. According to Virchow,
the fertility of European women who become acclimatized in the
tropics declines very gradually, but in the course of a few generations
is almost completely annulled.
The marriage of near kin is believed also to diminish fertility.
As regards inbreeding in the lower animals, it is well known that
when nearly related animals copulate, the number of the offspring
is below the average. Nathusius paired a sow with its own uncle,
the boar having proved productive in intercourse with other sows;
the litter numbered five to six only. This sow, which belonged to
the great Yorkshire race, was then paired with a small black boar,
380which in intercourse with sows of its own variety had procreated
litters numbering six or seven; as a result of her first pairing with
the black boar, the sow cast a litter numbering twenty-one whilst
the second attempt produced a litter of eighteen. Similar results
were obtained by Crampe, in his experiments in the inbreeding of
rats.
Some authorities declare that the results of inbreeding are similar
in the human species, that the marriages of near kin are less
fruitful than the average. Darwin writes in this connection:
“With regard to human beings, the question whether breeding
in-and-in is also deleterious, will probably never receive a direct
answer, for man reproduces his kind so very slowly, and cannot be
made the object of experiment. The very general disinclination
of nearly all races to the marriage of near kin, which has existed
from the very earliest times, is of weight in relation to this question.
Indeed we appear almost justified in applying to the human
race the experience gained by experiment on the higher mammals.”
Darwin’s assumption regarding the effect upon fertility of the
marriage of near kin in the human species, cannot, however, be
accepted without qualification. In ancient times there was no uniformity
of opinion on this topic. It is well known that among
the Phœnicians, a son might marry his mother, and a father his
daughter; and among the ancient Arabs it was the legal duty of
the son to marry his widowed mother. Moses, on the contrary,
forbade marriages between parents and children, between brothers
and sisters, also marriage with a father’s sister, with a wife’s mother,
and with an uncle’s widow.
Darwin considered that the marriage of first cousins was not unfavourable
to fertility. Of 97 such marriages, 14 were sterile,
whilst of 217 marriages of those not akin, 35 were sterile; the percentage
in both cases being almost identical. Mantegazza, who regards
kinship in marriage as unfavourable to fertility, found nevertheless
that among 512 marriages of near kin, only 8 to 9% were
sterile. It is widely believed that the dying out of many aristocratic
families is dependent on the inbreeding so common in this
class—but it must be admitted that scientific evidence in support
of this belief is lacking. Incest in the human species may certainly
result in fertilization. Among the Jews, marriages of near kin are
very common, and often prove extremely fruitful.
Göhlert made a statistical investigation of the fertility of the
reigning families of Europe, in order to throw light on this question.
In the Capet dynasty, 118 marriages of near kin took place, and of
381these 41 were sterile; in the Wettin dynasty (Saxony), there were
28 such marriages, of which 7 were sterile, and 1 produced one
child only; in the Wittelsbach dynasty (Bavaria), 29 such marriages,
of which 9 were sterile, and 3 produced only one child each. Thus
of 175 marriages of near kin, 57, or 32.6% remained sterile. Further,
in the Habsburg-Lothringen dynasty, of 110 marriages, 25
were marriages of near kin, and of these 33% remained sterile.
It has been assumed since the days of antiquity that temperament
and constitution exercise some influence on fertility. Hippocrates,
Soranus, and Diokles, are among the ancient authors who refer to
this matter. Soranus says very justly: “Since most marriages are
contracted, not from love, but for the procreation of children, it
is irrational, when choosing a wife, to have regard, not to her probable
fruitfulness, but instead of this to the social position and the
wealth of her parents.”
It would appear that a certain dissimilarity in physical constitution
and temperament between husband and wife is favourable
to the fertility of the marriage. For instance, a vivacious, dark
husband, and a lethargic, fair wife, are better suited to one another
than a husband and wife both extremely active, or both of extremely
phlegmatic temperament.
Toussaint Loua published the following figures regarding the
fertility of the women of the various countries of Europe:
| Country. |
Number of births per hundred inhabitants. |
Fertility of Women Between the Ages of 15 and 45 Years. |
| Married. |
Unmarried. |
Average. |
| Hungary |
4.94 |
|
|
17.8 |
| Russia |
4.12 |
|
|
20.5 |
| Austria |
3.93 |
|
|
16.4 |
| Germany |
3.77 |
34.8 |
2.9 |
17.7 |
| Italy |
3.67 |
28.8 |
2.4 |
16.1 |
| Holland |
3.67 |
35.3 |
1.0 |
16.0 |
| Finland |
3.63 |
|
|
15.8 |
| England |
3.58 |
29.7 |
1.6 |
15.5 |
| Scotland |
3.53 |
32.8 |
2.5 |
15.8 |
| Belgium |
3.25 |
33.7 |
1.8 |
14.8 |
| Denmark |
3.12 |
28.5 |
2.8 |
14.4 |
| Roumania |
3.12 |
|
|
13.5 |
| Norway |
3.10 |
29.3 |
2.2 |
14.0 |
| Sweden |
3.05 |
29.1 |
2.5 |
13.7 |
| Switzerland |
3.04 |
29.7 |
1.1 |
13.1 |
| Greece |
2.96 |
|
|
13.2 |
| Ireland |
2.69 |
29.8 |
0.5 |
12.3 |
| France |
2.63 |
20.3 |
1.8 |
11.6 |
382In towns, conjugal fertility is less, extra-conjugal fertility greater,
than in the country. An increase in factory labour gives rise to an
increase in the population, but to a decline in the vitality of the
offspring; that is to say, it causes a quantitative increase, and a
qualitative decrease, in fertility. An increase in agricultural labour
has precisely the opposite effect. The influence of war upon fertility
is unfavourable both quantitatively, and qualitatively. According
to Tschouriloff, the introduction of universal military service,
by withdrawing for a time all the most vigorous men from domestic
life, tends to diminish fertility. Extensive emigration from a
country in which the soil is fertile, and where the vital conditions
are generally favourable, is stated by Bertillon to cause an increased
fertility in the mother country; he further states that an increase
in the number of the proprietors of the soil is followed by diminished
fertility, and vice versa.
Prostitutes show as a rule a very low fertility. According to
the data of Tarnowskaja, the fertility of prostitutes in Russia is
34%, whilst married women of similar ages in Russia exhibit a fertility
of 51.8%. Gurrieri found 60% of prostitutes childless.
The fertility of female criminals was found by Lombroso to be
undiminished. On the average, poisoners had given birth to 4.5
children, other murderesses to 3.2 children, child-murderesses to 2
children; thus the prisoners whose crime is commonly dependent
on an abnormal eroticism had a fertility above the average.
The diminished fertility of prostitutes depends in part upon frequent
venereal infection, in part upon the unfavourable influence
of the mercury and iodide of potassium administered for the cure
of such infection, also upon the frequency with which they consume
excessive quantities of alcohol, upon the excessive frequency
of coitus, which exercises a traumatic influence, upon the irregular
mode of life, and upon their disinclination to be burdened with
children.
Conjugal fertility, that is to say, the ratio between legitimate
births and the number of married women between the ages of
15 and 50 years, has declined in Germany during the last decades.
It was:
| During the years 1872 to 1875 |
29.7% |
| During the years 1879 to 1882 |
27.4% |
| During the years 1889 to 1892 |
26.5% |
383This decline is small, but it is much more manifest in urban
than in rural districts. This fact is shown by the following figures,
relating to fertility in Prussia:
|
1872 to 1879. |
1894 to 1897. |
| In all towns |
26.9 |
24.0 |
| In Berlin |
23.8 |
16.9 |
| In other large towns |
26.7 |
23.5 |
| In rural districts |
28.8 |
29.0 |
This difference depends principally on the fact that in the large
towns of Germany (and still more in those of France) the use of
means for the prevention of pregnancy is continually increasing,
whereas the population of the rural districts is as yet less familiar
with the use of these measures.
According to Hellstenius, conjugal fertility, that is, the number
of children per married couple, is as follows:
| In the |
Netherlands |
4.88 |
| |
Norway |
4.70 |
| |
Prussia |
4.60 |
| |
Bavaria |
4.55 |
| |
Sweden |
4.52 |
| |
Saxony |
4.35 |
| |
England |
4.33 |
| |
Belgium |
4.23 |
| |
Denmark |
4.18 |
| |
France |
3.46 |
Talquist, who has published a statistical investigation concerning
the modern tendency to diminished fertility, arrives at lower figures
than Hellstenius. According to him, conjugal fertility is:
| In |
Prussia |
4.11 |
| |
England |
4.10 |
| |
Belgium |
4.12 |
| |
France |
2.09 |
| In |
various States of the American Union |
2.5 to 3.0 |
From the Almanach de Gotha Vacher obtained figures showing
that each family of the higher aristocracy has on the average the
following number of children.
| In |
France |
2.0 |
| |
Italy |
3.0 |
| |
Germany |
4.8 |
| |
England |
4.9 |
| |
Russia |
5.1 |
According to the figures we have published, the fertility of women
suffices for the production during the sexual life of a small number
384only of children, averaging, in fact, 4 to 5 children per marriage.
Many mothers, however, give birth to a very large number of children.
Among 73,000 families inhabiting Buda-Pesth, Körösi found
300 mothers who had had 15 children or more; 7 mothers who had
each had 21 children; and 3 mothers who had given birth respectively
to 22, 23 and 24 children.
A newspaper report states that the wife of a citizen of Buda-Pesth,
during the 43 years of her married life, gave birth to 32
children. In the year 1902, a Bohemian woman gave birth to her
twenty-fourth child. Stieda reports the cases of two mothers, one
of whom had 21, and the other 23 children. The wife of the German
Emperor, Albrecht I, and the wife of Prince Jost of Lippe-Biesterfeld,
each bore 21 children.
The so-called two-children-system obtains most commonly in
France.
It is true that even in France there are on an average nearly
three children born per marriage; but if we take into account surviving
children only we find an average per family of 2.1 children
only. Similar conditions obtain in New England, and in Transylvania;
and the same practice is spreading throughout the United
States. Another way in which the attempt is made to keep down
the population is that customary in Alsace, where, if there are
several children in a family one only marries, in order to avoid a
division of the family property. It cannot be denied that in France,
doubtless in consequence of the two-children system, a somewhat
widely diffused prosperity exists, a prosperity which is lacking in
the rare districts in France, such as Brittany, in which limitation of
the family is not practised. What a disastrous influence the general
use of measures for the prevention of pregnancy exercises on the
military power and political status of a nation has, however, in
recent years been made especially manifest in the case of France.
In that country, of ten million families, two million are absolutely
childless, and two million have only one child each, so that two-fifths
of the French families are as good as inactive in maintaining
the population of the country. The injury thus done to France is
shown still more clearly by a tabular comparison of the excess of
births over deaths in the German and French nations, respectively,
during the two decades 1874 to 1894 (from G. von Mayr’s Population
Statistics).
| 385 |
| Year. |
Germany. |
France. |
| 1874 |
+13.4 |
+4.8 |
| 1875 |
13.0 |
2.9 |
| 1876 |
14.6 |
3.6 |
| 1877 |
13.6 |
3.9 |
| 1878 |
12.7 |
2.6 |
| 1879 |
13.3 |
2.5 |
| 1880 |
11.6 |
1.7 |
| 1881 |
11.5 |
2.9 |
| 1882 |
11.5 |
2.6 |
| 1883 |
11.7 |
2.6 |
| 1884 |
11.2 |
2.3 |
| 1885 |
11.3 |
1.4 |
| 1886 |
10.8 |
1.5 |
| 1887 |
12.7 |
1.3 |
| 1888 |
12.9 |
2.5 |
| 1889 |
12.7 |
1.2 |
| 1890 |
11.3 |
–0.3 |
| 1891 |
13.6 |
–0.5 |
| 1892 |
11.7 |
+0.1 |
| 1893 |
12.2 |
–1.2 |
| 1894 |
13.6 |
–0.4 |
To what an extent in all times, and among all peoples, the fertility
of women was esteemed, is shown by religious writings and
traditional customs which aimed at enabling a wife who had had
no children by her own husband, to seek other conjugal embraces.
Among the Jews, it was the duty of a man to marry his widowed
and childless sister-in-law; if he were unwilling or unable to perform
this duty he was compelled to take a part in a ritual termed
“chaliza,” in which his foot was bared and the bereaved woman
spat upon him, because he was unwilling to maintain his brother’s
house. In the law book of the Hindoos of Manus, we read, “If
husband and wife have no children, it is proper for them to obtain
the desired offspring by a union between the wife and the husband’s
brother, or some other relative;” the child obtained in this way
was legally regarded as the child of the husband. Confucius wrote:
“If your wife is barren, take a second wife; she must be subordinate
to the first wife, for her only duty is the bearing of children.”
An analogy to this ordinance is to be found in the Bible; Abraham’s
barren wife Sarai says to Abraham: “Behold now, the Lord
has restrained me from bearing: I pray thee, go in unto my maid;
it may be that I may obtain children by her. And Abraham hearkened
unto the voice of Sarai.” In the same way the barren Rachel
speaks to her husband Jacob, “Behold my maid Billah, go in unto
her; and she shall bear upon my knees, that I may also have children
by her.”
Luther, in his treatise on marital love published in the year 1522,
bases, doubtless on the above biblical precedents, the following statement
386regarding fertility: “If a sexually potent woman is married
to an impotent man, if she is unable to take any other man openly,
yet is unwilling to do anything dishonourable, she should say to her
husband, “Dear husband, you cannot fulfil your duty to me, and
you have deceived my young body, you have endangered my honour
and my happiness, and in the eye of God our marriage is null, forgive
me therefore if I form a secret union with your brother or
with your nearest friend; the fruit of this union will be yours in
name, thus your possessions will not fall to strangers, and you will
willingly allow me to deceive you, because involuntarily you have
deceived me.””
In ethnography, the term endogamy is used to denote a law or
custom by which marriage is allowed only within the limits of a
specified race, tribe, or caste; thus, in the Old Testament, Jews are
forbidden to marry women of other races. The ethnographical
term exogamy indicates the prohibition of marriage between persons
who are more closely allied, as, for instance, the Mosaic prohibition
of marriage within certain degrees of blood-relationship.
Such exogamic prohibitions persist even in the legislation of the
present day. In many ecclesiastical and national laws we find the
marriage of first cousins and of uncle or aunt with niece or nephew
forbidden; and even a prohibition of the marriage of a man with
his deceased wife’s sister.
Hegar considers the danger of inbreeding to be very great in
the human species; for whereas in the lower animals breeders
employ a methodical and carefully considered selection of the best
specimens, nothing of this kind occurs among human beings; and
the health of modern civilized man is such that there are few
families without a skeleton in the closet. “Not only in families,
but also in villages, in small and large towns, even in classes, and
in entire nations, certain peculiar qualities, morbid tendencies, and
predispositions, are handed down from generation to generation.
We have, for instance, the tendency of the Jews to nervous disorders
and diabetes, that of the English to gout, that of the Germans
to myopia.” Strahan has therefore employed the term “social consanguinity,”
to indicate that by means of common customs, environment,
occupation, and mode of nutrition, a similarity in type is produced,
leading to a similar predisposition to disorders and diseases
transmissible from father to son.
The dangers of inbreeding are believed by Hegar to be, under
present-day conditions, so considerable that he would allow the marriage
387of near kin in exceptional cases only, and where the circumstances
are peculiarly favourable—for instance, where both parties
to the projected marriage are in excellent health, and where there
is no great similarity between them in feature or mental type.
Certain anomalies transmitted from remote ancestors, dependent on
deeply-marked peculiarities of the germ cells, may be so developed
by inbreeding as to become absolutely fixed characteristics. If the
morbid manifestations can be traced back for several generations,
if the bodily defects and disturbances of development (the so-called
stigmata of degeneration), are well marked and numerous, if the
functional disorders of the nervous system and of the sense organs
are pronounced, leading to idiocy, insanity, epilepsy, congenital deafmutism,
blindness, instinctive criminality,—there is in such cases
little or no hope of the regeneration of the family. It dies out,
because the members are sterile; because they are confined in
prisons or asylums; or because the children, if any are born, are
deficient in vitality, and fail to reach maturity.
According to the brief summary of the subject given by Hegar,
the peculiarities of the offspring at the time of birth depend upon:
Factors which give rise to peculiarities of the germ-cells:
I. Germinal rudiments derived from the ancestors;
II. Influences acting on the germ-cells within the parent
organism;
a. Owing to peculiarities of the fluids and tissues of the
parental body;
b. Owing to substances which penetrate the parental
body and reach the germ.
Germinal rudiments altered by the conjugation of the male and
female reproductive cells:
I. On the mother’s side;
a. Owing to peculiarities of the fluids and tissues of the
maternal body;
b. Owing to substances which penetrate the maternal
organism and reach the fertilized ovum.
II. On the father’s side, owing to substances which adhere
to the paternal reproductive cells, or are enclosed
within these.
The number of consanguineous marriages at the present day is
not less than 5½ to 6½ per 1,000; the fertility of these marriages
appears to be identical with the fertility of ordinary marriages.
Mayet has made a statistical investigation to determine the influence
388of consanguineous marriages in the pathogenesis of mental disease.
He finds that the number of those congenitally affected with mental
disorder is twice as great in the offspring of consanguineous marriages
as in the offspring of crossed marriages; in the case of
simple mental disorder, of paralytic dementia, and of epileptic
dementia, the ratio is actually greater than two to one (the actual
figures are 218, 257, 208 : 100). Thus we see that when there exists
any cause of inheritable mental disorder, blood-relationship of
the parents more than doubles the danger to the children. In the
case of imbecility and idiocy the danger is less in this respect (the
ratio is 150 : 100); the factor of inheritance plays a less prominent
part than in the case of other psychoses.
It was remarkable that among the offspring of marriages of
nephew and aunt, cases of mental disorder were almost entirely
lacking. Among the offspring of marriages of uncle and niece, the
inheritance of mental disorder was more prominent than among
the children of first cousins. It is interesting to determine the influence
of blood-relationship in cases in which the existence of inheritable
predisposition could not be proved. In these cases, as
regards simple insanity, paralytic dementia, and epileptic dementia,
the number of cases among the offspring of consanguineous marriages
was only one-half as compared with the offspring of crossed
marriages; whereas in the case of imbecility and idiocy this ratio
was reversed. In idiocy, where inheritance generally speaking plays
a small part, the origination of the disease would often appear to
depend directly on the blood-relationship of the parents; whilst as
regards other forms of mental disorder, if there is no inheritable
predisposition, blood relationship in the parents appears to be a
positive advantage; where, however, a family predisposition to insanity
exists the likelihood of actual insanity appearing in the offspring
is notably enhanced by a consanguineous marriage.
The Restriction of Fertility and the Use of Means for the Prevention of Pregnancy.
As we have already pointed out, a restriction of the fertility of
women occurs in the majority of marriages, to this extent, that the
potential reproductive powers of the wife are not fully utilized. In
recent times, however, the restriction of fertility, by the deliberate
use of measures for the prevention of pregnancy, has become so
widely diffused, that it appears unwise from the scientific standpoint
389simply to ignore the question, and it has become indispensable
to study how the practice developed, and to consider what are its
actual results. From our own point of view, it is the more necessary
to do this, for the reason that the use of preventive measures
has come to play an important part in the sexual life of woman,
and therefore deserves the fullest attention, not merely from the
standpoint of the sociologist, but in addition from the purely medical
point of view.
In many divisions of the population, and even in entire nationalities,
the prevention of pregnancy, not merely in illicit intercourse,
but also in married life, has become so general a practice that the
fertility of the nation as a whole has been profoundly modified.
Thus, in France at the present day, the average number of children
per marriage is less than two; and the two-children-system is almost
universally practised in Transylvania and Norway, whilst it is very
rapidly spreading in North America. In the principal towns of the
whole of Europe, this system is largely on the increase among the
upper classes of society. The marriages of the poor, partly owing
to ignorance, and partly to indolence, are as yet comparatively little
affected by this depopulative principle.
In the days of antiquity, many lawgivers endeavoured to set
bounds to excessive fertility, and artificial abortion was methodically
practised by those who wished to avoid an inconveniently large
family. Even among savage peoples, we find that certain preventive
measures are occasionally employed in sexual intercourse. Among
civilized peoples, however, until the beginning of the nineteenth century,
religious and moral ideas derived from the Bible continued to
dominate the sexual life. It is well known that Old Testament
law and Christian morality alike forbid any artificial restriction
of human increase. “Increase and multiply” was the command
given in Genesis to the first parents of the race; and the
psalmist exclaims, “Happy is the man that hath his quiver full” of
children.
A remarkable revolution in thought was initiated toward the beginning
of the nineteenth century by the great philanthropist and
powerful thinker, Thomas Robert Malthus, founder of the doctrine
of the propriety of checking the increase of population, author of
the work “An Essay on the Principle of Population,” London,
1798, whose Law of Population soon attracted world-wide attention.
Modern civilization having greatly increased the cost of
bringing up a family, while simultaneously there has been a general
390rise in the price of the necessaries of life, there has resulted an
extraordinary diffusion of Malthusianism; in comparison with the
causes just alluded to for the use of preventive measures, diseases
which render renewal of pregnancy dangerous to the mother’s life
have comparatively little to do with the causation of voluntary
sterility.
In his “Essay on the Principle of Population,” Malthus indicates,
as the cause which has hitherto hindered mankind in the
pursuit of happiness, the unceasing tendency of all organic life to
increase in excess of the means of subsistence. In the case of
plants and of unreasoning animals, the natural process is a very
simple one. Both animals and plants are impelled by a powerful
instinct to reproduce their kind, and the operation of this instinct
is quite undisturbed by any anxiety regarding the livelihood of their
offspring. The reproductive function is thus exercised at every
available opportunity, and the superfluous individuals of the next
generation are destroyed by lack of space and nutriment. In the
human species the restriction of population is effected by a more
complex mode of operation. Man is impelled to reproduce his kind
by an instinct not less powerful than that of other animals; but the
gratification of this instinct is checked by reason, which makes him
ask himself whether he is not about to bring into the world beings
for whom he will be unable to provide the means of subsistence.
If he is influenced by this consideration, the resulting restriction of
population may often entail serious consequences; if, on the other
hand, he gratifies his instinct, regardless of the appeal of reason,
the human species will inevitably tend to increase more rapidly than
the means of subsistence.
Malthus declared that population, when its increase was unrestricted,
doubled itself every twenty-five years, and therefore increased
in a geometrical progression; he considered that in the most
favourable circumstances the means of subsistence could not possibly
increase more rapidly than in an arithmetical progression.
The contrast between these two modes of increase will be more
striking if we write out the actual figures. According to the theory
of Malthus, the increase of human population would be represented
by the figures 1, 2, 4, 8, 16, 32, 64, 128, 256, whereas the simultaneous
increase in the means of subsistence would be represented
by the figures 1, 2, 3, 4, 5, 6, 7, 8, 9. Such an increase in population
is, however, always prevented by certain checks, classed by
Malthus as of two kinds, preventive checks and positive checks.
391A preventive check, in so far as it is voluntary, is peculiar to
the human species, and originates in the intellectual faculty which
enables man to foresee the consequences of his actions. A man
who looks around him, and sees the poverty into which those
with large families so often fall, who reckons up his present property
or earnings, which barely suffice to provide for his own personal
necessities, cannot fail, when he considers how hardly they
would suffice for seven or eight additional persons, to doubt whether
it would be possible for him to provide for the offspring he might
bring into the world. Such considerations as these are likely to
lead a large number of persons of all civilized nations to resist
their natural instincts, and to refrain from early marriage. If abstinence
entailed no serious consequences, it would be the least of
all evils resulting from the principle of population.
The positive checks to increase of population are manifold, and
embrace all the causes which are competent to lessen the natural
duration of human life. Among these we may enumerate: all unhealthy
occupations, severe toil, climatic conditions, poverty, errors
in the rearing of children, town life, excesses of all kinds, the whole
army of illnesses and epidemics, war, pestilence, and famine. In
all countries, preventive and positive checks are more or less powerfully
operative, and yet there are few in which the population is not
continually tending to increase beyond the means of subsistence. As
a further consequence of this tendency of population to increase, we
observe the wider diffusion of poverty among the lower classes, so
that any permanent improvement in their condition is rendered impossible.
After Malthus had carefully stated his thesis, he gave a summary
record of the conditions of population in nearly all nations of the
past and of his own time, in order to show how in all alike the
three principal means of limiting population, moral restraint, disease,
and poverty, had been in continuous operation.
He showed, for instance, how the population of the South Sea
Islands had been limited by certain conditions, cannibalism, castration
of the males, infibulation of the females, late marriages, the
sanctification of virginity, contempt for marriage, etc.
In ancient Greece, Solon’s laws permitted infanticide. Plato, in
“The Republic” asserts that it is the duty of the Government to
regulate the number of the citizens, and to prevent an immoderate
increase; men and women should be allowed to procreate only during
their period of maximum strength, all weakly children should be
392killed. Aristotle advised that men should not be allowed to marry
before the age of 37, and women before the age of 18; the women
should give birth to a limited number of children only; if, after this,
they again became pregnant, abortion should be induced. He maintained
that if all were at liberty, as was the case in most countries,
to bring into the world as many children as they pleased, poverty,
the mother of crime and insurrection, must inevitably ensue.
Among the Romans war was as a positive check unceasingly
operative: in this time of the Empire, preventive methods came into
general use, in the form of various kinds of sexual perversity.
Juvenal complains of the skilled methods employed in the induction
of abortion; during the later period of the Roman Empire, sexual
morality became so degenerate that marriage was hated and despised.
Passing to the consideration of the checks on population among
the nations of modern Europe, Malthus examined the registers of
marriages and deaths, and came to the conclusion that in few
countries is the mass of people sufficiently capable of self-restraint
to postpone marriage until they are reasonably assured of being
able to provide for all the children they are likely to have; still, he
ascertained that at the present day positive checks on population
were less active, and preventive checks more active, than in earlier
times and among savage races.
Malthus did not base upon his conclusions the advice that in
sexual intercourse means of preventing pregnancy should be employed,
as the modern “Malthusians” advise; in his eyes, moral
restraint, that is to say, sexual abstinence, was the only remedy for
the prevention of poverty and the other evil consequences of the
principle of population. Moral restraint was in his opinion the
only virtuous method of avoiding the evils of excessive fertility. It
was a man’s duty not to marry until he had a definite prospect of being
able to maintain his children; the interval between puberty and
marriage must be passed in strict chastity. Man’s duty is not the
mere reproduction of his species, but the reproduction of virtue and
happiness, and if he is not able to do the latter, he has no right
whatever to do the former. Malthus lays great stress on educating
the people in this matter; “in addition to the ordinary subjects of
instruction, it is necessary to explain the principle of population,
and the manner in which it gives rise to poverty.” In the nature
of the case, no lasting and general improvement in the condition of
the poor is possible without an increase in the preventive restriction
of population.
393The Malthusian doctrine of the law of population gave rise to
an enormous sensation, and some of his disciples soon proceeded to
translate his conclusions into practice; such authorities as James
Mill and Francis Place recommended measures by means of which,
“without any injury to health, or to the feminine sense of delicacy,
conception can be prevented:” the avowed aim of these
measures was to prevent the increase of population beyond the
means of subsistence. Physicians and physiologists joined the
ranks of these innovators; among others Raciborski, Robert Dale
Owen in his “Moral Physiology,” Richard Carlile in his “Book
of Woman,” the first work to give an exact description of the
means to employ for the prevention of conception, Knowlton in his
“Fruits of Philosophy.” In the year 1827 in the Northern counties
of England leaflets were for the first time distributed among the
working classes to instruct them in the use of preventive measures.
Bradlaugh founded the Malthusian Society, which aimed at the
dissemination of instruction in the use of preventive methods. There
is now in England a “Malthusian League,” numbering leading physicians
among its members; this supplies to all classes the means by
which the family can be artificially limited. A new edition of the
above-mentioned book, “The Fruits of Philosophy,” was circulated
in London in an edition of several hundred thousand copies, and
prominent persons spoke at congresses on the subject of Neo-Malthusianism.
In Germany, also, a “Union of Social Harmony”
was founded, for the free distribution of a hand-book on the use
of measures for the prevention of conception, and for an investigation
regarding the results of these.
We do not propose here to subject the teaching of Malthus to a
critical examination; he has found formidable opponents, who have
endeavoured to prove that his fundamental assumption is false;
they maintain that work or the power of work increases in direct
ratio with the population; and they also assert that population
tends to increase, not, as Malthus maintained, in a geometrical, but
simply in an arithmetical progression. We shall merely quote
Liebig’s reply to the law of Malthus, “when human labour and
manure are provided in sufficient quantity, the soil is inexhaustible,
and will continue to yield unceasingly, the most abundant harvests;”
and Rodbertus’ remark that “agricultural chemistry
will ultimately be competent to create nutritive materials; this
will some day be just as much within the power of society, as it
is at present to provide any requisite quantity of textiles, given the
394necessary amount of raw material.” The celebrated socialist Bebel,
is a strong opponent of Malthus. He writes: “The earth is doubtless
thickly populated, but none the less only a small fraction of its
surface is occupied and utilized. Not merely could Great Britain
produce, as has been proved, a far larger supply of nutritive materials
than at present, but the same is true of France, Germany and
Austria, and in a still higher degree of the other countries of Europe.
European Russia, were it as thickly populated as Germany,
could support, instead of ninety millions, as at present, a population
of four hundred and seventy-five millions. For the purposes of the
higher civilization, toward which we are striving, we have to-day in
Europe, and shall have for a long time to come, not an excess of
population, but an insufficiency, and every day brings new discoveries
and inventions whereby the means of subsistence are potentially
increased. In other parts of the world, the insufficiency of
population and the superfluity of ground are even more noticeable.
Carey is of opinion that the single valley of the Orinoco, fifteen
hundred miles in length, would suffice to provide nutritive material
in sufficient quantities to feed the whole existing population of the
world. Central and South America, and more especially Brazil,
have a soil of extraordinary fertility, but are as yet practically unutilized
by the world. To increase, not to diminish, the numbers of
the human race, that is the appeal made by civilization to mankind!”
A similar position on this question was recently taken by
Roosevelt, the President of the United States, himself the father of
six children, in a letter to two American women, Mrs. J. and
M. Van Vorst, authors of the book “Woman Who Toils
(Factory Life in America).” In this book, the writers prove that
in the United States the average size of the family is now less
than in any other country of the world, France alone excepted.
President Roosevelt, in his letter, declares himself an ardent supporter
of the biblical injunction, “increase and multiply!” He
writes: “Whoever evades his responsibilities, through desire for
independence, convenience, and luxury, commits a crime against
the race to which he belongs, and should be an object of contempt
and horror to a healthy nation. When men avoid becoming fathers
of families, and when women cease to regard motherhood as the
most important career open to them, the nation to which these men
and women belong has cause for uneasiness about its future.”
President Roosevelt continues: “To the American woman marriage
is no longer a life-duty, a profession, as it is to her sisters
395who are members of the older civilizations. A woman who manages
an extensive business, who supervises her own landed property,
or who plays her own part in the world of finance,—for such as
these, the ‘lottery of marriage’ is naturally something they dread
rather than desire.” President Elliott, of Harvard College, has expressed
similar views in a speech on this subject. He deplores the
late marriages and small families of the cultured Americans. According
to the last census, an American family has on the average
less than three children; twenty years ago the average number was
from four to five children.
I pass now to consider the medical point of view of this question
of the prevention of pregnancy. It is my opinion that the physician
as such should intervene in the matter, not in any case for the relief
of the dominant economic parental dread of insufficient means
for the upbringing of children, but only on account of the purely
medical consideration of the physical dangers of motherhood. That
is to say, the physician should lend his skilled assistance toward
the attainment of facultative sterility, only when his own special
scientific knowledge leads him to consider this urgently necessary;
it is not his province to assist in preventing the birth of an immoderate
number of offspring; his intervention is justified only
when deliberate reflection has convinced him that his patient’s health
or life would be endangered by pregnancy or childbirth. A woman’s
life and well-being must appear to him of greater importance than
the existence or non-existence of a possible infant. That this view
is morally sound, is shown by the fact that public opinion justifies
the accoucheur in the destruction of an already living child, when
the mother’s life is endangered. In this connection we may recall
the words of the great Napoleon; the physician Dubois, attending
Marie Louise in a difficult confinement, asked Napoleon whether,
if matters came to an extremity, he should save the mother or the
child; Napoleon, notwithstanding his strong desire for the birth of
an heir to his dynasty, replied, “The mother, it is her right.”
In isolated cases, which deserve always very serious consideration,
some pathological condition in the wife may justify the prevention
of pregnancy. In certain very serious general disorders, in diseases
of the heart or of the lungs, in pelvic deformity, and in pathological
changes of the female reproductive organs, it may be right to employ
means for the prevention of pregnancy—not merely sexual abstinence,
but actual measures to prevent fertilization.
The misuse of medical knowledge for the recommendation or employment
of preventive measures, on the ground of humanitarian
396sentiment or social and economic considerations, must, however, be
strongly resisted. Even leading gynecologists have erred in this
way. Saenger writes, “Scientifically-trained accoucheurs will do
much more to promote the health and well-being of women, and to
protect them from sexual and other diseases, than the humanitarian
efforts of the Neo-Malthusians, who transfer a purely scientific
question, such as the disproportion between the number of births
and the supply of nutritive material, to the sphere of medicine, regarding
themselves as justified in preventing conception whenever
they please, independently of considerations relating to the health
of the mother * * * * * * * *
A woman exhausted by frequent child-bearing, anæmic and suffering,
is certainly a figure to arouse everyone’s sympathy; in so far as
she is ill in consequence of injury received in childbirth, it is our
duty to prevent further injury, and to relieve to the best of our
ability that which has already occurred; in so far, however, as she
is not suffering from any affection of the reproductive organs, but
is ill owing to the lack of sufficient food, or from overwork,
it is the duty of society to render assistance. Here we have to do
with the social problem; the solution of which will be brought no
nearer by the use of the occlusive pessary.” Fehling also maintained
that a text-book of gynecology is not the proper place in which to
pass judgment on so important a socio-political question. The business
of the gynecologist in this matter is merely to say a word of
caution against the use of various measures which are so often
recommended as harmless, but are in fact dangerous to the woman
who uses them.
Kleinwächter, who declares that he is far from recommending the
use of preventive measures when a healthy woman wishes to save
herself the trouble of child-bearing, gives as legitimate indications
for their use: 1, the various forms of severe pelvic deformity;
2, certain tumours in the pelvic cavity; 3, after the removal of
malignant tumours of the reproductive organs, certain general disorders,
recently arrested pulmonary tuberculosis, organic heart
disease, etc. Regarding these cases, Kleinwächter writes: “The
wife’s life would be endangered by pregnancy, which must therefore
be prevented without forbidding coitus, and avoiding the practice
of coitus interruptus, which endangers her health, or of any
mode of intercourse repugnant to the feelings of wife or husband.”
The most trustworthy, but unquestionably at the same time the
least practicable method, for the prevention of pregnancy, is that of
397Malthus—permanent sexual continence. This recommendation, to
which Tolstoi in “The Kreuzer Sonata” gives his adhesion, has
recently found an advocate in a modified sense in a distinguished
gynecologist, Hegar, who considers that the great fertility of the
modern civilized countries of Europe entails many disadvantages—inferior
physical development, increased general mortality, emigration,
an unfavourable distribution of population in relation to
dwelling and occupation, occasional famine—and who sees the
only effective remedy in a “regulation of reproduction,” whereby
the tendency to marriage and the number of births are to be diminished.
The question “when is the number of children in a
family too large?” is answered by Hegar as follows “A maximal
limit is easy to establish. The most suitable age for child-bearing
is from twenty to forty. At an earlier and a later age than this,
both the mother and the offspring are liable to suffer. Between
two successive births there should be an interval of about two and a
half years; this would leave time for the birth of eight children.
If we assume that pregnancy lasts nine months, that lactation is
continued from nine to twelve months after delivery, (and if the
mother does not herself nurse the child, artificial feeding or careful
supervision of the wet-nurse will occupy her for a like period), to
devote an additional period of six months to nine months to the
complete restoration of the mother’s health cannot be regarded as
excessive. For this maximum family we assume a perfect state of
health on the part of the mother, a pure atmosphere, and a sufficient
supply of all the necessaries of life. Illnesses, weakness, or infirmity
of the mother, often indicate that the number of children should be
further limited. It is easier to provide a suitable dwelling and a
pure atmosphere for a small family than for a large one. The same
thing is true as regards the means of subsistence.
“If the reproductive function is to be intelligently controlled,”
continues Hegar, “above all it is necessary to devote attention to the
age and health of the parents; but occupation, dwelling, and general
environment, must also not be overlooked. Among the cultured
classes of our Fatherland, people are gradually learning to form
sound opinions about these matters. Among the working classes,
on the other hand, especially among those engaged in factory
labour, the heedless gratification of the sexual impulse is responsible
for untold misery.” Hegar’s advice may be summarized as follows:
If the marriage takes place after the attainment of complete
maturity, in the wife at twenty and in the husband at twenty-five,
398and if procreation is discontinued in the wife at forty and in the
husband at forty-five to fifty, if between successive deliveries the
intervals necessary for the wife’s restoration to health are maintained,
if illness and states of debility are taken into account, if
sickly, hereditarily-tainted individuals are forbidden to marry—the
excessive increase in population, as far as Germany is concerned,
will cease to give cause for anxiety. The regulation of reproduction
will, however, still be incomplete, unless we enforce a selection
too rigorous for our present views. Moderation and continence
must aid as far as may be necessary in preventing an undue increase
in population. Hegar does not fail to point out the evil
effects of an excessive limitation of the family. In a marriage when
one child only is born, this child is the object of unceasing anxiety
and attention, and real or imaginary dangers assume an excessive
importance in the morbidly excited imagination of the parents.
Hence we find a continuous excess of watchfulness and over-education
in the case of the only child, to whom independent thought and
action are entirely unknown. Boys become milksops, girls nervous
and hysterical. In the two-children-system, again, one or both of
the children may die when the age of the parents is already considerably
advanced. Still in those districts of France in which this
system obtains the population is well-to-do, and an exceptionally
large proportion of the males are fit for military service. The use
of various measures for the prevention of conception is considered
by Hegar to be harmful, at any rate in the case of young women;
this practice gives rise to anæmic conditions, and to nervous weakness
and irritability, seldom, however, to more serious disorders, as
indeed is apparent from the fact that the mortality of married
women as compared with unmarried women is lower in France than
in other countries.
Gräfe, with reference to the view that if for any reason conception
must be prevented, this should be done by abstinence from
sexual intercourse, remarks: “Doubtless an ideal demand, but one
which even those with exceptional strength of will are unlikely to
satisfy. And the worst of it is, that even a single indiscretion will
often result in impregnation. Moreover, it is distinctly contrary to
natural conditions, that a healthy married couple united by an intimate
affection should live together abstaining completely from sexual
intercourse. The question has already been much discussed,
both in speech and writing, and this will continue in the future,
without altering the fact that the physician will be asked, and will be
399compelled to give, advice regarding the use of means of the prevention
of pregnancy.”
Ribbing writes, “Although the sexual impulse is the product of a
powerful natural developmental force, still the temporary, and sometimes
even the permanent, control of this impulse is a moral civilizing
force of enormous importance.” This writer is opposed to the
use of artificial preventive measures; he considers them untrustworthy
and dangerous to health. Untrustworthy, for the reason
that nature has endowed living organisms with a strong impulse
toward conjugation and has equipped with very powerful forces the
processes by which fertilization is effected. Every physician is
familiar with cases in which preventive measures have proved ineffective.
This fact is proved also by the statistics of prostitution.
Although prostitutes are fully instructed in the use of preventive
measures, which they almost universally employ, nevertheless every
year a smaller or larger number of prostitutes become pregnant.
These measures are dangerous to health, partly because of their interference
with natural functions, because many of them are clumsy
and ill adapted; and partly, again, because owing to their use the
woman fails to enjoy the natural periods of repose which are entailed
by pregnancy, parturition, and lactation. Noteworthy also are
the psychical considerations adduced by Ribbing against the use of
preventive measures. The majority of well-bred women feel deeply
wounded if they believe themselves to be regarded merely as a
means of enjoyment, not as individuals, as persons with inalienable
rights. For the man also there is danger, for it is easy for him to
acquire a dislike to the wife who, even though on his own initiative,
occupies herself with the technique of the sexual life in a manner
which he feels instinctively to be opposed to the chastity and
puremindedness demanded by every man from his wife. Ribbing
therefore advises a certain measure of sexual abstinence in married
life.
Max Nordau also insists on the moral disadvantages of the wide
diffusion of the use of preventive measures. “If a race or nation
has reached this point in its downward career, the individuals of
which it is composed lose the capacity of loving in a healthy and
natural manner. The sense of the family disappears; the men will
not marry, because they find it inconvenient to burden themselves
with the responsibility for another human life, and to care for any
other creature than themselves; the women dread the pains and inconveniences
of motherhood, and if they marry, they endeavour,
400by the employment of the most immoral means, to ensure barrenness.
The reproductive instinct, of which reproduction has ceased
to be the aim, is in some annulled, whilst in others it degenerates
into the most peculiar and irrational perversities. The act of sexual
union, the most sublime function of the organism, is degraded into
a profligate act of lust; it is no longer undertaken in the interest of
the perpetuation of the species, but exclusively for the pleasure of
the individual, and without any relation to the needs of the
community.”
Alfred Russel Wallace has advocated sexual continence as a
preventive measure during the period of maximum vitality and
strength; he advises that the age of marriage of women should be
considerably advanced, in order to diminish their fertility. If
woman’s average age at marriage were 29, instead of 20 years, the
fertility of marriages would be reduced in the ratio of 8 : 5.
The desired goal of artificial sterility will not, however, be reached
through the advocacy of moderation and continence. The numerous
additional measures employed for this purpose may be classified as
physiological and artificial; the latter class may be further subdivided
into mechanical and operative.
By physiological means for the prevention of conception, we
understand measures which aim at producing sterility by reducing
the number of acts of intercourse and by restricting these acts to
certain defined periods of time. The physiological preventive
measures, apart from the higher ethical value they possess in comparison
with artificial measures, have the advantage that they may
be regarded as harmless to the general health of the woman and to
the integrity of her reproductive organs in particular; they have,
however, this very serious disadvantage, that the results of their use
are very uncertain, so that they offer no more than a probability,
and often a very moderate probability that conception will be prevented.
As a physiological measure for the attainment of facultative sterility
“without breaking any moral law,” Capellmann advised abstinence
from coitus during a period of fourteen days after menstruation
and three to four days before the commencement of the
flow. Without laying too much stress on the fact that by following
this recommendation the period during which the intercourse is
permissible would be extremely restricted, it is necessary to point
out that, whilst in this way the occurrence of conception may be
rendered less probable, its prevention is by no means guaranteed,
401for it is an established fact that a woman may be impregnated by
intercourse on any single day of the intermenstrual interval. Capellmann’s
advice, embodying, as he expresses it, the “only morally
permissible” means for the prevention of conception, was not
original, for the same recommendation was given at an earlier date
by Raciborski, who, however, regarded the measure as very uncertain.
Capellmann is of opinion that it is sufficiently trustworthy
for practical purposes.
Bebel, who is a declared opponent of Malthusianism, none the
less lays down positive rules for the diminution of procreative
capacity and of fertility by regulation of the diet. He refers to the
example of the bees, which, by a change of nutriment, can produce
a new queen-bee at will. “Thus the bees,” he says, “are in advance
of human beings in their knowledge of sexual development.
Presumably they have not been compelled, for a couple of thousand
years, to listen to sermons informing them that to occupy themselves
about sexual matters is ‘improper’ and ‘immoral.’ There is
no doubt whatever that the mode of nutrition has an influence on
the composition of the male semen, and also on the susceptibility to
fertilization of the female ovum; hence the increase in population
must to a very important extent depend on the mode of nutrition.
If this could be definitely established, we should have, in the supply
of nutriment, a means of regulating the population. As an example
of the effect, in this connection, of the mode of nutrition in the
human species, it is reported that in consequence of the fatty and
nutritious diet of the old Bavarian peasants, who lived chiefly on
very rich puddings, the marriages of the well-to-do peasants were
frequently childless. However, it must not be forgotten that pre-conjugal
intercourse, which was customary in that part of the
world, and was somewhat promiscuous in character, may have
contributed to cause this sterility.” Finally, Bebel points out that
the woman of the future “will be unwilling to bear a large number
of children. She will wish to enjoy a measure of personal freedom
and independence, and will not consent to pass half or three-quarters
of the best years of her life either pregnant, or with a child at
her breast. From this it will result that the population will be
regulated, without unwholesome sexual abstinence, and without the
employment of unpleasant preventive measures.” However, Bebel
gives us no details as to the precise manner in which this regulation
is to be effected.
Tolstoi, in his widely celebrated book “The Kreuzer Sonata,”
402condemns absolutely the gratification of the sexual impulse. He demands
the recognition of the fact that “sexual congress, in which
a man either avoids the natural consequences—the birth of children,—or
else throws the whole burden of these consequences on
the woman, is opposed to the simplest demands of morality, is in fact
utterly base.” To render possible the sexual abstinence he regards
as morally necessary, men must not only endeavour to live in a
natural way, but they must consume no alcohol, eat with great
moderation, abstain from meat, and not be afraid of hard work.
Tolstoi even demands that men and women shall be so brought up
“that both before and after marriage they may regard love, and the
sensual passion associated therewith, not as they do at present, as a
sublime and poetical state, but as a bestial condition degrading to
humanity.” Tolstoi is, however, utterly opposed to the use of preventive
measures: “first, because they liberate men from the cares
and sorrows entailed by having children, which must be regarded as
the penance to be paid for sensual love; and, secondly, because their
use is closely allied to the crime most repugnant to the human conscience,
the crime of murder.” Chastity is no less a duty after
marriage than before; after marriage man and wife must “continue
to pray to be delivered from temptation, and must endeavour
to replace sensual love by the pure relationship of brother and
sister.”
Eulenburg regards the modern diffusion and the continuous increase
in the use of preventive measures as signs of decadence;
Löwenfeld, on the other hand, regarding the social conditions of the
present day as the principal source of the use of preventive measures,
sees therein no moral decay, but on the contrary rather a rise
in the moral standard of life.
Another physiological means of prevention is to be found in
avoiding cohabitation in that season or month in which, judging by
the woman’s previous deliveries, she would appear to have been
peculiarly susceptible to impregnation. Cohnstein maintained that
in woman, as in the lower animals, the capacity for conception was
associated with a particular season of the year, that there was, in
fact, an individual time of predilection for impregnation. The
assumption that there is such a time of predilection is, however,
traversed by the fact, familiar to all who have recorded the birthdays
of children in large families, that these occur in the most
diverse months of the year. It has, indeed, been statistically proved
that certain months and seasons are especially favourable to conception,
that a maximum of conceptions occurs in the spring, and
403a second much smaller maximum in the winter; but these variations
in the number of conceptions depend mainly on social factors, as,
for instance, upon the customary season for marriage, opportunity
for intercourse between the sexes, common labours in the house or
in the open, etc. This alleged time of predilection for conception
cannot, therefore, seriously be considered in the discussion of
measures for the prevention of pregnancy.
As a physiological means for preventing conception, passivity of
the woman during sexual intercourse has also been recommended.
It is well known that an active participation on the part of the
woman in the sexual act, by increasing her voluptuous sensations,
gives rise to certain reflex actions, viz., descent of the uterus, rounding
of the os uteri, induration of the portio vaginalis, and, finally,
ejaculation of the secretion of the cervical glands and of the glands
of Bartholin; these changes accelerate the entrance of the semen
into the cavity of the uterus, and increase the motility of the spermatozoa.
Upon this fact is based the assumption, that, in consequence
of deficient sexual excitement during intercourse, either
spontaneous, or when the woman intentionally remains “cold,” the
reflex actions by which the upward passage of the spermatozoa is
favoured, fail to occur; there is a good deal of evidence in favour
of the truth of this view. Riedel reports regarding the women of
the Island of Buru, that they often have sexual intercourse with
strange men, “but during sexual congress in such cases they maintain
a passive and indifferent state, for the purpose of avoiding
impregnation.” Von Krafft-Ebing points out that prostitutes, when
having sexual intercourse with men to whom they are attached,
experience voluptuous excitement, whilst in intercourse with men
to whom they are indifferent they remain entirely passive. From
this it would appear that these uterine reflexes are under the dominion
of the conscious will; but sufficient dependence cannot be
placed on this fact in all circumstances for it to be possible to employ
such voluntary control as a trustworthy means of prevention.
Allied to this is previously-mentioned Chinese practice of Kong-fou,
a kind of hypnosis, in which during sexual intercourse the thoughts
are concentrated on some other matter, and thereby conception is
supposed to be prevented.
Artificial protraction of the period of lactation is an old and
well-known method, practised by many savage peoples, for the
prevention of fertilization. As a general rule, as long as lactation
continues, amenorrhœa persists, and sexual intercourse remains
unfruitful. But this rule also is not universally valid.
404Artificial means for the attainment of facultative sterility are
those by which the attempt is made to prevent pregnancy by some
mechanical hindrance to the contact of the semen with the ovum,
since without this contact conception cannot possibly occur.
The oldest of these means is that described in the book of Genesis
(ch. xxxviii, verses 9, 10), congressus interruptus, where, however,
the practice was punished by death, “And Onan knew that the seed
should not be his; and it came to pass, when he went in unto his
brother’s wife, that he spilled it on the ground, lest that he should
give seed to his brother. And the thing which he did displeased
the Lord, wherefore he slew him.” This mode of preventing pregnancy,
in which the membrum virile is completely withdrawn from
the vagina before the ejaculation of the semen takes place, is at
the present time a very widely diffused practice; and, when properly
carried out, it is thoroughly efficacious in the production of sterility.
Thompson relates that this practice is employed by the Massai
youths, who are allowed free intercourse with the girls, but if a
girl becomes pregnant she is put to death.
The prolonged practice of coitus interruptus leads in my experience—in
addition to the injury to the nervous system as a
whole in consequence of the intense hyperæmia of the uterus and
the uterine annexa, unrelieved by the occurrence of the orgasm—to
a condition of stasis in the female reproductive organs; and this
ultimately passes on into chronic metritis (with relaxation of the
uterus, retroflexion or anteflexion, catarrhal disease of the mucous
membrane, erosions, and follicular ulceration of the portio vaginalis),
oöphoritis and perimetritis. As a result of certain remarkable observations,
I must even regard it as not improbable, although actual
proof is still lacking, that the recent striking increase in the frequency
of neoplasmata of the female reproductive organs is causally dependent
on the ever-increasing employment in all circles of society
of means for the prevention of pregnancy.
The evil effects of coitus interruptus for a woman are dependent
on the fact that the woman fails to obtain complete sexual gratification,
and that this has an important influence upon her entire
organism. Owing to the failure of ejaculation to occur, the blood,
which during the stage of sexual excitement has accumulated in the
erectile structures and cavernous spaces of the genital passage, does
not, as in normal conditions, flow rapidly away; but the congestion
persists for an indefinite period, and is said by von Krafft-Ebing
to give rise to functional disorders, and also to serious tissue
405changes. The functional disorders take the form of hyperæmia of
the pelvic organs, and probably also of the lumbar portion of the
spinal cord (dull pain in the sacral region, a sensation of pain and
dragging in the pelvis and in the lower extremities, lassitude); these
symptoms often continue for several hours after intercourse. If
this ungratifying coitus is frequently repeated, in a voluptuous
woman, disorders of the reproductive organs ensue; and even more
frequently, nervous disorders, in the form of neurasthenia sexualis.
This author considers that, more especially in women, coitus interruptus,
and unphysiological modes of sexual intercourse in general,
are extremely potent causes of sexual neurasthenia—as potent
as masturbation.
Beard, in his work on sexual neurasthenia, maintains that the
sudden interruption of coitus (and also the use of condoms and
similar appliances) is not only far more deleterious than unduly
frequent normal intercourse; but he points out that it is necessary
also to take into account the fact that (inasmuch as, owing to the
unnatural mode of sexual intercourse, the possibility of fertilization
is almost completely prevented) sexual intercourse is apt, in
such cases, to be indulged in far more frequently, and often to gross
excess. More particularly in such circumstances are evil effects on
the nervous system likely to ensue, since we have a combination of
excessively prolonged and frequent sexual intercourse, and of interference
with complete sexual gratification.
Mantegazza believes that organic diseases of the spinal cord may
actually result from congressus interruptus.
Hirt considers that even when marital intercourse is carefully
regulated in respect of frequency, congressus interruptus may lead
to neurasthenic manifestations.
Von Hösslin believes it to be indisputable that preventive methods
of sexual intercourse may cause nervous troubles, and more
particularly neurasthenic disorders, manifesting themselves chiefly
in the sphere of the reproductive organs.
Eulenburg also declares that coitus interruptus is already a frequent
cause of sexual neurasthenia in women, and that its evil
influence in this respect is becoming more and more frequently manifest.
He publishes two typical cases, in which, from this cause, in
the one case, functional neuropathy, and in the other, local disorder
of the reproductive organs, ensued.
Freud describes an “anxiety-neurosis,” which is due to incomplete
gratification of the woman during sexual intercourse. Coitus
406interruptus is almost invariably harmful to the man; to the woman
it is harmful if the man thinks only of himself, and interrupts the
coitus as soon as ejaculation is imminent, without concerning himself
about the woman’s state of sexual excitement. If, on the
other hand, the man waits until the woman’s sexual gratification is
complete, the significance of such an interrupted coitus as far as
the woman is concerned is that of normal intercourse.
Isolated authorities, as for instance Stille and Thompson, have
contested the alleged evil consequences of preventive methods of
sexual intercourse. “It is habitual excess,” says Fürbringer, “which
does the mischief, not the unnatural character of the isolated act.”
Löwenfeld, who considers the opposition of medical men to “Malthusianism”
not wholly justified, and believes that the dangers to
health “which occur in isolated cases” are not very serious, maintains
none the less that the medical man must advise his patients
not to practise coitus interruptus. The mode in which conception
is prevented is not, he thinks, a matter of indifference to the woman.
The use of occlusive pessaries and similar appliances does not in
any way interfere with the normal development of sexual gratification
and cannot, therefore, have any direct influence in the production
of nervous disturbances. A forgotten occlusive pessary,
however, has in many cases caused local disorder in the vagina.
When the man is fully potent the use of condoms can do no harm
to the woman, since the only effect of the condom (in a very excitable
woman) is to render the development of the orgasm a little
more difficult, but not to prevent it. Congressus interruptus itself
is, according to Löwenfeld, harmful to the woman only when,
owing to deficient potency in the male or to deficient excitability
in the female, the interruption takes place before the occurrence of
the orgasm.
Valenta declared that coitus interruptus was one of the chief
causes of chronic metritis. Elischer saw perimetritis result from
this practice; Gräfe enumerates, as consequences of frequently repeated
coitus interruptus, chronic hyperæmia of the uterus and
oöphoritis; Goodell observed elongation of the cervix uteri; Mensinga,
infarction of the uterus, œdema of the portio vaginalis, ulceration
of the cervix, hysterical paroxysms, convulsions, cephalalgias,
cardialgias, etc. Lier reports a case in which, after three years’
continued practice of coitus interruptus, the menopause set in, with
atrophy of the uterus; Ascher, in a similar case, saw chronic
metritis ensue. According to Kleinwächter, coitus interruptus is
407harmful to the woman to an extent by no means trifling, whereas
the man, in whom ejaculation occurs, suffers comparatively little.
Fehling believes that when coitus interruptus is practised only a
small proportion of women experience sexual excitement. Neugebauer
states that among the very numerous cases of uterine carcinoma
he has treated, the majority of the patients admitted having
practised coitus interruptus. Pigeolot makes a similar statement.
It must, however, be admitted that a certain number of medical
men absolutely deny the dangers of coitus interruptus, whilst others
consider them altogether trifling. Just as the trend of modern
opinion is to believe that in normal men and women the dangers
of masturbation are far less serious than was formerly maintained,
so also many are now found to maintain that coitus interruptus is
harmful only to those with hereditary neuropathic predisposition.
Still more unwilling are many to admit that other preventive
methods do women any harm. Thus Wille maintains that the continued
fear of pregnancy will in most instances do more injury to
the feminine nervous system than all the preventive measures in
the world. To the nervously weak woman a trustworthy preventive
of pregnancy is therefore often necessary and most helpful.
An artificial method for the prevention of the ejaculation of
semen was communicated to me by a celebrated anatomist. It is
practised in Transylvania and in France. During intercourse the
woman, just before the male ejaculation begins, presses forcibly
with her finger on the base of the erect penis just in front of
the prostate; the urethra is occluded by this digital compression,
the semen regurgitates into the bladder and is subsequently evacuated
with the urine.
This practice may be compared with the mechanical expulsion
of the semen from the female genital passage immediately after
coitus. Tairi reports that women of the poorer classes in Italy
sit upright in bed immediately after intercourse, and by coughing,
in conjunction with pressure on the abdomen, effect the expulsion
of the semen. Morton informs us that the native women of Northern
Australia, when they have had intercourse with a white man
and wish to avoid impregnation, likewise deliberately effect the outflow
of the semen post actum. The woman squats upright, with
the legs widely separated, and by a sinuous movement of the
perineum and a simultaneous powerful bearing-down pressure she
expels the semen on to the ground.
Another way in which the attempt is made to avoid impregnation
408is by the use of vaginal injections; a fluid lethal to the spermatozoa
being used for this purpose immediately after coitus. Douches of
cold water, ½ to 1% solution of copper sulphate, 1% solution of alum,
¼% solution of sulphate of quinine, are the fluids most commonly
employed; but all these are quite untrustworthy, for it is impossible
to be sure that all the spermatozoa will be acted on and destroyed.
Allbutt, who as medical secretary of the Malthusian League in
London has unquestionably had a very wide experience, agrees
with Haussmann in denying that the widely advocated cold water
douche can be relied on for the prevention of pregnancy. The sudden
driving of the blood out of the vessels of the genital passage
at the very moment when they are intensely congested, which must
inevitably result from a cold douche, is, moreover, likely to give
rise to metritis, perimetritis and oöphoritis.
More trustworthy are the various apparatus, the aim of which
is to prevent the contact of the semen with the ova by the interposition
of an artificial wall. Although even as regards these we
must bear in mind the observation of Lott, who found that spermatozoa
were capable of passing through the intact membrane in
favourable regions in as short a time as ten minutes. The commonest
of all these apparatus is the article known as a condom,
which envelops the penis with a membrane, variously consisting of
isinglass, the lamb’s cæcum, or caoutchouc. Condoms, if made of
suitable material, and if carefully used, are the most trustworthy of
all preventives. Moreover, the injury caused by their use to the
woman’s health is trifling, for they do no more than diminish to a
degree the intensity of the stimulus, thus necessitating a somewhat
longer duration of its action in order to effect the most intense
orgasm, and thus to induce the natural physiological termination
of the nervous excitement. In fact, though somewhat delayed, the
normal reaction takes place in the reproductive organs. The evil
effect of the use of the condom bears no comparison with that of
coitus interruptus. There is, however, some justification for
Ricord’s well-known epigram, that the condom is “a spider’s web
for the prevention of danger, and a cuirass for the prevention of
voluptuous pleasure.”
When the gynecologist, from well-considered reasons based on
some pathological condition affecting his patient, feels justified in
recommending the prevention of pregnancy, it is my opinion that
the most trustworthy and least harmful measure at present available,
and one preferable to all other mechanical apparatus, is a carefully
selected and well-made condom.
409The condom was already in use in Italy in the middle of the
sixteenth century, in the form of a linen investment adapted to
the shape of the penis; subsequently, according to Grünfeld, condoms
were made from the cæcum of the lamb; while later still,
isinglass was employed for this purpose. According to Hans Ferdy,
the cæcal condom is made from the connective-tissue layer of the
cæcum of the sheep or of the calf (a very young animal); to
a less extent, also, the cæca of the goat, the stag, and the roe-deer,
are employed for this purpose. The different varieties of cæcal
condom are distinguished chiefly by variations in the thickness and
the softness of the membrane. Ferdy states that the four best
kinds are made from the cæcum of the sheep; these have a thickness:
I. 0.008 to 0.01 mm. (0.00032 to 0.0004 in.); II. 0.012 to
0.015 mm. (0.00048 to 0.0006 in.); III. 0.017 to 0.023 mm.
(0.00068 to 0.00092 in.); IV. 0.025 to 0.03 mm. (0.001 to
0.0012 in.) Next in quality come four varieties obtained from the
calf, varying in thickness from 0.015 to 0.04 mm. (0.006 to 0.016
in.) Finally we have three varieties obtained from the three other
animals already mentioned. Thus there are in all eleven varieties of
cæcal condom, and in so far as during the process of manufacture
the membrane has remained free from any injury, they are sold
as “undamaged.” But if in the process of preparation a hole has
been made in the membrane, this aperture is closed by sticking on a
small patch of membrane. Such patched condoms are naturally
quite useless, since the patch is readily loosened by the moisture to
which it is exposed, and falls off, when the protective and preventive
functions are entirely destroyed; nevertheless, such defective
condoms are often sold. Rubber condoms, continues Ferdy,
are prepared from a caoutchouc membrane 0.03 to 0.1 mm. (0.0012
to 0.04 in.) in thickness; but these, he says, are not hygienic, for
“such a rubber membrane, which both in the man and in the woman
completely covers the erogenic zones normally stimulated in coitus,
deadens the necessary stimulation, so that the sensations during
coitus are seriously dulled by the interposition of this foreign
body; by nervously predisposed individuals, this kind of condom
cannot be used regularly for a long period, without rendering
probable the onset of serious functional disturbances of the genital
apparatus.” This opinion appears to me to be unfounded. We must
also mention the “glans-condom,” made of rubber membrane,
which serves to cover the glans penis only during coitus, and to
retain the seminal secretion; its grave defect, however, consists in
410this, that in the act of withdrawing the penis, the condom is very
likely to be peeled off, when the semen will, after all, pass into the
vagina.
Passing now to the consideration of apparatus which are inserted
into the woman’s genital canal, in order to prevent impregnation,
we may first mention sponges, which have long been in use;
after thorough cleaning, these may be rendered aseptic by immersion
in carbolic acid or lysol solution. These sponges should be very
soft; they are cut into balls of 3 to 7 cm. (1.2 to 2.8 in.) in diameter;
before coitus they are introduced into the vagina and after
coitus they are withdrawn by means of the tape which should
always be attached to them. This method is, however, quite untrustworthy,
for the sponge offers no impermeable wall to the
passage of the spermatozoa, and on its withdrawal, some of the
semen may very likely be left in the vagina. The same objection
must be made to the similarly constructed anti-conceptional cotton-wool
plugs; sometimes these are moistened with a fluid intended
to destroy the spermatozoa. Recently Gunzburg has recommended
the introduction into the vagina of a cotton-wool plug moistened
with a three per cent. solution of carbolic acid in glycerine; he considers
this method safe, because the spermatozoa are immediately
destroyed on contact with the weakest carbolic acid solutions.
To destroy the vitality of the spermatozoa, vaginal suppositories
made of cocoa-butter medicated with hydrochlorate of quinine have
also been employed; these, the so-called “security-pessaries” or
“security-ovals,” are inserted into the vagina half an hour before
coitus; the cocoa-butter is melted by the body heat, and the vaginal
mucous membrane and the os uteri are covered with the medicated
fatty material, by which the spermatozoa are (or should be)
destroyed. This method is one easy to employ, but it is extremely
uncertain.
Even more uncertain are the insufflators charged with various
powders (boric acid, citric acid, thymol, etc.); the tube of the
insufflator having been passed into the vagina, the powder is blown
over the vaginal mucous membrane and the portio vaginalis. This
procedure may sometimes be followed by symptoms of intoxication;
and in any case, owing to the desiccative effect which the powder
has upon the vaginal mucous membrane, it exercises a disturbing
influence on coitus.
Kleinwächter, in cases in which pregnancy must be prevented in
the interest of a woman’s health or her life, has recommended the
411introduction into the vagina of globules of which the active constituent
is boric acid.
A rationally constructed apparatus, and one which in general appears
to fulfil its purpose very well, is the pessarium occlusivum
constructed by Mensinga, and now manufactured in various modifications.
The occlusive pessary is a hollowed hemisphere of rubber
membrane, around the margin of which passes a steel ring.
The size of the pessary must be adapted to the individual case.
It is introduced into the vagina in such a way that the outer surface
of the hemisphere occupies the vaginal fornix, while the steel
ring touches the vaginal wall all round; by this means, the vaginal
fornices and the os uteri are completely shut off from the lower
part of the vagina. The disadvantage of this instrument is, that
either the woman must wear it continuously, which involves numerous
inconveniences, or else it must be introduced by the skilled
hand immediately before coitus—and not every woman becomes
competent to adjust it herself, even after careful explanation, since
the pessary must be accurately placed with the anterior margin of
the ring immediately behind the pubic symphysis, and the posterior
margin of the ring behind the os uteri. Moreover, the instrument
may easily be displaced by violent movements, coughing, sneezing,
etc. In any case, the pessary must be carefully selected to correspond
within the configuration of the vagina, as otherwise it may
exercise a deleterious pressure upon the vaginal walls, and may give
rise to other bad consequences, such as are apt to attend the wearing
of any pessary for a prolonged period—excoriations, erosions,
fluor albus, etc. In the majority of cases it will be found that the
woman herself is not competent to introduce the occlusive pessary.
The skilled hand is needed for the proper adjustment of the surrounding
ring.
Gall’s balloon-occlusive-pessary consists of a soft elastic rubber
disc, surrounded by a thin-walled rubber ring, the interior of which
is connected by means of a fine tube with an inflating rubber ball.
The woman can herself insert the instrument and inflate the ring;
it occludes the vaginal passage without exercising any deleterious
pressure.
Other pessaries consist of hollow rubber balls containing some
fluid lethal to the spermatozoa, which can be discharged into the
vagina on opening a valve by pulling a string. These, however, are
as insecure as the above-mentioned vaginal discs and the insufflators.
The duplex-occlusive-pessary has the form of a truncated cone
412with double walls; in its base are a number of rounded apertures,
and a single elongated aperture; through this latter a boric acid
tablet is introduced into the cavity of the cone. By means of the
cone the passage to the uterus is mechanically occluded; the semen
passes through the apertures in the base into the interior of the
instrument, and as the boric acid tablet is dissolved by the moisture
to which it is now exposed, the vitality of the spermatozoa is destroyed.
The management of this apparatus is, however, not easily
effected by the woman herself. The “Matrisalus-Pessary” differs
but little from other occlusive pessaries. The latest instrument for
the prevention of impregnation is known as the “Venus-Apparatus;”
it consists of a syringe with two balls, a large and a small
one, at either end of a rubber tube; by pressure on the larger
ball, and subsequent relaxation of pressure, the smaller ball is
filled with a fluid for the destruction of the spermatozoa (prepared
by the solution of one of the “Venus-powders” sold with
the instrument); when filled, this smaller ball is introduced into
the vagina and remains connected by means of the tube with the
larger ball, which lies between the woman’s thighs. At the moment
of the male ejaculation the woman presses on this ball, and by this
means the fluid filling the smaller ball is expressed into her vagina.
All these mechanical occlusive pessaries are open to the objection
that they are apt to give rise to irritative conditions of the genital
organs, causing offensive discharges, pruritus, etc. (Recently in
order to diminish this drawback, the pessary has been constructed
of vulcanized cambric, instead of rubber, and appears then to have
a less irritating effect.) Still worse is the injury to the uterus and
to the cervical mucous membrane caused by certain intra-uterine
instruments which have been recommended for the prevention of
conception. The latest of these is an “obturator,” consisting of a
silver or silver-gilt tube, which is passed through the os uteri into
the interior of the uterus, and left in situ. It is claimed for it
that “it allows the menstrual discharge to flow freely away, but
renders the entrance of the spermatozoa extremely difficult.” Biermer
reports five cases in which serious injury to health followed the
use of one of these obturators. In one of these cases in which
there were very severe pains and a discharge from the uterus,
Biermer removed from the interior of the uterus a broken wing of
the obturator; the patient died, however, and the autopsy disclosed
perforation of the uterus. In another of the cases the apparatus
was also broken.
413Less dangerous is the recently invented tampon-speculum. This
is passed into the vagina by the woman herself, in order that
through it she may, by means of a special introducer, insert a tablet
of boric acid, hydrochlorate of quinine, citric acid, or some other
substance lethal to the spermatozoa. Without some such instrument,
the introduction of these “ovals” to the proper place is often found
difficult by women.
A very remarkable means of bringing about artificial sterility, one
resembling the operative procedures sometimes adopted in western
countries, is employed in various parts of the world, and notably in
the East Indies and in the Sunda Islands, namely, the induction of
an artificial malposition of the uterus, more especially of anteversion.
Thus, van der Burg writes from the Dutch Indies: “In the girls
the sexual impulse develops very early, and is gratified without fear
of consequences, when the services of certain skilled elderly women
have been requisitioned.” These women appear, in fact, to understand,
by means of pressure, rubbing, and kneading, through the
abdominal walls (not by the vaginal route), how to induce anteversion
or retroversion of the uterus, to such an extent as to prevent
the occurrence of conception. It is said that the only inconvenient
consequences of this procedure are trifling pains in the lumbo-sacral
and inguinal regions, and some trouble in passing water during the
first few days after the manipulations have been effected. Later,
when a girl who has been treated in this way wishes to marry and
become a mother, by a reversal of the manipulations the uterus
is restored to its natural position. It is said that these skilled
women have been called in by European women in the Dutch Indies,
who did not wish to have many children; but it appears that in a
woman who has once given birth to a child, the result of the
manipulations is less to be depended upon, than in the case of a
virgin.
A means of ensuring artificial sterility, which in all civilized
states is punishable as a criminal offence, and which is nevertheless
very frequently practised, is the artificial induction of abortion.
Especially in North America it would appear that there exist regular
professional abortionists. In this connection, Thomas, the well-known
American gynecologist, writes as follows: “Statistics showing
the frequency of criminal abortion are not, and probably never
will be, available, for this crime cannot be adequately controlled by
human society, and commonly eludes legal punishment. It seems
a hard saying, but it is a true one, to assert, that the law pursues
414unremittingly him who has killed his fellow-man, while it leaves
immune him who has killed the embryo in the mother’s womb. On
my table there lies at this moment one of the most widely circulated,
most respected, and most carefully edited daily newspapers of
New York—a paper which finds its way into the best circles of
society, and also into the hands of girls and women throughout
the country. In its columns I find fifteen advertisements which
emanate beyond all question from professional abortionists—from
men and women who gain their livelihood by child-murder.”
O. Reyher remarks also that in American newspapers advertisements
such as the following are of every-day occurrence: “Pills
for the regulation of the periods. Ladies expecting to be confined
are warned not to use them on any account, for if they do so
abortion will infallibly ensue.”
Emmet, in his “Textbook of Gynecology” also complains of the
terrible frequency of criminal abortion, so that “every day we see
more unhappiness and misery result from the misuse of conjugal
relationships than we see in an entire month as a result of births
which take place in a natural manner.”
Pomeroy also says that “The prevention of conception and the
destruction of the unborn life are pre-eminently American sins;”
and he adds that if no bounds are set to their spread, “they must,
sooner or later, lead to universal misfortune. In the course of our
practices we come into contact with women who would hesitate to
kill a fly, but who think nothing of having destroyed half a dozen
or more of their own unborn children.”
The American Medical Congress offered a prize for a brief and
readable essay, suitable for diffusion among women, showing the
criminality and the physical harmfulness of artificial abortion. The
prize was awarded to Storer’s essay, entitled “Why Not?”
Among the ancient Greeks, the fear of over-population led to the
practice of homosexual intercourse. The states of ancient Greece
were in most cases of a very small area, so that a very moderate
increase in population would render the means of subsistence insufficient.
Hence intercourse with women was avoided, and the
sexual impulse was gratified in unnatural ways. Inspired by this
fear of over-population, Aristotle urged upon men that they avoid
women, and should indulge in the love of men and boys, and at
an earlier date, Socrates had celebrated the love of boys as a
mark of higher culture. The most notable men of classical Greece
practised homosexual intercourse; authors and poets celebrated the
love of boys. Stimulated by their example, Sappho of Lesbos became
415the inspired poetess of the love of women for members of
their own sex (Lesbian love).
Among the Romans it was rather satiety in consequence of sexual
excesses which led in that country to the diffusion of the Greek
love of boys; the consequent childlessness diminished to such an
extent the numbers of the Roman burghers and patricians, that
Augustus, in the year 16 B. C., enacted the Julian law, by which
the procreation of children was rewarded, whilst celibacy became
a punishable offence.
At the present day the fear of an excessively large number of
children, in relation to the property possessed by the parents and in
regard to nutritive possibilities, has led among whole classes, and
even among entire nations, to the adoption of preventive measures
in sexual intercourse; these measures have, in fact, been developed
into a system, which finds adherents among all strata of the population,
but more especially, as it is easy to understand, among certain
well-to-do sections of the community. In France this system
has been adopted to such an extent as to amount to a national
calamity.
In few countries of the civilized world, remarks Bebel, are marriages
so frequent, relatively to the population, as they are in
France, whilst in no country is the average number of children per
marriage so small, or the increase of population so slow. The
French bourgeoisie long ago adopted this system, and the peasantry
and the artizan classes are following their example. In many parts
of Germany the same causes have led to the same results. In
France, in addition to the prevention of pregnancy and the practice
of artificial abortion, infanticide and the exposure of children are
also actually employed to keep down the population.
Operative measures for the production of artificial sterility have
been practised from very ancient times, and by civilized and savage
peoples alike. According to Strabo, the ancient Egyptians and
Lydians were acquainted with the art of removing the ovaries from
girls and women. The kings of Lydia, Andromytes and Gyges,
had the women of their harems castrated, ut iis semper ætate et
forma florentibus uteretur. Von Micklucho-Mackay reports that in
some parts of Australia the indigens remove the ovaries of certain
girls, in order to provide their young men with hetairæ who cannot
possibly become pregnant. M. Gillirray saw at Cape York a native
deaf and dumb woman whose ovaries had been removed, to prevent
her procreating deaf and dumb infants.
416We cannot refrain from reference to the astounding proposal
of C. A. Weinhold, contained in his work upon the over-population
of Central Europe and its consequences to the countries concerned
and to civilization in general. He advises, “as a general and
urgently required measure, the widespread practice of a sort of infibulation,
which is to be undertaken at the age of fourteen and
preserved until marriage, and is to be performed in the case of
all those individuals who can be proved not to possess sufficient
property for the upbringing of an infant, if they should become
pregnant as a result of extra-conjugal intercourse. And in those
who never attained a financial position in which they might be able
to bring up a family, the infibulated condition should be allowed
to persist throughout life!”
This proposal is, in fact, no novelty, inasmuch as the bringing
about of an artificial adhesion of the labia with a view to the
prevention of conception—the operation of infibulation—is practised
by many savage peoples. According to the detailed account
given by Ploss-Bartels, this operation, in which the inner surfaces
of the labia majora are freshened, stitched together, and allowed to
adhere, is practised by the Bedschas, the Gallas, the Somalis, the
inhabitants of Harrar, at Massaua, etc. The purpose of this practice
is to preserve the chastity of the girls until marriage, when the
reverse operative procedure is undertaken. If the husband goes
away on a journey, in many cases the operation of infibulation is
once more performed upon his wives. Slave-dealers also make use
of this operation so as to prevent their slaves from becoming pregnant.
It is reported, however, that the operation does not invariably
produce the desired effect. Hartmann informs us that in Nubia, in
Senaar, and in part of Kordofan, the præputium clitoridis or the
entire clitoris is cut away, and the margins of the nymphæ are then
freshened and stitched together, so that the only aperture left is
one sufficiently large for the outflow of the urine.
Brehm states that the operation is performed by old women, who
make the necessary incisions with razors; shortly before marriage,
the bridegroom sends the girl’s relatives a model of his penis, carved
in wood, according to the size of which an aperture is made between
the adherent nymphæ; when the woman becomes pregnant, the incision
is still further enlarged. In the kingdom of Darfur, the
labia majora as well as the nymphæ are freshened and stitched
together. In the Berber country, Werne became acquainted with a
young widow whose husband had had her submitted to the operation
417of infibulation no less than seven times. Another somewhat
less brutal method of performing infibulation is described by Ploss,
as being practised by many Eastern races; a ring is fastened through
the labia in such a way as to guard the introitus vaginæ In Europe,
during the Middle Ages, such and similar apparatus (“girdles
of chastity”) are said to have been employed for the protection of
the honour of an absent husband.
Of gynecologists who have advised operative measures for the
prevention of pregnancy, in women in whom that condition involved
serious dangers, the first, as far as I know, was Blundell. As a
result of experiments made on rabbits, he suggested division of the
Fallopian tubes as the best way of attaining this end. Later, Froriep
and Kocks also endeavoured to induce artificial sterility in women
by occlusion of the Fallopian tubes. Froriep’s idea was to bring
about obliteration of the lumen of the tubes by means of cauterization
with nitrate of silver; Kocks constructed for the same purpose
a galvano-caustic uterine sound. But, in the first place, both the
methods advocated are too uncertain to be relied upon; and, in the
second place, their application is neither easy, nor devoid of serious
risk.
Much more effective, however, is the method recommended by
Kehrer for the sterilization of women, namely, division of the
Fallopian tubes by the vaginal route. Kehrer considers that the
physician is justified in preventing the occurrence of pregnancy in
a number of morbid conditions—incurable nervous, cardiac, pulmonary,
gastric, and renal disorders; various constitutional affections;
and, finally, in cases of pelvic deformity of such a degree
that the delivery of a living child is impossible except by means
of Cæsarean section, but the patient does not wish to be exposed
to the risks of this operation. He believes, moreover, that all the
methods commonly recommended for the prevention of pregnancy
are untrustworthy. So powerful, however, is the sexual impulse,
that, as experience shows, the mere prohibition of sexual intercourse,
however earnestly made, invariably proves ineffectual. For
coitus interruptus to be effective, the interruption must occur at
the right moment; and this does not always take place. Cold water
douches after coitus are unhygienic; douches of warm water, medicated
with sublimate, alcohol, and other drugs lethal to the spermatozoa,
are indeed rationally conceived, but often fail of their effect,
either because they are deferred until too late, or else because they
fail to irrigate all parts of the vagina. Plugs of cotton wool,
418sponges, etc., are not always introduced in such a way as effectually
to occlude the vaginal passage. A suitable and properly introduced
occlusive pessary is, indeed, a relatively trustworthy preventive
apparatus, but if worn continuously it is apt to become very foul. A
thorough douching of the genital passage with an antiseptic solution,
performed by the skilled hand, immediately after coitus,
would doubtless destroy the spermatozoa with the like certainty
with which the same procedure destroys micro-organisms when
performed prior to a gynecological operation—but when carried
out by the layman, the value of the method is more than doubtful.
The operation, for a time actually fashionable, of extirpation of
the uterine annexa, certainly gives rise to sterility, but entails the
serious disadvantage that the consequent premature menopause is
attended by the same disturbances as the natural change of life.
On the other hand, section and ligature of the Fallopian tubes is
considered by Kehrer to induce sterility without in any other way
disturbing the functions of the female reproductive organs. By means
of anterior colpotomy we obtain a suitable route for the ligature and
section of both tubes at the isthmi. When carried out with the
proper antiseptic precautions the operation is almost entirely free
from risk; and when the organs are healthy the closure of both
the upper and the lower segments of the tubes is effected, and no
retention of secretions need be feared as a result of the operation.
With regard to the indications for the performance of this operation,
Kehrer insists that it should be undertaken only in cases of
serious disease, and when the pros and cons have been conscientiously
weighed. A consultation is also indispensable. Moreover, it
is essential that husband and wife should both fully understand
the nature of the proposed operation, and should form an unbiassed
judgment regarding its advisability. To avoid any possibility of
subsequent reproaches, Kehrer advises that a written report should
be drawn up, giving the reasons for undertaking the sterilization,
and that this should be subscribed by the physicians in consultation,
by the patient herself, and by her husband.
Arndt considers that in cases in which there already exists serious
constitutional disease, the performance of this operation may
lead to fever, severe hæmorrhage, injury to adjacent organs, and
even death. He holds, therefore, that in such cases the physician
should advise the use of some of the more ordinary methods of
preventing conception (if simple abstinence from intercourse cannot
be practised). Only in women with pelvic contraction of the
419second or third degree, in whom previous children have been still-born,
or subjected to craniotomy, is operative sterilization by
Kehrer’s method justifiable. But in preference to anterior colpotomy,
as recommended by Kehrer, he prefers the longitudinal incision in
the posterior vaginal fornix advised by Boileux. If the uterus is
drawn down firmly, and the portio vaginalis then pushed forward
against the pubic symphysis, it is easy, at any rate with the assistance
of a little abdominal pressure, to draw part of the Fallopian tubes
into the vaginal incision.
Recently Pincus has recommended the cauterization of the uterine
cavity with superheated steam (atmocausis, castratio uterina). He
advises it only in women who are incurably ill (tuberculosis, morbus
Brightii, hæmophilia), so that pregnancy and parturition would
involve almost certain death.
Kossmann considers that when pregnancy and parturition will
endanger a woman’s health and life, it is the physician’s duty to
acquaint both husband and wife with this fact; but having done
so his duty is fully discharged. “If, after being warned, the married
pair choose to indulge in sexual intercourse, they have knowingly
and voluntarily run into danger, and for this the physician is
in no way responsible.”
As indications for facultative sterility Levy enumerates tubercular
disease of the lungs, mental disorders, severe organic or functional
diseases of the central nervous system, active syphilis (in certain
circumstances), pernicious anæmia, hæmophilia, diabetes mellitus,
severe heart disease, chronic disease of the kidneys or liver, certain
pelvic deformities, and the tendency to habitual abortion.
I have myself before now stated my opinion that it is the duty
of the physician, in the case of a married woman suffering from
heart disease, with due regard to the danger which pregnancy will
entail upon her, to give needful advice in the matter of the prevention
of conception. In women affected with valvular heart
disease, and in whom there are serious disturbances of compensation,
conception is absolutely to be avoided; also in conditions of
marked cardiac degeneration, and when there are distinct symptoms
of insufficiency of the heart muscle. When, on slight exertion,
palpitation, increased frequency of the pulse, and respiratory need
(“air-hunger”), ensue; when there is extensive œdema of the
lower extremities which persists even after confinement to bed;
when the pulse readily becomes arhythmical both in respect of the
strength and the temporal succession of the beats; when the urine
420is scanty and contains varying quantities of albumen; when there
are frequent attacks of heart-weakness, with a small irregular
pulse, coldness of the extremities, a cyanotic tint of complexion,
nausea, dyspnœa, sense of faintness, or actual syncope—in all such
cases, whether dependent upon valvular disease, on pathological
changes in the arteries, or upon disease of the myocardium, the
occurrence of pregnancy is a true disaster, giving rise in most
cases to a grave aggravation of the heart trouble and often enough
costing the patient her life. I further regard it as a sound medical
axiom that in cases of cardiac disorder of a less severe type than
that just described the woman thus affected should not have more
than one or two children. This is the more necessary because with
each successive pregnancy the functional capacity of the diseased
heart decreases in geometrical progression and the danger to life
proportionately increases. But in such cases of heart disease the
prevention of pregnancy must never be effected by the interruption
of coitus by the man before ejaculation, for the reason that this
procedure gives rise to manifold reflex cardiac troubles, and
especially to paroxysms of tachycardia, with simultaneous diminution
in vascular tone, vasomotor disturbances, and states of mental
depression—and these entail exceptional dangers in women suffering
from heart disease.
The Determination of Sex.
The problem of the determination of sex in the human species
is one which has occupied natural philosophers from the very
earliest times, and has always greatly interested all classes of the
population.
The interest awakened by the subject depends principally on the
fact that female children have usually been less desired than male
in all periods of history and among almost all races. In the uppermost
circles of society the truth of this statement is manifested by
the fact that the birth of a prince is announced by a salute of 101
guns, that of a princess by a salute of 35 guns only.
It would serve no useful purpose to transcribe here the opinions,
or rather guesses, which were ventured on this topic in earlier
days when the very nature of the reproductive process was still
entirely unknown, and we shall merely mention that the curious
will find various references to the determination of sex in the works
of Hippocrates, Aristotle, Plutarch, Soranus, Susruta and Galen.
421Broadly speaking, the earlier theories may be said to diverge in
two main directions, some holding that the sex of the infant was
in some way determined by the mode of intermixture of the male
and the female elements in the act of generation, and others maintaining
that sex was already inalterably predetermined at the time
of intercourse either in the male or in the female sexual elements.
Pari passu with the modern development of the theory of evolution,
and with the enormous increase in recent days in anatomical
and physiological knowledge, the theory of the determination of
sex has been very widely extended. The rival views may be briefly
arranged in the four following categories:
I. That sex is already inalterably predetermined in the ovum,
upon the constitution of which it solely depends; there are therefore
male and female ova, and the process of fertilization exercises
no influence whatever upon the determination of sex. The alternative
theory to the above, that sex is determined solely by the constitution
of the fertilizing spermatozoon—i. e., that the spermatozoa,
and not the ova, are male and female, respectively—is one
which in recent years has tended more and more to disappear from
the field.
II. That sex is determined in the moment of fertilization by the
reciprocal interaction of male and female, of zoösperm and ovum.
One variant of this theory maintains that each reproductive element
strives for the reproduction of its own sex; that a struggle
takes place and that the victor in the contest stamps its own sex-likeness
upon the fertilized product. According to another view,
however, sex is not directly transmitted in this manner; it is supposed
that the more powerful the proper reproductive element
(according to this theory the ovum) the more strongly does it tend
to determine the reproduction of a stronger, i. e., a male organism;
thus the greater potency of the female element in the act of
reproduction tends to favour the determination of the male sex.
III. That sex is not determined until after fertilization, during
the early stages of the development of the embryo; the determining
causes are supposed to be various factors capable of influencing
the developing organism during this period, and more particularly
the nutritive conditions of the mother.
IV. That the determination of sex is not dependent solely upon
the action of any single one of the factors above enumerated, but
arises as a resultant effect of the operation on the germ of all three
of these acting in temporal succession.
422Modern physiology has endeavoured to solve this problem by
statistical investigations, by anatomical demonstration, and finally
by experiment.
I. Statistical Investigations.
Statistical data have been collected showing the ratios between
male and female births in the most varied conditions possible, and
from these data the attempt has been made to draw valid conclusions
regarding the causes of the determination of sex. Now in
the first place it is above all necessary to bear in mind that such
statistical data cannot possibly have any value unless they relate
to very numerous instances, and even then they are liable to be
invalidated by various sources of fallacy. We may with advantage
quote in this connection the remarks of Hensen in his work on the
“Physiology of Reproduction:” “Each individual instance is rendered
unique in kind by the interaction of certain incommensurable
elements; for instance the state of health of the individual organs
in their innumerable combinations, variations in the general health
of the parents, the frequency of coitus and the time at which it
took place, the desire of the parents to have a son and then no
more children, their social position—in these ways innumerable
complications are introduced into the problem, and the difficulty of
drawing valid conclusions is rendered almost insuperable, unless
the number of instances dealt with is enormously large.”
One fact definitely established is that more boys are born than
girls, the proportion between the two, known as the sexual ratio,
being 106 : 100. Statistics relating to the half of Europe (Oesterlen)
and dealing with 59,350,000 births, showed a ratio of 106.3 male to
100 female births; in individual countries variations from this mean
are found to occur, but these are not very extensive, the highest
ratio being 107.2 : 100, and the lowest ratio 105.2 : 100.
From the works of Hofacker (“Ueber die Eigenschaften welche
sich bei Menschen und Tieren von den Eltern auf die Nachkommen
vererben”—Concerning the Qualities transmitted from Parents
to Offspring in Men and Animals—Tuebingen, 1828) and Sadler
(“Law of Population,” London, 1830) conclusions have been drawn
regarding the effect of a variation in the age ratio of the parents
on the determination of sex. The deductions in question, known as
Hofacker and Sadler’s law, are as follows:
1. If the husband is older than the wife more boys are born than
girls.
4232. If husband and wife are the same age somewhat fewer boys
are born than girls.
3. If the wife is older than the husband the excess of female
births is larger still.
Hofacker’s actual figures were the following:
| Father younger than mother |
90.1 boys to 100 girls. |
| Father same age as mother |
93.3 boys to 100 girls. |
| Father 4 to 6 years older than mother |
108.8 boys to 100 girls. |
| Father 6 to 9 years older than mother |
124.7 boys to 100 girls. |
| Father 9 to 12 years older than mother |
143.7 boys to 100 girls. |
Sadler’s results were closely similar:
| Father younger than mother |
86 boys to 100 girls. |
| Father same age as mother |
94 boys to 100 girls. |
| Father 1 to 6 years older than mother |
103 boys to 100 girls. |
| Father 6 to 11 years older than mother |
126 boys to 100 girls. |
| Father 11 to 16 years older than mother |
147 boys to 100 girls. |
| Father 16 years and more older than mother |
163 boys to 100 girls. |
Goehlert found that the offspring of marriages in which the
husband was younger than the wife were 71 boys and 86 girls; of
marriages in which husband and wife were of the same age, 263
boys and 282 girls; and of marriages in which the husband was
older than the wife, 2,017 boys and 1,865 girls.
Wappaeus, combining the data supplied by these three investigators,
Hofacker, Sadler and Goehlert, obtained the following sexual
ratios for the entire 8,000 cases (i. e., the number of boys born to
each 100 girls born): When the husband was younger than the
wife, 88.2; when husband and wife were of the same age, 93.5;
when the husband was older than the wife, 113.0.
It will be observed that the mean sexual ratio of these 8,000
cases is 109.6; whilst, as we saw above, when a sufficiently large
number of instances is taken, the sexual ratio always closely approximates
to 106.3. From this it appears that the numbers dealt
with by Hofacker, Sadler and Goehlert in their investigations were
too small for the deduction of trustworthy averages.
The same criticism is applicable to the observations of Ahlfeld,
Breslau and Noirot, whose results conflict with those just given.
According to Ahlfeld, in the case of 1,376 births where the father
was at least 10 years older than the mother, the sexual ratio was
only 98.2. According to Noirot’s data, in cases in which the father
was older than the mother, this ratio was 99.7.
424Oesterlen gives the following brief summary of the researches
made for the establishment and confirmation of the law of Hofacker
and Sadler:
| Author. |
Father older than mother. |
Father and mother same age. |
Mother older than father. |
Sexual ratio. |
Number of instances. |
| Hofacker |
117.8 |
92.0 |
90.6 |
107.5 |
1,996 |
| Sadler |
121.4 |
94.8 |
86.5 |
114.7 |
2,008 |
| Goehlert |
108.2 |
93.3 |
82.6 |
105.3 |
4,584 |
| Noirot |
99.7 |
|
116.0 |
103.5 |
4,000 |
| Legoyt (Calais) |
109.9 |
107.9 |
101.6 |
107.9 |
6,006 |
| Legoyt (Paris) |
104.4 |
102.1 |
97.5 |
102.9 |
52,311 |
| Breslau |
103.9 |
103.1 |
117.6 |
106.6 |
8,084 |
The law of Hofacker and Sadler cannot be regarded as possessing
universal validity, although the figures on which it is based seem
to show pretty clearly that we are justified in regarding the mutual
interaction of the male and female reproductive elements at the
moment of fertilization as effective in the determination of sex.
In the investigations to which we have hitherto alluded it is only
the relative ages of husband and wife that have been taken into
account; but other researches have shown that the absolute age
alike of the husband and of the wife has an influence in the determination
of sex.
The influence of the absolute age of the mother in the determination
of sex has been very clearly established. Ahlfeld was the first
to draw attention to the fact that among the children of elderly
primiparæ there was always to be found an excess of boys, and
that there was an increase in this excess proportionate to the greater
age of the mother. Among 102 children born to primiparæ over
32 years of age the sexual ratio was 137 : 100; and a later investigation
made by the same author in conjunction with Schramm
showed that among 1,038 children born to primiparæ over 28 years
of age the sexual ratio was 124 : 100.
Hecker obtained similar results. Among 432 children born to
primiparæ over thirty years of age the sexual ratio was 133 : 100.
Winckel, dealing with primiparæ of the same ages, found a sexual
ratio of 136.8 : 100.
Düsing, examining the records of the lying-in hospitals of Leipzig,
425Dresden and Jena and thus obtaining a very large number of
instances whereon to base his conclusions, confirmed the view that
elderly primiparæ give birth to an excess of boys, and further that
the older they are the larger the excess of male births. He drew
up the following table:
| Age of primiparæ. |
Leipzig.
Boys. Girls. |
Dresden.
Boys. Girls. |
Jena.
Boys. Girls. |
Total Nos.
Boys. Girls. |
Sexual ratio. |
| 15 |
1 : − |
1 : 2 |
1 : − |
3 : 2 |
549 : 494
= 111.1 |
| 16 |
4 : 4 |
6 : 10 |
2 : 2 |
12 : 16 |
| 17 |
23 : 13 |
20 : 15 |
9 : 7 |
52 : 35 |
| 18 |
67 : 55 |
103 : 100 |
17 : 13 |
187 : 168 |
| 19 |
110 : 103 |
152 : 141 |
33 : 29 |
295 : 273 |
| 20 |
148 : 147 |
187 : 185 |
32 : 45 |
367 : 377 |
807 : 781
= 103.3 |
| 21 |
157 : 145 |
241 : 201 |
42 : 57 |
440 : 404 |
| 22 |
120 : 133 |
191 : 207 |
48 : 53 |
359 : 393 |
903 : 962
= 93.9 |
| 23 |
106 : 108 |
168 : 149 |
51 : 51 |
325 : 308 |
| 24 |
71 : 105 |
111 : 118 |
37 : 38 |
219 : 261 |
| 25 |
79 : 57 |
73 : 72 |
35 : 27 |
187 : 156 |
531 : 469
= 113.2 |
| 26 |
45 : 35 |
30 : 43 |
20 : 20 |
125 : 98 |
| 27 |
31 : 35 |
52 : 55 |
10 : 12 |
93 : 102 |
| 28 |
32 : 33 |
26 : 33 |
19 : 16 |
77 : 72 |
| 29 |
19 : 10 |
26 : 18 |
4 : 13 |
49 : 41 |
| 30 |
9 : 15 |
30 : 13 |
9 : 6 |
48 : 34 |
155 : 104
= 150.0 |
| 31 |
3 : 8 |
15 : 11 |
3 : 3 |
21 : 22 |
| 32 |
5 : 6 |
12 : 9 |
7 : 3 |
24 : 18 |
| 33 |
2 : 2 |
5 : 5 |
5 : 2 |
12 : 9 |
| 34 |
4 : − |
8 : 5 |
2 : − |
14 : 5 |
| 35 |
2 : − |
9 : 3 |
2 : 1 |
13 : 4 |
| 36 |
1 : − |
3 : 3 |
1 : 1 |
5 : 4 |
| 37 |
4 : 1 |
4 : 3 |
1 : − |
9 : 4 |
| 38 |
− : − |
− : 1 |
1 : − |
1 : 1 |
| 39 |
− : − |
4 : − |
1 : − |
5 : − |
| 40 |
1 : 1 |
2 : 1 |
1 : − |
4 : 2 |
| 41 |
− : − |
− : 1 |
− : − |
− : 1 |
As an explanation of this statistically proved fact, that elderly
primiparæ gave birth to a large excess of boys, Düsing suggests that
these women who conceive for the first time comparatively late in
life, are, prior to the conception, in a state corresponding with that
of a lower animal species suffering from a deficiency of males, and
for this reason exhibit a tendency to procreate a larger number of
individuals of the deficient sex. In multiparæ also it is possible to
trace the influence of a deficiency of male individuals. When there
is such a deficiency the interval between successive births is unduly
protracted. Düsing found (once more from the records of the
lying-in hospitals of Dresden, Leipzig and Jena) that the longer
426the interval between one parturition and the next the longer, that
is to say, the mother has had to wait for her next conception, the
greater is the excess of male births. Düsing therefore lays down
the law: “Delayed impregnation gives rise to an excess of male
births.”
| Age of primiparæ. |
Leipzig.
Boys. Girls. |
Dresden.
Boys. Girls. |
Jena.
Boys. Girls. |
Total Nos.
Boys. Girls. |
Sexual ratio. |
| 1 |
162 : 158 |
194 : 178 |
58 : 45 |
414 : 381 |
108.6 |
| 2 |
366 : 307 |
374 : 361 |
168 : 145 |
908 : 813 |
111.6 |
| 3 |
198 : 196 |
207 : 194 |
116 : 94 |
521 : 484 |
107.7 |
| 4 |
127 : 109 |
132 : 106 |
59 : 45 |
318 : 260 |
115.7 |
| 5 |
59 : 54 |
55 : 54 |
38 : 38 |
152 : 146 |
| 6 |
61 : 62 |
52 : 49 |
49 : 24 |
162 : 135 |
121.9 |
| 8, 9 and 10 |
18 : 16 |
41 : 23 |
16 : 24 |
75 : 63 |
| 11 and more |
5 : 15 |
12 : 9 |
4 : 6 |
41 : 30 |
| Totals: 4,903 births, 2,591 m.; 2,312 f.; sexual ratio = 112.06. |
Bidder considers that his own observations entitle him to modify
Ahlfeld’s dictum regarding the influence of age in primiparæ in
giving rise to an excess of male births. He tabulates his results
as follows:
| Age of Mother. |
Number of cases. |
Sexual ratio. |
| 17 to 20 |
80 |
122.2 |
| 20 to 22 |
405 |
130.1 |
| 22 to 24 |
369 |
109.9 |
| 24 to 26 |
1,138 |
104.6 |
| 26 to 30 |
2,049 |
105.5 |
| 30 to 32 |
878 |
112.5 |
| 32 to 36 |
1,120 |
119.6 |
| 36 to 39 |
676 |
123.1 |
| 40 and upward |
215 |
131.5 |
and formulates the following thesis: Very young primiparæ give
birth to an excess of boys; primiparæ in the first bloom of womanhood
give birth to an excess of girls; later, however, as the age
of the primiparæ increases the excess of male births soon reappears
and rapidly increases.
Hofacker’s data and the researches of Hampe agree with those
of Bidder in showing that to very young primiparæ, as well as to
427elderly primiparæ, an excess of boys is born. Among the offspring
of 363 mothers, at ages varying from 16 to 26 years, Hofacker
found the sexual ratio to be 121; among the offspring of 1,056
mothers, at ages 26 to 36, the ratio was 101; and among the offspring
of 567 mothers at ages 36 to 46, the ratio was 111. Hampe
tabulated 5,992 instances as follows:
| Age of Mother. |
Number of instances. |
Sexual ratio. |
| Below 20 years |
56 |
107.7 |
| 20 to 25 years |
871 |
90.6 |
| 25 to 30 years |
1,633 |
114.9 |
| 30 to 35 years |
1,631 |
108.3 |
| 35 to 40 years |
1,185 |
117.1 |
| Over 40 years |
616 |
124.0 |
We learn, therefore, that if the age of the progenitors is to be
regarded as one of the causes by which sex is determined, we must
take into consideration not only the relative ages of husband and
wife but, in addition, the absolute age of the wife.
Goehlert undertook a statistical investigation in which the absolute
age of the husband was taken into consideration as well as
that of the wife. From this it appeared that the maximum sexual
ratio was exhibited when the father was between the ages of 30
and 35 years. When the age of the mother is treated as the determining
influence, we find the maximum sexual ratio in the offspring
of mothers between the ages of 25 and 30 years. Goehlert
believes, however, that the paternal influence is more powerful than
the maternal in the determination of sex. The respective influences
are compared in the following table:
| Age of Father. |
Age of Mother. |
| 20 to 30 years. |
30 to 40 years. |
Over 40 years. |
Totals. |
| 25 to 35 years |
105.76 |
107.87 |
109.14 |
106.6 |
| 35 to 45 years |
102.8 |
105.1 |
105.3 |
104.7 |
| Over 45 years |
|
104.3 |
103.9 |
109.1 |
| In general |
105.25 |
105.97 |
104.9 |
105.5 |
428Geissler, studying the data obtainable regarding the sexual ratio
during a 10–year period in the Kingdom of Saxony, ascertained
that in families possessing two children or more there was a very
definite distribution of the possible sex-combinations. Where there
was an even number of children those families were in the majority
in which the number of boys and girls was identical. If the
number of children in the family is an unequal one, those combinations
are most frequent in which the number of boys exceeds the
number of girls by one; next in frequency are those combinations
reversed to this, i. e., in which the number of girls exceeds the
number of boys by one. All other combinations are comparatively
infrequent in proportion as the discrepancy in number between
boys and girls is larger. Rarest of all are families in which the
children are all of the same sex; and among these, again, the most
unusual are those consisting of boys only.
This distribution of the sex-combination is believed by Geissler
to depend upon the fact that in the first birth and all the subsequent
births there is generally speaking a slight advantage in
favour of the male sex. It has not been proved that the sex of
the first-born exercises a determining influence on the sex of the
subsequent children. It does, however, seem clear that in the case
of parents who have given birth in succession to several children
of one sex only, there exists some definite obstacle to the procreation
of children of the opposite sex. Putting these exceptions out of
consideration, there seems to exist a tendency in the later births
of a series toward the procreation, more especially of that sex
which has been absent or deficient in the earlier births of the series.
The strength of this equalizing tendency increases as soon as it has
for the first time manifest itself. It is always greater when
the sex deficient in the earlier births of the series has been the
male.
I have myself undertaken a statistical investigation of the births
occurring in the reigning families of Europe and in the families
of the leading members of the aristocracy. The necessary particulars
are to be obtained from the genealogical court calendars; and
it is my belief that the data obtained regarding these uppermost
strata of society are comparatively free from many sources of error
by which the ordinary statistics of the subject are apt to be invalidated.
For 556 marriages there were 1,972 births, comprising 1,023
boys and 949 girls, and thus exhibiting a sexual ratio of 107.7.
In relation to the relative ages of the parents, the following table
was drawn up:
| 429 |
|
Boys. |
Girls. |
Sexual ratio. |
| Husband older than wife by one to five years |
294 |
283 |
103.8 |
| Husband older than wife by more than five and less than ten years |
327 |
306 |
106.8 |
| Husband older than wife by more than ten and less than fifteen years |
190 |
167 |
113.7 |
| Husband older than wife by more than fifteen years |
138 |
113 |
122.1 |
| Husband same age as wife |
34 |
42 |
80.9 |
| Husband younger than wife |
40 |
38 |
105.2 |
From these figures we may deduce the following conclusions,
which are not wholly concordant with the law of Hofacker and
Sadler: When the husband is older than the wife the excess of
male births among the offspring is greater than it is in the case of
an average drawn from the offspring of all marriages (in my cases
the difference was 111.8 as compared with 107.7). But a closer
analysis shows the difference to be less simple than at first sight
appears. If the husband is older than the wife by one to five years,
the excess of male births among their offspring (103.8) is less
than in the average of all marriages (107.7); the same is true of
the offspring of marriages in which the husband is more than five
and less than ten years older than the wife, though the difference
here is very trifling (106.8 as compared with 107.7). It is not till
we come to the offspring of marriages in which the husband is
from ten to fifteen years older than the wife that the increase in
the excess of male births becomes notable (113.7 as compared with
107.7); and when the husband is more than fifteen years older than
the wife the excess of males is higher still (122.1).
If we arrange these data so as to show, in cases in which the
husband is older than the wife, the additional influence of the
absolute age of the wife, we obtain results which partially conflict
with those of Bidder, as follows:
| Husband Older than Wife. |
Boys. |
Girls. |
Sexual ratio. |
| Wife’s age, 15 to 20 years |
280 |
287 |
97.6 |
| Wife’s age, 20 to 26 years |
595 |
513 |
116.0 |
| Wife’s age, 26 to 33 years |
74 |
69 |
110.1 |
430Thus we see that when the wife is very young, i e., less than
twenty years of age, even though the husband is older than the wife,
there is among their offspring no excess of male births, but the
contrary—a sexual ratio of 97.6 only. Most marked is the excess
of boys in cases in which the husband is older than the wife, and
the age of the wife is from twenty to twenty-five years. When the
husband is older than the wife, and the wife’s age lies between
twenty-five and thirty-two years, the excess of male births is not
so great, though still considerable.
Hence it appears that the law of Hofacker and Sadler, which
cannot be regarded as fully valid in the terms in which it was
originally expressed, must be modified as follows: If the husband
is at least 10 years older than the wife, and the latter is at an age
when her reproductive capacity is at its maximum (twenty to twenty-five
years), the offspring exhibit a notable excess of male births.
There is still a considerable excess of male births in the offspring
of marriages in which the husband is at least ten years older than
the wife, and the wife is more than twenty-five years of age. On
the other hand fewer boys are born than girls as the offspring of
marriages in which, although the husband is older than the wife,
the wife has not yet attained the age of maximum reproductive
capacity—i. e., is less than twenty years of age. The excess of
female births is most marked when the husband and wife are of
the same age. When the wife is older than the husband there is
a moderate excess of male births.
I admit, however, that the figures upon which I have based these
conclusions are, like those of Hofacker, too few in number for the
foundation of trustworthy inferences. The instances in my computation
number 1,972; those in that of Hofacker, 1,996; but, as I
have already remarked, there are reasons for believing that the
data I have employed admit of the introduction of fewer sources
of error.
The influence of the absolute age of the mother in the determination
of sex having been statistically proved, many have inferred
that this determination is not effected during the instant of fertilization,
but occurs at a later stage of intra-uterine life, and is influenced
by the manner in which the embryo is nourished by the
maternal organism. It is suggested that elderly and immature
mothers are unable to furnish the embryo with nutriment so well
as those mothers who are at the age of maximum reproductive
capacity, and that upon this fact depends the excess of male births
431in the latter case. (We shall return to this matter—the influence
of deficient nutrition in relation to the excess of male births). But
the proof of the fact that the absolute age of the father has also
an influence in the determination of the sex of the offspring offers
a ground for opposing this assumption that the sex of the embryo
is determined during intra-uterine life subsequent to fertilization,
and suggests that the father also exercises a determining
influence in the origination of sex during the act of fertilization.
The absolute age of the husband seems also to have some influence
upon the sexual ratio. The absolute age, like the relative age,
of the father appears favourable to the procreation of a greater
excess of boys. Thus, Hofacker found in 1,193 cases, in which
the age of the father was from twenty-four to thirty-six years, that
the sexual ratio was 100; in 683 cases in which the age of the father
was from thirty-six to forty-eight years, the sexual ratio was 114;
and in 105 cases, in which the age of the father was from forty-eight
to sixty years, the sexual ratio was 169.
In investigations based upon larger collections of cases Schumann
and Düsing have endeavoured to determine the variation in the
sexual ratio according to the absolute age of the father.
Düsing examined the statistics of births in Norway, Alsace-Lorraine
and Berlin, and from the data thus obtained he compiled the
following table:
| Age of Mother. |
30 to 35 Years. |
25 to 30 Years. |
20 to 25 Years. |
| Age of Father. |
Boys. |
Girls. |
Sexual ratio. |
Boys. |
Girls. |
Sexual ratio. |
Boys. |
Girls. |
Sexual ratio. |
| 15 to 30 years |
8,525 |
7,887 |
108.1 |
27,389 |
25,843 |
106.0 |
21,560 |
20,330 |
106.0 |
| 30 to 35 years |
23,283 |
21,823 |
106.9 |
23,394 |
23,486 |
103.9 |
7,954 |
7,469 |
106.5 |
| 35 to 40 years |
17,885 |
17,070 |
104.7 |
10,272 |
9,838 |
104.2 |
2,426 |
2,416 |
100.4 |
| 40 to 45 years |
7,972 |
7,681 |
103.8 |
3,165 |
3,058 |
103.5 |
1,154 |
1,100 |
105.0 |
| Over 45 years |
4,220 |
3,997 |
105.6 |
1,734 |
1,525 |
113.8 |
In this table we find the births arranged in relation to varying
ages of the fathers and in relation to mothers whose ages are tabulated
in three classes, the ages of the latter being those at which
they are most prolific. The table shows clearly that the excess of
boys is larger at the beginning and at the end of each column.
Thus, the age of the mother remaining constant, young fathers and
elderly fathers procreate a larger proportion of boys than do fathers
of intermediate age.
432But I find in this table, which is based upon a very large number
of instances indeed, a confirmation of the thesis which I stated
above, for the highest sexual ratio of 113.8 is in this table found
in the case of fathers over forty-five years of age who are married
to mothers of ages twenty-five to thirty years; this is, as I said,
the case in which “the husband is at least ten years older than the
wife, and the latter is at the age at which her reproductive capacity
is at its maximum.”
From such figures as these, which seem to show the influence of
the absolute age of the father upon the determination of sex, it
has by many been inferred that the man exercises a preponderating
influence upon the determination of the sex of the embryo, impressing
his own sex upon it, and that the greater the sexual potency
of the begetter the more powerful also is the influence exercised
by the latter; that the point of first importance in this connection
is the sexual capacity of the man; and that the excess of male
births increases pari passu with the increase in the potency of the
procreating male.
Two additional considerations have been adduced to demonstrate
the influence of the father in determining the sex of the offspring.
The first of these is a comparison of the ratio between male and
female births in towns and in rural districts, respectively; and the
second is a comparison between the ratio of males to females in
the offspring of married and of unmarried parents, respectively.
In towns the excess of male births is smaller than it is in the
country. The average sexual ratio in Prussia during the five-year
period, 1875 to 1880, is given by Düsing as follows:
| In Berlin |
105.70 |
| In other large towns |
105.72 |
| In medium sized towns |
105.44 |
| In small towns |
106.17 |
| In rural districts |
106.62 |
The indisputable fact that in towns more girls are born than in
rural districts is referred to the fact that in the country the husband
usually enters on marriage with his virile powers completely
unimpaired, whereas in towns many men only marry after they
have for many years expended their best forces in irregular sexual
intercourse, and thus reserve for their wives only the dregs. But,
as we shall show presently, the difference between town and country
in this respect is susceptible of a different interpretation.
It has also been asserted (Horn) that extra-conjugal sexual intercourse
is favourable to the procreation of boys, the suggestion
433being that the greater sexual vigour in the former case determines
a preponderance of males in the offspring; but this assumption is
invalidated by the statistical evidence which now accumulates, that
among illegitimate offspring there is a smaller excess of boys than
among legitimate offspring. Babbage, for instance, came to this
conclusion as a result of the comparison of 1,000,000 illegitimate
births with 14,000,000 legitimate births. On the other hand, the
following utterance of Ploss appears extremely artificial: “In a
country in which illegitimate births are very numerous, in which
the illegitimate children are for the most part begotten by enervated
debauchees, the excess of male births is smaller; but in a country
in which the illegitimate births are less numerous, and in which the
illegitimate infants are for the most part the fruit of love and are
begotten by youthful lovers, the excess of male offspring is larger.”
Next to the age of the progenitors, their nutritive condition is
shown by statistical investigations to exercise an important influence
in the determination of sex. The following proposition has,
in fact, been established: Where the supply of nutriment is deficient,
the offspring contains an excessive proportion of boys.
Ploss, in an article on “The Causes of Variations in the Sexual
Ratio,” published in twelfth volume of the “Berliner geburtsh.
Monatsheft,” has collected a number of statistical data to demonstrate
that the determination of sex is principally dependent upon
the nutritive condition of the mother. In his opinion the determination
of the sex of the embryo depends neither upon the quality
of the ovum nor upon that of the spermatozoon, nor again upon
the reciprocal influences exerted by ovum and spermatozoon on
one another. During the earliest time after fertilization the embryo
is sexually neutral and only later, as a result of some new influence
acting upon it, does it receive an impulse toward the formation
either of the male or of the female sex. Among all the external
conditions which are capable during this period of exercising a
determinative influence the most important are the nutritive conditions,
for nutrition is the most important factor in determining
the form of the young animal, and most of the other outward
conditions, such as light, heat, and chemical changes, affect the
embryo in a mediate manner only, through the changes they are
respectively capable of inducing in its nutrition and metabolism.
But Ploss is not content with asserting that the nutritive condition
of the mother is of great importance in determining the sex of the
embryo; he goes further than this, and declares that it is scanty
434nutrition of the mother which especially gives rise to the birth of
males, whereas abundant nutrition of the mother tends to give rise
to the birth of females. He refers to observations made in respect
of other animals than man. St. Hilaire observed that among the
underfed animals in menageries there was an excess of male births.
Hofacker and Girou de Bazarcingues have noted similar phenomena
in the case of domestic animals; they found that when these were
richly fed they gave birth to an excess of females, but that when
they were poorly nourished they gave birth, on the contrary, to an
excess of males. Among sheep, with whom the number of male
and of female births is approximately identical, Martegoute found
that those animals which had given birth to female lambs had on the
average a greater weight than those ewes which had given birth to
male lambs. During the period of lactation, also, the former lost
weight more than the latter.
When Ploss had further ascertained that among those engaged
in the fur-trade it is the established belief that from fruitful regions
the skins chiefly of female animals will be obtained, but from barren
regions, on the other hand, among the skins obtained those of male
animals will preponderate, it appeared to him that he was justified
in drawing the conclusion that among the mammalia a well-nourished
mother, one capable of providing abundant nutriment for
her offspring, is, on the whole, more likely to give birth to a female
than to a male, and conversely. He then endeavoured, by reference
to the statistics of population, to show that in the case of
human beings also, when the mother is exceptionally well nourished,
there is especial likelihood of a girl being born; whereas when the
mother is ill nourished she is more likely to give birth to a boy—odd
as it may seem, at first sight, that a rich diet should determine
the production of the so-called less powerful sex, the female; and
conversely. (Ploss, be it noted however, denies that male new-born
infants are more powerful than female.) The fact that in
the country, comparatively speaking, many more boys are born than
in towns (vide supra) is explained by Ploss as dependent on the
fact that townswomen are on the whole better nourished than the
countrywomen, owing to the greater consumption of meat by the
former.
The circumstance again (likewise alluded to above), that in the
case of illegitimate births almost always the excess of male births
is less marked than in the case of the offspring of legal unions, is
regarded by Ploss as offering further proof of the influence of
435nutritive conditions upon the determination of sex. Illegitimate
mothers are on the average women at the very best age for child-bearing,
women who have worked vigorously, are themselves well
nourished, and are therefore better able to nourish their unborn
offspring than (on the average) married women. Further, it is
a remarkable fact that in Saxony, regions of which the elevation
above the sea-level is less than 1,000 feet, produce comparatively
more girls than regions at an altitude of 1,000 to 2,000 feet above
the sea. This Ploss refers to the worse nutrition of the women
living at the higher altitude, for the fact is well known that the
higher we go above the sea the less fertile is the soil and the more
limited is its produce.
Starting from the view that the lower classes of the population
are in good years better nourished than they are in bad years,
Ploss compared statistically the rise and fall of the prices of
foodstuffs, in Saxony, with the variations of the sexual ratio in the
same kingdom; and he found, in correspondence with his theory,
that in bad times there was a greater excess of male births than
there was during periods in which food was cheaper. Moreover,
the consumption of meat appeared to have more influence upon the
variations in the sexual ratio than was exercised by the consumption
of vegetable foodstuffs. Ploss endeavoured to show graphically
that with an increase in the price of provisions there corresponded
an increase in the excess of male births, and vice versa.
That after times of great wars, pestilence, and emigration, in
which the male portion of the population has been decimated,
there occurs a notable increase in the excess of male births, is explained
by Ploss by the assumption that in consequence of the
deficiency of male labour, the general supply of provisions is deficient,
just as it is after years of bad harvests; hence, in consequence
of the scanty nutrition of the mothers, the number of female
births is depressed and the number of male births increases. Those
countries which in general possess a more thriving population, such
as Saxony, England, Belgium, Prussia, etc., exhibit a smaller excess
of male births when compared with those countries in which a more
widespread poverty exists, such as Russia, Lombardy, Bohemia,
and even France. With increasing prosperity, fruitfulness increases,
and there is an increase also in the proportion of female
births.
These views of Ploss’s are, however, rightly contested by Breslau
and Wappaeus.
436Breslau (“The Causes of the Determination of Sex”) offers in
the first place theoretical objections to the view that nutritive conditions
in the mother are determinative in the production of the sex
of the offspring; and he then proceeds to quote statistical data
which are opposed to any such theory. He rightly insists, in the
first place, that, inasmuch as it is unquestionable that in the act of
fertilization the spermatozoon induces in the ovum certain changes,
the effect of which is manifested in days far later than those of
intra-uterine life, by the production of the most manifold and various
somatic and psychical resemblances to the father, it is obvious
that this single occurrence of the fusion of the spermatozoon, the
bearer of the paternal influences, with the ovum is competent to
induce in the ovum a molecular arrangement upon which the determination
of sex may be supposed to depend—it is not necessary
to suppose that for this determination, repeated actions, or a
prolonged period of time, is requisite.
In this connection a reference to birds is instructive, for in this
division of the animal kingdom we seem absolutely compelled to
assume that the sex of the offspring is irrevocably determined in the
moment of fertilization. “In birds, who lay an egg every day,
eggs which are kept all at the same temperature during the period
of incubation, and some of which develop into cock and others into
hen birds—how is it possible to imagine that the nutritive condition
of the parent is determinative of the sex of the offspring,
since this nutritive condition cannot reasonably be supposed to
change to any notable extent from one day to the next and then
back again?”
The paternal influence in the determination of sex is regarded
by Breslau as likely to be at least as important as that exercised
by the mother. Unquestionably the semen is subject to certain
variations in quality and in quantity, and it is possible that these
variations may make themselves felt in the subsequent development
of the embryo. Of the semen, as of all secretions, we can assume
with some probability that in certain conditions (conditions which
are, indeed, but little understood), it may exhibit a greater or less
intensity in its stimulating qualities, and that in this way it may be
subject to changes, according to which it will tend to influence the
development of the embryo, now in the female, and now in the
male direction. Again, in view of the continued interchange of
nutritive materials between the embryo and the maternal organism,
437it is probable enough that the constitution of the maternal organism
and likewise that of the ovum, at the moment of fertilization, are
not matters of indifference to the determination of sex. But to
attribute to the nutritive condition of the maternal organism the
sole or even the principal influence in the determination of the sex
is an unjustifiable assumption.
The proofs alleged by Ploss from the animal world in support of
his thesis, viz., that in the case of poorly nourished animals there is
a marked excess of male offspring, are justly controverted by
Breslau with the remark that the observations on animals are but
few in number, and further that we know nothing whatever regarding
the normal sexual ratios among the offspring of such animals
as lions, tigers, hyænas, bears, etc., in the free state.
If, again, domestic animals when well nourished give birth to an
excess of female offspring, and when ill nourished and overworked
to an excess of male offspring, in the former case we can only regard
the excess of female births as a pathological phenomenon, inasmuch
as a superabundant supply of nutriment is not that which furnishes
the highest powers or is most suited to the preservation of life.
Again, the accounts given by fur-dealers are quite untrustworthy,
since these men commonly obtain their goods at third and fourth
hand; moreover, most of the animals whose pelts form articles of
commerce, are beasts of prey, such as the otter, the lynx, the bear,
the wolf, the fox, etc.—and these animals have no “pasturage.”
Among vegetable-feeding animals the females are no doubt found
on the pasturage more often than the males, for the reason that the
females have to nourish both themselves and their young, whereas
the males, which have themselves only to provide for, are contented
with less food and inhabit chiefly more retired and less fertile
regions; they are also shyer and are less easily shot and trapped.
Regarding statistical data relating to the influence of nutrition on
the production of boys, Breslau shows, from the figures of the
Canton of Zurich, that with few exceptions, the years in which the
price of corn was lowest were the years in which the production of
boys was greatest, and vice versa—the exact opposite of the results
obtained by Ploss from his examination of the figures relating
to births and the price of provisions in Saxony.
Wappaeus contests the conclusions of Ploss even more vigorously,
and adduces the statistics of Sweden in the 20–year period 1770
to 1790, in which period this kingdom repeatedly suffered from
438famine in consequence of failure of the crops, so that the births and
deaths were largely affected. It appeared, however, that the more
abundant or more scanty nutrition of the inhabitants of Sweden
during this period had no marked influence upon the sexual ratio.
If scanty nutrition of the mother had, in fact, any influence upon
the determination of the sex of the embryo in the direction alleged
by Ploss, viz., so as to bring about the birth of a greater excess
of boys, this influence should be manifested with exceptional
clearness in the case of twins, for it is obvious that the nutriment
that is insufficient for one embryo would be still scantier for two.
Hence various statistical investigations have been undertaken to determine
the sexual ratio in the case of twin births. Ploss found
that in Saxony, in the case of 23,420 twin births, the sexual ratio
was 106.7 boys to 100 girls; Moser gives the sexual ratio in the
case of twin births as 106; Meckel von Hemsbach gives it as 105.4;
Hecker, 116 and 122; Sickel, 112.3. Düsing combined the figures
relating to twin births in various lying-in hospitals, published by
Hecker, Sickel, Baillarger, Siebold, Elsässer, and Levy, respectively,
and thus obtained a sexual ratio of 121.5 boys to 100 girls. This
excess of boys is notably greater than among births in general.
But other statistical data are available which show a reversed
condition, viz., that in the case of twin births the sexual ratio is
lower than usual. According to von Frick’s collection of twin
births in Prussia, the sexual ratio was 104.7 boys to 100 girls;
whereas in the case of single births in the same country the sexual
ratio was 106.35 to 100. Riecke, in Württemberg, in the case of 60
twin births found 58 boys and 62 girls. In the case of twin births
observed by Braun, Chiari, and Späth, 94 in all, the children were
in 64 of these of identical sexes, namely, in 30 instances boys, and
in 34 instances girls. According to Breslau, in the case of twin
births in the Canton Zurich, the sexual ratio was 104.1 to 100;
whereas in the case of single births the sexual ratio was 106.2
to 100.
As regards triplets the reports of the sexual ratio vary from
111.76 : 100 (Meckel von Hemsbach) to 104.55 : 100 (Neefe).
It is obvious that the statistical data at present available regarding
the sexual ratio in the case of multiple births are far too
variable for it to be possible to base upon them any valid conclusions
as to the influence of the nutritive condition of the mother
upon the determination of the sex of the offspring. And taken as a
439whole the statistical data hitherto available do not enable us to infer
with confidence that nutritive conditions, and more especially the
nutritive state of the maternal organism, exercise any effect upon
the determination of the sex of the offspring.
Another attempt at the utilization of statistics has been to ascertain
whether the time of fertilization in relation to menstruation,
(in the first days after the flow, or later in the intermenstrual interval)
has any influence upon the determination of sex. The
starting point in this investigation was the earlier view that sex
depends upon the state of the ovum, and the belief that a very
favourable state of ovum and sperm favours the production of the
female sex. The ovum, after its discharge from the ovary, like
the spermatozoon after its discharge from the testicle, tends sooner
or later toward death, and the only thing that can save either from
this ultimate fate, is for the two to unite to form a new organism.
Precisely what moment in the history of the detached ovum is the
most favourable, is a matter regarding which we have no exact
information, but it is probable that at the moment of its discharge
from the ruptured follicle, it is at the zenith of its vital powers.
On this theory the determination of sex depends upon the period at
which, after its liberation from the follicle, the ovum encounters
a spermatozoon; the ovum which is fertilized early in its career
becomes a female embryo; the ovum, on the other hand, which is
not fertilized until it has become comparatively old, becomes a male
embryo. But, as Hensen points out, a spermatozoon, according to
its condition, may either fail sufficiently to fortify an ovum which
itself is in good condition; or, on the other hand, a powerful
spermatozoon may fortify an ovum of deficient vitality. But it is
difficult to say precisely on what considerations the greater or less
vitality of the spermatozoon depends—or, to speak more in accordance
with the terms of the theory, we do not know exactly what
makes it a good spermatozoon or the reverse. It may be “bad,”
either because it has remained too long in the testicle or because it
has been discharged too quickly, is too recently secreted; moreover,
a long sojourn of the spermatozoon in the uterus will doubtless
suffice to lower its vitality.
The Jews, more especially, whose religious ordinances forbid
them to have sexual intercourse either during or shortly after menstruation,
and among whom there is a great excess of male births,
have been adduced as a proof of the thesis that sexual intercourse
440during the later part of the intermenstrual interval tends to favour
the procreation of boys. In Leviticus xv. 19, we read: “And if
a woman have an issue, and her issue in her flesh be blood, she
shall be put apart seven days.” From the commentary in the Talmud
it appears that these seven days are to be reckoned from the
commencement of the flow. Statistical reports from various countries
show that among the Jews there is a greater excess of male
births than among the other inhabitants of the respective countries.
The overplus of male births exhibited by the Jews varies from 1
to 15%, the difference probably depending on the fact that the number
of instances under consideration is too small for uniform
results to be possible. In Prussia, during the period 1820 to
1834, the sexual ratio among the Jewish births was 111 : 100; during
the period 1849 to 1852 it was 106 : 100; in Hungary during
the period 1835 to 1855 it was 117.1 : 100; in Sweden, 1851 to 1855,
it was 108 : 100. Among illegitimate children of the Jewish community
the sexual ratio was, in Austria, 123.9, in Prussia, 118.6.
Fürst, examining the cases in von Braun’s clinic, and making a
statistical collection of the days of conception and of delivery, has
endeavoured to prove that “there is an excess of boys when conception
occurs during the period of post-menstrual anæmia.” His
figures show, in fact, a very notable excess of boys in cases in
which conception has occurred during the five days immediately following
the cessation the menstrual flow; and an excess of girls
when conception has occurred during the later part of the intermenstrual
interval. Thus, in the former case the excess of boys
is represented by the figures 37 : 12; in the latter case the excess of
girls is represented by the figures 79 (girls) : 65 (boys). These
figures are explained by Fürst on the theory that in the human
species conception during the period of post-menstrual anæmia
probably leads to an enormous excess of male conceptions (owing
to the fact that the unfertilized ovum is badly nourished during the
days just before conception); whereas in the later part of the
intermenstrual interval the better nourishment of the ovum probably
leads to the procreation of an excess of girls—hypotheses
which are based on a quite inadequate number of instances. Fürst
gives the following table:
| 441 |
| Number of Days Between Reputed End of Menstruation and Reputed Occurrence of Conception. |
Number of boys born. |
Number of girls born. |
Boys and girls together. |
| 1 |
7 |
1 |
8 |
| 2 |
6 |
3 |
9 |
| 3 |
9 |
5 |
14 |
| 4 |
15 |
3 |
18 |
| 5 |
3 |
6 |
9 |
| 6 |
5 |
6 |
11 |
| 7 |
6 |
5 |
11 |
| 8 |
2 |
8 |
10 |
| 9 |
4 |
5 |
9 |
| 10 |
6 |
4 |
10 |
| 11 |
6 |
5 |
11 |
| 12 |
3 |
6 |
9 |
| 13 |
4 |
5 |
9 |
| 14 |
6 |
5 |
13 |
| 15 |
1 |
2 |
3 |
| 16 |
2 |
5 |
7 |
| 17 |
2 |
3 |
5 |
| 18 |
3 |
|
3 |
| 19 |
1 |
3 |
4 |
| 20 |
1 |
2 |
2 |
| 21 |
1 |
1 |
2 |
| 22 |
4 |
1 |
5 |
| 23 |
|
1 |
1 |
| 24 |
1 |
|
1 |
| 25 |
|
2 |
2 |
| 26 |
2 |
|
2 |
| 27 |
|
1 |
1 |
| 28 |
1 |
1 |
2 |
| 31 |
1 |
|
1 |
| |
102 |
91 |
193 |
Baust gives a report, based, he says, upon “thoroughly trustworthy
data,” furnished by personal friends, regarding 14 cases,
which show, in his opinion, that every conception occurring in a
week after the cessation of the menstrual flow leads to the birth of
a girl; but that when conception occurs on the fifth or sixth day
after menstruation the result varies as regard sex. Swift, from
a report of 20 cases, draws the conclusion that in the intermenstrual
interval, boys, in the latter part of the interval girls are conceived.
The influence of the strength of menstruation upon the determination
of sex has also been studied by the statistical method, starting
with the idea that menstruation, in proportion to its strength,
affords on the average a measure for the subsequent nutrition of
the embryo, and this nutrition is further supposed to determine the
442sex. Düsing therefore arranged the births occurring in the lying-in
hospitals of Dresden, Leipzig and Jena, according to the information
given regarding menstruation in the clinical history of each
case; it appeared that when menstruation was comparatively scanty,
there was a greater excess of boys than when menstruation was
comparatively abundant. The actual figures were the following:
|
Abundant menstruation. |
Scanty menstruation. |
| Dresden |
902 |
847 |
495 |
431 |
| Jena |
66 |
69 |
56 |
45 |
| Leipzig |
21 |
22 |
239 |
211 |
| Totals |
989 |
938 |
790 |
687 |
| Sexual ratio |
105.4 |
114.7 |
Here also we may append the figures obtained by Düsing regarding
the births of foals at the Prussian stud-farms, which he
regards as supporting his view that by natural selection all animals
have acquired the faculty, whenever stronger demands are made
upon their sexual capacity, of procreating a larger number of
individuals of their own sex. In the tables we learn how many
mares on an average a stallion had covered in each year, that is,
we learn how great were the demands made upon the sexual capacity
of the stallion in that particular breeding stable in that year.
The figures relating to the years 1859 to 1892 were tabulated and
averages were drawn with the following results:
| Number of Mares Served. |
Number of Foals Born. |
Sexual ratio. |
| Colts. |
Fillies. |
| 60–70 |
42,445 |
41,933 |
101.22 |
| 55–59 |
56,511 |
66,226 |
100.49 |
| 50–54 |
59,940 |
61,096 |
98.18 |
| 45–49 |
57,077 |
59,216 |
96.39 |
| 40–44 |
59,967 |
62,007 |
96.71 |
| 35–39 |
38,348 |
40,181 |
95.44 |
| 20–34 |
26,354 |
27,069 |
97.35 |
443From these figures, which relate a very large number of instances
indeed, we learn that when greater demands are made upon the
stallion, more males are procreated. In fact, except for two slight
divergencies, the rise in the sexual ratio proceeds strictly pari passu
with the increase in the number of mares covered.
I must, however, draw attention to the fact that this assumption
when applied to the human species, that the man on whom whose
sexual capacity especially extensive demands are made, procreates
an especially large number of male children, is not confirmed by the
sexual ratio among the offspring of polygamous marriages in
which unquestionably greater demands are made upon the husband’s
sexual powers than is the case in monogamic unions.
The reports of travellers of earlier days, to the effect that in
Oriental countries more girls are born than boys, have recently
been confirmed by several observers. Campbell states that in the
harems of Siam the number of boys and girls born is equal.
Clarke states that among the Mohammedan Indians more girls are
born than boys. According to McLennan Indian experience teaches
us that where polyandry prevails male offspring predominate in
numbers; but where polygamy prevails there is, on the contrary,
an excess of female infants. The following data collected by
Goehlert from historical reports and from genealogical writings,
regarding the progeny of notable persons living in polygamous
unions, show certainly a large excess of female offspring over male:
|
Children. |
Sexual ratio. |
| Male. |
Female. |
| Morocco: Muley Scherif |
24 |
124 |
19.4 |
| Palestine: Rehoboam, King of the Jews |
28 |
60 |
46.6 |
| Arabia: Imon of Sana |
14 |
74 |
18.9 |
| Turkey: nine sultans |
110 |
128 |
85.9 |
According to Tousenel, love marriages give rise to more daughters
than sons, whereas among the offspring of conventional or
compulsory marriages, male children predominate. Further, among
the offspring of legitimate unions, the excess of males is greater
than among the offspring of illegitimate unions. A physician, V. J.
Cook, maintains that boys are procreated in the evenings (before
444midnight), but girls during the early morning hours—at which
latter time women are less “impressionable” than during the evening
hours.
Düsing, starting from the common belief that all animals have the
faculty, when there is a lack of individuals of one sex, of procreating
an excess of offspring of the sex which is deficient and
thus of restoring the balance between the sexes, maintains that
numerous factors, through the co-operation of which the sexual
ratio is regulated, act in temporal succession. He shows that the
individuality of the mother has an influence upon the sex. But
this finds expression through the qualitative constitution of the
ovum; hence already before fertilization there must exist a tendency
toward the development of one sex or the other—for example,
younger ova tend to become females; older ova, on the contrary,
to become males. It has further been shown that the individuality
of the father, that is to say, the qualitative constitution of the
sperm, has an influence in the determination of sex. Thus, by
means of the influence of the sperm, the already-mentioned pre-existing
tendency of the ovum can in some instances be counteracted
and overpowered. The influences in the personality of the father
and of the mother, which during fertilization find expression in the
qualitative constitution of the sperm and of the ovum, respectively,
can thus bring about a resultant tendency, acting in one direction
or the other with varying force. Thus, after fertilization, we have
this resultant tendency toward the formation of a male or female
embryo.
But, Düsing continues, at this time the sex is not definitely determined.
The influence of the nutritive condition in which the
fertilized ovum finds itself has yet to make itself felt. This influence
on the determination of sex through the maternal nutrition,
continues (in the human embryo) for as long as three months, but
even when the reproductive organs of the embryo have definitely
begun to diverge in the direction of the masculine or the feminine
type, as the case may be, some nutritive influence, if it is sufficiently
powerful, may yet turn the balance in the other direction, so that a
partial or complete hermaphrodite results, a being uniting the characteristics
of both sexes.
Actual inheritance of sex, of which people used to speak, cannot,
in Düsing’s opinion, possibly occur. The mode in which one sex
or the other develops is indeed inherited; but the decision which
sex shall develop does not depend upon inheritance, but is determined
445by the co-operation of several outward influences. The
qualities by which this is effected are acquired by adaptation to
general or special vital conditions.
Wilckens (“A study of the Sexual Ratio and of the Causes of the
Determination of Sex in Domestic Animals”) opposes the views
of Düsing, on account of the results of his own investigations, relating
to the births of 30,000 domestic animals. He formed the
following conclusions:
1. Locality (soil and climate) has an influence upon the sexual
ratio and upon the determination of sex in domestic animals, but
this influence is probably indirect only, being exerted through the
intermediation of the nutrition of the embryo in utero.
2. The season in which the domestic animal is conceived affects
the sex; the hot season favours the production of males, the cold
season that of females; in the hot season, in general, the appetite
and nutrition of domestic animals diminish, whereas in the cold
season these increase.
3. Regarding the male progenitor, neither his age, nor his sexual
energy, nor the demand made upon that energy, nor the age of the
semen, has any influence upon the sexual ratio or the determination
of the sex of the offspring.
4. The age of the female progenitor influences the sexual ratio
and the determination of the sex of the offspring in this way, that
in general, primiparæ and young mothers conceive a larger number
of female offspring. This influence of age may be referred to the
fact that in general young mothers nourish their offspring in utero
better than older mothers.
5. The nutrition of the fruit in utero influences the determination
of sex, speaking generally, in the following way, that better nutrition
favours the determination of the female sex, worse nutrition
favours the determination of the male sex.
6. In addition to the influence of nutrition of the fruit upon the
determination of sex, other influences, whose nature still remains
obscure, must also co-operate, because one and the same progenitor
in similar nutritive conditions does not always procreate offspring
of the same sex.
7. Owing to the operation of these unknown influences, prediction
of the sex of the offspring, and voluntary determination of the
sex of the offspring, remain impossible. All we can say is that
there is some probability that young and well-nourished mothers
will procreate a comparatively larger number of female offspring,
446whilst elderly and ill-nourished mothers will procreate a comparatively
larger number of male offspring.
II. Anatomical Investigations.
Of anatomical investigations and discoveries, those more
especially relating to the sex-relationships of twins and triplets have
been applied to the elucidation of the problem of the determination
of sex.
The first and most important fact in this connection, one that is
not merely a rule confirmed again and again by anatomists and
gynecologists, but is further, as Mayrhofer has demonstrated as a
result of his researches in von Braun’s clinic, a “natural law,” is
this, that twins and triplets enclosed in a common chorion are
invariably of the same sex. The sex-identity of such twins has
been referred to the similarity of their nutritive conditions
(Leuckart, Ploss), and more especially to the communication between
their bloodvessels; and an intimate connection between these
relationships and the determination of sex has been believed to
exist.
Mayrhofer, however, opposes this assumption by the following
deductions (“The Determination of Sex in the Human Species”);
“Fœtuses enclosed within a single chorion always possess a common
placenta, in which the blood-channels from both umbilical cords
frequently, in the case of twins perhaps invariably, communicate.
It might therefore be supposed that the sex-identity of embryos
enclosed within a single chorion is due to the intermixture of their
blood in the placenta. Hyrtl, however, describes a triplet’s placenta,
in which, though all three fœtuses were enclosed within a single
chorion, the vessels passing to the umbilical cord of one of the
fœtuses were entirely distinct from the vascular area common to
the two other fœtuses; it is therefore probable that in the case also
of twins enclosed within a single chorion there is not necessarily
any communication between their bloodvessels in the common
placenta. But even if it were proved that in the case of twins enclosed
within a single chorion their bloodvessels always do communicate
in the common placenta, we could not therefore infer that
the intermixture of the blood of the two fœtuses is the cause of
their sexual identity.
“For the intermixture of the blood of the two fœtuses in the
common placenta could never lead to a complete identity in the
composition of the blood of the two; it could only lead to a diminution
447of the differences which would exist between the bloods if
their placental circulations were entirely distinct, and the similarity
in the bloods thus established could not be expected to do more
than make it a general rule that such twins or triplets should be
of the same sex; but to this rule exceptions might be expected to
occur in certain cases, as when hæmatopoiesis in the two (or three)
fœtuses was very different, or when the circulation through the
intercommunicating bloodvessels was interfered with through the
pressure of fibrinous deposits—differences between the bloods
would then arise sufficient to cause differences in sex (if identical
composition of the bloods is presumed to be the cause of the sexual
identity).
“Experience teaches us that the existence of communicating vessels
in the placenta does not suffice to induce a close similarity of
growth and of the formation of the organs in twin fœtuses; nor
does it prevent the illness and death of one fœtus leaving the health
of the other undisturbed, although the communicating channels remain
open; so that, if we except acardiac monsters, it is correct to
say that each fœtus pursues a secluded life, uninfluenced by the
life of its neighbour. Acardiac monsters, on the other hand, always
receive blood which has already served for the nutrition of the
normal fœtus, and the result of this is an arrested development
and a striking preponderance of connective tissue in the acardiac
twin. But notwithstanding the fact that the failure of its own
proper circulation (which is indeed rendered possible by the existence
of the communicating vessels in the placenta) leads to its defective
nutrition with a blood inferior to that supplied to the normal
fœtus, the acardiac monster is always of the same sex as the normal
twin.”
From these considerations Mayrhofer rightly infers that the
identity of sex of two fœtuses contained in a single chorion, since
it does not depend upon the existence of communicating vessels in
the placenta, must arise from a developmental tendency already
existing in the two germs at the time of conception—or, in other
words, that at the time of conception their sex is already inalterably
determined.
This conclusion with respect to the sex of twins contained in a
single chorion may very readily be extended to the inference that
in the case of all human fœtuses the sex is already determined at
the time of conception.
Another anatomical fact is that many twins are contained in a
448single chorion for this reason, that they originate from two germinal
vesicles within a single ovum. It is an open question whether it is
not possible for two embryos contained in separate chorions to
come to lie in a single chorion through atrophy of the intermediate
wall. If this is indeed possible, the invariable identity of sex in
the case of fœtuses lying in a single chorion must lead us to agree
with Mayrhofer in inferring that two ova lying within a single
follicle, simultaneously fertilized, give rise to embryos of identical
sex.
B. S. Schultze and Ahlfeld, as a result of the investigations regarding
twins, also came to the conclusion that the sexual identity
of twins depends upon their derivation from a single ovum. If, in
accordance with what has been said above, an explanation of the
sexual identity of certain twins is to be found in the fact that for
such twins there has been a single conception only, and hence the
influence, whatever it may be, by which sex is determined acts on
both germs at the same time—still the sexual identity of twins in
general is remarkable and has not yet been fully explained. The
sexual identity in fact occurs much more frequently than appears
to correspond to the percentage of twins derived from a single
ovum. Von Fricks examined the data relating to multiple births
in Prussia during the period of 1826 to 1879 and compiled the
following table:
| Per Cent. |
Twins. |
Triplets. |
Quadruplets. |
Quintuplets. |
| Boys only |
32.6 |
24.5 |
14.3 |
33.3 |
| Girls only |
30.3 |
22.5 |
19.4 |
|
| Boys and girls |
37.1 |
53.0 |
66.3 |
66.7 |
| |
2 B. 1 G. |
28.5 |
|
|
| |
1 B. 2 G. |
24.5 |
|
|
| |
|
2 B. 2 G. |
23.4 |
|
| |
|
3 B. 1 G. |
19.5 |
|
| |
|
1 B. 3 G. |
23.4 |
|
| |
|
|
4 B. 1 G. |
33.3 |
| |
|
|
3 B. 2 G. |
33.3 |
According to Ahlfeld, of twin births in general, the ratio of those
with a common chorion to those with separate chorions is 1 : 8.15.
If, however, we wished to explain the frequency with which twins
449are of identical sex from the occurrence of such twins derived from
a single ovum, we should expect to find a very different ratio,
namely, 1 : 3.84; that is to say, twins with a common chorion would
have to be nearly three times as common as they actually are.
From these facts Düsing endeavours to draw the conclusion that
external conditions have an influence upon the determination of
sex, for very many external conditions are identical in the case of
twins; as, for instance, the age of the father, the age of the mother,
the nutritive conditions of the ova and of the spermatozoa, the
nutrition of the embryo, etc.—all of these would influence both the
twins in the same direction. A difference in the sex of twins, on
the other hand, might be due to two successive fertilizations.
B. S. Schultze has been led by his embryological studies to the
conclusion that there are male and female ova. Thus he believes
that sexually identical twins originate from a single ovum with two
germinal vesicles, thus assuming that a double fertilization of such
ova is possible. But since in such cases the sexes of the resulting
twins are always identical the spermatozoon can have no influence
upon the determination of sex, but the conditions leading to the
development of one sex or the other must pre-exist in the ovum—i. e.,
there must be male and female ova.
That as a matter of actual fact in some cases the female progenitor
exercises an overwhelming influence on the determination of
sex, and that the opinion held by so many that this determination
depends upon the mother alone is sometimes supported by facts, is
shown by the incident recorded by Darwin (“Descent of Man,”
Vol. I.), that an Arab mare was delivered seven times successively
of a filly, never of a colt, although she was covered by seven different
stallions. On the other hand, the circumstance, if it is not to
be attributed to pure chance, can also be explained by the constitutional
vigour of this mare (Hensen) without adopting the above
hypothesis.
Recently Upjohn has maintained that there are two kinds of
spermatozoa, male and female; the latter are the commonest, but
the former are the more energetic.
An interesting anatomical fact bearing upon this question has
been discovered by M. Nussbaum, namely, that in ascaris megalocephala
the reproductive glands are indicated already before the
separation of the germinal layers; and Nussbaum suggests that this
is also the case in all animals, although the proof cannot be obtained
in every instance.
450Semper has shown also in the case of some of the plagiostomata
that long before the beginning of the definitive development of the
reproductive organs, the apparently hermaphrodite embryo already
possesses at least the tendency toward the constitution of one sex
or the other. For in these animals, at a time so early that as yet
the reproductive glands exhibit no sexual differentiation whatever,
the sexes can nevertheless be distinguished by what appears to be a
secondary sexual character. In the female, namely, one ovary only
is developed; and very early indeed in the embryos destined to
become females we can observe an asymmetrical development of
the two germinal furrows. By this characteristic the two sexes can
be distinguished far earlier than it is possible to do so by the recognition
of a histological differentiation of the reproductive glands.
According to Mayrhofer the prepotency of the male gives rise
to the procreation of an excess of males in this way, that physical
prosperity of the male probably leads to the generation of boys,
whereas prosperity of the female tends to give rise to the generation
of girls. Moreover, economizing of the semen by infrequent
sexual intercourse tends to originate offspring of the male sex. In
this connection Hensen remarks, apropos of the greater excess of
male offspring among the Jews: “We might ask whether, in consequence
of the comparative sexual continence of the Jews which
demands a definite power of endurance on the part of the ova,
there may not be effected a certain selection of the ova; and thus
we may perhaps explain how it is that in this race an exceptional
vigour is somewhat more often to be observed than in other races.”
Bock assumes that “thinner semen,” such as results from more
frequent sexual intercourse, favours the procreation of the female
sex, whereas when intercourse is less frequent a larger number of
boys is likely to be born. Janke indicates as two important fundamental
principles of scientific physiology that, (1) sexual intercourse
represents as it were a contest between the two parties to
the sexual act as to which shall transmit his or her sexual influence
to the child, the victor in the contest determining the sex of the
offspring, and (2) that a crossed inheritance occurs, inasmuch as
whichever progenitor proves stronger in this contest transmits to
the child the sex other than his or her own. He therefore advises
women who long to have a boy to drink a glass of champagne before
fulfilling their conjugal duties in order to gain increased sexual
vigour.
Fiquet also expresses the opinion that when a vigorous, passionate,
451and sanguine male progenitor has intercourse with a frigid and
phlegmatic woman there will be a preponderant tendency for the
offspring to be female; whereas, when the conditions are the opposite
of these, the male progenitor being phlegmatic and cold, the
female on the contrary sanguine, passionate, and ardent, the offspring
will probably be of the male sex.
In opposition to these opinions of Fiquet and Janke, to the effect
that the temperament and the sexual vigour of the progenitors have
a determining influence in the origination of the sex of the offspring,
Düsing insists that the quality of the reproductive products
are alone influential. Düsing lays down the following proposition:
“The greater the scarcity of individuals of one sex is, the more
extensive consequently the demands made upon the sexual capacities
of the individuals of that sex, the more rapidly their reproductive
products are employed; and the younger these products therefore
are when employed the more individuals of their own sex will
appear among the offspring.”
Richarz believes, on the contrary, that the prepotency of the male
gives rise to the procreation of more girls; a mother of high reproductive
capacity will have more boys, one of less reproductive
capacity, on the other hand, more girls.
Starkweather (“The Law of Sex,” London, 1883) states his view
in the proposition: “The superior parent produces the opposite
sex;” and he holds the quaint view that this superiority is displayed
in certain anatomical characters of the face of the progenitor. He
endeavours from the shape of the head and from the facial expression
to deduce the superiority of the male and the female progenitor
respectively. A high, square forehead, with prominent
supra-ciliary ridges, constitutes, according to Starkweather, one of
the principal symptoms of this superiority; important also are a
strongly developed middle third to the nose, narrow lips, etc. He
declares that in families known to him the possession of this Roman
nose in the father is signalized by the possession also of a large
number of daughters, while a Roman-nosed mother has many sons.
The more the parents’ noses resemble each other the more equal
will be the distribution of the sexes among the offspring. He connects
this fact (!) also with the fact that the possessor of the
aquiline nose is the ruler of the family. Men of great strength of
character procreate chiefly daughters; women, on the other hand,
with a powerful character and a firm will bring into the world a
notable excess of boys. In the Southern States of the American
452union Starkweather found confirmation of his theory, since he observed
there that among the offspring of white fathers and coloured
mothers there was an excess of girls amounting to 12 to 15 per cent.
Among the half-castes of Java, the so-called Lipplapps, in the third
generation girls only are born, and these are sterile. The excess
of girls in these cases depends upon the superiority of the white
father; this superiority is transmitted to the few sons of the second
generation, and these therefore procreate girls only to constitute
the third generation; the latter are not powerful enough to bear
children at all.
Roth has revived the old view that one ovary provides the germs
for the male offspring, the other those for the female offspring. He
believes further that in the process of cohabitation the mechanical
impressions and stimuli received by one-half of the external genital
organs, reinforced by contact with and pulling on the pubic hair,
are transmitted through the pudic nerve and the hypogastric plexus
to the corresponding half of the vagina and the uterus, to the
Fallopian tube of that side and to the corresponding ovary. If, now,
we can consider it as established (?), that in the human female
one ovary discharges male ova only and the other female ova only,
it seems to him that it is the corresponding half of the external
genital organs, when specifically stimulated in sexual intercourse,
and the consequently increased vital activity in the pudic nerve and
its connections with the hypogastric plexus, that must be regarded
as the organ by means of which sex is determined. Roth has also
been informed by laymen that when for some time they have procreated
daughters only they subsequently procreated sons, “when,
having been accustomed to sleep on one side of their wife, they
adopted the practice of sleeping on the other.”
Ricardi reports that in Modena the peasants say that a man whose
wife has hitherto had daughters only, must, if he wishes to have a
son, assume some other posture than usual in the performance of
coitus.
III. Experimental Investigations.
A considerable number of years ago, Thury attacked the problem
of the determination of sex by the experimental method. In his
series of experiments he ascertained, using 29 cows, that in the
case of 22 of these, which were served early in their heat, the calves
were without exception heifers, while in the case of the remaining
7, which were served late in their heat, the calves were equally
453without exception bull-calves (Thury, “The Law of the Determination
of the Sexes,” Leipzig, 1863); in the record of these experiments
no mention is made of the age of the cows. Thury concluded
that the sex was determined according to the fertilization of the
ovum soon or late after its liberation from the ovary; namely, that
an ovum fertilized soon after its discharge produced a female,
whilst an ovum which had become comparatively old before it was
fertilized became a male.
Thury’s sensational experiments gave rise to a succession of similar
experiments, made mostly by cattle-breeders, above all in agricultural
colleges and in stud-farms.
Some of these experiments were made in the agricultural colleges
at Proskau and Eldera. The cows, which according to
Thury’s views should have been delivered of heifers, were served
as soon as their heat was observed (the heat lasted as a rule from
24 to 30 hours); these were delivered of 5 heifers and 5 bull-calves
(in Proskau) and of 3 heifers and 5 bull-calves (in Eldera); the
sexual ratio in these cases was therefore normal. On the other
hand, cows which were not served until their heat had lasted for
20 hours were delivered (in Proskau) of 1 heifer and 4 bull-calves.
Further experiments (in Waldau) gave the result that cows
served early were delivered of 1 heifer and 1 bull-calf. In another
series (in Eldera) 9 cows served as soon as heat was observed (or,
speaking strictly, in from ½ to 1½ hours of this), gave birth to
7 heifers and 2 bull-calves.
Experiments made at the Royal Friedrich Wilhelm Stud-Farm
gave the following results: In the case of 20 mares, which if
Thury’s theory had been correct should all have given birth to
fillies, 11 only fulfilled this expectation; but 10, on the other hand,
were colts. Touchon, in his experiments at Hohenhau, obtained
11 calves and 2 foals, exhibiting the sex expected in accordance
with Thury’s theory.
Düsing made a compilation of the figures given in all the experiments
made to test Thury’s theory, with the following results:
Cows fertilized early were delivered of 13 bull-calves and 29 heifers;
mares fertilized early were delivered of 10 colts and 13 fillies;
cows fertilized late were delivered of 5 bull-calves and 2 heifers.
Gerbe made experiments on rabbits, putting the buck to some
doe-rabbits soon after the beginning of their heat, but to others as
late as possible in their heat. On examining the young in the horns
of the uterus, from the ovary downward, the distribution of the
sexes was found to be approximately equal.
454Whilst Coste’s experiments on a hen gave results contradictory
to Thury’s theory, Albini’s experiments, made also on the common
fowl, gave results in agreement with that theory. He found that
the hens began again to lay fertilized eggs 3 to 6 days after intercourse
with the cock (from which they had previously been kept
separate); on the average, the distribution of the sexes in the
chickens hatched from these eggs was approximately equal, with,
however, a slight preponderance of cock birds. On the ninth and
tenth days after separation from the cock the eggs laid were half
fertilized and half unfertilized; on the twelfth day after separation
from the cock the unfertilized eggs were in a great majority; but
even as late as the eighteenth day after separation some of the eggs
laid were still fertilized. The fertilized eggs laid from the tenth to
the fifteenth day after separation when incubated produced a great
preponderance of hen birds.
We have to thank breeders for a large number of experiments,
such as those made by the breeder Fiquet, at Houston in Texas,
who found that a bull upon whose sexual capacities excessive
demands were made, procreated bull-calves exclusively; whereas in
herds containing numerous bulls there were found among the calves
born a preponderance of heifers. In thirty experiments on cattle
Fiquet always found that the larger the number of cows a bull had
to serve, and the longer they were kept in service, the larger was
the proportion of bull-calves among their offspring. On the other
hand, if certain cows had their sexual desires first satisfied by a
gelded animal and were then served by a vigorous and lusty bull,
an excessive proportion of heifers was born to these animals.
Janke obtained similar results in the breeding of sheep. In a
report made to Düsing he states that in the early part of the lambing
season more ewe-lambs are born than rams; in the latter part
of the lambing season, on the contrary, more rams than ewes. The
explanation he gives is that at the commencement of the pairing
the rams are fresh and lusty, whilst later their potency is comparatively
exhausted. In stud-farms, according to the same observer,
it is a familiar experience that the most vigorous stallions
serving a mare in the morning commonly procreate a filly; but if
later in the day they serve a second mare they almost always procreate
a colt. This, he thinks, finds its explanation in the fact that
the stallion, when he serves the second mare, is in a condition of
comparative sexual exhaustion, the more so because he usually
covers the first mare twice.
455Maritegoute’s breeding experiments at the sheep-farm of Blanc
(Haut-Garonne), on the other hand, gave divergent results. In
the early part of the pairing season, as long as the ram’s sexual
powers were completely unimpaired, he procreated more male than
female lambs. But when a few days later a great number of the
ewes were simultaneously on heat and the ram, owing to very frequent
acts of intercourse, began to be sexually exhausted, the procreation
of female lambs was in excess. But when, finally, this
period of maximum demands upon the ram’s powers was past,
and the number of ewes on heat became once more small, the procreation
of male lambs in preference to female was again observed.
The data obtained by Düsing from the Prussian stud-farms, in
which, when greater sexual demands were made on the stallions,
more males were procreated, have been already mentioned.
Fiquet made interesting experiments on cows and believed that
in this way he was able to demonstrate the influence of nutrition
upon the determination of sex—to such a degree, indeed, that he
believed it was possible to breed calves of either sex at will. The
following method gave him positive results in more than thirty instances.
He never had the cow served by the bull at the first heat,
but only at the second (if a cow is left unserved when on heat,
the heat recurs after an interval of three weeks). The interval of
three weeks was utilized in the preparation of cow and bull for the
copulatory act. If a bull-calf was wanted the cow was supplied
with the most invigorating fodder and was kept on the richest
pasture available. The bull, on the other hand, that was to serve
this cow was turned out to graze on the poorest pasture and was
given poor fodder. At the end of the three weeks, when the cow
came on heat for the second time, its sexual appetite was as intense
as possible, whereas the bull showed but slight inclination to the
sexual act. If the bull now served the cow a bull-calf was procreated.
The opposite procedure led to the procreation of a heifer.
For this purpose Fiquet kept the cow on low diet during the interval
between the first and second heats, and had her first served by a
castrated animal. When in this way, and by the low diet, the
sexual appetite of the cow had been sufficiently diminished, it was
served by a lusty bull, which for a long time had not been put to
any cow, and the sexual potency of which had been increased to
the uttermost by feeding it for several weeks on the most invigorating
fodder.
The results of these experiments, according to which the nutrition
456of the parent-animals before the copulatory act has an influence
upon the determination of sex, is explained by Düsing in this
way, that nutrition influences also the quality of the reproductive
products. “Poor nutrition gives rise to diminished functional
capacity of the genital apparatus. Thus, for example, the production
of semen is lessened. It can, in fact, hardly be replaced as
quickly as it is used up. This occurs when there is a lack of
adequate means of subsistence, and also when there is a lack of
comparatively young males. In both cases alike we trace the effects
in the birth of an excess of males. Converse conditions give rise
to an excess of female offspring.”
Passing now to consider investigations made by physiologists,
Born, at the anatomical institute at Breslau, has endeavoured to
solve the problem of the determination of sex by means of experiment.
He employed for this purpose rana fusca, an animal with
which positive results can be obtained in a comparatively short
period of time. He examined the sex both of the frogs in the
free state (165), and also of larvæ which he had bred in specially
arranged aquaria. Whereas among the frogs developing in the
open, the numbers of the sexes appeared to be approximately equal
(there was an excess of females amounting to 2 or 3 per cent.);
among those bred in the aquaria there was an enormous preponderance
of females (96 per cent.). This remarkable result is referred
by Born to the inadequate supply of nutriment in the case of the
larvæ bred by him (he fed them on hydræ and on putrefying frog
and tadpole meat); from an examination of the alimentary canal
of tadpoles caught in the open Born ascertained that their normal
food was the mud of the pools in which they were hatched, containing
infusoria, radiolariæ, diatoms, algæ, etc. The accuracy of
this explanation appeared to Born to be more convincingly shown
by the results in the case of one of his twenty-one aquaria. In this
one alone the percentage of males was as high as 28 per cent., and
the tadpoles in this attained the same size as those developed under
natural conditions in the open, whilst in all the other aquaria the
tadpoles remained abnormally small. This particular aquarium,
owing to an oversight, had pond-mud on its floor, whilst all the
other aquaria were floored with clean sand.
A. von Griesheim disputes Born’s results and believes that the
latter, determining the sex of the tadpoles by means of a
hand lens, must have mistaken a great many female tadpoles for
males. He himself, by repeated enumerations of a large number
457of tadpoles (685), part caught in the open and part taken from a
large aquarium, found that the ratio between the sexes in the case
of rana fusca was regularly 36.7 males to 63.3 per cent. females.
E. Pflüger refers the divergence between Born’s results and his
own and those of von Griesheim not to any error made by Born
in the diagnosis of the sex of the tadpoles, but to the fact that in
the latter’s aquaria the mortality of the male tadpoles was probably
greater than that of the females. Pflüger endeavoured to ascertain
whether the concentration of the semen might have an influence
in the determination of sex. A quantity of frog-spawn was fertilized
with concentrated semen, taken direct from the seminal
vesicles, and another quantity of spawn was fertilized with diluted
semen, obtained by making an aqueous extract of the incised testicles.
The ratio between the sexes in the case of the two lots of
tadpoles, which were kept in separate aquaria, proved, however, to
be mathematically identical. But another experiment showed that
the number of males was very different, according to the kind or
race from which the animals were derived. He therefore believes
that for the character of the development of the reproductive
organs, the race of the parent animals is determinative. There is
very little likelihood of being able to modify this inherited sexual
ratio by means of outward influences affecting the ova and the ripe
semen prior to fertilization, and just as little by means of a number
of abnormal influences (change of climate, of water, of nutriment,
etc.) acting on the fertilized ova.
Düsing,—who in his work on “The Regulation of the Sexual
Ratio” (Jena, 1884) most ingeniously advocates the thesis that all
animals have the power, when there is a lack of individuals of one
sex, of procreating an excess of individuals of this deficient sex,
or, to put it in another way, that an excess of one sex determines the
procreation of an excess of the other sex,—instituted experimental
investigations regarding the determination of sex in the following
manner (in accordance with a suggestion made by Pflüger): About
ninety guinea-pigs were distributed in two pens in such a way that
in one pen there was a great deficiency of males and a great excess
of females, whilst in the other there was a deficiency of females
and an excess of males. Thus the sexual ratios in the two stalls
were opposed. In accordance with Düsing’s theory, therefore,
more males should have been born in the first pen and more females
in the second pen. Every week each pen was examined once or
twice, the sex of the new-born young was ascertained, and they
458were distinguished by small incisions in the margin of the ear. A
week later, when the young animals had developed a little further,
they were re-examined to make sure that no mistake had been made.
At first, in the pen containing the original excess of females,
there occurred a quite remarkable excess of male births. This,
however, was merely the result of chance, for soon the relationships
of the sexes among the new born was reversed, and thenceforward
many more females were born than males. But if all the births
occurring in this experiment are taken into consideration the number
is still far too small to allow trustworthy conclusions to be
drawn.
Düsing emphasizes the fact that such an experiment as this, in
order to furnish results worth consideration, must be continued
until the sexual ratio has become constant, so that it is no longer
subject to alteration by chance variations. If we assume that
Düsing’s theory is false, the results obtained would be the following:
In both the pens, in that in which there was originally an
excess of females and in that in which there was originally an excess
of males, the births, if observed through a sufficient period,
would present a definite sexual ratio which would be the same in
both the pens. But if the theory is well founded the sexual ratio
of the new born would vary in the two pens: in the stall in which
there had originally been a deficiency of males there would be an
excess of births of males over females; whereas in the pen in which
there had originally been a deficiency of females there would
on the contrary be an excess of births of females over males.
Düsing recommends that for such experiments even more fruitful
animals, such as rats and mice, should be utilized.
Institutes for pisciculture would also be extremely suitable for
such experiments in breeding for the determination of the matter
under discussion because, owing to the fact that in these animals
fertilization is effected outside of the body of the parents, a direct
examination of the ova and the semen used in the experiments can
be undertaken, and the fertilization can be made to occur under
conditions subjected to various alterations; also we can employ the
roe and the sperm of fishes whose age, life history, weight and size
are accurately known.
Much attention has recently been paid to the theory of Schenk,
based, as he states, upon numerous experiments regarding the influences
by which sex is determined. This observer also starts from
the principle that ovulation is not independent of the influences of
459nutrition and metabolism. He believes that in the cases in which
combustion in the body is effected in such a manner that remnants
of unconsumed substances, still capable of heat-production, make
their appearance in the urine, the ovum of the human female in
process of formation is not so far advanced in its development as
it is in cases in which the urine is entirely free from sugar, or at
any rate is free from any demonstrable traces of the presence of
this body. In the former case we shall find that the ovum is not
only less mature, but also that it is presumably less well nourished.
In his view such an ovum is less completely endowed in respect of
the indwelling qualities and forces of its protoplasm, and it appears
for this reason to be adapted only for the development of a female
individual. But when, on the contrary, in the maternal individual,
all the substances formed in and assimilated by the organism have
undergone combustion so completely that there is no sugar in the
urine, not even in the minutest discernible traces, the maternal body
is in a condition suitable for the development of an ovum adapted
to become a male individual. From these inferences, weak though
the chain of argument is, Schenk draws the conclusion, that by
the regulation of the nutritive material supplied to the organism,
and by the suitable choice of that material, we are to a considerable
extent enabled to support an ovum in its process of maturation
in such a manner as to cause it to develop into a male individual.
The nutritive material selected for this purpose must be of
such a nature that the elimination in the urine of even the minutest
quantities of sugar may be prevented; the urine must appear free
from sugar even when the phenyl-hydrazine test is employed. Thus
in every case in which we wish to influence a woman’s nutrition in
such a way as to lead to the procreation of a male individual we
must above all ascertain whether, in the woman in question, the
normal quantity of sugar is present in the urine. If after the most
careful examination no trace of sugar can be found in the urine,
and if reducing substances are present in this excretion in abundance,
no change need be made in the diet, and all we have to do is
to recommend that the requisite fertilization should be effected as
soon as possible, since there is every probability that in this condition
the embryo will prove to be of the male sex. But when, on the
other hand the “normal” quantity of sugar is present in the urine,
or when even traces only of that substance can be detected, it is
necessary by changes in the diet to cause the disappearance from
the urine of every trace of sugar, and at the same time to bring
460about the appearance in that fluid of an abundance of reducing
substances. Schenk claims by the experiments he has made along
these lines to have obtained results which show that it is possible
in this way to influence the determination of sex.
His method is to nourish the mother mainly on nitrogenous materials
and fat, and to give in addition only so much carbohydrate as
is necessary to prevent the absence of this from being seriously felt.
This diet should be continued for a considerable period, at best for
two or three months before the fertilization is effected. After conception
also, the same diet should be continued. In such a manner
we are able in certain cases to bring about the procreation of male
offspring. On the other hand, the desire for the procreation of
female offspring remains one which as yet we have no direct means
of fulfilling.
These vague experiments and ill-grounded theories of Schenk’s
do not, as a matter of fact, constitute an important advance in the
theory of the voluntary determination of the sex of the human offspring.
What in reality are the decisive influences in the determination
of sex, and how the final impulsion in one direction or the
other is actually effected, remain altogether obscure. Prediction of
the sex of the offspring, and the voluntary procreation of male or
female infants, remain problems for the solution of which the most
essential data are still lacking.
Ernest Hæckel writes regarding Schenk’s theory: “This important
‘discovery,’ which at the time of its first announcement attracted
throughout the world an attention rarely given to true
scientific advances, has now dwindled to the incomplete demonstration
that the nutritive condition of the mother exercises a certain
influence upon the determination of the sex of the child. But we
knew this much a long time ago. Düsing and others, partly by
physiological experiments and partly by statistical demonstrations,
had shown that changes in the quantity and the quality of the nutriment
supplied to either parent is capable of influencing the procreation
of boys or girls. But if what Professor Schenk maintains
were really true peoples living chiefly upon meat (as, for instance,
in the pampas of South America) should have an exceptionally
large proportion of male offspring; whereas those living mainly on a
proteid-free diet (on meal, sugar, and other carbohydrates), should
have an exceptionally large proportion of female offspring (as, for
example, the rice-eating Indian and Mongolian nations). But this
is by no means the case. And many other well-known facts are
461likewise opposed to the ‘epoch-making’ theory of Schenk.
Whether the fertilized ovum develops into a boy or a girl, depends,
I am convinced, upon far more complex, and to a large extent still
entirely unknown, physiological causes. The final judgment upon
the ‘Schenk theory’ must be, ‘Much Ado About Nothing.’”
Our exposition of the present standpoint of the doctrine of the
origination of sex in the human species, has, in fact, shown that
hitherto by statistical work, nor by anatomical investigations, nor,
finally, by the experimental method, have results been obtained
which render it possible to predict the sex of the unborn infant.
And even in respect of the study of those influences which exercise
a determining influence upon the origination of sex, no positive,
indisputable conclusions have been reached. We can only say it
appears probable that there exist several causes of the determination
of sex the co-operative action of which proves effectual. Not in
the ovum alone, nor in the spermatozoon alone, but in the reciprocal
influence they exert one upon the other in the act of conception
is sex determined. In the latter connection the relative and absolute
ages of the progenitors appear to have a certain influence in the
determination of the sex of the embryo; of importance also is the
greater or less demand made upon the sexual capacity of the begetter;
of influence too is the time at which the ovum is fertilized
after its discharge from the ovary. It appears to be fairly well
established that when the husband is at least ten years older than
the wife, while the latter is at the age at which a woman’s reproductive
powers are at a maximum, more boys are conceived than
girls (Kisch); also that one of the progenitors upon whose sexual
capacities the greater demands are made, tends to procreate an excess
of individuals of his or her own sex (Piquet, Düsing); and,
finally, that intercourse a considerable time after the cessation of the
menstrual flow (in the second week of the intermenstrual interval
or later) is favourable to the procreation of a male infant (Thury,
Hensen). The influence of nutritive conditions in the determination
of sex is less clearly established.
Statistical evidence has proved beyond dispute that given a sufficiently
large number of instances in varying conditions the sexual
ratio is 106, and this fact suggests that the determination of sex
is dependent upon the interaction of two influences operating in
opposite directions within narrow limits, in such a manner that the
chances of the birth of a male infant preponderate over the chances
of the birth of a female infant in the proportion of 106 to 100. In
462elucidation of this fact Hensen makes the following comparison:
“Let us imagine a balance the beam of which has two arms
of equal length; from the two extremities of this beam two balls
of nearly equal weight begin to roll toward one another; if one
ball rolls more quickly than the other, if one is lighter than the
other, or if one starts to roll before the other, the opposite end of
the beam will sink. The three influences are variously distributed;
one influence may reinforce another, or may counteract another;
but a decisive sinking of one end of the beam will always ultimately
ensue. A minimal shortening or lightening of one arm of the
balance will make the chance that the other arm will descend correspondingly
greater.”
Sterility in Women.
When we study the history of human civilization we find that
sterility in women is regarded, not merely as a misfortune, but as
a reproach. Among savage races, and in the Orient, where the position
of women is one of strict subordination, she does not attain
an honourable status until she becomes a mother. In Persia, a
sterile woman is always divorced by her husband. In India, also,
when a sterile married woman has in vain employed the various
religious measures advocated for the relief of her barren condition
she is sent back to her parents. Both in China and Japan, a barren
woman is regarded as a most miserable creature. Among the
negro races, a woman who fails to bear children is the object of
scorn and contempt. Among the Dualla negroes, a man whose
wife fails to bear children demands from her parents the return of
the sum which he paid for her at the time of marriage. Many of
the indigenous tribes of South America also make a practice of
divorcing a sterile wife. Among the better-class Circassians, the
women do not attain an assured position until they have borne a
child. In Angola a barren woman is the object of universal contempt,
and she often feels the ignominy of her position so keenly that
she commits suicide. Alike among the Jews and among the Turks,
barrenness in a wife is a recognized ground for divorce, and the
woman who has been divorced for this reason will hardly ever succeed
in obtaining another husband, for she is regarded as one whose
body is not properly developed. According to old German law,
barrenness in a wife and impotence in a husband were both grounds
for divorce. The code of the Emperor Justinian allowed of divorce
in cases in which for the space of two years a husband had been
unable to fulfil his marital duties, and such a union was termed
463innuptæ nuptæ. Among the ancient Romans, although they regarded
barrenness as a mark of the divine disfavour, according to the laws
of Augustus failure to bear children was a punishable offence, and
such a punishment was incurred by any married woman who had
attained the age of 20 years without having become a mother. In
ancient Greece also, divorces due to the barrenness of the wife
were by no means uncommon. Among the Slavonic peoples sterility
was so greatly despised that there is a Slavonic proverb which
runs: “A woman is no woman until she has borne a child”: and in
Istria a sterile woman is known by the nickname “Scirke,” which is
equivalent to “hermaphrodite.” The Jewish view of the matter is
expressed in the Talmudic rabbinical saying: “A wife’s duties are
beauty, gentleness, and the bearing of children”; and again, “the
poor, the leprous, the blind, and the childless, are like the dead”;
and, finally, “he who refrains from marriage with the deliberate
intention of having no children, incurs the guilt of murder.” In
the Koran we find the fatalistic expression, “God makes a woman
barren in accordance with his will.”
We can therefore readily understand that in the most ancient
medical writings the question of sterility in women is a matter of
earnest consideration. In the works of the early physicians of
Hindustan we find several apt remarks on the subject. Susruta
says: “Pregnancy most readily results from intercourse during
menstruation. At this time the os uteri is open, like the flower of
the water lily in the sunshine.” In the Old Testament, in which the
newly-created human couples receive the command, “Be fruitful
and multiply, and replenish the earth,” we find frequent references
to barrenness as a state equally dishonourable and unfortunate, and
the use of certain plants is recommended as a means of cure. The
Talmud contains several essays dealing with the causes and treatment
of sterility.
The Hippocratic collection of writings contains a number of
passages dealing with the causes of sterility and with the means to
be employed for its relief. We shall have occasion later to refer
to these recommendations. Celsus, on the other hand, has little to
say on this subject. In the works of Pliny, and also in those of
Aristotle, there are references to the topic of sterility.
Among the writers of the first century of our era, Soranus discusses
exhaustively the capacity for conception and sterility.
In his work we find, among other passages, the unquestionably
accurate remark: “Since the majority of marriages are concluded,
464not from love, but in order to procreate children, it is
difficult to understand why, in the choice of a wife, less regard is
paid to her probable fertility than to the worldly wealth of her
parents.”
In the middle ages, Paulus Agineta more especially treats of the
diseases of women, and among these, of sterility in women. That
in Arabian medicine much attention was paid to this question, we
can learn from the writings of Maimonides.
By sterility in women we understand the pathological state in
which a woman who is sexually mature fails to conceive, notwithstanding
frequently repeated, normal sexual intercourse throughout
a considerable period of time.
Sterility is termed congenital (or absolute) when, notwithstanding
repeated intercourse throughout a long period (not less than three
years), pregnancy has always failed to ensue; it is termed acquired
(or relative), when women who have already been pregnant once or
more often, cease to conceive, although they are still quite young
enough to do so, and have experienced regular sexual intercourse
for a long period (not less than three years). In a wider sense of
the term, we say that a woman is sterile, when, notwithstanding
prolonged and repeated sexual intercourse, in circumstances favourable
to procreation, she has failed to give birth to a living and viable
infant.
English authors also make a special distinction regarding that
form of acquired sterility (which is no great rarity), in which a
woman gives birth to a single infant and subsequently remains
sterile (“only-child sterility”).
The civilization of the present day, with its shady side, has
made it necessary for us to pay an increasing attention to
facultative sterility, dependent upon the use during intercourse of
means for the prevention of conception; and very recently
the surgical tendency of modern gynecology has brought into being
a new variety of sterility in women, viz., operative sterility.
The period which must elapse after marriage, before the absence
of pregnancy must lead us to regard a woman as sterile, is fixed
at three years. This limitation is based upon the statistical data
which (see Table on page 368) I gave regarding 556 fruitful
marriages.
The ideal state of fertility, that in which conception is the immediate
result of the first act of intercourse between husband and wife,
the conception being followed in due course by the birth of a child,
465is, like most other ideals, one very rarely attained. In the human
species, conception as the immediate result of the first act of sexual
intercourse, is an extremely unusual occurrence. To invoke medical
assistance for women who have failed to conceive during the first
three months of married life, which my experience shows to be
more frequently done now than formerly, is devoid of all justification;
and still worse is it, in this period of “early love” to subject
women, as has often been done recently by overenergetic gynecologists,
to local treatment, even to the extent of operative procedures.
We are not justified in speaking of the existence of actual sterility
until three years of marital intercourse have failed to result
in conception; still, when the commencement of the first pregnancy
is delayed for more than sixteen months after marriage, there is
considerable probability that the woman is sterile; and this probability
increases month by month till the expiry of the second year,
whilst as the end of the third year approaches, it becomes tantamount
to certainty.
Sterility is one of the commonest of the functional disorders of
women, and one of those which most often demand gynecological
assistance.
By a statistical study of the marriages of the royal and princely
families of Europe and of the marriages of the highest families of
the aristocracy, I learned that of 626 marriages, 70 were barren;
thus the ratio of fruitless to fruitful marriages proved to be as
1 : 8.87. But in other circles of society, in so far as data relating
to the matter were obtainable in my practice, the statistics of infertility
were by no means so unfavourable, the ratio working out
at about 1 barren to 10 fruitful unions. I must point out, however,
that these statistics, like all statistics of fertility, are to a degree
invalidated by the fact that in a certain number of the instances
included among the barren, an unnoticed abortion may have
occurred.
Simpson, in his investigation regarding the frequency of sterile
unions, found a ratio of 1 : 8.5 (in 1252 instances). In the English
aristocracy, where the marriages are for the most part restricted
among the members of a comparatively small number of families,
the ratio was 1 : 6.11 (495 instances); on the other hand, among
the population of Grangemouth and Bathgate, consisting chiefly
of persons engaged in seafaring and agricultural occupations, the
ratio of barren to fruitful unions was as 1 : 10.5.
466Spencer Wells and Marion Sims, as a result of their investigations,
give a ratio of 1 : 8.
According to Seeligmann, in Hamburg, among marriages of persons
in all classes of society, 11.5% are barren. Prochownick found
among 2500 women, all of whom had been married for eighteen
months or more, and none of whom were more than 40 years of
age, that 9% had failed to conceive.
According to Frank and Burdach, who do not publish the figures
upon which their estimate is based, only 1 marriage in 50 proves
barren. Lever, who also gives merely his percentage result, states
that 5% of married women are completely infertile. Hedin, dealing
with a Swedish community of 800 persons, states that the percentage
of sterile unions is barely 10.
According to Goehlert’s statistical investigations, in the dynasty
of the Capets, among 450 marriages, 19.7% were sterile: in the
Wittelsbach dynasty (Bavaria), among 177 marriages, 23.7% were
sterile; and among the ruling families of Germany (more than 600
marriages), 20.5% were sterile. In this investigation, however, no
attention is paid to the age of husband or wife; marriages and
remarriages are classed together without discrimination; and those
marriages only in which a living child was born are counted as fruitful,
so that the unions counted as sterile must contain many in which
abortion or stillbirth occurred. In three Esthonian communities
in Livonia, Oehren found that among 2799 marriages, 8.4% were
barren, but in this instance also stillbirths were ignored.
Ansell reports that of 1919 marriages of women belonging to the
upper classes, their mean age being 25 years, 152 proved barren, a
proportion of 1 : 12, or about 8%.
Matthews Duncan communicates the following data. In the year
1855, in the cities of Edinburgh and Glasgow, 4447 marriages were
contracted, and of these 725 proved barren, a proportion of 1 : 6.1;
75 of these may however be excluded from consideration, inasmuch
as the wives were already at the age of 45 or upwards. Among
the remaining 4372 marriages, 662 proved barren, a proportion of
1 : 6.6. In other words, 15% of all marriages of women between the
ages of 15 and 44 proved sterile.
From France we obtain figures showing a much higher proportion
of sterile unions. According to Rochard, in France in the year
1888, of ten million families, two million had no child at all, and
two million had each an only child, so that two fifths of the families
of France were taking no practical part in the maintenance of the
467population. According to Chevin, the proportion in France of
barren to fruitful marriages is as 1 : 5. 20% are entirely barren, while
24% exhibit only-child-sterility.
From Massachusetts, Morton reports that according to the last
census returns, one fifth of all married women are childless.
In England, numerous trustworthy statistics can be obtained regarding
the frequency of sterile marriages. The average proportion
of barren to fruitful unions was:
| Among the patients in St. Bartholomew’s Hospital |
1 : 8 |
| Among the inhabitants of Grangemouth |
1 : 10 |
| Among the inhabitants of Bathgate |
1 : 10 |
| Among the British peerage |
1 : 6 |
| Among the upper classes |
1 : 12 |
| Among the inhabitants of Edinburgh and Glasgow |
1 : 7 |
Matthews Duncan compiled the following table relating to 504
absolutely sterile women met with in his practice:
| Age at Marriage. |
Number of Years Married. |
| Less than 3. |
4 to 8. |
9 to 13. |
14 to 18. |
19 to 23. |
24 to 28. |
29. |
Totals. |
| 15 to 19 |
12 |
19 |
15 |
4 |
7 |
2 |
1 |
60 |
| 20 to 24 |
70 |
66 |
37 |
24 |
13 |
9 |
|
219 |
| 25 to 29 |
47 |
51 |
20 |
8 |
8 |
|
|
134 |
| 30 to 34 |
26 |
20 |
8 |
|
1 |
|
|
59 |
| 35 to 39 |
6 |
13 |
4 |
|
|
|
|
23 |
| 40 to 45 |
6 |
3 |
|
|
|
|
|
9 |
| Totals |
167 |
172 |
84 |
40 |
29 |
11 |
1 |
504 |
Ansell bases upon the observations made by him in the case of
152 sterile women the conclusion that there is no longer any chance
of the occurrence of pregnancy if a woman is:
| More than 48 years old, and has had no child for |
2 years |
| More than 47 years old, and has had no child for |
3 years |
| More than 46 years old, and has had no child for |
4 years |
| More than 45 years old, and has had no child for |
6 years |
| More than 44 years old, and has had no child for |
8 years |
| Less than 44 years old, and has had no child for |
10 years |
If we take into account also cases of acquired sterility, the proportion
of barren to fruitful marriages becomes even more unfavourable,
and the proportion increases enormously if, with Grünewaldt,
we number among the barren women those who fail to continue
child-bearing up to the normal climacteric period. Grünewaldt,
dealing with about 1500 women suffering from affections of
the reproductive organs, excluded all those who were either virgins
468or widows, and also all those who at the time of the observed barrenness
were over 35 years of age; this left more than 900 women suffering
from affections of the reproductive organs, all of whom were
sexually mature, and were living in marital intercourse; of these,
nearly 500 were barren, 300 being instances of acquired sterility,
and 190 instances of congenital sterility. Thus, according to this
observer, disease of the reproductive organs in women led in more
than 50% of the cases to disturbance of the reproductive capacity;
about one in every three women, previously competent to bear
children, became barren when affected with disease of the reproductive
organs; and among every five gynecological patients of the
condition already specified as regards age and sexual intercourse,
one proves congenitally sterile.
It must not, however, be forgotten, that sooner or later after
marriage artificial sterility tends to come into being, its early or late
appearance depending upon the degree of civilization and upon the
national and economical conditions of the people and the individuals
concerned. This fact must not be left out of the account.
The manner in which, in the human species, fertilization is
effected, is still far from clear in all its details; hence it is easy to
understand, that the etiology of sterility remains in many respects
obscure. It is impossible in every case to find a definite cause.
Whereas, on the one hand, notwithstanding the existence of apparently
insuperable obstacles, impregnation may nevertheless be
effected; so, on the other hand, sterility may exist in cases in
which all the circumstances appear favourable to the occurrence of
conception. Hence a classification of the different varieties of sterility
from the etiological standpoint, is a very difficult task, and the
conclusions thus obtained are often vitiated.
Although it cannot be denied that mechanical causes are competent
to lead to sterility in women, Sims, in his advocacy of the
mechanical doctrine of sterility, widely overshoots the mark. His
authority, however, has led to a general acceptance of this doctrine,
which is by no means justified by facts. The theory of mechanical
obstruction, according to which sterility in women depends upon
mechanical obstacles to the passage of the spermatozoa towards
the ovaries, is from time to time strikingly illustrated by cases
coming under our notice—cases the nature of which can hardly be
overlooked; but it is quite wrong to suppose that this causation accounts
for the majority of instances of sterility in women, and
469strict limitations should be placed upon the employment of surgical
measures based upon this mechanical theory of sterility.
The mechanical view has been counterposed by Von Grünewaldt
with a doctrine in which especial stress is laid upon obstacles
to utero-gestation, sterility being regarded as a functional disorder
brought about by affections of the female reproductive organs rendering
the uterus unfit for the incubation of the ovum. It cannot
be denied that the elucidation of this casual influence was a valuable
contribution to the theory of sterility, and it is unquestionable that
many morbid conditions of the uterus exist capable of giving rise
to sterility in this manner; but we must avoid the error of regarding
this doctrine as a full explanation of the cause of sterility.
If, however, both of these theories of sterility are insufficient,
we cannot regard a third theory, that of Matthews Duncan, as filling
the gaps in our knowledge. It would be most unfortunate if this
author were right in maintaining that all our knowledge of the
causes of sterility is to be summed up in the phrase “deficient reproductive
energy;” we cannot agree with Duncan in his belief that
“Sterility is an imperfection devoid of all perceptible, measurable
characteristics;” nor can we follow him when he maintains that
local causes, whether they are such as hinder conception, or such as
hinder utero-gestation, have a very limited sphere of activity. Matthews
Duncan adopts an incomprehensible standpoint when he regards
sterility as dependent upon a law of nature, as a condition
which may affect distinct classes or an entire population.
According to the latest doctrine of sterility, only in quite exceptional
instances is the woman regarded as responsible for the
occurrence of sterility; contrariwise, the male genital organs are
commonly blamed for the affection, which is in the overwhelming
majority of cases supposed to be due to azoospermia, usually dependent
upon gonorrhœal infection; compare with this, affections
of the female reproductive organs are said to play a quite subordinate
role in the etiology of sterility. But for my part, though I recognize
the important share that gonorrhœa in the male plays in the
causation of sterility, I am of opinion that the extreme view just
mentioned is by no means justified by the facts.
Sterility, a functional disturbance of an extremely complicated
nature, can, in my opinion, be most usefully elucidated from the
etiological standpoint by starting with the assumption that three
conditions are absolutely essential to procreation:
4701. that ovulation proceeds in a perfectly normal manner, the
maturation of the discharged ova being complete;
2. that normal spermatozoa have access to these normal ova (conjugation
of male and female pronuclei);
3. that the uterus is properly adapted for the gestation of the
fertilized ovum.
My classification of the varieties of sterility corresponds to these
conditions of procreation:
1. sterility due to incapacity for ovulation;
2. sterility due to some hindrance to the conjugation of ovum
and spermatozoon (under this head come also those cases in which
the male is at fault—azoospermia, and the like);
3. sterility due to incapacity for gestation.
It must also be admitted that there are additional causes of sterility,
causes which lie beyond our control. Moreover, as I have
already mentioned, in most cases of sterility, we have to do, not with
a single cause, but with the resultant of two or more cooperating
causes.
Incapacity for Ovulation.
Incapacity for ovulation, the first and most decisive cause of
sterility in women, may be absolute and irremediable, or relative and
transient. We have to do with the former in cases in which the
ovaries are entirely wanting, or when they are affected with organic
disease to such a degree that they have become incapable of fulfilling
their function of ovulation; incapacity for ovulation is, on the other
hand, relative and transient in certain pathological states of the
ovary and neighbouring organs, when there is incomplete development
or partial atrophy of the ovaries, when there are new-growths
of the ovaries, in cases of oophoritis and perioophoritis, in consequence
of disturbances of innervation, diseases of the central and
peripheral nervous system, violent emotional disturbance, constitutional
disorders, such as syphilis, chlorosis, anæmia, universal
lipomatosis, scrofula, alcoholism, and morphinism, also in consequence
of changes in the supply of nutriment and in the general
mode of living, or of senile changes, and finally in consequence of
hereditary influences.
The diagnosis of the etiological influence of suppressed or incomplete
ovulation in the production of sterility in women is at
times beset with great and even insuperable difficulties. The state
of the menstrual function, suppression of the flow, or the regularity
or irregularity of its occurrence, serve indeed to inform us as to
471the general activity or inactivity of the function of ovulation; but
the variations in this function give no certain information as to
whether a woman is fertile or infertile. Knowing as we do that
generally speaking an intimate connexion subsists between menstruation
and ovulation, we are indeed able to assert that regular
menstruation and fertility in women run a parallel course, and
further, that the greater the irregularity of the menstrual function,
the greater the tendency to sterility. Recently, great advances have
been made in the technique of manual exploration of the ovaries,
and by means of vaginal and rectal bimanual examination, we are
now able to obtain accurate information regarding abnormalities
in the size, shape, and position of these organs, and regarding any
other intrapelvic disorders. In this way we have been enabled to
recognize a number of pathological states of the ovaries which
affect the functions of these organs. In some cases also there are
general symptoms which furnish us with the means of drawing
conclusions, more or less trustworthy, regarding the state of the
ovarian functions; for instance, the general development of a
woman’s body, the condition of the external genitals, the vulva,
the mons veneris, the pubic hair, the clitoris, and the mammae.
Again, we can derive information from various troubles of which
women complain; such as sacrache; a sense of weight and pressure
in the pelvis; feelings of tension and shooting pains in the breasts;
flushings of the face; haemorrhage from the nose, mouth, or rectum,
recurring at regular intervals and vicarious in nature. In many instances,
however, it will only be by obtaining data regarding the
age, mode of life, and family history, of the person affected, that it
will be possible to draw conclusions as to the cause of the sterility.
The female reproductive glands, the ovaries, may, owing to developmental
disturbances during foetal life, either be entirely wanting,
or they may merely be deprived of certain structural constituents,
especially their epithelial elements. In the former case, we
have congenital complete unilateral or bilateral absence of the
ovary, a condition most commonly associated with the absence or
with a rudimentary condition of other portions of the reproductive
apparatus; in the latter case, we have the condition somewhat inappropriately
named congenital atrophy of the ovary.
Complete absence of both ovaries necessarily leads to absolute
sterility. Both congenital absence and congenital atrophy of the
ovaries, will usually be found in association with other anomalies
of the sexual organs. Absence of one ovary, on the other hand,
by no means entails sterility; on the contrary, when a single well-formed
ovary exists, ovulation usually proceeds in a perfectly
472normal manner. When such women marry, pregnancy usually follows
in the normal proportion of cases; and, in complete opposition
to one of the theories of the determination of sex to which allusion
has been made, such women bear children of both sexes.
Morgagni described a case of congenital absence of both ovaries
in a woman 66 years of age, in whom the external genital organs,
the vagina, and the uterus, were imperfectly developed, but the
Fallopian tubes were of normal size. Careful examination of the
upper borders of the broad ligaments of the uterus disclosed no
trace of ovary on either side.
Quain, in a virgin 33 years of age, found the vagina rudimentary,
with its mucous membrane but slightly corrugated; at the
upper end of this passage was a semilunar fold which probably
represented the uterus. The ovaries were absent; a small gland-like
body embedded in the left wall of the vagina was regarded by
him as a rudimentary ovary. The configuration of the body was
feminine, feminine also the disposition; moreover, there was a
monthly recurrent epistaxis.
The atrophy of the ovaries which normally takes place at the
climacteric period, to be more minutely described in the section on
the menopause, has constitutional effects similar to those dependent
upon absence or congenital atrophy of the ovaries.
A rudimentary condition of both ovaries, or bilateral atrophy of
these organs, with or without associated atrophy of the entire reproductive
system, commonly entails sterility. In such cases, in addition
to amenorrhœa, we usually find that the breasts are but
slightly developed, the pubic hair is scanty, the labia majora and
labia minora are small, whilst sexual appetite is deficient, and during
coitus the woman is entirely passive. On the other hand, we must
not make the mistake of inferring from the fact that the sexual
appetite is keen and coitus pleasurable, that therefore the capacity
for ovulation is normal. Even after operative removal of both
ovaries, some women have assured me, not only that the sexual
impulse was as strong as formerly, but even that they continued to
experience the sexual orgasm in its full intensity. This is analogous
to the well known fact that men who have undergone castration
after arriving at sexual maturity may remain capable of
performing coitus. It is a matter of history that in the lupanars of
ancient Rome, castrated men were kept to enable women to enjoy
the pleasures of sexual intercourse without fear of consequences;
and it is said that such men are to be found in Italian brothels to
this day. In the case of the lower mammals, it appears to be the
rule that when the reproductive glands are removed in early youth,
every trace of sexual desire disappears.
Incomplete development of the ovaries, with consequent defective
ovulation, may result from marriage in girls who are still
473immature—a fact already known to Aristotle, who wrote, “premature
marriage leads to a scanty progeny—that this is the case in
man as well as the lower animals is witnessed by the weakly inhabitants
of regions in which child-marriage is common.”
It is shown by statistical data that the age at which puberty
occurs, the age, that is, at which the menstrual flow begins, has a
relation to sterility; and the same is true as regards the age at
marriage. In the former connexion, women in whom puberty is comparatively
early, are less often sterile than those in whom puberty
is comparatively late. Emmet, in an investigation embracing
2330 cases, showed that in our climate the average age at which
the first menstruation occurred was 14.23 years, and that in the
case of women who subsequently proved fertile, the first flow took
place on an average 26 days earlier than in the case of women who
subsequently proved barren. We also learn from Emmet’s tables
that the mean duration of menstruation and the mean quantity of
the flow are larger in fertile than in barren women.
As regards the influence of the age at marriage upon fertility,
in women who marry between the ages of 20 and 24 years, sterility
is most infrequent; it is commoner in women who marry between
the ages of 14 and 20; after the age of 25, the proportion of sterile
women increases with each year to which marriage is postponed.
Premature atrophy of the ovaries, with consequent incapacity for
ovulation, may occur in a great variety of conditions; it has been
observed in scrofula, diabetes, rickets, phthisis, and malarial cachexia;
it also occurs in certain chronic intoxications, as from the
long-continued use of opium or morphine, and from the abuse of
alcoholic beverages. According to the observation of Burkart,
Levinstein, and Erlenmeyer, morphinism is a condition which may
be relied upon to bring about amenorrhœa and temporary sterility
from cessation of ovulation. It has been asserted but by no means
proved, that the long-continued administration of quinine hinders
ovulation. As a result of various acute and chronic disorders, a
simple atrophy of the ovarian follicles can be detected, dependent
upon simple fatty degeneration; this has been seen by Grohe in
children as a result of general atrophy, and also following caseous
and suppurative diseases of the respiratory organs; by Slavjansky in
children after chronic pneumonia and chronic dysentery, and in
adults as a sequel of typhoid, and in one instance as a sequel of
puerperal septicaemia.
Hyperplasia of the ovarian stroma, in slighter degrees of the
affection, leads to menstrual disturbances, partly of nervous and
partly of inflammatory nature, and in more severe degrees leads to
sterility dependent upon the hindrances which the thickened tunica
albuginea offers to the bursting of the mature follicles. Klebs believes
474that this anomaly is always due to a disposition acquired very
early in life, and perhaps at the time when the ovaries are first
developed.
Follicular cysts of the ovary, which are formed mostly at the
time of puberty, and originate under the influence of menstrual
congestion, from graafian follicles near to ripeness, are competent
to cause sterility, owing to the pressure they exercise upon the
superficially placed rudimentary follicles, leading to the atrophy of
these latter. Other new-growths of the ovaries have similar effects,
such as adenomata, carcinomata, dermoid cysts, cystomata, sarcomata,
and fibromata. In many cases of these disorders, however,
the ovarian follicles may for long periods remain unaffected; and
in these instances, ovulation, menstruation, and even conception,
may proceed undisturbed. Even in cases in which a neoplasm attains
a great size, if it affects one ovary only, ovulation may occur
normally in the other, and conception may ensue; and even in the
diseased ovary, if small portions of its tissue remain unaffected,
ovules may be discharged from these portions. The minutest portion
of healthy ovarian tissue, though all the remainder has been
destroyed by disease, may suffice to bring about conception.
Ovarian tumours appear with considerable frequency to be complicated
with sterility; but in such cases the question always remains
open, whether in the majority of instances the sterility is to be regarded
as the cause or as the consequence of the ovarian disease.
Boinet’s figures dealing with this problem are the most striking of
all. He states that of 500 women with ovarian tumours, 390 were
childless. But these results are challenged by other observers.
Veit’s estimates, based upon a compilation of the figures of Lee,
Scanzoni, and West, is that 34% of women with ovarian tumour are
sterile. On the other hand, Negroni’s collection of 400 cases of
ovarian tumour, including both married and unmarried, contained
43 only who had never been pregnant. Other lists show: 13
sterile women among 45 suffering from ovarian tumour (von
Scanzoni); 1 sterile among 21 (Nussbaum); 8 sterile among 63
(Olshausen). Winckel, among 150 sterile married women, found
32 suffering from ovarian tumour, which in two of these cases
only was bilateral. Atlee, in 15 cases of ovarian tumour, observed
premature cessation of menstruation at the ages of 30, 39, 40 and
42, respectively.
Although in many cases sterility develops coincidently with the
growth of an ovarian cystoma, yet in many other women such
tumours have no influence in diminishing fertility. Martin in a
case in which sterility existed in connexion with a unilateral ovarian
cystoma, the other ovary being healthy, observed pregnancy as a
sequel of the removal of the diseased ovary. In one of these cases,
475after removal of the ovarian cystoma, Martin punctured in the
other ovary a dropsical follicle which had attained nearly the size
of a walnut. Pregnancy in this case also followed the resumption
of marital intercourse. Müller reports that in his clinique within
recent years pregnancy complicated with ovarian tumour has been
observed in 7 instances; in one of these cases the pregnancy occurred
notwithstanding the fact that the new-growth was so large
as almost to fill the abdominal cavity. Holst reports the case of a
multipara 43 years of age who died in the 18th to the 20th week
of pregnancy; at the post mortem examination the left ovary was
found to be transformed into three cysts each the size of an apple,
whilst in place of the right ovary was a medullary carcinoma the
size of a man’s head; on neither side could a trace of normal ovarian
tissue be detected. Spiegelberg, in a woman who died shortly after
giving birth to her second child, found that both ovaries were transformed
into myxo-sarcomatous tumours; in a woman aged 42, who
died four weeks after her eleventh confinement, both ovaries were
found to be transformed into nodular carcinomatous tumours each
larger than a child’s head; in none of these ovaries was any normal
stroma to be found. Ruge reports the case of a woman 36 years
of age, who miscarried in the sixth month of pregnancy; she had
myxo-sarcoma of both ovaries, one weighing 5620 grammes the
other 480 grammes.
All these cases indicate that, notwithstanding the existence of
extensive degeneration of both ovaries, some minute remaining
fragment of healthy ovarian stroma is competent to produce normal
mature ova—a fact which has often been proved also by microscopical
examination. That under the influence of pregnancy, existing
ovarian tumours often take on extremely rapid growth, is
also indicated by some of the above cases.
Castration (oöphorectomy, spaying, Battey’s operation), the
removal of both ovaries, naturally results in sterility. If in
the literature of the subject cases are to be found in which,
after this operation, not menstruation merely, but even pregnancy
has occurred, this is to be explained either by the fact that in the
stump there was left a fragment of the ovary, still containing tissue
capable of producing mature ova; or else by the existence of a
supernumerary ovary. Schatz reports the case of a woman in
whom pregnancy occurred after double oöphorectomy. In the
month of February, 1880, this operation was performed on a girl
twenty years of age; she married in April, 1884; and in May,
1885, she was delivered of a mature female infant. The history of
the case and the details of the operation showed clearly that the
left ovary had been completely removed, with the outermost third
of the left Fallopian tube; the right ovary was cut away in such a
476manner that a strip of tissue of at most two millimetres (one
twelfth of an inch) in width was left in the body, whilst the right
Fallopian tube was left intact. This case teaches us that the smallest
remnant of the ovary is competent to render normal pregnancy
possible; and further, that a small size of the ovary no more constitutes
a hindrance to the proper reception of the ovum in the
Fallopian tube, than does an abnormally large size of the ovary,
or an unusual shape of this organ.
Miklucho-Mackay relates that among the indigens of Australia
the removal of the ovaries is often practised, in order to create a
special kind of hetairæ incapable of becoming mothers. McGillivray
saw at Cape York a native girl whose ovaries had been removed
because she was a congenital deaf-mute, with the object of preventing
her giving birth to deaf-mute infants. In the beginning of the
last century there existed in Sayn-Wittgenstein a small religious
sect whose custom it was always to conclude their religious services
by indiscriminate carnal union among the members of the community;
when women and girls were first admitted as members of
this sect, an attempt was made to render them unfitted for conception
“by means of a painful and dangerous compression of the ovaries.”
(Ploss.)
A transient, relative hindrance to ovulation may be brought about
by various pathological states of the ovaries. Acute oophoritis
usually suspends the ovarian functions; chronic oophoritis has
sometimes a similar effect, not only because the profound changes
that take place in the ovary hinder the formation of the ovules, but
also because, as we shall later explain more fully, the expulsion of
the ova and their reception by the Fallopian tubes are hindered. In
severe oophoritis and perioophoritis, more especially in parenchymatous
inflammation, sterility may be brought about by an absorption
of the finely granular contents of the follicles, which collapse,
with adhesion of their walls; when all or most of the follicles are
thus affected, the ovaries become small and hard.
In perioophoritis, the exudation leads to the formation of cord-shaped
or ribbon-shaped adhesions between the ovaries and the
broad ligaments, the uterus, and the peritoneal folds of the neighbourhood.
The ovary in such cases may also be displaced, or may
undergo atrophy from pressure.
In the case of 200 sterile women, I found in 46 instances chronic
oophoritis and perioophoritis. Olshausen reports that of 12 married
women suffering from chronic oophoritis, five were barren, whilst
of the remaining 7, three only had given birth to more than one
child. Matthews Duncan, on the other hand, saw pregnancy in a
case of bilateral ovarian inflammation, in which the organs were
considerably enlarged.
477Further, local or general peritonitis may lead to parenchymatous
inflammation of the ovaries, and this, spreading from the periphery
towards the centre of the organ, attacks the follicles irrespective of
their ripeness. Again, during the puerperium, the interstitial form
of oophoritis is by no means rare, and this may at times lead to
permanent sterility in either of two ways: it may be in consequence
of the onset of a secondary parenchymatous inflammation, which
destroys all the follicles; it may be because a thick and tough layer
of sclerosed tissue forms around the periphery of the ovary, which
mechanically prevents the maturation and rupture of the follicles.
According to Slavjansky, puerperal disease is the principal cause of
this form of oophoritis. Olshausen indicates as the most frequent
cause of primary perioophoritis, an inflammation propagated from
the Fallopian tubes, leading to the formation of masses of exudation,
which envelop the ovary, and by the pressure they cause, and by
interfering with the blood-supply, lead to atrophy of the gland.
Sometimes the chronic inflammatory induration by means of which
the stroma of the ovary is rendered denser and firmer, is due to
changes in the vessels, and depends upon valvular defects of the
heart—upon venous congestion. In this way, heart disease may
hinder ovulation and bring about sterility. Both syphilis and gonorrhoea
may give rise to chronic inflammatory changes in the ovary,
usually leading to premature contraction of the tissues and to the
formation of numerous adhesions. According to Olshausen, amenorrhœa
is not a common feature of ovarian disease, except in cases
of defective development of these organs, of cirrhosis of the ovaries,
and of bilateral new-growths. Disease affecting only a single ovary,
even tumour of considerable size, rarely causes amenorrhœa until
profound constitutional disturbance has ensued. An exception to
this rule is found in the case of carcinomatous tumours of the ovary;
these, indeed, are commonly bilateral; but even when confined to
a single ovary, amenorrhœa is a comparatively early symptom.
According to the same author, sterility is a common consequence
of chronic oophoritis and its sequelae, and is usual also in cases of
bilateral new-growths; on the other hand, tumours affecting a
single ovary often fail to prevent conception even though they have
attained a great size.
Syphilis in women must be regarded as a frequent cause of
sterility, by interference with ovulation, but is in this regard by no
means an absolute bar to the occurrence of pregnancy. According
to Parent and Duchatelet, under whose observation during the space
of 12 years there came annually an average number of 2625 syphilitic
prostitutes, the average annual of births in these cases was 63 only.
According to Marc d’Espine, 2000 prostitutes gave birth on an
average to two or three children in all during a year. (That there
478are other causes besides syphilis for the remarkable infertility of
women of the town, will be explained later). According to Bednar,
Mayr, and others, constitutional syphilis in women invariably leads to
sterility; others, as for instance Zeissl, believe that women suffering
from inveterate syphilis are commonly, but not invariably, sterile;
whilst according to Rosen, conception only takes place in syphilitic
women in whom the disease has passed into the tertiary form. Experience
shows, however, that neither early nor late forms of
syphilis necessarily lead to sterility in women. It must also be
pointed out, that syphilis in the male may be the cause of sterility,
and must be the cause thereof when the disease is localised in the
testicles, and the consequent degeneration of the glandular substance
leads to the occurrence of azoospermia, more particularly when
syphilitic or gummatous orchitis is bilateral. According to Lewin,
we fail to find spermatozoa in 50% of men, otherwise powerful,
suffering from syphilitic dyscrasia. Hanc, on the other hand, failed
to find azoospermia in any one of ten men suffering from lues. In
animals also syphilis is said to cause sterility.
The manner in which certain anomalies of the blood (anæmia
and chlorosis), general disturbances of the nervous system, febrile
states, and such constitutional disorders as scrofula, have a temporary
or permanent influence in checking ovulation, is far from being
understood; but the fact that ovulation is checked by such conditions,
has been established beyond question by numerous observations.
It is well known that severe fevers, more especially typhoid, suspend
the ovarian function; that in various chronic disorders of an enfeebling
nature, and notably in chlorosis, all signs of menstrual
activity disappear; and that in certain nutritive disturbances, as in
extreme obesity, amenorrhœa also occurs; finally, numerous cases
are on record in which some sudden affection of the nervous system
has instantaneously inhibited ovarian activity.
In anæmia and chlorosis, it is probable that the degree of menstrual
congestion is insufficient to ensure the bursting of the graafian
follicle. The sterility often observed as a sequel of typhoid, malaria,
the acute exanthemata, cholera, and septicaemia, is probably due in
most cases to the occurrence of parenchymatous oophoritis, with
consequent destruction of the ovarian follicles. The researches of
Slavjansky have shown that in acute disorders inflammatory changes
often occur in the graafian follicles. When infectious disorders
ran an acute course, this observer usually found that the parenchymatous
inflammation of the ovary had occurred near the periphery,
in the cortical layer, the destruction being limited almost exclusively
to the primitive follicles; when the course of the primary disorder
was more chronic, the mature or nearly mature graafian follicles
were the ones destroyed. When inflammation of a follicle has led
479to its destruction, it is replaced by a linear scar. Lebedinsky found
similar changes in the ovary after scarlatina—destruction of a lesser
or greater number of follicles, with formation of scars. Thus,
parenchymatous oophoritis as a sequel of acute diseases, may, if
severe, lead to destruction of all the rudimentary follicles, with consequent
sterility. In the post mortem examination of such cases,
the condition of the ovaries is similar to that which is elsewhere in
this work described as characteristic of these organs after the
menopause: the ovary is diminished in size, its surface is furrowed,
the tissue is indurated in consequence of overgrowth of fibroid
tissue; often not a single follicle is to be detected on section of the
organ.
Immoderate obesity is a disorder of nutrition favoring the occurrence
of sterility.
In very obese women of an age which normally is the reproductive
prime, amenorrhœa or scanty menstruation is a very common accompaniment.
In 215 such cases which came under my own observation,
amenorrhœa was present in 49, and menstruation was
scanty in 116; thus in nearly three fourths of these obese women
menstruation was either deficient or entirely wanting. Very remarkable
also is the high percentage of sterile women among the
obese. In the 215 cases already mentioned (all married women),
48 were sterile—a percentage of 21. Whilst the ordinary ratio of
barren to fruitful marriages is 1 : 10 or 1 : 9, in the cases in which
the wives, or both wives and husbands, are extremely obese, the
ratio is according to my own observations, 1 : 5—or, if we include
cases of only-child-sterility, 1 : 4.
We cannot wonder at this great frequency of sterility in obese
women when we remember that, apart from the menstrual deficiencies
which so commonly accompany this disorder of nutrition, obesity
is apt to entail many other disorders of the reproductive organs, as
for instance a morbid state of the uterine and vaginal secretions,
chronic metritis, and displacements of the uterus; still, it cannot be
denied, that in many instances we are unable in such obese women
to detect any disorder of the reproductive organs competent to
account for the sterility, and we must therefore assume that the
excessive development of fat has some direct influence in preventing
ovulation, or at least that it in some way exercises an unfavourable
influence upon the reproductive process.
That excessive obesity hinders fertility, is shown by experience
both as regards the vegetable and the animal kingdom. All animal-breeders
are familiar with the fact that undue production of fat
limits fertility. Thus, equally in the case of turkeys and in the
case of the common fowl, if the hens are overfed and become fat,
they cease to lay.
480Hippocrates already indicated obesity as a cause of sterility.
Writing of the wives of the Scythians, he pointed out as a proof
that their excessive obesity was the cause of the sterility from which
they commonly suffered, the fact that their female slaves, who were
thin, were readily impregnated by intercourse with the Scythian
males. The oft repeated dwindling and disappearance of ruling
families in India and in Egypt, has doubtless in part depended upon
the extreme obesity of the female consorts of such rulers.
In many instances, indeed, a great accumulation of fat on the
front of the abdomen and in the vulva, suffices to cause a simply
mechanical hindrance to the proper performance of a fertilizing
coitus. It is possible also that the phlegmatic temperament of very
fat women is a contributory cause to their sterility—if indeed it is in
general true that frigidity during sexual intercourse is unfavourable
to conception, as is expressed by the old proverb, quo salacior mulier,
eo foecundior. It is unquestionable that in very obese women
sexual sensibility is commonly greatly deficient, and that their husbands
often complain of their coldness and lack of passion. In
several cases that have come under my observation, dyspareunia
occurred in obese and sterile women.
The dependence of sterility upon obesity is often proved in the
most striking manner ex juvantibus. A “cure” for the reduction
of fat often results favourably in respect also of rendering the
woman who undergoes it readily impregnable—a result by no means
ardently desired.
It must also be pointed out that very obese women form a considerable
section of those suffering from only-child sterility, and this
largely in consequence of their strong predisposition towards abortion.
As the impregnated uterus enlarges, the space for its accommodation
is insufficient, owing to the great development of the panniculus
adiposus, and thus obesity, like intra-abdominal tumour,
predisposes to abortion. The excessive accumulation of fat within
the abdomen, by exercising pressure upon the inferior vena cava or
on its principal tributaries, hinders the venous return, and gives rise
to a chronic stasis in the uterine bloodvessels, those alike of the
muscle and of the mucous membrane.
Notwithstanding the fact that sterility is so common in very
obese women, the fact remains that some such women are remarkably
fertile, and have very large families indeed.
Towers-Smith, Duke, and Rodriguez, who have recently all been
engaged in examining the relations between obesity and sterility,
agree in asserting that sterility due to obesity may be cured by
dietetic treatment for the relief of the primary disorder of metabolism.
Though menstruation is usually deficient or absent in obese sterile
481women, and though it is commonly supposed that amenorrhœa
implies sterility, it is necessary to point out that whilst failure of
menstruation is a frequent and important sign of suppression of
ovulation, it by no means invariably has this significance. It is an
established fact, and one borne out by my personal experience, that
women who have never menstruated have nevertheless become
pregnant; others, again, have become pregnant although they have
ceased to menstruate for several years, and this has even occurred
in women at a comparatively advanced age. Hence, from the
fact that amenorrhœa exists, we cannot with certainty infer that a
woman is sterile. Moreover, we must remember that physiologically
amenorrhoeic women often enough conceive—during lactation. Although
we hold the opinion that there is an intimate connexion
between ovulation and menstruation, yet it is always possible in
cases in which menstruation fails to occur, that ovulation has taken
place, but that the stimulus which that process has exercised upon
the reproductive organs has been insufficient to give rise to the
customary flow of blood.
The following remarkable case came under my own observation:
Mrs. B., 26 years of age, had lived in sterile wedlock for six years,
had never menstruated, nor had she ever had any sanguineous discharge
from the genitals. The body was delicately formed, the breasts
were fairly well developed, the external genital organs showed no
abnormality. For some weeks before consulting me, this woman,
hitherto childless, and living in regular sexual intercourse with her
husband, had noticed a remarkable enlargement of the abdomen.
Another medical man whom she had consulted had diagnosed ovarian
tumor and had urged operation. A more careful examination of
the pelvis showed, however, that the woman was in the sixth month
of pregnancy, a diagnosis which was duly confirmed by the delivery
of a full-time child. In another of my cases, a woman married at
the age of 45 years, having ceased to menstruate two years previously.
She became pregnant and gave birth to a child in quite
normal fashion. The following instructive case also came under
my own observation: The wife of one of my colleagues, living in
sterile wedlock for 17 years, extremely obese, had since puberty
menstruated but scantily and with great irregularity. The menstrual
interval was several months, and when the discharge did appear,
it was pale in colour and small in quantity; it lasted moreover but
a day or two. Last winter, the flow as usual failed to appear for
several months, and since the woman had at the same time become
fatter than ever, Turkish baths and energetic muscular movements
were prescribed. The result of this treatment was a striking one—abortion.
After 17 years of marital intercourse she had for the first
time become pregnant.
482In the case of sterile women who are amenorrhoeic, even when
the amenorrhœa has never been interrupted by a menstrual discharge,
or when it appears entirely dependent upon obesity, it is
nevertheless necessary to be extremely cautious in making a diagnosis,
and above all in employing an intra-uterine sound. In such
cases I have known the most eminent gynecologists unwittingly
bring about abortion.
Cleveland, Godefroy, Haschek, Ritschie, Sommerus, Stark, Taylor,
and Young, have all reported cases in which pregnancy occurred
in women suffering from amenorrhœa; but all such cases must be
regarded as quite exceptional. Szukits examined 8000 sexually
mature women, and found among them fourteen only who had
never menstruated. Of these, four were multiparae.
Saint Moulin reports the case of a woman 24 years of age who
had never menstruated, but who none the less became pregnant and
gave birth to a fine girl. One of the most striking cases of this
nature is the one reported by Rodzewitsch, regarding a woman
who first began to menstruate at the age of 36 years. This woman
had however been married when fifteen years of age, and in the
subsequent twenty-one years she gave birth to 15 children, remaining
the whole time amenorrhoeic.
Puech reports the case of a woman who ceased to menstruate at
the age of 40 years, and remained amenorrhoeic for the subsequent
six years. Then menstruation recurred for a year, and finally ceased
definitively in consequence of the occurrence of pregnancy, which
terminated in the normal birth of a healthy boy. Loewy, in a woman
31 years of age, who had previously been amenorrhoeic all her
life, saw menstruation appear for the first time shortly after the
birth of her sixth child. Ahlfeld had under observation the case of
a woman who was the mother of eight children, and had never
menstruated.
Krieger reports the case observed by Mayer, of the wife of an
artizan, who between the ages of 17 and 28 years had given birth to
five children, and had had one abortion. After the age of 22, she
had no trace of menstrual discharge, but notwithstanding this, she
subsequently gave birth to three children. Krieger himself saw a
woman who had had her last child at the age of 33, and in whom
now, at the age of 48, menstruation had just ceased entirely. Two
years later, irregular menstrual discharges recommenced; when these
ceased, it appeared that the woman was once more pregnant, and
she was normally delivered of a full-time girl.
Renaudin relates the case of a lady 60 years of age who gave
birth to a child, menstruation having ceased 12 years earlier. Deshhayes
saw the delivery of a woman 50 years of age, two years
subsequent to the occurrence of a normal menopause. Capwron,
483quotes the ease of a woman who became pregnant at the age of 65
years. In this case menstruation had recurred, having ceased many
years before in a normal menopause. This woman aborted at three
months, and the foetus was well-formed.
In such cases of late conception, which occur after the normal
cessation of menstrual activity, we cannot be certain whether we
have to do with a simple persistence of ovarian activity, associated
with temporary or permanent cessation of menstruation; or whether
both functions, ovulation and menstruation, had ceased, and were
aroused to renewed activity by some determinate cause. It is possible
that in coitus we have such a stimulus, capable of reawakening
the slumbering ovarian functions. That this may be the case, we
are led to suppose by the fact that pregnancy at an unusually advanced
age most frequently occurs as a result of marriage late in
life. In Scandinavian countries, where the difficulties of providing
for a family are so great that a very large number of marriages
are inevitably postponed till comparatively late in life, the number
of pregnancies occurring in elderly women is correspondingly large.
However, pregnancy late in life occurs also in women who have
married early, and the most probable assumption to account for
such cases is that ovulation has occurred in the absence of menstruation.
Although by these cases the proposition is established that amenorrhœa
is by no means equivalent to incapacity for ovulation, still,
the former must indubitably be regarded as in general a most important
indication of disturbed ovulation. When a woman attains
the age of 20 years without having ever menstruated, or even having
experienced menstrual molimina, we may in the great majority of
such cases infer with justice that there is complete or partial failure of
development of the ovaries and the reproductive apparatus generally.
In some of these cases, examination discloses the fact that the uterus
is in an infantile condition. When we are able to bring about the
regular establishment of menstruation, we may hope also to remove
the sterility dependent upon the defective ovarian functional capacity.
General tonic treatment for the relief of chlorotic amenorrhœa quite
as often, in the case of previously barren married women, results in
the occurrence of pregnancy, as happens in cases of amenorrhœa
and sterility due to obesity, when this latter condition has been
relieved and menstruation has been re-established by suitable dietetic
treatment. Much less often is it possible to relieve the sterility of
scrofulous (tuberculous) persons, for in the majority of such cases,
in consequence of the scrofulous (tuberculous) constitutional disorders,
pathological changes have occurred in the ovaries already
in early youth, and these it is difficult or more often impossible to
remove.
484Scrofula (tuberculosis) is, according to my own experience, the
constitutional disorder which of all most frequently and most seriously
affects ovulation; and it appears that the ovaries are subject
to changes produced by this disease similar to those which occur
in other glandular organs. In cases in which no cause of the
existing sterility is ascertainable, the presence of scars due to scrofulous
(tuberculous) changes in the lymphatic glands may serve as an
indicator to show that the capacity for ovulation has been annihilated
or seriously diminished in early life by scrofulous (tuberculosis)
disease.
Among the causes of sterility, these three conditions: anæmia,
chlorosis, and scrofula (tuberculosis), play a leading part; indeed,
their importance in this connexion has hitherto been underestimated,
more especially in regard to the comparative frequency with which
they cause sterility. A large part of the favourable influence in
the relief of sterility in women which is exercised by the “cures”
at various watering places, depends upon the amelioration which
is thus effected in the aforesaid constitutional disorders.
It has been assumed that diabetes, which renders men impotent, is
competent also to cause sterility in women. Hofmeier reports a
case which appears decisive on this point. In a woman 20 years
of age, who had menstruated regularly since she was 14 until a
year previously, when the flow had ceased, he found the uterus
extremely small, barely 5 cm. (2 in.) in length, extremely atrophied,
the ovaries also atrophied and very small; the urine contained large
quantities of sugar. Here was doubtless a case of atrophy of the
reproductive organs secondary to diabetes.
In England, where the excessive use of alcohol is observed very
frequently in women as well as in men, sterility has frequently
been regarded as a result of chronic alcoholism. Matthews Duncan
reports cases which lead to the belief that alcohol has a specifically
deleterious effect upon fertility. Apart from the general or constitutional
disturbances dependent upon the abuse of alcohol, this
agent has in many cases a well-recognized pathogenic influence
upon the female reproductive organs, the morbid condition which
is most frequently and most readily assignable to this cause being
chronic oophoritis. The obesity which so frequently results from
alcoholic excess is a contributory cause of sterility.
Certain drugs, more especially quinine and morphine, are reputed
to cause sterility. Davies, reviving an old opinion, considers that of
all drugs tannin is the most effective in leading to sterility, and he
considers tea-drinking as responsible for this effect.
The influence of certain cerebral affections and psychical disorders
in checking ovulation has been established. Thus, de Montyel has
recently shown that in families subject to hereditary mental disorders,
485there is an unusually large proportion (1 : 7) of barren
marriages.
In addition, there are many influences which are known to prevent
or to diminish ovulation in the case of the lower animals, and which
may therefore be assumed with considerable probability to have a
similar effect in women. More especially we are here concerned
with external influences affecting unfavourably nutrition and innervation,
and therewith also ovulation; also near kinship between the
parties to the act of intercourse; and finally hereditary predisposition.
In animals, captivity, exposure to cold, over-exertion, insufficient
or unsuitable food, and inbreeding, have been proved to result
in infertility.
Doubleday asserted that “a too abundant supply of nutriment
hinders reproduction, whereas on the other hand insufficient or
improper food favours reproductive activity and increases the number
of the offspring.” Spencer, however, rightly points out that the
infertility noticed in these circumstances is not the direct result of
prosperity, but depends upon the pathological obesity which is thus
engendered by overfeeding.
No less interesting are the observations that have been made
regarding sterility in animals in confinement. In such animals there
are wide differences. Some refuse to cohabit, or have lost sexual
desire; others, again, show excessive sexual desire and cohabit too
often, without any result; or even if fertilization occurs, abortion
often ensues. In yet other cases, though conception follows intercourse,
and the animals go on to full term before delivery, the young
are still-born, or are weakly and misshapen. Caged birds often
lay no eggs at all or very few; or if they do lay, they neglect their
eggs; or if incubated, the eggs fail to hatch out. In France, experiments
regarding this matter were made with domestic fowls. If
the hens were given great freedom, 20 per cent only of the eggs
remained unhatched; with less freedom, 40 per cent of the eggs
were failures; whilst if the fowls were kept in a coop, 60 per cent
of the eggs were unhatched.
“Convincing proofs,” writes Darwin, “have been obtained to the
effect that wild animals which have recently lost their freedom have
their fertility diminished to a most remarkable extent. This infertility
is not dependent upon any degeneration of the reproductive
organs. There are many animals of the most diverse species, which,
whilst they copulate freely in confinement, fail in these circumstances
to conceive; others again, even if they conceive and have living
young, give birth to these in numbers which are unquestionably
much smaller than would be the case were the parents in the free
state.”
Interesting observations have been made by pigeon breeders.
486They state that when pigeons brought up in the same nest pair, the
number of their offspring is usually very small.
The influence upon fertility of unfavourable conditions of temperature,
either excessive heat or excessive cold, is very great. In the
case of pigeons, for instance, if the pigeon cot is adjacent to the
heated wall of a dwelling house, the pigeons sometimes begin to lay
as early as January, and may have young as often as eight times
in a single year. When the dovecot is cold, on the other hand, the
number of broods is smaller. In general, the procreative capacity
is greater in summer than in winter.
As regards inbreeding, many facts are on record showing the
influence of this practice in leading to the birth of malformed
offspring and to sterility. Darwin writes, “if in a pure race,
characterized by a certain tendency to sterility, we allowed only
brothers and sisters to pair, in a few generations the stock would
become extinct.” If animals closely related by blood pair, the number
of their offspring is always less than the average.
In the case of the human species, however, the influence of the
marriage of near kin in diminishing fertility cannot be regarded as
definitely proved.
Occasionally the incapacity for ovulation and the sterility dependent
thereupon are hereditary—paradoxical as this may appear.
It is necessary to assume, that just as the sperm is at times unsuited
for effective fertilization, so also the ova may be in a less or greater
degree insusceptible of fertilization. In the present state of our
knowledge, indeed, we are not in a position to be precise as to the
exact nature of such incapacity. It is possible that the enveloping
membrane of the ovum varies in its resistance to penetration, as
Schenk claims to have proved in respect of certain of the lower
mammals. In his experiments on artificial fertilization outside the
body of the mother, he ascertained that the cells derived from the
discus proligerus, surrounding the ovum in immediate contact with
the zona pellucida, are in some instances easily separable one from
another, so that the spermatozoa can readily obtain access to the
zona pellucida; whereas in other instances, in which the ovum is
of the same size and apparently in the same stage of maturation
as before, these cells remain closely attached each to the other, and
thus prevent the passage of the spermatozoa. This condition of the
ovum, so unfavourable to fertilization, may be hereditary in certain
families, and its transmission may render certain members of the
stock infertile. Such instances as the following from my own
practice are by no means rare. Of three sisters, whose family life
was intimately known to me, one had one child only, a girl, whilst
the two others remained childless. The girl of the second generation
married and remained childless. In England it is well established
487that when, in cases of only-child-sterility, the offspring is of
the female sex, this child will probably herself be barren. Galton
found that in the case of 14 heiresses (i. e. the only children of
wealthy parents), all of whom were married, 8 remained absolutely
barren, whilst of the others, 2 had each an only child.
It was formerly believed that when a woman gave birth to twins
of opposed sexes, the female infant would prove to be barren, this
barrenness being associated with defective development of her reproductive
apparatus. John Hunter (Animal Economy) ascertained
that in the case of twin calves of opposed sex, the genital organs
of the female twin were almost invariably imperfectly developed.
But the supposition that this is true also of the human species has
not been confirmed by experience. I know several married women
who had twin brothers, and these women have borne normal children;
however, the number of their offspring is remarkably small.
Simpson, in Edinburgh, recorded the results of the marriage of 113
women who had been born with twin brothers; of these, 103 had
proved fruitful, and 10 (i. e., about one eleventh of the whole)
barren, although of these latter women, one had been married upwards
of 5 years, and the remaining 9 for periods ranging from
10 to 40 years. Simpson also gave the history of four women
who were all the fruit of triple births, some of which had consisted
of two boys and one girl, others of two girls and one boy. All
four of these women were parous. Again, a woman who had been
one of a quadruple birth (three boys and one girl), herself gave
birth to triplets. A collection of all the figures accessible to me
relating to this subject, indicates that about ten per cent of the
women born in such circumstances prove barren—a ratio which
corresponds closely with the ratio of infertility in general.
Interference with Conjugation, Conditions Preventing Access of the Spermatozoa to the Ovum.
A condition essential to fertilization is a material union between
the sexual products of the male and the female respectively—the
act of conjugation. Thus, all conditions which prevent the spermatozoa
from obtaining access to the ova, bring about sterility.
Spermatozoon and ovum being normal, a great variety of pathological
conditions may prevent the one from gaining access to the
other. It is necessary for fertilization that the mature ovum should
leave the ovary, enter the Fallopian tube, and there come into contact
with the male sperm. Interference with any one of these essentials
may lead to sterility.
Thus, the constitution of the ovum itself may be at fault; or the
entrance of the ovum into the Fallopian tube may not be normally
effected; defects in these earliest stages of the process of fertilization
488are precisely the commonest and the most important. The emergence
of the ovum from the graafian follicle may be rendered
difficult or entirely prevented by pathological states of the ovary;
again, by inflammatory processes in the ovary, the tubes, or the ligaments,
by developmental defects in the tube, and by obstructions in
its interior, the entrance of the ovum into the tube, and its free passage
along the tube may be prevented. Numerous abnormalities
and diseases of the uterus may on the one hand prevent the entrance
of the ovum into the uterine cavity, and on the other may prevent
the upward passage of the spermatozoa to their goal. Amongst
conditions competent to produce these effects we must enumerate:
displacements of the uterus, structural changes in this organ and its
annexa, and other congenital defects and acquired states; more
particularly must be mentioned, uterus infantilis, acquired atrophy
of the uterus, flexions and versions of the uterus, new-growths and
inflammatory states of that organ, abnormalities in the shape or size
of the cervix uteri, and, finally, all conditions of the vagina or
vulva which hinder the proper performance of the act of intercourse.
In diagnosing the cause of sterility, in determining whether in
any particular instance it is due to some hindrance to the indispensable
conjugation between the male and female reproductive elements,
we have in the first place to ascertain the presence or absence of any
of the numerous conditions which interfere with the proper passage
of the ovum from the ovary through the Fallopian tube to the
interior of the uterus. The simpler mechanical hindrances to conception,
such as displacements of the uterus, or tumours of that
organ or its annexa, are easily recognized; and the same is true
of atresia of the cervix uteri, and of congenital or acquired stenosis
of the vagina. When obliteration or stricture of the genital tract
exists, a very careful examination, visual, digital, and instrumental,
must be made, rectal examination not being forgotten. Not infrequently,
amenorrhœa is attributed to ovarian disease, and only
subsequently on local examination is the cause ascertained to be
hymeneal atresia, with haematocolpos; many a woman has believed
herself to be pregnant, until examination has disclosed the fact that
the hymen is still intact, and that coitus has hitherto been effected
through the urethra. The importance of these stenotic conditions
as causes of sterility must not, however, be overestimated, for,
although they are common among the hindrances to conception,
the obstacle is by no means always insuperable.
Morbid changes in the secretions of the genital passages, whereby
the vitality of the spermatozoa may be destroyed before they have
time to reach the ovum and effect fertilization, are hard to diagnose,
for the conditions upon which such changes depend have not as yet
been adequately investigated.
489
Diseases of the Ovaries and the Fallopian Tubes.
Among the conditions which, although the maturation of the ovum
proceeds normally to a conclusion, may prevent conjugation between
the male and female elements, we must in the first place consider
an abnormal condition of the tunica albuginea of the ovary, a
thickening of this membrane in consequence of inflammatory processes
or of new formation of connective tissue, whereby the dehiscence
of the follicle is rendered difficult or entirely prevented.
Such thickenings of the ovarian envelope are the residue of perioophoritic
processes.
Such a hindrance to conception may be permanent or transient,
and thus the sterility dependent thereupon may be relative or absolute.
Similar is the effect of inflammatory processes affecting the
peritoneal investment of the uterus, the broad ligaments, and the
peritoneum clothing the floor of the pelvis; these conditions, perimetritis,
perisalpingitis, and pelvic peritonitis, resulting in the formation
of thick and extensive pseudomembranous bands, or in less
severe cases leaving merely slight adhesions and filaments, which
drag the uterus and the ovaries out of place, and thus render conception
difficult or impossible.
Perimetritic adhesions are apt to lead to dislocation of the tubes
either forwards or backwards, and most commonly into the pouch
of Douglas, thus giving rise to sterility. Rokitansky and Virchow
already insisted on the great importance of perimetritic processes
in causing sterility.
That congenital defects of the Fallopian tubes may lead to sterility,
is indeed a possible, but certainly a rare occurrence. The
defect may be unilateral or bilateral; or it may be that merely a
portion of one tube may be wanting. Bilateral absence of the Fallopian
tubes is usually associated with defective development of the
uterus, while the ovaries may be apparently normal. Such a case
is described by Foerster and Kussmaul. The vagina opened into
the urethra, the uterus was not calibrated, and diverged above into
two solid horns, to which the round ligaments and the ovaries were
attached. A congenital cause of sterility is to be found also in
atresia of the tubes, the abdominal extremities of which are closed;
this condition is met with also in other mammals. It is also assumed,
with less accuracy, that a supernumerary ostium tubae may lead
to sterility, in consequence of the ovum, which has found its way
into the normal ostium, returning into the abdominal cavity through
the supernumerary orifice. An unfavourable influence upon fertility
is exercised also by a form of hyperplasia of the tubes which sometimes
arises in consequence of erroneous development at the time
of puberty; the tubes, increasing unduly in length, become serpentine
490in form instead of being nearly straight; this tends to lead to
accumulation of the secretions, and renders the passage of the ovum
difficult. (Freund.) Yet another defect of development which, as
Klebs has pointed out, may lead to sterility, is absence of the fimbria
which normally retains the abdominal orifice of the Fallopian tube
in proximity with the ovary, in which case these structures may
be separated by a wide interval.
The entry of the ovum into the tube may thus be rendered difficult
by abnormalities of the abdominal orifice of the tube or of the fimbriae;
but still more is this the case when the mucous membrane
of the tube is diseased. The fringed border of the tubal orifice has
a distinct tendency to independent disease. As Klebs’s anatomicopathological
studies have shown, inflammatory changes are common
in this region, leading to contraction. The free margin of the
tube then appears to be strictured by overgrowth of fibrous tissue
on the serous surface, the opening being thus narrowed or even
entirely closed, whilst the fimbriae themselves may be drawn within
the aperture. In other cases, the ring of fimbriae is adherent to
some neighbouring part, especially to the ovary itself, when this
also is diseased. Further, on the fringed margin of the tube we
see papillary growths, telangiectases, or oedema with formation of
cystic cavities.
In the interior of the tubes also, pathological processes occur,
catarrhal inflammations, haemorrhagic or purulent exudations, sealing
up the passage completely. In some cases these exudations lead
to great distension and even to rupture of the tube. Thus, among
the causes of sterility must be enumerated: simple catarrh of the
tube, with swelling of the mucous membrane; purulent catarrh,
leading to its distension with pus—pyosalpinx; serous effusion
into the tube, hydrosalpinx; and haemorrhagic effusion, haematosalpinx;
further, that peculiar form of tubal inflammation, described
by Chiari and Schauta under the name of salpingitis isthmica nodosa,
in which hyperplasia of the muscular coat of the tube occurs at
irregular intervals, so that it appears to be beset with nodes. Special
mention must also be made of gonorrhoeal salpingitis, which will
subsequently be described in detail.
Inflammatory states of the tube may hinder conception, either
mechanically, by swelling of the mucous membrane, or by obstruction
of the lumen of the tube by exudations, by injury or destruction
of the ciliated epithelium, by lesion of the musculature of the
tube, affecting its peristaltic movements—all these hindering or
entirely preventing the passage of the ovum downwards or of the
spermatozoa upwards; or, again, chemically, by the deleterious influence
of many of the morbid secretions that are formed in these
conditions upon the vitality of ova or spermatozoa. These inflammatory
491states of the tubes may also lead to stricture or obliteration
of their abdominal extremities, or to displacement of the ostia, and
thus lead to sterility; in other cases these same conditions, leading
to distortion and displacement of the tube, may prevent the downward
passage of the ovum while leaving possible the upward passage
of the spermatozoa, and thus give rise to tubal gestation—a condition
which we shall not now consider.
It must not be forgotten that tuberculosis of the genital canal
attacks the tubes with especial frequency; in these organs we may
find miliary tubercles, and more commonly diffuse caseous masses,
completely filling the lumen of the canal. Finally we have to mention
the diverse forms of saccular dilatation of the tubes (Ger.
“Tubensäcke”), all of which possess the common pathological characteristics
of enlargement of the tubes and their conversion into saccular
cavities; the contents of these distended tubes may, however,
be extremely various, and such conditions may depend upon manifold
mechanical disturbances and inflammatory processes of the
uterus and its annexa.
When we consider how common, during the sexual life of women,
are perioophoritic inflammations, more or less intense, but often
without severe symptoms (and hence apt to be overlooked); when
we remember that the very process of ovulation and also the puerperal
state furnish opportunities for slight or severe pelvic peritonitis
to arise; and when we further take into account the frequency
and importance of gonorrhoeal pelvic peritonitis—we cannot fail
to admit that the results of these morbid conditions, such as adhesions
between the ovary and the ostium tubae, or closure of the tube
with consequent hydro- or pyosalpinx, must be reckoned among the
principal causes of sterility. If the frequency and importance of
these conditions is still underestimated, two reasons can be adduced
for this: first, that the slighter degrees of intrapelvic inflammation
often, as previously mentioned, elude diagnosis; and, secondly, that
even when the treatment is expectant merely, the exudations are
frequently absorbed, the adhesions give way, and the capacity for
conception is gradually fully restored.
When considering the etiology of acquired sterility, especial attention
must be devoted to gonorrhoeal pyosalpinx, the most important
and the most dangerous of the morbid manifestations of gonorrhoeal
infection in the female. Gonorrhoeal salpingitis and perisalpingitis
are very serious affections, in the first place because they are apt to
give rise to oophoritis and perioophoritis, as well as to pelvic peritonitis,
and other local inflammatory states. The minuteness of the
uterine orifice of the Fallopian tube, and the downward direction of
the ciliary movement in the interior of the tube, combine to safeguard
against the entrance of gonococci, but none the less they too
492often find their way up the tube, and small quantities of gonorrhoeal
pus enter the pelvic cavity and give rise to inflammations, in which
the ovary partakes.
According to Saenger, this gonorrhoeal disease of the uterine annexa
is found with especial frequency in women either wholly sterile
or affected with only-child-sterility, and is to be regarded as the
cause of their infertility; “infertility is indeed the rule, fertility the
exception, in all cases in which gonorrhoeal disease has passed
upwards beyond the os uteri externum.” The same author maintains
that, putting aside tuberculosis and actinomycosis, if, in a case
of infective inflammation of the uterine annexa, septic infection can
be excluded, and more especially when the disease affects both tubes,
when it is reluctant to yield to treatment, and when relapses are
frequent, we have no option but to believe that the affection is of
gonorrhoeal origin.
In 155 cases of chronic inflammatory disease of the Fallopian
tubes, von Rosthorn was able in 37 instances to prove that the
affection was the direct result of gonorrhoeal infection.
Recently, however, Noble has published cases which lead us to
believe that even pyosalpinx does not necessarily prevent the occurrence
of pregnancy. In operating for the relief of a unilateral
pyosalpinx, the uterus was opened, and a seven months’ foetus was
removed. In another case, the autopsy on a woman who had succumbed
to severe peritonitis arising immediately post partum, disclosed
a large pyosalpinx.
Closure of the ostium may also be brought about by chronic
metritis and endometritis, by chronic catarrhal states of the uterine
mucous membrane, and in general by pathological changes in
that membrane associated with local hyperaemia or abnormal
secretions. In some cases, salpingitis with consequent sterility
is the result of puerperal infection; and such a sequence of
events is especially common after an abortion followed by retroflexion
of the uterus, leading to elongation and kinking of the tubes.
An important hindrance to the entry of the ovum into the uterus
is sometimes offered by uterine polypi or myomata; growing from
the fundus, these may so fill the uterine cavity that the uterine
orifices of the tubes appear to be completely occluded.
At times, also, quite small myomata, growing close to the tubes,
may push these latter upwards, closing them, and thus giving rise
to sterility; such myomata may also lead to saccular dilatation of the
tubes, as occurred in the following case:
Mrs. S., aged 39 years, had one child when 20 years of age, but
since then had been barren. For several years she had suffered from
profuse menorrhagia. Owing to the enormous thickening of the
abdominal wall, bimanual examination of the uterus was impossible;
493the vagina was relaxed, enlarged, and contained an excess of mucous
secretion. The uterus was high up in the pelvis, anteverted,
enlarged, movable, sensitive to pressure; the portio vaginalis was
enlarged, soft, and excoriated; no tumour could be detected either
in the uterus or in the uterine annexa. The menstrual flow recurred
at intervals of from two to three weeks, lasting from one to two
weeks, and being extremely profuse; menstruation was painful.
Whilst the patient was under my observation an excessive menstrual
haemorrhage came on quite suddenly, with slight rise of evening
temperature (38.2° C.—100.8° F.), but severe general disturbance;
there were paroxysms of intense abdominal pain, violent vomiting
of greenish bilious masses, which after a time became haemorrhagic,
the abdomen was tense and sensitive to pressure, there was
cardiac weakness with general failure of strength; treatment proved
unavailing, and the patient died in collapse on the third day. The
autopsy disclosed: fibroma uteri submucosum, parietale, et subserosum,
haematosalpinx dextra, pyosalpinx sinistra, peritonitis. The
subserous myoma, of about the size of a pea, was in the middle of
the fundus uteri; the submucous myoma, of about the size of a
chestnut, filling the uterine cavity, sprang from the posterior wall of
the body of the uterus; the intramural myoma, of about the size of
a bean, was in the right wall of the corpus uteri. Both tubes were
greatly elongated, exhibiting serpentine windings. The right tube
was much distended, filled with sanguineous fluid; the left, partially
collapsed, contained greyish-green purulent material, having an extremely
offensive odour; some of this fluid had flowed through
the ostium abdominale into the abdominal cavity. Death in this case
ensued with great rapidity in consequence of rupture of the pyosalpinx,
and evacuation of its contents into the abdominal cavity.
Cystic formations in the round ligament (hydrocele of the round
ligament) sometimes lead to sterility. In the form of elongated
tumours of about the size of a hen’s egg they may fill the inguinal
canal, and even pass forwards into the labia majora. When as
large as this, they demand operative interference. Hennig records
a case in which such hydrocele of the round ligament was the cause
of sterility lasting 14 years, the woman becoming pregnant after
the tumour had been removed by operation. Similarly, infertility
may depend upon solid tumours of the round ligaments—myomata,
fibromyomata, or sarcomata.
Retro-uterine haematocele often gives rise to sterility. As a rule,
prior to the formation of a blood-tumour in the pouch of Douglas,
various menstrual disturbances occur, more especially menorrhagia;
or it may be preceded by some puerperal disease, especially perimetritis,
which by itself, indeed, seriously limits the fertility of the
woman thus affected; but when haematocele is superadded, her child-bearing
494capacity is much more gravely impaired, owing to the permanent
displacement of the uterus, to the perimetritic exudations,
to the adhesions formed around the ovary, and to stricture or occlusion
of the tubes. Still, sterility is by no means an inevitable
consequence of haematocele.
By many it is assumed that in cases in which the tubes are perfectly
normal, disturbances of innervation are competent to cause
sterility (or tubal gestation). It is supposed that nervous influences
affect the functions of the Fallopian tubes by leading to spastic
contractures of the circular muscular fibres of these structures, or
in other cases to paralysis; in this way nervous disorder may lead
to the retention within the tube of the unfertilized (or already fertilized)
ovum.
Diseases of the Uterus.
Pathological changes in the uterus may in various ways lead to
sterility dependent upon prevention of conjugation (physical contact
of the male and female reproductive elements). Thus, the
incapacity for fertilization may, on the one hand, depend on
hindrances to the passage of the ovum from the tube to the interior
of the uterus; or on the other, on some abnormal condition
of the vaginal portion of the cervix, whereby the passage of the
spermatozoa from the vagina into the uterus is prevented; or, finally,
upon displacements of the uterus or pathological structural changes
in that organ, whereby the implantation of the fertilized ovum in
the uterine cavity and its development therein are impeded.
The uterus may be entirely absent, but this is an extremely rare
condition; much less infrequent is a rudimentary condition of that
organ. In the latter case, it is either represented by a nodular rudiment,
or else it is conical or bicorned; whatever its shape, it is a
solid mass of muscular and connective tissue. In association with
absence or a rudimentary condition of the uterus, the vagina also
may be wanting, or may be represented merely by a small, blind
pouch; the Fallopian tubes may in such cases either be normally
developed or rudimentary. The number of instances of this kind
that have been observed is very large (Kussmaul, Klebs, Cusco,
Klinkosch-Hill, Cruise, Freund, Fürst, Engel, Gusserow, Nega,
Kiwisch, Rokitansky, Braid, Jackson, Lucas, Duplay, Dupuytren,
Renaudin, Crédé, Saexinger, and many others).
The uterus and the vagina may be absent in cases in which the
vulva is developed in a perfectly normal manner, with a mons
veneris projecting as usual, and covered with a proper growth of
hair. Ormerod and Quain have reported cases of this kind, in
which the external sexual characters were those of a fully mature,
perfectly developed woman, but in whom the uterus and ovaries
were entirely wanting.
495These defects of development necessarily entail complete sterility.
Sometimes during life the cause of the sterility is entirely overlooked,
and only discovered by chance or in post mortem examination.
Although the vagina usually shares to a marked extent in the
defects of the uterus, and at puberty undergoes a rudimentary development
merely, the marital intercourse of such individuals commonly
appears to be perfectly normal. As a result of frequently
repeated and vigorous attempts at intercourse, the rudimentary
vagina becomes accommodated to the needs of the case; and even
when the vagina is absent, the rudimentary depression by which
it is represented becomes distended into a large blind sac capable
of accommodating the erect penis. In other such cases, the penis
finds for itself some abnormal channel, and the husband may continue
to indulge in intercourse for a long period without discovering
that there is anything unusual. Sometimes it is the urethra which
becomes dilated and takes on in part the function of the vagina;
in other cases intercourse is effected per anum.
The following most remarkable case came under my own observation.
The patient’s husband was a physician, who nevertheless was
in complete ignorance of his wife’s abnormalities. The woman was
26 years of age, of medium stature, somewhat obese, breasts moderately
well developed, pubic hair well grown. She stated that before
marriage she had menstruated regularly, and that it was only after
she had married four years previously that menstruation had ceased—statements
which were unquestionably false. She consulted me
on account of amenorrhœa and sterility, which her husband believed
to depend upon her increasing obesity. Examination showed that
the vagina admitted two fingers and was 10 cm. (4″) in length;
but it was completely blind, and the mucous membrane was strikingly
smooth. On bimanual examination, only a rudiment of the
uterus could be detected, a mass no larger than a hazel-nut; the
ovaries could not be felt.
A similar case is recorded by Heppner. A Finnish peasant
woman 31 years of age consulted him on account of amenorrhœa
and sterility. She had been married for 12 years, and neither before
marriage nor since had menstruated or had had any periodic vicarious
bleeding. The pubes and the labia majora were thinly
covered with hair; the latter were very flaccid and but slightly
prominent; the nymphæ hung down like an apron for as much as
an inch below the genital fissure, and were very thin; the clitoris
was but slightly developed. The urethral papilla was of normal
size, the lacunæ around it were extremely well marked; the urethral
orifice had the form of a zigzag slit. Behind this latter was an
aperture environed by radiating folds, and this was the entrance to
496a blind passage about two inches in length; this aperture could
not, however, be identified as the introitus vaginae, for the reason
that there were no carunculæ myrtiformes, and moreover the callosity
of the mucous membrane characteristic of the vaginal orifice
was wanting. Behind the strongly projecting commissura labiorum,
however, the fossa navicularis appears as a separate depression.
The blind passage was clothed with a soft, pale-red mucous membrane,
and was entirely devoid of any trace of columnæ rugarum;
at the extremity of this passage there was neither scar nor induration.
On rectal exploration, no trace of uterus, normal vagina, or
ovaries could be felt, notwithstanding the fact that the abdominal
walls were very flaccid and examination was therefore easy. The
general configuration was feminine, the breasts were flabby and
dependent, the waist and hips were those of a woman.
Tauffer reports the case of a woman 25 years of age, married 2½
years, absolutely amenorrhoeic; on examination she was found to
have atresia vaginae with rudimentary development of the uterus.
The breasts were small, the mons veneris was deficient in fat, but
thickly covered with hair, the labiæ and the clitoris were normal.
R. Levi describes a case in which, in a patient 19 years of age,
the uterus was wanting, though the general physical development
was that of a normal woman. The breasts were well formed, and so
also were the external genital organs; a blind passage 4 cm. (1.6 in.)
in length, and admitting two fingers, represented the vagina. In
the position normally occupied by the ovaries, were two bodies
which were doubtless the rudiments of these organs. Menstrual
molimina had never been experienced.
Von Hoffmann, in making a post mortem examination on an
elderly married woman, found that the vagina ended blindly at a
depth of 6 cm. (2.4 in.), whilst the uterus was represented merely
by a pyramidally arranged bundle of fibres in the broad ligament.
Lissner reports a case in which the physician was the first to draw
the husband’s attention to the fact that his wife had no uterus.
Ziehl, in a married woman 57 years of age, found that the uterus
was completely wanting; the vagina ended blindly half an inch
from the surface; the tubes and ovaries were present. Boyd, in a
married woman 72 years of age, found a blind vagina half an inch
in length, and the uterus represented by a nodular rudiment on the
posterior wall of the bladder.
Rare cases are also recorded in the literature of the subject, in
which, notwithstanding the absence of the uterus, normal ovaries
were present, and in these latter periodic ripening of the graafian
follicles took place. A case of this kind was described by Burggraeve.
Complete sterility is entailed also by a persistence of the foetal
497condition of the uterus. In these cases, the uterus retains the form
it possessed at the beginning of the second half of intra-uterine life.
The portio vaginalis projects but slightly into the vagina, and the
os uteri externum appears as a small rounded opening. The cervix
is comparatively long and wide, and the folds on the mucous membrane
of the cervical canal are fully formed. The body of the
uterus is imperfectly developed, triangular in shape, with thin walls;
it is shorter than the cervix, and its interior is marked by folds of
mucous membrane converging towards the os. In these cases
menstruation is absent or scanty; the other reproductive organs,
including the breasts, are usually in a state of arrested development.
Women with foetal uterus are capable of sexual intercourse, and
carry on most of the functions of their sexual life in a manner
apparently normal; they are, however, invariably sterile.
An analogous cause of sterility is presented by the condition
known as uterus infantilis, in which at puberty the uterus fails to
undergo the changes proper to this period, and remains in the condition
characteristic of infancy. The cervix is disproportionately
large, whilst the body of the uterus is cylindrical in form, and the
mucous membrane lining its cavity is always smooth. The muscular
substance is unduly thin. The vagina may be normal, sometimes,
however, it is narrow, and the mucous membrane is less rugose than
normal. Associated with an infantile condition of the uterus we
find commonly, but by no means invariably, imperfect development
of the external genital organs, the labia, the clitoris, and the vagina;
the mons veneris is but thinly covered with hair; the breasts are
small. As a rule, menstruation is entirely wanting. Occasionally
the ovaries are wanting. This infantile condition of the uterus is
by no means extremely rare. According to Beigel’s figures, among
155 sterile women, in four the uterus was infantile.
Among 200 cases of sterility in which it was possible for me to
make a searching enquiry for the cause, I found 16 instances of
infantile uterus. Neither in the general physical configuration of
these women, nor in the state of their menstrual functions, was there
any striking abnormality; in the condition of the external genital
organs, however, in cases of defective development of the uterus
and ovaries, certain striking peculiarities were, in my experience,
almost invariable, and deserving therefore of close attention. The
mons veneris was extremely small, sometimes completely bald, or
covered very thinly with hair; and the hair when present, did not
exhibit the curliness usually seen in the pubic hair of married
women. On examination, the uterus, small in all its diameters from
arrest of development, could in every case be detected.
How exceptional it is in adult females with well developed internal
reproductive organs for the pubic hair to be scanty or completely
498wanting, has been shown by the investigation recently made by R.
Bergh on this hitherto neglected subject. In 2200 individuals engaged
in clandestine prostitution, he found the pubic hair extremely
scanty in 148, and the genital region nearly or completely bald in 6.
He states that early vigorous growth of the pubic hair is a trustworthy
sign of early sexual development; but he remarks that the
opinion of Aristotle that women in whom the pubic hair is slight or
absent are always sterile, is erroneous.
Note.—The author’s statement regarding the extreme infrequency of
absence or deficiency of the pubic hair in women with properly developed
internal reproductive organs, while true of European women, does not apply
to all races. In Japanese women, for instance, the pubic hair is as a rule
much scantier than in European women; and baldness, complete or nearly
complete, of the mons veneris is by no means uncommon. It is the exception,
in Japanese prostitutes, to find a thick and vigorous growth of genital
hair.—Transl.
In the Talmud, there is an interesting reference to this subject,
to the effect that it may be assumed that a woman is sterile if by the
20th year of her life the pubic region be not yet covered with hair,
if the breasts be not developed, if coitus be difficult, and if the tone
of the voice be masculine.
Madame Boivin, Dugès, Lumpe, and Pfau, maintain that the
development of the uterus from the infantile condition to that
characteristic of the sexually mature virgin, often occurs very late
and very slowly; and that women in whom we find the uterus in an
infantile condition, may later begin to menstruate and may become
pregnant. It has been suggested that in these cases there has been
confusion with primary acquired atrophy of the uterus. Still, that
it is necessary to be most cautious in cases of infantile uterus in
asserting that a woman is permanently sterile, has recently been
forcibly impressed on me by a remarkable instance. A married
woman consulted me some years ago on account of amenorrhœa
and sterility; examination showed clearly that the uterus was in the
infantile condition, and for this reason, not I alone, but several
leading gynecologists, assured her that there was no hope of her
ever becoming a mother; recently, however, after ten years of sterile
wedlock, she was safely delivered of a healthy child.
A sub-variety is constituted by the uterus pubescens, a uterus
which indeed at puberty has undergone a certain degree of development,
but has failed to attain the normal size; in such cases
the menses are regular, but sometimes painful. This form of
arrest of development of the uterus may occasion sterility, which,
however, often proves curable when by frequent sexual intercourse
and the congestion dependent thereon, the genital organs have been
stimulated to the completion of the process of development; the
499muscular strength of the uterus then becomes adequate, and the
dysmenorrhœic troubles disappear. In general it may be said that
if the rudimentary or imperfectly developed uterus is at all competent
to carry out the function of gestation, the necessary changes sometimes
occur in the organ with remarkable rapidity, and result in
normal pregnancy and parturition.
Uterus unicornis, when occurring alone, and not associated with
other defects or errors in development, is not a cause of sterility.
Women with a uterus unicornis, with or without an accessory horn,
menstruate, conceive, and pass through pregnancy and parturition,
in a perfectly normal manner; indeed, some women with this developmental
defect have given birth to twins. The assumption that
uterus unicornis predisposes to abortion does not always hold good.
If, however, pregnancy occurs in a rudimentary horn, rupture of the
membranes is inevitable, and the ovum or embryo passes into the
abdominal cavity, with the usual accompaniment of fatal haemorrhage.
The rupture commonly occurs between the third and the
fourth month of foetal life (months of four weeks each).
The uterus bicornis, with which may or may not be associated
duplication of the vagina, does not as a rule offer any hindrance
to conception; and the same statement is true also of the uterus
bilocularis or septus. Women with these defects of development
may give birth to healthy children; and some such women have had
twins, each foetus occupying a separate half of the uterus. Still,
births in cases of double uterus and vagina are rare occurrences.
Such cases have been published by Lasarewitsch, Litschkus, and
Készmarsky. In very rare cases of uterus bicornis associated with
double vagina, an obstacle to conception is offered by the fact that
one side only of the double vagina, the larger, is utilized in sexual
intercourse, and that this is a blind passage.
In cases of uterus bilocularis seu septus, the conditions as regards
pregnancy and parturition are similar to those that obtain in cases
of uterus bicornis. The twin uterus, uterus didelphys, the condition
in which the uterus is represented by two completely separated
halves, each of which has developed into an independent organ,
has been observed, as P. Müller has shown, in adults as well as in
infants; this condition offers no obstacle to conception, unless, indeed,
as occurred in a case of Tauffer’s, the vagina is rudimentary,
so that normal sexual intercourse is impossible. Satschoma reports
a case of uterus didelphys in which pregnancy occurred simultaneously
in both uterine cavities.
A careful distinction must be made between the congenital condition
known as the infantile uterus (i. e., congenital atrophy) and
acquired atrophy of the uterus, affecting the whole organ, or either
500of its segments, the body or the cervix; the latter condition may
offer merely a transient and curable obstacle to conception.
Acquired primary atrophy of the uterus occurs in weakly girls
who, just before the age at which the uterus normally undergoes
its transformation into the adult state, have suffered from constitutional
disorders, from chlorosis or anæmia, or from some other exhausting
affection. The uterus is then small, limp, and flaccid,
it is usually anteflexed, with a small, often insignificant portio
vaginalis; the anterior lip of this structure failing to project from
the vaginal fornix; the vagina is usually short and narrow. This
form of atrophy of the uterus is distinguished from the foetal
and from the infantile uterus more especially by the fact that no
disproportion exists between body and cervix, that the muscular
wall is better developed, and that the general configuration of the
uterus is rather that characteristic of the normal uterus of the sexually
mature woman. Persons with primary atrophy of the uterus,
are, moreover, backwards in the general development of their
sexual characters; the breasts are small, the pubic hair is scanty,
the menstrual flow is insufficient or entirely wanting, whilst severe
dysmenorrhœal manifestations are usual.
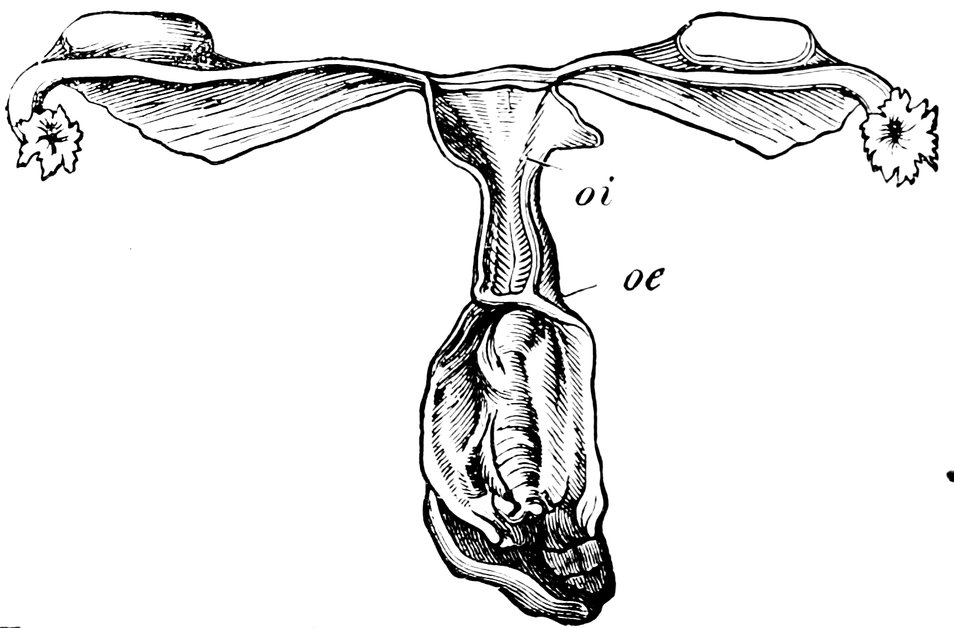
Fig. 70.—Congenital Atrophy of the Uterus (after Virchow), oi, Ostium internum; oe, Ostium Externum.
In favourable circumstances, when the constitution becomes more
powerful, in these cases of primary atrophy of the uterus, improvement
takes place; the uterus undergoes further development, menstruation
becomes more abundant, and the woman may become
pregnant. Such a favourable prognosis cannot, however, be entertained
if a severe flexion of the uterus is associated with the atrophy
of the organ; or if the ovaries are also atrophied.
Sterility results also from puerperal atrophy of the uterus. This
condition is a sequel of severe puerperal diseases, metritis, parametritis,
501and perimetritis; sometimes, even in the absence of such
inflammatory processes, it is due to puerperal hyperinvolution, occurring
especially in women previously weak in constitution, and
manifested by the fact that, notwithstanding the weaning of the
child, the menstrual flow remains for months in abeyance. The
uterus loses its firm consistency; it is sometimes shortened, sometimes
of normal length, but the walls are always greatly thinned,
so that, as Schroeder points out, the sound can be readily felt,
through the abdominal wall. Puerperal atrophy is a curable condition,
so that the sterility dependent upon this disease is not necessarily
permanent. Thus, in a case of P. Müller’s, a woman in whom
a twin delivery had been followed by extreme atrophy of the uterus,
with well-marked symptoms both objective and subjective, became
once more pregnant eighteen months after the termination of the
twin pregnancy.
Other forms of atrophy of the uterus have a similar deleterious
effect to that exercised by puerperal atrophy, as, for instance,
atrophy from the pressure of tumours of the uterus, or of solid
ovarian tumours; or, again, atrophy due to defective innervation of
the pelvic organs, occurring in various forms of paralysis, and
characterised by amenorrhœa and extreme smallness of the uterus.
Von Scanzoni has seen several cases in which young women, previously
healthy and menstruating with regularity, have been attacked
by paralysis of the lower extremities, and thenceforwards have suffered
from amenorrhœa and great contraction of the uterus; in
some of these cases a post mortem examination was made, and disclosed
the existence of true atrophy of the uterus. Jaquet saw a
similar case of atrophy of the uterus in a lady who had been
frightened by witnessing the storming of a barricade in front of her
dwelling; she was then in her 22nd year, and had given birth to
her second child 1½ years previously; thenceforwards she was completely
amenorrhoeic, and her uterus measured only 3 cm. (1.2 in.)
in length.
Displacements of the uterus (flexions and versions), and abnormalities
in the cervix uteri, are among the conditions which lead
to sterility by interfering with conjugation—by preventing the
necessary physical contact between the male and the female reproductive
elements. The frequency with which these diseases give
rise to sterility is, however, far from being so great as is commonly
asserted by those who maintain a mechanical theory of conception.
Pathological Changes in the Cervix Uteri.
In very early times, the attention of physicians was directed to
abnormalities in the shape of the cervix uteri, as offering hindrances
502to the entry of the semen into the uterus. Amongst the
writers of antiquity who have alluded to this matter, the names of
Hippocrates and Soranus must especially be mentioned.
The normal cervix uteri (Fig. 72) has the form of a flattened
ellipsoid, perforated throughout its longitudinal axis. On making
a longitudinal section of the cervical canal, we see that it is dilated
in the middle, and tapers towards either extremity, having thus
the shape of a spindle; the internal os is, however, somewhat smaller
than the external. The latter (os uteri externum, os tincæ, often
referred to without qualification as “the os”), has normally the
form of a transverse fissure, which, however, tends more towards
the circular form, the smaller it is, and the more widely its margins
are separated. In childhood, in consequence of the infolding of its
margins, the external os has usually a radiated form, later it becomes
rounded, and only with the attainment of sexual maturity
does it assume the form of a transverse slit. This form is maintained
throughout the epoch of active sexual life; but after the
climacteric, owing to the separation of the margins of the orifice, it
becomes once more rounded.
With regard to the greatly varying size and shape of the portio
vaginalis, it may be said that in general its anterior lip appears the
shorter of the two, owing to the lesser depth of the anterior vaginal
fornix, but that in reality the anterior wall of the cervical canal is
longer than the posterior; the actual length of the anterior lip of
the portio vaginalis, measured from the summit of the anterior
fornix, is from ½ to 1 cm. (0.2 to 0.4 in.), whilst the posterior lip,
from the summit of the posterior fornix to the end of the lip measures
1½ cm. (0.6 in.) and upwards. The position of the cervix is
such that, owing to the oblique direction of the long axis of the
uterus, superadded to the absolutely greater length of the anterior
lip of the cervix, the plane across the extremities of the two lips
faces almost straight backwards. The axis of the portio vaginalis
forms a right angle with the axis of the vagina; the cervical canal,
however, is not usually straight, but has a slight S-shaped curvature.
The mean length of the cervical canal in the virgin uterus
is 3 cm. (1.2 in.). (Lott.)
The “ideal” form of the cervix uteri and of the os uteri externum
is described by Sims in the following terms: “The vaginal
portion should measure about one fifth, certainly not more than one
fourth, of the entire length of the cervix uteri; that is, the anterior
lip should have a length of one-fourth to one-third of an inch, and
the posterior lip should be a fraction longer. The cervical canal
should either be straight, or have a forwardly directed curve; the
cervical axis should form a right angle with the vaginal axis; the
cervix should not be markedly anteverted or retroverted.” Sims
503is of opinion that every woman whose uterus is in this condition will
conceive within three or four months from the time when she first
enters upon conjugal intercourse; he adds, however, the important
proviso, “be it understood, that all else is in order.”

Fig. 72.—Normal Portio Vaginalis.

Fig. 73.—Conoidal Portio Vaginalis.
In conception, the cervix uteri subserves the important function
of providing for the free passage of the spermatozoa to the interior
of the uterus; and when we consider the nature of the processes of
sexual intercourse and fertilization, and more especially when we
bear in mind that normally the two lips of the cervix and the upper
segment of the vagina form a chamber for the retention of a portion
of the seminal fluid in contact with the os uteri externum, we are
readily led to assume that any great abnormality, in size of the cervix
(enlargement or diminution), in its shape (malformation), or in its
position (displacements—flexion, version, or prolapse), or, finally,
stenosis of the cervical canal,—may offer mechanical hindrances to
conception. And experience shows that this assumption is justified,
at any rate as regards conical elongation of the portio vaginalis
(Fig. 73), as regards an apron-shaped or beak-shaped hypertrophy
of the anterior lip of the cervix (Figs. 74 and 75), as regards
flexion upwards of the elongated cervix, and also as regards stenosis
or obliteration of the external or the internal os; although the
reservation must be made that no matter how unfavourable the
shape of the portio vaginalis, no matter how extensive the changes
in the cervix uteri, as long as a permeable upward passage for the
spermatozoa exists, conception is still possible, and in exceptional
cases may occur.
504

Fig. 74.—“Apron-shaped” Vaginal Portion. a. Greatly elongated anterior lip; b. Shorter posterior lip of the cervix.
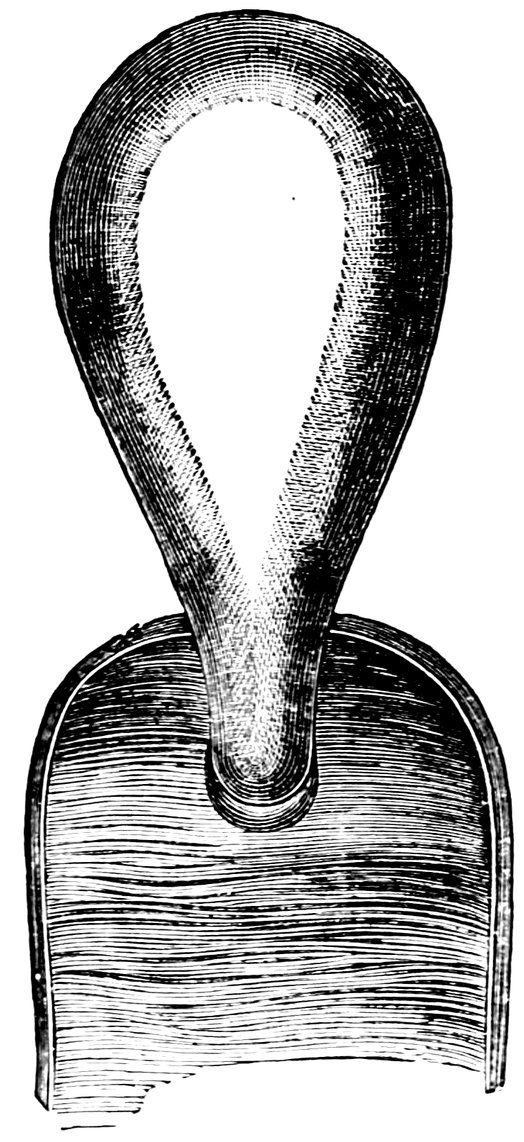
Fig. 75.—“Beak-shaped” Vaginal Portion. Posterior aspect.
When the cervix is hypertrophic and greatly enlarged, and the
vaginal fornix consequently much elongated, conception is rendered
difficult, for the reason that in such cases, either the semen rapidly
flows out of the vagina, or else a proper juxtaposition between the
penis and the external os no longer occurs, and the semen is ejaculated
at some distance from the os. The change in the shape of
the portio vaginalis, and also the elongation of the cervical canal,
are additional obstacles to the entrance of the spermatozoa into
the interior of the uterus; as regards the former condition, in
nulliparae the portio vaginalis is commonly conical, or pointed,
whilst the external os is very small, thus rendering the passage of
the spermatozoa a difficult matter; but in parous women, it is lobulated,
owing to the presence of deep fissures, whereby the penis
is conducted into the vaginal fornix, and the ejaculation of the
semen in this locality is facilitated. Hence, such hypertrophy of
the cervix and the portio vaginalis often coincides with the occurrence
of sterility. The hypertrophy is less apt to cause sterility
when it is limited to one lip of the cervix, unless, indeed, the affected
lip (more commonly the anterior) is so greatly enlarged that it
bends over and occludes the external os, whilst conducting the penis
into the fornix and away from the orifice. Cases have been known
505in which a single lip of the cervix was hypertrophied to such an
extent as to protrude between the labia.
The commonest malformation of the cervix is the conical cervix,
when the cervix is not merely elongated, but tapering; associated
with this condition is usually found a notable diminution in size
of the os uteri externum. According to Sims we find “conical
cervix in 85% of all cases of natural sterility.” According to the
same author, even in the absence of the conical form of cervix,
“sterility is probable in cases in which the portio vaginalis projects
fully half an inch into the vagina; if the cervix projects more
than one inch, sterility almost inevitably results; whilst if elongation
is even greater than this, so that the vaginal portion measures
from one and a half to two inches, sterility is absolutely certain.”
On the other hand, congenital smallness of the portio vaginalis,
the condition in which this organ appears merely as a slightly projecting
nodule on the upper part of the anterior wall of the vagina,
the anterior vaginal fornix being almost non-existent, and the
posterior fornix very extensive—a wide cul-de-sac—is also unfavourable
to conception. The probable reason is that, in consequence
of this deformity, the semen, after being ejaculated into the
posterior fornix, flows away down the posterior wall of the vagina,
without coming into contact with the short portio vaginalis.
According to Beigel, another frequent cause of sterility is to be
found in the existence of the so called “apron-shaped” portio
vaginalis, the condition in which, either from congenital deformity,
or else from hypertrophy or some other disease, one lip of the
vaginal portion is so formed as greatly to exceed the other in
length.
In consequence of hypertrophy, the portio vaginalis may assume
other, very various forms; in some cases it may increase in size to
such an extent that it projects into the vagina as a thick, hard
ball, and thus offers a serious obstacle to the reception of the semen;
or, again, in the form of the elongated, slender cervix, it may
become doubled upon itself, and in this way hinder the passage of
the spermatozoa (Figs. 76 and 77). Deformities of the cervix due
to hypertrophy of the portio vaginalis, rarely cause congenital
sterility, but more commonly the acquired form; for such hypertrophy
is hardly ever congenital, occurs but rarely in virgins, and
is usually met with in married women who have had difficult deliveries,
and consequently have suffered from uterine disease.
Another deformity of the vaginal portion of the cervix which
is important in its relations to sterility is the “snout-shaped cervix.”
Here the cervix is thinnest immediately at its insertion into the
vaginal fornix, and thickens gradually below, so that the organ
resembles a swine’s snout in form. As a rule, this deformity is
506due to diffuse hypertrophy of the connective tissue of the cervix,
the result of chronic endometritis and cervicitis.

Fig. 76.—Simple Hypertrophy of the Portio Vaginalis, which projected from the Vulva.
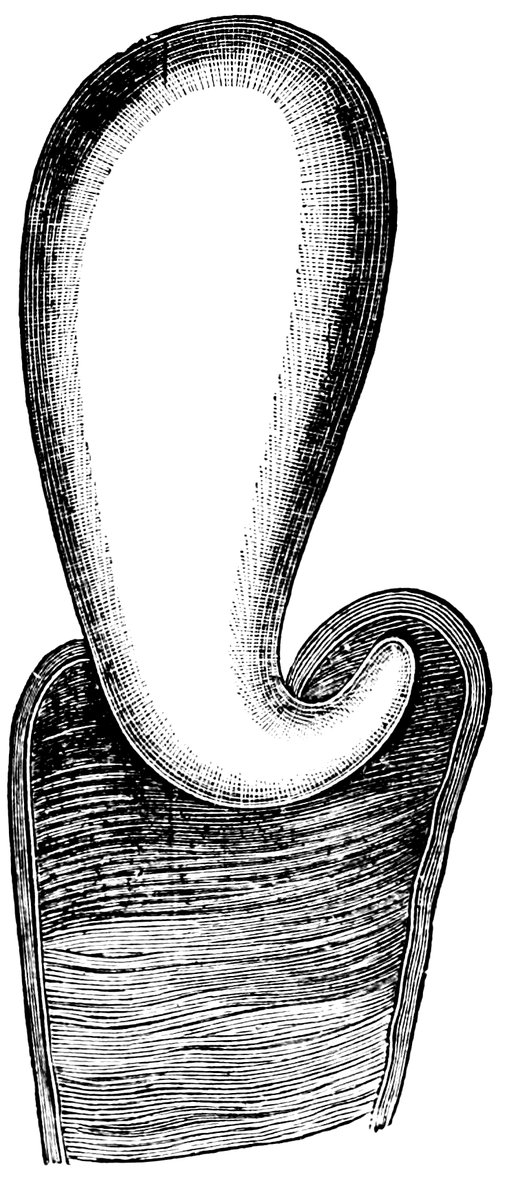
Fig. 77.—Elongated Cervix, bent upwards.
Fritsch, however, in two cases of characteristic col tapiroid, saw
pregnancy occur after the relief of the previously existing uterine
catarrh; in one of these cases the condition of the organs was
virginal, so that it was hardly possible to believe that the patient
was a multipara; even after she had had three children, the os
uteri externum with difficulty admitted the passage of the uterine
sound.
Pajot has devoted especial attention to the hindrances that are
offered to the entrance of the spermatozoa by displacements of the
cervix. In these cases, during coitus, the extremity of the glans
penis is not in contact with the os uteri externum, but passes into
a kind of cul-de-sac; in retroversion the posterior fornix; in anteversion,
the anterior fornix; in lateral version, the lateral fornix of
the side opposed to that towards which the lower extremity of the
cervix points.
Complete absence of the vaginal portion of the cervix puts difficulties,
though not very serious ones, in the way of conception,
507since the segment of the uterus which combines with the upper
segment of the vagina to form a receptaculum seminis, is wanting.
How important in predisposing to fertilization is efficient contact
of the external orifice of the vaginal portion with the ejaculated
semen during and immediately after intercourse, seems to be established
by my own observation, that women of small stature married
to men of average height exhibit much higher proportional fertility
than women of average stature. In the case of these small women,
the favourable circumstance is obvious, inasmuch as intimate contact
is facilitated between glans penis and portio vaginalis. I have
frequently heard complaints, from the husbands of such women,
that a single coitus is sufficient to ensure conception; and again
and again I have been informed by such women that they have had
10, 12, or 16 children. In one such instance known to me, the wife
had been pregnant 23 times, and had given birth to 19 normal children.
Contrariwise, women with a very long vagina, and with a
high position of the portio vaginalis, do not so easily become pregnant.
Of special importance in the causation of sterility is stenosis of
the cervical canal. This may be congenital, and then usually affects
the whole length of the canal; or it may be acquired, being dependent
upon inflammation of the mucous membrane. In these latter
cases, the swollen follicles of the mucous membrane burst, and their
granulating walls adhere. Other causes of acquired stenosis are
trauma, severe operative procedures during parturition, puerperal
inflammations, syphilitic ulceration, adhesion of the opposed granulating
surfaces after operative measures (as, for instance, after
severe cauterization, or after amputation of the portio vaginalis),
and, in short, from scar-formations however caused.
General swelling of the tissues leading to stenosis occurs at the
external os in hyperplastic uteri of virgin configuration; the small
round orifice characteristic of the virgin uterus becomes narrowed,
or even completely occluded, by the swelling of the tissues of the
vaginal portion. True adhesion of the walls does not occur in
these cases, but the minute aperture left by the swelling of the
walls of the canal is plugged by the epithelium, so that a small
blind depression in the centre of the portio vaginalis is all that
remains of the cervical canal. Such a condition is seen with especial
frequency in cases of prolapse of the vaginal portion, and is often
erroneously regarded as an obliteration of the os uteri externum
by epithelial adhesion (Klebs). Finally, stenosis of the cervical
canal may be caused by tumours, and also by the flexions and
versions of the uterus presently to be discussed.
Congenital atresia of the uterus is generally associated with other
developmental anomalies of the reproductive organs. In some cases,
508all that is at fault is that the mucous covering of the vaginal portion
passes uninterruptedly from one lip to the other; but in others, the
cervix is unperforated throughout, and the vaginal portion is but
slightly developed.
Acquired obliteration of the cervical canal may affect either the
external or the internal os, with a shorter or longer portion of the
rest of the canal. When very extensive necrosis of tissue has
occurred, as a sequel of difficult delivery, the adhesion may include
the adjoining segment of the vagina (utero-vaginal atresia).
The more marked the stenosis of the cervical canal, the smaller the
passage by which the vagina communicates with the uterus, the more
difficult will it be for the passage of the spermatozoa to be effected,
so that of the millions of spermatozoa deposited in the neighbourhood
of the os uteri, thousands will, as in normal cases, find their
way to the uterine orifices of the Fallopian tubes. So much the more,
then, is the contact between spermatozoon and ovum rendered difficult,
and so much the more unlikely is it that conception will occur. Moreover,
in consequence of the stenosis, there is retention of the cervical
mucus, which becomes thick and glutinous, and offers a further
obstacle to the passage of the spermatozoa. The unfavourable influence
upon the possibility of conception is, finally, increased if,
as is often the case, in association with the stenosis, the cervix
becomes elongated and assumes a conical form (these secondary
changes probably resulting from the inflammatory states of the
cervix common in cases of stenosis); and an additional obstacle is
offered to conception by the association with the stenosis of flexion
or version of the uterus. It is in such complicated cases that we so
often have the associated symptoms of dysmenorrhœa and sterility;
the dysmenorrhœa being due to the fact that the menstrual discharge,
if abundant, is unable to flow away with sufficient rapidity
through the greatly narrowed cervical canal; exuding from the
vessels of the uterine mucous membrane more rapidly than it can
be discharged, it accumulates in the uterine cavity, and gives rise
to painful contractions of the uterus.
Precisely what degree of narrowing of the cervical canal it is
which constitutes pathological stenosis, is in practice by no means
easy to define; and only in regard to extreme cases of pathological
constriction can there be no possibility of dispute. In cases of
congenital stenosis of the cervical canal, the diagnosis is very
easy, for the os uteri externum is then always extremely small;
often the aperture is no larger than a small pin’s head, a very
fine probe can be passed through it with considerable difficulty
and its passage is opposed all the way up to the internal os.
But in cases of acquired stenosis of moderate severity, the
diagnosis is often difficult. Owing to the small size of the
509orifice, and to the distensibility of the soft parts by which it is
surrounded, exact measurements are impossible. When the os is
with difficulty detected by the skilled finger, when the sound is not
readily introduced by the experienced hand, slipping past again and
again, and inserted only after repeated efforts—such an os is, as
Olshausen insists, always pathological. The normal virgin os uteri
permits the easy passage of a thick uterine sound with a diameter
of 3 to 4 millimeters (⅛ to ⅙ in.); but there are cases in which,
though a sound of this normal size can be passed, the os gives to the
examining finger the sensation of being contracted. If, in such a
case there is typical mechanical dysmenorrhœa with sterility, Olshausen
considers that we are justified in assuming the existence of
pathological stenosis of the os uteri, and in treating the case accordingly.
However, as Kehrer insists, it may be one of the greatest difficulties
in diagnosis—a difficulty not always to be resolved even
when all the attendant circumstances have received the fullest and
most painstaking consideration—to determine whether in any individual
case an anomaly of the cervix, such as stenosis of the
external os or of the whole cervical canal, is or is not to be regarded
as a cause of sterility. When stenosis is extreme, there need be no
two opinions about the matter; the difficulty is in cases lying
somewhere between a moderate degree of contraction and the lower
physiological limit of smallness. Every experienced gynecologist
will have seen such cases as Kehrer describes, in which before
marriage the os appeared extremely small, and yet soon after marriage
the woman became pregnant. For this reason we are justified,
with O. Johannsen, in reverting rather to the functional than to the
anatomical conception of stenosis, and in maintaining that so long
as the cervical canal is sufficiently large to permit the uterine secretions
to flow freely away, any stenosis that may exist is devoid of
pathological significance. Only when the outlet for the uterine secretions
is insufficient, so that the uterine cavity becomes distended
(as manifested by an elongation of the canal in the supravaginal
portion of the uterus, and by various disorders, amongst others
chronic endometritis), is the stenosis with its consecutive dilatation
of the uterus a serious obstacle to conception. “In such cases, the
contractions of the uterus during coitus will not suffice to express
the secretions it contains through the narrowed os, and the inevitable
consequence of the incomplete evacuation of the uterus is that the
aspiratory phase of the orgasm fails to occur.”
According to Winckel, stenosis of the external or of the internal
os is a cause of sterility only in cases in which it arises from a
follicular inflammation of the cervical mucous membrane; in such
cases, the os, (internal or external, as the case may be), being
510greatly narrowed by the numerous retention cysts, offers an obstruction
to the evacuation of the glutinous secretion of the follicles
yet remaining open. This secretion may offer an insuperable hindrance
to the passage of the spermatozoa; but in the absence of
catarrh of this character, a moderate degree of contraction of the
cervical canal will not prevent the outflow of the menstrual discharge,
or the upward passage of the spermatozoa.
The experience of horse and cattle-breeders also shows the
etiological importance of stenosis of the cervix in the production
of sterility: and in the case of mares and cows who are unfruitful
from this cause, artificial dilatation of the cervix has often been
performed, with resulting restoration of fertility.
Swelling of the follicles of the mucous membrane of the cervical
canal or of the cavity of the uterus, a condition which often results
from cervical catarrh, will, equally with stenosis of the cervical
canal, lead to sterility; pushing the mucous membrane before them,
and becoming pedunculated, these swollen follicles ultimately enlarge
to form polypi of the cervical canal or the uterine cavity, and may at
times completely occlude the uterine canal. In Fig. 78 is depicted a
polypus of this kind, which I removed from the cervix of a barren
woman 30 years of age. On the apex of the polypus was a large
ovulum Nabothi.
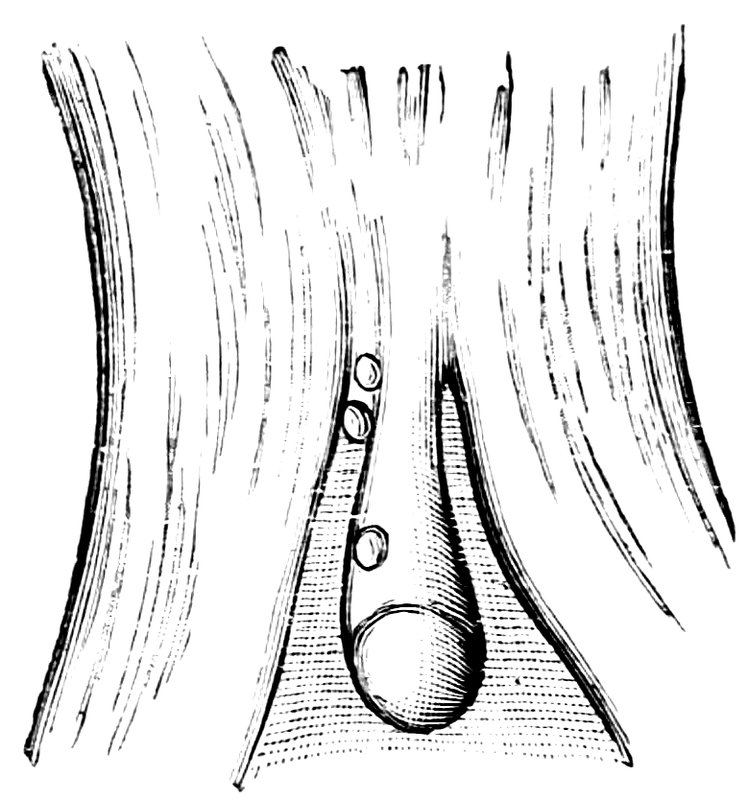
Fig. 78.—Cervical Polypus, originating from an Ovulum Nabothi.
Long-standing cervical catarrh readily leads to stenosis of the
cervical canal, and consequently to sterility. The swelling and
hypersecretion of the cervical mucous membrane the more readily
hinders the entrance of the semen, inasmuch as the mucous folds on
the anterior and posterior walls of the cervical canal which combine
to form the plicae palmatae are in the normal state already sufficiently
prominent; but in cases of catarrhal swelling they may project to
such an extent as completely to occlude the canal. Stagnation of
the thickened secretion offers in these cases a further hindrance
511to the passage of the spermatozoa, a stagnation which becomes
aggravated if in course of time the os becomes stenosed by overgrowth
of scar tissue. Ultimately, also, in cases of chronic catarrh,
a flexion of the enlarged and flabby corpus uteri readily occurs, and
this imposes an additional difficulty in the way of conception.
It is for these reasons that those women who in girlhood have
suffered from prolonged cervical catarrh, so often remain childless.
The sequence of events is that already described: follicular catarrh,
stagnation of secretions, stenosis of the cervical canal, enlargement
and loss of tone of the uterus; the thin-walled, enlarged, and flaccid
uterus ultimately gives way before the intra-abdominal pressure,
bending back, usually, into the pouch of Douglas. Thus, retroflexion
of the uterus is a common sequel of cervical catarrh (Hildebrand).
In some cases of sterility dependent upon cervical catarrh,
this sequence of troubles has not occurred, and it is merely the
mucus in the canal which prevents the passage of the spermatozoa.
B. Schultze reports the case of a woman who had lived for 13
years in sterile wedlock, but became pregnant after a single removal
of the cervical mucus.
The significance of chronic cervical catarrh in the causation of
sterility explains how it is that in many cases of barren marriage
the blame ultimately rests upon the husband, who, when he married,
was suffering from “latent gonorrhoea,” the inconspicuous relic of
an acute attack, undergone, it may be, months and even years
previously, and infected his wife with the disease. Such a gonorrhoeal
catarrh is in women especially apt to assume a chronic
form, and will then induce all the secondary morbid conditions
previously described, and thus lead to sterility.
Gonorrhoea in women frequently results in sterility. In addition
to the effect of cervical stenosis and of a morbid condition of the
cervical mucus in preventing the upward passage of the spermatozoa,
this disease may lead to many other changes inimical to
fertility. Thus, gonorrhoeal infection in women often leads to
inflammatory manifestations in the peritoneum, the perimetrium, and
the parametrium, and to catarrhal changes in the Fallopian tubes
(salpingitis, hydrosalpinx, pyosalpinx); these prevent the contact
of spermatozoon and ovum, or cause pathological distortions of the
walls or calibre of the tubes, which constitute permanent hindrances
to the occurrence of conception. Young married women, whose
husbands at the time of marriage were the subjects of incompletely
cured gonorrhoea, and who shortly after marriage suffer from
cervical catarrh, the discharge from the inflamed mucous membrane
not infrequently having a suspicious greenish colour analogous to
that seen in recent gonorrhoea in the male, often remain sterile for
long periods, owing to this gonorrhoeal cervical catarrh, endometritis,
512and tubal catarrh. For the diagnosis in such cases, in addition
to noticing the virulent character of the inflammation of the vulva,
urethra, and vagina, we must invoke the aid of the microscope; and
it will often be possible to decide at once that the inflammation is
gonorrhoeal by finding Neisser’s diplococci enclosed within the pus
cells of the cervical secretion.
The influence of “latent gonorrhoea” in diminishing the fertility
of women has been especially asserted—and overestimated—by
Nöggerath. From the fact that about 90% of sterile women are
married to men who have suffered from gonorrhoea either before
or during their married life, he infers that the sterility is due to
latent gonorrhoea communicated from husband to wife. If this
inference were justified, sterility would be far commoner than it
actually is. Nöggerath makes use of the term “latent gonorrhoea”
because the woman becomes infected without the obvious outbreak
of any acute phase of the disorder. The disease remains latent,
and a radical cure is not to be expected until the menopause. According
to Nöggerath, there are four varieties of this disease:
acute, recurrent, and chronic perimetritis, and oophoritis, always
accompanied by catarrh of the mucous membrane of the genital
organs.
Saenger, also, has asserted that 12% of all cases needing gynecological
treatment are of gonorrhoeal origin; and he even considers
that the consequences of gonorrhoea are in women more dangerous
and destructive than those of syphilis. E. Martin has also maintained
that endocervicitis leading to stenosis of the os uteri externum
and of the cervical canal is, in the majority of sterile young
wives, due to gonorrhoeal infection derived from a chronic, unhealed,
but inconspicuous, gonorrhoea in the husband. He further
considers it possible that various kinds of mechanical stimulation,
for example, intra-vaginal onanism, may, in certain conditions, give
rise to inflammation eventuating in cervical stenosis.
Of great interest are the mutual relations between dysmenorrhœa
and sterility, a matter to which some allusion has already been
made. A high degree of stenosis of the cervical canal is competent
to produce both these symptoms; but dysmenorrhœa may arise from
many other causes which have no direct influence in preventing conception.
Too much stress has, in fact, been laid upon the association of
dysmenorrhœa with sterility, and I must therefore point out that
I have seen numerous instances of dysmenorrhœa, including the so-called
spasmodic form of the disease, in women who have given
birth to many children; that objectively, in such cases, there
was an absence of that rigidity of the cervix to which Matthews
513Duncan attached so much importance; and, finally, that even when
the dysmenorrhœal pains had subjectively all the character of labour
pains, the introduction of the sound could be effected without using
any great force, and without giving rise to any severe pain.
Unquestionably, those authors, with Sims at their head, go too
far, who regard dysmenorrhœa as a constant sign of stenosis of the
cervical canal, and hence infer that in all cases in which sterility is
associated with dysmenorrhœa, the sterility is due to such stenosis—an
opinion contested by Schultze on the ground of anatomical investigations.
Dysmenorrhœa gives no indisputable sign that the cervix
is stenosed to such a degree as to hinder the occurrence of conception;
and Sims’s view, that in the great majority of cases dysmenorrhœa
is due to mechanical obstruction, is not supported by experience.
Women who suffer from severe dysmenorrhœa, frequently
become pregnant, though later, it may be, than women in whom
menstruation is normal and painless. Dysmenorrhœa is not due
solely to contraction of the cervical canal, but also to a variety of
other pathological conditions. The anomalies of the genital organs
which give rise to dysmenorrhœa do not, for the most part, offer
any obstacle to conception; and, on the other hand, stenosis of the
cervical canal may exist in women who are entirely free from dysmenorrhœa.
In order to test Sims’s theory of the mutual interdependence of
dysmenorrhœa and sterility, Kehrer conducted an investigation into
the state of menstruation both before and after marriage in relation
to the fertility or infertility of the marriage. He ascertained that in
sterile women virginal dysmenorrhœa had only been a very little
commoner than in fruitful women. Hence, the changes in the reproductive
organs upon which the occurrence of dysmenorrhœa
depends, must not be regarded as necessarily constituting hindrances
also to conception.
English gynecologists differ from those of Germany in believing
that there is an intimate causal relation between dysmenorrhœa, and
more especially spasmodic dysmenorrhœa, and sterility. The assumption
is, that the contractions of the uterus, which by their violence
during menstruation give rise to pains like those of labour,
occur also during coitus; by these contractions, the entry of the
semen into the uterus is prevented, or, if the semen does enter the
uterus, it is speedily expelled. This spasmodic dysmenorrhœa has
also been called mechanical or obstructive dysmenorrhœa, in order
to call attention to the theory that the aim of the cramp-like contractions
of the uterus is the expulsion of the menstrual blood which
has accumulated in the uterine cavity; although Duncan himself is
compelled to admit that neither the alleged mechanical obstruction,
514nor the accumulation of menstrual blood, nor yet the dilatation of
the uterine cavity, can actually be proved to occur.
Note.—The author is not quite correct in his contrast between “English”
and “German” opinion in this matter. Most English gynecologists follow
Matthews Duncan in calling attention to the fact that, as Herman puts it,
“spasmodic dysmenorrhœa is often associated with sterility”; but almost
all careful writers insist that while the association is proved, the nature of
the causal connexion, if such exists, has not been elucidated. For instance,
writing on this very question of the association of dysmenorrhœa with
sterility, Hart and Barbour remark, “after a careful survey of the literature,
we come to the conclusion that any discussion of sterility in which mechanical
considerations have a prominent place, must be inadequate, and will always
be bootless.” It is true that Matthews Duncan writes (Diseases of Women,
Lecture on Sterility), “The most generally recognized cause of sterility is
spasmodic dysmenorrhœa”; but a careful perusal of the whole lecture will
show that Duncan is saying more than he really means in using the word
“cause,” and that what he wishes to insist upon is the frequent and indisputable
association of the two conditions. In the lecture on Spasmodic
Dysmenorrhœa he writes, “Latterly it has been generally described as
obstructive or mechanical dysmenorrhœa; these words ‘obstructive’ and
‘mechanical’ implying a theory of the disease which ... I am sure is
quite erroneous.” Obviously, then, Kisch does injustice to Matthews Duncan
when he writes that the latter is “compelled to admit” (obgleich Duncan
selbst zugeben muss), what he was as a fact one of the first to maintain,
in the face of considerable opposition!—Transl.
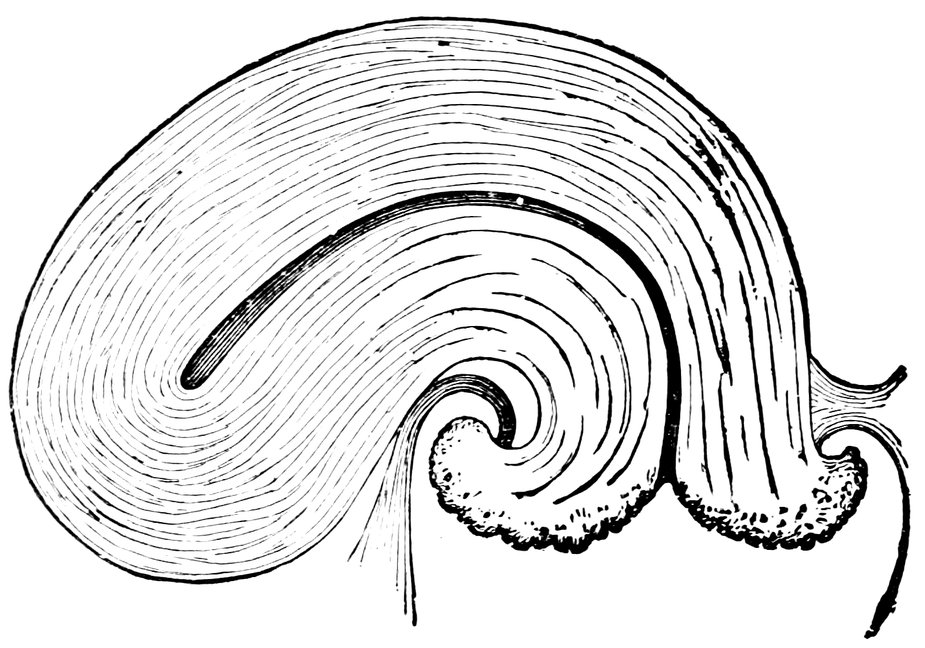
Fig. 79.—Ectropium in a Case of Bilateral Laceration of the Cervix. After A. Martin.
Duncan goes so far as to maintain that no actual or suspected
local disturbance has such significance in connexion with the doctrine
of sterility as spasmodic dysmenorrhœa. It possesses this significance
owing to the probable connexion between the dysmenorrhœic
neurosis and the outflow of the semen, the deficiency of the
sexual impulse and of sexual pleasure, and other disturbances of
sexual excitement during coitus. With the relief of the dysmenorrhœa,
we have, Duncan holds, made a long stride towards the cure
of the sterility. Among 332 married women who were absolutely
sterile, Duncan found 159, nearly half of the total number, who were
affected with spasmodic dysmenorrhœa.
515Burton, in order to ascertain with certain beyond question
whether stenosis of the external or internal os gives rise to dysmenorrhœic
troubles, examined six women during menstruation and at
the time when they were experiencing the greatest pain; he found in
no one of them any trace of narrowing of the canal. Owing to the
congestion that occurs at this time, the uterus becomes erect, and
any moderate flexion that may exist is temporarily straightened. In
all the cases, the sound could be passed with extreme ease.
Ectropium of the lips of the cervix (“granular erosion”) constitutes
a hindrance to conception which is by no means rare; the condition
is due to deep lateral lacerations of the cervix. The gaping
of the cervical canal arising from such old-standing, often overlooked,
cervical lacerations and from the parametric scars associated
therewith, causes various irritative manifestations: blenorrhoea,
blennorrhagia, cystic degeneration of the mucous membrane, and
these secondary conditions may be contributory causes of sterility;
but lacerations of the cervix with ectropium interfere in a manner
purely mechanical with the proper constitution of a receptaculum
seminis and with the aspiration of the semen into the cervical canal.
(Fig. 79.) In an earlier section of this work I laid stress on the
fact that in the act of conception the musculature of the cervix had
in a sense an active part to play; and the proper performance of this
role is prevented by cervical lacerations. The cervical glands also
suffer in cases of ectropium, and their function in facilitating the
entrance of the spermatozoa into the uterine cavity is no longer
properly performed. Finally, it is worthy of note that sexual gratification,
the sensation of voluptuous pleasure during the sexual act,
seems to be diminished in women with cervical lacerations, a fact
noted especially by Mundé and Ill. The last-named found that in
34 women thus affected, sexual gratification was no longer experienced
in intercourse; whilst in 27 of these cases, restoration of the
integrity of the cervix by operation was followed by return of normal
sexual feeling. In women who have given birth to one or two
children, and then for a long time have remained barren, we not infrequently
find deep cervical lacerations. Breisky, Spiegelberg,
Schultze, and Goodell have operated in such cases, and shortly after
the operation pregnancy has recurred.
Displacements of the Uterus.
With less justice than in the case of the pathological changes in
the cervix above described, it is maintained that displacements of
the uterus form a very frequent cause of mechanical hindrances to
conception, and thus give rise to sterility.
It certainly cannot be denied that displacements of the uterus are
found very commonly in sterile women; and, on the other hand,
516among women with pathological flexion of the uterus, the percentage
of the sterile is far higher than among women with a uterus
normal in position and shape—but from these facts it would be
erroneous to infer the general conclusion that displacements of the
uterus offer a mechanical hindrance to conception. The casual connexion
is less simple than this as a rule. In most cases in which
displacements of the uterus are associated with sterility, there are
additional pathological states of the uterus and its environment,
relics of previous inflammation in the uterus, the uterine annexa, or
the parametrium, or displacements of the uterine annexa; these
changes may be either the cause or the result of the existing displacement
of the uterus, and it is upon them, and not primarily
upon the displacement, that the sterility depends. The accuracy of
this view is proved by the experience, by no means an uncommon
one, that in such cases, when the actual cause of the sterility is removed,
the woman will become pregnant, although the displacement
of the uterus persists.
How difficult it is, in a particular case, to determine whether the
pathological anteflexion is the true obstacle to conception, or the
antecedent parametritis posterior and the concomitant metritis and
endometritis! How can we decide whether a retroflexion is the
simple mechanical cause of sterility, or whether the latter condition
does not rather depend upon complicating perimetritis and oophoritis?
On the other hand, we must not fly to the other extreme, and
absolutely deny that a displacement of the uterus can be the mechanical
cause of sterility. We meet with cases in which we are forced
to assume that the flexion interferes both with the outflow of the
menstrual blood and with the ingress of the seminal fluid. And
this is true, not merely of flexion to an acute angle, often associated
with infantile dimensions of the cervical canal or of the external or
internal os, but also of those advanced degrees of flexion in which,
doubtless in part also from the accompanying catarrh, complete stenosis
of the os uteri externum has resulted. The combination of
displacement of the uterus with stenosis of the cervix, is in these
cases the essential hindrance to conception. When the os is reasonably
large, a moderate flexion of the uterus forwards, backwards, or
to one side or the other, will not often prevent conception, for the
action of the muscular bands in the various ligaments of the uterus
will retain the os in a sufficiently favourable position. But if a contracted
os is associated with flexion, sterility is very likely; and
almost inevitable, if fixation of the flexed uterus has occurred from
inflammatory exudation and fibrosis in one of the broad ligaments.
That the belief that displacements of the uterus constitute an
obstacle to conception is a widely diffused one, is shown by the fact
517that among certain nations a means employed for the prevention of
pregnancy is the artificial production of displacements of the uterus.
Of the displacements of the uterus, the versions, anteversion, retroversion,
and lateral version, have a more pronounced influence in
hindering conception than the flexions; for, in the case of version of
the uterus, the uterus moves as a whole round a horizontal axis, so
that when the fundus moves in one direction, the portio vaginalis
moves in the opposite. When the neck of the uterus is thus displaced,
the tip of the glans penis fails during coitus to come into
contact with the os uteri externum, as it normally should do, and
passes into a vaginal cul-de-sac, in retroversion, the posterior fornix,
in anteversion, the anterior fornix, and in lateral version the lateral
fornix of the side opposite to that towards which the cervix uteri is
directed. In high degrees of this malposition, the vaginal fornix
covers up the os externum as with a valve. (Beigel.)
Von Scanzoni has especially insisted upon the frequency with
which sterility results from chronic metritis complicated with anteversion.
In 59 sterile women affected with chronic metritis, he
found in 34 instances more or less pronounced anteversion, and
hence was led to infer that this particular combination of disorders
plays a great part in the production of sterility.
Especially frequent is sterility in cases of anteversion of the uterus,
if in addition there is some contraction, even though moderate in
degree, of the os uteri externum; this combination of disorders is
one extremely unfavourable to the entrance of the spermatozoa into
the uterus.
Flexion of the uterus offers less hindrance than version to the
entrance of the spermatozoa, for the reason that in the former condition
the relations between the vaginal portion and the glans penis
during coitus are not affected. But when the flexion is extreme in
degree, the cervical or uterine canal may at some point become absolutely
impassable for the spermatozoa; and further, extreme flexion
is apt to lead to the occurrence of parametritis and perimetritis.
But, generally speaking, flexions of the uterus are far less often the
cause of sterility, than was formerly supposed. It used to be believed
that flexion of the uterus was followed by stenosis of the os
uteri externum, by which the outflow of the menstrual blood and the
ingress of the semen were equally prevented. It is true that infantile
acute-angled flexion of the uterus is often associated with infantile
stenosis of the cervical canal or of the internal or external os; and
it is also true that extreme degrees of flexion associated with uterine
catarrh, favour the occurrence of stenosis and obliteration of the
external os; but B. Schultze rightly insists that in most of the cases
in which a diagnosis is made of stenosis of the uterine canal associated
with a flexion of the sexually mature uterus, the supposed
518“stenosis” merely represents the difficulty which has been experienced
in passing the customary rigid uterine sound past the angle in
the uterine canal. Still, the fact remains, that among women with
uterine flexion there is a larger percentage of sterile individuals than
among women whose uterus is normal.
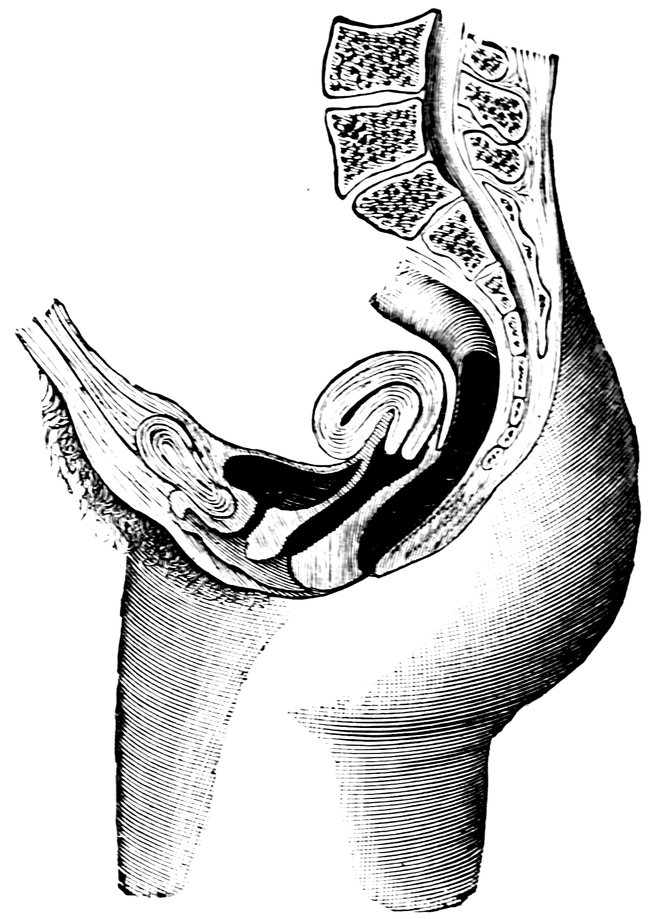
Fig. 80.—Anteflexio Uteri. After A. Martin.
As regards anteflexion of the uterus, either the congenital, uncomplicated
anteflexion of the uterus, due to developmental anomaly, or
the acquired form, due either to subinvolution of the uterus during
the puerperium, or to parametritic or perimetritic processes,—may
offer mechanical obstacles to conception, and thus give rise to sterility;
sterility with anteflexion occurs especially in cases in which the
anteflexion is dependent upon parametritis posterior, associated with
metritis and endometritis, or when any other complication is present
to make the flexion a severe one. In some sterile women, we find
anteflexion associated with supravaginal elongation of the portio,
and in such cases both states would appear to result from catarrh
of the uterine mucosa. How frequent is the combination of anteflexion
of the uterus with sterility, is shown by the figures published
by Sims, who in 250 cases of congenital sterility found 103 cases of
anteversion, and in 255 cases of acquired sterility found 61 cases of
anteversion.
519Fritsch writes in the following terms regarding the difficulty with
which impregnation is effected in women suffering from anteflexion
of the uterus: “In cases of anteflexion of the uterus, the vagina is
remarkably long, the portio vaginalis often badly formed; the ejaculated
semen flows away rapidly from the contracted vagina, without,
perhaps, ever coming into contact with the portio vaginalis.” He
states it as a fact that women with anteversion conceive less readily
than those with retroversion of the uterus (when this latter is
moderate in degree); for in slighter degrees of retroversion, the
axis of the uterus is a continuation of the axis of the vagina, so that
the orifice of the male urethra and the os uteri externum will be in
contact during intercourse—more especially because in such cases,
owing to the portio vaginalis being low in the pelvis, the vagina is
short; in cases of anteversion, on the other hand, the cervix is high
up, and the vagina is long and narrow. Fritsch considers that generally
speaking the fact that the internal or the external os is small is
of little importance; but the serious factors, those leading to sterility
in cases of anteversion—apart from all other considerations—are
the unfavourable high position of the portio vaginalis, the occlusion
of the os by the close application of the posterior vaginal wall, and
the presence of glutinous mucus in the cervical canal. Since in
cases of anteflexion we very commonly find hypersecretion of the
uterine mucous membrane, whilst, owing to the narrowing of the
external os, the mucus is unable to flow freely away, but accumulates
and becomes inspissated, we have the uterine mucous membrane
covered with a tenacious coating, which may perhaps render
the implantation of the ovum a very difficult matter, even though
the upward passage of the spermatozoa be still possible. The clinical
association of pain produced by drawing forward the portio vaginalis,
with marked anteflexion of the uterus, dysmenorrhœa, and
sterility, is a strikingly common one.
Schröder points out that, although sterility is common in cases
of anteflexion, cases are yet seen in which, notwithstanding the existence
of extreme anteflexion, conception occurs very speedily after
marriage. The fact that in cases of anteflexion we have difficulty,
not impossibility, of conception, explains how it is that of two
women suffering from anteflexion of the same severity, one will
readily become pregnant, whilst the other remains permanently
barren.
Retroversion and retroflexion offer obstacles to conception chiefly
in cases in which this displacement is a congenital anomaly, or when
it has developed immediately after puberty; or when complications
exist, especially when the retroflexed uterus is fixed by exudation.
In nulliparae, these deviations backwards will not rarely be found
to be the cause of the sterility. Much less often does sterility ensue
520when retroversion or retroflexion occurs in women who have already
given birth to several children, i. e., when the displacement is a puerperal
disorder; the reason why such cases are not often sterile, is to
be found in the fact that the wide cervical canal favours the passage
of the spermatozoa, and the softness of the tissues prevents any
serious obstacle to their upward progress being offered at the angle
of flexion; on the other hand, severe retroflexion in a woman who
has not yet borne a child offers a serious hindrance to conception,
on account of the smallness of the cervical canal, and the sharp
flexion of the more rigid uterus.
In general, then, retroflexion can be regarded as offering but a
slight hindrance to conception. In fact, many women with retroflexion
become pregnant again and again, and may abort several
times in a single year. When in parous women suffering from retroflexion,
sterility ultimately occurs, B. Schultze considers that it is
not the retroflexion which is primarily to blame, but rather the
secondary consequences so common in this disorder: uterine catarrh;
the general constitutional debility due to such catarrh, and to the
accompanying menorrhagia; perimetritis, and oophoritis.
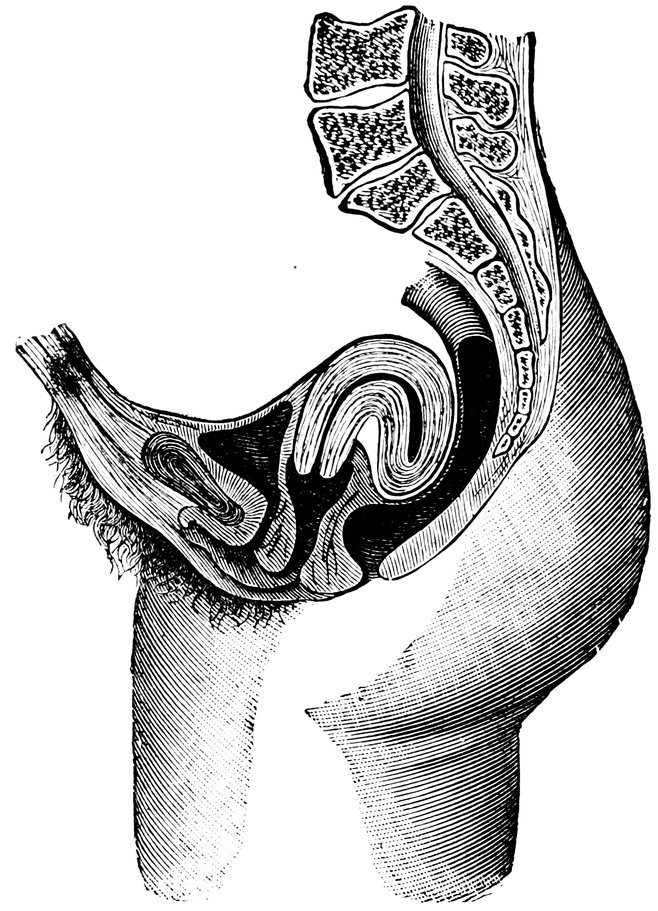
Fig. 81.—Retroflexio Uteri. After A. Martin.
Retroflexion and retroversion of the uterus occur chiefly in women
who have previously given birth to children; the bend is commonly
521obtuse or right-angled, and above the upper end of the cervical canal;
sterility in such cases, usually acquired, has a favourable prospect
of cure. As Kehrer points out, sterility appears to be constant only
in cases of retroflexion in which the uterus is fixed; the reason probably
is that by the backward inflexion of the uterus the abdominal
orifice of the Fallopian tube is dragged away from the ovary, and thus
the ovum, when it is discharged from the follicle, fails to find its way
into the tube.
Among 57 cases of retroflexion of the gravid uterus, E. Martin
found that in 6 the patient was pregnant for the first time, from
which it may be inferred that the anomaly existed prior to the occurrence
of conception.
That in some cases of sterility it is the retroflexion of the uterus
that is to blame, is shown very clearly ex juvantibus, inasmuch as
reposition of the uterus and maintenance of the organ in its proper
position relieves sterility perhaps of long standing, together with all
the other troubles secondary to the displacement of the uterus. As
an example, I quote one case from among several of the kind of
which I have notes. Mrs. N., 25 years of age, married 6 years,
childless, suffers from severe dyspeptic troubles, leading to emaciation
and profound depression. She has been treated fruitlessly for
gastric catarrh, but has not previously been subjected to gynecological
examination. I insisted on making such an examination, and
found the uterus somewhat enlarged and completely retroflexed.
The successful replacement of the organ was followed by the cessation
of the previously constant vomiting after meals, and by the
disappearance of the other dyspeptic troubles; shortly afterwards the
lady became pregnant, and pregnancy ran a normal course. Since
then, she has had three children; there has been no recurrence of the
dyspepsia.
According to Sims, retroversion of the uterus is frequently associated
with sterility. Among 250 married women who had never
been pregnant, we found no less than 68 cases of retroversion;
among 255 women who had had one or more children, but had then
ceased to be fruitful, he found 111 cases of retroversion; and in
some of these cases the retroversion was uncomplicated. Grenser
and Vedeler also found retroflexion to be a common cause of sterility;
the last-named, examining 7 nulliparous married women, found
retroversion in 5; in these cases, however, there was associated disease
of the uterus or of its environment.
Inversion of the uterus, even in the minor degrees of the affection,
in which coitus is still possible, almost invariably causes sterility,
owing to the occlusion of the uterine orifices of the Fallopian tubes.
Moreover, in inversion of the uterus, the position assumed by the
os uteri externum is such as to render the entrance of the semen
522almost impossible. Finally, when the uterus is inverted, the mucous
membrane undergoes changes which render it unfit for the implantation
of the ovum; the researches of P. Ruge show that it is thinned
and that the epithelium is cast off and replaced by granulation tissue.
In cases in which the inverted uterus has long projected through the
genital fissure, its surface becomes covered by a multilaminar pavement
epithelium; at the same time, the glandular apparatus undergoes
atrophy, only the fundi of the glands being preserved, and the
muscular substance is hypertrophied. None the less, in exceptional
cases, which have been reported by Emmet, Macdonald, and Tyler-Smith,
pregnancy has occurred after long-enduring inversion of the
uterus. Lauenstein had a patient in whom an inverted uterus was
replaced after a year and a half; the following week she became
pregnant. Stevens saw a case in which the woman became pregnant
six months after the reduction of an inversion of the uterus of
nine months’ standing.
Prolapse of the uterus is seldom the cause of sterility, inasmuch
as during coitus replacement of the organ is effected. It may even
be said that in cases of prolapse, the low position of the uterus and
the enlargement of the os uteri externum, favour the direct ejaculation
of the semen into the cervical canal (likewise enlarged), and
that thus the conditions are advantageous for impregnation. In
fact, conception more commonly occurs in cases of prolapse than
might have been anticipated in view of the various consecutive disorders
apt to complicate this affection—chronic metritis and endometritis,
erosion, hypertrophy of the cervix, displacement and laceration
of the annexa, etc. The extent to which the capacity for conception
is unfavourably affected in cases of prolapse of the uterus,
is proportional to the amount of descent undergone by the uterus,
for the nearer the os approximates to the vaginal orifice, the farther
removed from the os will be the point at which the semen is ejaculated.
In cases of complete prolapsus it has happened that coitus
has been effected directly through the everted os uteri, and has resulted
in conception; a case of this kind is reported by Hervey.
Unbiassed gynecological experience in no way supports the views
of Sims and Hewitt regarding the frequency with which displacements
of the uterus constitute mechanical causes of sterility. Sims
supports his views with the figures previously quoted, from which
the following table is compiled:
|
No. of cases. |
Anteversion. |
Retroversion. |
Total cases of displacement. |
| First class |
250 |
103 |
68 |
171 |
| Second class |
255 |
61 |
111 |
172 |
| |
|
|
|
|
| Totals |
505 |
164 |
179 |
343 |
| |
|
|
|
|
523From this it appears that in the 1st class, among 250 married
women who had never given birth to a child, there were 103 cases
of anteversion, and 68 cases of retroversion; whilst in the 2nd class,
among 255 women, who had had children, but for one reason or
another had become unfruitful earlier than the natural age for this
occurrence, there were 61 cases of anteversion, and 111 cases of retroversion.
The general result of these figures is to show that two-thirds of
all sterile women, without regard to the especial cause of the displacement,
suffer from one form or the other of uterine displacement,
and that the relative frequency of anteversions and retroversions
is reversed in the two classes, the nulliparous married women,
and the married women previous parous but latterly become sterile,
respectively.
Hewitt similarly regards malpositions of the uterus as frequent
causes of sterility. He analysed 296 cases of flexion and version of
the uterus treated by him at University College Hospital during the
years 1865 to 1869, partly in the wards, and partly in the out-patient
department. Of these 296 women, 235 were married; 100 were
cases of retroflexion, and 135 were cases of anteflexion. Of the 235,
81 had had no full-term children, 57 of the 81 having never been
pregnant, and the remaining 24 having had miscarriages only. Of
the remaining 154, married and parous women, a large proportion
were sterile at the time when they applied for treatment; though in
the years immediately after marriage they had given birth to one
or more children, they had subsequently ceased to be fruitful.
All that these figures prove to an unbiassed judgment is, however,
that displacements of the uterus are apt to render conception
difficult; or that, in addition to other pathological states of the pelvic
organs, they are frequently met with in sterile women—but in and
by themselves, displacements of the uterus do not offer any very
serious or very frequently occurring obstacle to conception.
That conception is possible in spite of the very notable mechanical
hindrances which certain displacements of the uterus may offer to
the occurrence of pregnancy, is shown by many striking examples
in gynecological literature. Winckel, Olshausen, and Holst have
all seen pregnancy occur in women who at the time of conception
were wearing intra-uterine pessaries; and von Scanzoni has published
cases in which fertilization took place, notwithstanding extreme
anteversion which stenosis of the os uteri, and in another
instance, notwithstanding the presence of a polypus filling the
external os.
Myoma of the Uterus.
Among the mechanical obstacles to conception which act by preventing
or rendering difficult the contact of spermatozoon and
524ovum, must be enumerated uterine myomata, and these must therefore
be included among the causes of sterility.
According to their number, their size and their situation, uterine
myomata give rise to different and manifold mechanical disturbances.
When there are numerous intramural myomata, even when
these are of a moderate size, the uterine cavity becomes bent and
narrowed, and retention of the secretions may ensue, often lasting
for a lengthy period. Submucous fibromyomata, when situated low
down, near the internal os, may occlude this orifice completely;
when implanted higher up in the uterine cavity, they are apt to
cause flexion of the uterus; large, pedunculated fibromyomata of the
uterus may descend into the vagina and narrow this passage.
Myomata interfere with conception in very various ways. Mechanically,
they may occlude the uterine orifices of the Fallopian
tubes, or may give rise to displacement of either tubes or ovaries,
or, again, by blocking the uterine cavity, they may hinder the
descent of the ovum and the upward passage of the spermatozoa;
their presence may cause catarrhal disease of the uterine mucous
membrane, or give rise to profuse hemorrhage, and either of these
secondary changes may interfere with the implantation of the ovum;
and there is yet another way in which myomata may interfere with
conception, and give rise to sterility—this is a subject to which
especial attention has been given by Winckel, and to which we may
here most conveniently allude. The continued growth of small
submucous myomata often gives rise to a hyperæsthetic state of the
genital organs analogous to vaginismus, and this interferes with
coitus. Large myomata, on the other hand, give rise to catarrhal
states of the uterine cavity and to hyperplasia of the mucous membrane,
constituting hindrances alike to conception, and to the implantation
and further development of the embryo if fertilization
should be effected; moreover, the growth of large myomata often
causes perimetritis, perisalpingitis, and perioophoritis, and these,
partly by abnormal fixation of the uterus, and partly by closing up
the tubes and so thickening the tunics of the ovary as to prevent
the rupture of the graafian follicles, give rise to sterility.
The existing statistics regarding the relation of the growth of
myomata of the uterus to fertility, incomplete as they are and
lacking in exactitude, suffice nevertheless to show that the fruitfulness
of women suffering from uterine myomata is notably diminished
by the growth of these tumours; more particularly, we learn
that whilst the number of women with uterine myomata who have
one child is sufficiently large, the number of multiparae thus affected
falls greatly below the average of fertility. A characteristic feature
of the influence of myomata in producing sterility is clearly
shown by the statistics, inasmuch as pregnancy is comparatively
525common in the case of women with subserous myomata, in whom
the uterine cavity and mucous membrane are as a rule least affected,
whilst fertility is far more seriously impaired in the case of women
with submucous myomata.
West, in the case of 43 married women with myomata of the
uterus, found 7 childless; the remaining 36 had in all given birth
to only 61 children, and 20 of these had only one child each. Of
Beigel’s patients, 86 married women with uterine myomata, 21
were sterile; of McClintock’s 21 patients similarly situated, 10
were sterile. Von Scanzoni’s investigation showed 38 sterile women
among 60 married women suffering from myoma uteri; Michel, 26
sterile among 127; Winckel, 134 sterile among 415. From a table
showing the number of children born to each of 108 women with
myoma uteri of whom 46 were observed by Winckel, and 62 were
in Süsserott’s collection, it appears that on an average 2.7 children
were born to each woman thus affected, whereas in Saxony the
average number of children born to each married woman is 4.5.
Many other gynecologists have published statistics regarding this
matter, Gusserow, Röhrig, Schröder, E. von Flamerdinghe, and
others, some of them dealing with a very large number of cases,
and all show that 30% and upwards of married women with uterine
myomata remain sterile.
On the other hand, Hofmeier maintains, in opposition to the
prevailing view, that in the great majority of cases myomata are
not to be regarded as giving rise to sterility. His investigation
embraced 313 persons, of whom 25% were unmarried, and 75%
married, and of these latter, 25 to 30% were sterile. (It must be
pointed out that compared with the average percentage of sterile
marriages—about 10%, this figure of 25 to 30% is a very high one.)
From a comparison of the age of the sterile married woman with
the duration of married life in each case, Hofmeier is led to believe
that it is not the myomata which have exercised an influence unfavourable
to fertility, and that the occurrence of sterility in these
cases is referable to other causes. The origination of myomata
he regards as etiologically independent of the exercise or non-exercise
of the sexual act. The apparently overwhelming preponderance
of the occurrence of myomata in unmarried and in
sterile married women is, he thinks, to be explained by the fact
that unmarried women and nulliparous married women seldom have
occasion to consult a gynecologist, but that the one condition that
renders it necessary for them to do so is the growth of a uterine
myoma. Generally speaking, pregnancy seldom occurs after the
age of 35 years, precisely the age at which the growth of uterine
myomata begins to be common. If, however, at this comparatively
late age pregnancy does occur, it is so often found to be complicated
526by the presence of a uterine myoma, that Hofmeier is even led to
infer that the presence of such a tumour must have a certain favouring
influence upon the occurrence of conception; the facilitation of
conception in these cases he explains by the fact that the growth
of the tumour renders the blood-supply of the whole reproductive
apparatus more active than is normally the case, and protracts the
duration of ovarian activity.
Diseases of the Vagina and the Vulva.
Various pathological states of the vagina and vulva may cause
incapacity for fertilization by rendering copulation impossible.
Such states may be either congenital or acquired.
In rare cases the hindrance consists in abnormal smallness of
the vulva, but this condition is usually associated with other defects
in development of the reproductive organs, which combine to give
rise to sterility. Congenital adhesion of the labia minora and
majora is sometimes met with, with or without atresia of the
urethral orifice, the connexion between the labia may be superficial
and epithelial merely, as in a case recorded by Ziemssen; or
the labia may be firmly united throughout their whole thickness.
Much less common is acquired adhesion of the labia, causing atresia
vulvae, and rendering coitus difficult or entirely impossible. Various
other abnormalities of the reproductive organs which may give
rise to sterility have already been described in the section on the
pathology of cohabitation, these are: abnormalities of the hymen;
anomalous formation and hypertrophy of the labia; excessive size
of the clitoris; anomalies of the vagina, its absence, stenosis, atresia,
duplication, and abnormal termination.
More detailed mention must, however, be made here of vesico-vaginal
fistula as leading to sterility. Such a fistula is rightly regarded
as one of the conditions preventing conception, but it does
not render the occurrence of pregnancy absolutely impossible. It
will readily be understood that the unpleasant symptoms commonly
met with in these cases, will be apt to deprive both husband and
wife of inclination toward sexual intercourse; again, apart from
this psychical influence, the functions of the female reproductive
apparatus are commonly disturbed to a very serious degree by the
existence of a vesico-vaginal fistula; and, finally, the unfavourable
influence of the urine on the semen must also be taken into consideration,
for, as an acid fluid, the urine will notably check the
activity of the movements of the spermatozoa—still, notwithstanding
all these unfavourable influences, conception will sometimes
nevertheless occur in such cases. But of those who acquire a vesico-vaginal
fistula as the result of a difficult labour, a very small proportion
only will again become pregnant.
527Freund draws attention to Simon’s experiences, reminding us
that the latter, in his cases in which women with vesico-vaginal
fistula become pregnant, invariably saw the pregnancy terminate
in abortion or premature labour; but still, Freund quotes also a
case of Schmitt’s, and mentions another of his own, showing that
this premature termination of the pregnancy is not absolutely inevitable
in such circumstances. Schröder, indeed, goes far in the
opposite direction, and writes: “Such women not rarely become
pregnant, and their pregnancy usually runs a normal course.”
Kroner made a statistical investigation of the question, and found
that of 60 women suffering from vesico-vaginal fistula, 6 became
pregnant during the persistence of the fistula. Winckel reports a
remarkable case in which, after the ordinary means of curing the
fistula had been vainly tried, transverse obliteration of the vagina
was undertaken; the operation was not completely successful, as a
small passage remained patent; the patient returned home for a
time, and became pregnant, the spermatozoa having found their
way through this passage. Simon reports another noteworthy case,
that of a woman 57 years of age, with a vesico-vaginal fistula close
to the external os; during the 26 years the fistula had lasted she had
complained of cessatio mensium; when the fistula was closed by
operation, she again began to menstruate.
Sometimes we meet with abnormalities of the vagina—not
strictly speaking morbid states—which, though they may not at
first sight appear to be of much significance, yet suffice to render
conception difficult, or even impossible. One of these conditions is
extreme shortness of the vagina, leading to the formation of a
“poche copulatrice” (Courty), in which during coitus the semen
is ejaculated at a distance from the os uteri externum; another is
excessive length and width of the vagina; another, some displacement
of the vagina which diminishes the prospect that the semen
will enter the cervical canal. Such vaginal false passages, “fausses
routes vaginales,” have been described more especially by Pajot as
causes of sterility.
Another cause of sterility is the rapid outflow of the semen after
coitus, either in consequence of dyspareunia, or on account of some
abnormality in the configuration of the vagina, or, finally, owing to
deficient action of the constrictor cunni (or bulbocavernosus muscle)
and the muscles of the pelvic diaphragm. In cases of profluvium
seminis, the woman herself will often call the physician’s
attention to the defect.
Many cases of sterility depend upon a cause the recognition of
which in this connexion is comparatively recent, namely, the hermaphroditism
of the person concerned. Witness the following case
described by Dohrn: The individual had been baptised and brought
528up as a girl. At the age of twenty years she began to suffer from
a distressing sensation of pressure, recurring at intervals of four
weeks. A local examination was made by a physician, who assured
the mother that “there was no hindrance to menstruation, but
that when she married an incision would become necessary.” After
a time she became engaged and was married; and shortly afterwards
her husband demanded a renewed gynecological examination.
This was undertaken by Dohrn, who declared that the supposed
girl was of the male sex. The external reproductive organs had
the feminine form. The labia majora were large and well-formed;
in the anterior extremity of each labium was a rounded, sensitive,
soft body, of the size of a large bean, which was capable of being
drawn forwards towards the abdomen; the labia were beset with
muscular fibres; the clitoris was 4 cm. (1.6 in.) in length, resembling
an imperforate infantile penis, it was slightly erectile; in the
vestibule there were two openings, the anterior of which was the
urethra, the posterior led into a blind passage 2 cm. (0.8 in.) in
length, representing the fused lower extremities of the ducts of
Müller; per rectum no trace could be found of vagina, uterus, or
ovaries, but also no trace of prostate. The marriage, in which this
individual declared himself to be happy, was annulled. Leopold
observed a similar case, in which the individual had lived as a wife
for the space of 25 years. Another striking case is recorded by
Steglehner. As Zweifel remarks, to decide the true sex of such
individuals is often extremely difficult. “At the present day, indeed,”
he continues, “it is no longer the fate of those who from no
fault of their own have had imposed on them the name and upbringing
of another sex than that which is truly theirs, and who
have thus been led to contract marriage with one who in reality is
of their own sex, to be treated with the horrible injustice which was
meted out to them in the middle ages, when, as we learn from contemporary
writers, they were haled before the bar of “ecclesiastical
justice,” charged with profaning the sacrament of marriage, and
threatened with death at the stake—but even now a mistake in the
decision of an infant’s sex entails in later life a thousand distresses
and inconveniences.”
Recently, Neugebauer has made as complete a collection as possible
of all the recorded cases of hermaphroditism.
Secretions of the Genital Organs.
The constitution of the secretion of the vaginal mucous membrane,
or of the secretion formed in the cervical canal, or both of
these in combination, may constitute hindrances to the normal contact
of spermatozoon and ovum.
529The secretions of the female genital organs are manifold. The
outer surface of the labia majora is covered with skin, containing
sebaceous and sweat glands; but the inner surface of the labia
majora and the rest of the external genital organs are covered with
mucous membrane, the outer stratum of which consists of stratified
pavement epithelium; this epithelium contains sebaceous glands
and mucus glands. The intermixture of the secretions of these
glands with the epithelial scales which are constantly being cast off
in large numbers, constitutes the whitish material with which this
region is smeared, known as “smegma.” A mucus secretion of
a fluid consistency is discharged from the vulvo-vaginal glands
known by the name of Bartholin’s glands.
The mucous lining of the vagina is poor in glands; it contains
very numerous papillæ, which do not, however, project from the
surface of the membrane, since the depressions between the papillæ
are filled in by the stratified epithelium with which the entire extent
of the vaginal mucous membrane is covered. The secretion of the
vaginal mucous membrane is a fluid of thin consistency with an
acid reaction; the admixture of numerous morphological elements,
in the form of epithelial cells cast off from the superficial layers of
the stratified epithelium, often, however, makes the vaginal secretion
thick and opaque. The epithelial lamellae are frequently covered
with heaps of lepthothrix granules, and among the granules are
seen vibriones and bacteria and also numerous lepthothrix threads
of varying length.
The same stratified epithelium extends on to the neck of the
uterus to a distance which varies in different individuals; gradually,
however, the number of layers diminishes, the flattened cells give
place to thicker, prismatic cells, until we have a single-layered prismatic
epithelium; finally the cells become columnar and ciliated,
and this columnar ciliated epithelium covers the whole of the interior
of the uterus. The mucous lining of the cervical canal contains
numerous mucous glands, some of which are simple tubular
glands, whilst others are racemose; they are lined with columnar
ciliated epithelium, and secrete a dense, gelatinous, alkaline mucus,
containing a few epithelial cells and occasional leucocytes. The
mucous membrane of the uterine cavity is beset with simple tubular
glands, lined with a single layer of prismatic epithelium; these
glands secrete a grayish alkaline fluid. The secretion formed in
the uterine cavity is thinner in consistency than that formed in the
cervical canal.
Normally, the secretion of the vaginal mucous membrane is not
more than is sufficient to keep the surface of the canal moist and
slippery; it is a thin fluid of an acid reaction, and almost as clear
as water. Shortly before and after menstruation, the secretion of
530the vaginal mucous membrane becomes more abundant; it is even
thinner than at other times; the reaction remains acid. The secretion
of the cervical canal is normally, in the absence of sexual
intercourse, small in amount, so that a free flow of secretion from
the os uteri externum is by itself sufficient to indicate that the mucous
membrane of the canal is in an abnormal condition. The vitreous,
gelatinous, alkaline mucus secreted by the glands of the cervical
canal is normally retained within the canal, and is seen on examination
with the speculum to fill the os uteri externum. In consequence
of the congestion of the uterus that occurs during menstruation,
and for the same reason during sexual excitement, the
secretion of the cervical canal is more abundant, it also becomes
less tenacious, and flows out through the os into the vagina. But
this evacuation of the cervical secretion through the os is a normal
occurrence only during menstruation and as a result of sexual intercourse;
in these circumstances it appears in the form of a clear
or somewhat yellowish drop of fluid exuding through the os uteri
externum.
In catarrhal states, the secretions of the genital passage, like
those of other mucous membranes, become abnormal. There is an
increase in the number both of epithelial elements and of leucocytes;
and in very acute catarrhs, erythrocytes also mingle with the secretion.
On microscopical examination we find that the catarrhal
secretion differs in its characters according to the part from which
it is derived: the mucus from the cervical canal forms gelatinous
accumulations; that from the vaginal mucous membrane forms thick
opaque masses; and in the mixed secretion which exudes from the
vulva, we find also smegma from the external genital organs. In
addition to cells from the laminated epithelium, we see often young
cells, somewhat oval or polyhedral in form, with granular protoplasm,
and a vesicular nucleus. In some inflammatory states,
pus corpuscles will also make their appearance. Various micro-organisms
are in addition to be found in the catarrhal secretions.
The reaction of the vaginal secretion is normally faintly acid;
should it become strongly acid, the movements of the spermatozoa
are immediately suspended. The mucus of the cervical canal, the
alkaline reaction of which is extremely favourable to the onward
movement of the spermatozoa, may, owing to catarrhal processes,
be so altered that it becomes acid; it then destroys the spermatozoa,
and gives rise to sterility. This fact can sometimes be proved by
microscopical examination. In several cases in which endometritis
existed in sterile women I made a microscopical examination of the
cervical mucus shortly after the completion of sexual intercourse;
and in a number of these, no living spermatozoa were to be seen,
but only dead, motionless spermatozoa (Fig. 82). I had, of course,
531in these cases, previously assured myself that the husband’s semen
was normally active.

Fig. 82.
Mucus from the Cervical Canal, taken one hour after sexual intercourse, from a woman suffering from chronic endometritis.
Among the epithelial cells, pus cells, and finely granular masses, we see a few motionless, dead spermatozoa.
According to Nöggerath, in cases of uterine catarrh, we may
find one of three different varieties of secretion. In some cases it
is small in amount, and very thin in consistency; in others, it is
moderate in amount, very thick, non-transparent, bright yellow, and
gelatinous in consistency; in the third class of cases, we have numerous
degrees of variation, starting from the normal, purely mucus,
transparent secretion, mixed with yellow flocculae, up to a secretion
which has almost the aspect of pure pus. The first described
variety is, according to Nöggerath, met with chiefly in women whose
uteri are small, with indurated tissues, and its discharge seems to
depend upon commencing atrophy of the mucous membrane. The
second form is the most obstinate, the catarrh being situated chiefly
in the cervical and probably also the uterine glands; whereas the
first variety of secretion is rather a serous transudation, and contains
very few formed elements. The third form is characterized
by extensive denudation of the superficial epithelium, and is mixed
with a smaller or larger quantity of pus.
Levy, who made microscopical examinations in sterile women
(39 cases), gives it as a “constant fact” that when the cervical
secretion contains epithelial and pus cells in large quantities, the
spermatozoa never retain for long their power of movement.
Whereas in examinations made repeatedly on healthy women 25
hours after sexual intercourse, he found numerous spermatozoa
532still in active movement, in women having a catarrhal discharge
with the characters just mentioned, five hours after intercourse the
movements of the spermatozoa had almost entirely ceased.
Not only may the secretions of the genital passage be injurious
to the spermatozoa by their quality, but further a very abundant
secretion may interfere with fertilization. In the first place a very
abundant secretion is apt to be very dilute, and if the spermatozoa
are immersed in a fluid of which the specific gravity is too low, they
swell up from imbibition of water, and their movements are suspended.
But excessive secretion, such as is sometimes met with
in cases of cervical catarrh, may also have a purely mechanical
deleterious action, by washing away the semen out of the vagina.
If, again, the quantity of the ejaculated semen is unusually small,
contact with the normally acid vaginal mucus may suffice to render
the spermatozoa speedily motionless. Finally, when the cervical
secretion is of a too tenacious consistency, so that it fills the os as
with a plug, the upward passage of the spermatozoa may be barred.
Such tenacious cervical mucus will give rise to sterility especially
in women who have not previously born children; whereas in
parous women, owing to the more patulous condition of the os, the
entrance of the spermatozoa is not so effectually prevented. The
same distinction between nulliparous and parous women must be
made, as von Scanzoni has pointed out, also as regards the production
of sterility by hypersecretion of uterine mucus. Women
who become affected with uterine blenorrhoea only after having had
one or more children, will readily become pregnant again; but
when such blenorrhoea affects a woman who has never been pregnant,
sterility almost invariably results.
Von Grünewaldt has drawn attention to a somewhat rare form of
chronic endometritis with tenacious secretion, leading to sterility.
The shape, size, and consistency of the uterus appear normal, the
organ is often virginal, but with the speculum we see exuding from
the os a greyish green, extremely tenacious secretion, which is wiped
away with difficulty. He saw 24 women affected with this disease;
10 of these had lived in marital intercourse for many years without
ever having become pregnant; in 10 others there was acquired sterility,
i. e., they had at first borne children after marriage, but had
subsequently ceased to be fruitful; in the remaining 4 it was not
possible to ascertain whether they were fruitful or sterile, since
two of them were living apart from their husbands, whilst in the
case of the other two only two years had elapsed since the birth of
the last child. In any case, not one of the women thus affected had
ever become pregnant subsequent to the time at which she acquired
this form of endometritis, notwithstanding the fact that in several
of the cases the symptoms were alleviated by treatment.
533We must here consider also the effect of gonorrhoeal infection in
giving rise to sterility in women. Sterility may arise from gonorrhoea
in women in various ways. Sometimes the abundance of the
cervical secretion is alone sufficient to prevent the entrance of the
spermatozoa into the uterus; in other cases the hindrance to fertility
depends upon the inflammatory conditions in the pelvis that so
frequently result from gonorrhoeal infection—perimetritis and
parametritis; it may be catarrhal changes in the tubes—salpingitis,
hydrosalpinx, and pyosalpinx—by which the contact between
spermatozoon and ovum is prevented. Chronic gonorrhoeal endometritis
may give rise to such changes in the uterine mucous
membrane as to unfit it permanently for the implantation of the
ovum, even should there be no obstacle to fertilization. Finally,
double gonorrhoeal oophoritis may result in rendering the formation
of mature ovum an entire impossibility—bringing about a
condition analogous to azoospermia in the male, and causing absolute
sterility. Although in many cases the detection of the gonococcus
affords indisputable evidence of the existence of gonorrhoeal
infection, it must be remembered that it is often difficult, and sometimes
entirely impossible, to make the diagnosis with certainty; and
for this reason it is possible that gonorrhoeal infection plays a
much larger part in the causation of sterility than has until lately
been believed.
The observant physician will in cases of sterile marriage frequently
find in husband or wife or both, evidence of previous or still
existent gonorrhoea; but he will cautiously weigh all the circumstances
before deciding that such gonorrhoeal infection is the
efficient cause of the sterility. In many cases, however, the
etiological relation is too obvious to be overlooked, and we can
trace all the distresses of the unfortunate wife to the injury she
unwittingly received upon the momentous wedding night.
Still, we have to remember how extraordinarily common, more
especially in the so-called upper classes of society, is gonorrhoeal
infection, and what an enormous percentage of men entering upon
married life have previously experienced one or more attacks of the
disease—so that were sterility a frequent sequel of such infection,
fertility would be the exception rather than the rule. By inquiry
among friends and patients as to whether when they married they
had previously suffered from gonorrhoea, in conjunction with information
regarding the fruitfulness of their marriages, I have been
led to the conclusion, which appears to me to be one of considerable
importance, that the proportion of sterile to fruitful women among
the wives of men who have suffered from gonorrhoea before marriage,
is about the same as the proportional fertility of all marriages
considered independently of gonorrhoeal infection, viz. 1 : 10. This
534depends, as it appears to me, not only upon the fact that very frequently
in men gonorrhoea is completely cured, but also upon the
fact that in women gonorrhoeal infection does not necessarily cause
sterility. It may indeed be regarded as definitely established that
women actually suffering from gonorrhoea may become pregnant,
and that the pregnancy may proceed to its natural termination.
The recent investigations regarding the frequency with which gonococci
may be detected in the genital secretions of pregnant and
parturient women—and they are to be found in a surprisingly
large percentage—suffice to prove that gonorrhoeal infection
offers no insuperable obstacle to conception. That the discovery of
gonococci in a man’s urethra does not justify us with apodictic
certainty in forbidding the man thus affected to marry is in fact
proved by the following remarkable case, which came within my
own experience. A young man who had had several attacks of
acute gonorrhoea, wishing to marry, had himself examined by two
specialists in genito-urinary disease. Both detected gonococci in
his urethra, and both forbade him to marry. The patient, however,
would not be advised, and married the lady of his choice; now, six
years after marriage, he is the happy father of four blooming children,
and his wife is in perfect health.
Gosselin, in an elaborate work published in 1853, was the first to
point out the serious consequences as regards a man’s future
potentia generandi which are entailed by an attack of gonorrhoea
followed by epididymitis. He insisted that the inflammation might
lead to the obliteration at some point of the vas deferens, whereby
the secretion of the testicle was prevented from mixing with the
secretions of the prostate, Cowper’s gland, and the seminal vesicle;
and hence the ejaculated sperm was lacking in its principal constituent.
In such cases, either in the epididymis (usually in the
globus minor of that organ), or else in the course of the vas deferens,
somewhere between the epididymis and the vesicula seminalis,
some relic of the former inflammation is usually to be detected,
the globus gonorrhoeicus, and this usually represents the seat of
strangulation of the excretory duct of the testicle.
In the year 1872 Nöggerath published his book, written with
flaming fiery zeal, entitled “Latent Gonorrhoea in the Female Sex.”
In the most startling colours he depicted all the misery and distress
which formed the wedding gift of the gonorrhoea-infected husband
to his wife; when sowing his wild oats, such a husband is preparing
for the crop by which his young wife’s happiness is destroyed, her
health ruined, her life endangered, and her hopes of offspring
annulled. While we may admit that Nöggerath’s motives were of
the noblest, we cannot but wonder that the wickedness of the male
sex has not yet entailed the destruction of the whole human race,
overwhelmed as by a new fall of Sodom and Gomorrah.
535Nöggerath maintained that 90% of men infected with gonorrhoea
remained uncured; and that of the women married by men thus
permanently infected with gonorrhoea, barely 10% remained free
from the disease. It is gonorrhoeal infection, of which this author
gives so gloomy a picture, which is, in his opinion, the principle
cause of sterility in women. According to his observations, of 81
women thus infected, 49 remained absolutely sterile; only 31 became
pregnant; 23 were delivered at full term, 3 had miscarriages,
and 5 premature delivery. Thus, not so many as 1 in 3 of these
women had a full-time child. Of the 23 who were delivered at full
term, 12 never had more than 1 child each; 7 had 2 children each;
3 had 3 children each; 1 only had 4 children, the normal average
fruit of healthy marriages. In all, the 81 women had only 39
children. If we take 4 to be the average number of the offspring
of a healthy married pair, there was but one normal woman among
the whole 81. Forty-nine were absolutely sterile; 11 of the remainder
had 1 child, and did not again conceive during periods
ranging from 3 to 18 years after the recorded delivery; thus there
were 60 sterile women among 81.
Nöggerath’s doctrine regarding the relation between gonorrhoeal
infection and sterility obtained at first little credence—perhaps for
the reason that he drew such far-reaching conclusions from so
limited a material—Schröder mentions Nöggerath’s opinions only
to dismiss them as extravagant; but the idea that the husband was
mainly to blame for the occurrence of sterility in marriage continued
to form the topic of scientific discussion. The indignation
which Nöggerath’s assertions, unquestionably too sweeping, had
aroused in gynecological circles, gradually subsided, as every
gynecologist devoted his attention to supporting or refuting Nöggerath’s
conclusions.
It soon became evident, that gonorrhoea in the male had a deleterious
influence upon the fertilizing quality of the semen, and this
far more frequently than had previously been supposed. Fürbringer,
as a result of the examination of 124 cases, laid down the
important proposition, that when epididymitis or funiculitis gonorrhoeica
duplex had been observed to occur, the probability that the
patient would be an azoospermist was expressed by the ratio of 9 : 1,
and this in direct opposition to the views of Zeissl, who had maintained
that in this respect the consequences of gonorrhoea were
trifling.
Seeligmann conducted a pathologico-anatomical investigation
which led him to conclude that in cases of gonorrhoeal epididymitis,
in addition to the inflammation of the epididymis, phlebitis and periphlebitis
of the plexus pampiniformis occurs, and also lymphangitis
of the extensive system of lymphatic vessels which pass through
536the spermatic cord from the testicle; the changes left in the blood
and lymphatic vessels by the inflammation, result in the testicle being
for the future imperfectly nourished, and often therefore lead to impairment
of the functions of this organ; thus the oligospermia so
frequently seen as a sequel of gonorrhoeal epididymitis (the ejaculated
semen containing but few spermatozoa, and these with little
or no vitality), is not always due to a complete obliteration of the
vasa deferentia by the inflammation, but in many cases to the functional
derangements of the testicle brought about in the manner
above described. It is probable also that lues may give rise to
azoospermia as a result of endarteritic processes. The remarkable
result of Seeligmann’s investigations was that in as many as
75% of the sterile marriages that came under his observation, the
husband was the one to blame.
Latterly, the view that gonorrhoeal infection plays a very considerable
part in the etiology of sterility in women, has been widely
accepted. Among German gynecologists, Olshausen, a man of
enormous experience, considers that Nöggerath’s book, notwithstanding
much exaggeration, is substantially accurate in its main
conclusions. A similar view of Nöggerath’s work is taken by E.
Schwartz, Bandl, A. Martin, and Hofmeier.
According to the exhaustive work of E. Schwartz, gonorrhoea is
in women one of the commonest causes of sterility. Sterility due
to this disease may be either primary or secondary. In some cases
no ovum can find its way into the uterus, either because the ovaries
are completely enveloped in masses of exudation and pseudo-membranes,
or on account of dislocation of the ovaries and the Fallopian
tubes, or because the tubes have been rendered impermeable by
inflammatory stenosis or flexion, or by loss of their ciliated epithelium;
in other cases the ovum, indeed, enters the uterus, but fails
to be implanted upon the diseased mucous membrane; again, it is
conceivable that even when ovum and spermatozoon are properly
formed and encounter one another in the normal manner in the
tube or in the uterine cavity, and when the uterine mucous membrane
is in a condition suitable for the implantation of the fertilized
ovum, contact with gonorrhoeal secretions may have impaired the
vitality of the ovum or of the spermatozoon, or of both, to such a
degree, that either fertilization fails to occur, or the fertilized ovum
is incapable of further development. In some instances, sterility
dates from the first infection of the wife; but more commonly it
does not develop until after the completion of one or more pregnancies.
Hofmeier rightly points out that whilst gonorrhoeal infection in
women may cause sterility, such sterility is by no means an inevitable
consequence of the disease.
537Other gynecologists are even more reserved in admitting the
importance of gonorrhoea as a cause of sterility in women. Fritsch
is of opinion that in many cases a casual relation is believed to
exist, when in reality there is nothing more than a coincidence.
Sterility and slight perimetritis, he remarks, are common in women;
gonorrhoea is common in men. But it does not follow that the
frequent gonorrhoea of the husbands is the sole cause of the frequent
sterility and perimetritis of the wives. “For several years,” he
continues, “I have examined all the men I possibly could for
evidence of the existence of gonorrhoea, and have enquired for a
history of previous attacks of the disease. To my astonishment
I discovered that the fathers of many children, whose wives had
come to consult me for some quite disconnected condition, had
quite as often suffered formerly from gonorrhoea as the husbands
of sterile wives.”
M. Saenger is one who very vigorously upholds Nöggerath’s
views. He insists that, excluding puellae publicae from consideration,
no less than 12% of all gynecological disorders depend upon
pathological processes referable to gonorrhoeal infection of the
female genital organs. To establish this thesis, it is not necessary
to prove that Neisser’s gonococcus is or has been present; the
diagnosis must be based principally upon clinical considerations.
Chronic vaginitis and urethritis, inflammation of the uterine mucous
membrane, tubal suppuration, oophoritis, and perimetritic adhesions
(especially those which unite all the lateral pelvic organs into a
shapeless knot)—these are conditions thoroughly characteristic of
gonorrhoea.
No less unfavourable an influence of gonorrhoeal infection upon
fertility is shown by the observations of Glünder. Women numbering
87 were in attendance at the gynecological department of the
Policlinik of the University of Berlin, all of them seeking advice
on account of sterility. In the case of 24 of these, the husband
was also present; 19 of these men admitted having previously
suffered from gonorrhoea; the remaining 5 denied such infection,
although the wives of all of these had symptoms pointing unmistakably
to gonorrhoeal infection; among the other 63 women, there
were 8 only in whom the genital organs were found perfectly
normal, whilst in 38 of them there were signs of previous gonorrhoeal
infection. Thus we see that of these 87 sterile women,
62 (71.3%) had had gonorrhoea; and Glünder, assuming that in
these cases the gonorrhoea was the efficient cause of the sterility,
and regarding the average percentage of sterile marriages as 12.34
in every 100 contracted, is led to the conclusion that of every eleven
or twelve marriages, one is rendered sterile in consequence of
gonorrhoea.
538To the same opinion, that gonorrhoea is the principal cause of
sterility, Lier and Ascher were led by an investigation of numerous
clinical histories. Moreover, they believe that in the large majority
of sterile marriages, the husband is directly or indirectly responsible.
Directly, in so far as a very large percentage of men have their
reproductive capacity annihilated by gonorrhoea; indirectly, because,
of those who retain their fertilizing powers, so large a
number infect their wives with gonorrhoea, and thus render them
incapable of conceiving, that chronic gonorrhoea—in the female
harder to eradicate even than in the male—must be regarded as
the arch-enemy of fertility. Of 80 men affected with azoospermia,
all cases observed by Prochownik, in 75 the disease was the sequel
of gonorrhoea; of the remaining 5 cases, two were due to syphilitic
disease of the testicles, one to tubercular disease of the same, whilst
two were due to long continued masturbation, with consecutive
atrophy of the testis and epididymis.
But that the obstacle offered to conception by gonorrhoeal infection
is by no means so powerful as Nöggerath and his supporters
believed, is shown by the investigations of Oppenheimer, who, in
Kehrer’s clinique at Heidelberg, examined 108 pregnant women for
the presence of gonococci, and found these organisms, pathognomonic
of gonorrhoeal infection, in no less than 30 of them, that is, in 27.7%.
Thus, in this large number of cases, pregnancy had occurred notwithstanding
the presence of gonorrhoea. Lower, again, in
Schröeder’s clinique, examined 32 patients during the lying-in period,
and detected the presence of gonococci in 26; an experience which
also proves that gonorrhoeal infection is no bar to pregnancy. Dunstone
has recently recorded 5 cases in which, notwithstanding the
existence of gonorrhoea, the women became pregnant once or several
times.
In the “Medical Brief” the question was mooted, “Can a woman
have children subsequently to being infected with gonorrhoea?”
Numerous affirmative answers were received; and among them one
mentioning the case of a woman who was infected with gonorrhoea
at the age of 18, and subsequently gave birth to 8 children.
The question of sterility in prostitutes has also attracted attention,
since these women may be regarded as invariably infected
with gonorrhoea. Meissner and Jeannel speak of the infertility
of prostitutes as a well-known fact; and the latter states that,
whereas, according to Montesquieu, to every 100 women in France,
on an average 341 children are born, of which 200 grow up, to 100
prostitutes in Bordeaux there were born 60 children only, and of
these but 21 attained maturity. Marc d’Espine affirms that among
2,000 prostitutes not more than two or three will have children in a
year. Parent-Duchatelet, on the other hand, regards the sterility of
539these women as a purely temporary affair, and writes: “les prostituées
conçoivent souvent, mais elles avortent fréquement;”[49] and
this frequency of abortion he attributes to two causes, in the first
place to deliberate induction of abortion, and in the second place, to
their mode of life. He continues: “cette fécondité a lieu surtout
lorsque, quittant leur mettier, elles se marient ou s’attachent à un seul
homme; dans ce cas les grossesses se succèdent, elles sont toujours
heureuses et les infants qui en proviennent sont aussi vivaces que les
autres;”[50] thus, in his opinion the sterility of prostitutes lasts only
as long as they pursue their occupation.
The question as to what influence, if any, gonorrhoeal secretion
has per se upon the semen, has often been asked, but not yet satisfactorily
answered. We have no certain knowledge whether the
gonococci, the pus cells, or one of the toxins of the secretion, exercises
a deleterious influence upon the vitality of the spermatozoa;
it is certainly possible that this may be the case, for the diplococci,
just as much as streptococci and staphylococci, are found not only
within the cells, but also in the intercellular fluid and in the detritus,
and so must be brought into intimate contact with the spermatozoa;
but inasmuch as quite a number of persons who are at the time
actually suffering from gonorrhoea beget children, we are compelled
to assume that for the harmful influence, if any such exists,
to be exercised, a prolonged contact of the semen with the gonorrhoeal
pus is necessary. In cases of gonorrhoeal epididymitis and
prostatitis, and also in gonorrhoeal urethritis, no such prolonged contact
occurs; but when the vas deferens or the vesicula seminalis is
inflamed, the contact is more prolonged, and may suffice to destroy
the vitality of the spermatozoa, which are extremely sensitive to
chemical stimuli. In 8 cases observed by Kroner, the fruitful coitus
was unquestionably effected when the husband was suffering from
still active gonorrhoea; in all the cases the children were born
at full term, and all suffered from conjunctival blenorrhoea. That
gonorrhoea often fails to induce sterility, is shown by the familiar
fact that a woman frequently has one child after another, all infected
with this conjunctival form of gonorrhoea, showing that the mother
remains fertile notwithstanding the persistency of the gonorrhoeal
infection.
Upon the investigation of 60 carefully written clinical histories,
dealing with the relation between proved gonorrhoeal infection and
a sterile marriage, Grechen has drawn up the following table,
540showing the various ways in which chronic gonorrhoea may give
rise to sterility:
A. Absolute Sterility.
a. Owing to impossibility of fertilization, in consequence of defective
formation of spermatozoon or ovum:
- I. In the male:
- 1. Aspermatism.
- 2. Azoospermia.
- II. In the female:
b. Owing to impossibility of pregnancy, although semen and
ovum may be normal, and fertilization can be effected:
Gonorrhoeal endometritis of atrophic character.
B. Relative Sterility.
a. Owing to mechanical interference with the conjugation of
spermatozoon and ovum:
- I. In the male:
- 1. Epididymitis duplex.
- 2. Strictura impermeabilis urethrae.
- II. In the female:
- I. Perioophoritis and perimetritis, and their results, viz., adhesions and displacements of the reproductive organs. 2. Tubal catarrh, pyosalpinx, kinking and other forms of obstruction of the tubes.
b. Owing to extension of the gonorrhoeal process to the decidua,
causing abortion in the early period of pregnancy:
Endometritis gonorrhoeica chronica, and endometritis decidualis.
Benzler has endeavoured to elucidate the problem of the relations
between gonorrhoea and sterility by a collective investigation in the
army. The investigation was concerned with 474 men who during
their period of service with the colours had been treated for gonorrhoea,
and who subsequently had married. Dealing with all cases
alike, without regard to complications which had been observed in
some cases but not in others, of the 474 wives, there were 64 who
never became pregnant = 13.5%; 78 who had one child only = 16.5%;
total, 142 = 30%.
Leaving out of consideration the cases in which epididymitis had
been observed, there remained 363 cases of uncomplicated urethritis;
of the 363 wives of these men, there were 38 who never became
pregnant = 10.5%; 63 who had one child only = 17.3%; total 101
= 27.8%.
Thus, in the cases in which the husbands had had uncomplicated
urethritis, the percentage of absolute sterility was only 10.5; while
541in the unselected cases of gonorrhoea, it was no more than 13.5.
The figures show clearly that the influence of uncomplicated gonorrhoea
is but trifling; indeed, it is obvious that this must be the
case, for it is probable that not less than 80% of men experience at
least one attack of gonorrhoea, and did this give rise to sterility,
either directly by its influence on the men themselves, or indirectly
by transmission to their wives, the human race would soon die out.
Moreover, the frequent occurrence of ophthalmia neonatorum is a
sufficient proof that notwithstanding gonorrhoeal infection in all
these cases, pregnancy and delivery have taken place.
To sum up, it is my opinion that in recent years the influence
of gonorrhoeal infection in inducing sterility in women has been
painted in far too gloomy colours, and it is time that these extreme
views should be abandoned.
This is a convenient place to insist upon the fact that in cases
which are by no means rare, in the absence of aspermatism and
azoospermia, and altogether independently of gonorrhoeal infection,
it is the husband who is responsible for the occurrence of sterility;
in such cases the sterility is due to failure of conjugation between
spermatozoon and ovum, dependent upon congenital or acquired
defects of the penis. The great majority of cases of this kind are
due to hypospadias.
A case of sterile marriage is reported by Lier and Ascher, in
which the husband had suffered from hypospadias and had been
operated upon for the relief of that condition. Although erection
of the penis was normal, and coitus terminated in the usual orgasm,
with sense of ejaculation, the semen did not find its way into the
vagina; it accumulated in the artificial cul-de-sac between the former
abnormal urethral orifice and the artificially constructed meatus,
and after coitus the semen had to be expelled from this region by
digital pressure.
Miclucho-Mackay reports that among the Australian aborigines,
hypospadias is artificially induced, in order to prevent fertilization.
In young boys, an incision is made through the lower wall of the
urethra from the meatus as far up as the scrotum, and care is taken
that the several surfaces do not reunite. During coitus, the semen
flows away without entering the vagina. This mutilation is practised,
not only in South and Central Australia, but also by the
indigens of Port Darwin.
That hypospadias does not in all cases offer an insuperable obstacle
to impregnation, is, however, shown by a striking case which came
under the notice of Labalbary. He saw a hypospadiac who, in
micturating, had to crouch down in the feminine posture, because
he was unable to project the stream of urine forwards; in coitus,
he deposited his semen only on his wife’s vulva. But his wife gave
542birth to two sons, about whose paternity there could be no reasonable
doubt, since both exhibited the same malformation as their
putative father.
Occasionally, phimosis offers an obstacle to impregnation, and
only after relief of the condition by operation, is the wish for
offspring fulfilled. A case of this nature is recorded by Amussat.
In cases of severe stricture of the urethra, sterility may result,
although the constitution of the semen is perfectly normal. During
erection of the penis, the stricture is completely closed, and the
semen accumulates in the urethra above it; when the penis becomes
flaccid, the semen flows away, outside the vagina. In some such cases,
the semen regurgitates into the bladder, and is not discharged until
the patient makes water. Although the supposition is not one in
which strict proof is obtainable, it is probable that the man is at
fault in cases in which the wives of two or more brothers fail to
conceive. I have seen several instances of the kind. Three brothers,
all quite healthy, and of virile aspect, were married to women in
whom on gynecological examination no significant abnormality
could be detected; they had been married respectively for 14, 9, and
8 years; all were childless. Three brothers, two of whom were
practising physicians, had lived a number of years (20, 4, and 14,
respectively) in sterile wedlock; one of them (a physician) informed
me that he ejaculated always a very small quantity of semen, and
thought it possible that this was the cause of the sterility. Of four
brothers, two had lived long in barren wedlock; the third had no
child for 14 years after marriage, when at last his wife became
pregnant after a visit to a spa; the fourth brother is a misogynist
and a confirmed bachelor.
Sexual Sensibility in Women.
In our consideration of the various influences by which the contact
of ovum and spermatozoon may be prevented, the degree of
sexual excitement experienced by the woman during the sexual
act must not be overlooked, for this plays a part not to be underestimated,
even though it is a matter on which it is difficult to
obtain accurate information.
It is extremely probable that an active participation on the
part of the woman in coitus has an important influence upon the
attainment of fertilization, i. e., that sexual excitement in the woman
is a link in the chain of conditions leading to conception. This
excitement has a reflex influence, but the influence may be exercised
in either (or both) of two ways: first, it may cause certain reflex
changes in the cervical secretion, whereby the passage of the spermatozoa
is facilitated; or, secondly, it may give rise to reflex changes
543in the vaginal portion of the cervix, to a rounding of the os uteri
externum and a hardening of the consistency of the cervix (changes
of an erectile nature) coupled with a slight descent of the uterus—changes
which likewise favour the entrance of the semen into the
uterine cavity. Theopold goes so far as to say that it is only
women who experience erotic excitement who are capable of being
impregnated.
My own opinion is that considerable importance is to be attached
to voluptuous excitement of the woman during coitus, for the former
of the two reasons mentioned above, namely, because such
excitement leads to the occurrence of reflex secretion of the cervical
glands, the secretion thus produced maintaining or enhancing the
activity of the spermatozoa; and contrariwise, in the absence of
voluptuous excitement on the woman’s part there is a failure of the
reflex secretion, and the passage of the spermatozoa into the uterine
cavity is consequently less easily effected. That sexual excitement
has great influence upon the production of the first appearance of
menstruation, has frequently been shown; and an analogy between
such an influence and the suggested effect of sexual excitement in
favouring the occurrence of conception, must not lightly be rejected.
It is well known that the first menstruation occurs at an earlier
age in girls living in towns than in those living in the country;
not solely (if at all) in consequence of the better nutriment and
easier life of the former, but also, unquestionably, owing to nervous
influences. It is, moreover, a familiar experience that factory girls,
who from early youth are exposed to sexual stimulation, attain
sexual maturity at an extremely early age. Again, from early
times it has been the prevailing opinion of the common people
that for the impregnation of a woman it was necessary for her to
experience voluptuous excitement, or at least, that in the absence
of such excitement, conception was rendered difficult. Riedel relates
of the indigens of the Island of Buru, that they often have
sexual intercourse with foreigners, “but during such intercourse
they remain quite passive, in order to avoid impregnation.” It is
not an unusual experience in gynecological practice for a sterile
woman, in the absence of any prompting, to complain that during
coitus she has no “feeling” whatever, and to attribute to this lack
of feeling her failure to conceive.
A cultured lady, the mother of several children, assured me, not
only that she was always aware, whether an act of intercourse would
or would not lead to impregnation, but further, that it was within
her power to determine whether the intercourse should or should
not be fruitful. If she was passive during intercourse, or if, to
use her own expression, her attitude was one of “laisser faire,
laisser aller,” conception would not occur; but if, on the other
544hand, she took an active part in the coitus, so that she experienced
a powerful voluptuous sensation, pregnancy would result from the
intercourse.
In some cases, the previously described condition of dyspareunia
is the cause of the sterility. In fact, the combination of dyspareunia
with sterility is so strikingly common, that my own observations
have led me to infer that there is a casual connexion between the
two states, at least in a considerable proportion of cases.
I append a short note of a few instances of this kind: Mrs. G.,
aged 27, married 6 years, sterile; an anæmic, delicate lady, who has
never experienced the sense of ejaculation. The semen flows away
from the vagina immediately after the completion of coitus. No
abnormality to be detected on gynecological examination. Mrs. S.,
aged 24, married 5 years, sterile; during intercourse remains completely
cold, and has experienced the sense of ejaculation in dreams
only. Gynecological examination disclosed the existence of slight
cervical catarrh, but no other abnormality. Mrs. E., aged 30,
married 10 years, had a child 9 years previously, a difficult delivery
followed by puerperal disease, since then sterile; she states that
since her delivery she has not experienced the sense of ejaculation,
with which she was formerly familiar; further, since that time she
has suffered from profluvium seminis. On gynecological examination
the uterus was found to be enlarged and retroflexed. Mrs. K.,
aged 28, married 6 years, sterile; amenorrhoeic, has never experienced
the sense of ejaculation, and finds sexual intercourse so unpleasant
that, “in order to be left in peace,” she has herself begged
her husband to keep a mistress. Examination showed the uterus to
be in an infantile condition.
Whilst I have notes of numerous cases similar to those just quoted,
I must also insist upon the fact that I have sometimes had complaints
of dyspareunia from wives whose fertility has been proved
by the birth of numerous children. And, again, anyone whose
position permits him frequent glimpses of what passes behind the
scenes of married life, will from time to time have noticed as signs
of relative dyspareunia instances in which the faithless wife is far
more readily impregnated by her lover than by the husband to
whom she is indifferent or whom she actually dislikes.
To relative dyspareunia dependent upon sexual disharmony we
must refer also those instances in which a man and a woman prove
sterile while living together for a considerable period as man and
wife, but after separation both prove fertile in fresh unions. Several
such cases have come within my own experience, and similar instances
attracted the attention of the observers of antiquity—Aristotle,
for example. Haller, for this reason, lays stress on the lack
545of mutual affection as a cause of sterility; and Virey, also, believes
that sterility may often depend upon the absence of the “harmonie
d’amour.”
It is possible that the custom, which in certain rural districts has
persisted into quite recent times, of a temporary experimental cohabitation
of candidates for matrimony, was based on an attempt
to discover the existence of such a sexual harmony. Ploss, for
instance, reports that in East Prussia, in 1864, he was informed that
among the Mazurs this custom of an experimental year of cohabitation
was in force. If during this year the woman became pregnant,
the young couple were married; but if pregnancy failed to
occur, they separated, considering they were not formed for one
another.
A well-known historical example of relative sterility is furnished
by the two marriages of Napoleon I. His first marriage to Josephine
remained sterile, though Josephine had children by Beauharnais;
and Napoleon, remarried to Marie Louise, had a son by
the latter.
Von Gutceit, a physician of wide experience, points out that
“sensitive women, who have a mental or physical antipathy to cohabitation,
or who have a secret but ardent affection for some
other man, often fail to conceive as a result of intercourse with
their husbands; but when, in illicit intercourse, they experience the
voluptuous sensations to which they have hitherto been strangers,
pregnancy often speedily ensues.” He maintains, further, “that such
women, in consequence of the stimulation of the genital organs in
the absence of sexual gratification, become affected with all kinds
of menstrual irregularities, with fluor albus, prolapse of the uterus,
and chronic metritis; they suffer from digestive disturbances and
constipation, leading to emaciation; and they are prone to hysterical
manifestations.”
Analogous phenomena have been noted, and with much greater
distinctness, in the animal world. Darwin, writing on this subject,
remarks: “It is by no means a rare occurrence, that certain males
and females will not be fruitful in intercourse together, whilst the
same individuals prove perfectly fertile in intercourse with other
members of their species—and this in cases in which there is no
evidence that the subsequent fertility is due to any change in the
conditions of life. The cause is probably to be found in an innate
sexual disharmony between the infertile pair. A very large number
of instances of this kind have been reported to me by well-known
breeders of horses, cattle, pigs, dogs, and pigeons. Sometimes
a breeder will fail to obtain offspring from a male and a
female of known fertility whom he wishes to couple for some special
reasons. The most celebrated living horse-breeder informed me
546that frequently a mare, which in other seasons with other stallions
has proved fertile, may be coupled with a stallion likewise of proved
reproductive potency, and will fail to be impregnated; yet this same
mare will shortly afterwards be impregnated by another stallion.”
Pflüger reports that he has often seen a thoroughbred stallion,
which was fully prepared, at a moment’s notice, to serve a thoroughbred
mare, prove extremely unwilling to serve a common mare on
heat, and only induced to do so with the greatest difficulty, and indeed
by a trick. The stallion is placed in the central one of three
stalls, on one side of him is the thoroughbred mare, whilst in the
third stall is the common mare, covered with a cloth. The stallion’s
head is turned to show him the thoroughbred mare; immediately his
appearance undergoes a change. Every muscle of his body appears
to quiver, and never does a fine animal appear more beautiful than
at such a moment, full of pride, fire, and vitality.[51] As soon as
the stallion makes ready to serve the mare, he is rapidly led to the
other stall, and suitably assisted to the actual commencement of
intercourse with the substituted mare. But it sometimes happens, as
Pflüger himself has seen, that the stallion becoming aware of the
deception, refuses to complete the coitus, withdraws his penis,
and immediately turns to the mare of his choice.
Matthews Duncan, among 191 sterile women, found that 39 had
no sexual appetite, and 62 had no voluptuous sensations during
coitus. He regards abnormal sexual appetite as one of the principal
causes of sterility.
Notwithstanding these facts, it must not be forgotten that many
cases are recorded in medical literature of women conceiving after
intercourse effected against their wishes, as by rape, or when they
were in a state of intoxication, or asleep, or in the entire absence of
all voluptuous sensation. Moreover, the erection of the vaginal
portion of the cervix, and the reflex movements and secretory
changes in the uterus, may also occur independently of sexual
desire and voluptuous sensation; but such cases are certainly exceptional,
and their credibility is frequently open to suspicion. In
547numerous instances in which conception is stated to have followed
intercourse in a state of unconsciousness, judicial proceedings have
elicited the fact that the intercourse was not entirely involuntary
on the woman’s part, and that the alleged force was no more than
a vis grata. Von Maschka reports a case in which a girl asserted
that she had been violated whilst in a condition of epileptic unconsciousness,
but she remembered every detail of the act with precision.
Casper, again, in a case in which it was asserted that defloration
had been forcibly effected whilst the girl was in a state of
alcoholic coma, showed that there had been no more than moderate
intoxication combined with great sexual excitement. Assertions
that pregnancy has resulted from intercourse effected during sleep,
in a state of unconsciousness, or in the “magnetic” or “hypnotic”
state, should always be accepted with reserve.
It is interesting to note in this connexion that the Chinese physicians
enumerates among the causes of sterility the practice of
“congfou” by the man, this name being given to a manipulation
analogous to hypnotism, whereby the voluptuous sensation during
intercourse is diminished or abolished by distracting the attention
elsewhere.
A proof of the importance of specific sexual sensation for the
attainment of conception is afforded by the fact that in the majority
of women voluptuous excitement is absent at the first act of intercourse,
and only gradually develops thereafter; in correspondence
with this, we find that the first conception does not usually occur
until some time after marriage, and that the period of its occurrence
frequently coincides with the full development of voluptuous sensation
during intercourse. Thus, even in the woman fully fitted for
conception, the actual capacity for impregnation is only developed
gradually, and after a sufficient experience of intercourse.
This transient incapacity for conception may, indeed, also depend
upon the fact that at first coitus is apt to be incompletely effected,
and for this both husband and wife are to blame; but unquestionably
in many cases the reason is the one first mentioned.
In some cases, certain psychical influences which affect the intensity
of the voluptuous sensation, manifest its significance. Thus,
in some instances, the influence of stimulation of the clitoris in leading
to conception has been clearly shown; in others, the performance
of coitus in some unusual position, varying with the woman concerned,
is alone competent to arouse sexual sensibility to its full
extent, and to bring about the orgasm. One occasionally receives
confidential information from a husband that his wife experiences
a voluptuous sensation only when coitus is performed in the lateral
posture, or more bestiarum, or in the situs inversus, etc., etc.
548Excessive frequency of intercourse, prolonged and repeated sexual
excitement, on the other hand, induce sterility, as is well seen in
prostitutes, who rarely become pregnant.
Finally, perverse sexual impulse must be mentioned as a possible
cause of sterility. This may be an acquired perversion, due to the
fact that at the epoch of the menarche, the commencement of
puberty, owing to the strength of sexual desire whilst intercourse
is an impossibility, or simply from evil example, the girl has become
a confirmed onanist, and continues the habit even after marriage.
In other cases we have to do with a psychopathic state, a form of
mental degeneration due to very various causes, or in some cases
inverted sexual sensibility exists in a person whose mind is in other
respects normal. In women with sexual inversion, ordinary copulation
with the male is insufficient to arouse the sexual orgasm,
and for this reason, as well as because persons thus affected avoid
coitus as much as possible, sterility commonly ensues.
In sterile homosexual women, and equally so in women addicted
to masturbation, gynecological examination may disclose no abnormality
whatever; but in other cases of the kind we may find a contributory
cause of sterility in the fact that the internal genital
organs are imperfectly developed, or even completely absent. In
sterile women, if on gynecological examination we find certain
characteristic changes in the reproductive organs, a strong suspicion
will be aroused that the sterility is due to abnormal modes of sexual
gratification. The changes in question are: hypertrophy of the
clitoris, enlargement and a bluish colouration of the labia minora,
retroversion of the uterus, neuralgia and displacement of the ovaries,
leucorrhoea, and menorrhagia.
The question has been mooted by Cohnstein, whether, as is commonly
assumed, a woman is capable of becoming pregnant at any
time during the year, or whether, as in the lower animals, the reproductive
capacity can be exercised only at certain seasons, or
again, whether there may not be individual moments of predilection
for the occurrence of conception. He found that in the great
majority of women there were such seasons of predilection, and
only in a minority could conception be effected indifferently at any
time of the year. As a proof of this assertion, he appends the following
case: A married woman, 33 years of age, had several
years before been delivered prematurely of a still-born child, and
since then had not again been pregnant. Her reproductive organs
were normal. The husband’s semen was examined, and also found
to be quite free from abnormality. In the course of the three following
years an attempt was made to cure the sterility by dilatation
of the cervical canal, suggestions for the proper regulation of sexual
intercourse, etc., but all without effect. Cohnstein now calculated
549the date at which the full term of the previous pregnancy would
have fallen, and found that this was the middle of February; he
therefore inferred that intercourse effected at the beginning of
May would result in impregnation. As a fact, the woman conceived
at this time, and at full term gave birth to a healthy girl.
The assumption that such a time of predilection for the occurrence
of conception exists is, however, contradicted by the well known fact
that in the case of large families the children’s birthdays are irregularly
distributed throughout the year.
Baker-Brown describes a special form of sterility due to “sympathetic
or reflex action.” It depends upon diseases of the organs
adjoining the uterus, such as vascular tumours of the urethra, bleeding
piles, fistula, fissure, and prolapse of the anus, schirrus of the
rectum, ascarides. “These diseases produce sterility in consequence
of the loss of blood, the menstrual disturbances, the morbid congestion
of the uterine system, and the reflex neuroses, to which they
give rise.” Courty reports a case belonging to this category in
which in a young married lady sterility was due to fissure of the
anus, which had long existed without recognition; after the fissure
had healed, conception occurred. Palmay recently reported a case
in which “taenia solium was the cause of sterility. In a woman
20 years of age, who had lived in sterile wedlock for three years,
the presence in the intestine of a tapeworm, which she had harboured
for many years, gave rise to dysmenorrhœal troubles. The
complete expulsion of the worm relieved the dysmenorrhœa, the
woman became pregnant, and gave birth to a child at full term;
since then menstruation has been painless.” The presence of the
tapeworm may have had an unfavourable influence upon the blood-supply
and the innervation of the uterus. But cases of this nature
do not constitute a special form of sterility; they must be classed,
either with cases due to interference with ovulation, or with those
due to prevention of the contact of ovum and spermatozoon.
Incapacity for Incubation of the Ovum.
The fertilization of the ovum is, as previously described,
probably effected in man, as in other mammals, in the upper
third of the Fallopian tube. The fertilized ovum is then swept
down into the uterus by the action of the cilia which line
the tube, assisted by the peristaltic movement of the muscular
wall of the canal. The uterine mucous membrane at this
time is thickened and thrown into folds, and in these latter the fertilized
ovum is entangled; by its presence the ovum now exerts a
reflex stimulus leading to a still greater proliferation of the cells of
the uterine mucous membrane, which grows up over the ovum and
550soon shuts it off completely from the uterine cavity. Thus the
ovum comes to be entirely imbedded in the substance of the mucous
membrane.
Thus for the implantation of the ovum, it is first of all necessary
that the uterine mucous membrane should be in a normal condition;
pathological changes in this membrane, and indeed any morbid
structural alteration in the uterine tissues, may prevent the implantation
and incubation of the ovum, and may thus give rise to sterility.
The uterine cavity is normally lined with ciliated epithelium, the
cells of which have an elongated elliptical form. The movement of
the cilia is directed downwards. The epithelium is perforated by
the orifices of the uterine glands; these glands are simple tubular
glands, passing through the mucous membrane with an S-shaped or
corkscrew curve; between the glands lies a rich germinal tissue,
made up of rounded cells. The rounded connective tissue cells have
processes which build up the scaffolding of the mucous membrane.
Among the connective tissue cells of the uterine mucous membrane,
wandering leucocytes are almost always to be seen. Menstruation
is characterized by a swelling of the mucous membrane, and by enlargement
of the uterine glands. At the same time, blood extravasations
appear between the more superficial layers of the membrane,
and on its free surface, and various portions of the surface
of the membrane are cast off.
Very numerous are the morbid states of the uterus and its annexa
whereby the implantation and incubation of the ovum are prevented;
and incapacity of the uterus for the fulfilment of these functions is
therefore a common cause of sterility in women.
That developmental defects of the uterus, even when they are not
such as render conception impossible, may yet often give rise to
sterility, has been already explained in writing of the conditions of
the uterus which prevent the contact of ovum and spermatozoon;
for defects of development which are not sufficiently severe to prevent
this contact, may yet suffice to render the uterus unfit for the
implantation and incubation of the fertilized ovum. Inflammatory
disorders, such as perimetritis and the formation of exudations in
the parametrium, may render the uterus unable to undergo the enlargement
necessary to pregnancy. Tissue changes in the uterine
musculature may likewise prevent the implantation of the ovum, or
the proper development of the uterus during pregnancy. New-growths
of the uterus or its neighbourhood may bring the development
of the fertilized ovum to an untimely conclusion. Above all,
however, it is diseases of the uterine mucous membrane which unfit
the organ for the implantation of the ovum, and thus give rise to
sterility. All those inflammatory states which lead either to softening
or to induration of the uterine parenchyma, or to swelling and
551thickening of the endometrium or parametrium, may offer a hindrance
more or less serious to the normal incubation of the ovum.
The diagnosis whether in an individual case we have to do with
sterility dependent upon impotentia gestandi, is often difficult, because
the conditions which cause it are frequently associated with
those which cause sterility by preventing the contact of ovum and
spermatozoon. In any case, a careful examination of the pelvic
organs must be made, not only to determine whether there is any
displacement or enlargement of the uterus, chronic metritis or perimetritis,
parametric exudations, or new growths of the uterus or of
neighbouring organs, but also, if necessary by dilating the cervical
canal, to ascertain the condition of the uterine mucous membrane,
and whether there is hyperplasia or atrophy thereof. In this connexion,
examination of the uterine secretion is of especial importance:
a purely mucous, transparent, vitreous, tenacious secretion in
the os and in the cervical canal, indicates the existence of catarrhal
endometritis; a markedly haemorrhagic secretion signifies hyperplastic
endometritis; profuse purulent secretion containing gonococci,
indicates gonorrhoeal endometritis; the discharge of pieces of membrane
shows that there is exfoliative endometritis; the discovery of
fragments of carcinomatous tissue indicates the breaking down of a
malignant tumour of this nature; etc.
Finally, it is necessary to obtain a careful history of the case, asking
whether there have been menstrual irregularities, or miscarriages,
and the characters of previous labours (in cases of acquired
sterility); any pathological conditions in other organs should be investigated;
and the condition of the blood and the state of general
nutrition should receive attention. Chlorosis, anæmia, and scrofula
often give rise to catarrhal endometritis; severe disease of the heart
may lead to congestive troubles of the genital organs; after abortion
or difficult labour, chronic metritis or endometritis are common.
Further, the differential diagnosis between erosion and carcinoma of
the portio vaginalis, must often depend upon consideration of the
patient’s age and general health, and upon the nature and duration
of the haemorrhage. Pain on micturition, appearing soon after marriage,
and lasting often a few days only, will indicate the probability
of gonorrhoeal infection, etc.
Von Grünewaldt has vigorously insisted upon the fact that the
notion of sterility, i. e., impotentia generandi in women, is not coincident
with the notion of impotentia concipiendi, and there is an
important distinction between cases in which it is impossible that
fertilization should be effected, and cases in which, though fertilization
may take place, the implantation and incubation of the ovum fail
to ensue. In this author’s opinion, the only absolute mechanical
hindrance to the entrance of the semen is to be found in atresia of
552the genital passage, and the role of impotentia concipiendi is of quite
minor importance as compared with incapacity on the part of the
uterus for the implantation and incubation of the ovum, an opinion,
which, notwithstanding the record of exceptional cases in which
pregnancy has occurred in spite of the existence of mechanical obstacles
to conception, I must regard as altogether beyond the mark.
On the other hand, it is indisputable that for the occurrence of pregnancy
it is necessary, not only that contact of ovum and spermatozoon
should be possible, but further, that the uterus should be in a
condition favourable for the implantation and further development
of the ovum subsequent to fertilization. For this reason, diseases
of the uterine tissues must play an important part in the causation
of sterility, though we cannot go so far as to admit with von Grünewaldt
that these diseases are the principal cause of reproductive incapacity
in women.
Various metritic processes, and also venous hyperaemia consequent
upon heart disease, may lead to atrophy of the uterine mucous
membrane, which then appears thin and smooth, whilst the uterine
glands are destroyed, or transformed into small cysts. The same
condition may result from retention of secretions in the uterine
cavity—hydrometra and haematometra. In all these cases, the epithelium
probably loses its cilia. The process has a serious influence
antagonistic to the reproductive capacity inasmuch as the implantation
of the chorionic villi is rendered difficult (Klebs).
Hyperplasia of the uterine parenchyma, affecting either the whole
organ or a large part, and characterized either by enlargement of
the entire organ, or only by thickening and elongation of the cervix,
may hinder the incubation of the ovum. It may be due to endometritic
catarrhal processes; to venous hyperaemia, especially in cases
of valvular heart disease; to subinvolution; and sometimes to excessive
sexual stimulation, as in prostitutes. Both the change in
the shape of the cervix, and the changes undergone by the uterine
mucous membrane in cases of extensive uterine hyperplasia (it commonly
becomes atrophic and discharges a watery secretion), interfere
with the reproductive capacity.
In all cases of chronic metritis, the hyperaemia and hyperplasia of
the uterus may give rise to haemorrhages; these sweep away the
ovum, and thus lead to impotentia gestandi. And the nutritive
changes in the mucous membrane that occur in chronic metritis also
interfere with the implantation and incubation of the ovum. Moreover,
it is well known that in these cases, even if conception is
effected, abortion is extremely apt to occur, owing to the pathological
state of the endometrium, which interferes with the normal development
of the decidua. Haemorrhages occur in the decidua, and
are followed by abortion. And further, the replacement of portions
553of the muscular tissue of the uterine wall by fibrous tissue, a change
which is apt to occur in long continued metritis, interferes with the
proper expansion of the uterus during pregnancy, and thus leads to
abortion.
On the other hand, it cannot be denied that frequently enough
patients with well marked chronic metritis nevertheless conceive in
a normal manner, and give birth to a healthy child; and this not
once only, but again and again.
As sterility due to mesometritis, von Grünewaldt classes the
numerous cases in which sterility ensues upon a confinement in
which the patient reports that inflammation followed delivery—or
sometimes in which nothing abnormal was noticed. The results of
local examination are negative: there is no displacement, no exudation
or swelling, and no relevant affection of the endometrium. But
the characteristic feature of these cases is, according to von Grünewaldt,
that after her last full-time delivery, a woman has had a miscarriage
or a premature delivery, and subsequently has been completely
sterile. The degenerative process is at first partial, so that
it does not prevent conception, but renders it impossible for the
pregnancy to go on to full term; subsequently it extends throughout
the mesometrium, and conception is no longer possible.
Cole of San Francisco regards as the most frequent cause of
sterility ensuing upon a single delivery, subinvolution of the uterus,
most commonly due to rising too early after delivery. He therefore
considers it of especial importance after a first delivery that the physician
should satisfy himself that no serious injury has been effected
by the process.
Chronic endometritis is a very frequent cause of sterility: in the
first place, the catarrhal swelling of the mucous membrane, which
often extends from the os uteri externum to the ostium abdominale
of the Fallopian tubes, offers an obstacle alike to the downward
passage of the ovum and the upward passage of the spermatozoa;
and secondly, in long standing cases, the large size of the uterine
cavity and the smoothness of the surface of the atrophied mucous
membrane, render the lodgment of the ovum in the uterus very unlikely.
A further powerful obstacle to impregnation in cases of endometritis
is offered by the profuse muco-purulent secretion which
usually, though not invariably, accompanies that disease. This
secretion, in some cases flowing freely over the surface of the membrane,
but in others adhering to it with tenacity, whitish-yellow in
colour, rendered cloudy by admixture of pus, or tinted red by admixture
of blood, sometimes of a gelatinous consistency with a
strongly alkaline reaction, contains globules of mucus, ciliated and
cylindrical epithelial cells, pus corpuscles, bacteria and cocci,—and,
if the endometritis is of gonorrhoeal origin, the gonococcus of
554Neisser. This secretion, when profuse and thinly fluid, pours out
through the os, and sweeps away the semen; when tenacious and
gelatinous, it fills up the dilated cervical canal above the constricted
os uteri externum, and constitutes a powerful barrier to the upward
passage of the spermatozoa; when purulent, it is destructive to the
vital activity of the spermatozoa. The changes in the mucous membrane
in cases of long standing endometritis whereby the uterus is
rendered unfit for the implantation and incubation of the ovum, are
the following. The epithelial cells, as usual in cases of continued
catarrh, change in form, the ciliated cells disappear, and are replaced,
first by cylindrical cells, later by polymorphic cells, approaching
in type those of pavement epithelium. The mucous membrane
is swelled, the vessels are dilated, there is hyperplasia of the glands,
with a moderate amount of small-celled infiltration of the interglandular
tissue (Fig. 83). Ultimately the mucous membrane undergoes
atrophy, its glands disappear, it comes to resemble a thin
stratum of connective tissue.
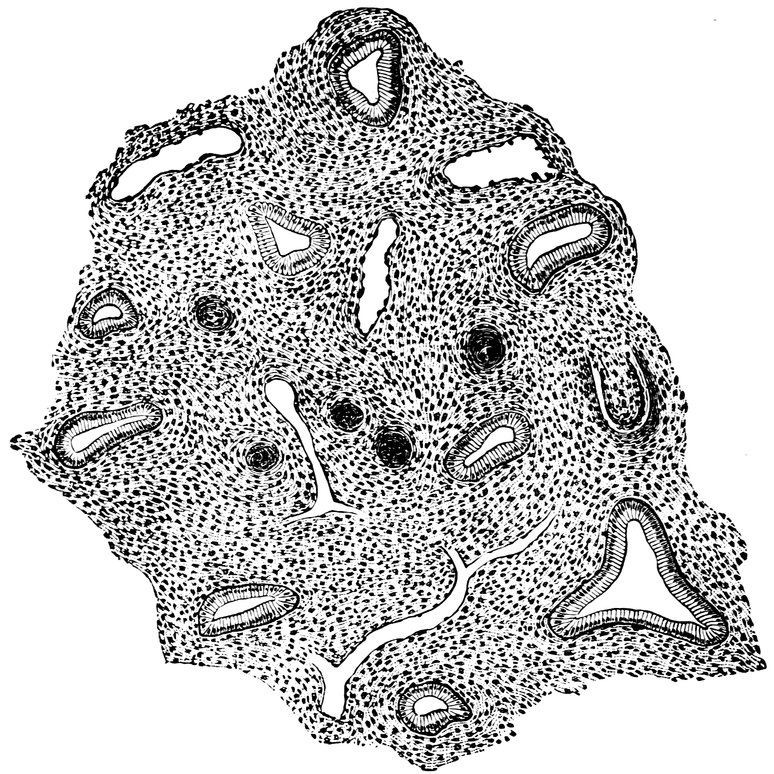
Fig. 83.—Uterine Mucous Membrane in Endometritis. (After A. Martin.)
Thus, in severe and long-continued endometritis, the changes that
occur in the uterine mucous membrane render the implantation of
555the ovum and the formation of normal decidua impossible; even if
conception does occur, the fertilized ovum is speedily discharged.
Frequently, in cases of endometritis, there is consecutive displacement
of the uterus which acts as a contributory cause of sterility.
When endometritis lasts a long time, proliferation of connective
tissue in the uterine parenchyma also occurs, leading often to hypertrophy
of the cervix, and to stenosis of the cervical canal. Since in
so many different ways endometritis may give rise to sterility, the
importance that must be attached to this condition is evident.
The great significance of gonorrhoeal infection in relation to sterility
in women depends, not only on the changes this disease causes
in the Fallopian tubes, leading to interference with the necessary contact
of ovum and spermatozoon, but further, upon the occurrence of
gonorrhoeal cervical and corporal endometritis, of perimetritis, and
secondary parenchymatous metritis. Still, under appropriate treatment,
the inflammatory changes consequent on gonorrhoeal infection
are in many cases curable, and, after absorption of the exudations
and restoration of the normal nutritive conditions of the tissues, conception
may take place. Fritsch, who points out that in the woman
infected with gonorrhoea, sterility ensues in a manner analogous to
that in which it occurs in the male (for in the latter it is not the
primary urethritis, the disease of the passage, but the secondary inflammation
of the testicle that leads to sterility), states that he has
observed cases in which beyond question conception has occurred,
notwithstanding the existence of gonorrhoeal endometritis.
In my own experience, whilst gonorrhoeal endometritis is, among
inflammations of the endometrium, the most frequent cause of sterility,
the place of next importance in this connexion is occupied by
exfoliative endometritis, or membranous dysmenorrhœa. This name
is given to a pathological condition in which from time to time,
usually during menstruation, fragments of membrane, or even an
entire sac-like cast of the uterine cavity, are expelled from the
uterus; since this condition is apt to hinder the incubation of the
ovum, it is commonly associated with sterility—a fact mentioned
already by Denman in 1790, and since then confirmed by numerous
observers. I have had under observation several cases of dysmenorrhœa
membranacea; in two cases it existed from the time of marriage—in
one case 14 years, in the other 8 years—and in both
sterility was absolute. In the latter of the two cases, vigorous treatment
was undertaken, even curettage of the uterus, but quite without
avail. In other cases, the sterility was acquired, the membranous
dysmenorrhœa having begun after the woman had already had one
or more children; but as I have never seen a case in which a woman
became pregnant after the development of this affection, I am compelled
to regard it as one of the most severe hindrances to conception.
556As a general rule, exfoliative endometritis terminates only with
the onset of the climacteric age; in very exceptional cases, however,
a cure may take place earlier. In cases in which this premature termination
has been observed, pregnancy has been known to ensue,
cases of this nature having been observed by Solowieff, Fordyce
Barker, and Thomas. And recently, cases have been reported, in
which the disease has returned after such a pregnancy. Fritsch, indeed,
is of opinion that exfoliative endometritis does not cause
sterility, and that in this disease abortion is no commoner than in
other diseases of the uterus. Charpignon, Hennig, and Bordier have
also observed conception occur in the course of this disease. In 42
cases of membranous dysmenorrhœa collected by Kleinwächter,
pregnancy occurred in four during the existence of the disease.
Löhlein also reports that, among 27 patients affected with membranous
dysmenorrhœa, six became pregnant, after the symptoms had
been clear and unmistakable for a shorter or longer period. Two of
these patients had been already pregnant before the first appearance
of the exfoliative endometritis; subsequently they became pregnant
and were delivered at full term. The other four had suffered for
varying periods and with varying severity from the affection, before
they first became pregnant. In three of these cases curettage of the
uterus was performed; but in one only, in which pregnancy ensued
very speedily on the operation, could a causal connexion be inferred.
In two of the cases the mothers of the patient had also suffered
from the affection.
It has been asserted by B. Schultze and others that curettage of
the uterus renders it difficult or impossible for pregnancy subsequently
to occur. There is, however, no evidence to justify such an
opinion.
Especial attention should be given to inflammatory processes in
the perimetrium and the parametrium as diseases giving rise to sterility
in women. They are extremely common, and at times are
so insidious, running their course without giving rise either to pain
or to fever, that even when very extensive, and even when they have
led to the formation of secondary tumour-growths, they may yet be
overlooked. Hence their pathological significance in the causation
of sterility in women is still underestimated. Chronic pelvic peritonitis
and parametritis may lead to the onset of sterility in various
ways: changes may occur in the cervix, this organ becoming indurated,
fixed, and retroposed, and painful when the uterus is moved;
inflammatory changes may affect the body of the uterus, the ligaments
of the ovary, and various portions of the pelvic peritoneum;
displacement of the uterus may occur; one or both ovaries or tubes
may be dislocated and fixed, either to the side of the uterus, or
behind it, in the pouch of Douglas; all kinds of adhesions or inflammatory
557nodules may result from these processes. Further, in
the scarred, contracted, sclerosed parametric tissue, the blood and
lymphatic vessels of the parametrium are compressed, and in part
obliterated, and the intimate connexion between the pelvic cellular
tissue and the uterus readily leads to the onset of endometritis,
whereby the implantation of the ovum is interfered with. The occurrence
of sterility in cases of pelvic peritonitis and parametritis,
depends in part on the indirect effects of the inflammatory exudations,
and in part on the direct result of the extension of the inflammation
to other regions. The perimetritis, parametritis, and pelvic
peritonitis that result from gonorrhoeal infection have thus an
especially disastrous influence, for the reason that in these cases
cervical metritis and endometritis with blenorrhoea are commonly
superadded. This is the principal cause of the almost invariable
sterility of prostitutes, in whom, however, we must also take into
consideration the influence of the absence of voluptuous sensation
in an act which to them has become a mere matter of business.
The investigations of Bandl in the post mortem room show that
residues of perimetritic and parametritic inflammation are to be
found in the bodies of 58.4% of parous women, and 33.3% of the
bodies of women (married or unmarried) who have had experience
of sexual intercourse but have never had a child. This, he thinks,
is the explanation of the great frequency of childless marriages and
of relative sterility in women. In the nulliparae mentioned above,
Bandl commonly found an indurated, functionless, in places cicatrized,
narrowed cervix, paraoophoritic and perisalpingitic residues,
and morbid changes in the tubes and the ovaries. In some cases also
the husbands of such sterile women were found to be affected with
azoospermia. The connexion between azoospermia in men and the
discovery of inflammatory residues in their childless wives, is a very
intimate one. The husband at the time of marriage was suffering
from an imperfectly cured gonorrhoea, and infected his wife. In
the other class of cases, in which the women had had children, and
subsequently become sterile, the limitation of fertility depended
chiefly upon inflammatory residues in and around the ovaries and
the tubes. In the majority of such cases, pregnancy is not rendered
impossible, but merely difficult, for, notwithstanding the presence
of very extensive inflammatory residues, the tubes are often pervious,
and the ovaries fully or partially functional. Therefore, even
in cases in which intrapelvic inflammation has been very severe,
we must be cautious in giving a prognosis that pregnancy has been
rendered impossible, for the cases in which both ovaries are imbedded
completely in pseudo-membranes, or in which both tubes
have been rendered impervious, are unquestionably rare.
558Carcinoma of the uterus rarely causes sterility. In its initial
stages, in which there is merely papillary proliferation of the portio
vaginalis, or carcinomatous infiltration of the deeper layers of the
mucous membrane, no hindrance is offered to conception; but even
in the later stages of the disease, when ulceration has occurred,
and when there is extensive necrosis of the cancerous masses, there
is not necessarily any absolute impossibility of the occurrence of
conception, so long as cohabitation remains possible, and no insuperable
hindrance has risen to the contact of ovum and spermatozoon.
The cases are numerous in which pregnancy has been
observed, notwithstanding extensive carcinomatous disease of the
cervix, with necrosis of the tumour tissue; and Cohnstein even asserts,
though in this he goes too far, that cancer of the cervix
actually favours impregnation. Among 127 cases of this kind,
there were 21 in which the disease had existed for a year or more
before the occurrence of conception.
Winckel summarizes in the three following propositions his experience
regarding the relation between uterine carcinoma and
sterility: 1. Married women form the very large majority of those
affected with carcinoma of the uterus; 2. The marriage of such
women has very rarely proved sterile; 3. On the contrary, the
women affected with this disease have generally been exceptionally
fertile.
Other tumours of the uterus cause sterility, not merely by giving
rise to mechanical interference with the necessary contact of ovum
and spermatozoon, but also by leading to catarrhal states and hyperplasia
of the mucous membrane, which interfere with the implantation
of the ovum, even when fertilization has been effected.
Uterine polypi give rise to mechanical obstruction of the os uteri
externum or of the cervical canal; but they predispose to sterility
in an additional way, inasmuch as in a woman affected with such a
new growth any vigorous bodily movement is apt to cause profuse
uterine haemorrhage.
In cases of myoma of the uterus, apart from the mechanical
hindrances to conception imposed by these tumours, there is also
interference with the implantation of the ovum. When numerous
myomata have formed in the uterine wall, the mucous membrane
is usually smooth and atrophied, and discharges a watery secretion,
and for these reasons the imbedding of the ovum in the uterine
cavity is rendered extremely difficult. But that there is often an
additional cause of sterility in cases of myomata uteri, has been
shown by the researches of Schorler, who examined 822 patients
affected with fibromyoma of the uterus. He found that in most
of those in whom sterility was observed, the tumours were not
submucous but subserous, and that the sterility was to be explained
559in these cases by the frequent occurrence of partial peritonitis, with
its evil results to the uterine annexa.
Schorler appends the following table:
|
|
|
Sterile. |
Percentage. |
| Of |
85 |
women with interstitial myoma |
21 |
24.7 |
| Of |
92 |
women with subserous myoma |
44 |
47.8 |
| Of |
18 |
women with submucous myoma |
7 |
38.8 |
| Of |
44 |
women with polypous myoma |
4 |
9.0 |
| Of |
14 |
women with cervical myoma |
3 |
18.7 |
| |
|
|
|
|
| |
253 |
|
79 |
31.2 |
When there are polypous new formations in the uterine cavity,
even if conception occurs, abortion follows, for the reason that the
rupture of the hypertrophied capillaries in the growths themselves
and in the neighbouring tissues, prevents the normal development of
the embryo. Horwitz has, however, described a case in which
pregnancy went on to full term, notwithstanding the existence of
growths of this nature.
Owing to the frequency with which chronic metritis and endometritis
ensue upon parturition, it can readily be understood that delivery
itself is often the primary cause of subsequent sterility. A
temporary sterility often follows the first delivery. It is well known
that the birth of boys is in general more difficult than the birth
of girls; Pfannkuch collecting information regarding the first and
second deliveries of 300 married women, ascertained that after 166
of the first deliveries, in which boys were born, the average lapse of
time to the second delivery was 30.2 months, whereas after 134 of
the first deliveries in which girls were born, the average lapse of
time to the second delivery was only 27.4 months.
The importance of previous delivery in leading to sterility, in
consequence of mesometritis and diffuse connective tissue hyperplasia
of the uterus, is shown by von Grünewaldt, who published
the following figures as a result of his investigations. Of 56
women affected with chronic metritis, 46.4% were sterile; in 19.2%
of these the sterility was congenital, in 80.7% it was acquired. Of
134 women suffering from myometritis and its consequences, 71.6%
were sterile; in 17.7 of these the sterility was congenital, and in
82.2% it was acquired. On the other hand, of 321 women suffering
from endometritis, 29.5% were sterile; in 28.4% of these the
sterility was congenital, and in 71.5% it was acquired.
Lier and Ascher also insist upon the importance of puerperal
diseases in the causation of acquired sterility, basing their opinion
upon Prochownick’s clinical material. They draw, however, the
following distinction. If the puerperal infection takes place by way
of the external organs of reproduction, through the vagina to the
560cervix and thence to the connective tissue of the pelvis—the most
common form, that which occurs soonest after delivery, and the
most severe in its course—the women thus affected are likely soon
to become pregnant again; if, on the other hand, the disease is pelvic
peritonitis, the exciting cause of the inflammation proceeding
from the interior of the uterus through the Fallopian tubes to reach
the peritoneum, in the majority of cases the women thus affected
will prove sterile for a long time or in perpetuity. In almost all the
cases in which sterility resulted, the pelvic peritoneum had been
severely affected by the puerperal inflammation. Regarding sterility
in women, the two following general propositions are laid down
by Lier and Ascher: 1. Hardly any single cause of sterility in
women is so severe as to be competent by itself to render sterility
inevitable throughout the period of sexual maturity, with the exception
of defects of development and premature cessation of sexual
activity. 2. Most of the hindrances to conception in women depend
upon affections of the internal superficies of the reproductive
organs, from the vulval mucous membrane upwards to the pelvic
peritoneum; of these, the most important are affections of the endometrium.
On the other hand, it must not be forgotten, that the general
tendency of a previous delivery is to increase the capacity for impregnation.
Olshausen especially insists upon the well-known
gynecological fact, that as a result of the first delivery, there occurs
an enlargement of the os uteri, which facilitates conception throughout
the remainder of the period of sexual maturity. This is well
shown by the not infrequent cases in which sterility persists for
several years after marriage, and then, with or without artificial aid,
the first pregnancy occurs; thereafter one child after another appears
in rapid succession.
Spiegelberg has pointed out that cervical lacerations may give
rise to sterility by interference with the incubation of the ovum.
Olshausen maintains that this affection is liable to cause abortion,
for the reason that by the gaping of the cervical canal the inferior
pole of the ovum is from time to time exposed, and this gives rise
to reflex contractions of the uterus.
Von Grünewaldt publishes figures in support of his opinion that
disturbances of the integrity of the uterus, whereby the implantation
and further development of the ovum are interfered with, play
on a whole a greater part in the causation of sterility than the
various conditions previously described which interfere with contact
of ovum and spermatozoon. But in this, we think, he goes too far.
Finally, in this connexion, must be mentioned among the hindrances
to fertilization, sexual excesses, such as are so common during
the first weeks of married life. Too frequent coitus gives rise to
561enduring congestion of the uterus, and hence to an irritable state of
the uterine mucous membrane, whereby the implantation of the
ovum is rendered difficult. In prostitutes chronic metritis, due to
the excessive frequency of intercourse, may be a contributory cause
of the sterility which is almost invariable in these women; doubtless,
however, the principal cause of their sterility is gonorrhoeal
perimetritis.
As a variety of the third kind of sterility, sterility due to incapacity
for implantation or further development of the ovum, must
be classed the cases in which, though conception and implantation
of the ovum are known to occur, and the first stages of development
of the embryo certainly take place, the woman proves incapable
of giving birth to a viable infant. Some of these cases depend
upon abnormal modes of development, myxoma of the chorion and
the like. In rare cases, women abort every month, discharging
every four weeks a fully developed decidua vera, in which sometimes
no trace of ovum can be detected. But this monthly abortion
ceases as soon as marital relations are interrupted.
It would be passing beyond the scope of this work to discuss the
pathological processes which lead to premature interruption of the
pregnancy, after conception, implantation of the ovum, and the first
stages of development, have occurred in a normal manner; to discuss,
in short, the causes of abortion. Moreover, these pathological
processes are outside the concept of sterility. It is sufficient here
to enumerate the principal conditions in which abortion occurs.
They are: various tissue disorders of the uterus, chronic hyperaemia
of the mucosa, displacement of the uterus with fixation, parametric
and perimetric exudations, laceration of the cervix with
ectropium; further, various constitutional disorders, such as the
specific fevers, acute infective processes, chronic circulatory disturbances
consequent upon cardiac, pulmonary, renal and hepatic
disease, syphilis, anæmia, chlorosis, diabetes, etc.
Only-Child-Sterility.
Until recently, only-child-sterility had received attention in England
only, for the reason that it is comparatively common in that
country; but this form of relative sterility is by no means rare with
us (in Germany and Austria) also. I had a collection made in
Austria of the number of children resulting from 2000 fruitful
unions, and found that among these there were 105 marriages in
which one child only had been born; thus the ratio of these marriages
to those which proved fully fruitful was about 1 : 19. But
the figures are untrustworthy, since abortions and deaths in infancy
were not taken into account. Ansell found that in England, among
5621767 fruitful marriages in which the mean age of the wives at marriage
had been 25, there were 131 cases of only-child-sterility, giving
a ratio of the latter to the fully fruitful unions of 1 : 13.
This form of relative sterility, in which the wife gives birth to
one child, and thereafter remains barren, was referred by Matthews
Duncan, either to a premature exhaustion of the reproductive capacity,
the general bodily powers remaining unaffected, or else to
a simultaneous weakening of the sexual powers and of the constitutional
force in general. This explanation is a very inadequate one.
The significant fact upon which an understanding of the nature of
only-child-sterility must be based, is that the first delivery is the
one which entails the greatest dangers to the mother, and that the
subsequent sterility is attributable to the difficult delivery, and to
the illnesses that follow in its train. In fact, only-child-sterility is
observed chiefly after difficult deliveries, followed by long enduring
inflammatory processes of the uterus and the uterine annexa, which
seriously affect the woman’s reproductive capacity. It occurs especially
in delicately organized, anæmic, scrofulous women, whose
powers of resistance have been undermined by a single pregnancy
and parturition. Finally, it is met with in women suffering from
myoma uteri, a form of tumour which beyond others renders the
recurrence of pregnancy difficult and unlikely. This form of sterility
has been seen also in cases in which comparatively soon after the
birth of her first child, the mother has suffered from typhoid, scarlatina,
or some other severe infective fever, which appears in some
way to interfere for the future with the development of normal ova.
We must also take into consideration the fact that at the time of
the wife’s first confinement, when the love which brought about the
union has often already begun to diminish in intensity, the husband,
finding too irksome the continence enforced upon him by his wife’s
condition, is not unlikely to go elsewhere for temporary sexual
gratification, and to acquire a venereal disease, which he subsequently
transmits to his wife, and which is responsible for the latter’s
future sterility. And we must not forget to take into account
the adoption of means for the prevention of pregnancy after the
first child has been born. Again, I saw three cases of only-child-sterility
in which the husbands were respectively 24, 26, and 29
years older than their wives, and in these instances no profound
search was needful for the discovery of the cause of the wife’s unfruitfulness;
it was obvious that in each case the elderly husband’s
reproductive powers had sufficed for the procreation of a single
child, but had then been completely exhausted. My experience in
the mysteries of sterility in women has informed me of yet another
cause of only-child-sterility, met with in cases in which the only
child was born after several years of unsuccessful marital intercourse.
563In most of these cases, the wife has finally been impelled
to seek a substitute for her husband, whose reproductive powers
have proved insufficient; having succeeded in obtaining the child
she desires, the wife does not again wander in strange pastures, and
consequently remains sterile.
According to Kleinwächter—who gives a somewhat wider significance
to the term “only-child-sterility,” including as he does
cases of premature interruption of the first and only pregnancy,
since these even more frequently entail permanent sterilization—only-child-sterility
is by no means rare. Among 1081 gynecological
cases, he observed it in 90, that is, in 8.32% of the cases. In these
90 cases, there were 69 instances in which the sterility ensued upon
full term delivery, and 21 instances in which it followed abortion
or premature delivery. Kleinwächter, moreover, on the basis of his
personal experience, supports my view of the importance of the
sterilizing influence of the first delivery; but he has been unable to
determine whether early marriage has any influence in the production
of only-child-sterility.
Lier and Ascher also class as instances of only-child-sterility
those cases in which a woman has had a single miscarriage, and
subsequently remained sterile, since by this miscarriage the capacity
of the woman for impregnation has been proved, and the
question of capacity for full-term delivery has nothing to do with
that of capacity for conception. As causes of this form of sterility,
they lay especial stress upon puerperal infection, gonorrhoeal infection,
perimetritis, tubo-ovarian tumours, etc.
Operative Sterility.
Finally, in order to complete the etiologically classified series of
forms of sterility, we must allude to yet another variety of sterility
which is due to the surgical direction of modern gynecology, viz.,
operative sterility. However much we may prize the gains we owe
to modern operative gynecology, it cannot be denied that the new
developments have brought many evils in their train. Not the least
of these is operative sterility, due to operative procedures involving
the female reproductive organs, by which, whether intentionally or
unintentionally the reproductive capacity is destroyed. Doubtless,
in certain severe organic diseases of the female reproductive apparatus,
in which the use of the knife is indicated, the fact that by
operating we are sterilizing the patient cannot even be taken into
consideration; but many sins have been committed in this kind, and
with a ready hand, and, be it openly admitted, with an easy conscience,
many an eager operator has undertaken the destruction of
a woman’s potentialities for motherhood, without having given the
564careful consideration that is demanded by the irreparable character
of his undertaking. Happily, however, the time has nearly passed
away, in which it could be said of many a gynecologist, that no
ovaries and no Fallopian tubes were safe from his operative zeal,
and from his desire to heap up a mountain of statistics.
Three operative measures very commonly undertaken at the
present day are responsible for the production of operative sterility:
ovariotomy, oophorectomy, and salpingotomy.
The removal of the ovaries, with the object of permitting to the
women concerned unbridled sexual indulgence without risk of consequences,
was performed, according to Strabo, by the ancient Egyptians
and Lydians. The same practice is described by modern
writers as occurring in Hindustan (Roberts), and in Australia
(Miklucho-Mackay).
With a curative aim, the removal of the ovaries was first undertaken
in the early years of the nineteenth century, although the
operation had already been discussed as a possibility by leading
physicians of the eighteenth century. The first ovariotomy for the
removal of an ovarian tumour was performed by MacDowell in the
year 1809. During the last three or four decades, the operation has
become an extremely common one, and is performed by the surgeons
of all nations. Removal of a single ovary, as long as the other
ovary is healthy, does not necessarily lead to any impairment of
fertility; but when both ovaries are removed, operative sterility is
the necessary result. In order to avoid this, Schröder has recommended
that a fragment, at least, of healthy ovarian tissue should
be left behind, in order to preserve the reproductive capacity. In
discussing the subject of impaired ovulation, we have already mentioned
cases in which pregnancy has occurred after bilateral removal
of the ovaries, a circumstance explicable only on one of two
assumptions, either that a fragment of ovarian tissue was left behind,
or else that a supernumerary ovary existed.
The extirpation of healthy ovaries, or at any rate, of ovaries
which are not notably enlarged, is known as oophorectomy (spaying,
Battey’s operation, in Germany, castration). It dates from the
year 1869 (Koeberlé); but in the strictly modern sense the operation
was first performed by Hegar in the year 1872. [Lawson Tait
removed both ovaries for pain in October, 1871. Battey’s first operation
of this kind was successfully performed on August 17th, 1872;
this was three weeks subsequent to the first performance of the
operation by Hegar of Freiburg. But Hegar’s patient died from
the operation, and Hegar did not publish the case at the time—Transl.]
The aim of ovariotomy is to remove an ovarian cystoma;
if the other, apparently healthy, ovary is removed, it is with the
object of removing an ovarian tumour in the initial stage. Oophorectomy
565has an altogether different purpose, namely, to relieve or
cure pathological manifestations in other organs which are believed
to depend on the periodical recurrence of ovulation, to cure them by
instituting a premature menopause. At one period, when overzealous
operators performed oophorectomy for the supposed relief
of comparatively unimportant nervous affections, and the statistics
of the operation began to assume gigantic proportions, operative
sterility actually came to play no inconspicuous part on the stage of
sterility in general. But a reaction inevitably followed; severe
diseases were alone considered as furnishing sufficient indications
for the operation; of late it has been performed chiefly in cases in
which the primary disorder has already rendered the occurrence of
pregnancy impossible, or at any rate very unlikely, or, finally, if
probable, yet to be avoided, on account of the dangers it would entail.
In short, the fertility of women is no longer seriously threatened
by this operation.
Some years ago, I was consulted by a beautiful married woman,
26 years of age, of a blooming and healthy aspect. When a young
girl, she had suffered every month at the time of the menstrual
flow from violent vomiting, accompanied by various spasmodic
troubles. Just at this time, oophorectomy was the fashionable operation
for the relief of nervous troubles; this girl was subjected to
the operation, and the vomiting at the periods ceased, but the other
nervous symptoms persisted without alleviation—indeed were at
times worse than before. Since then, she had married a man belonging
to the upper circles of society; and now, after living for
four years in sterile wedlock, she came to me to ask my advice as to
whether anything could be done to enable her to have a child! Two
other cases have come within my own knowledge, in which women
whose ovaries had been removed on account of nervous troubles,
had subsequently married, and felt most unhappy owing to their
hopeless state of sterility.
It is impossible to make even an approximate estimate of the number
of women who in recent years have had their ovaries removed
during the period of sexual maturity, and who have thus been made
the subjects of operative sterility; nor is it possible to ascertain in
what proportion of cases the healthy ovaries, the normal female
reproductive glands, have been removed for the problematical relief
of nervous troubles or of uterine haemorrhage, and in what
proportion of cases there has existed a genuine indication, owing to
the presence of fibromyoma of the uterus, for the induction of an
artificial and premature menopause. Unquestionably, the number
of women thus operated on during the menacme is by no means a
small one. In a work by Hermes, “On the Results of Oophorectomy
in Cases of Myoma of the Uterus,” Archiv für Gynecologie,
5661894, we find that, among 55 women whose ovaries were removed
on account of myoma of the uterus, there were 52 who were between
the ages of 21 and 45, i. e., in the period of sexual maturity. The
assumption that all these patients were already sterile before the
operation, on account of a degenerate condition of the uterine annexa,
cannot be justified.
Keppler, indeed, puts forward a very remarkable defence of
the removal of the ovaries of women who are competent to become
mothers, asserting that such oophorectomy offers no obstacle to
marriage, and that many women who have been operated on in this
manner are extremely happy in conjugal life. Marriage with a
wife whose ovaries have been removed is the ideal Malthusian
marriage, the one way in which Malthusianism can be practised
without endangering the health and life-happiness of the participators!
Another danger soon appeared, one which threatened the fertility
of women to an even greater extent, in the form of operations on the
uterine annexa—the first salpingotomy was performed by Hegar
in 1877. As knowledge advanced of the various diseases of the
Fallopian tubes, salpingitis, hydrosalpinx, and pyosalpinx, whilst at
the same time the development of the antiseptic method rendered
operative gynecology continually bolder and bolder in its undertakings,
there was disclosed an extensive field for radical measures
in removal of the tubes, generally combined with removal of the
ovaries, since these latter organs commonly were found to have
suffered from association in the destructive inflammatory process.
The operation of salpingo-oophorectomy soon became a very common
one; and since patients with diseased tubes are for the most
part still comparatively young, in the period of sexual maturity,
there arose a new and frequent variety of operative sterility, and
one which the zeal of American gynecologists made especially common
on the other side of the Atlantic. An American gynecologist,
indeed, has sarcastically observed that “It is the dish-full of excised
tubes that shows the master gynecologist”; and Landau has been
impelled to lament that “salpingotomy has been performed on a
very large number of women who have complained of nothing
more serious than uterine haemorrhages, or of insignificant pains,
and even on some women who have come to the gynecologist with
no other complaint than that—they are sterile”! Fritsch, also,
writing of the too rapidly formed diagnosis “tumor of the annexa,”
and the consequent resort to operation, remarks: “I know many
a happy mother who at one time had worn every variety of pessary,
had been through every kind of ‘cure,’ and had visited every accessible
spa; until, at last, she came to consult me, with the express wish
to have her ovaries removed. Latterly, she had been advised to this
567course by every physician she had consulted. I agreed, in such
cases, to perform the operation, with the stipulation that first of all,
for the space of an entire year, the patient should not see a single
doctor, should visit no spa, should take no medicine, and, in short,
should pay no attention whatever to her health. The success of this
course of ‘treatment’ was often extraordinary. As soon as the
reproductive organs were left in peace, recovery ensued.” The
conservative tendencies of the surgery of the last decade, have manifested
themselves also in the department of gynecology, for the
happy protection of woman and her reproductive capacity. Operative
measures are now commonly restricted to the relief of certain
severe forms of disease of the uterine annexa; in cases of chronic
inflammation of the annexa, the surgeon often contents himself with
dividing or breaking down the adhesions, and leaves the organs in
situ; even in cases of bilateral disease, one tube only may be removed;
whilst in the most recent method of all, after opening the
abdomen, and separating the pelvic organs from their adhesions,
an aperture is made in the closed tube, and this artificial ostium is
brought into apposition with the ovary by the insertion of sutures.
In a word, surgeons have come to realize that they have in the
past been too ready to sterilize their patients by the performance of
double salpingo-oophorectomy, and are much more reluctant than
formerly to sacrifice the ovaries and the Fallopian tubes.
Porro’s operation is another cause of operative sterility, excision
of the ovaries being combined with the partial excision of the uterus,
whereas sterility was seldom the consequence of the older method of
Caesarian section. Indeed, Porro’s operation has been extolled precisely
on this account, that, indicated as it is for the relief of extremely
difficult labour, it renders it impossible for the same difficulty
and danger ever to recur.
The classical operation of Caesarian section, if the patient makes
a favourable recovery, does not involve sterility, unless in very exceptional
cases (as in one described by Lecluyse, in which, after the
Caesarian section, a communication persisted between the uterine
cavity and the cavity of the abdomen, through which the semen
passed during coitus). Occasionally, also, in performing the older
operation, the operator has thought it right to prevent the future
recurrence of pregnancy by adding an oophorectomy to the primary
operation.
Pregnancy and parturition are still possible after the healing of
spontaneous or traumatic ruptures of the uterus; but it must be remembered
that after such serious injuries, as after extensive operative
procedures on the pelvic organs, widespread peritoneal inflammation
is apt to occur, with perimetritic and parametritic exudations,
leading commonly to sterility.
568Amputation of the vaginal portion of the cervix, an operation
sometimes undertaken for the relief of sterility in cases of hypertrophy
of the cervix, may on the other hand lead to sterility in
cases in which a cicatricial stenosis of the cervical canal results
from the operation.
By the too frequent application of caustics to the cervical canal,
or by the employment of these agents in too powerful a form, occlusion
of the os externum may be caused, or even adhesion of the
opposing walls of the vagina just below the cervix, thus giving rise
to sterility. Rough use, also, of the uterine sound, and maladroit
and violent gynecological massage, have often enough been responsible
for the occurrence of sterility, by giving rise to perimetritic
inflammation. Landau enumerates among the causes of intrapelvic
abscesses, “whereby the specific functions of womanhood are nullified
in consequence of degeneration of the tubes or the ovaries,”
“certain therapeutic procedures,” and more especially, intra-uterine
therapy, (the use of the sound, curettage, injections, cauterization),
and operations on the cervix or the vagina, on which intrapelvic
inflammation and even suppuration has ensued. How easily pelvic
peritonitis and its consequences lead to sterility in women, has been
shown many times in the course of our exposition of this subject.
Finally, we must class with operative sterility the result of surgical
procedure undertaken by gynecologists to save women, whose
lives have already been seriously threatened by pregnancy or parturition,
from a repetition of this experience. In such cases, Blundell
recommends division of the Fallopian tubes, having found
from experiments upon rabbits that this is a safe and certain
means for the prevention of conception. Frorieps and Kocks have
both frequently brought about an artificial sterility in women by
closure of the tubes, the first-named by cauterization with nitrate of
silver—the caustic being attached to the end of a piece of whalebone
and introduced through a canula into the uterine orifice of the
Fallopian tube—whilst Kocks has constructed for the same purpose
a galvano-caustic uterine sound, which is only rendered red-hot
by passage of the current after it has been introduced into the
uterine ostium of the tube. Both these methods are in the first
place too uncertain to be relied upon for the attainment of the
desired end, and in the second place their employment appears to
be neither easy, nor free from danger.
As the importance of conservative methods of procedure becomes
once more fully recognized in modern gynecology, cases of operative
sterility will become ever more and more rare.
569
TABLE SHOWING THE CAUSES OF STERILITY IN WOMEN.
I. Sterility due to Incapacity for Ovulation.
ABSOLUTE AND IRREMEDIABLE.
Complete absence of the ovaries.
Congenital atrophy of both ovaries.
Premature atrophy of the ovaries, in
consequence of infectious disorders,
constitutional diseases, and toxic
influences.
New-growths of the ovaries, destroying
all the follicles.
Senile changes in the ovaries.
Complete oophorectomy, or any
equivalent form of operative sterility.
RELATIVE AND TRANSIENT.
Incomplete development of the
ovaries.
Imperfect formation of ova, owing to
marriage when still too young
(amenorrhœa).
Ovarian tumours and oophorectomy,
whereby, however, a remnant of
healthy ovarian tissue is spared.
Chronic oophoritis and perioophoritis;
syphilitic disease of the ovaries.
Excessive obesity, anæmia, chlorosis,
scrofula, morphinism, alcoholism,
various conditions affecting unfavourably
the innervation or nutrition
of the ovary; change of climate
or mode of life; emotional disturbance;
inbreeding, hereditary predisposition.
II. Sterility due to Interference with the Contact of Normal Spermatozoon and Ovum.
A. On the Part of the Wife.
ABSOLUTE AND IRREMEDIABLE.
Congenital or acquired universal
thickening of the tunica albuginea
of the ovaries, preventing the dehiscence
of the follicles.
Absence of both tubes, developmental
defects of these organs.
Absence or rudimentary condition of
the uterus. Foetal uterus.
Congenital atresia of the uterus with
arrest of development.
Complete absence of the vagina.
Extreme contraction of the pelvis,
whereby the vagina is rendered inaccessible.
Hermaphroditism.
RELATIVE AND TRANSIENT.
Remediable thickening of the tunica
albuginea, inflammatory remnants
of perioophoritic processes, diseases
of the cervical glands, dislocations
and adhesions of the tubes, narrowing
or obliteration of the ostia, inflammation
of the tubes, pyosalpinx,
obliteration of the lumen of the
tube.
Retro-uterine haematocele.
New growths in the uterine cavity.
Infantile and pubescent uterus.
Primary atrophy of the uterus.
Puerperal atrophy of the uterus.
Displacements of the uterus—versions
and flexions.
Hypertrophy or atrophy or changes
in the shape of the cervix, cervical
stenosis.
Cervical catarrh, especially when gonorrhoeal.
Ectropium of the cervix.
Spasmodic dysmenorrhœa.
Atresia of the vagina, obliteration of
the canal by scars or tumours.
Abnormal termination of the vagina—vesico-vaginal
and recto-vaginal
fistula.
570Absence of the external organs of
generation and partial absence of
the vagina, without defect of the
internal organs of generation.
Abnormalities of the hymen.
Pathological states of the genital secretions.
Vaginismus.
Dyspareunia.
Perversion of the sexual impulse.
B. On the Part of the Husband.
ABSOLUTE AND IRREMEDIABLE.
Diseases of the central nervous system,
and certain constitutional diseases.
Congenital or acquired absence of
both testicles.
Atrophy of the testicles.
Complete azoospermia and aspermatism.
Senile impotence.
RELATIVE AND TRANSIENT.
Developmental defects of the penis,
and acquired deformities of that
organ.
Stricture of the urethra.
Oligozoöspermia.
Nervous impotence.
Gonorrhoeal and syphilitic infection.
The employment of measures for the
prevention of pregnancy (facultative
sterility).
III. Sterility due to Incapacity for the Implantation and further Development of the Ovum.
ABSOLUTE AND IRREMEDIABLE.
Arrested development of the uterus.
Complete atrophy of the uterine
mucous membrane.
RELATIVE AND TRANSIENT.
Chronic metritis.
Chronic endometritis, especially gonorrhoeal
and exfoliative endometritis.
Perimetritis, parametritis, pelvic peritonitis;
the consequence of these
inflammations.
Tumours of the uterus.
Displacements of the uterus.
571
III. SEXUAL EPOCH OF THE MENOPAUSE.
The Menopause.
That time in a woman’s life at which her sexual activities come
to their natural termination, marked by the cessation of menstruation,
is known as the menopause, climax, or climacteric period.
This “change of life,” from a condition of sexual maturity to a
condition of quiescence of sexual functions, is not a sudden one,
the symptoms of sexual retrogression making their appearance gradually,
until the cessation of the monthly recurring menstrual flow
indicates that the termination of sexual activity has arrived, and
that sexual death is taking place.
The influence of this period of life is not manifested by the sexual
organs alone—in these latter indeed various changes may be detected
already before the cessation of menstruation, whilst after that
cessation, the atrophic changes characteristic of old age proceed in
these organs with a slow but continuous advance,—but the disturbances
evoked by the climacteric involve the entire organism and
affect the functions of numerous organs, giving rise to a true storm
of irritant phenomena, and to manifestations of decay of manifold
nature.
The stormy manifestations, the occurrence of which led the
ancients to denote this period as the “critical age” of a woman’s
life, are in the first place due to changes in the ovaries; the tissue
changes in these organs give rise to a powerful ovarian stimulus,
which, by irradiation and reflex action, leads to the occurrence of
a number of nervous disturbances, vasomotor manifestations, and
circulatory disorders; whilst owing to the cessation of the internal
secretions of the ovaries, numerous and intense pathological disorders
of metabolism arise. These various symptoms become apparent
at the very outset of the menopause, when the oncoming
entire cessation of menstruation is already foreshadowed by irregularity
in the periods, gradual diminution in the quantity of the
flow, and variations in the number of days during which the flow
on each occasion persists.
The manifestations of the menopause are in fact so striking, that
from ancient times down to the present day a widespread belief has
prevailed that especial danger to a woman’s life is threatened by
572the climacteric age. The statistics available on this subject are,
however, of dubious significance. Although it cannot be denied
that the changes in the entire organism which attend the extinction
of sexual activity, bring numerous dangerous influences into
play, yet I feel bound to maintain that these dangers are by no
means so great as those which are involved by the sexual life in its
ripest period of development—the dangers of pregnancy, parturition,
and the puerperium.
It is often asserted that in this “critical period” of the menopause,
the mortality of the female sex is notably increased. The
data available are somewhat conflicting, but a careful examination
leads us to believe that, if due allowance is made for the natural
increase in mortality with advancing years, no important increase in
the mortality of women can be traced as due to the troubles and
disturbances of the climacteric period.
The age at which a woman’s last sexual epoch begins is a very
variable one. The duration of the “change of life,” the length of
time during which the occurrence of the “change” is manifested
by local and general disturbances, also varies greatly. Not less
variable are the intensity and the general distribution of the symptoms
which mark the climacteric.
The external configuration of woman at the climacteric age is
usually characterized by signs of over-ripeness, and these changes
appear to exercise upon certain men—more especially very young
men—a peculiar kind of erotic stimulus. Many women remain
long at this period quite fresh looking, with a vivid, youthful colouring;
others, however, early manifest alterations in their finer
feminine characteristics, hairs, for instance sprouting on the chin,
and the voice becoming deeper in tone.
The outward characters of senescence, with withering of the
tissues, are not commonly manifested at this time, but first make
their appearance in later years, after the completion of the menopause.
A tendency to the excessive accumulation of fatty tissue is one
of the most distinctive characteristics of the menopause, varying,
however, greatly in degree according to race, family predisposition,
and nutritive conditions. The dominant tone is thus given to the
physical configuration by the deposit of fat. The face comes to
have a rounded, spherical appearance, the eyes looking smaller in
proportion, whilst the furrows and folds which form the natural
boundaries between the features become indistinct. The formation
of the “double chin,” and the abundant deposit of fatty tissue in
the supraclavicular region, gives to these extremely obese women
an appearance of such a shortening of the neck, that head and
thorax seem to be connected as it were by a great mass of fat,
573marked by furrows in the thyroid and sub-hyoid regions. The
breasts sometimes attain an enormous size, hanging down to the
gastric and even to the umbilical region. The abdomen is greatly
enlarged, the fat in the anterior abdominal wall projecting more
especially in the hypogastric region, hanging down in two or three
horizontal rolls over the tops of the thighs, and pushing the mons
veneris downwards, so that this latter itself projects over the genital
fissure. The posterior projection of the buttocks is also greatly increased,
until they form a huge elastic cushion, of which the sensual
orientals, who regard obesity in women as a beauty, poetically
write: “Her face is like the full moon, and her buttocks are like
two pillows.” Occasionally, so huge a mass of fat forms beneath
the tuberosity of the ischium, that the configuration of the nates
reminds us of the well-known steatopyga or fat-rump of the Hottentot
and Bosjesman women. In the genital organs, as already
mentioned, the genital fissure is hidden by the projection of the
mons veneris. The labia majora are also greatly enlarged by
the deposit of fat, so that they look like two great cylinders lying
side by side. Another way in which the characteristic sexual
beauty is often lost in extremely obese women, is by the falling out
of the pubic hair.
Moreau, in his work on The Natural History of Woman, describes
the changes occurring in a woman at the climacteric in similar terms,
and concludes: “The only elements of a woman’s beauty that may
sometimes be saved from the wreck, to persist for a shorter or
longer time after the climacteric, are, the abundance of her hair, the
vivacity of her glance, and sometimes also the amiable expression of
her countenance; gradually, however, even these last remnants of
beauty disappear, and old age takes possession with its irresistible
force.”
None the less, some women may preserve substantial elements of
beauty for a long time after the menopause. A classical example
of this fact is furnished by Ninon de l’Enclos. When she
died, at the age of 90, she was still beautiful. At the age of 65 she
aroused the passionate love of a young man, who, unfortunately,
was her own son. When informed of this, he committed suicide.
A young abbé fell in love with her when she was 75 years old.
The psychical life of woman is profoundly affected by the stormy
physical changes of the climacteric. Not merely does a woman
entertain the disturbing thought that the critical age has begun,
bringing in its train certain dreaded dangers to her health and even
her life, but she is further depressed by the consciousness that she
is about to lose her feminine attractions, and to decline in sexual
esteem, and that her reproductive capacity is now to be extinguished.
She realizes vividly that the beautiful past, the loving and beloved
574womanhood, is now to be left behind for ever, and by this an intelligent
and sensitive woman cannot fail to be profoundly affected.
Her feelings at this time were never more characteristically expressed
than by the Frenchwoman who said “Autrefois quand
j’étais femme.” If, indeed, a woman has been so fortunate as to
have made a happy marriage, to have borne healthy children, and
to be living a satisfactory family life, she will be enabled to bear
with comparative equanimity the disappearance of her sexual life;
but it is different with the childless wife and with the unmarried
woman, who, at the onset of the climacteric, must bury all their
sexual aspirations, and who see the remainder of their lives stretch
before them without hopes for the future. The psychical predisposition
and the intellectual education of the woman concerned,
will now determine whether she will bear the onset of the menopause
with composure and resignation, or whether she will become
a prey to melancholia. Women of the former kind will seek to find
employment for the powers set free by their sexual non-activity, in
services of neighbourly affection, in works of benevolence, and in
the performance of social duties; women less happily endowed will
display their hostility to the world in ill-nature, scandal-mongering,
and intrigue, thus giving vent to their inward bitterness; whilst
those, finally, with hereditary predisposition to nervous degeneration,
will become the prey of veritable psychoses.
A by no means rare result of the excited fantasy and of the eager
desire not to grow old, is displayed at the climacteric in the form of
self-deception. The women thus affected cannot understand, and
cannot be made to believe, that the cessation of menstruation is the
natural sign of their sexual decadence, they trick themselves into
believing that in their case it is a sign that they have become pregnant.
We must not indeed forget that the enlargement of the
abdomen, so common at the commencement of the climacteric, in
association with the unexpected failure of the menstrual flow to
appear, the frequent dyspeptic troubles, and the enlargement of the
breasts in consequence of the deposit of fat in these organs, often
enough lead to appearance which have a deceptive resemblance to
the clinical picture of early pregnancy. The mistake is the more
readily made because the breasts sometimes secrete a serous fluid,
whilst sacrache is not infrequent, and peristaltic movements of the
intestines are mistaken for the movements of the foetus. Cases of
this kind, in which all the objective signs of pregnancy appear to be
present, and in which it is impossible to convince the woman that
she has been deceiving herself, and that all the signs and symptoms
are due to the menopause, are mentioned already by very early
writers, and have been frequently reported by modern gynecologists.
575(An example of spurious pregnancy especially familiar to English
readers is that of Mary I, Queen of England. Transl.)
Sexual desire in woman by no means reaches its physiological
term with the climacteric and the cessation of menstruation. On
the contrary, we have observed it to be the rule that shortly before
and at the commencement of the climacteric, there is a considerable
increase in the libido sexualis, and at the same time an increase in
sexual sensibility during coitus. This sexual erethism makes its
appearance in a manner often extremely surprising to the husband—and
especially surprising in the case of women who have previously
been characterized by a certain frigidity in sexual matters,
and who have, perhaps, always needed strong persuasion before they
would consent to perform their marital duties. It is by no means
rare for the increased sexual impulse to manifest itself in some
pathological form. Even some time after the menopause, when
senile changes in the genital organs are far advanced, the sexual
impulse may still be remarkably active. There is an interesting
analogy in the fact that Glaevecke observed that the sexual impulse
was persistent in women in whom an artificial menopause had been
induced by oophorectomy; and that Lawson Tait and L. Smith have
reported cases in which dyspareunia, which had existed prior to the
operation, passed away after the removal of the ovaries, so that
after the artificial menopause, voluptas coeundi for the first time
made its appearance. Other authors, Goodell, for instance, report
that libido sexualis is retained only for a short time after oophorectomy,
but subsequently disappears, as in the course of the physiological
menopause, and that at the same time the voluptas coeundi
is entirely extinguished.
When the menopause is fully established, and the processes of
involution in the reproductive organs have taken place in a normal
manner, the woman has had time to acquiesce in the inevitableness
of the changes that have occurred, and she often attains a state of
emotional repose which was quite unknown to her in the earlier
phases of her sexual life. More particularly, those women who
hitherto during menstruation, and for some days before and after
the flow, have been the prey of numerous nervous symptoms and
troubles, rejoice, after the menopause, at their new-won freedom
from these pains and disquiets, at their delivery from the excitements
of the reproductive system, at their now uninterrupted state
of well-being.
I once saw a group of statuary by Pietro Balestra, entitled “Time
carries off Beauty.” A beautiful woman was striving in vain to
resist the overwhelming might of Chronos, whilst Cupid, about to
be abandoned, was standing sorrowfully by. Here we have a symbolic
representation of the sexual epoch of the menopause.
576In a recently published romance, “Les Demi-Vieilles,” Yvette
Guilbert has described in a manner most true to nature the feelings
of the “Half-Old,” the mental condition of women at the climacteric,
“They endeavour to remain young, to hide their defects, they
seek once again the intoxication of love. But that which aforetime
in hours of depression they have foreseen, now becomes a dreadful
reality. When the lemon has been squeezed dry, the skin is thrown
away.”
Sooner or later after the completion of the menopause, the signs
of senile marasmus become apparent. The soft, feminine configuration
of the face disappears, the features become coarser, approaching
the masculine type, hairs appear on the upper lip and on the
chin. The voice becomes deeper and harsher. As decrepitude begins,
the breasts wither, a change that occurs sooner in proportion
to the degree in which their functions have been in previous years
exercised by suckling; but also sometimes after a life of complete
sexual inactivity. Even in cases in which the loss of substance of
the breasts is apparently small, the glandular tissue of the organs
has really disappeared, and has been replaced by fat. In advanced
age, the breasts become quite small, wrinkled, flaccid, and dependent,
and sometimes atrophied to become mere cutaneous folds. The
nipples project more prominently, they are darker in colour, and
their surface is wrinkled. In the genital organs, the fat disappears
from the mons veneris, which becomes flattened, whilst the pubic
hair ceases to be curly, and much or all of it is ultimately shed. The
labia majora become thin and flaccid, until they are mere empty
folds of skin; they are widely separated, so that the vaginal orifice
is closed only by the withered nymphæ, until these latter are themselves
ultimately indicated by mere traces.
Where the menopause has been artificially induced, the signs of
senescence do not appear immediately after the removal of the
ovaries; their development is a very gradual one. The sexually
mature woman, from whom these tokens of femininity have been
removed, experiences at first little change in external configuration,
beyond a somewhat exaggerated tendency to the deposit of
fat; the other changes described do not usually set in until the
physiological climacteric age is attained. A few cases only have
been observed in which after oophorectomy a rapid change to the
masculine configuration has been observed.
Seldom if ever does it happen that menstruation suddenly ceases
without any notable constitutional disturbance, so that in a moment,
as it were, the menopause is effected, without any period of transition.
Rarely, even, do we meet with cases in which the peculiar
manifestations foreshadowing or accompanying the cessation of
menstruation last for no more than a few weeks. Most commonly
577the irregularities of the menstrual function (of which the most noteworthy
characteristic has hitherto been its extreme regularity), and
the associated symptoms of the climacteric period, endure for months,
and occasionally for years. According to my own observations, the
mean duration of the climacteric manifestations is from two to three
years, the limits of variation in individual cases being, however,
exceedingly wide.
The manifestations which accompany the cessation of menstruation
are as a rule the following: The woman is for some months
in an irritable condition, complains of digestive disturbances, constipation,
meteorism, epistaxis, haemorrhoidal flux, congestions of
the head, increasing fugitive sensations of heat (Ger. fliegende
Hitze), and a tendency to profuse perspiration.
The length of the intermenstrual interval commonly increases,
to as much as six or eight weeks; the flow itself becomes scantier.
In other cases, however, the flow becomes much more abundant, and
the intermenstrual intervals much shorter than normal. In some
cases, the regularity of the flow is altogether lost, it appears now
soon, now late, and is now scanty, now profuse. Sometimes the
intervals are several months, it may be 6, 8, and even 10 months,
then again the flow will occur every two or three weeks; in exceptional
cases, a scanty flow persists right through what should be
the interval, so that menstruation becomes continuous, with periodic
increases in the flow. Not infrequently, after a sudden cessation of
the flow lasting for many months, menstruation recurs, and continues
at regular intervals for a long time, until the final cessation
of menstrual activity.
The mode of cessation which is most favourable to a woman’s
general health, is for the duration of the intermenstrual interval
gradually to increase, whilst pari passu with this increase, the
amount of the flow progressively decreases, until it ceases altogether.
In such cases, the general constitutional disturbance is reduced to
a minimum. On the other hand, the sudden cessation of menstruation
gives rise to profound disturbance of the domestic economy
of the feminine organism, and causes violent changes therein. But
even the gradual cessation of menstruation causes notable disturbance
of the woman’s mental and physical equilibrium, if the irregularities
in the menstrual process are very great and spread over a
very long period—more especially when the loss of blood is extensive.
Even after the menopause, after the final termination of the flow,
there persists a more or less regular recurrence of certain symptoms
referable to the continuance of ovulation. Sacrache, a sense of
abdominal tension, a feeling of heat and fullness in the pelvis,
dragging pain in the hypogastrium, and general irritability, occur at
578intervals, so that the woman thus affected sometimes describes herself
as suffering from the continuance of a “bloodless menstruation.”
Tilt made observations in 637 women, in order to ascertain the
various modes in which the menopause occurs, and obtained the
following results. The menopause occurred:
| By gradual diminution of the amount of the flow |
in |
171 |
women, or |
26.84 |
per cent. |
| By sudden interruption of the flow |
in |
94 |
women, or |
14.76 |
per cent. |
| By sudden interruption and a terminal attack of metrorrhagia |
in |
43 |
women, or |
6.75 |
per cent. |
| By a terminal attack of metrorrhagia |
in |
82 |
women, or |
12.87 |
per cent. |
| By a series of attacks of metrorrhagia |
in |
56 |
women, or |
8.79 |
per cent. |
| By alternations of very profuse and very scanty menstruation |
in |
36 |
women, or |
5.65 |
per cent. |
| By irregular recurrence of menstruation, at intervals exceeding 21 days |
in |
99 |
women, or |
15.54 |
per cent. |
| By irregular recurrence of menstruation, at intervals of less than 21 days |
in |
33 |
women, or |
5.18 |
per cent. |
| By irregular recurrence of menstruation, the intervals being sometimes longer and sometimes shorter than 21 days |
in |
23 |
women, or |
3.61 |
per cent. |
| |
|
|
|
|
|
| Totals |
|
637 |
|
99.99 |
|
The two principal dangers of the climacteric period in women are,
first, the great tendency to profuse uterine haemorrhages, and,
secondly, the liability to the occurrence of malignant tumours, more
especially to carcinomatous disease of the ovaries, the uterus, and the
mammae.
With regard to the question whether, in any particular individual,
the course of the menopause is likely to be favourable or unfavourable,
there are, in my experience, four considerations of principal
prognostic significance: the condition of the woman during the
menarche, the state of the general health at the time of commencement
of the menopause, the degree to which the sexual functions
have been and are being exercised, and the manner in which the
cessation of menstruation takes place.
As a rule, the disturbances and pathological states of the climacteric
period will be especially frequent and severe in women whose
sexual development at the time of the menarche was accompanied
by severe disturbances of the general condition. In every individual,
there appears to be a certain connexion between the manifestations
attending the menarche and those attending the menopause,
of such a nature that according as puberty has been passed through
with little or with much disturbance of the general condition, a
similar favourable or unfavourable course of the menopause may
be prognosticated. If, at the time of the menarche, there were
severe nervous manifestations, or heart troubles of a serious kind,
579the passage of the menopause may be expected to give rise to
neuropathic affections and to cardiac disturbances in a similar
manner.
The woman’s state of general health is likewise of importance
in determining whether the course of the menopause will be favourable
or unfavourable. Perfectly healthy women, with a quiescent
temperament, and in favourable circumstances of life, will pass most
easily through the climacteric period without disturbance of their
general condition. Every departure from normal health has an unfavourable
influence upon the course of the climacteric. In women
of a plethoric habit of body, there is an especial tendency at this
time to the occurrence of symptoms of stasis and hyperaemia.
Chlorotic and anæmic women are more prone than others to suffer
at the time of the menopause from uterine haemorrhages. Women
of a sanguino-erethistic constitutional disposition often manifest at
this epoch a tendency to neuroses and psychoses. Those women
have the best prospect of a smooth and undisturbed passage through
the climacteric age, who enter upon it in a state of perfect health.
Less favourable is the prognosis in the case of those women who
already some time before the climax, at the outset of the fourth
decade of their lives, have begun to complain of severe haemorrhages
and various other pathological states.
Regarding the influence which the sexual activity of a woman
during the menacme exercises upon the course of the climacteric,
it may be said, generally speaking, that a previous free exercise
of the sexual functions in normal conditions has a favourable influence
upon the state of health during the menopause. Women who
have been married for many years, who have had many children,
and who have suckled these children, pass through the changes of
the climacteric much more easily than old maids, than women who
have lived for many years in continent widowhood, or than women
who have had very few children or none at all. The practice of
prohibitive coitus, i. e., the use during intercourse of methods of
preventing the occurrence of conception, a form of sexual immorality
which has become extraordinarily common during the last
few decades, has an unfavourable influence upon the course of the
climacteric. Unfavourable, also, is the effect of great sexual activity
during the four or five years immediately preceding the menopause.
Women who marry shortly before the commencement of the climacteric,
and those who have given birth to a child shortly before this
time, commonly experience very severe disturbances during the
menopause. Prostitutes who continue the active pursuit of their
profession until the climacteric age, have at this time much to
suffer. Women who have had difficult deliveries, or several miscarriages,
or severe puerperal illnesses—and indeed, speaking generally,
580those women who have been subject to any kind of disease
of the reproductive organs—are apt to suffer from serious disturbances
of the general health during the climacteric period.
The mode in which the cessation of menstruation takes place, is
also causally connected with the easy or difficult course of the menopause.
Premature cessation of menstruation, or very sudden interruption
of this function, has a deleterious effect, manifesting itself
both by local disorders of the reproductive organs, and by general
disturbances in the nervous system and in the circulatory organs.
On the other hand, a late menopause and a gradual cessation of
menstruation, are both usually accompanied by a favourable course
of the climacteric phenomena.
The influence of sexual activity upon the course of the climacteric
is described by Busch in the following terms: “Women who
have led an exhausting mode of life, who have had intercourse too
frequently, those who have been given to onanism or to some other
sexual irregularity, and who therefore enter upon the menopause
with flaccid and deteriorated reproductive organs, are liable to
haemorrhagic and mucous fluxes, to prolapse, carcinoma, dropsies,
enlargements, and suppurative processes. Women, on the other
hand, who have lived a life of strict isolation, and who have forcibly
repressed all sexual inclinations, frequently suffer from ossifications,
indurations, and atrophic conditions of the reproductive organs, and
also from neoplasmata.”
After an artificial menopause, induced by the operative removal
of the ovaries, similar manifestations occur to those witnessed during
the natural menopause. Similar disturbances and troubles occur
in both cases, but in the artificial menopause they are commonly
more severe than in the natural; they last also for a longer time,
varying usually from three to six years; moreover, in the artificial
menopause, as in the natural, the disturbance of health is more
severe and lasts longer in proportion to the youth of the individual.
Further, in the artificial menopause also, the intensity and the duration
of the climacteric manifestations are influenced by the constitutional
state and by the condition of the genital organs at the
time when the operation is performed. We note, moreover, that,
just as in the physiological menopause, the attendant troubles are
most violent in the initial period, and then gradually subside, so
also after the induction of an artificial menopause by the removal of
the ovaries, the resultant disturbances rapidly increase in severity,
to attain their maximum in from three to six months, and then, after
lasting for a year or so, they gradually become less severe, until they
are ultimately extinguished.
The extensive process of transformation which goes on in a
woman’s system during this period of the sexual life, from the very
581first diminution in ovarian activity to the complete extinction of the
reproductive functions, manifests itself throughout the organism by
means of a series of changes which can for the most part be referred
either to states of blood-stasis and their consequences—congestion
of various organs, haemorrhages, and disorders of secretion—or
else to perversions of nervous function.
The most manifold symptoms of disordered circulation may occur:
hyperaemic states of the central nervous system, flushings of
the face, the so-called fugitive heats (Ger. fliegende Hitze), a tendency
to epistaxis, to haemorrhoidal flux, and to profuse perspiration.
The changes which take place in the reproductive organs at
the time of the menopause give rise to venous engorgement and to
collateral congestions. Such a condition of venous hyperaemia may
occur in the gastric and the intestinal mucous membrane, giving
rise to various dyspeptic manifestations, and at times, when severe,
even to actual gastric and intestinal catarrh. Hyperaemia of the
liver may also arise. In this case, the pressure of the distended
bloodvessels on the biliary ducts may interfere with the outflow of
the bile, and thus give rise to a slight icterus. Further, the intra-abdominal
venous congestion leads to overfilling of the haemorrhoidal
veins, and hence to bleeding piles.
When the congestion is long-lasting, various further morbid
changes may arise, pulmonary hyperaemia may eventuate in bronchitis,
hyperaemia of the cerebral meninges may cause very severe
headache, there may be syncopal attacks, tinnitus aurium, choroidal
congestion, impaired vision, etc.
Congestion of a more active nature arises from an increased and
usually accelerated flow of blood through the vessels of a part in
which the resistance to the blood stream has been lowered proportionately
to its propulsive force. In this way arises that characteristic
symptom of the menopause known as ardor fugax—fugitive
heat—one link in the long chain of vasomotor manifestations
occurring at this period of life. Fugitive heats are commonly most
clearly marked in the face, head, and neck, in which region there
suddenly occurs a reddening of the skin, with diffuse and increasing
subjective sensation of heat. At the same time there is often a sense
of tension, as if the part were about to burst. Actual slight swelling
may be noticed, the eyes sparkle and are somewhat prominent,
the head feels heavy, stupid, and dizzy. Sometimes these symptoms
last for a considerable time; at other times they terminate speedily
and suddenly with a local perspiration or with an attack of epistaxis.
Not infrequently, after lasting a short time in one region, they pass
away as rapidly as they came, but are immediately succeeded by a
similar attack in some other part of the body, or by vasomotor
582phenomena of a slightly different kind. Thus, such a flushing and
heat of the face may be replaced by a sudden sense of heat in the
small of the back or in the sacral region, by pruritus of the extremities,
by palpitation of heart, or by an attack of pseud-angina.
A further consequence of active hyperaemia is the onset of those
confused states, so common in the climacteric age, of mental and
bodily disquiet, which find expression, now in states of excitement,
and now in states of depression. So we often observe change of
disposition, associated with incapacity for regular work, whilst sleep
is restless, and much disturbed by dreams; and again states of dizziness,
a sense of mental uneasiness and confusion, and even actual
delirium.
In the skin, in addition to the fugitive heats, we often have a
peculiar pricking, itching, or stabbing sensation, and various kinds
of hyperaesthesia, frequently associated with disturbances of tactile
sensation. We observe also muscular twitchings, and general weakness
of the organs of locomotion.
In association with the passive and active hyperaemias of the
menopause, we frequently see increase or some qualitative change
in the various secretions. Above all, these changes affect the
various secretions of the different reproductive organs, but we have
also increased intestinal secretion, leading to diarrhoea, increased
excretion of urinary deposits, and increased secretion by the skin.
Symptoms which are common at the menarche, and frequently recurs
at the menopause, are: headache, migraine, a state of pseudo-narcotism,
slight hysterical attacks, indications of moral insanity,
lumbo-abdominal neuralgias, neuralgia of the breasts, leucorrhoea,
and various skin eruptions.
According to Tilt, the changes occurring in the organism at the
climacteric period may be summarized under the following heads:
- 1.
- Increased elimination of carbonic acid by the lungs,
- 2.
- Increased elimination of uric acid in the urine,
- 3.
- Increased perspiration,
- 4.
- Increased mucous flux,
- 5.
- Haemorrhages from various organs.
As regards the first point, the extensive researches of Andral and
Gavaret have shown that in the female sex the quantity of carbonic
acid eliminated by the lungs diminishes when menstruation first
appears at puberty, but increases again at the climacteric age, when
menstruation ceases—whereas in the male a gradual diminution
in the elimination of carbonic acid begins already in the 36th year of
life; in old age the quantity eliminated is greatly reduced in both
sexes alike.
583
Changes in the Female Reproductive Organs at the Menopause.
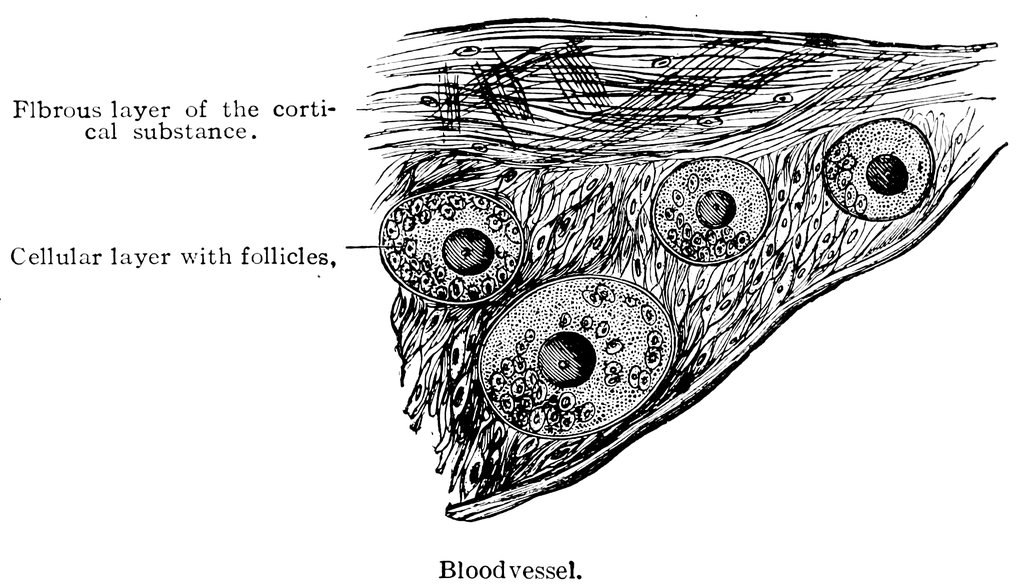
Fig. 84.—Sagittal section through the ovary of a girl aged 16.
In considering the changes that take place in the female reproductive
organs at this period of life, we must distinguish between
the proper period of the climacteric, with its various manifestations
antecedent to and associated with the irregularity and ultimate cessation
of menstruation, from the condition of old age in which
menstruation has actually and completely ceased, in which the menopause
has been fully accomplished, and in which the changes of
senescence have set in at once in the organs of the reproductive
system and in the organism as a whole.
The most important and most significant changes of this sexual
epoch are unquestionably the anatomical alterations in the ovaries.
A good many years ago I undertook an investigation whose purpose
was to follow the natural involution of the graafian follicles from
the time of the climax on into old age, and for this purpose I examined
a very large number of ovaries of women at ages varying
from 42 to 75 years (Archiv. für Gynecologie, Bd, XII., Heft 3).
Throughout these years a slow but continuously progressive
atrophy proceeds in the ovaries; they become smaller and denser,
diminishing especially in height and width; their surface becomes
extremely uneven; and in extreme old age they wither away until
no more is left in the region formerly occupied by the ovaries than
a flattened fibro-vascular thickening (Figs. 84–88). The histological
characteristic of the changes in the ovary which proceed
584gradually from the commencement of the menopause to extreme old
age, may be summed up as consisting in a continual increase and
new formation of the connective tissue stroma at the expense of the
cellular layer, accompanied by retrogressive metamorphosis of the
graafian follicles.
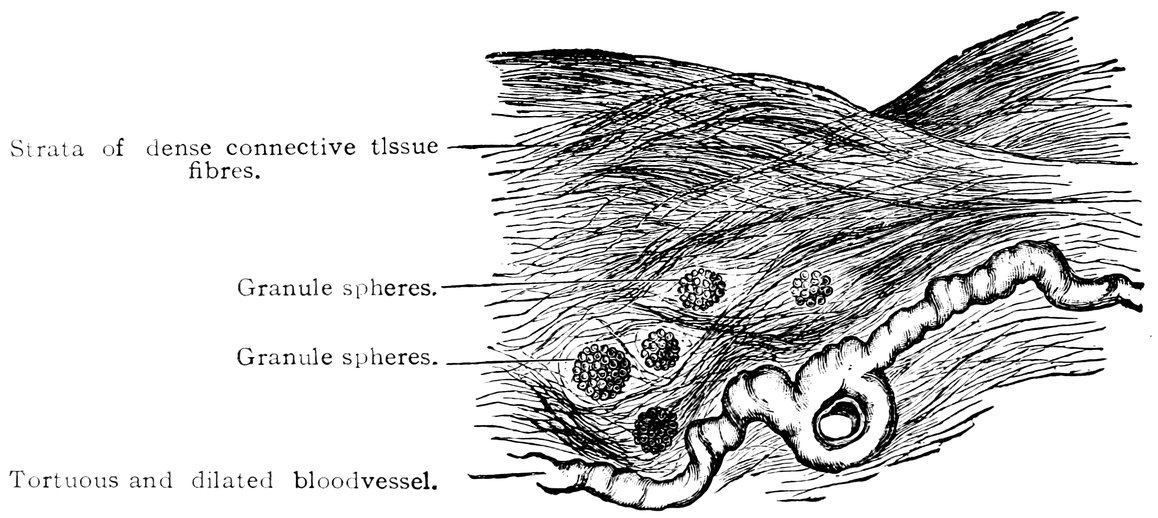
Fig. 85.—Sagittal section through the ovary of a woman aged 72 years.
The connective tissue ground substance of the ovary increases
from the periphery towards the centre, and progressively compresses
the epithelial structures of the organ. In the outermost layer of
the ovarian stroma, the so-called tunica albuginea, the strata of
short, dense connective tissue fibres increase notably in number, so
that whereas at first three layers at most could be distinguished, the
tunic ultimately comes to consist of from six to eight layers; at the
same time also the interior ovarian stroma becomes exceedingly
dense, so that numerous well-defined interlacing bundles of fibres
can be made out in its substance.
The first retrogressive metamorphosis which can be observed in
the graafian follicles is fatty degeneration, the formation of granule
spheres. Whilst the membrana propria (the theca folliculi) of the
follicle remains quite unaltered, we observe in the membrana granulosa,
in addition to the ovum, and the ordinary cells of this layer,
spherical aggregates of fat droplets, the granule spheres, which continually
increase in size, until ultimately of the cellular contents of
the follicle nothing whatever remains, and it now appears full of
granule spheres and fluid. The theca folliculi has now lost its
spherical shape, and assumes an ovid form (Fig. 89).
In a later stage of the degeneration of the graafian follicle, it
appears as a vesicular body with a relaxed wall, thrown into
numerous folds, this folded wall being formed by the theca folliculi.
585The cavity of the follicle is reduced to a mere cleft, filled with a
transparent substance, and the space between this cleft and the
inner surface of the theca folliculi is occupied by round cells and a
fibrous intercellular substance, and is traversed by a vascular network.
This second stage of the retrogression of the follicle may
therefore be designated the stage of vesicular degeneration
(Fig. 90).
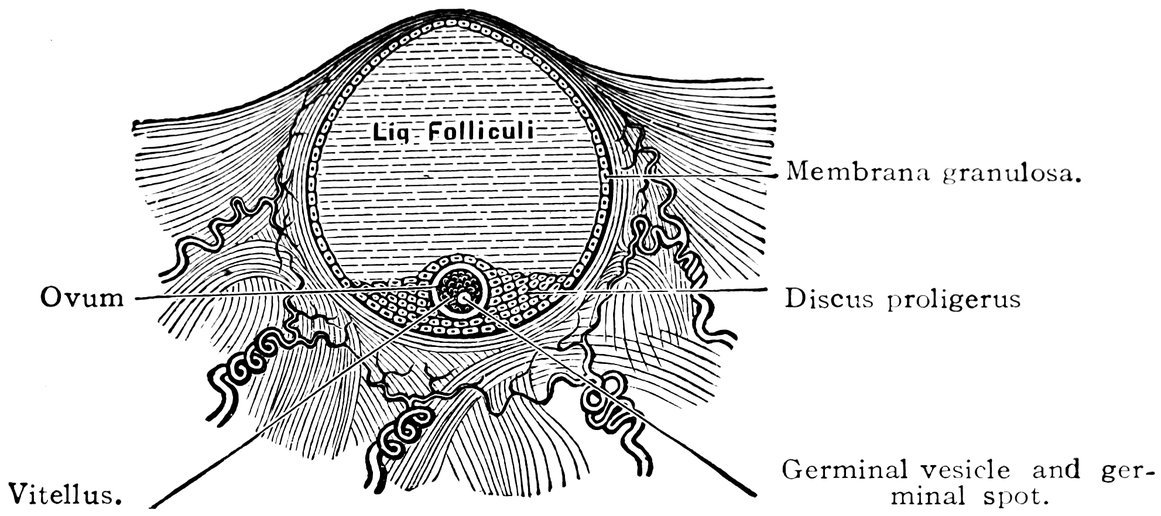
Fig. 86.—Diagrammatic representation of the Graafian Follicle.
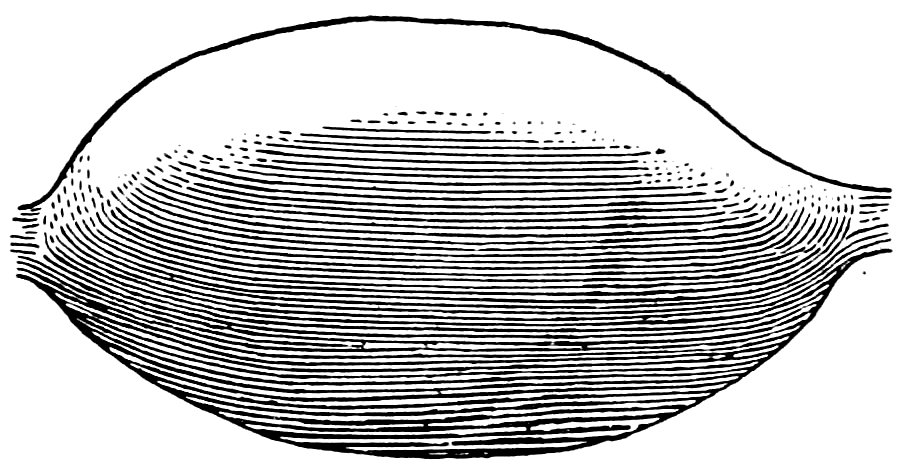
Fig. 87.—Ovary of a girl aged 19 years. (Normal size.)
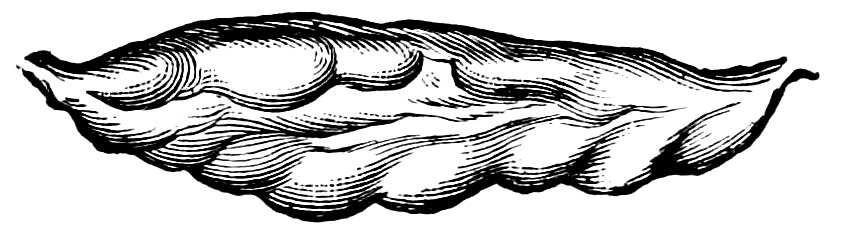
Fig. 88.—Ovary of a woman 72 years of age. (Normal size.)
In the last stage of this retrogressive metamorphosis, we find the
follicle completely transformed to a fibrous mass. It appears as an
elongated oval body, much lobulated, connected with the surrounding
stroma by thick strands of fibres; a trace of the original cavity
can still be distinguished in the form of a narrow cleft, without
distinguishable contents. The tissue of this body consists of connective
tissue fibres, with interspersed nuclei and nuclear fibres
(Fig. 91).
The three stages I have observed in the retrogression of the
follicle, of which I have given a summary account above, may, I
think, be explained in the following manner: When the woman’s
reproductive activity ceases, the graafian follicles become subject to
a retrogressive metamorphosis, a fatty degeneration setting in in the
cells of the membrana granulosa and in the ovum, until ultimately
586the whole of the granular epithelium has undergone atrophy. The
follicle now undergoes a vesicular transformation with shrinkage
of its cavity, and with the formation of a new tissue which appears
to be young connective tissue. As time goes on, this new connective
tissue is formed in increasing quantities, until finally the entire
follicle is transformed into a firm fibrous mass.

Thus we are led to infer that the gradual but extensive thickening
of the tunica albuginea (i. e., the outer, condensed layer of the
ovarian stroma), which, as we have seen, always occurs at the
climacteric period, offers a hindrance to the bursting of the follicles
as they mature, and in this we find the explanation of the irregularity
of menstruation and of the various troubles which attend the
performance of that function at the time of the menopause. It is
reasonable to assume that the resistance of this thickened tunica
albuginea is responsible for the fact that the interval between the
bursting of the successive follicles is now greater than normal, as
much as six or eight weeks—this retardation of menstruation being
one of the commonest ways in which the onset of the menopause is
first manifested. Another phenomenon connected with the onset of
the menopause also finds a plausible explanation in the anatomical
grounds just mentioned. As already pointed out, in parous women
the menopause sets in later than in nulliparae. At every pregnancy,
the ovaries share in the more abundant nutrition of all the reproductive
organs, due to the general dilatation of the intrapelvic
vessels which accompanies this process; hence the ovaries become
larger, richer in lymph, and therefore softer, the cellular elements
increase in size, and perhaps also in number, and it is readily conceivable
587that in such ovaries the cellular elements are able for a
longer time to resist the induration and the new formation of connective
tissue which occur at the climacteric.
The numerous nervous disturbances of the climacteric epoch
would appear also to depend upon the hyperplasia of the ovarian
stroma which we have observed to be the characteristic anatomical
change in the ovaries at this period of life.
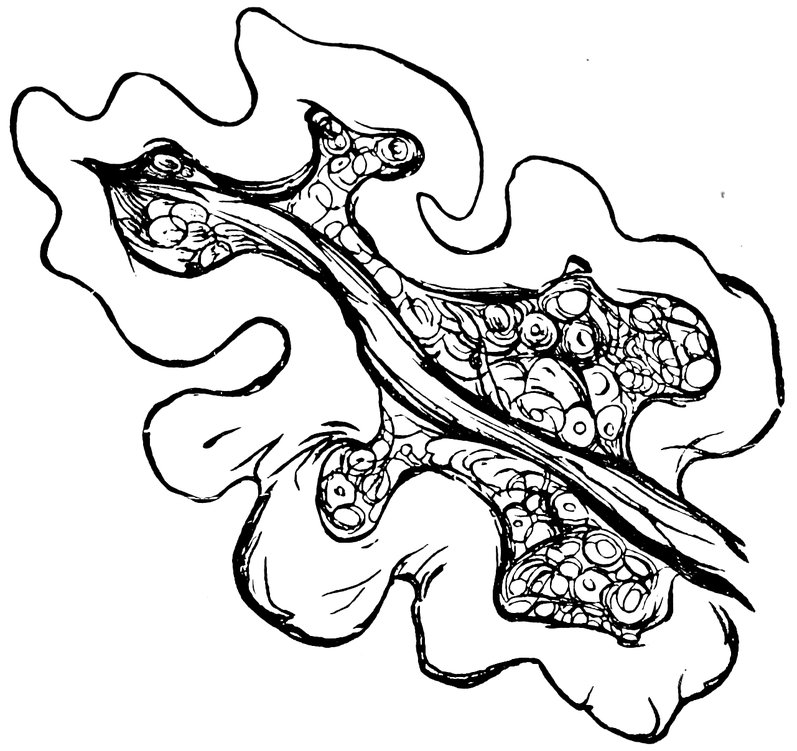
Associated with the fibrous transformation of the graafian
follicles there is, however, a failure of the so-called internal secretion
of the ovaries, a matter to which much attention has recently been
paid. Brown-Séquard has especially maintained that the ovaries
secrete a substance which enters the blood, a substance which, notwithstanding
the fact that its presence cannot be proved either by
chemical or any other means known to us, yet is of considerable
importance for the maintenance of the equilibrium of mental and
physical well-being. It is supposed that the various profound disturbances
of the general system occurring at the menopause[52] are
dependent upon the cessation of this internal secretion of the ovary—disturbances
which rise to a maximum as the atrophy of the
ovary proceeds, and which only gradually pass away after a considerable
lapse of time.
After the menopause is completely over, in the ovaries, as in
other parts of the female reproductive organs, the signs of senile
degeneration make their appearance.
588In old women, we find the ovaries either shrunken to the form of
small fibrous cords, or else degenerated to form cysts of smaller or
larger size, the stroma surrounding these cysts being extremely
hard, dense, and tough.
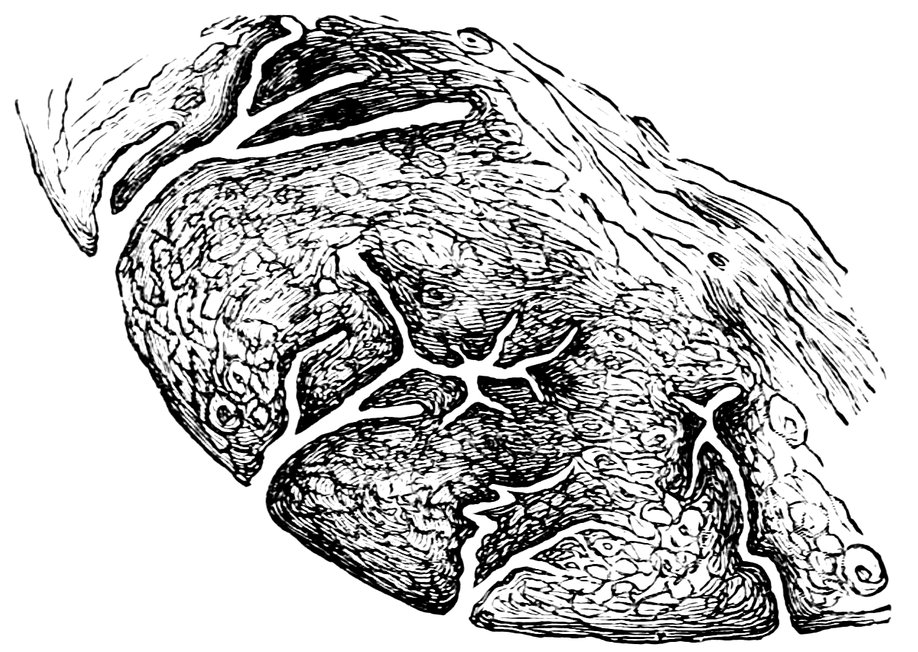
Fig. 92.—Sagittal section through the Cervix of a woman 26 years of age. Dendriform branched Glands.
589
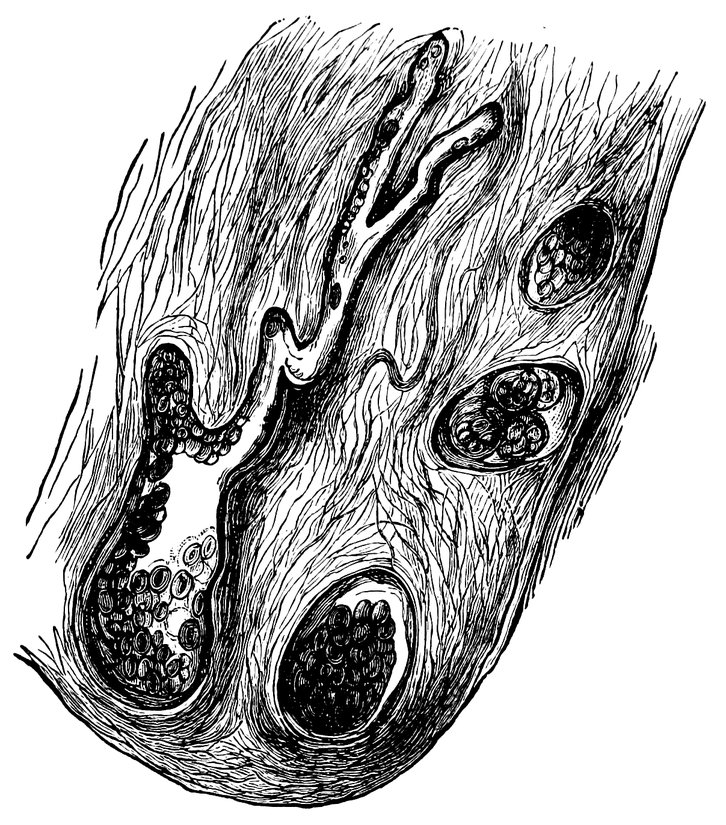
Fig. 93.—Sagittal section through the Cervix of a woman 65 years of age. Glands which have undergone Cystic Degeneration.
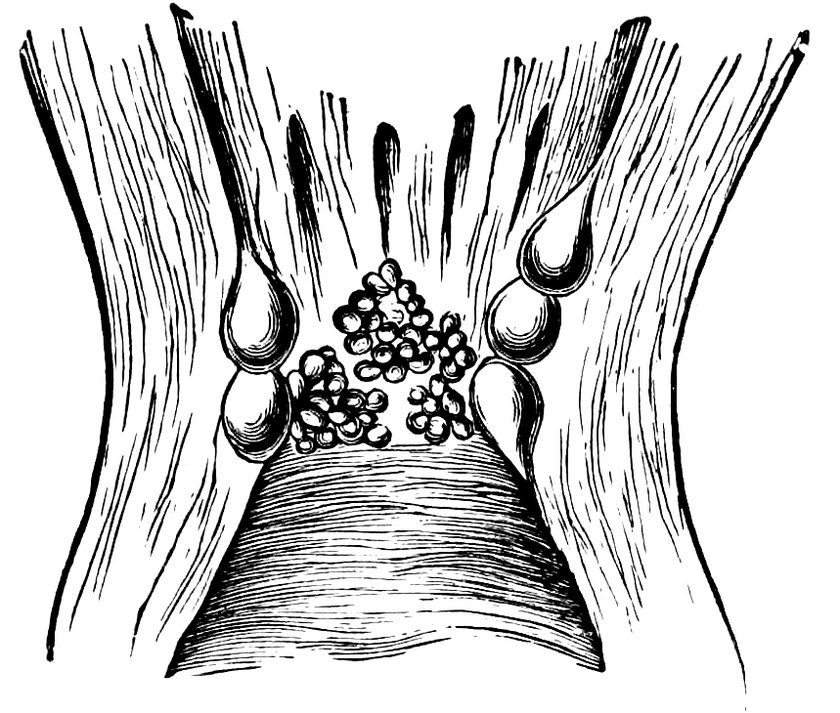
Fig. 94.—Cervix of a woman 70 years of age. The Cervical glands have undergone Cystic Degeneration.
Whereas at the commencement of the climacteric period, the
uterus commonly exhibits a slight increase in size, owing to the
condition of passive hyperaemia already described, subsequently a
gradual diminution in the size of the organ may be observed. This
atrophy begins with the portio vaginalis and proceeds upwards.
Whilst the body still appears undiminished in size, the vaginal portion
will be found already shorter, more slender, and more flaccid.
Gradually, however, the entire organ is involved in the atrophic
process. The uterus is then smaller than formerly, its walls are
thinner, its cavity reduced in size. Its vascularity and its sensibility
are alike diminished. The external os is smaller, and the
internal os is sometimes entirely obliterated. There is a tendency
at the climacteric period for the tubulo-racemose glands of the
cervical mucous membrane (Fig. 92) to undergo a cystic degeneration
(Fig. 93), and hence arise the cysts which are so commonly
met with on the portio vaginalis of women at this time of life,
cysts varying in size from that of a millet seed to that of a pea.
590In advanced life, the formation of such cysts may be regarded as
normal, and sometimes in the form of grape-like clusters they almost
completely occupy the lumen of the cervical canal. (Figs. 94, 95,
96, and 97).
Not infrequently, these cysts lead to the formation of polypi, by
enlarging until the mucous membrane projects so far that a stalk
is formed.
Examining the bodies of 47 women who died at ages varying
from 42 to 80 years, I found in 28 ovula Nabothi in the cervical
mucous membrane, for the most part at the os uteri externum, but
in some cases also extending up to the os internum, sometimes
between the plicae palmatae, sometimes isolated, sometimes grouped.
Sometimes in old women no trace of a vaginal portion remains,
and the uterus is found to be transformed to a small, thin-walled,
shrunken body, no more than one-fourth of its original size; in
such cases the saying of Graaf appears to be justified, that after
the menopause the uterus returns to the size it has in the young girl.
In the majority of such cases, the cavity of the uterus is also contracted
(concentric atrophy). It sometimes happens, however, that
in old age the os externum and the os internum are the seat of
atresia, whilst the intermediate portion of the cervical canal remains
unaffected. In this way, especially when the cervical canal and the
cavity of the body of the uterus are distended with mucus or with
fungous growths, is produced what is known as the uterus bicameratus
vetularum.

Fig. 95.—Ovula Nabothi in the Portio Vaginalis.
In many cases, when the cervical canal has been obliterated, we
find the uterine cavity distended with mucous secretion (excentric
591atrophy). The substance of the uterine wall is in old age commonly
dense and tough, but occasionally, in extreme old age, less firm
than formerly, withered and friable, and traversed by degenerated
arteries, and in this state it is predisposed to haemorrhages (apoplexia
uteri). Such intramural haemorrhages usually occur in the
fundus; the friable uterine substance has then a blackish-red appearance,
infarcted with extravasated blood; sometimes the uterine
cavity is also filled with blood. In general it may be said that
when the menopause is completely over, when uterine activity has
entirely ceased, the uterus returns to the state in which it was
before the menarche—it is physiologically dead.
The tubes become flaccid, thinner, shorter, and are at times obliterated.
In the mucous membrane of the tubes in old women we no
longer find any trace of the glands described by Hennig; the epithelial
cells have also lost their cilia.
During the climacteric period, the vagina is usually relaxed and
roomy, the mucous membrane is smooth, injected and secretes
freely; subsequently, in old age, it becomes firm, tough and dry.
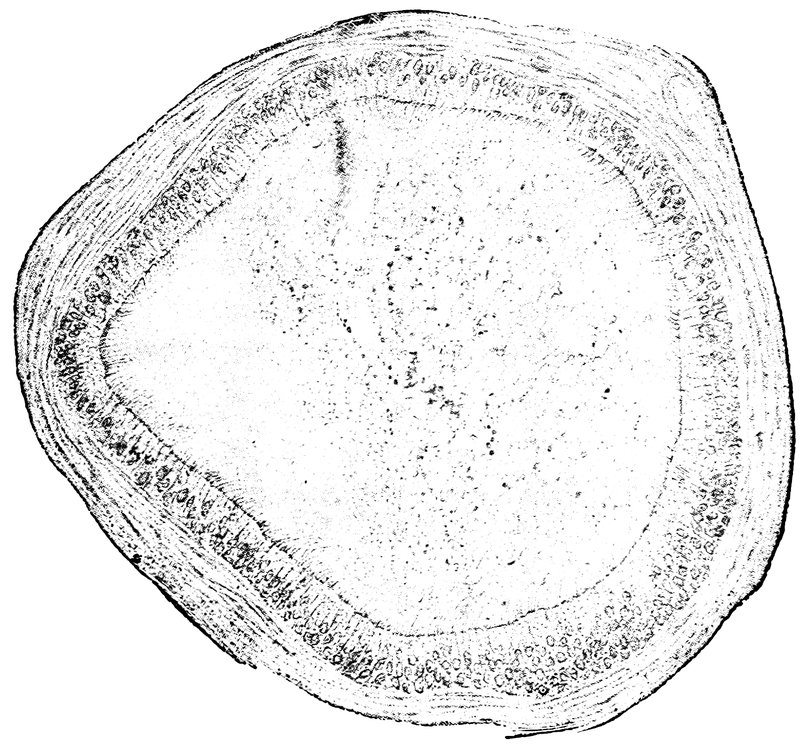
Fig. 96.—Vesicle (Ovula Nabothi) from the Uterine Mucous Membrane.
Wendeler found that the initial change of the climacteric in the
ovary is a chronic and progressive endarteritis obliterans; the
result of this process is, in addition to the obliteration of the follicles,
a continually increasing hyaline degeneration of the smallest arteries
and the arterioles, especially along the line of transition between
the cortical and the medullary substance of the organ; this degeneration
extends to the surrounding connective tissue, and thus leads to
592the formation of peculiar, vitreous, translucent foci of sclerotic connective
tissue, containing few cells or none; these are the so-called
corpora fibrosa or corpora albicantia. Only subsequently to the formation
of these bodies does the characteristic wrinkling of the surface
of the ovary occur, with general shrinkage of the organ, these
changes being due to the contraction that sets in in the numerous
scattered foci of connective tissue, which, as already mentioned, are
situated in close proximity to the cortex.
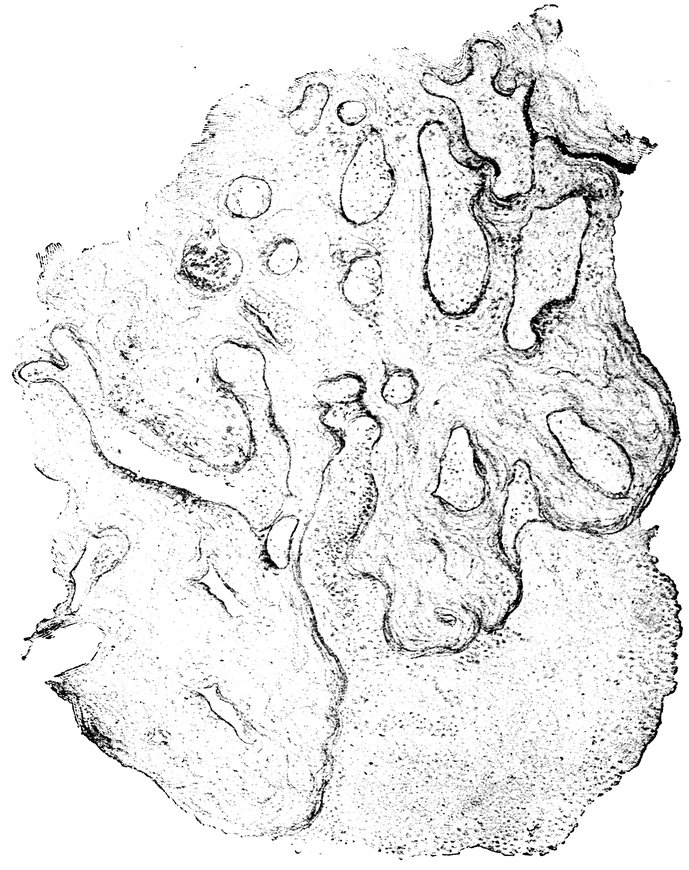
Fig. 97.—Mucous glands undergoing Cystic Degeneration.
The gradual atrophy of the uterus after the extinction of its
sexual activity leads to a diminution in all the diameters of the
organ, so that in old women it becomes flattened as in childhood, all
its curves having disappeared; the muscular substance is replaced
593by connective tissue; and the portio vaginalis dwindles and even
entirely disappears.
As regards the bacterial flora of the genital organs of elderly
women, Menge and Koenig find that the vagina for the most part
contains bacteria which do not thrive when cultivated aërobically on
alkaline agar plates. In exceptional cases, however, such bacteria
are found, and may even be sufficiently vigorous to produce pyogenic
infection. According to Strogamoff, the vagina in all circumstances
contains a great variety of micro-organisms—cocci, diplococci and
rod-forms. Rod-forms are the prevailing types found in normal
conditions in elderly women, but they are much smaller than in
women who are still in the period of reproductive activity. Organisms
liquefying gelatine were found in one instance only, a case of
vaginal prolapse. In one half of the cases examined, there was no
development of culture media inoculated from the cervix uteri,
whether on agar or gelatine.
The Time of the Menopause.
The age at which the menopause begins is one which varies owing
to manifold conditions, congenital and acquired, owing to the local
influences which have been brought to bear on the reproductive
organs during the menacme, and to the general circumstances of
life during this period. In Northern Europe it commonly begins
some time between the ages of 40 and 50 years. According to the
most trustworthy statistical data, the commonest age for the onset
of the menopause is between the ages of 45 and 50 years. Next to
these in frequency we find the menopause commencing between the
ages of 40 and 45 years. If, however, the menopause does not
begin during the fifth decennium, it is more apt to occur during
the quinquennium after 50 than during the quinquennium preceding
40 years of age; that is to say, an abnormally late menopause is
more often met with than an abnormally early menopause. In a
very small proportion of women does the menopause begin either
after the age of 55 or before the age of 35.
The Age at Which the Menopause Occurs.
My own observations show that the age at which the menopause
begins is affected by the following circumstances:
1. The race (nationality) of the woman.
2. The age at which the menarche occurred.
3. The sexual activity of the woman during the period of the
594menacme, the number of her pregnancies, the exercise or neglect of
the function of lactation.
4. The social circumstances of the woman’s life.
5. General constitutional and pathological conditions.
1. Race.
From the statistical data regarding the age at which the menopause
occurs among the women of the various nations of Northern
Europe, it appears that the latest average age for the cessation of
menstruation is met with in Lapland, namely 49.4 years; next comes
Norway, where the average age is 48.9; next Germany, where the
average age is 47; next England, 46.1; next Russia, 44; and
finally Austria, 42.2. In the four principal capital cities, the average
age is: in London, 45.5; in Paris, 43.65; in Vienna, 43, and in
Berlin, 47. Generally speaking, in southern countries the cessation
of menstruation occurs at an earlier age than in northern countries,
as the following comparison shows: northern countries: England
(Tilt), 48 to 50; France (Courty), 50; North Germany (Mayer),
50; Austria (Szukits), 42; southern counties: Persia (Chardin),
27; Java, 30; various Asiatic races, 30 to 40.
In the case of 500 women of various nationalities in whom I
was able to ascertain by personal observation the age at which
menstruation ceased, I found that the menopause occurred:
| In the quinquennium |
35 to 40 in |
48 |
women |
| In the quinquennium |
40 to 45 in |
141 |
women |
| In the quinquennium |
45 to 50 in |
177 |
women |
| In the quinquennium |
50 to 55 in |
89 |
women |
| |
|
|
|
| |
|
455 |
|
Thus we see that in about one tenth of my cases, menstruation
ceased between the ages of 35 and 40; in more than one-fourth,
between the ages of 40 and 45; in more than one-third between the
ages of 45 and 50; and in about one-sixth between the ages of 50
and 55. In 267, that is, in more than one-half of the 500, menstruation
ceased between the ages of 42 and 51. In 28 women, menstruation
ceased before the age of 35; and in 17, after the age of 55.
In a very large majority of my 500 cases the women were of
German or Austro-Hungarian nationality; next, in order of frequency,
came Poles, Russians, women of various southern countries,
Swedish women. In women of Slavonic nationality, menstruation
ceased remarkably late as compared with women of German
nationality.
Brierre de Boismont, Tilt, Courty, and various other observers,
have published statistical data regarding the age at which menstruation
ceases in women of different nationalities. Krieger, compiling
595from several authors, statistics relating to 2291 women (European)
gives the following average results: menstruation ceased
| Between the ages of 35 and 40 in |
272 |
women |
11.87 |
per cent. |
| Between the ages of 40 and 45 in |
595 |
women |
25.97 |
per cent. |
| Between the ages of 45 and 50 in |
940 |
women |
41.03 |
per cent. |
| Between the ages of 50 and 55 in |
334 |
women |
14.58 |
per cent. |
| Before 35 and after 55 in |
150 |
women |
6.54 |
per cent. |
| |
|
|
|
|
| |
2291 |
|
99.99 |
|
We append a statistical table showing the average age at which
menstruation ceases in women of different European nationalities:
|
Germany. |
Austria-Hungary. |
France (Paris). |
England (London). |
Russia. |
Denmark. |
Norway. |
Lapland. |
| Number of cases |
824 |
256 |
178 |
500 |
100 |
312 |
391 |
34 |
| Average age at the cessation of menstruation |
47.0 |
42.2 |
44.0 |
46.1 |
45.9 |
44.8 |
48.9 |
49.4 |
| Observer |
Magar |
Szukits |
Brierre de Boismont |
Tilt |
Lieven |
Hannover |
Faye and Vogt |
Vogt |
2. The Age at Which the Menarche Occurred.
Until recently, it was generally believed that the earlier the age at
which menstruation first made its appearance, the earlier also would
the menopause occur; and that, on the other hand, the later the
age at which the flow began, the later also would it cease. Virey
summarized this opinion in the saying: prius pubescentes prius
senescunt. This view of the matter is, however, true only in respect
of the influence of climate upon sexual development. In a cold
climate, a woman begins to menstruate late and ceases to menstruate
late; in a hot climate the opposite conditions prevail. But if we
make our comparison between women living in similar conditions
as regards latitude and climate, we find that Virey’s saying is far
from accurately describing the facts.
In general, and climatic influences apart, it may be said that the
earlier in any woman the age at which menstruation first occurs,
the later will be the age at which menstruation ceases.
In order to ascertain the influence of the age at the menarche
upon the disappearance of menstrual activity, I placed in comparison
first the cases of 50 women in whom menstruation had first
appeared between the ages of 12 and 16—i. e., cases of early
menarche; and secondly the cases of 50 women in whom menstruation
596had begun between the ages of 16 and 20—i. e., cases of
late menarche. The result was the following:
In the 50 women in whom the menarche had been early, the menopause
occurred
| At ages 35 to 40 in |
5 instances |
| At ages 40 to 45 in |
12 instances |
| At ages 45 to 50 in |
25 instances |
| At ages 50 to 55 in |
8 instances |
On the other hand, in the 50 women in whom the menarche had
been late, the menopause occurred
| At ages 35 to 40 in |
9 instances |
| At ages 40 to 45 in |
28 instances |
| At ages 45 to 50 in |
10 instances |
| At ages 50 to 55 in |
3 instances |
Thus whilst among the women in whom the menarche had been
late, there were thirteen only who continued to menstruate until
they were at least 45 years of age; among those in whom the menarche
had been early, the number in whom menstruation thus
continued up to the age of 45 or beyond was 33, nearly three times
as great.
On the other hand, in those cases in which the menarche occurred
at an abnormally early age, i. e., before the age of 12 years, the
menopause was also a remarkably early one. The menopause also
came on very early in women in whom the menarche had been extremely
retarded, until the age of 20 and upwards. An extremely
early and an extremely late menarche alike tend to be followed by
a premature menopause.
To this rule there are, however, exceptions, and we occasionally
meet with women whose reproductive energies are so powerful, that
the menarche occurs at an unusually early age, and the menopause
is postponed to an age considerably beyond the average. Thus,
among 100 women in the Salpetrière, Raciborski observed 29 in
whom menstruation had begun at the exceptionally early age of 12
years, and who, notwithstanding this, all experienced a very late
menopause. Three of them were still menstruating at the age of
57, 1 at 56, 2 at 52, 2 at 50, 3 at 48, 3 at 45, and 13 at an age less
than 45.
Brierre de Boismont reports the case of a woman who began to
menstruate in her 12th year; she married, had several children, and
continued to menstruate regularly until she was 60 years of age.
The results obtained by W. Guy, who examined a series of 250
cases, confirm the proposition stated above, that the earlier menstruation
begins (the extremely early cases being excluded), the later
it ceases.
According to Cohnstein, who bases his conclusions upon the observation
597of 400 cases, in women who begin to menstruate early, the
menopause occurs on an average three years later, than in women
who begin to menstruate late. Puech also states that menstruation
lasts longer in women who begin to menstruate early, than in those
who begin to menstruate late. According to Scanzoni, in women
who begin to menstruate in very early youth, the climacteric age is
commonly reached earlier, than in those in whom puberty occurs
at the normal age—commonly between the ages of 40 and 42 years.
The homology between the pathological states which, in any
particular individual, occur at the respective periods of the menarche
and the menopause, is sometimes extremely remarkable; the very
same symptoms by which the first appearance of menstruation was
preceded, recur as antecedents of the menopause. This is seen in
the case of certain eczematous conditions of the skin, of dyspeptic
manifestations, epistaxis, nervous disturbances, hysterical and epileptic
seizures, vasomotor symptoms, congestions, cardiac troubles,
albuminuria, etc. Alibert pointed out that certain skin-diseases may
appear twice only during life, once shortly before the commencement
of menstruation, and the second time shortly before the cessation
of menstrual activity. Brierre de Boismont alludes to the occurrence
of hysteria and epilepsy before both these important epochs
in a woman’s life, whilst in the intervening period the patient had
remained entirely free from such troubles. H. Marsh records the
observation that women who just before puberty have suffered from
repeated attacks of epistaxis, have suffered from the same trouble
as a predominant symptom of the climacteric period. Tilt has seen
in several cases the outbreak of numerous furuncles with subsequent
diarrhoea, and still more frequently peculiar attacks of severe
vertigo, occurring in women just before the two critical epochs in
her life, whilst in the intervening period there has been no trace of
such troubles, either in connexion with menstruation, with the puerperium,
or with lactation.
3. The Woman’s Sexual Activity.
An important influence upon the early or late onset of the menopause
is exerted by the degree to which a woman’s reproductive
functions have been exercised during the menarche. My personal
observations have shown me that in women who are in good health
and of a powerful build, whose menstrual flow has always been
regular and sufficient in quantity, whose reproductive organs have
been adequately and properly exercised, who have had a physiological
amount of sexual intercourse, have given birth to several
children, and have suckled these children, the cessation of the
menstrual flow generally occurs much later than in women in whom
the conditions of the sexual life have been the opposite of those
598just mentioned. The more regular menstruation has been, and the
more normal the deliveries, the later does the menopause ensue.
Especially striking is the influence of the number of deliveries
upon the time of occurrence of the menopause. In women who
have given birth to a number of children, menstruation as a rule continues
for several years later than in sterile women, or in those who
have had one or two children only. If a woman suckles her children,
the date of the menopause appears also to be postponed.
Deliveries late in life seem likewise to delay the onset of the menopause,
whereas abortions accelerate its occurrence. If, however,
pregnancy succeeds pregnancy at extremely short intervals, the
menopause is likely to occur early; the same result is brought about
by sexual intercourse at too early an age. The menopause occurs
latest in women who have begun to menstruate early, who have
married, have given birth to more than three children, and have
been delivered of their last child at full term when 38 to 42 years
of age.
As regards the 500 women previously mentioned, in whom I
made personal observation as to the age at which the menopause
occurred and the circumstances by which its onset was influenced,
the effect of marriage and the number of children born is shown
by the following details:
Of the 48 women in whom the menopause occurred between the
ages of 35 and 40, 16 were unmarried, 6 married and childless, 18
married with one or two children, 8 married with more than two
children.
Of the 141 women in whom the menopause occurred between the
ages of 40 and 45, 3 were unmarried, 4 married and childless, 46
married with one or two children, 88 married with more than two
children.
Of the 177 women in whom the menopause occurred between the
ages of 45 and 50, 1 was unmarried, 2 were married and childless,
32 married with one or two children, 142 married with more than
two children.
Of the 89 in whom the menopause occurred between the ages of
50 and 55, none were unmarried, none were childless, 19 were
married with one or two children, 70 were married with more
than two children.
Of the 17 women in whom the menopause occurred at an age
above 55 years, there were two only who had not had more than
two children, whilst there were 10 who had had six to eight
children.
The influence of lactation is shown by the fact that in the case of
40 women who had not suckled their children, the mean duration
599of menstrual activity was four years less than the established mean
duration of 27 years.
4. The Social Circumstances of the Woman’s Life.
The conditions in which a woman passes her life are not without
influence upon the time of onset of the menopause. In general it
may be said that among the women of the labouring classes, whose
livelihood is so often precarious, and who are apt to suffer from
habitual physical overwork, menstruation ceases at an earlier age
than among the women of the well-to-do classes and those who lead
an easier life. But though the climacteric thus occurs earlier among
the lower than among the upper classes, the difference is not a
considerable one.
According to Mayer’s calculation, the mean age at which menstruation
ceases is, in upper class women, 47.13 years, in lower class
women, 46.97 years. Small as this difference appears, amounting
on the average to no more than two months, it must not be forgotten
that among the upper classes, menstruation begins earlier
than among the lower classes, by an amount which averages 1.31
years. Thus the total duration of sexual activity is almost one and
a half years longer in the upper than in the lower classes.
5. General Constitutional and Pathological Conditions.
An important influence upon the time of occurrence of the menopause
is exerted by the individual and hereditary predisposition of
the woman, by her constitutional state, and by certain illnesses
from which she has suffered. Women who by inheritance are constitutionally
weakly and delicate, in whom the menstrual flow has
always been pale and scanty, in whom the intermenstrual intervals
have been excessive, and who have a slender habit of body, attain the
climacteric age earlier than women with vigorous bodily development
and powerful muscles, with large breasts, and in whom menstruation
has always been regular and abundant. Women with a
great tendency to obesity cease to menstruate earlier than women
of more normal proportions; blondes earlier than brunettes; women
of phlegmatic temperament earlier than women of a sanguine and
ardent temperament.
In general it may be said, that all influences which have a
weakening effect upon the feminine organism, tend also to accelerate
the onset of the menopause: such are, severe labour, great
sorrow, wearisome occupations, severe menstrual losses, rapidly
succeeding pregnancies, and abortions; also a number of pathological
general states shortly to be discussed, as well as local diseases
of the reproductive organs.
600Fritsch points out that menstruation continues to a later age in
proportion as the woman’s state of general nutrition is a good
one. He also asserts that women with a very large uterus, who
have always had an abundant menstrual flow, those with retroflexion,
with hypertrophy of the portio vaginalis, or chronic endocervicitis
and endometritis, and those with small myomata which have
given rise to no marked symptoms, often continue to menstruate
far beyond the usual age.
The mean duration of the climacteric phenomena, from the commencement
of these until the final cessation of menstruation, is
about two years. This mean is made up of extremely wide individual
variations; in a small proportion of the cases the climacteric
manifestations may last no more than a month or two, whilst at the
other end of the scale we meet with cases in which the duration
extends to 4, 6, 8, and even 18 years.
In considerably more than half of all the cases, however, the
duration of the climacteric manifestations varies between six months
and three years. Thus, in Tilt’s series of cases, the duration of
the “change of life” was
| 6 months in |
12.07 of all cases |
| 1 year in |
22.64 of all cases |
| 2 years in |
18.62 of all cases |
| 3 years in |
9.43 of all cases |
6. Premature, Delayed and Sudden Onset of the Menopause.
In exceptional cases, the menopause, instead of taking place between
the fortieth and the fiftieth year of life, occurs at an abnormally
early or an abnormally late age.
Premature cessation of menstrual activity, in the third or the
fourth decennium of life—very rarely indeed before the third
decade—depends in part upon disturbances of metabolism and of
haematopoiesis, and in part upon diseases of the female reproductive
organs; in some cases, however, it may be due to some hereditary
constitutional peculiarity; or it may occur suddenly, in consequence
of some violent shock to the nervous system.
Among the disorders of metabolism which may lead to a premature
menopause, excessive adiposity, lipomatosis universalis, occupies
the first place. Next in order of importance come a chloro-anæmic
condition of the blood, pernicious anæmia, splenic leukaemia,
certain of the acute infectious disorders—typhoid, cholera,
scarlatina, acute articular rheumatism,—further pulmonary
tuberculosis, diabetes mellitus, Graves’ disease, Addison’s disease,
and myxoedema. These various conditions may give rise, in part
by infective processes, and in part in consequence of the general
cachectic condition, to atrophy of the ovaries with destruction of the
601graafian follicles, and to atrophic processes in the uterus, and these
changes lead to the premature cessation of menstrual activity.
Excessive obesity has a restrictive influence upon ovarian activity,
manifested in part, as already mentioned, by the occurrence of
sterility, but in part also, in very obese women, by the onset of a
premature menopause. Among 215 cases of extreme obesity in
women, I found 49 in which the menopause occurred at a remarkably
early age. In these cases the menopause occurred at the
following age:
| In |
1 woman at the age of |
17 years |
| In |
14 women at the age of |
20 to 25 years |
| In |
11 women at the age of |
25 to 30 years |
| In |
9 women at the age of |
30 to 35 years |
| In |
14 women at the age of |
35 to 40 years |
In none of these cases did the local examination of the reproductive
organs disclose the existence of any noteworthy disease.
Of the diseases of the genital organs which are competent to give
rise to a premature cessation of menstrual activity, the most important
are the puerperal infective processes and other inflammatory
states of the reproductive organs, with their results—chronic metritis,
perimetritic and parametritic exudations, chronic oophoritis,
atrophy of the uterus and the ovaries.
After infective puerperal processes, it sometimes happens that
there is far-reaching destruction of the uterine musculature, degeneration
of the uterine mucosa, permanent and irreparable atrophy
of the uterus, and suppuration and atrophy of the ovaries—conditions
which result in an extinction of menstrual activity. A similar
result may ensue upon the persistent and long-continued
pressure upon the uterus and the ovaries of a large intrapelvic
exudation; such exudation being commonly post-puerperal, but occasionally
arising in the absence of pregnancy. Further, according
to Freund, chronic atrophic parametritis may give rise to an incurable
atrophy of the uterus, by interference with the circulation of
the blood through the broad ligaments, and consequent impairment
of the nutrition of the uterus. Gonorrhoeal inflammation may also
lead to the termination of menstrual activity, when it gives rise to
intramural inflammatory deposits in the uterus, and to chronic inflammatory
processes in the ovaries. Tumours of the uterus and the
uterine annexa may likewise induce a premature menopause.
We also meet with cases in which after a pregnancy, to all appearance
normal in its course and termination, a premature menopause
results. To this category belong the cases, according to
Kleinwächter of no extreme rarity, in which perfectly healthy
women are attacked by profuse uterine haemorrhage during the
602course of a normal, full-term labour, or during miscarriage; subsequently,
though the lying-in period is passed without further misadventure
or abnormality, and in the absence of lactation, the patient
becomes permanently amenorrhoeic. The normal involution of the
uterus passes on into hyperinvolution, and ultimately complete
atrophy of uterus and ovaries results. In some cases, moreover, such
hyperinvolution with consecutive atrophy follows normal labour or
abortion without the occurrence of any excessive haemorrhage.
Much more frequently do we find that rapidly successive pregnancies,
with long-continued exercise of the lacteal function, in
badly nourished, anæmic women, give rise to a premature menopause,
due to permanent atrophy of the uterus and ovaries, which
are in such cases so poorly supplied with blood. This “lactationatrophy”
is described by Frommel and Thorn as a concentric
atrophy first of all affecting the corpus uteri, and to this, if the
disease advances, there succeeds a general atrophy of the muscular,
connective, and fatty tissues of the parametrium, the vagina, the
pelvic floor, and ultimately of the ovaries, leading, when permanent,
to a premature menopause.
Trauma of the genital organs may also lead to uterine atrophy and
to premature menopause.
By many authors it is believed that too-early marriage, sexual
excesses, and prostitution, may be the cause of cessatio praecox. In
some cases, there is unquestionably a hereditary predisposition to
a premature climacteric, since the mothers of the women in whom
it occurs have themselves been similarly affected. In the remarkable
case which came under my own observation, of a woman from
Smyrna, there was hereditary predisposition. This woman began
to menstruate when 12 years of age; menstruation was always
scanty; she married when 15 years of age; and she ceased to menstruate
for ever at the age of 19. In other cases we find there is
a family tendency for menstruation to be delayed in its first appearance
to a comparatively advanced age, and to cease at the usual time.
In cases of cessatio mensium praecox (unless the failure of menstruation
has been quite a sudden one), and after the premature
menopause is fully established, we find in the uterus and the ovaries
anatomical changes similar to those met with after the natural
climacteric—diminution in the size of the uterus with thinning of
its walls, density and firmness of the tissues of the organ, smallness
and a soft consistency of the ovaries; sometimes, also, the mammae
are atrophic.
In cases of premature menopause, the troubles attending the
change are commonly more severe and more enduring than those
that occur at the natural menopause. Especially is this the case
when the premature menopause is quite a sudden occurrence, but this
603phenomenon is rare. Most commonly the premature menopause is
gradual in onset; the flow becomes more scanty month by month,
until at last it fails altogether to appear. Irregularity in the menstrual
rhythm is not often seen in such cases. Early senescence is
exceptional in these women in whom a premature menopause occurs.
Emaciation, greyness of the hair, wrinkling of the skin, the growth
of hairs on the face, etc., are not usually associated with the atrophy
of the reproductive organs; the physiognomy and figure of
women with cessatio praecox being usually similar to those seen in
women of corresponding age in whom menstruation still continues.
Tilt enquired regarding the cause of cessatio praecox in 27 instances,
with the following results:
-
- In 3 instances, parturition and lactation. In 1 instance, abortion. In 2 instances, a
fall on the sacrum during menstruation. In 2 instances, suppression of menstruation from
chill. In 1 instance, haemorrhage from the arm during menstruation. In 1 instance,
celebration of nuptials during menstruation. In 2 instances, severe medicinal purgation.
In 2 instances, cholera. In 2 instances, rheumatic fever. In 2 instances, febrile
bronchitis. In 9 instances, intermittent fever.
In 1 case Tilt saw cessation of menstruation occur at the age of
29, in consequence of metritis. Atlee, in 15 cases of ovarian tumour,
saw the menopause occur at ages of 30, 39, 40 and 42. Puech saw
a premature menopause at the age of 30 in 3 cases, in each a sequel
of cholera. Blondel reports a case of cessatio praecox after prolonged
galactorrhoea, although the woman had not suckled her
infant; Gottschalk and Rokitansky, cases following injury to the
cervix uteri; Kiwisch, Simpson, and Kleinwächter, cases following
full-time, normal deliveries, in which, however, severe losses of
blood had taken place.
Courty and Brierre de Boismont report cases in which the menopause
occurred as early as the age of 21; Mayer, 2 cases at the age
of 22; Krieger, 1 case at 23; Brierre de Boismont, 1 case at 24;
Mayer, 2 cases at 25; Brierre de Boismont, 1 case at 26, and 1 case
at 27; Guy and Tilt, each 1 case at the age of 27; Brierre de Boismont,
Courty, and Guy, each 1 case at the age of 28; Brierre de
Boismont, Courty, and Mayer, each 1 case at the age of 29; Guy and
Tilt, each 1 case at the age of 30; and Mayer, 5 cases at the age
of 30.
An unusually late climacteric, the continuance of menstruation
beyond the age of 50 years, is not an extremely rare occurrence, but
604is less often seen than cessatio praecox. There is, however, in these
cases a difficulty which must not be underestimated, namely, to distinguish
between a genuine menstrual bleeding and the other uterine
haemorrhages which are common precisely at this age of life, due
either to textural changes in the uterus, or to neoplasmata—more
especially because in these non-menstrual haemorrhages also a certain
periodicity may often be detected. When on careful examination
no abnormality can be discovered in the reproductive organs,
when the bleeding in question recurs at the intervals and in association
with the general symptoms to which the woman thus affected has
been accustomed during her previous menstruations, and when the
amount of blood discharged is not abnormal, it is permissible to
conclude that we have to do with a persistence of true menstruation,
even though the woman has some time since completed the fifth
decennium of her life. In some women, in fact, the reproductive
system is so energetic, that ovulation continues to an age far beyond
the average, and such women are to be regarded as sexually
long-lived.
Although the instances of protracted menstruation contained in
the older literature of the subject are open to suspicion, owing to
the fact that at that time it was not possible to distinguish with
certainty between menstrual and pathological uterine haemorrhage,
quite recently numerous incontestable cases of enduring sexual
vitality have been put on record.
I have myself seen no less than 106 cases in which the menopause
did not occur until after the age of 50 years; among these there
were 4 in which the age at the menopause was 56; 5 in which it
was 57; 2 in which it was 58; 1 in which it was 59; and 1 in which
it was 60. Tilt records 128 cases of menopause occurring after 50;
among these there were 4 in which the woman was 56 when menstruation
ceased; 2 who were 57; 4 who were 58; 1 who was 59; 1
who was 60; and 2 who were 61. Courty reports a case in which
menstruation persisted after the age of 65; Mayer, 3 cases of menopause
at 64; Beigel, 2 cases, 1 in which menstruation continued to
the age of 65, the other, to the age of 72. Kleinwächter observed
33 cases in which menstruation continued to an age varying from
50 to 57 years. Emmet, in the year 1886, published the case of a
woman who was then 70 years old, and who at this advanced age
continued to menstruate regularly.
That not every case in which after the age of 50 years there
is recurrent, more or less periodic, haemorrhage from the genital
organs, is to be regarded as an instance of delayed menopause, we
are taught by the records of post mortem examination in several
cases of the kind. Scanzoni reports the case of a woman who at
the age of 60 was affected with a fairly regular periodic discharge
605of blood from the vagina. During one of these haemorrhages, she
died of pneumonia, and the autopsy showed that the ovaries were
completely atrophied and transformed into dense scar tissue, and
contained no trace of corpus luteum or of fresh extravasation of
blood, whilst in the upper part of the cervical canal there were two
mucous polypi each of about the size of a bean. In another case,
that of a woman 64 years of age, periodic losses of blood, at intervals
of from three to four weeks, continued to the time of her death.
This woman suffered from mitral valvular insufficiency, and it was
clear that the haemorrhages had been due to the venous engorgement
consequent upon imperfect compensation. The ovaries were
completely atrophied, and showed no trace of any recent maturation
of ova; the uterus was enlarged, the mucous membrane hyperaemic,
and the cavity contained a recent clot.
Not infrequently, the haemorrhages attributed to the persistence
of menstruation are really due to senile arteriosclerosis—to rigidity
and brittleness of the uterine arteries; in other cases they arise from
varicosity of the veins of the cervical canal. A common cause of
such bleedings from the genital passage in comparatively advanced
life, is to be found in the growth of uterine myomata.
To myoma uteri we must attribute a part, though by no means all,
of the cases in which menstruation seems to recur some years after
the menopause has, to all appearance, been fully established. In
most of these cases, indeed, we have to do with pathological haemorrhages,
the cause of which is, however, but too often obscure. Still,
cases certainly occur in which, two or three years or even longer
after the menopause, some unknown stimulus leads to the regular
recurrence of menstruation. The possibility of such an occurrence
is, in my opinion, fully proved by post mortem examinations of the
bodies of elderly women in whom the menopause has been fully established
and yet the ovaries are found to contain follicles of various
degrees of ripeness, and also fresh corpora lutea—signs that ovulation
may persist for a considerable time after the complete cessation
of menstruation. Another proof of the last fact is the well
known experience that women who have some time ago ceased to
menstruate, may nevertheless become pregnant. Waldeyer, indeed,
asserts that when four years have elapsed since the menopause,
follicles are never to be found in the ovaries, but this negative experience
is not decisive, especially as regards the cases in which
regular menstruation is resumed some time after the occurrence of
a premature menopause.
I have myself seen several cases in which the menopause occurred
at 35, 38, 39, and 42 years, respectively; 3, 4, or 5 years later, as a
result of hydropathic treatment, regular menstruation recurred. In
606one case, a woman who had ceased to menstruate ten years before,
gave birth to a child at the age of 45.
Numerous indisputable cases of this kind are reported in the recent
literature of the subject. Krieger had under his personal observation
a woman of a robust habit of body, in whom menstruation
ceased at the age of 48 years, her eighth child having been born
fifteen years before. Two years later irregular menstruation recurred,
and on the cessation of these haemorrhages, it appeared that
the woman was once more gravid; she was delivered at full term
of a girl. Mayer observed the following case: A strong working-class
woman 33 years of age had begun to menstruate regularly
when 13 years old; between the ages of 17 and 28 she gave birth to
five children, and in addition had one miscarriage when 19 years
old. Widowed at the age of 29, she fell ill, and on examination the
uterus was found to be small and relaxed, whilst the vaginal portion
of the cervix was reduced to a mere rudiment. Since she had been
22 years of age she had had persistent leucorrhoea, but no trace of
menstrual haemorrhage; yet since that age she had had three children.
Renaudin delivered a woman 61 years of age, who had
ceased to menstruate 12 years earlier. Meissner reports a case in
which a woman first began to menstruate at the age of 20, had her
first child when 47 years old, and gave birth to the last of her eight
children when 60 years of age.
The sudden and permanent cessation of menstruation, whether at
the normal climacteric age, or earlier in life, is always a pathological
occurrence. As compared with the normal, gradual disappearance
of menstruation, associated with the usual climacteric symptoms,
such a sudden extinction of menstrual activity is, moreover,
quite rare. When it does occur, the cause is to be found in one of
various pathological general states, such as one of the acute infectious
disorders, or some other exhausting disease, or sometimes in
some local disease of the reproductive organs; occasionally, however,
it may occur in perfect health, in consequence of some powerful
physical or mental stimulus, such as a severe blow or intense
fright.
This sudden menopause has been observed after severe labour or
abortion with profuse haemorrhage, or after cholera or typhoid; we
must assume that in such cases the anæmia of the genital organs
has disturbed the function of ovulation; whilst in cases due to mental
shock, the interference with ovulation must be through the intermediation
of the nervous system. Frequently, of course, in these
cases, the sudden menopause is also a premature one.
Tilt reports a case in which a sudden menopause ensued upon
phlebotomy during menstruation; several cases also in which women
at ages varying from 30 to 34, or 39 years, ceased to menstruate
607suddenly and permanently in consequence of grief at the unexpected
death of the husband; and another case of sudden menopause due
to a fall down stairs. Courty reports three cases of sudden menopause
at the age of 30, consequent upon an attack of cholera.
Dusourd has seen three cases in which, in women aged 40 to 43
years, severe haemorrhoidal bleeding was followed by sudden and
permanent cessation of menstruation. Mayer reports the case of a
delicate middle-class woman 34 years of age, who had begun to
menstruate at the age of 14, had married at the age of 20, and at
the age of 21 after a normal delivery, ceased for ever to menstruate;
and another case of a working-class woman 34 years of age who
first menstruated at the age of 13 years, married at the age of 20,
had two children in rapid succession, and finally ceased to menstruate,
in consequence of a fright, at the age of 30 years. Krieger
reports the case of a very nervous woman who first menstruated at
the age of thirteen, and in whom at the age of 23 a sudden menopause
ensued upon a nervous attack; in another case reported by
the same observer, a sudden menopause occurred in a delicate
woman 41 years of age owing to her husband’s death—this woman
had previously experienced six months amenorrhœa in consequence
of sorrow at the death of one of her children. The following remarkable
case is reported by Brierre de Boismont: A sempstress
began to menstruate at the age of 13 years; she married very soon
after this, and gave birth to four children, the last when 21 years
of age. In the course of the following year there was a fire in the
house, and owing to this fright a sudden menopause occurred. Similar
cases have been reported quite recently by Bossi and Walter.
The harmful influence which the occurrence of a sudden menopause
exercises upon the general condition of the woman who
experiences it, is manifested chiefly by violent circulatory disturbances,
hyperaemia and congestion of the brain, lungs, and abdominal
organs, and by states of excitement and depression of the nervous
system. Of the vicarious haemorrhages which are apt to ensue upon
such a sudden menopause, we have already spoken.
Generally speaking, women in middle life, in whom the whole
organism is accustomed to the onset and decline of the menstrual
hyperaemia, endure the functional disturbances induced by a sudden
and complete cessation of menstruation much more easily than
women who have already entered upon the climacteric age, or have
nearly attained that age. The climacteric age is one in which women
are already predisposed to circulatory disturbances in the pelvic
organs, and it will readily be understood that in them the sudden
interruption of the menstrual haemorrhages will have more serious
consequences than in women in the prime of their sexual life, and
therefore endowed with a greater power of resisting disturbances
of the normal functions.
608
Pathology of the Menopause.
Diseases of the Genital Organs.
Among the commonest of the symptoms of the sexual epoch of
the menopause is menorrhagia. It occurs especially in plethoric
women, in those who during the prime of their sexual life have
been accustomed to menstruate abundantly, and in those who have
given birth to many children or had many miscarriages; but it is
seen also in weakly and delicate individuals, in whom the tissues of
the genital organs have become extremely flaccid and loose in
texture. A luxurious mode of life, more especially a free consumption
of alcoholic beverages, and also frequent sexual intercourse
during the climacteric period, appear to favour the occurrence of
menorrhagia at this epoch.
Not infrequently, menorrhagia is the first sign of the commencement
of the climacteric, menstruation having been hitherto regular,
and not excessive in amount. Generally, when this climacteric
menorrhagia begins, the intervals also become shorter, the menstrual
period being reduced to three or even two weeks. At times, however,
the more profuse menstruation recurs at longer intervals, six
weeks, two months, or even longer. In any case, the occurrence at
the climacteric age of a severe or atypical haemorrhage, renders it
the imperative duty of the physician to undertake a local examination
of the genital organs; for it is necessary to ascertain without
delay whether such a haemorrhage is a true climacteric phenomenon,
or whether it is due to some actual disease of the reproductive
organs—a neoplasm, or the like.
If the haemorrhage is due solely to the change of life, the vaginal
portion of the cervix will usually be found soft and flaccid, bleeding
readily on slight injury, and sometimes eroded; there is generally
associated leucorrhoea. This relaxation and loss of firmness in the
uterine tissues at the time of the menopause is the cause of the predisposition
to excessive haemorrhage. An additional cause exists
in the circulatory disturbances in the pelvic organs. We presume
that women affected with menorrhagia at this time of life suffer
from some persistent disturbance in the region of the inferior vena
cava, whereby the outflow of blood from the veins of the pelvis is
hindered, and a chronic condition of stasis in the uterus is conditioned.
Hence arises distension of the vessels of the uterine mucous
membrane, and this rhexis is relieved by the excessive haemorrhages.
In these considerations lies the explanation of the fact that women
who have had many children or many miscarriages, are especially
prone to suffer from climacteric menorrhagia; and also women who
for any reason are predisposed to intra-abdominal stasis.
609Another cause of climacteric menorrhagia is to be found in the
frequent occurrence at this epoch of advanced arteriosclerotic
changes in the uterine blood vessels, the disease being in some cases
limited to the uterine arteries, and in others part of a general
arterial degeneration. The blood may be derived from ruptured
sclerotic capillaries of the mucous membrane; but in other cases it
exudes in consequence of passive hyperaemia, without actual rupture
of the bloodvessels. To such haemorrhages from atheromatous
vessels we must refer many of the attacks of uterine haemorrhage
that occur in elderly women, such as were formerly, before
their true nature was understood, commonly regarded as instances
of a very late return of menstruation. By careful examination the
exact source of the blood can often be detected in such cases.
According to Theilhaber, one cause of the haemorrhages occurring
at the climacteric is to be found in the atrophy of the uterine muscle
which takes place at this period of life. Except during pregnancy
and the puerperium, the uterus is usually in a state of moderate contraction;
during the height of the menstrual flux, however, the
uterus is relaxed. Then, as contraction of the muscle sets in, the
menstrual hyperaemia and consequent haemorrhage are gradually
brought to an end. When this contraction is insufficient, the
hyperaemia and swelling of the uterus are more enduring. In
association with the atrophy of the uterine muscle at the climacteric,
there usually occurs a notable diminution in the size of the uterine
vessels, so that, notwithstanding the diminished strength of the
muscular contractions, any excessive loss of blood is prevented.
But if this diminution in the calibre of the vessels fails to take place,
the atony of the uterine muscle leads to hyperaemia, to haemorrhage,
and often, in addition, to oedema of the organ, with elongation and
thickening of its walls—hyperplasia uteri preclimacterica.
Among diseases of the uterus which during the climacteric may
give rise to severe haemorrhage, and may lead to the mistaken
opinion that menstruation still continues, we must in the first place
mention carcinomatous disease of the cervix and of the body of
the uterus; next in importance come myoma and fibrous polypi; less
frequent causes of such haemorrhages are fungous endometritis,
erosions, mucous polypi, prolapse of the uterus, and ovarian cystoma.
The climacteric age gives rise to a predisposition, not only to
bleeding, but also to other pathological changes in the reproductive
organs. We can by no means endorse the opinion of Currier—one
long ago expressed also by Brierre de Boismont—that women during
the sexual epoch of the menopause are less disposed to diseases
of all kinds, and among them to diseases of the genital organs,
than younger women, for the reason that their tissues are endowed
with less vitality, and are, therefore, more resistent to all the causes
610of disease. On the contrary, the number of pathological disorders
liable to affect the reproductive organs precisely at this period of
life, is strikingly large. Among my 500 cases of women at the
climacteric age, there were 440 who complained of such symptoms,
the diseases from which they suffered being, in order of frequency:
| Profuse haemorrhages in |
286 cases |
| Chronic metritis in |
79 cases |
| Leucorrhoea in |
327 cases |
| Displacements of the uterus |
117 cases |
| viz., prolapsus in |
65 cases |
| anteflexion and retroflexion in |
52 cases |
| Genital pruritus in |
46 cases |
| Vaginismus in |
12 cases |
| Carcinoma uteri in |
3 cases |
| Myoma uteri in |
5 cases |
| Tumor mammae in |
8 cases |
I need hardly point out that in many individuals more than one
of these diseases were present at the same time.
The most obvious feature of these statistics is the extraordinary
frequency of uterine haemorrhage and of leucorrhoea in climacteric
women. The former condition was present in more than half my
cases; the latter actually in three-fourths.
The same two pathological states were also those most frequently
recorded in Tilt’s statistics. This author, in 446 women at the
climacteric, found the following diseases of the reproductive apparatus:
| Haemorrhages in |
138 cases |
| Leucorrhoea recurring at irregular intervals in |
146 cases |
| Leucorrhoea recurring monthly in |
12 cases |
| Remittent menstruation in |
33 cases |
| Vaginitis in |
4 cases |
| Follicular inflammation of the vulva in |
10 cases |
| Inflammation of the labia in |
4 cases |
| Ulceration of the cervix uteri in |
9 cases |
| Prolapsus uteri in |
5 cases |
| Uterine polypi in |
4 cases |
| Fibrous tumours of the uterus in |
4 cases |
| Cancer of the uterus in |
4 cases |
| Chronic ovarian tumours in |
3 cases |
| Irritation and swelling of the breasts in |
14 cases |
| Lacteal or gelatinous secretion in breasts in |
2 cases |
| Hard, non-malignant tumour of the breast in |
2 cases |
| Chancre of the breast in |
1 case |
| Frequent sedimentation in the urine in |
49 cases |
| Difficult and painful micturition in |
9 cases |
| Incontinence of urine in |
4 cases |
| Haematuria in |
2 cases |
| Perineal abscess in |
2 cases |
Chronic metritis and endometritis come under observation with
considerable frequency during the climacteric age, but as a rule
611these diseases have originated during the period of sexual maturity,
and in exceptional instances only does the cessation of the menses
appear to be the etiological starting point of these disorders. In
fact, this occurs only when the menopause is premature, or when
it is quite sudden in onset, whether this be due to noxious influences
or to constitutional disorder. For the menstrual process quite normally
gives rise to a certain congestion of the genital organs; and
should menstruation be suddenly suppressed, the blood-stasis in the
uterus becomes so extreme that morbid tissue changes are very
likely to ensue. And when chronic metritis has occurred before,
the congestion and stasis in the uterus at the climacteric will usually
suffice to light up the inflammatory process afresh. This is the explanation
of the fact that symptoms of slight metritis make their
appearance at the very beginning of the climax, manifested by thickening
of the corpus uteri and of the portio vaginalis of the cervix,
by swelling and softening of the mucous membrane, and by abundant
secretion. In those who, either after full-term delivery or
after abortion, have suffered formerly from chronic metritis or endometritis,
but who have been quite free from any symptoms of
these troubles for many years prior to the climacteric, it often happens
that the change of life is ushered in by symptoms of congestion
of the uterus with associated leucorrhoea. With the completion
of the menopause, however, the resulting involution of the uterus
exerts a favourable influence upon all such chronic inflammatory
processes in the genital organs; as the atrophy progresses, the periodic
attacks of congestion cease to recur. Thus it happens that
women who for years have suffered from haemorrhages, from inflammatory
disorders of the genital organs, and from various other
troubles of a similar nature, will, once the menopause is fully over,
feel quite well up to an advanced period of life—they seem as it
were to begin life afresh.
According to Bennet, the characteristic signs of climacteric metritis
are that the inflammatory symptoms are less pronounced, that
the pains are less severe, that elongation of the cervix is less often
seen, and that fungous changes are less marked, than is the case
in the chronic metritis of younger women. On the contrary, the
cervix appears smaller, often somewhat lobulated, it is harder,
granulations are numerous, ulceration is rare, the enlargement of
the uterine cavity is but slight. Bennet’s views are, however, opposed
by Scanzoni, who maintains that there is no notable difference between
the chronic metritis of younger women and the disease as it
occurs in women at the climacteric.
In fact, the chronic metritis and endometritis of women during
the climacteric age, differs in no important respect from these diseases
as they are seen in women during their sexual prime. We
612merely note that the enlargement of the uterus is less marked; but
the thickening and extreme hyperaemia of the mucous membrane are
the same in both cases, the secretion is increased in quantity, the
vaginal portion of the cervix is elongated, and usually displays erosions,
excoriations, or ulcers. The subjective troubles appear less
pronounced than in the case of the metritis of the menacme. The
prognosis is as a rule a more favourable one than in the earlier
years of sexual life, for as soon as the series of involuntary processes
is completed, when the retrogressive changes in the genital
organs are at an end, when senile atrophy of the uterus and the
uterine annexa has set in, a cure of the troubles formerly so obstinate
and so enduring speedily takes place.
Quite recently, much has been written upon the subject of a
peculiar senile endometritis (Patru, Skene, Mundé, Rüder, Sheldon,
Herman, and others), and it has been described as “a peculiar form
of senile, haemorrhagic, leucocytal hyperplasia of the uterine mucous
membrane” (Gottschalk). According to Maurange and Lorain it
occurs in as many as 7.2% of elderly women. It is seen especially
in women who earlier in life have suffered from diseases of the
genital organs, more especially those who have previously suffered
from endometritis; at times a senile vulvitis or vaginitis is the cause
of the disease. Displacements of the uterus with kinking of its
canal, whereby retention of the secretion and its decomposition are
induced, has been assigned as an additional cause of the disorder,
also prolapse of the uterus, and, in isolated instances, necrotic fibromata.
According to the degree to which the atrophy of the tissues
has proceeded, and according as the mucous membrane is still partly
retained or entirely destroyed, and according to the extent to which
the uterine vessels have been affected with the sclerotic processes
of old age, does the pathologico-anatomical picture of senile endometritis
vary. It may affect the body only of the uterus, it may extend
also to the cervix, the vagina, and even the vulva; upwards it
may pass to the uterine annexa and to the peritoneum. The first
and most important symptom of this senile endometritis is the outflow,
usually intermittent, rarely continuous, of a sero-purulent, and
sometimes sanguineous discharge, with a powerful foetid smell;
there are colicky pains, which pass off when the uterus has emptied
itself; often, also, there are atypical bleedings, which are not profuse.
The uterus is usually found to be larger than the atrophy general at
the patient’s age would have led us to expect, it is often retroflexed,
the cervix is thickened, the lips of the os uteri are usually everted
and raw. When persistent, this senile endometritis causes profound
constitutional disturbance, and is often difficult to differentiate from
carcinoma of the uterus.
613Under the name of senile irritation of the uterus, Maxwell has
described a disease occurring at the climacteric, characterized by an
enormously increased irritability of the uterus, with marked reflex
manifestations; in these cases also we may perhaps have to do with a
senile endometritis. The most pronounced symptom is a severe and
constant uterine pain, to which in the course of the disease are superadded
pains in the gastric and cardiac regions, the rectum, and the
spinal column; these pains lasted a long time, and their severity was
such that it became necessary in some cases to remove the uterus.
Hydrometra is a disease which makes its appearance principally
late in the climacteric period, when menstruation has already completely
ceased, and when the adhesions associated with the climacteric
atrophy of the uterus have led to atresia of the cervical canal.
Among 74 cases of hydrometra (from the material of the Pathologico-Anatomical
Institute of Prague, in the years 1868 to 1871) not
one of the women was less than 40 years of age; the age distribution
of the cases was in fact the following:
| Quinquennium 40 to 45 |
3 cases |
| Quinquennium 45 to 50 |
2 cases |
| Quinquennium 50 to 55 |
2 cases |
| Quinquennium 55 to 60 |
8 cases |
| Quinquennium 60 to 65 |
18 cases |
| Quinquennium 65 to 70 |
12 cases |
| Quinquennium 70 to 75 |
11 cases |
| Quinquennium 75 to 80 |
8 cases |
| Quinquennium 80 to 85 |
4 cases |
| Quinquennium 85 to 90 |
6 cases |
In 40 of these cases, the occlusion was in the region of the os
internum, in 23 it was in the region of the os externum, in 9 cases
the whole length of the cervical canal was obliterated, and in 2 both
the internal and the external os were occluded, the intervening portion
of the cervical canal being still patent. In the two latter cases,
there was hydrometra bicamerata, with retroflexion of the uterus.
Late in the climacteric period, haematometra also occurs, though
less often than hydrometra. When, in cases in which the os uteri
externum is occluded, in consequence of adhesion between the
vaginal walls and the vaginal portion of the cervix, as a sequel of
the vaginitis ulcerosa adhesiva of elderly women, there is haemorrhage
from the atheromatous vessels of the uterus or the tubes,
the blood necessarily distends the uterine cavity.
During the climacteric period, leucorrhoea is so extraordinarily
frequent, as the figures previously given show, that the assumption
is justified that with the diminution or cessation of the menstrual
flow, this hypersecretion from the genital mucous membranes forms
as it were a kind of vicarious flux. Sometimes, as in 12 cases recorded
by Tilt, we actually have a periodic “menstrual leucorrhoea”;
614in one of these cases the discharge recurred at regular monthly intervals
for 12 months, in another for 18 months, in several for 2
years, and in one for as long as 7 years. It is only by careful examination
that the exact source of the discharge can be determined, for
during the climacteric also, as well as earlier in life, leucorrhoea may
be due either to endometritis or to colpitis. A muco-serous or
sanguino-serous secretion may also be due to slight vulvitis.
A peculiar form of inflammation occurring after the completion
of the menopause, and after the atrophic process in the vagina is
considerably advanced, is known as colpitis senilis. In this disease,
ulceration readily occurs, followed by cicatricial adhesion between
the anterior and posterior walls of the vagina (vaginitis adhaesiva
vetularum); in other cases herpetiform eruptions arise, with a tendency
to pustule formation; occlusion of the vagina may lead to
hydrometra and pyometra; sometimes the obliteration of the vagina
is complete, so that there is neither outlet for blood from the uterus,
nor inlet for the penis during coitus. This vaginitis adhaesiva vetularum
is by no means rare in the climacteric period; as a rule it
does not give rise to very serious trouble, the most prominent symptom
being usually somewhat persistent haemorrhage, unaccompanied
by any evil odour. On local examination, the characteristic strings
of scar tissue are felt, passing from the portio vaginalis to the
narrowed, senile vaginal fornix; from the cervical canal there exudes
a usually somewhat vitreous mucus, mixed with blood. The
cervix itself is thin and atrophied, the uterus also is greatly diminished
in size.
The frequency at the time of the menopause of such catarrhal
inflammatory processes in the vagina and vulva is said by Duprès to
depend on the weakness or paresis of the bladder which is so common
in women at this time of life. Owing to the incomplete evacuation
of the urine, cystitis very readily ensues; the urine is evacuated involuntarily
during sleep, and some of this fluid passes through the
vaginal orifice, giving rise all the more readily to colpitis, because
the secretion of the atrophic mucous membrane no longer possesses
the normal acid bactericidal properties. According to Scott, vulvitis
may also arise as a sequel of calculus-formation in the glands of Bartholin,
a frequent occurrence in elderly life, followed by inflammation
and abscess-formation in these glands. Among the diseases of
the genital organs at the climacteric period, Fritsch also enumerates
urethral caruncle and carcinoma of the clitoris.
Displacements of the Uterus.—Among the commonest of the displacements
of the uterus occurring during and after the menopause,
is prolapse of the organ. Previously existing descent of the uterus
is apt to be greatly aggravated at the climacteric, a partial prolapse,
615for instance, becoming complete; or prolapse of the uterus may
first set in at this period of life.
There are several contributory causes of the liability to prolapse
at this particular epoch, especially in women who have had a great
many children, and in those with either enlargement of the uterus
or with lacerated perineum; the most powerful of these causes being
the weakening of the uterine supports in consequence of the general
relaxation of the pelvic tissues. At the menopause, the connective
tissue by means of which the uterus is attached to surrounding
structures, withers; simultaneously the vagina atrophies, and this
source of support is weakened; the whole pelvic floor loses its firmness
and power of support. For these reasons, a uterus which has
hitherto been in correct position readily becomes retroverted and to
some extent prolapsed; whilst one that was already thus far displaced
prior to the menopause, will now be apt to descend still
further till it rests upon the perineum. With the disappearance
from the vulva and the perineum of the adipose tissue on which
their firmness so largely depends, complete prolapse of the uterus
is now likely to ensue. Prolapse of the urethra may also result
from senile involution of the pelvic contents.
Among my 500 cases of women at the climacteric, there were 65
instances of more or less severe prolapse of the uterus. The frequency
of prolapse in women at the climacteric and in those at a
more advanced age, is shown by the following figures, which are
compiled from the post mortem statistics of the Pathologico-Anatomical
Institute of Prague (years 1868 to 1871). Prolapse of
the uterus was found:
| In the quinquennium 30 to 35 in |
2 women |
| In the quinquennium 35 to 40 in |
2 women |
| In the quinquennium 40 to 45 in |
6 women |
| In the quinquennium 45 to 50 in |
3 women |
| In the quinquennium 50 to 55 in |
6 women |
| In the quinquennium 55 to 60 in |
8 women |
| In the quinquennium 60 to 65 in |
6 women |
| In the quinquennium 65 to 70 in |
4 women |
| In the quinquennium 70 to 75 in |
4 women |
| In the quinquennium 75 to 80 in |
4 women |
| In the quinquennium 80 to 85 in |
2 women |
Flexions and versions of the uterus, common as they are at the
time of the menopause, have no longer the same importance that
they possessed during the prime of the sexual life. For on the one
part the size of the uterus is greatly diminished, in consequence of
the lessened blood-supply and of senile involution of the organ; and
on the other, after the cessation of menstruation, the profuse
haemorrhages and severe colicky pains which for the most part
occurred during menstruation in these cases of kinking of the
uterine canal, and which gave rise to such severe general disturbance,
616now no longer occur. Herein lies the explanation of the fact,
well known to all experienced practitioners, that women who have
for many years suffered from retroflexion or retroversion of the
uterus associated with severe and painful symptoms, cease to suffer
after the menopause is established, and regain excellent health,
although the local condition of the uterus remains unrelieved.
Neoplasmata of the Uterus and of the Uterine Annexa.—The
most serious danger to the life of a woman during the climacteric
period is to be found in the strong tendency to the occurrence
of carcinomatous disease of the uterus—a predisposition so marked
that not less than one-half of all illnesses affecting the reproductive
organs of women at this age are cases of carcinoma of the uterus.
The disease occurs especially at the beginning of the climacteric,
between the ages of 45 and 50 years, most often in the form of
carcinoma of the portio vaginalis, whereas after the completion of
the menopause, carcinoma of the body of the uterus is the preponderant
form. The true reason for the frequency of the occurrence
of carcinoma at this period of life will only become clear to us when
we are more fully acquainted with the nature and origin of this form
of malignant disease. Meanwhile, it would seem that the predisposition
to cancer during and shortly after the menopause depends
upon the anatomical changes in the reproductive organs at the
time of involution, which render these organs a more suitable soil
for the proliferation of malignant growths; and further it is
probable that the loss of the acid, bactericidal quality of the vaginal
secretion, opens the door for the entrance of pathogenic micro-organisms.
Noteworthy is the observation of Baer and Leopold, that
very frequently a preclimacteric or climacteric fungous endometritis
forms the stage of transition to the development of carcinoma of the
body of the uterus. At the time of the menopause there is also
an increased liability to the occurrence of cancer of the ovaries.
Numerous statistical data have been published regarding the frequency
with which carcinoma of the uterus occurs at various periods
in women’s lives, and, notwithstanding all variations, one fact
stands out clearly, namely, that this disease occurs most frequently
in the fourth and fifth decennia, and above all during the climacteric
period.
From Gusserow’s collection of 526 cases, observed by Lebert,
Kiwisch, Chiari, Scanzoni, and Saexinger, the following table has
been drawn up, and it shows very clearly the great preponderance of
the disease in the fifth decennium of a woman’s life:
| At ages of from 20 to 30 there were |
12 cases |
| At ages of from 30 to 40 there were |
161 cases |
| At ages of from 40 to 50 there were |
217 castes |
| At ages of from 50 to 60 there were |
102 cases |
| At ages of from 60 to 70 there were |
38 cases |
| At ages of from 70 and upwards there were |
5 cases |
617From the mortality statistics we obtain a similar result as regards
the age incidence of carcinoma of the uterus. Thus, in England
there died of this disease in one year:
| Women at ages of from 15 to 25 |
44 |
| Women at ages of from 25 to 35 |
184 |
| Women at ages of from 35 to 45 |
717 |
| Women at ages of from 45 to 55 |
1110 |
| Women at ages of from 55 to 65 |
1116 |
| Women at ages of from 65 to 75 |
876 |
Coming now to the consideration of fibromyomata of the uterus,
we cannot share the opinion that at the climacteric age there is a
special predisposition to the origination of such tumours, or that the
climax favours the growth of already existing fibromyomata. It
appears to us that in the preclimacteric epoch and the commencement
of the climacteric, the symptoms of existing fibromyomata
become more troublesome, the haemorrhages are more severe, the
pains more violent; but that as the menopause is established, these
troublesome symptoms decline progressively in intensity, and not
only is there an arrest in the growth of the tumours, but often an
actual diminution in their size.
I have myself repeatedly observed such cases, in which I had the
opportunity of watching the growth of the myomata during a period
of ten years or more. Other cases, indeed, show that myomata
may increase in size after the menopause, at times with remarkable
rapidity, and further that at this period of life a malignant degeneration
may occur in such tumours. Carcinomatous, sarcomatous,
and myxomatous degeneration have been observed, and also the
transformation of a myoma into a soft fibrocystic tumour.
Atrophy of fibromyomatous tumours at the menopause, associated
with the atrophy of the uterus that then occurs, has been observed
by Playfair and by Doran. The tumour shrinks, its muscle-cells
become smaller, and undergo fatty degeneration, there is an increase
in the interstitial connective tissue, so that ultimately the fibromyoma
is transformed into a firm and dense fibroid swelling. Cases
in the older literature and also a recent observation of Yamagiron
have shown that calcification of uterine fibromyomata sometimes
occurs, leading to the formation of the so-called “uterine calculi.”
In the case of pure myomata, the diminution in size occurring at
the climacteric is generally due to resorption and fatty degeneration,
whereas in the case of fibromyoma it depends on induration and
atrophy. It remains uncertain whether the growth of purely fibrous
tumours is also affected by the climacteric.
Whilst the influence of the climacteric on the growth of fibromyomata
is thus usually advantageous to the patient, exceptions occur,
618as is shown by cases recorded by Lawson Tait, Schorler, and Boerner;
the last-named author points out that at the climacteric there is
a tendency for the transformation of fibromyomata into sarcomata.
Kleinwächter had under observation 78 cases of fibromyomata of
the uterus in women who were older than 45 years; in only 8 of
these was a diminution in the size of the tumour observed at the
menopause; in 11 cases at this time, the tumour increased in size
more or less rapidly; in 3 cases, a carcinomatous change occurred in
the tumour; in 3 cases, the tumour was first observed at the time of
the menopause; in 13 cases, the haemorrhages appeared to undergo
a complete arrest at the menopause, but the size of the tumour was
not affected; in the remaining 48 cases, no influence, either favourable
or unfavourable, appeared to be exercised by the menopause on
the fibromyoma of the uterus.
Cases reported by Rogival, Simpson, and Gusserow indicate the
existence of a certain predisposition to the growth of sarcomata of
the uterus at the climacteric period. Gusserow more particularly
insists on the fact that we must bear in mind the likelihood of
the origination of a fibrosarcoma or of the sarcomatous transformation
of a fibromyoma, in all cases in which a fibrous tumour of the
uterus first attracts attention at the climacteric period; or in which
a tumour hitherto small and inconspicuous and giving little or no
trouble, begins at this time to increase in size or to give rise to
troublesome symptoms.
Neuroses of the Reproductive Organs.—One of the commonest
neuroses of the reproductive organs at the climacteric period is
pruritus vaginae et vulvae, and it is one of the most distressing
symptoms of which women of this age complain. The disorder depends
upon a hyperaesthesia of the sensory nerves of the vagina
and the external organs of generation. It is characterized by enduring
sensations of itching and burning, which may be either
periodic (and then usually nocturnal) or continuous; at times it becomes
so severe that the women thus affected have an unceasing
desire to scratch, avoid all society, and ultimately find life quite
unbearable. In the slighter degrees of pruritus, no objective
changes are to be observed in the genital organs, or at most some
slight hyperaemia of the vaginal orifice. In the more severe forms,
however, there are local nutritive changes: the labia are swollen,
their surface has an erythematous blush, a number of the hair-follicles
are enlarged and prominent; the vaginal orifice is abnormally
sensitive, it is scarlet or livid-red in colour and here and there denuded
of epithelium, and there are scattered mucous follicles distended
with a serous or purulent fluid; these small vessels are to be
seen chiefly on the inner surfaces of the labia minora and around
the clitoris. At the same time, the vulva secretes an acid, burning
619fluid, which greatly increases the patent’s sufferings, and at times
impels her irresistibly to the practice of masturbation. In cases of
long standing, we find hypertrophy, elongation, and deformity of
the nymphæ, and pigmentation of these organs, with the formation
of varices.
According to Fritsch, in exceptional cases pollutions are the
originating cause of the pruritus, and this may be the case in women
who are not sexually passionate. It occurs, indeed, especially in
matrons who have not had sexual intercourse for years, and who
have quite ceased to think about sexual matters; during the night,
such a woman will begin to have voluptuous dreams, associated with
a degree of sexual stimulation which is described as being actually
painful. The woman often suffers greatly from these lascivious
sensations. She complains that she cannot understand how it is
that she has become affected with such utterly undesired feelings.
She becomes profoundly depressed. Coitus often gives no relief
whatever; but many women thus affected declare, as Fritsch points
out, that by powerful, almost involuntary scratching, the stimulus
is speedily subdued, and that for this reason they are absolutely
compelled to scratch. It will readily be understood, that in this way
persistent pruritus will arise, with local effects of scratching, and
vulval eczema. According to the same author, in some instances
pruritus is due to great insufficiency of secretion, such as occurs in
the endometritis atrophicans which he was the first to describe.
This scanty secretion, as it passes over the external genital organs,
gives rise to irritation and itching. Haemorrhoids also play a part
in the etiology of pruritus.
Diseases of the Mammae.—The sympathy which in the earlier
phases of the sexual life—during the menarche, during pregnancy,
and during the puerperium—so obviously exists between the
breasts and the uterus, is seen also during the climacteric period. It
now finds expression chiefly in the marked tendency to new growths
in the mammae, a matter to which attention was already drawn by
Galen. The commonest of these neoplasmata is carcinoma mammae,
a disease which occurs chiefly during the climacteric epoch. In the
great majority of cases, cancer of the breast is a primary disorder;
in exceptional cases, however, the carcinoma of the breast arises by
metastasis from a cancer of the uterus or the ovary. Sometimes
the breast tumour is preceded by Paget’s disease of the nipple. For
several years the patient suffers from what appears to be a chronic
dermatitis of the nipple, the areola mammae, and the surrounding
skin; but ultimately, and hardly ever before the commencement of
the menopause, carcinoma of the breast ensues.
The older statistical enquiries of Birkett, Lebert, Scanzoni, and
Velpeau, showed that carcinoma mammae most commonly occurred
620between the ages of 40 and 50 years, and next to that in frequency
between the ages of 50 and 60 years.
A general hypertrophy of the mammary gland, affecting not only
the enveloping and intra-lobular adipose and connective tissue, but
also the proper glandular substance, is very rarely observed during
the climacteric period; but in the preclimacteric epoch and in the
early part of the climacteric, we not uncommonly see a hyperplasia
of the adipose tissue of the breast, either as a local manifestation of
a developing general obesity, lipomatosis universalis, or as a purely
local excessive deposit of fat. In such circumstances, the mammae
may at times be transformed into monstrous tumours.
Diseases of the Organs of Circulation.
Among the cardiac disorders of the menopause, the earliest and
the commonest is, in my own experience, the following. At the
time of the menopause, exceptionally not till after the complete cessation
of menstruation, but usually at the commencement of this
period of life, some time, that is to say, between the age of 40 and
50, either when menstruation has become irregular, the intermenstrual
interval having become longer or shorter than has hitherto
been the case, or when the discharge has become abnormal in character,
a woman who has not before suffered from any kind of
cardiac disorder, will begin to complain of paroxysms of palpitation.
In some cases the attacks of palpitation occur in the absence of any
discoverable exciting cause; in others, some trifling stimulus gives
rise to them. They may arise when the patient is in any position,
walking, standing, sitting, or recumbent; sometimes even during
sleep. The subjective sensation aroused by the increased force and
frequency of the cardiac action is described as extremely distressing;
it is associated with a feeling of anxiety (Angst), with a
sense of pressure in the chest, with forcible pulsation of the carotids
and of the abdominal aorta; frequently also with a feeling of a
rush of blood to the head, with fugitive heats, and severe headache;
sometimes towards the end of the attack there is a sense of flickering
before the eyes (as of muscae volitantes), tinnitus aurium,
dizziness, and in rare cases actual syncope.
Objectively, during the paroxysm, a notable increase in the frequency
of the heart’s action can be detected, the pulse-rate rising to
120 or even 150 per minute. In most of my cases, the pulse
throughout the attack remained strong, well-filled, and regular.
Sphygmographic tracings taken during the seizures showed a remarkably
high pulse-wave, the ascending limb of the curve rose rapidly
and suddenly, the descending limb fell with corresponding steepness
and rapidity, and it reached an unusually low level before the commencement
621of the dicrotic elevation, which latter was exceptionally
large; the predicrotic elevations, on the other hand, were but slightly
developed. On auscultation, the tones of the heart were pure, but
were louder than normal.
Sometimes during a paroxysm a sudden reddening of the face
was noticeable, extending often to the neck and the thorax. In the
areas mentioned, vivid red patches would suddenly make their appearance,
disappearing more gradually after lasting a few minutes—this
appearance was associated with a burning sensation of the
affected areas. In some cases during the paroxysm there was an
outbreak of perspiration on the head and the back.
Associated with these cardiac troubles of women at the climacteric
we usually find a state of physical and mental disquiet; less common
associations are, an incapacity for regular work, sleep uneasy and
much disturbed by dreams, great general nervous irritability, or
signs of passive congestion in various organs; occasionally there is
oedema of the lower extremities; the urine remains free from
albumen.
In most of the cases of this nature which came under my own
observation, a certain plethora was noticeable; among women at
the menopause, it was especially the well-nourished, powerful,
sanguine individuals, that were liable to palpitation of the heart.
Direct examination of the blood sometimes showed a very high
haemoglobin richness—110, 115, or even 120, as compared with a
haemoglobin-richness of 93 in normal woman. Several of my
patients presented the clinical picture of the plethoric form of
lipomatosis universalis.
In all, during ten years, I observed 67 cases of paroxysmal
tachycardia in climacteric women. The age distribution was the
following:
| 36 years of age |
1 woman |
| 38 years of age |
1 woman |
| 39 years of age |
2 women |
| 40 to 45 years of age |
37 women |
| 45 to 50 years of age |
28 women |
| Over 50 years of age |
8 women |
Five of the patients were unmarried, three were married but
childless, the remaining 59 were parous women.
As a general rule, women live in great dread of all manifestations
of bodily disorder during the menopause; those who become
affected with paroxysmal tachycardia are exceptionally anxious, and
regard themselves as threatened by a “stroke.” This pessimistic
view is however, by no means justified. These cardiac disorders
may make their appearance some time before the menopause, they
may persist throughout the period during which menstruation is
622irregular, they may even endure for some time after the total cessation
of the flow—but serious consequences of this climacteric
tachycardia have never come under my observation. As regards
treatment of the disorder, I have seen very favourable results from
the following measures: The systematic employment of mild purgatives,
combined with suitable dietetic and hygienic regulations
(bland diet, regular and strenuous exercise, cold ablutions, and wet
compresses surrounding the abdomen).
When we enquire regarding the cause of the tachycardiac
paroxysms occurring at the menopause, we must first of all bear in
mind that in the cases which have come under my own observation,
the cardiac impulse was powerful, the pulse strong and well-filled,
that signs of general vasomotor disturbance (ardor fugax, etc.)
accompanied the tachycardiac seizures,—hence we are led to infer
that we have to do with a stimulation of the excito-motor nerve
fibres, which would appear to be due to the climacteric changes
previously described as occurring in the female reproductive organs.
This view receives support from the fact that after oöphorectomy,
when, as in the normal climacteric, atrophic processes occur in the
internal reproductive organs, paroxysms of nervous palpitation are
frequently observed. The same explanation applies to the fact that
in women at the climacteric affected with these tachycardiac
troubles, we frequently see in association therewith the symptoms of
uterine dyspepsia.
But in addition to these local anatomical changes in the reproductive
organs, to which an etiological role must be assigned in the
production of climacteric tachycardia, the irritable state of the accelerator
nerves must also depend in part upon that general nervous
hyperexcitability which is so often a characteristic feature of the
climacteric period in women, manifesting itself in manifold hyperaesthesias,
hyperkinesias, neuralgias, and, in extreme cases, mental
aberration. The sensory nerves are more irritable than in their
normal state, so that every stimulus acting upon them evokes a
greater central effect than heretofore, and upon this ensues an exaggeration
of various reflex manifestations, which appear altogether
disproportionate to the strength of the exciting cause; among these
disproportionate reflex effects, is to be numbered the tachycardia
just described.
But in addition to the causes of climacteric tachycardia already
enumerated, we have to take into consideration the results of recent
investigations concerning the organo-therapeutic employment of
the chemical constituents of the ovarian tissue; it would seem that
when at the menopause the ovaries undergo atrophy, so that their
internal secretion is no longer poured into the blood, the resulting
623alteration in the chemical constitution of that fluid gives rise to a
disturbance of the vasomotor centre in the medulla oblongata.
In some cases, the tachycardiac paroxysms appear to be connected
with the erotic excitement to which women are sometimes subject
at the climacteric, voluptuous crises and ejaculation occurring; it is
possible that in some of these cases masturbation plays a part.
A second group of cardiac troubles occurring in climacteric
women consists of cases which are very common, but not often very
severe. The cases in question depend upon the liability to an increased
deposit of adipose tissue in the body at the time of the menopause,
and in this connexion the plethoric form of lipomatosis universalis
almost invariably predominates. It is a well-known fact
that between the ages of 40 and 50 years women have an excessive
tendency to obesity, and that even those women who have hitherto
been extremely lean are apt to become quite plump at the climacteric
period. Chiefly in consequence of this increasing obesity, there
occurs in climacteric women a series of cardiac troubles of very
variable intensity. If the deposit of fat is effected very gradually,
and if the obesity does not become extreme, it is only after vigorous
bodily exercise, such as fast walking or going upstairs, and after
meals, that the patient is troubled with a little shortness of breath
and moderate palpitation; appetite, digestion, and sleep remain
usually unaffected in cases of this degree of severity. Definite attacks
of cardiac asthma, and well-marked signs of cardiac insufficiency
affecting the entire circulatory system, will very rarely occur
in such persons.
It is an interesting fact, that the troubles which arise from fatty
deposits around the heart are in general far less severe in climacteric
women than they are in obese men of corresponding age. This
may be due to the circumstance discovered by W. Müller, in the
course of his investigations on the proportions of the human heart,
that in the development of general obesity, the pericardial fat increases
proportionately to a greater extent in the male than in
female. But in my opinion the true explanation is to be found in
the fact that variations in the amount of fat in the body are normally
far more extensive in women than in men; at puberty, during pregnancy,
and during lactation, extensive though gradually effected
changes in the amount of adipose tissue in various parts of the body
occur, so that experience has rendered the organism ready to adapt
itself to the further changes that take place at the climacteric—above
all, the heart has become competent to meet very various demands
upon its powers.
Only in women who from youth onwards have exhibited a marked
tendency to obesity, and in whom at the climacteric age such obesity
624has become extreme, do the cardiac troubles attendant on the menopause
become very severe. In such persons, palpitation and shortness
of breath occur on slight exertion, and attacks of cardiac
asthma are frequent. In consequence of the diminished propulsive
power of the heart, circulatory difficulties make their appearance in
the most widely divergent venous areas; the forms most commonly
met with are, varices in the veins of the lower extremities, permanent
dilatation of certain of the small superficial veins of the skin,
phlebectases of the rectal veins (i. e. “piles”), and ultimately we
see the well-known series of symptoms of venous engorgement—oedema
of the feet, passive congestion of the lungs, albumen in the
urine, etc.
When such cardiac troubles are present, the objective examination
of the heart shows in the early stage no gross abnormality; at most
the heart-tones seem somewhat weakened, with a moderate enlargement
of the area of percussion-dulness, whilst the impulse is displaced
a little outwards, and is weaker than normal. In some cases,
however, a marked dulness on percussion over the sternum indicates
an extensive deposit of fat in the mediastinal tissues. In the second
stage of the fatty heart, when the symptoms have become more
severe, we find a considerable enlargement of the area of cardiac
dulness both in the vertical and the horizontal extent; the cardiac
impulse is diffused as well as feeble. The sounds of the heart are
usually pure but faint—in some cases they remain loud and clear.
Exceptionally, a short blowing murmur is heard with the first
sound; and sometimes this sound is reduplicated.
Whilst in the first stage the pulse is hardly abnormal, in the second
stage, very various changes occur; often it is subdicrotic or dicrotic
in character.
In the great majority of instances, in these cases of cardiac disorder
at the menopause, provided a suitable dietetic regimen is early
adopted and perseveringly carried out, we may give a hopeful prognosis.
A third, less common but far more serious form of cardiac disorder
occurring at the menopause, displays the well-known symptoms
of cardiac failure. Those thus affected are usually slightly
built, delicate women, who during the years of development suffered
from chlorosis, who in adult life were troubled with anæmic symptoms,
and in whom the menopause was ushered in by very severe
losses of blood; sometimes, again, they are women who throughout
their sexual prime have been accustomed to menstruate very abundantly,
who have had numerous and severe deliveries, or who have
had frequent miscarriages—it is in those who have thus been
weakened by frequent and profuse haemorrhages, that the symptoms
of cardiac failure ensue at the climacteric period. The women thus
625affected also frequently suffer from palpitation of the heart; the
pulse is abnormally frequent, small, low, and easily compressible,
and sometimes intermittent or arrhythmical. The heart’s action is
weak and devoid of energy. The heart-sounds are usually obscure,
and sometimes a systolic murmur is audible. The patients are short
of breath and are subject to attacks of cardiac asthma, not infrequently
associated with angina pectoris. In conjunction with these
symptoms, we see signs of venous congestion: sudden attacks of
coldness in the hands and feet, often also oedema of the feet; the
urine at times contains albumen. The haemoglobin-richness of the
blood is always notably diminished. I need not discuss in further
detail the well-known symptoms of cardiac insufficiency, and I need
only insist that when these symptoms are met with in women at the
climacteric, it is of the greatest importance, alike from the prognostic
and from the therapeutic standpoint, to make a careful examination
of the reproductive organs, so as to determine the exact
source of the recurrent bleedings which usually constitute the
primary cause of the patient’s sufferings.
In several cases of this kind, I found that the haemorrhages were
due to a relaxation of the uterine tissues, and that this relaxation
was itself referable to intrapelvic circulatory disturbances, dependent
upon obstruction in the vena cava inferior, whereby the venous
return from the pelvis was rendered difficult, and an engorgement
of the uterine vessels was brought about.
In some instances of cardiac failure at the menopause, chronic
inflammation within the pelvis is to blame for the menorrhagia upon
which the cardiac failure depends. Often, again, the haemorrhages
are referable to vasomotor influences, such as are liable during the
menopause to affect various vascular areas. In other cases, the
recurrent bleeding is due to retroflexion of the uterus, to prolapse
of that organ, or to tumour, it may be myoma, polypus, or carcinoma.
Finally, during the menopause, more especially in women in whom
menstruation has continued up to or beyond the fiftieth year, or in
those who have given birth to a large number of children or have
lived lives of severe bodily exertion, cardiac troubles may arise dependent
upon arteriosclerosis of the great vessels. The signs of
such changes in the walls of the bloodvessels are clearly marked:
the cardiac impulse is heaving, the second sound of the heart is
accentuated; the pulse is full and large, usually giving a very
powerful blow to the examining finger, whilst its sphygmographic
tracing exhibits characteristic signs in the exceptional height and
great distinctness of the first predicrotic elevation. The subjective
troubles are in these cases very severe; dyspnoea and attacks of
626asthma or of vertigo are common, and sometimes albumen may be
found in the urine.
We may thus summarize the cardiac disorders met with at the
menopause, and more or less directly dependent upon the changes
undergone by the feminine organism at that period of life:
1. Paroxysmal tachycardia, a reflex neurosis due to the climacteric
changes in the ovaries.
2. Nervous palpitation in women who were similarly affected at
the time of the menarche, and in whom the trouble is merely the
expression of a very unstable nervous system, and one influenced with
especial readiness by impressions proceeding from the reproductive
organs.
3. Cardiac disorder due to the obesity so commonly occurring as
a part of the general metabolic changes of the menopause, but more
particularly dependent upon a deposit of fat in the neighbourhood
of the heart itself.
4. Symptoms of cardiac failure, due to excessive losses of blood
at the menopause, either as an exaggeration at this time of menstrual
processes, or as a result of some actual disease within the
pelvis.
5. Cardiac disorder in women in whom the menopause occurs at
an unusually advanced age, and dependent upon arteriosclerosis.
Particular consideration must be given to a symptom not infrequently
occurring in association with the cardiac troubles of climacteric
women, and referable to the circulatory disturbances characteristic
of this period of life, namely, vertigo. The attack in some
cases comes on without apparent cause, in others it occurs on the
performance of some unusual movement or the adoption of some
peculiar posture (stooping, or the like); the patient is suddenly
seized with a sense of rotation, either of his own body, or else of his
visible and palpable environment; with this is associated a sensation
of disturbance of equilibrium, flickering before the eyes (muscae
volitantes), tinnitus aurium, palpitation of the heart, increased frequency
of the pulse, which may be either full or small, redness or
pallor of the face, coldness of the hands and feet, muscular twitchings,
a sense of great anxiety, and the outbreak of a cold perspiration.
The vertigo occurs in paroxysms, usually of short duration—a
few minutes to a quarter of an hour. It is especially plethoric
and obese women who are liable at the climacteric to suffer from
this disorder.
A somewhat similar condition is described by Tilt under the name
of “pseudo-narcotism,” as frequently occurring in climacteric
women. Tilt indeed states that in 500 such women, he noted its
presence in no less than 277.
627Many hypotheses have been promulgated to account for the vertigo
that so frequently occurs at the menopause. Both anæmia and
hyperaemia of the brain have been assumed as causes, alike dependent
upon the irregularity of menstruation, which is supposed to have
a reflex influence upon the cerebral circulation. Others regard the
vertigo as a climacteric neurosis, since it occasionally occurs before
the menstrual irregularities begin, and in such cases a reflex disturbance
of the cerebral circulation cannot be supposed to have
arisen. According to Matusch, climacteric vertigo is a manifestation
of epilepsy—an explanation which has been often extended to
include all the menstrual psychoses. Windscheid believes that in
many of the cases the vertigo is to be explained by the existence of
arteriosclerotic changes in the blood vessels, such as are already by
no means rare at the age at which the menopause usually occurs;
whilst in other cases, he believes, the vertigo is to be regarded as
one of the symptoms of a nervous disorder. That in any case the
vertigo is dependent in some way upon the changes that occur in the
reproductive organs at the climacteric period, is shown by the fact
that after the final cessation of menstrual activity the patient as a
rule ceases to suffer from this symptom.
To the circulatory disturbances consequent upon the menopause
we must also refer ardor fugax, fugitive heat, the sudden rushes of
blood to which women are prone at this period of life.
The cardiac troubles of the menopause are seen especially in
women in whom the cessation of menstruation occurs quite suddenly,
and in those in whom menstrual activity ceases at an exceptionally
early age. It would seem that in such cases, owing to the continuance
of periodic maturation of the graafian follicles associated with
congestion of the intrapelvic organs, in the absence of the periodic
relief to that congestion afforded by the menstrual flux, there results
a summation of stimuli, whereby the accelerator nerves of the
heart are very powerfully affected.
Thus, I had under my care a lady from Smyrna 36 years of age.
She had begun to menstruate when 12 years of age and menstruation
was always scanty; she married when 15 years old, and finally
ceased to menstruate when 19 years of age; she was sterile, and no
abnormality could be detected on physical examination of her reproductive
organs. Every month she suffered from severe paroxysmal
tachycardia, with dyspnoea, rush of blood to the head, perspiration
of the face, etc.
In another case, that of a woman 45 years of age, menstruation,
hitherto regular, was suddenly suppressed, during the flow, in consequence
of a severe fright. The next month the flow failed to
appear at the usual time, but instead the patient was affected with
severe cardiac distress, accompanied by sudden sensations of heat
628in the face, palpitation of the heart, and vertigo; these symptoms
lasted for several days, and since then have recurred at intervals of
three or four weeks.
The cardiac troubles of the menopause are seen with especial frequency
in women who were affected with similar disturbances at the
time of the menarche. Experience clearly shows that a certain
connexion exists between the manifestations that accompany the
commencement of sexual activity, and those that accompany the
decline and extinction of that activity; and a physician will rarely
be mistaken if he bases on the fact that the general health was or
was not seriously affected at the age of puberty, a prognosis that the
course of the climacteric will be an unfavourable or a favourable one,
respectively. In other words, in women whose nervous system is
an unstable one, and in those with hereditary predisposition to the
occurrence of cardiac disorder, the changes that take place in the
reproductive organs both during the menarche and during the menopause,
are likely during these vital phases to arouse reflex disturbances
of the cardiac functions. The facts thus noted are analogous
to those observed by Potain, who distinguishes a peculiar form of
chlorosis, occurring in delicate individuals at the age of puberty,
and, though apparently cured during the menacme, recurring in its
primitive severity at the time of the menopause.
Again, women with a sanguine and erethistic temperament are
more inclined to suffer from cardiac troubles at the menopause than
women of a tranquil temperament and those endowed with an
unimpressionable nervous system.
Finally, elderly virgins, women who have for many years lived
in chaste widowhood, sterile women, women who have married
shortly before the menopause, or who at this time have recently
been delivered, are all more inclined to the cardiac troubles of the
climacteric period than women whose sexual life has been of a less
abnormal character.
In the literature of the subject, we find numerous references to
the fact that among the disorders of the climacteric, circulatory disturbances
play a part. But a full and accurate account of these
disorders is lacking alike in the literature of gynecology and in that
relating to diseases of the heart—and this is true even of the most
recent publications.
Among striking individual cases, one recorded by Moon may be
mentioned here, a case of tachycardia consequent upon a sudden
menopause: “In a woman 35 years of age the menses were suppressed
owing to chill; the pulse-frequency increased from 80 to 200,
without any apparent change in the heart or its valves; the symptom
lasted for several days, when menstruation became once more
established, and the pulse-frequency fell again to the normal.”
629Tilt expresses the opinion that the heart is but little involved in
the disturbances of the climacteric, his experience coinciding with
that of Quain. Boerner and Glaevecke, on the contrary, describe
the heart troubles of the climacteric in terms very similar to those
employed by myself.
A. Clément describes a peculiar form of disturbance of the functions
of the heart at the climacteric period, to which he gives the
name of Cardiopathie de la Ménopause, and of which he has seen
four cases. The age of his patients varied from 46 to 50 years.
They were all vigorous women, free from hysterical symptoms, and
they had never suffered from rheumatism or from any functional
disturbance of the heart. In all these cases the cardiac disorder
occurred at a time of life when menstruation still continued, but had
already become somewhat irregular. Usually the trouble in question
makes its first appearance during the flow, or, if occurring independently
of menstruation, becomes more severe at that time. Prior
to the development of the actual heart symptoms, we observe for a
time, two or three months it may be, signs of general exhaustion
and weakness. Then occurs an attack of palpitation of the heart,
rapidly succeeded by faintness, sense of precordial anxiety, and
dyspnoea. During repose the patient does not usually suffer from
any difficulty in breathing, but sleep is apt to be disturbed by
paroxysms of palpitation and severe precordial anxiety. As the
disease advances, dyspnoea is observed on the slightest exertion.
Ultimately, the symptoms mentioned, palpitation, precordial anxiety
and dyspnoea, become permanent, but are less severe when the
patient is at rest. Constant now is also the feeling of weakness and
faintness, which from time to time increases to actual syncope with
complete loss of consciousness, and coldness of the entire surface of
the body. Examination of the heart gives negative results. The
cardiac impulse is a little stronger than normal; the cardiac rhythm
may be either regular or irregular, but actual intermission of the
beats does not occur. The heart-sounds are pure, there is no murmur;
the first sound, if altered at all, will be stronger, not weaker
than normal. Neither swelling of the jugular veins nor venous pulsation
is to be observed. The most striking symptom of heart
affection, indeed the only positive physical sign, is the great increase
in the frequency of the heart’s action, the pulse rate often being as
much as 150 or 160 per minute, and in addition weak and somewhat
variable in strength. At the outset of the disease, no oedema of
the lower extremities is to be observed, and it only appears after
three or four attacks. In all the patients the extreme pallor of the
face is a striking feature. An increased quantity of urine is eliminated.
The course of the disease is characterized by a series of successive
630paroxysms, separated by periods of almost complete remission.
At first, these remissions last for a month or two, but they
gradually become shorter and shorter, whereas the duration of the
attacks continually increases, until it is as much as seven or eight
days. At this stage, disturbance of digestion ensues, the appetite is
lost, and the general vigour declines. Recovery ultimately occurs,
but very gradually. Clément refers the disease to a profound disturbance
of the cardiac innervation through the sympathetic nerves,
but believes that anæmia constitutes a contributory cause of the
cardiac disorder.
Kostkewitsch has made observations regarding the influence of the
climacteric upon previously existing heart-disease, and has thereby
been led to conclude that the influence is unfavourable. The functional
disturbances of the cardio-vascular apparatus which commonly
accompany the menopause, readily lead, should organic heart-disease
exist, to the onset of severe cardiac weakness, which may have a
rapidly fatal termination. In 55.5% of the women who enter the
climacteric period with organic disease of the heart, the menopause
gives rise to a failure of compensation. Such failure of compensation
is especially likely to occur in women suffering from valvular
insufficiency; it is least probable in cases of arteriosclerosis without
valvular defect. The symptoms of defective compensation—dilatation
of the heart, increased frequency of the pulse, arrhythmia
cordis, etc.—are manifested especially during the menstrual flow.
Diseases of the Digestive Organs.
The congestions which, as we have already pointed out, constitute
the pathological basis of the majority of the disorders of the climacteric,
manifest themselves in the abdominal organs in the well-known
form of plethora abdominalis, chronic venous congestion of the gastric
and intestinal mucous membrane, hyperaemia of the liver,
hyperaemia of the mucous membrane of the bladder, catarrh of the
bladder, distension of the haemorrhoidal veins, and the various
symptoms dependent upon these several forms of congestion.
Bleeding from the haemorrhoidal veins and chronic diarrhoea are
two of the troubles proceeding from the above mentioned congestion
of the intra-abdominal vessels, which occur so frequently during
the climacteric period that since the days of antiquity they have been
regarded as critical manifestations of the menopause, the object of
which is to afford a vicarious outlet for the menstrual flux, now
become irregular and intermittent. It can, indeed, be readily understood
that a discharge of blood and an increased secretion from the
mucous membrane of the lower part of the intestine may, if not too
violent, exercise a favourable influence upon the congestive states
631of the climacteric, by relieving the distension of the abdominal vessels—by
a local blood-letting which regulates the disordered circulation.
In this way, even though we have ceased to regard it as a
“critical” manifestation, haemorrhoidal bleeding, accompanied by
an increased secretion from the intestinal mucous membrane, may
at the climacteric period have a distinctly favourable influence upon
a woman’s general condition.
Hippocrates already in his aphorisms pointed out the salutary
effect of epistaxis and of diarrhoea in women suffering from suppression
of the menses. Other authors have assigned a critical
significance to diarrhoeas occurring at the climacteric, and have
warned against their suppression. According to Tilt, diarrhoea
occurred in 12% of all women of this age coming under his observation;
in 4% of the climacteric women, this diarrhoea recurred at regular
monthly intervals, whilst in 8%, the recurrence was irregular. In
500 women during the climacteric age, Tilt observed the following
abdominal disorders:
| Swollen haemorrhoids in |
62 cases |
| Diarrhoea in |
60 cases |
| Enduring disturbance of the biliary secretion in |
56 cases |
| Bleeding haemorrhoids in |
24 cases |
| Intestinal haemorrhages in |
20 cases |
| Icterus in |
6 cases |
| Hæmatemesis in |
4 cases |
| Monthly intestinal haemorrhages in |
2 cases |
| Monthly bleeding from haemorrhoids in |
1 case |
In my own observation, constipation is more frequent in climacteric
women than diarrhoea, the constipation being also a symptom
of abdominal congestion. Sometimes, when diarrhoea occurs, it is
really secondary to constipation. The accumulation of the faecal
masses stimulates the intestinal mucous membrane, and gives rise to
a profuse aqueo-mucous secretion; the firm faecal masses are then
liquefied, the intestinal wall is lubricated, and the constipation gives
place to diarrhoea lasting perhaps for several days. This is the explanation
of many cases in which there is a periodic recurrence of
diarrhoea.
Dyspeptic disturbances are rarely absent during the climacteric
period. Most often we see disordered appetite, sluggish digestion,
pyrosis, eructation, at times nausea and retching, and actual vomiting
of a watery or bilious fluid. Occasionally, an abnormal sensation
of hunger follows each meal, associated, however, with a feeling
of distension of the stomach. A very distressing symptom is an
excessive formation of gas within the intestine. At times such
meteorism is extreme, and it then gives rise to very severe abdominal
pain. The gas is evacuated slowly and with difficulty, the
patient is compelled to loosen all her clothing; more especially after
632a meal she is compelled to take off her stays and undo all the bands
of her petticoats and skirt. At the same time we see difficulty in
breathing and tachycardia. Such an accumulation of gas within
the abdomen may give rise to serious errors in diagnosis, the swelling
being attributed to pregnancy or to abdominal tumour.
Noteworthy also at the time of the menopause is the occurrence
of vomiting, either as an isolated symptom, or in association with
some other well-known climacteric disorder. When this vomiting
is associated with some unmistakable form of excessive secretory
activity (hyperhydrosis, etc.), we may readily suppose that the
vomiting is due to undue secretory activity on the part of the gastric
mucous membrane. An excessive production of gastric juice, perhaps
altered in quality as well as quantity, combined with some other
disorder of gastric innervation (hyperaesthesia, or hyperkinesia)
will sufficiently explain the occurrence of the sometimes excessive
vomiting, even though in many of the cases there may be no reason
to suppose that there exists any primary stimulation of the vomiting
centre. In other cases, however, it is probable that the trouble is
really due to a primary disorder of that centre; and a careful study
of the clinical features of the case will be needed to show how far
there may be associated with this other disorders of gastric innervation
(Boerner).
Disturbances of the biliary secretion, icterus of greater or less
severity, are by no means rare manifestations of the abdominal congestion
of climacteric women, and such disorders have also been
regarded as vicarious processes originated by the cessation of the
menstrual flux (Aran, Bennet, Henoch, and others.) Frerichs also
has pointed out that with the cessation of menstruation at the climacteric
we not infrequently observe swelling of the liver, which
disappears when, after a considerable period, the menstrual flow
recurs—a sequence of symptoms which may be repeated again and
again for a considerable time.
Diseases of the Skin.
The most characteristic symptom of disorder of the skin met with
at the climacteric period—one which, indeed, may be said to be
never absent—is ardor fugax, fugitive heat; and scarcely less common
is hyperhydrosis, an excessive secretion of sweat. Almost
invariably, at the commencement of the menopause, women complain
of a feeling of burning heat, rising up from the breast to the
face; and if they are kept under observation we see from time to
time a sudden redness of the face, and sometimes also of the neck
and chest, associated with the outbreak of a thin perspiration. Moreover,
in nearly all climacteric women, we notice an increased secretion
633of sweat over the whole surface of the body, and at times this
secretion is extremely profuse.
In association with these symptoms we often see the hyperaemic
processes in the skin known by the names of erythema and roseola,
taking the form of larger or smaller bright red patches, which are
most frequently seen on the sides of the neck, the front of the chest,
and the face.
In many women, at the menstrual periods, when the flow has
become scanty or has already entirely ceased, we observe the occurrence
of eczematous eruptions, which have for this reason received
the distinctive name of climacteric eczema. In the majority of these
cases, the eczema does not make its appearance until the regular
menstrual flux has completely ceased to occur; and in the less common
cases in which the flow persists after the climacteric eczema
has begun, menstruation is rarely regular, but has begun to exhibit
the variability and disorder characteristic of the time of the menopause.
If the eczema comes on after the menopause is completely
established, it usually appears in from six to twelve months after
the cessation of the flow; but in some cases, the eruption appears
very soon after the menopause, whilst in others, its onset may be
delayed for as long as four or five years. Climacteric eczema is obstinate,
and shows no tendency to spontaneous cure. With regard
to the localization of the eruption, Bohn found that in three-fourths
of the cases it affected the hairy scalp and the ears; Rayer and
Hebra also state that the eczema of the menopause is most frequently
seen in these two situations, whilst the next commonest
site for the eruption is the face. As regards other parts of the skin,
it is only that of the extremities that is ever affected by this disease,
especially the hands and the fingers, less often the forearms or the
backs of the feet; it never appears on the trunk. With regard to
the types of eczema occurring in connexion with the menopause, we
see almost exclusively the squamous and the weeping forms of the
disease.
In general, at the climacteric period, the skin is extremely sensitive,
and devoid of powers of resistance to outward noxious influences.
Alternations of dampness and dryness or of heat and cold
readily give rise to redness, infiltration, and the formation of scales
and fissures of the skin; sometimes this occurs merely after cold
ablutions. These acute stages of swelling, redness, and vesiculation
of the skin, readily pass on into chronic and obstinate dermatitis.
Not infrequently, during the climacteric, as during the menarche,
inflammation of the sebaceous glands occurs, acne, at times accompanied
by seborrhœic manifestations. In other cases, we see disfigurations
of the face in consequence of vascular dilatations, especially
on the nose and on the adjoining portions of the cheeks,
634rosacea, in which disease also there is associated inflammation of the
sebaceous glands. Another disorder of the skin of the face which
is greatly dreaded by women at this time of life, owing to the unsightly
appearance it produces, is the development of sinuous dilatations
of some of the superficial vessels, at times associated with
connective tissue proliferation in the form of red or violet-coloured
painless nodules.
An extremely distressing affection, and one which is especially
apt to attack women during the change of life, is the previously
mentioned pruritus genitalium. The itching is in some cases confined
to the external genital organs, whilst in others it extends into
the interior of the vagina; also it may pass backwards over the
perineum, and on into the gluteal folds. In some cases, some local
pathological condition will be found to account for the disorder:
catarrh of the vagina or of the cervix uteri; displacements, inflammations,
or new-growths of the uterus; anomalies of the ovary, the
bladder, or the urethra. Cohnstein draws attention to a circular
hyperplasia of the vaginal portion of the cervix, occurring during
the menopause, and, “owing to the vascular dilation by which it is
characterized, possessing close analogies with haemorrhoids;” the
worst symptom of this affection is pruritus. That in these cases
the pruritus is actually dependent upon the “haemorrhoidal
hyperplasia” of the portio vaginalis, Cohnstein considers to be
proved by the fact that, whilst local applications give no more than
momentary relief to the itching, this symptom is completely relieved
by the abstraction of blood from the cervix. But in addition to such
cases as these, we have from time to time to deal with patients suffering
from violent genital pruritus during the climacteric period, in
whom we shall vainly seek for any local pathological changes, to
the cure of which our therapeutic zeal may be directed. Analogy
with some other disorders of the climacteric leads us to conclude
that in these cases also we have to do with an idiopathic neurosis
(Boerner).
The frequent recurrence of pruritus vulvae leads ultimately to the
formation of nodules and papular eruptions.
Many authors state that they have observed the frequent occurrence
of erysipelas during the climacteric period; others assert that
furunculosis, prurigo, urticaria, and herpes zoster, are seen with
especial frequency at this period of life.
Tilt, in his 500 cases of women at the climacteric age, made the
following observations:
201, or 40.2%, suffered from heats and tendency to perspiration.
2, or 0.4%, suffered from monthly recurrence of periods of perspiration.
63584, or 16.8%, suffered from profuse perspirations.
13, or 2.6%, suffered from cold sweats.
14, or 2.8%, suffered from dry heats (dry flushes).
186, or 37.2%, remained free from such attacks of heat or perspiration.
Krieger gives as an example of the “occurrence of new troubles”
at the change of life, furunculosis; so also does Boerner. “The discolouration
of the face, occurring usually in connexion with pregnancy
or with diseases of the reproductive organs, and known as
chloasma uterinum,” has been seen by Cohnstein, during the climacteric
period, “chiefly in cases in which, owing to some degree of
failure of general nutrition, the skin has been thrown into folds.”
Wilson regarded prurigo and eczema as the commonest skin-diseases
of the climacteric period; whilst Boerner draws attention to a
connexion between climacteric conditions and the outbreak of
herpes zoster.
Disorders of Metabolism.
Among the disorders of metabolism to which women are especially
prone at the climacteric period, we must in the first place
allude to obesity (lipomatosis universalis), and to gout (arthritis
urica).
Numerous observations have shown us that the time of the change
of life, the period between the ages of 40 and 50 years, is the one
especially favourable in women to the extensive deposit of fat in
the tissues.
In 200 cases of great obesity (lipomatosis universalis) in women,
in which I instituted enquiries regarding the age at which an excessive
deposit of fat in the tissues had first been noticed, I obtained
the following results:
| In early childhood in |
19 cases |
| At the age between 15 and 20 years in |
30 cases |
| At the age between 20 and 30 years in |
45 cases |
| At the age between 30 and 40 years in |
52 cases |
| At the age between 40 and 50 years in |
54 cases |
| At ages over 50 years |
0 cases |
We learn from these figures that it is between the ages of 40 and
50 years that there is the greatest tendency in women for the accumulation
of fat; but that as early as between the ages of 30 and 40
years this accumulation may in many instances begin. Speaking
generally, there is in women an obvious connexion between the development
of obesity and the state of the reproductive functions,
inasmuch as at puberty, during the puerperium, and above all at
the climacteric, there is a special tendency to the accumulation of
fat in the subcutaneous tissues. At the commencement of the menopause,
636it is more especially in the abdominal wall, the breasts, and
the buttocks, that we witness the deposit of fat. In the abdomen,
owing to the thickening of the subcutaneous tissues and of the great
peritoneal folds—especially of the great omentum—a marked protrusion
occurs, whilst the umbilicus becomes more deeply hollowed,
and ultimately funnel-shaped. In some instances, the deposit of fat
around the navel favours the occurrence of umbilical hernia. After
an artificial menopause, induced by oöphorectomy, it has also been
noticed in from 42 to 52% of the cases that a marked general deposit
of fat has occurred, affecting especially the breasts and the buttocks.
This obesity in climacteric women, not only impairs to a serious
extent their good looks, but brings in its train a number of troubles,
and gives rise to manifold morbid manifestations, and among these,
changes in the heart, which may readily threaten the patient’s life.
In consequence of extensive fatty deposits in the myocardium, associated
with actual fatty degeneration of the muscular fibres, cardiac
insufficiency ensues, with all its distressing and disastrous consequences.
It is further necessary to insist upon the fact that obesity
during the climacteric very definitely favours the occurrence of
menorrhagia.
On examining 282 women, 5 years after the complete cessation of
the menstrual flow, Tilt found that
| 121 |
had become stouter than before, |
| 71 |
were unchanged in this respect, and that |
| 90 |
were thinner than formerly. |
Alike in the third class and in the first were a very large proportion
of women in whom the change of life had entailed much
illness and suffering; but in the first class, the women who had
been thus affected had at that time lost weight, and only in the
latter half of the climacteric period, when their troubles had become
less severe, had the condition of embonpoint made its appearance.
Passing now to the consideration of arthritis urica in women at
the climacteric, it is worthy of mention that Hippocrates was so
much struck by the association that he went so far as to deny that
gout occurred at all in women before the menopause. The fact of
the matter is that whilst women are in general less disposed than
men to the occurrence of gout, the tendency of women to this
disease during the climacteric period is so marked, that at this epoch
of life the disease is far more common in women than it is in men
of corresponding age.
It is in obese women, with a soft, white, and lax integument, with
a pallid, somewhat bloated countenance, a poorly developed muscular
system, extensive varicosities of the veins of the legs, marked
637dyspeptic troubles, and habitual constipation, that during the preclimacteric
and climacteric periods, gout is especially apt to make its
appearance. It is then characterized by the following symptoms.
From time to time the woman suffers from tearing or shooting
pains in the joints, lasting at first a short time only, and returning
after longer or shorter intervals. With the frequent return of the
pains, the affected joints become swollen; and finally the patient
suffers from the characteristic attacks of acute gouty arthritis, with
the well-known consecutive symptoms of this affection.
According to the observations of Geist, during the climacteric
period, 28 women suffer from gout as compared with 4 men of corresponding
age. Tilt publishes the following figures showing the
mortality of women from gout in England:
| At ages from 20 to 30 years |
56 women |
| At ages from 30 to 40 years |
121 women |
| At ages from 40 to 50 years |
291 women |
| |
| At ages from 50 to 60 years |
152 women |
| At ages from 60 to 70 years |
104 women |
Regarding diabetes mellitus during the menopause, Lawson Tait,
who maintained there was a distinct form of climacteric diabetes,
asserted that this disorder of metabolism was less severe, and runs
a longer course during the climacteric period than at other times
of life.
Diseases of the Nervous System.
The disturbances of the nervous system that occur during the
climacteric period, manifest themselves chiefly in the form of
hyperaesthesia and hyperkinesia. The sensory nerves appear to
me for the most part to be more irritable than normal, inasmuch as
every stimulus by which they are affected arouses a comparatively
greater sensation, and gives rise to an excessive reaction in the
sphere of consciousness. The cutaneous hyperaesthesia of climacteric
women is shown in very various ways, the commonest being
the anomaly of sensation which gives rise to the symptom known
as pruritus, characterized by paroxysms of itching in more or
less extensive areas of skin, with consecutive nutritive changes in
the affected portions of the integument. The commonest and the
most distressing form of this disorder during the menopause is
pruritus vulvae.
In addition to such manifestations of cutaneous hyperaesthesia,
vasomotor disturbances of the skin are of frequent occurrence,
characterized by redness, rise of temperature, and sometimes the
formation of nodules in the affected areas. Almost without exception,
at the outset of the climacteric period, and sometimes also
638in the preclimacteric epoch, women complain of a very distressing
feeling of fugitive heat in various portions of the surface of the
body, manifested objectively by the rapid appearance and no less
rapid subsidence of a red colouration of the skin of the face, the
neck, and the chest. Such fugitive heats are due to disturbances of
vasomotor innervation giving rise to sudden variations in the
amount of blood passing through the vessels of the affected areas
of skin.
Hardly less frequent during the climacteric are the sensations of
imaginary movement which give rise to the subjective symptom
known as vertigo. Often in women at this time of life it occurs
quite without apparent cause, but in other cases on the performance
of some unusual movement or the adoption of some unusual posture;
there is a sudden perception of rotatory movement, either of the
patient’s own body or else of her visible and palpable environment.
With this feeling of disturbed equilibrium, there is often associated
optical and auditory hyperaesthesia, flickering before the eyes
(muscae volitantes), tinnitus aurium, painful sensations in the head
and more especially in the occipital region, nausea, vomiting, sense
of anxiety, cold sweats, muscular twitchings, alternating redness
and pallor of the face, and coldness of the feet. The vertigo occurs
in paroxysms, usually of short duration, varying from one to fifteen
minutes. It is especially in plethoric and obese women that climacteric
vertigo occurs.
A peculiar form of this climacteric vertigo is that described by
Tilt under the name of “Pseudo-Narcotism” of climacteric women,
characterized by a sense of swimming movements, uncertainty in
the gait, vacancy of expression, a confused look in the eyes like
those of a drunken person, and a kind of mental stupor which the
patient cannot shake off without considerable effort. The women
thus affected state that they feel as if they had had too much to
drink, as if something had gone to their heads; indeed their great
fear is that they will be supposed to be intoxicated by those who
see them walking in the streets; they feel even that they must refuse
to receive the visits of their acquaintances if they wish to preserve
their reputation for sobriety. They suffer also from great
drowsiness, from a disagreeable sense of weight or pressure in the
head, from a feeling “as if the brain was clouded, or needed to
have some cobwebs swept away.” They feel a disinclination to
both mental and physical exertion, and their memory and all other
intellectual powers are impaired.
Boerner maintains that the attacks of vertigo so frequently occurring
at the menopause are in a minority of cases only dependent
upon hyperaemic states (arising from the cessation of the menstrual
flow); on the contrary, he believes that the cause more often lies
639in hysteria, in chronic disorder of the digestive tract, or, finally, in
anæmia. In his opinion, vertiginous attacks dependent upon cerebral
anæmia are very common indeed during the climacteric period,
and even for a long time afterwards; and he believes that their
nature is often completely misinterpreted.
Another very unpleasant indication of disordered nervous function
during the climacteric period is the sleeplessness that is so
common at this time of life. Women who during the day time feel
comparatively well, suffer at night, sometimes periodically at exactly
the same hour night after night, from a state of general restlessness,
and for this reason are unable to obtain the sleep for which they
long. They throw themselves uneasily from side to side of the
bed, or wander restlessly about the room, and before long, owing to
this want of sufficient repose, become greatly depressed.
Among the neuroses of the sensory apparatus, the various kinds
of cutaneous neuralgia are less common than during the menarche
and the menacme; but on the other hand, in my personal experience
at any rate, the visceral neuralgias are commoner, more especially
cardialgia and hypogastric neuralgia. Of the superficial neuralgias,
hemicrania and intercostal neuralgia are those which occur most
often during the climacteric period.
During the change of life, hemicrania most commonly occurs in
typical association with menstruation; or, if the flow has already
ceased, the attacks of hemicrania recur at what should be the
menstrual periods. This affection is characterized by the paroxysmal
occurrence of a severe boring pain in the side of the head, more
often the left side than the right, affecting the temporal, the parietal,
or the occipital region, or the entire side of the calvaria at once,
usually accompanied with redness and local rise of temperature of
the painful part; the duration of the paroxysms varies in different
cases from one or two to many hours; with the pain are associated
chilliness, nausea, exhaustion, and a severe feeling of general
malaise.
Of the intercostal neuralgias, one form deserves especial mention
in this connexion: I refer to mastodynia, which is both physically
and mentally one of the most distressing affections to which women
are subject during the climacteric period. For a middle-aged
woman suffering from mastodynia—the “irritable breast” of
Cooper—almost invariably feels assured that these pains localized
in the breast and its immediate vicinity are indications of a commencing
cancer of the breast; and it is an exceedingly difficult
matter, in most cases, to convince her that her fears are without
foundation. In this manner, partly in consequence of the directly
depressing effect of the pains, which are commonly intensely severe,
and partly owing to the disturbance of mind produced by the belief
640that an incurably fatal disorder has begun, I have in several instances
seen cases of profound melancholia originate.
According to Windscheid, among the enduring painful sensations
of the climacteric period, pains in the lower extremities are of somewhat
frequent occurrence. Day after day the patient suffers from
distressing tearing or lancinating sensations in the legs; the trouble
is insusceptible of more exact description, but is none the less a
very severe one. In addition to the lower extremities, the back, the
spinal column, and more particularly the lumbo-sacral region, are
often the seats of incessant pain. In the thoracic region of the
back, the pain is usually diffuse; when confined to the spinal column,
however, it is commonly limited to individual vertebrae, the spinous
processes of those affected being also sensitive to pressure. The
sacral pains may in some cases predominate to such an extent, that
it is on this ground alone that the patient comes to seek medical
advice. The sacrache is equally severe when the patient is standing,
sitting, or recumbent; it often radiates into the lower extremities.
Boerner draws attention to the fact that in many cases the
pains in the sacrum or higher up in the back may be due to excessive
tension of the abdominal parietes in consequence of the great
accumulation of fat. Among motor manifestations, Windscheid
draws especial attention to a certain degree of weakening of the
muscles of the lower extremities. Although on examination no
abnormality can be detected, fatigue and functional incapacity,
more especially in the lower extremities, ensue in a manner altogether
disproportionate to the exertion, so that the patient is most
unwilling to take even a short walk, to go upstairs, etc. In pronounced
cases, the patient will never go out walking without carrying
a campstool, so that she can sit down to rest directly she begins
to feel fatigued. In association with these disorders of motility we
most commonly see the above-mentioned painful sensations in the
legs, and by these latter the functional incapacity of the lower
limbs is of course increased. Weakness of the arms is far less
frequently observed; but occasionally we hear complaints that on
the performance of domestic duties, needlework, etc., which previously
could be carried out quite easily, the arms and hands are
now speedily fatigued, and rendered functionally incapable.
Of the visceral neuralgias, cardialgia is by no means rare during
the climacteric period; the pain is concentrated in the epigastric
region, but not infrequently radiates to the back and to the chest.
Hypogastric neuralgia is also not uncommon, pain in the lower part
of the abdomen, associated with a sense of pressure in the bladder,
the uterus, and the rectum, and sometimes radiating to the thighs
and to the region of the haemorrhoidal nerves.
The opinion expressed by several authorities, that the menopause
641favours the occurrence of cerebral apoplexy, must, according to
Windscheid, be received with caution; we have to remember that
with advancing years atheromatous changes are apt to occur in the
cerebral arteries, and it is to these changes, altogether independently
of the climacteric, that cerebral haemorrhage is due. It
appears, however, to be a fact that the menopause favours the onset
of progressive paralysis. According to Jung, 60%, and according
to von Krafft-Ebing, 27%, of women affected with paralysis were
first affected in this way during the climacteric period. Von Krafft-Ebing
explains this occurrence by the fact that during the menopause
fluxions of vasomotor origin are common, and these serve
as the starting point of transudative processes.
Among the neuropathic manifestations of the climacteric period
we must reckon the at times excessive increase of the sexual
impulse. We have already insisted upon the fact that the sexual
impulse is not normally extinguished in women at the time of the
cessation of menstruation; on the contrary, sexual desire commonly
persists long after the menopause, and on this fact is largely dependent
the frequency with which elderly women espouse quite
young men. But in some cases, the sexual impulse is enormously
enhanced during the climacteric period, and the patient experiences
paroxysms of intense voluptuous sensation, associated with manifestations
of abnormal reflex and psychical reaction, with increased
frequency of the pulse and the respiration, emotional excitement,
it may be loss of consciousness, and even general convulsions.
Some of these cases of disordered sexuality occur in those previously
affected with pruritus vulvae et vaginae.
More particularly Guenceau de Mussy and Boerner have described
cases of such excessive libido sexualis during the climacteric
period, voluptuous crises with pollutions, occurring independently
of any external cause; the women thus affected have a continued
succession of erotic ideas, they experience an itching and burning
sensation in the genital organs, and from time to time this culminates
in a paroxysm of sexual feeling, with orgasm, and increased
secretion from the glands of the vulva.
Boerner has observed that characteristic variations in the libido
sexualis commonly occur at the climacteric period. Not infrequently
at this time the sexual desire becomes greatly diminished
in intensity, or even entirely disappears; more often, however, the
desire persists throughout this epoch; finally, in many instances,
the desire undergoes an increase, at times to a degree amounting
to positive torment. The first of these changes, the decline in the
intensity of the sexual desire, harmonising as it does with the
general extinction of the sexual functions at the change of life,
642might have been expected to be the normal occurrence. And it is
a fact that in many cases characterized by an increase of libido
sexualis at the climacteric epoch, Boerner found that there existed
anatomical abnormalities in the reproductive organs (fibromata,
flexions, etc.). Be this as it may, an increase in the intensity
of sexual desire, as long as that increase is not altogether
excessive, may be regarded as one manifestation of the visceral
hyperaesthesias so general at this time of life. In the excessive
degrees of this affection, however, those in which at times the
sexual crisis is associated with general convulsions, we must, with
Romberg, recognize the existence of a direct neuralgic state of the
spermatic plexus. It is especially before the commencement of an
actual menstrual period, or before a due period which fails to
occur, that during the critical years complaint is made of this state
of excessive sexual desire and sensibility; and in many instances
the trouble begins at the very first appearance of the menstrual
irregularities which foreshadow the menopause.
Windscheid draws attention to the fact that occasionally the
nervous manifestations may make their appearance prior to the
occurrence of any menstrual irregularity, so that it is by the nervous
disturbance that the woman or her physician is warned of the
approach of the menopause. “When the menstrual anomalies
begin,” continues Windscheid, “that is to say, at the commencement
of the climacteric, the nervous troubles may have already
attained their maximum and have begun to decline in intensity.
As a general rule, however, the appearance of the nervous disturbances
coincides with the commencement of the menstrual irregularities.
It may happen that these disturbances are intensified
with each recurring period, but this is not the rule. Sometimes,
however, we may observe that when menstruation occurs with excessive
frequency—a by no means rare phenomenon at the
outset of the climacteric—the nervous disturbances become more
severe; and especially is this the case when the unduly frequent
flow is also abnormally profuse, as indeed often happens.” The
manifestations of climacteric neurosis occur, as Windscheid rightly
insists, most frequently in the sphere of the psyche. “We observe
a change in the disposition, which usually becomes more excitable.
A woman previously calm and composed becomes irritable, inclined
to emotional disturbance and to fits of temper, and unable
to bear with equanimity the pinpricks so frequent in daily life, and
especially in the daily life of a housewife. In other cases, however,
the disturbance of the psyche is rather in the direction of depression:
we observe a kind of spiritual inhibition, a deficiency of vital
energy, an indifference to things which formerly gave pleasure.
643Almost always, also, complaints of loss of memory are among the
indications of such depression. To these intellectual anomalies
are superadded disturbances of sensibility. There is excessive
sensitiveness to bright lights, loud noises, and strong odours. Frequently,
also, in such cases, we see great intolerance to alcohol,
quite small doses giving rise to extremely disagreeable sensations in
the head.”
Climacteric Psychoses.
The powerful influence which the changes occurring at the
climacteric period has in the origination of psychoses, has long
been recognized, the menopause, in fact, being a favourable soil
for the cultivation of mental disease. The fact is embodied in
medical terminology, since many authors speak of “climacteric insanity,”
assuming that the psychoses of this period of life present
a definite and characteristic clinical picture.
In an earlier part of this work it was shown that the process
of menstruation has generally a marked effect upon the psyche,
and that disturbances of menstrual activity are competent to exercise
a pathogenic influence upon the mental condition of the woman
who suffers from them; still greater and more intense is the influence
of the cessation of menstrual activity, with its powerful and
widespread disturbance of the entire organism, with its destructive
oscillations of equilibrium in the spheres of sensation, perception,
ideation, and volition. It is easy to understand how the rarer recurrence
of menstruation, the occasional profuse losses of blood,
the complete suppression of menstruation, the conditions peculiar
to the climacteric period of stasis and congestive hyperaemia of the
brain, are competent, more especially in hereditarily predisposed
persons, to give rise to the development of psychoses; whilst in
those already suffering from mental disorder, the menopause will
be likely to bring about an aggravation in their symptoms. At this
time of life, also, we have to take into account the effect of certain
ideational influences to which allusion has already been made, the
thought that womanhood and its joys are passing away for ever,
and the fear of the dangers attendant upon this critical period of
the change of life. A French proverb alludes to “le diable de
quarante ans, si habille à tourmenter les femmes.”
Mental disorder will be more likely to ensue at the climacteric
period in those women whose nervous systems have always been
unduly irritable, and in those affected with hereditary predisposition
to insanity. Further, it is more likely to occur in those in whom
the menopause takes place quite suddenly, in a catastrophic manner,
than in those in whom the climacteric proceeds gradually, and
644unaccompanied by any stormy manifestations in the organism at
large.
It is not in my opinion possible to recognize any specific form
of mental disorder peculiar to the climacteric period, but nevertheless
the psychoses occurring at this time of life do exhibit certain
striking and characteristic features, more especially in this respect,
that states of mental depression with melancholia predominate,
whilst erotic influences are manifest in their etiology. In the
slighter forms, volition and ideation are unaffected, and the trouble
manifests itself in the form of hypochondriacal moods, associated
with bodily troubles. In more severe cases we see emotional depression,
states of anxiety, limitation of the powers of conception
and judgment, indecisiveness, low-spiritedness, and apathy; or on
the other hand, restlessness, an inclination to continued moving
about, the eager pursuit of continually varying occupations, loquacity,
etc.; finally, if the mental disorder becomes still more
severe, hallucinations, delirium, paroxysms of intense excitement,
and in exceptional instances, fully developed mania.
As with regard to the other disorders attending the climacteric,
so also in respect of the climacteric psychoses, women who have
been or are married, who have had a reasonable number of children,
and have been accustomed to a sufficiency of sexual activity, are
more favourably situated, are far more immune, than women whose
sexual circumstances have been the opposite of those mentioned,
who have had one or two children only, who have indulged in
intercourse only when protected from pregnancy by the use of
preventive measures, or have remained sexually unsatisfied, and,
finally, women who have never married, and those who for many
years prior to the commencement of the menopause have lived in
chaste widowhood. In “old maids,” to the somatic effects of
sexual abstinence (or in some cases of abnormal sexual gratification),
are superadded the effects of the intellectual and emotional
recognition of a wasted life. Again, it by no means rarely comes
under our observation that women who in youth, at the time of the
menarche, suffered from psychical disturbances, are apt once again
to be affected with transitory mental disorder at the change of life.
Once, however, the menopause is completely at an end, a condition
of mental quiescence is as a rule established, and then it may happen
that previously existent mental disorders undergo amelioration;
but on the other hand we have in all cases to reckon with the possibility
that they may take an unfavourable turn in the direction
of the development of senile psychoses.
Of considerable interest is the fact, first pointed out by Glaevecke,
and subsequently confirmed by other observers, that in cases of
artificial menopause, melancholic mental disturbances not infrequently
645follow the operation, in some instances so severe as to lead
to weariness of life and actual suicide; and in general, after the
artificial induction of the menopause, psychical disturbances are by
no means rare, and are sometimes very severe. Such disturbance
of the mental balance is seen after oöphorectomy especially
in women who are still comparatively young, and whose sexual
powers are still in a ripe state; whereas when the operation is performed
in women of a more advanced age, whose ovaries were
already nearly or completely functionless, no psychopathic changes
are likely to ensue. In women belonging to the former category,
the same etiological influences come into operation as in the
physiological menopause, the patient, that is, is affected by the
psychical influences of the removal of the ovaries—not only by
the cessation of menstruation and the disappearance of the internal
secretion of the reproductive glands, leading to a disturbance of
the physical equilibrium, but also by the intellectual recognition of
the loss of sexual potency, and a consequent disturbance of the
mental balance.
In Schlager’s opinion the climacteric has a potent influence in
promoting the development of psychical disturbances in women,
even when the involution occurs at the normal age. The course of
these disturbances is as follows: soon after the commencement of
the process of involution, when for a few months already the menstrual
periodicity has been irregular, or the flow has been unduly
profuse, a change of disposition makes its appearance, at first
hardly noticeable, but after a little time manifesting itself clearly
in the form of an increase in irritability. The woman finds fault
with everything and everybody, becomes mistrustful, suspicious,
full of complaints, imagines that the most insignificant annoyances
are due to intentional slights; at the same time she complains of
continued sleeplessness, palpitation, various indescribable sensations,
and of headache. Occasionally, congestions of the head occur,
with alarming dreams, and the moodiness may increase greatly; in
this condition three such patients of Schlager’s were impelled to
attempts at suicide. Schlager further draws attention to the fact
that in 22 cases known to him in which suicide was performed or
unsuccessfully attempted by women, in eleven of these the patient
was at the climacteric age. He believes that the most important
etiological influence in the production of climacteric mental disorder
in such cases is the sudden suppression of menstruation. In the
majority of these instances, the mental disorder takes the form of
mania; exceptionally, however, the form of chorea or of catalepsy.
By Tilt the following forms of “climacteric insanity” are distinguished:
delirium, mania, hypochondriasis, melancholia, impulsive
insanity, and perversion of the moral instincts. The same
646author publishes the following table showing the age incidence in
1,320 cases of mental disorder in women, from which it appears
that during the age of the menopause, a very considerable number
of the cases originate, but that after the change of life comparatively
few cases occur.
In these 1,320 cases the women were:
| Under 15 years of age in |
9 instances |
| Over 15 and under 20 years in |
61 instances |
| Over 20 and under 25 years in |
216 instances |
| Over 25 and under 30 years in |
223 instances |
| Over 30 and under 35 years in |
217 instances |
| Over 35 and under 40 years in |
218 instances |
| Over 40 and under 45 years in |
162 instances |
| Over 45 and under 50 years in |
153 instances |
| Over 50 and under 55 years in |
122 instances |
| Over 55 and under 60 years in |
57 instances |
| Over 60 and under 65 years in |
55 instances |
| Over 65 and under 70 years in |
27 instances |
Fuchs tabulated the ages of 26.300 insane persons. Reducing his
results to the ratios per 10,000, he obtained the following results:
|
Women. |
Men. |
| At ages under 20 |
563 |
649 |
| At ages over 20 and under 30 |
1,895 |
2,132 |
| At ages over 30 and under 40 |
2,557 |
2,614 |
| At ages over 40 and under 50 |
2,180 |
2,080 |
| At ages over 50 and under 60 |
1,362 |
1,247 |
| At ages over 60 |
1,443 |
1,278 |
According to Esquirol, among 198 women who committed
suicide, there were 77 between the ages of 40 and 50 years—a
number considerably larger than those in any other age-decade.
Among 235 women suffering from dementia, a moiety had first
come under treatment during the climacteric age. The same
author published the following data regarding the age-incidence of
insanity in the case of 6.713 female patients:
| At ages under 20 years |
348 cases |
| Between the ages of 20 and 25 |
563 cases |
| Between the ages of 25 and 30 |
727 cases |
| Between the ages of 30 and 40 |
1,607 cases |
| Between the ages of 40 and 50 |
1,479 cases |
| Between the ages of 50 and 60 |
954 cases |
| At ages above 60 years |
1,035 cases |
Matusch found that among 551 women suffering from mental
disorder, there were:
| At ages 0 to 10 years |
9 cases |
| At ages 10 to 20 years |
73 cases |
| At ages 20 to 30 years |
140 cases |
| At ages 30 to 40 years |
114 cases |
| At ages 40 to 50 years |
107 cases |
| At ages over 50 years |
38 cases |
647According to von Krafft-Ebing, among 858 insane women, there
were about 60 in whom the disorder of the mind appeared to depend
upon the influence of the climacteric, and in 25 of these there
was hereditary predisposition to mental disease.
From Kowalewski’s interesting work on the psychoses of the
climacteric, we quote the following:
“In women, the climacteric has a distinct influence upon the mental
life, and that influence is strongly manifested more especially
in cases in which during the age of puberty mental disturbance had
previously been noticed. The mental condition in which women
approach the change of life is a very variable one, and it is one
largely dependent upon the circumstances in which the active years
of the sexual life have been passed. In some cases, a woman has
been so fortunate as to marry early and from affection, and her
whole married life has been passed without disturbance; her labours
have not been exhausting, and her children have enjoyed good
health; all have passed through the years of childhood without
untoward incident, and their development has been a happy and successful
one; in a word—everything has gone well with her and
hers. Such a woman will give thanks to God for the rare felicity
she has enjoyed; and quietly, patiently, and with understanding
will endure the inevitable end of her sexual life. For such a
woman, more especially if she comes of a healthy stock, the changes
which occur in her reproductive organs at the epoch of the climacteric,
need not entail any serious shock to her nervous system, nor
need they form the culture ground for morbid manifestations in
her nervous system or in her mind. Even if any anomalies in
nervous working should occur, it will be such only as are aroused
by the disturbance of the normal menstrual rhythm; in such cases,
they will rarely prove of a serious or enduring character.
“But look, on the other hand, upon this picture. A woman has
married without affection and from pure necessity. Her husband
has been a drunkard, and rough and unfaithful. She has
had a great many children, her labours have been tedious and difficult
and accompanied with severe losses of blood. Some of the children
fell sick and died; those that survived proved idle, good-fornothing,
and a burthen. The family life is dominated by quarrelsomeness,
disorder, and insufficiency of means. The mother is
affected with some chronic disorder of the reproductive organs,
and is hardly ever out of the doctor’s hands. After 25 or 30 years
of a life of this kind, the woman enters upon the change of life.
Physically exhausted, weary of life, never having known happiness,
after an existence full of trouble and wretchedness, with
nothing joyful either in her memories of the past or in her prospect
of the future—the chief hope of such a woman is that her troubles
648may soon end with her life. Where the soil is thus physically and
mentally exhausted, the development of a neurosis or a psychosis
is only too probable on the most trifling exciting cause. Her life
seems of so little worth, that thoughts of suicide are likely to be
very near at hand. Thus, when the climacteric alterations in the
reproductive organs are superadded, melancholia is very likely to
supervene. When, however, the case is complicated by hereditary
predisposition to insanity, and by the occurrence of actual degenerative
changes in the central nervous system, instead of the passive
depression of melancholia, we shall rather see the ideas of persecution
of paranoia. As an actual fact, these two psychoses, melancholia
and paranoia, are the commonest forms of mental disorder
at this period of a woman’s life.
“These are the two extremes in woman’s mental state at the
time when the physical changes of the climacteric period begin in
her reproductive organs. It will, of course, be readily understood
that between these two extremes lies a series of combinations any
one of which may in individual cases occur.
“The conditions of life during earlier years have thus a strong
determinative influence in the production of mental disorder; and
not infrequently in these conditions alone shall we find the efficient
cause of the mental degeneration. At times, the memories of her
own life have in a woman at the climacteric age so serious an
effect, that these memories alone constitute the causal agent of the
development of a psychosis, or at least so influence the soil as to
make it a suitable culture-ground for the development of mental
disorder, the actual exciting cause of the pathological state being a
disturbance of the ordinary menstrual rhythm.
“In considering the mental condition of women at the outset of
the climacteric period, we must not forget those who are called
‘old maids.’ In their youth these maidens also have had their
ideals, their hopes, their plans, and their sorrows. They also had a
natural impulse to love and to be loved in return; they hoped to become
wives and mothers. But life has failed to fulfil their hopes and
their wishes, and their longings have remained unsatisfied. Some
of them have taken up their cross without murmuring, and have
devoted their talents, their intelligence, and their love to the service
of those nearest to them. But others make an active protest
against fate in the form of vindictive feelings towards their environment,
of quarrelsomeness, scandal-mongering, etc. Here we
see contrasted the two principal types of such women. On the one
hand are those who devote their intellectual and spiritual powers
to the service of society; these are unselfish sisters-of-mercy,
untiring medical women, invaluable school-teachers and governesses,
649fanatical political agents, etc. Such as these have ceased to
live for themselves. In the fullest sense of the words, they mortify
the flesh, and guide their conduct by lofty moral principles. They
have killed their sexual life, and they remain for ever virgins—both
morally and physically. If, owing to a pathological inheritance,
faulty conditions of life, exhausting illnesses, etc., a psychosis
develops, the hallucinations and delusions from which they suffer
very rarely assume a sexual character, nor are they of a degrading
type. The sexual side of life seems, in fact, be they sane or insane,
to have undergone complete atrophy. They suffer from simple
melancholia with stupor, or their insanity takes a religious turn,
but very rarely indeed has it an erotic character.
“Very different is it with old maids of the second type. They
are dissatisfied with life, irritable, quarrelsome, envious, and malicious.
They are spiteful and revengeful, gossips and scandalmongers,
boast of their own chaste and innocent lives, and never
forgive any real or imaginary attempt upon their spotless virtue.
At the same time they never lose hope for the future, and are full
of imaginary love-affairs, in which they pass through scenes by
no means chaste or innocent; they do not shrink from self-abuse
and the abnormal gratification of the sexual needs, in which the
lacking partner in the sexual act is supplied by the imagination.
Under the influence of such abnormal conditions of life, these
women frequently become affected by nervous disorders; migraine,
neuralgia, cephalalgia, nervous depression, rachialgia, debility,
anæmia, diseases of the reproductive organs, etc. Thus, when
they enter the climacteric age, the soil is fully prepared for the
development of mental disorder, which in such individuals is often
characterized by hallucinations of sexual sensation and perception,
erotic visual and auditory hallucinations, delusions of similar character,
increased sexual irritability, a search for abnormal means
of sexual gratification, a propensity to obscene speech and conduct,
etc.
“Mental disorder is so common during the climacteric period,
that the term ‘climacteric insanity’ has now become established
in the literature of mental alienation. In almost all the textbooks
of the subject we find an allusion to this form of mental disease,
but there is no real ground for Maudsley’s assumption
that there is a climacteric insanity sui generis. At the climacteric,
very various forms of mental disorder may occur—paranoia,
melancholia, and mania; the only common feature in the attacks,
owing to which they are classed as ‘climacteric insanity’ being
the fact that the final determining cause in each case is the onset of
the change of life. In fact, this period is not without influence
650upon the manifestation of the disease—its stamp is imprinted upon
the clinical picture, it endues the disease with certain characteristic
features—but still, the peculiarities common to the cases of mental
disorder occurring at this time of life in women are not so great
as to justify us in describing them as a separate variety of psychosis.”
According to Kowalewski, this so-called climacteric insanity is
met with in two principal forms: in many cases the mental disorder
recurs in periodic paroxysms, associated either with the commencement
of the menstrual flow, or having the periodicity of
menstruation after the flow has already ceased to appear; in the
other class of cases the psychosis has no direct connexion with
menstruation, and is dependent upon the joint influence of all the
manifestations of the climacteric period. Cases belonging to the
former class have been distinguished by Bartel as “climacteric
pseudomenstrual insanity.”
The psychoses dependent upon the climacteric influences may,
according to Kowalewski, appear in almost all the known forms
of mental disorder: precordial anxiety, melancholia, mania, amentia,
paranoia, etc.; and although they exhibit no features which are
absolutely characteristic, or which, as already said, enable us to
distinguish a specific “climacteric insanity,” yet they all bear a
common imprint by means of which we are enabled to detect in
their causation the influence of this critical period of life. Thus,
precordial anxiety occurs in paroxysms having a more or less regular
periodicity, corresponding with that of the expected menstruation.
The same feature is observable in the periodic exacerbations
of hysterical and epileptic paroxysms. Often, also, there occur at
this time sudden changes in the emotional disposition and in the
character, in one direction or the other, without the development
of actual melancholia or mania. The melancholia of the climacteric
period occurs chiefly in married women, more especially in those
whose circumstances are unhappy; and it is often manifested by
attempts at suicide.
Mania is comparatively rare at the climacteric period; when it
does occur, it commonly assumes a sexual form—sexual impulses,
hallucinations, and delusions, and obscene conduct. Such manifestations
are seen most often in widows, in “old maids” whose
morals are not above reproach, and, speaking generally, in those
whose sexual needs have remained partially or completely ungratified,
and in those who have greatly erred in the conduct of
this side of life. Amentia also occurs at this time of life; rarely
in maniacal form, more frequently in association with menstruation
as a periodic psychosis, or as a continuous disorder of mind with
651exacerbations corresponding to the menstrual periods; it is often
characterized by pronounced eroticism.
Much more frequent during the climacteric period is the occurrence
of paranoia, as Kowalewski rightly insists. It is most often
met with in “old maids” with psychopathic predisposition. The
imagination of such individuals is always concentrated upon men;
they imagine that men in general, but more particularly certain individuals
of the opposite sex, are continually regarding them, making
eyes at them, making signs to them, in some way or other striving
to attract their attention. The most ordinary and invariable forms
of polite intercourse are regarded by these women, whose powers
of observation are morbidly stimulated, as being indications of a
special “attention” paid to themselves. They persecute these men
with their own attentions, and imagine that it is the men who are
persecuting them. Often this morbid mental state is associated
with sexual malpractices, masturbation, etc. Not rarely, such degenerates
are affected with lascivious dreams. Often they experience
hallucinations of sexual perception in the form of supposed
assaults on their virginity. All these states are apt speedily to
develop into a condition of general suspiciousness and ideas of
persecution. The ideas of persecution assume a peculiar form,
one especially characteristic of the climacteric period. The patients
believe that a man, often personally unknown to them, and perhaps
living in another town, enters into spiritual and bodily intercourse
with them. These relations are supposed to be effected in most
cases by means of spiritualism, hypnotism, or electricity. The
patient importunes the man in question with letters, supposes herself
to be legally united with him, and not infrequently wishes to
give him the pleasure of paying her bills and providing her with
money. It is a very common occurrence for a Catholic priest to be
worried by such a woman, her delusion being grounded upon the
fact that the priest is supposed to assume an exceptionally intimate
spiritual relationship with members of his flock. The patient with
ideas of persecution often herself becomes an actual persecutor,
not only pestering her victim with innumerable letters, but in her
jealousy making “scenes” whenever she can encounter him, and
sometimes giving rise to serious scandal. With such a mental state
we often see associated sexual hallucinations and delusions; the
patient believes herself to be pregnant, imagines herself to have
been violated, or to be living in carnal intercourse with a man—some
one, it may be, with whom she is not even acquainted.
Medical men are especially apt to suffer from the accusations of
such women, whom they may have examined in private in entire
ignorance of the patient’s mental condition. Frequently, such ideas
652of sexual persecution are associated with paroxysms of violent
nymphomania, and in this way also the unwary physician may
find himself placed in an extremely unpleasant position. It occasionally
happens in such patients that abnormalities of the sexual
instinct arise, and they begin to feel desire towards individuals of
their own sex.
Such delusions of persecution by means of hypnotism, spiritualism,
the telephone, etc., in association with sexual delusions and
nymphomania, are so frequent during the climacteric period, that
they may be regarded as pre-eminently constituting climacteric insanity.
Frequently some old hysterical state underlies this form
of mental disorder.
Thus these peculiar manifestations of eroticism must be regarded
as the distinctive characteristics of climacteric insanity and more
particularly of climacteric paranoia. A second characteristic of
climacteric insanity is, according to Garat, the marked development
of jealous emotions and delusions.
In addition to these fully developed psychoses, there occur in
degenerates at the climacteric age paroxysms of impulsive insanity
in the form of dipsomania, kleptomania, pyromania; exhibitionism;
irresistible impulse to suicide, homicide, infanticide, etc. Such
paroxysmal impulsive manifestations are, according to Kowalewski,
commonly associated with menstrual disturbances; they occur most
frequently at the due dates of menstruation when the flow fails to
appear.
One hundred and sixty-nine cases of climacteric psychosis were
classified by Matusch as follows:
| Melancholia |
36 cases |
| Mania |
2 cases |
| Melancholia passing on into paranoia |
28 cases |
| Melancholia passing on into secondary dementia |
17 cases |
| Paranoia |
43 cases |
| Neurasthenia during the climacteric period followed by mental disorder |
19 cases |
| Neurasthenia prior to the climacteric period, followed by mental disorder during the climacteric period |
10 cases |
| Apoplexy, cerebral abscess, dementia |
6 cases |
| Epilepsy |
2 cases |
| Alternating insanity |
3 cases |
| Paralytic dementia |
5 cases |
Von Krafft-Ebing classified 60 cases of climacteric psychosis as
follows:
| Melancholia |
4 cases |
| Alternating insanity |
1 case |
| Acute delirium |
1 case |
| Primary insanity: |
|
| a. With primordial delirium |
36 cases |
| b. Paralytic dementia |
12 cases |
653The prognosis in cases of climacteric psychosis is regarded by
Kowalewski as unfavourable; unfavourable vital conditions are
associated with retrogressive metamorphosis of the tissues, hence
mental disorder arising at this time of life is hardly less serious
than that due to actual degeneration of cerebral tissues. Indeed,
according to Schüle there is during the climacteric period an
especial danger of the development of atrophic cerebral processes
(Encephalitis atheromatosa) with apoplectic and epileptic seizures.
Schlager also regards the prognosis of climacteric insanity as unfavourable;
but Merson, on the other hand, observed among women
suffering from climacteric psychoses a recovery rate of over 50%.
On previously existent psychoses in women, the onset of the
climacteric exercises in most cases an unfavourable influence, and
very exceptionally only at this time do we observe the cure or remission
of a chronic mental disorder to occur. Kowalewski has
seen cases of chronic mania in which a cure was obtained at the
climacteric period; a somewhat excessive excitability and inclination
to violence remained, however, as vestiges of the former
insanity. Matusch, keeping under observation 60 women affected
with chronic mental disorder as they attained the climacteric
period, noticed that in 14 instances the mental condition
changed for the worse at this period, whilst in 13 the character
of the mental disease underwent a change, excitement giving
place to apathy and dementia. Griesinger had earlier pointed out
that at the time of the cessation of menstruation there would
occasionally occur amelioration, and even cure, of a previously
existing chronic mental disorder; more often, however, the influence
of the menopause was an unfavourable one, a hitherto changeable
and irritative form of mental disease becoming transformed
into chronic insanity with inalterable delusions, or into dementia.
The course of mental disorder, such as melancholia, first making
its appearance at the climacteric epoch, was also regarded by
Griesinger as likely to be unfavourable.
Hygiene During the Menopause.
During the critical years of a woman’s life it is the aim of
hygiene to employ all the means available to counteract the
changes in the circulation of the blood, the disturbances in the
working of the nervous system, and the nutritive disorders, which
are in various ways dependent upon the changes occurring in the
reproductive organs during the climacteric period; its endeavour
should be so to regulate the conduct of life in this epoch that the
important episode of the gradual decline and ultimate extinction
654of sexual productivity shall be effected with as few local troubles
as possible, and as slight variations in the general condition.
By means of baths of various temperature, duration, mode of
application, and composition, and by other selected hydrotherapeutic
procedures, we are enabled during the disturbances of the menopause
to exert upon the skin a powerful derivative influence, and
in this way to diminish the passive hyperaemia of the uterus and
the uterine annexa; by the same means we can exercise a sedative
influence on the peripheral nerves and thus further upon the entire
nervous system, whenever such measures are called for by the
manifold indications of increased irritability; further, by the use
of baths we can influence the circulation of the blood, we can
increase the sudatory activity of the skin, and in various additional
ways we can affect heat production and metabolism, thus modifying
the processes occurring in the reproductive organs, making the conditions
favourable for the absorption of exudations, and promoting
a healthy tissue-change in the mucous membrane of the genital
passages.
In climacteric women, the most usual indications are for the
employment of water-baths at an indifferent temperature. 35 to
37° C. (95 to 98° F.), of moderate duration, 15 to 20 minutes,
the bath being one of simple immersion, not of douche or affusion,
and the temperature being kept constant by continuous inflow of
a sufficient quantity of hot water. Such baths as these promote in
a mild but continuously efficient manner the functions of the skin—so
important during the climacteric epoch; and they lessen the
almost constant tendency to perspirations and to the development
of diseases of the skin (the commonest of which is climacteric
eczema). The moderate degree of thermic stimulus exercised by
baths at such an indifferent temperature leads them to have an
equable sedative effect upon the nervous system, which is probably
dependent upon an influence exerted through the intermediation
of the sensory nerve-terminals in the skin; and this is most beneficial
in lessening the increased general irritability, both spontaneous
and reflex, so commonly manifested by the nervous system at
the climacteric period. In women at this time of life, such baths
are most useful in allaying the common cutaneous hyperaesthesias
and neuralgias, and have a reflex influence also upon the visceral
neuralgias and psychical hyperaesthesias.
In climacteric women suffering from abnormal sensitiveness to
sensory impressions, to strong light and loud noises, or from painful
sensations in the most diverse nerve areas; in those subject to
palpitation of the heart after some trivial exciting cause; in those
affected with cramp-like seizures in the pharynx, the œsophagus,
655the stomach, and the intestinal tract; in women with distressing
sensations of itching and burning in the reproductive organs, or in
those in whom there is a great increase in the intensity of the
sexual impulse—in all these common disturbances of the menopause,
by the daily use of such immersion baths of water at an
indifferent temperature, best taken immediately before retiring to
rest, we shall often succeed in inducing both local and general
repose, in diminishing the spontaneous and reflex irritability of the
nervous system, and in inducing quiet and restorative sleep.
In other cases of disturbances of health during the climacteric
period, however, more benefit may be derived from hot immersion
baths, taken at a temperature well above blood heat, (37° C.—98.4°
F.) and lasting longer than the warm baths just described.
These are indicated when we wish to increase the activity of the
circulation through the skin, to give rise to hyperaemia of the
superficial structures of the body, to stimulate powerfully the
cutaneous nerves, to promote cutaneous perspiration—in short, to
exercise a powerful derivative effect, to promote resorption, and
to accelerate the general processes of tissue-change. This method
of treatment is suitable for cases in which at the commencement
of the menopause there are already pathological conditions of the
reproductive organs, the morbid states being now aggravated by
the processes of the climacteric—such conditions are metritis and
endometritis, chronic inflammations of the intrapelvic connective
tissue and of the pelvic peritoneum; and one of the first aims of
treatment must be to promote the softening and subsequent absorption
of these inflammatory products. Again, in cases in which the
climacteric troubles, dependent in part on increased general arterial
blood-pressure, manifest themselves chiefly in the form of active
congestions, fugitive heats, vertigo, etc., the employment of hot
baths is likely to be most useful by leading to a notable enlargement
of the cutaneous capillary bloodvessels and consequent lowering
of arterial blood-pressure. Further, in cases of compensatory
fluxes, periodic diarrhoeas, periodic leucorrhoea, following the suppression
of the menstrual flow, in cases of vicarious haemorrhage
(especially periodic epistaxis and periodical haemorrhoidal bleedings),
the use of hot baths is often competent to restore the functional
activity of the ovaries when this has undergone premature
cessation. In addition, their use assists us in our endeavours to
counteract excessive obesity and gouty disorders, diseases which
tend especially to make their appearance in women at the epoch
of the menopause, disorders of metabolism intimately associated
with the disturbances of the uterine and ovarian functions characteristic
of the change of life.
656In all the conditions just enumerated, if we desire a still more
powerful influence than that exerted by ordinary hot baths, it is
in our power to employ hot mineral water baths, by means of
which a chemical, and perhaps also an electrical, stimulation of the
cutaneous nerves is superadded to the simple thermic stimulus
conveyed by the hot water. The different effects of the various
mineral baths depends upon both the saline and the gaseous constituents
of the different springs, and upon the peculiar physical
properties of the mineral waters.
Sudorific baths are of various kinds. Some, Russian baths, consist
of hot air saturated with moisture; others, Roman-Irish baths,
consist of dry hot air; the most recent of all are the electric light
baths, in which the radiant heat of electric lamps is utilized. But
owing to the great increase in the body temperature which they
cause, with consequent increased frequency of pulse and breathing,
and still more on account of the rapid and extensive increase in
blood-pressure to which they give rise, these powerful sudorific
baths are rarely suitable for climacteric women, and if used at all
in such cases the greatest caution must be employed. Their use is
indicated only in women in whom at the time of the menopause
the rapid onset of obesity has given rise to serious troubles, but in
whom the heart is perfectly sound and in whom the blood vessels
show no trace of sclerosis.
Far less often than warm or hot baths, or mineral water baths,
are cold baths employed during the climacteric period, for baths
at a temperature considerably below the indifferent point, and other
hydrotherapeutic procedures in which cold water is used, stimulate
the nervous system so powerfully and give rise to so great an
increase in blood-pressure, that their use is generally to be avoided
in climacteric women, since indeed it is apt to entail serious dangers
both physical and mental. Immersion baths, plunge baths, or
sponge baths, in which the water employed is at a temperature of
18° C. (64° F.) or less, are contra-indicated, for they act too energetically,
abstract heat too powerfully, to be safely employed at
this epoch of life. If we seek by means of hydrotherapeutic
measures to counteract states of congestion at the time of the
menopause, and at the same time to bring about a general invigoration
of the patient’s nervous system, immersion baths the water
of which is not below 20° C. (68° F.), and lasting from five to
fifteen minutes, would appear to be indicated. In the majority
of such cases, however, a somewhat higher temperature is preferable,
from 26 to 28° C. (79 to 82° F.), the patient lying at full
length in the bath, immersed to above the shoulders, and the water
not being agitated except by a moderate rubbing of the surface
of the body whilst the patient is in the bath. When, however, the
657patient sits in the bath, the water covering only the lower half
of the body as high as the navel, a somewhat lower temperature is
permissible, 20 to 25° C. (68 to 77° F.); but the duration should
not exceed five minutes, moderate mechanical manipulations being
carried out meanwhile; such baths appear to reduce nervous irritability
and to have a sedative effect in the manifold nervous disturbances
of the climacteric period. Sitz-baths, again, of a longer duration,
twenty to sixty minutes, the water reaching only to the navel,
and being at a temperature varying from 16 to 25° C. (60 to
77° F.), are useful in relieving chronic inflammatory states of the
reproductive organs and the associated erotic states and abdominal
pain and irritability. Colder sitz-baths, even of brief duration,
should, on the other hand, be avoided. Similarly, a shower-bath
of water at a temperature of 18 to 24° C. (64 to 75° F.), lasting
one to two minutes, and the water falling only from a very slight
elevation above the head, have a valuable sedative action; but, on
the other hand, a colder shower-bath, of water falling from a
greater height, has an exciting action, and is to be avoided at this
time of life. When there are severe congestive symptoms, friction
of the hands and feet for a short time with water at a temperature
from 12 to 17° C. (54 to 63° F.), followed by a quarter
of an hour’s rest in bed, may be recommended; also immersion of
the feet for a minute in water at a temperature of 10° C. (50° F.),
the feet being vigorously rubbed the while, followed by a walk in
the open for five or ten minutes. In cases of sleeplessness at the
menopause due to congestion, a useful method is to dip the feet
for twenty or thirty seconds in water at a temperature of 8 to
10° C. (46 to 50° F.), the feet being briskly rubbed whilst in
the water, or moved rapidly up and down with treading movements;
after withdrawal, they are quickly dried, and the patient immediately
goes to bed. Another useful mild soporific measure is to
apply before going to bed bandages wrung out of cold water; these
reach from the foot to the knee, and are left on for the whole
night. In cases of climacteric menorrhagia, my vaginal refrigerator
should be used for the direct application of cold to the reproductive
organs; this is a cylindrical apparatus introduced into
the vagina, cold water flows through the interior of the apparatus
without wetting the vaginal mucous membrane. This cooling apparatus
is useful also in troublesome cases of genital pruritus; cold
douches to the vulva for one or two minutes at a time are likewise
valuable in the relief of this affection.
For climacteric women, cold sea-bathing is as little to be recommended
as other cold hydrotherapeutic measures, owing to its
powerful refrigerative effect, and the great mechanical influence
658of the moving water in the waves. But in certain cases, in which
sea-air is likely to be beneficial, lukewarm sea-baths may also be
recommended; their effect is similar to that of weak brine-baths
at a similar temperature.
During the climacteric period, especial attention must be paid to
the care of the skin. Owing to the extreme sensitiveness of the
skin at this time of life to outward noxious influences, it is necessary
to exercise great care to dry the skin very thoroughly after
ordinary ablutions of the face and hands; irritating soaps should
be avoided, and a bland powder should be applied after drying.
During the earlier part of the climacteric period, when menstruation
has already ceased, and senile changes in the skin with atrophy of
the subcutaneous tissues have commenced, the extreme dryness of
the skin may be relieved by lukewarm baths with wet packs to
follow; after the bath, the woman is enveloped in moist linen cloths
and then covered over all with a blanket. When the skin chaps
readily, inunction of lanolin ointment will be found useful.
Cleanliness of the genital organs, at all times of importance, is
doubly so during the climacteric period, for the reason that neglect
in this respect is apt to lead to the onset of genital pruritus. Not
only after defæcation, but after each act of urination as well, the
external genital organs and the anus should be carefully washed
over with a pad of clean absorbent wool moistened with lukewarm
water. After the washing, either powder or ointment should be
applied, the former in cases in which the skin of the parts is usually
damp from a natural tendency to excessive secretion, the latter in
cases in which the skin is dry and tends to crack.
Bodily exercise, carefully selected and regulated to suit the individuality
of each patient, is a powerful means of relieving the
disturbances of the menopause. Regular and methodical bodily
exercise—to which it must be remembered, women at the climacteric
period commonly feel considerable aversion—manifests its
good effects in the form of improvement in the nutritive conditions
and functional activity of all the organs, and increased activity of
all metabolic changes, which are commonly sluggish in women at
the change of life. Moreover, muscular exercise, by increasing the
volume of blood passing through the muscles, has a beneficial
derivative influence in diminishing the congestion of the brain
and the other troublesome congestive symptoms which are liable
to occur in women during the menopause. Again, in cases of
excessive obesity such as so commonly occur in women at the
change of life, the increased combustion of fat promoted by regular
muscular exercise, cannot fail to have a beneficial effect. Finally,
suitably selected muscular exercise has a favourable influence also
659upon the nervous system, the functional activity of which it facilitates,
while at the same time it strengthens the powers of the will.
It is therefore of importance that at the time of the menopause
women should continue to undertake appropriate active exercise,
regular daily walks, which should include walking up a moderate
incline. As a preparation for such exercise (in persons hitherto
unaccustomed to walk much), or in bad weather, or, again, when
there are special reasons against open air exercise, and finally as
a supplementary exercise to walking, gymnastics and massage may
be employed. Such gymnastic procedures are to be chosen as will
serve to deplete the vessels of the head, will have a favourable
influence upon the portal circulation, and will withdraw the blood-stream
from the pelvic organs; such are, in addition to general
gymnastic exercises, methodical deep breathing, methodical exercise
of the abdominal muscles, exercises involving the extensors of the
back and the abductors and external rotators of the thigh, and
exercises of the extremities. Various gymnastic apparatus may be
employed with advantage, and more especially those in which the
various muscular movements are effected against a resistance. But
in all cases extreme care must be taken to avoid over-fatigue and
over-exertion. A graduated form of bodily exercise combined with
passive gymnastics, suitable for climacteric women, is massage, in
which by mechanical stimulation, by pressure and friction of the
whole body or of certain parts, the nutrition of the muscles is
favourably influenced, and the activity of the general circulation
is increased. In the use of massage also, in climacteric women, all
undue excitation of the nervous system is to be carefully avoided,
a mild form of this powerful agent must alone be employed; gentle
stretching and rubbing of the skin of the lower extremities, the
back, and the abdomen, followed by gentle kneading of the muscles.
Massage of the internal reproductive organs (the method of Thure
Brandt), in view of the common tendency to sexual excitability in
women at the climacteric, is mentioned only to be prohibited. For
the same reason, and also on account of the frequency with which
at the time of the menopause women suffer from tachycardia and
from other disorders of the heart, bicycling is in most cases an
unsuitable exercise at this time of life.
A matter of great importance is the regulation of the diet of
women during this phase of life, the aim of such regulation being
one which the older physicians sought to fulfil by means of venesection
and wet cupping, namely, to overcome the abnormality in
the constitution of the blood which arises from the cessation of
the internal secretion of the ovaries, and further to relieve the
symptom-complex of abdominal plethora and the various passive
hyperaemias and collateral congestions; and in addition to subdue
660the great general nervous irritability, the sensibility to external
stimuli, the inclination to excessive reflex manifestations, characteristic
in women during the climacteric period.
The diet must be regulated in respect both of quality and quantity,
and it is obvious that the regulation must be thoughtfully
adapted to the needs of each individual case.
As regards quantity, the main general principle of dietetics for
climacteric women is that over-nutrition is to be avoided, that the
quantity of nutriment must be reduced to the absolute minimum
necessary to supply the needs of the tissues. In view of the fact
that we are concerned with women at a comparatively advanced
period of life, whose physical labours are not as a rule exhausting,
that quantity of food will usually be sufficient which is competent
to furnish 35 to 40 calories per body-kilogram per diem.
If we assume that the mean body-weight of a woman as the
climacteric age is 60 kilograms, the heat-equivalent of the food required
daily by such a woman may be estimated at 2,100 to 2,400
calories. This will be approximately supplied by a diet consisting
of 100 grams albumen, 60 grams fat, and 350 grams carbohydrate.
The customary preference for a large amount of nitrogenous
food is, however, not dependent upon physiological requirements,
and provided that the needful minimum of albumen
is supplied (about 1.5 gram per body-kilogram per diem), the
requisite number of calories may be furnished by very various
combinations of the different nutritive elements.
The general principles of the qualitative regulation of the diet
of climacteric women are: first that after the necessary minimum
of albumen has been supplied, there shall be added an amount of
carbohydrate and of fat varying in relative proportions and quantities
according to the physiological requirements of the individual,
but taken together sufficient to supply the necessary heat-equivalent;
secondly, that there should be an abundant consumption of
water; thirdly, that stimulating dietetic adjuvants should as far as
possible be avoided.
The nitrogenous equilibrium of the body may be maintained
either by animal or by vegetable proteids; in the case of the former
(animal albumens), the climacteric woman should avoid those
containing considerable quantities of nucleo-albumen or of deleterious
products of tissue-change; in the case of the latter (vegetable
albumens), she should avoid those likely to cause undue stimulation
of the intestinal tract. Of flesh foods (mammals, birds, and
fishes), those kinds are to be preferred which contain small quantities
only of extractives (kreatin, xanthin, etc.) since these substances
are supposed to have a stimulating influence upon the
661nerves and the heart. Hence, boiled meat is better than roasted, and
the flesh of young animals (veal, for instance) and fish are to be
preferred to game, and the last-mentioned is to be avoided especially
for this reason, that the flavours for which it is valued by the
gourmet are products of partial decomposition arising from prolonged
hanging; for similar reasons, meat extracts, animal soups,
sausages, smoked flesh and fish, and preserved (potted) meats,
should all be avoided. From the intimate connexion between the
ingestion of nuclein and the formation of uric acid, albumens rich
in nuclein are to be forbidden; such are the various foods consisting
chiefly of gland-cells—sweetbread, liver, brain, kidneys, etc.
As well as from the appropriate flesh-foods, the requisite albumen
may most suitably be obtained from eggs and milk (including
buttermilk); on the other hand, caviare is unsuitable owing to
its stimulant action on the genital organs, cheese because it contains
large quantities of the products of decomposition of casein and
milk-fat; the fermented milks, koumiss and kefir, are likewise unsuitable.
Suitable vegetable foods for the supply of albumen (in
addition to carbohydrates) are porridge, bread, and the leguminosae;
nuts, on the other hand, cause too much irritation of the
stomach and intestines.
For women during the climacteric period we recommend a mixed
diet moderate in quantity; the amount of flesh and fat in the diet
should not be large, whilst cereals, green vegetables, and fruit may
be taken in greater abundance; irritant vegetable foods must be
avoided, and especially those which tend to stimulate unduly intestinal
muscular activity and intestinal secretion. It is important
that an abundance of water should be taken, not less than two or
three pints daily, and a pure, fresh, spring water is preferable to
the aerated waters, natural or artificial. Alcoholic beverages are
to be avoided, and more especially those which are rich in extractives
as well as in alcohol. For this latter reason, beer and champagne
are harmful, whilst spirits and liqueurs are to be condemned
on account of the high percentage of alcohol they contain. The
stimulating alkaloidal drinks, tea and coffee, are also to be avoided,
or if taken at all, only in a very dilute form. With regard to the
preparation of the food, the cardinal principle is that it should be as
little irritant as possible; neither mechanically irritating the alimentary
tract by an excess of indigestible or undigested residue, nor
irritating it chemically by an excessive admixture of sugar, salt,
vinegar, pepper and other spices; nor, finally, giving rise to thermal
irritation by being excessively hot or extremely cold.
The individual meals are preferably small ones and they must
therefore be taken at comparatively short intervals, five times daily,
the principal meal being taken at one or two o’clock in the afternoon,
662and the supper (which should be small) comparatively early,
at seven or eight o’clock.
Note.—In his discussion of the details of diet for women during the
climacteric period, hours of meals, actual dishes, etc., the author refers exclusively
to Austrian and German customs in these matters. The translator
has not attempted to adapt the following pages to the needs of English
readers, as he feels that the general principles already given will enable the
English medical man to construct without serious difficulty suitable diet-tables
for the cases with which he has to deal.
Suitable articles of food are the following:
Soups, Broths, and other Liquid Foods: Soups and broths made
from the flesh or bones of beef, mutton, veal, chicken, or pigeon,
without the addition of meat extract, or of meat juices, peptones,
somatose or nutrose, but with the addition of barley, oatmeal, rice,
wheatmeal, ryemeal, peas, beans, lentils, vermicelli, or macaroni;
also broths or porridge made from any kind of ground cereal, or
from potatoes, or from peas, beans, or lentils.
Flesh Foods: Lean beef, veal, mutton, roast or boiled, pigeon,
chicken; certain fresh fish—pike, haddock, sole, perch, and trout.
Unsuitable are: pork, goose, eels, salmon, herrings, oysters, caviare,
lobster, crab, smoked meat, hare, venison, wild-duck, brain,
liver, kidneys.
Vegetables, Sweets, and Savouries: Green peas, spinach, cauliflower,
carrots, turnips, buttered eggs, omelette, boiled and baked
puddings, rice boiled in milk, apples and rice, whipped cream,
salads, wheaten bread, French rolls, biscuits, and rusks.
Fruits: Almost all fruits may be taken, raw, cooked, or preserved;
also in the form of currant and other fruit cakes, and as
fruit-ices.
Beverages: Milk, buttermilk, water, the same acidulated with
various fruit-juices and essences (as lemonade, etc.), weak tea with
plenty of milk, cocoa, chocolate. To be forbidden are: beer, strong
and sweet wines, distilled spirits.
An example is subjoined of a simple diet-table compiled on the
above principles:
|
|
Quantity in grams. |
Albumen. |
Fat. |
Carbohydrate. |
| Afternoon: |
|
|
|
|
| |
A cup of milk |
150 |
5.4 |
5.4 |
7.5 |
| |
Roll and butter |
70 |
4.9 |
0.4 |
39.2 |
| Middle of Morning: |
|
|
|
|
| |
Soup |
100 |
1.1 |
1.5 |
5.7 |
| |
Roll |
70 |
4.9 |
0.4 |
39.2 |
| Mid-Day Meal: |
|
|
|
|
| |
Soup |
100 |
1.1 |
1.5 |
5.7 |
| |
Roast meat |
100 |
38.2 |
1.7 |
|
| |
Green vegetables |
100 |
1.6 |
0.4 |
8.4 |
| |
Pudding |
200 |
17.4 |
30.0 |
57.8 |
| |
Fruit |
100 |
3.0 |
|
15.0 |
| |
Bread |
35 |
2.4 |
0.2 |
19.0 |
| 663Breakfast: |
|
|
|
|
| |
A cup of milk |
150 |
5.4 |
5.4 |
7.5 |
| |
Roll |
70 |
4.9 |
0.4 |
39.2 |
| Supper: |
|
|
|
|
| |
Soup |
100 |
1.1 |
1.5 |
5.7 |
| |
Two soft eggs |
90 |
11.2 |
10.8 |
0.4 |
| |
Bread |
70 |
4.9 |
0.4 |
39.2 |
| |
Fruit |
100 |
3.0 |
|
15.0 |
| |
|
|
|
|
|
| Total |
1,617 |
110.5 |
69.9 |
304.5 |
| |
|
|
|
|
|
| |
| In addition, water, ad libitum, and perhaps a little light wine. |
In many cases, however, a mainly vegetarian diet may be more
suitable, and more particularly a mainly fruit diet, in order to
diminish persistent congestive symptoms. In such cases the following
diet-table may be recommended for short periods:
First breakfast: An apple and an orange.
Second breakfast: 25 grams of white bread with butter and
three baked apples.
Dinner (mid-day): 100 grams fish or meat, potatoes, green
vegetables, 3 boiled or baked apples.
Afternoon: An orange, or an apple, or a pear, or some grapes.
Supper: Milk, apples and rice, oranges, grapes, figs.
Beverages: Water, with or without fruit juices or essences.
Changes in the above diet-table could very readily be effected,
whereby the quantity of carbohydrate could be increased and the
quantity of albumen lessened.
In women of sanguine temperament and full habit of body, who
at the time of the menopause very rapidly become obese, important
changes in the diet become necessary. The main principles of a
fat-reducing diet are the following: Avoidance of all overfeeding,
reduction of the quantity of food taken below the former average
amount, with retention, however, of a sufficiency of nutrient material
to maintain the metabolic equilibrium of the essential tissues;
the maintenance of this metabolic equilibrium demands a sufficiency
of nitrogenous foods, but the fats in the diet may be reduced to a
minimum, and the carbohydrates may also be very greatly diminished.
At the same time, there must be systematic bodily exercise,
and the hours of sleep must not exceed a nightly average of seven.
For obese women at the climacteric period, a suitable average
diet would contain 160 grams albumen, 12 grams fat, and
120 grams carbohydrate, yielding a daily heat-equivalent of 1,250 to
1,300 calories.
664A sample diet-table constructed on these principles is appended:
|
|
Quantity in grams. |
Albumen. |
Fat. |
Carbohydrate. |
| Breakfast: |
|
|
|
|
| |
A cup of weak tea |
150 |
0.45 |
|
0.9 |
| |
With milk, but no sugar |
30 |
1.29 |
0.9 |
1.2 |
| |
White bread |
50 |
4.8 |
0.4 |
30.0 |
| |
Lean cold meat |
50 |
19.1 |
0.9 |
|
| Dinner (Mid-Day): |
|
|
|
|
| |
Small cup of clear soup |
100 |
1.1 |
1.5 |
5.7 |
| |
Lean beef |
200 |
76.4 |
3.4 |
|
| |
Green vegetables, salad, etc. |
100 |
1.6 |
0.4 |
8.4 |
| |
Fruit |
100 |
3.0 |
|
15.0 |
| |
Roll |
35 |
2.4 |
0.2 |
19.6 |
| Afternoon: |
|
|
|
|
| |
A cup of weak tea |
150 |
0.45 |
|
0.9 |
| |
With milk, but no sugar |
30 |
1.29 |
0.9 |
1.2 |
| Supper: |
|
|
|
|
| |
Soup |
100 |
1.1 |
1.5 |
5.7 |
| |
Lean roast meat |
100 |
38.2 |
1.7 |
|
| |
Roll |
50 |
4.8 |
0.4 |
30.0 |
| |
|
|
|
|
|
| Total |
1,245 |
155.9 |
13.2 |
118.6 |
| |
|
|
|
|
|
In the selection of individual articles of diet, it is important to
bear in mind the fact that in all climacteric women it must be our
aim to stimulate intestinal muscular activity (peristalsis) and intestinal
secretion to a moderate extent, for by more active intestinal
secretion abdominal congestion is to some extent relieved, and
by intestinal transudation and by diminution of the lateral pressure
the circulation through the abdominal vessels is facilitated. By
thus lowering the intra-abdominal blood-pressure, we shall assist
in relieving a number of chronic hyperaemic states of the pelvic
and various other organs, from which women are prone to suffer
at the menopause. Hence all articles of diet must be forbidden
which have a tendency to give rise to constipation. But we must
also forbid all substances which leave extensive undigested residues,
such as the rinds of fruits, large quantities of porridge, etc., hard
meats, nuts, and the like. Most suitable are those articles of diet
which contain large percentages of fluid constituents, such as milk,
thin soups, weak tea (infused only a short time, so as to contain
little tannic acid, which is very constipating), white meat—veal,
breast of chicken, etc. Of vegetables, those are best which contain
plenty of water and an abundance of the organic acids, young,
fresh garden produce, lettuce, cauliflower, young green peas, young
carrots, turnips, etc. Juicy fruits are good, apples, pears, cherries,
and plums. Butter and honey are also excellent. In many persons
665suffering from constipation, all that is necessary for their relief
is to give a tumblerful of cold water the first thing in the morning;
with others, the use in addition of whole-meal bread with
plenty of butter and honey and uncooked fruit, is required.
In women suffering from the various disturbances of the climacteric
period in an aggravated form, either because the menopause
occurs at an unusually early age, or because the suppression of
menstruation has taken place suddenly instead of gradually—especially
in cases of heart-trouble, severe vertigo, pronounced vasomotor
disturbances, or mental excitement (also erotic excitement),
I have sometimes found a methodical milk-cure carried on for
several weeks most beneficial. By this I do not mean an exclusive
diet of milk, but a diet consisting chiefly of milk and milk-foods;
owing to the absence of all irritation of the nervous and vascular
systems, this diet has a very definite sedative influence in such cases.
The milk should be skimmed, and should be given four times daily
in gradually increasing quantities, the total amount rising from ten
ounces to fifty ounces daily. The only other meal should be a substantial
mid-day dinner, consisting of soup, roasted white meat,
young green vegetables, and a little fruit. In some instances, to
prevent constipation, it is necessary to add ten grams of milk sugar
to each glass of milk; in other cases it is necessary to dilute the
milk with water. It is obvious that the quantity of milk given is
not alone sufficient to maintain the metabolic equilibrium of the
body; but the defect in this respect is made up by the substantial
meal given at mid-day.
Among the stimulating influences which during the sexual epoch
of the menopause are as far as possible to be avoided we must unhesitatingly
include the practice of coitus, inasmuch as at this time
of life there already exists a strong tendency towards the occurrence
of hyperaemia of the reproductive organs; and sexual intercourse,
increasing as it inevitably must this tendency to hyperaemia,
should be indulged in as little as possible. And yet precisely in
women of the climacteric age, in “la femme demi-vieille” there often
exists a strong desire to drain the cup of sexual pleasure to its
dregs. Not infrequently, therefore, the physician is asked to advise
regarding the proposed marriage of a woman in whom the
menopause is drawing near, the desired husband being young, or at
least still fully virile. If the advice is given in all sincerity with a
sole eye to the woman’s health, the medical man will definitely forbid
the marriage.
When, however, the changes of the menopause are fully completed,
when the woman’s reproductive organs have undergone
complete senile atrophy, there is no medical reason why a couple
who wish to give a tenderer name to an intimate friendship between
666man and woman, should refrain from marriage—provided
that both have attained a like stage of sexual decline. “But,”
writes Tilt, “a union between frosty January and blooming May
is likely to be as dangerous to the health as it is to the happiness
of both.”
Whilst attending to the regulation of the physical diet of his climacteric
patient, the physician should not overlook her psychical
regimen. A woman’s mind is very powerfully affected by the processes
of the menopause. On the one hand, her fears are stimulated
by the thought that she is entering upon the “critical age,” of whose
dangers she has often been warned; and, on the other hand, she is
mentally depressed by the knowledge that she is about to lose the
charms of womanhood, and to decline in sexual esteem. It is well,
therefore, for women during the years of change, to have some
kind of employment, which fills their hours, occupies their thoughts,
and—leaves a certain scope for the exercise of feminine vanity.
Works of benevolence or of general utility, and literary occupations,
are thus of great advantage to climacteric women. Plato,
indeed, pointed out that women at this time of their lives should
occupy themselves with literature and intellectual culture.
Just as it is the duty of the physician, more especially of the
family physician, to enlighten the maiden on the threshold of her
sexual development regarding the processes of the awakening sexual
life, and to give her the necessary instruction concerning the
hygienic measures which it is proper for her to adopt—so also is
it his duty to convey medical information to the woman who stands
on the threshold of sexual decadence. A woman’s ignorance is
often equally profound at both these epochs of the sexual life. A
woman in the early forties often does not suspect, or at least refuses
to acknowledge, that she is gradually drawing near to the end
of her sexual life; and she is still farther from the knowledge that
definite rules of general and sexual hygiene must be observed by
her if she wishes to minimize the dangers of the critical period.
The medical friend, in an earnest though far from gloomy manner,
will expound to her the nature of the physiological processes
of the menopause, and will instruct her regarding the corresponding
preventive measures—diet, exercise, clothing, care of the skin,
and the regulation of sexual intercourse. Moreover, the physician,
by means of skilfully directed enquiries regarding certain symptoms,
will be enabled to gain early information about the occurrence
of abnormal processes at this period of life, and will in this way
detect the first beginnings of many diseases which are amenable
to treatment only at the very outset of their course. For example,
Brierre do Boismont, an early and accurate observer of this sexual
epoch in the life of woman, points out that in cases in which, during
667the change of life, a woman experiences an increased inclination
for sexual intercourse, nineteen times out of twenty, a local examination
will disclose the existence of some disease of the reproductive
apparatus. Similarly, every gynecologist is now familiar
with the fact that unusually free, atypical haemorrhages during
the climacteric period, are commonly indications of the existence of
a uterine neoplasm.
Much evil may be avoided, and much suffering can be diminished
if the physician, in accordance with the advice of Hippocrates, does
not limit his activities strictly to the exercise of the healing art,
but stands by a woman’s side as her mentor and confidant during
the troublesome years of her sexual decline. And he will best fulfil
these functions, if he succeeds in convincing the climacteric woman
of the profound truth embodied in the saying of the great French
philosopher:
Qui n’a pas l’esprit de son âge,
De son âge a tout le malheur.
669
INDEX
[References are to pages.]
- Abdominal pains, 46.
- Abdominal pressure, 46.
- Aberration, moral, 46.
- Absence of mind, 154.
- Absence of ovaries, 182.
- Abnormalities, mental, 155.
- Abortion, 223, 414.
- Abstinence, 256, 398.
- Acromegaly, 102.
- Act of intercourse, 84.
- Activity, sexual in women, 597.
- Acton, 276.
- Actual intercourse, 84.
- Adamites, 302.
- Africa, 43, 45.
- Age, average, at marriage, 200.
- Agineta, 464.
- Ahlfeld, 308, 333, 424, 448.
- Air hunger, 419.
- Albert, 331.
- Albertus Magnus, 1.
- Albini, 454.
- Albuminuria, 93.
- Alcohol, 155, 258, 270.
- Algeri, 155.
- Alibert, 408, 597.
- Almquist, 262.
- Ahlfeld, 482.
- Amenorrhœa, 84, 128, 160.
- Amentia, 103.
- America, 43.
- Amputation of clitoris, 184.
- Amussat, 542.
- Amyntor, 219.
- Anæsthesia, 184, 187.
- Anatomical changes, 8, 50, 141, 209.
- Anderson, 331.
- Andral, 582.
- Aneurysm, 98.
- Anger, 183.
- Angina pectoris, 240.
- Anjel, 191.
- Anomalies of vagina, 331.
- Antipathic sexuality, 194.
- Antitoxic functions, 21.
- Ansell, 365, 466, 561.
- Ansty, 135.
- Anxiety neurosis, 405.
- Apes, 22.
- Appetite, loss of, 46, 107.
- Aqueo-mucous vaginal discharge, 46.
- Arabian women, 30.
- Aran, 632.
- Areola mammae, 208.
- Aretæus, 1.
- Aristotle, 1, 211, 392, 420, 463, 473, 498, 544.
- Arius, 502.
- Arndt, 233, 343, 418.
- Arthritis, 635.
- Artificial fertilization, 317.
- Asher, 406, 538, 541, 559, 563.
- Ashwell, 109.
- Asia, 42.
- Aspermatism, 317.
- Athenaeus, 302.
- Atlee, 474, 603.
- Atmocausis, 419.
- Atri, 266.
- Atrophy, concentric, 590.
- Atrophy, excentric, 590.
- Atrophy, gradual, 592.
- Atrophy of uterine muscle, 609.
- Azoospermia, 316.
- Babbage, 433.
- Bacon, 271.
- Bacterial flow, 593.
- Baer, 616.
- Bain, 203.
- 670Bailly, 183.
- Baillarger, 438.
- Bainbridge, 331.
- Baker-Brown, 546.
- Balestra, 575.
- Ball, 156.
- Balzac, 193.
- Bandl, 536, 557.
- Barker, 556.
- Barnes, 161.
- Bartels, 47, 331.
- Bartholin’s gland, 529.
- Basch, 296.
- Baths, 116, 117, 280, 654.
- Battey, 475, 564.
- Baumes, 260.
- Baumgarten, 166.
- Baust, 441.
- Bazaraignes, 434.
- Beard, 106, 405.
- Beauty, attribute of, 23.
- Beauty, curve of, 24.
- Beauty, decline in, 23.
- Beauty of woman, 200, 206.
- Bebel, 77, 394, 401, 415.
- Beck, 296.
- Becker, 305.
- Bednar, 478.
- Beer, 161.
- Beigel, 165, 300, 496, 505, 517, 525, 604.
- Bélot, 193.
- Bennet, 64, 88, 632.
- Benzler, 540.
- Bergh, 210, 496.
- Bernard, 78.
- Bernstein, 365.
- Bertillon, 218, 264, 382.
- Berwitz, 101.
- Bidder, 436, 439.
- Biermer, 412.
- Billroth, 337.
- Birch, 305.
- Birkett, 619.
- Birsmont, 29, 42, 45, 135, 594, 603, 607, 666.
- Bischoff, 136, 140.
- Bladder, irritable, 107.
- Blindness, 108.
- Blondes, 45.
- Blood, anomalies of, 478.
- Blood pressure, 16.
- Blumbenbach, 132.
- Blundell, 90, 417, 568, 603.
- Blushing, spontaneous, 46.
- Bock, 353.
- Bodily exercise, 658.
- Brehm, 62, 331.
- Bömer, 182, 618, 629, 632, 640.
- Bohn, 635.
- Boileux, 419.
- Boinet, 474.
- Boireau, 2.
- Boivin, 498.
- Bonton, 88.
- Bonvalot, 17.
- Books, 121.
- Bordier, 556.
- Born, 305, 456.
- Bottermund, 146.
- Bossi, 607.
- Bouchardat, 130.
- Bowditch, 46.
- Bowels, regulation of, 121.
- Boyd, 496.
- Bradlaugh, 393.
- Braid, 494.
- Braun, 234, 326, 332, 438, 446.
- Breasts, 213.
- Brehm, 416.
- Breisky, 326, 334, 515.
- Breslau, 423, 435, 437.
- Breuer, 92.
- Brill, 326.
- Broudardel, 72.
- Brown-Sequard, 20, 587.
- Bruce, 364.
- Brunettes, 45.
- Bruntzel, 182.
- Buckle, 378.
- Buddha, 168.
- Buffon, 167.
- Bulimia, 107.
- Bulwer, 260.
- Burdach, 294, 466.
- Burg, 413.
- 671Burggraeve, 496.
- Burkart, 473.
- Burton, 515.
- Busch, 2, 580.
- Butlin-Smythe, 235.
- Butti, 193.
- Cæsarean section, 567.
- Calderini, 44.
- Campbell, 443.
- Cantharides, 186.
- Capellmann, 400.
- Capwron, 482.
- Cardiac disorders, 94, 97, 236, 243, 344, 626.
- Cardiopathie de la ménopause, 629.
- Cardiopathy, uterine, 235.
- Care of genital organs, 279.
- Care of skin, 658.
- Carey, 394.
- Carlile, 393.
- Carlier, 195.
- Carus, 80, 364.
- Casper, 189, 292, 547.
- Castan, 86.
- Castration, 419, 475.
- Catamenial flow, 83.
- Catarrh, gastric, 229.
- Catarrh in vagina, 614.
- Catarrh in vulva, 614.
- Cattle-breeders, 358.
- Causes of early development of menarche, 49.
- Causes for lack of sexual impulse, 188.
- Causes for intensity of sexual impulse, 188.
- Causes of ungratifying coitus, 357.
- Caustics, 119, 568.
- Cavum uteri, 56.
- Celibacy, 173.
- Celsus, 463.
- Cervix uteri, absence of, 506.
- Cervix uteri, deformities of, 503.
- Cervix uteri, hypertrophy of, 334.
- Cervix uteri, ideal form of, 502.
- Cervix uteri, normal form of, 502.
- Cervix uteri, pathological changes of, 501.
- Charpignon, 556.
- Champonière, 17.
- Change of life, 571.
- Changes in the skin, 148, 208.
- Characteristics, inherited, 25.
- Charcot, 100.
- Charrin, 21.
- Chassaignac, 107.
- Chassagne, 260.
- Chastity, 123.
- Chazan, 138.
- Checks to increase of population, 391.
- Chevin, 466.
- Chiari, 438, 490, 616.
- Chlorosis, 21, 86, 91.
- Christianity, diffusion of, 6.
- Chrobak, 214, 298.
- Chronic endometritis, 87.
- Chronic metrometritis, 87.
- Circulatory organs, 149, 240, 620.
- Circumcision of women, 328.
- Civilization, progress of, 6.
- Clarke, 443.
- Cleanliness of genital organs, 658.
- Cleft, vulval, 51.
- Clément, 629.
- Cleveland, 482.
- Climacteric insanity, 643.
- Climacteric phenomena, 600.
- Climacteric psychoses, 643.
- Climacteric psychoses, prognosis of, 653.
- Climacterium, 571.
- Climacterium, dangers of, 578.
- Climatic conditions, 27, 37, 117, 132.
- Clitoris, 74, 330.
- Clitoris crises, 352.
- Clothing, 114, 121.
- Coccygodynia, 107.
- Coffee, 121.
- Coffignon, 189.
- Cohen, 108.
- Cohn, 148.
- Cohnstein, 402, 548, 558, 634,
- Coitus interruptus, 345.
- 672Coitus, obstacles to completion of, 335.
- Coitus, prohibitive, 529.
- Coitus, undue frequency of, 294.
- Cold nature, 188.
- Cold sponging, 281.
- Cole, 553.
- Collins, 139.
- Colpotomy, 418.
- Combys, 79.
- Comedones, 110.
- Compensation, disturbances of, 254.
- Competence for marriage, 250.
- Conception, 137, 299, 304, 308, 366, 483.
- Conditions essential to procreation, 469.
- Condoms, 405, 409.
- Confucius, 385.
- Congestion, premenstrual, 142.
- Congfou, 403, 547.
- Congressus interruptus, 220, 225.
- Congressus reservatus, 225, 227.
- Conjugation, interference with, 487.
- Conjunction, 108.
- Conservants, 109.
- Constipation, 107, 228.
- Constitution, 38.
- Constitutional conditions and menopause, 599.
- Constrictor cunni muscle, 348.
- Consumption of nitrogen, 22.
- Continence, sexual, 400.
- Continence, sexual, enforced, 172.
- Contraction, pelvic, 334.
- Contrectation, 176.
- Control of instinctive impulses, 25.
- Control of reproductive function, 397.
- Convulsions, 152.
- Cook, 302, 443.
- Cooper, 639.
- Copulation, 200, 284, 323.
- Corpora albicantia, 592.
- Corpora fibrosa, 592.
- Corpus luteum, 59.
- Corset liver, 122.
- Corsets, 90, 122.
- Cosmophil nerves, 17.
- Coste, 136, 304, 454.
- Courty, 25, 29, 46, 132, 329, 361, 549, 594, 603, 607.
- Craisson, 292.
- Crampe, 380.
- Crédé, 494.
- Crimes committed during menstruation, 159.
- Critical age, 571.
- Critical period, 572.
- Croom, 164.
- Cros, 378.
- Cruise, 494.
- Culture, modern, 6.
- Curetting, 119.
- Currier, 609.
- Curve of the sexual life of woman, 4.
- Cyon, 16.
- Cysts, 588.
- Dangers to sexual life, 276.
- Dante, 171.
- Dark rings around the eyes, 46.
- Darwin, 170, 376, 379, 380, 449, 485, 545.
- Davis, 340, 484.
- Decaisne, 165.
- Defloration, 326.
- Degeneration, stigmata of, 387.
- De Graaf, 136.
- Debay, 168, 482.
- Dehio, 116.
- De la Motte, 364.
- Delivery, previous, 560.
- Delusianne, 258.
- Demange, 21.
- Demosthenes, 271.
- Denis, 130.
- Denman, 555.
- Dental transverse ridges, 57.
- Derangement, 103.
- D’Espine, 40, 82, 477, 538.
- Desqué, 128.
- Determinants as to marriage, 259.
- Determination of sex, 420.
- 673Determination of sex, influences on, 421, 436, 445.
- Detumescence, 176.
- De Villeneuve, 144.
- Devilliers, 337.
- Dewees, 365.
- Diamant, 79, 158.
- Diarrhœa, 144.
- Diderot, 192.
- Diet, 112, 127, 659.
- Diet, regulation of, 660.
- Digestion, disorders of, 107.
- Digestive organs, 145, 630.
- Diminution of procreative capacity, 401.
- Diokles, 381.
- Disinclination to physical exercise, 93.
- Disorders, various, 85.
- Disparity in age, 265.
- Disturbances, nervous, 587.
- Disturbances of general system, 587.
- Dohm, 527.
- Doran, 617.
- Double chin, 572.
- Doubleday, 485.
- D’Outreport, 80.
- Dragging sensations, 46.
- Dreams, erotic, 107.
- Dubois, 135.
- Duchatelet, 477.
- Duerer, 210.
- Duesing, 231, 424, 442, 449, 453.
- Dugès, 498.
- Duhousset, 190.
- Duke, 480.
- Duncan, 146, 360, 367, 377, 466, 484, 513, 546, 562.
- Dunlap, 165.
- Dunn, 161.
- Duplay, 494.
- Duprès, 614.
- Dupruyten, 494.
- Duration of sexual period, 26, 30, 130, 181.
- Dysmenorrhœa, 160.
- Dysmenorrhœa, inflammatory, 162.
- Dysmenorrhœa, intermediate, 164.
- Dysmenorrhœa, mechanical, 162.
- Dysmenorrhœa, nervous, 162.
- Dysmenorrhœa, symptoms of, 163.
- Dyspareunia, 187, 347, 355, 358, 359.
- Dyspepsia, 23, 107, 227, 229, 631.
- Edebohls, 165.
- Edis, 294.
- Effects of marriage on hysteria, 257.
- Effertz, 173.
- Egger, 118.
- Eggle, 211.
- Eichstadt, 298.
- Eisenhart, 107, 234.
- Ejaculatio praecox, 225.
- Ejaculation, 349.
- Elberskirchen, 173.
- Elder, 235.
- Elephantiasis of labia, 530.
- Elliott, 395.
- Ellis, 169.
- Elsaesser, 438.
- Emancipation, 200.
- Embrace, intimate, 84.
- Emmet, 45, 150, 414, 473, 522, 604.
- Endogamy, 386.
- Endometritis, 87, 235, 611.
- Energy of woman, 200.
- Engagement, 142.
- Engel, 494.
- Engelhardt, 244.
- Engelmann, 137, 142.
- English, 293.
- Engstroem, 40.
- Enlightenment of young girls, 35, 124, 273.
- Enteroptosis, 90.
- Epilepsy, 102, 257.
- Epithelioid cells, 60.
- Epistaxis, 165.
- Equal moral rights, 264.
- Equilibrium, mental, 153.
- Erb, 172.
- Erethism, sexual, 575.
- Erlmeyer, 473.
- Eroess, 78.
- Erotic dreams, 107.
- Erotic element, 173.
- 674Erotic problem, 264.
- Erotic sphere, 172.
- Eroticism, 652.
- Erysipelas, 634.
- Esquirol, 81, 646.
- Etienne, 21.
- Exogamy, 386.
- Eulenburg, 123, 199, 338, 354, 402, 405.
- Europe, middle, 41.
- Europe, southern, 42.
- Eustache, 293.
- Excess, habitual, 406.
- Excess, sexual, 560.
- Excessive prudery, 88.
- Excessive sexual desire, 178.
- Ezekiel, 47.
- Facial aspect, 46.
- Fainting fit, 102.
- Fallopian tube, 489, 568.
- False shame, 340.
- Family life, 5.
- Febris amatoria, 92.
- Federns, 16.
- Feeling of weakness, 46.
- Feeling of numbness, 46.
- Fehling, 17, 396, 407.
- Fellner, 260.
- Female companion, 192.
- Female organs, diseases of, 83.
- Feokstitow, 309.
- Ferdy, 409.
- Féré, 258.
- Ferrero, 302.
- Fertility in woman, 363.
- Fertility, conjugal, 382.
- Fertility, ideal of, 365.
- Fertility, influences on, 374, 378.
- Fertility, maximum, 373.
- Fertility, monogenous, 373.
- Fertility of female criminals, 382.
- Fertility of prostitutes, 382.
- Fertility, physiological, 365.
- Fertility, restriction of, 388.
- Fertilization, 137, 300, 305, 317, 321, 322.
- Feydeau, 193.
- Finkelstein, 148.
- Finlayson, 366.
- Fiquet, 450, 454.
- Fischel, 165.
- Flamerdinghe, 525.
- Flaubert, 193.
- Fleischer, 16.
- Fleischmann, 146, 165.
- Flow, suppression of, 103.
- Follicles, graafian, 57.
- Follicles, primitive, 57.
- Follicles, ripening, 61.
- Foods suitable for menopause, 662.
- Foerster, 489.
- Fordyce, 556.
- Forensic significance of women during menses, 159.
- Foster, 135.
- Frænkel, 86, 91.
- Franchi, 165.
- Frank, 331, 466.
- Free love, 261.
- Free secretions, 51.
- Freedom of the male, 33.
- Freedom, sexual, 264.
- Frerichs, 632.
- Freud, 405.
- Freund, 103, 223, 225, 490, 494, 527, 601.
- Fricke, 109, 438, 448.
- Fricker, 165.
- Friedmann, 100, 104, 157.
- Friedreich, 108.
- “Friends,” 193.
- Frigidity, partial, 173.
- Fritsch, 143, 320, 341, 506, 519, 537, 555, 566, 600, 614, 619.
- Froehlich, 86.
- Frommel, 602.
- Froriep, 417, 568.
- Frost, 343.
- Fuchs, 646.
- Fürbringer, 168, 312, 317, 406, 535.
- Fürst, 440, 491.
- Function, sexual, 173.
- Galen, 1, 77, 135, 187, 210, 251, 420.
- Gallard, 88.
- 675Gallemairts, 165.
- Garat, 652.
- Gastric secretion, 228.
- Gastro-intestinal affections, 235.
- Gautier, 193, 318.
- Gavaret, 582.
- Gebhard, 40, 79, 138, 142, 163.
- Geissler, 427.
- Geist, 637.
- Gendrin, 136.
- General disturbances, 145.
- General fatigue, 46.
- General weakness, 46.
- Genital organs, diseases of, 529.
- Genital organs, secretions of, 528.
- Genital organs, secretions of, reactions of, 529.
- Gerbe, 453.
- Gilbert, 89.
- Gilles de la Tourette, 109.
- Gillirray, 415.
- Giordano, 172.
- Giraud, 156, 186, 318.
- Girdles of chastity, 417.
- Girdwood, 136.
- Glaevecke, 138, 166, 182, 575, 629, 644.
- Glands, reproductive, 20.
- Glands, sebaceous, 51.
- Globules, polar, 305.
- Glünder, 537.
- Godefroy, 482.
- Goehlert, 370, 380, 423, 427, 443, 466.
- Goethe, 3, 120, 167.
- Goitre, 108.
- Goltz, 21, 237.
- Gonococcus, 26.
- Gonorrhea, 200, 220, 278, 511.
- Gonorrheal infection, 533, 553.
- Goodell, 183, 406, 515, 575.
- Goodman, 18.
- Gosselin, 534.
- Gottschalk, 235, 603, 612.
- Graafian follicles, 57, 584, 587.
- Gräfe, 398, 406.
- Graily-Hewit, 234, 296.
- Grawitz, 90.
- Great uterine plexus, 16.
- Grechen, 539.
- Greeks, unchastity of, 192.
- Grenser, 521.
- Griesheim, 456.
- Griesinger, 105, 653.
- Grillparzer, 285.
- Grimmaldi, 81.
- Grisolle, 260.
- Grohe, 298, 473.
- Grünewaldt, 467, 532, 551, 559.
- Grünfeld, 110, 118, 209, 409.
- Grusdeff, 41.
- Gunzburg, 410.
- Gurrieri, 87, 382.
- Gusserow, 494, 525, 616.
- Gutceit, 105, 289, 350, 545.
- Guy, 30, 596, 603.
- Gynandry, 190.
- Gynecological examination, 119.
- Gyurkovechky, 315.
- Hæckel, 460.
- Hæmicrania, 100, 154.
- Hæmmorhages, 604.
- Hæmotopoiesis, 21, 89.
- Hahn, 165.
- Hair, pubic, 51, 110.
- Haller, 80.
- “Half old,” 576.
- Haller, 2, 364, 544.
- Hammerschlag, 89.
- Hammond, 258.
- Hampe, 426.
- Hanau, 260, 478.
- Hang, 148.
- Hannover, 31.
- Hardening of constitution, 25.
- Harley, 320.
- Hartmann, 202, 416.
- Haschek, 482.
- Hasler, 306.
- Hauff, 182.
- Haussmann, 299, 331, 408.
- Haycraft, 378.
- Hayem, 113.
- Headache, 107.
- Heart, degeneration of, 238.
- Heart, female, at puberty, 98.
- 676Heart, puberal development, 98.
- Heart, spasms of, 98.
- Heat, 136, 139.
- Heat, fugitive, 577, 581.
- Hebe, 210.
- Hebephrenie, 101.
- Heber, 148.
- Hebra, 146, 634.
- Hecker, 308, 424, 438.
- Hedin, 466.
- Hegar, 17, 91, 140, 168, 173, 182, 218, 224, 243, 278, 282, 292, 346, 386, 397, 564.
- Heidenreich, 108.
- Heinberger, 108.
- Heine, 98.
- Heitzmann, 147, 325.
- Hellwald, 181.
- Helmont, 2.
- Hemsbach, 438.
- Henle, 58, 597.
- Hennig, 19, 99, 215, 333, 493, 556.
- Henoch, 632.
- Henrik, 235.
- Hensen, 137, 179, 249, 304, 308, 348, 422, 439, 449.
- Heusinger, 165.
- Heppner, 495.
- Hereditary predisposition, 245.
- Herman, 343, 612.
- Hermes, 565.
- Herodotus, 185, 301.
- Herpes, 111.
- Hettstenius, 383.
- Hewitt, 522.
- Hey, 46.
- Hildebrand, 341, 511.
- Hippocrates, 1, 101, 103, 129, 135, 306, 381, 420, 480, 502, 631.
- Hirsch, 135.
- Hirschfeld, 305.
- Hirt, 405.
- His, 304.
- Hoesslin, 405.
- Hofacker, 422, 426, 429, 434.
- Hoffmann, 69, 74, 89, 296, 331, 334, 344, 496.
- Hofmeier, 80, 305, 484, 525, 536.
- Hohl, 296.
- Hollaender, 100.
- Holst, 300, 475, 523.
- Homosexuality, 189, 198, 548.
- Horace, 271.
- Horn, 432.
- Horse breeders, 358.
- Hortle, 165.
- Horton, 326.
- Hottentot apron, 212, 328.
- Huchard, 252.
- Hughes, 100.
- Humbold, 2.
- Humming top murmur, 96.
- Hunter, 486.
- Hydrometra, 613.
- Hydrotherapeutics, 115.
- Hygiene during menacme, 261.
- Hygiene during menarche, 111.
- Hygiene during menopause, 653.
- Hygiene of marriage, 265.
- Hygiene, rules of, 125.
- Hymen, 63, 333.
- Hymen, various forms, 66, 67.
- Hyperæmia, 581.
- Hyperæsthesia, 107, 178.
- Hyperplasia, 612.
- Hyrtl, 61, 213, 330, 446.
- Huysmans, 206.
- Hysteria, 154, 245.
- Icard, 203.
- Ideal passion, 36.
- Ill, 515.
- Impotence, complete, 337.
- Impotence, paralytic, 336.
- Impotence, psychical, 335.
- Impotentia concipiendi, 551.
- Impotentia generandi, 551.
- Impulse, sexual, 76, 123, 166, 168, 169, 182, 190, 201.
- Impulse, sexual, inverted, 548.
- Impulse, sexual, perverted, 548.
- Impulse toward reproduction, 169.
- Inability to marry, effects of, 261.
- Inbreeding, 386, 486.
- Incapacity for inoculation of ovum, 549.
- 677Incapacity for inoculation, causes for, 552.
- Incest, 197.
- Incontinence, 278.
- Indifference, sexual, 171.
- Individual variations, 133.
- Infective germs, 220.
- Infibulation, 416.
- Infidelity, marital, 357.
- Inflammatory processes, 87, 238.
- Influences on female organism, 15.
- Injuries in parturition, 223.
- Injuries in parturition, complications, 224.
- Injuries to vagina, 331.
- Inner tunic, 59.
- Insanity, 152, 249.
- Insomnia, 107.
- Instinct for preservation of species, 201.
- Intensity of sexual life, 26.
- Intercourse, sexual, at early age, 27.
- Intercourse, sexual, during menstruation, 140.
- Intercourse, sexual, frequency of, 275.
- Intercourse, sexual, lack of, 257.
- Intercourse, sexual, need of, 281.
- Intercourse, sexual, promiscuous, 301.
- Intercourse, sexual, restraint in, 276, 301.
- Intermenstrual pain, 164.
- Intermenstrual period, 140.
- Interval between periods, 132.
- Intestinal meteorism, 46.
- Investigations, anatomical, 446.
- Investigations, experimental, 452.
- Investigations, statistical, 422.
- Iridochoroiditis, 108.
- Irritable weakness, 336.
- Irritation, senile, 613.
- Islam, 129.
- Itching sensation in genital organs, 46.
- Jackson, 494.
- Jacobi, 18.
- Jaffé, 235.
- Janovsky, 147.
- Jarowski, 112.
- Jealousy, 651.
- Jeamin, 208.
- Jeannel, 538.
- Jewesses, 45.
- Joachim, 45.
- Johannsen, 509.
- Johnstone, 138.
- Jolly, 186.
- Joseph, 147.
- Joubert, 42.
- Jung, 641.
- Janke, 450, 454.
- Justinian, 48.
- Juvenal, 192, 273, 392.
- Kahane, 89, 112.
- Kahlbaum, 101.
- Kahlden, 141.
- Kaltenbach, 292.
- Kapysa, 266.
- Katatonia, 103.
- Kehrer, 293, 299, 316, 417, 509, 513, 521, 538.
- Kennedy, 337, 365.
- Keratitis, 108.
- Keppler, 566.
- Kerley, 165.
- Készmarsky, 499.
- Key, Ellen, 201, 262.
- Kidney, movable, 122.
- King, 364.
- Kirn, 103.
- Kiss, 285.
- Kiwisch, 494, 603, 616.
- Klebs, 473, 490, 494, 507, 552.
- Kleinwaechter, 396, 406, 410, 556, 563, 601, 618.
- Klinkosch-Hill, 494.
- Koblanck, 364.
- Kocks, 417, 568.
- Koeberlé, 182, 564.
- Koenig, 593.
- Koeroesi, 372, 375, 384.
- Kokkogam, 291.
- Koran, 294.
- 678Kossmann, 419.
- Kostkewitsch, 630.
- Kowalewski, 102, 155, 647, 653.
- Krafft-Ebing, 77, 103, 155, 159, 176, 184, 186, 189, 196, 258, 282, 349, 353, 358, 403, 641, 647.
- Krause, 290, 348.
- Krausold, 195.
- Kretschy, 16.
- Krieger, 28, 31, 40, 43, 98, 130, 134, 145, 482, 594, 603.
- Kristeller, 297.
- Krönig, 257.
- Kroner, 335, 539.
- Krugenstein, 159.
- Kuehne, 116.
- Kulischer, 181.
- Kundrat, 89, 137, 142.
- Kussmaul, 81, 182, 189, 489, 494.
- Labalbary, 541.
- Labia, 212.
- Labial hernia, 328.
- Laboring classes, 27.
- Lacasella, 192.
- Lactation, 139, 403.
- Lafarque, 197.
- Lambert, 191.
- Lamy, 232.
- Landau, 143, 240, 566, 568.
- Lantier, 80.
- Larcher, 260.
- Lasarewitsch, 499.
- Lascivious procedures, 195.
- Lateral sacral arteries, 14.
- Lauenstein, 522.
- Laurent, 81.
- Laval, 146.
- Law, 109, 165.
- Lawrence, 161.
- Lawson Tait, 102, 139, 564, 618, 637.
- Lebedinsky, 479.
- Lebert, 260, 616, 619.
- Lecal, 45.
- L’Eclos, 573.
- Lecluyse, 567.
- Lee, 474.
- Le Fort, 165, 339.
- Legoyt, 377.
- Legrand du Saulle, 159, 198.
- Legs, paræsthesia of, 107.
- Lehmann, 241.
- Leopold, 137, 141, 326, 528, 616.
- Léseurs, 318.
- Leube, 93.
- Leuckart, 446.
- Lever, 466.
- Levi, 496.
- Levinstein, 473.
- Levy, 419, 438, 531.
- Lewin, 478.
- Lewy, 235.
- Leyden, 233, 252.
- Libido sexualis, 641.
- Lichtenberg, 109.
- Liebig, 393.
- Liégois, 166.
- Lier, 406, 538, 541, 559, 563.
- Limitation of offspring, 283.
- Linea alba, 208.
- Linnæus, 132.
- Lipomatosis, 93, 635.
- Lippich, 377.
- Liquor folliculi, 59.
- Litschkuss, 499.
- Litzmann, 168, 296.
- Local causes, 48.
- Local disturbances, 145.
- Local irritations, 177.
- Lode, 305.
- Loehlein, 556.
- Loewenfeld, 106, 173, 256, 308, 402, 406.
- Loewenhardt, 137.
- Loewenthal, 304.
- Loewy, 22, 482.
- Lombard, 118.
- Lombroso, 46, 81, 159, 170, 186, 192, 203, 210, 262, 301, 382.
- Lona, 381.
- Lorain, 612.
- Lott, 408, 502.
- Louis, 332.
- Love, free, 305.
- Love in woman, 170, 285.
- Love, Lesbian, 189, 415.
- 679Love of early youth, 77.
- Love, perfect, 263.
- Love, platonic, 171.
- Lower, 538.
- Lucas, 494.
- Lucian, 192.
- Lumbar enlargement, 226.
- Lumbar pain, 46.
- Lumpe, 498.
- Lutaud, 320.
- Lutein cells, 60.
- Luther, 168, 269, 385.
- Lycurgus, 272.
- Lymphatic vascular system, 15.
- Mabille, 155.
- Mackenzie, 109.
- Macnaughton Jones, 161, 163.
- McClintock, 525.
- Macdonald, 522.
- MacDowell, 564.
- McGillivray, 476.
- McLennan, 443.
- Magnan, 178, 198.
- Mahommedan people, 62.
- Mahomet, 269.
- Mainländer, 168.
- Mairet, 158.
- Male, prepotency of, 450.
- Malthus, 376, 389.
- Malthusian League, 393.
- Mamma, 73, 75, 619.
- Mandl, 142, 235.
- Mania, 249, 650.
- Manipulations, intra-uterine, 238.
- Mantegazza, 23, 76, 170, 190, 193, 198, 207, 213, 380, 405.
- Manus, 266, 385.
- Marasmus, senile, 576.
- Marcé, 155, 250.
- Marie-Clement, 2.
- Marholm, 205.
- Mariagalli, 17.
- Marilegoute, 434, 455.
- Markzellen, 89.
- Marotte, 102.
- Marriage, at what age, 266.
- Marriage, consanguineous, 387.
- Marriage, immoral, 262.
- Marriage of near kin, 267.
- Marriage, premature, 473.
- Marsa, 364.
- Marsh, 597.
- Martial, 189.
- Martin, 80, 139, 299, 331, 337, 342, 474, 512, 536.
- Martineau, 81, 190.
- Maschka, 61, 66, 72, 190, 195, 331, 547.
- Masochism, 194.
- Masturbation, 88, 104, 124.
- Maternity, 200.
- Maturation, 140, 188.
- Matusch, 627, 646, 652.
- Maxwell, 613.
- Mayer, 31, 40, 45, 131, 297, 332, 384, 478, 599, 603.
- Mayet, 382.
- Means for exciting voluptuous sensations, 361.
- Meinert, 90.
- Meissner, 365, 538, 606.
- Melancholia, 103, 257.
- Membrane, uterine mucous, 217.
- Menacme, pathology of, 218.
- Menacme, physiology of, 201.
- Menacme, sexual epoch of, 200.
- Menarche, 37.
- Menarche and menopause, 595.
- Menarche, pathology of, 82.
- Menarche praecox, 78, 82.
- Menarche tardiva, 78, 82.
- Mende, 365.
- Mendes de Leon, 142, 235.
- Menge, 593.
- Menopause, 571.
- Menopause and race, 594.
- Menopause, artificial, 580.
- Menopause, changes in, 582.
- Menopause delayed, 600.
- Menopause, pathology of, 608.
- Menopause, premature, 600.
- Menopause, sudden, 600.
- Menopause, time of, 593.
- Menorrhagia, 86, 160, 608.
- Menses, suppression of, 233.
- 680Mensinga, 406, 411.
- Menstrual blood, 129, 130.
- Menstrual cycle, 19.
- Menstrual psychoses, 193.
- Menstrual stimulus, 103.
- Menstrual style, 148.
- Menstruation, 124.
- Menstruation, anomalies of, 83.
- Menstruation and age, 32, 38.
- Menstruation and climate, 32.
- Menstruation and nationality, 32.
- Menstruation, beginning of, 30.
- Menstruation, bloodless, 578.
- Menstruation, cardiac activity during, 143.
- Menstruation, cessation of, 576.
- Menstruation, disorders during, 144.
- Menstruation, disturbances of, 219.
- Menstruation, first appearance, 45, 82.
- Menstruation, irregular, 134.
- Menstruation, late, 483.
- Menstruation, pathology of, 143.
- Menstruation, praecox, 79.
- Menstruation, regular type of, 134.
- Menstruation, remittent, 135.
- Menstruation, vicarious, 164.
- Mental disturbances, 145, 161.
- Mental stimuli, 84.
- Mercier, 118.
- Merson, 653.
- Messalina, 185.
- Metabolic balance, 94.
- Metabolism, 19, 635.
- Metamorphosis, retrogressive, 584.
- Metritis, chronic, 611.
- Metritis, virginal, 232.
- Metrorrhagia, 86.
- Metschnikoff, 32.
- Meyerhofer, 300, 304, 446.
- Michel, 525.
- Michelet, 6, 273.
- Micklucho-Mackay, 415, 476, 541, 564.
- Mill, 393.
- Miller, 108.
- Mind, disturbances of, 226.
- Minor troubles, 226.
- Misuse of medical science, 395.
- Moebius, 268.
- Moericke, 141.
- Moist appearance, 51,
- Molitor, 80.
- Moll, 175, 189, 194, 198.
- Mons veneris, 210.
- Montesquieu, 378, 538.
- Montgomery, 80.
- Mooren, 108, 160.
- Moraglia, 194.
- Moral demand, 36.
- Morality, sexual, 36.
- Morbus virgineus, 92.
- Moreau, 122, 332, 573.
- Morgagni, 472.
- Morityel, 484.
- Morning sickness, 231.
- Morphological elements of semen, 310.
- Mortality of married men, 174.
- Mortality of married women, 218.
- Morton, 407, 466.
- Mosaic law, 129, 270.
- Moser, 438.
- Motherhood, dread of, 201.
- Mother’s supervision, 120.
- Moulin, 478.
- Maurange, 612.
- Mucus, alkaline cervical, 133.
- Mueller, 168, 233, 300, 320, 332, 475, 499, 528, 623.
- Mundé, 515, 612.
- Murmurs, systolic, 149.
- Murphy, 334.
- Museums, 120.
- Mussy, 292, 641.
- Myoma, 240.
- Naegele, 137.
- Nagel, 60.
- Napier, 161.
- Nathusius, 379.
- Natural frigidity, 172.
- Natural instincts, 120.
- Nausea, 107.
- Neefe, 438.
- Nega, 494.
- Negri, 17.
- 681Negroni, 474.
- Neisser, 537, 554.
- Nerves, 10.
- Nervous disturbances, 150, 161, 248.
- Nervous diseases, 243, 244, 637.
- Nervous irritability, 145.
- Nervous system, 99.
- Neudoerfer, 108.
- Neugebauer, 407, 528.
- Neumann, 245.
- Neuralgia, 151.
- Neurasthenia, 107.
- Neurasthenia, sexual, 123.
- Neuroses, 149, 225.
- Neusser, 17, 89.
- Nieden, 365.
- Nietsche, 202.
- Noble, 492.
- Noegerath, 512, 531, 534, 537.
- Noirot, 423.
- Noorden, 21, 90.
- Nordau, 399.
- Nothnagel, 113.
- Novels, 120.
- Nussbaum, 449, 474.
- Nutrition and genesis, 376.
- Nymphomania, 184.
- Obesity, 23, 92, 479, 636.
- Obermeier, 165.
- Obturator, 412.
- Ocular trouble, 108.
- Oceania, 43.
- Odebrecht, 119.
- Oehlschlaeger, 304.
- Oehlshausen, 249, 343, 474, 476, 509, 523, 537, 560.
- Oesterlen, 122, 331, 422.
- Official examination before marriage, 265.
- Old maids, 644.
- Olfactory sense, 109.
- Oligozoöspermia, 316.
- Onanism, 199, 404.
- Onanism, mechanical, 106.
- Onanism, mental, 106.
- Onanism, peripheral, 106.
- Onanism, psychical, 351.
- Only-child-sterility, 464.
- Oöphorectomy, 139, 475.
- Operative measures, 415.
- Oppenheimer, 538.
- Organ of hearing, 148.
- Organ of vision, 148.
- Ormerod, 494.
- Ostium uterinum tubæ, 56.
- Ott, 18, 20, 146.
- Otto, 328.
- Outer tunic, 59.
- Ovals, 413.
- Ovarian tenderness, 100.
- Ovaries, 216, 471, 473, 474.
- Ovaries, anatomical alterations, 583.
- Ovaries, atrophy of, 583.
- Ovaries, changes in, 8.
- Ovaries, diseases of, 489.
- Ovaries, extirpation of, 564.
- Overstrain, intellectual, 120.
- Ovid, 213.
- Ovulation, 136, 470.
- Ovum, discharge of, 136, 304, 306, 307.
- Owen, 393.
- Paget, 619.
- Pagliani, 46.
- Pajot, 293, 506, 527.
- Pajot-Négrier, 135.
- Palmay, 549.
- Palpitation, 46, 95, 97, 107.
- Panecki, 234.
- Papa, 194.
- Paranoia, 152.
- Paré, 285.
- Parent-Duchatelet, 81, 193, 477, 538.
- Parsons, 165.
- Pathological conditions in woman’s life, 599.
- Patriarchical relationship of woman, 5.
- Patru, 610.
- Pauli, 147.
- Péan, 182.
- Pelmann, 155.
- Pelvic viscera, 9.
- Penis captivus, 340.
- 682Percy, 314.
- Period of sexual pleasure, 350.
- Peripheral nerves, 16.
- Peristalsis, 107, 229.
- Perversion, sexual, 195, 360.
- Pessaries, 406, 411.
- Petiteau, 165.
- Peyer, 293.
- Pfaff, 190.
- Pfannenstiel, 59.
- Pfannkuch, 369, 559.
- Pfau, 498.
- Pflueger, 136, 475, 546.
- Philo-Indicus, 156.
- Physical disturbances, 153.
- Physical exercise, 113.
- Physician’s duty to enlighten girls, 125.
- Picture galleries, 120.
- Pigeolot, 407.
- Pigmentation, 161.
- Pincus, 419.
- Pisciculture, 458.
- Place, 393.
- Plato, 265, 391, 666.
- Pleasurable sensations, 177.
- Plenk, 333.
- Plicæ palmetæ, 296.
- Pliny, 185, 273, 463.
- Plon, 38, 46, 62, 81, 185, 214, 291, 308, 361, 416, 433, 446, 476, 545.
- Plutarch, 190, 302, 420.
- Plyette, 79, 165.
- Pollutions, 352.
- Polypus, 510, 590.
- Pomeroy, 276, 414.
- Porro’s operation, 567.
- Portio vaginalis, 503.
- Position, different modes of, 291.
- Potain, 150, 628.
- Potentia coeundi, 309.
- Potentia generandi, 309.
- Pouchet, 136.
- Power, 108.
- Pozzi, 343.
- Pregnancy, 139, 245, 247.
- Preventive measures, 255, 292, 388, 399, 410.
- Prévost, 7.
- Prima nox, 302.
- Primitive conditions of society, 5.
- Prior, 365.
- Prochownick, 559.
- Prochownik, 538.
- Profluvium seminis, 358.
- Prohibited degrees, 268.
- Pro-nucleus, female, 305.
- Pro-nucleus, male, 305.
- Prostitution, 195, 262.
- Pruritus, vaginal, 107.
- Pruritus, vulvæ, 107, 634.
- Pseudo-narcotism, 626, 638.
- Psychical influences, 17.
- Psychical manifestations, 18.
- Psycho-neuroses, 23.
- Psychopathia sexualis, 184, 257.
- Psychopathic states, 152.
- Psychoses, 155.
- Puberty, 37, 200.
- Pudendum, female, 204.
- Pudic nerve, 111, 348.
- Puech, 29, 109, 165, 182, 478, 597, 603.
- Pulse, 94, 96, 144.
- Pye-Smith, 100.
- Pyrosis, 107, 228.
- Quain, 166, 472, 494, 629.
- Quetelet, 366, 379.
- Rabba, 129.
- Rabbi Akita, 129.
- Rabbi d’Azai, 129.
- Rabbi José, 129.
- Rabbi Joshua, 266.
- Rabbinowicz, 129.
- Rabuteau, 18, 19.
- Race, 38.
- Rachitis, 117.
- Raciborski, 26, 122, 247, 258, 260, 268, 274, 399.
- Railway accidents, 84.
- Rape, 295.
- Raschi, 129.
- Ratgen, 165.
- Ratios between male and female births, 422.
- 683Ravn, 43.
- Rayer, 633.
- Recreation, domestic, 121.
- Reflex disturbances, 230.
- Regeneration, post-menstrual, 143.
- Regnier, 163.
- Regulation of sexual intercourse, 269.
- Reichert, 137.
- Reine, 18, 163.
- Relations of healthy and unhealthy female organs to other organs of the body, 25.
- Renaudin, 482, 494.
- Reproductive organs of girl of ten, 53.
- Reproductive organs of new born, 52.
- Reproductive organs of virgin, 55.
- Respiratory organs, 107, 146, 254.
- Rest cure, 113.
- Retching, 107.
- Retroflexion, 88, 230.
- Reuter-Gabriele, 201.
- Reyher, 414.
- Rheinstein, 143.
- Rhythmical variations, 20.
- Ribbing, 26, 122, 247, 258, 268, 274, 399.
- Ricardi, 194, 452.
- Richard, 265.
- Richarz, 451.
- Richter, 22.
- Ricord, 408.
- Riecke, 13.
- Riedel, 403, 544.
- Riese, 438.
- Rights of physical love, 203.
- Rights of women, 173.
- Ritschie, 482.
- Roberts, 564.
- Rochard, 466.
- Rodbertus, 393.
- Rodriguez, 480.
- Rodzewitsch, 365, 482.
- Roehrig, 15, 525.
- Rogival, 618.
- Rokitansky, 489, 494, 603.
- Romberg, 642.
- Roosevelt, 394.
- Rosen, 478.
- Rosenbach, 252.
- Rosenthal, 352.
- Rosenstadt, 180.
- Rosin, 116.
- Rossi, 109, 317, 332.
- Rosthorn, 12, 214, 492.
- Roth, 211, 452.
- Roubaud, 287, 289, 362.
- Rouget, 296.
- Rousseau, 103, 124, 213.
- Routh, 181.
- Rouvier, 42.
- Rueder, 612.
- Ruettel, 364.
- Rugæ, 216.
- Ruge, 475, 522.
- Runge, 121, 176, 221, 261.
- Rush, 365.
- Russ, 100.
- Rut, 136, 139.
- Sacher-Masoch, 193.
- Sacrache, 46.
- Sadism, 194.
- Sadler, 366, 369, 377, 422, 430.
- Saenger, 119, 396, 492, 512, 537.
- Saexinger, 494, 616.
- St. Hilaire, 434.
- St. Prospêre, 171.
- Salmon, 21.
- Sand, 262.
- Sappho, 190.
- Satschoma, 499.
- Scanzoni, 72, 275, 326, 474, 517, 523, 597, 604, 616, 619.
- Schaefer, 155.
- Schatz, 475.
- Schauenstein, 191.
- Schauta, 144, 147, 162, 245, 260, 490.
- Schenk, 458, 486.
- Schichareff, 18, 20.
- Schiller, 271.
- Schlager, 154, 645, 653.
- Schlesinger, 141.
- Schmalfuss, 166, 182.
- 684Schmidt, 29, 365.
- Schnürleber, 122.
- Schnurthorax, 90.
- Schoeltz, 116.
- Schoenfeld, 330.
- Schönlein, 108.
- Schopenhaur, 168, 202.
- Schorler, 559.
- Schottlaender, 60.
- Schrader, 19, 126, 146.
- Shreiner, 312.
- Schroeder, 155, 341, 521, 525, 538, 564.
- Schubert, 116.
- Schüle, 153, 186, 653.
- Schuermayer, 197.
- Schultze, 210, 448, 556.
- Schwartz, 536.
- Schwing, 147, 365.
- Scott, 614.
- Scrofula, 117, 484.
- Seaside, 117.
- Seasonal variations, 180.
- Seborrhœa, 110, 118.
- Sebum, 110, 118.
- Sée, 100.
- Seeligmann, 165, 466, 535.
- Segmentation sphere, 306.
- Seiler, 92.
- Self-deception, 574.
- Semper, 450.
- Senator, 146.
- Senescence, 572.
- Sensation of fulness in hypogastric region, 46.
- Senses, organs of, 108, 145, 250.
- Sensibility, sexual, in women, 542.
- Sergi, 170.
- Sex combination, 427.
- Sex relations, 35.
- Sex, third, 201.
- Sexual abuses, 258.
- Sexual impulse, 179.
- Sexual life, central perceptions of, 177.
- Sexual life, development of, 176.
- Sexual needs, 33.
- Sexual neurasthenia, 199.
- Sexual satisfaction, 177.
- Shakespeare, 277.
- Sheldon, 612.
- Sheltered life, 212.
- Sickel, 438.
- Signs, prodromal, 129.
- Siebold, 438.
- Simon, 130, 527.
- Simpson, 218, 465, 487, 603, 618.
- Sims, 297, 314, 318, 365, 466, 513, 521.
- Sinéty, 141.
- Sintemma, 136.
- Skene, 612.
- Skin, diseases of, 146, 632.
- Skin, eruptions of, 146.
- Skopstki, 184.
- Slavjansky, 473.
- Sleep, 115.
- Sloan, 108.
- Smegma, 51, 529.
- Soaps, 118.
- Social circumstances, 599.
- Social significance of sexual life, 33.
- Socrates, 269.
- Sodomy, 190.
- Solanieff, 556.
- Solon, 269, 273.
- Sommerus, 482.
- Song of Solomon, 23.
- Soranus, 308, 381, 420, 463, 502.
- Spaeth, 438.
- Spallanzani, 317.
- Spartan custom, 272.
- Spasms, clonic, 102.
- Spasms, tonic, 102.
- Spencer Wells, 182, 376, 466, 485.
- Spermatozoa, 304, 306, 310.
- Spiegelberg, 475, 515, 560.
- Spietschka, 110, 118, 209.
- Stadion, 193.
- Staël, 3.
- Stark, 482.
- Starkweather, 451.
- Stays, tight, 97.
- Steatopyga, 573.
- Steglehner, 528.
- Stein, 202.
- Steinbow, 203.
- 685Steiner, 100.
- Stenokardia, 98.
- Stepanow, 109.
- Stephenson, 85.
- Sterility, absolute, 540, 569.
- Sterility, artificial, 413, 462, 464, 468, 484.
- Sterility, one-child, 561.
- Sterility, operative, 563.
- Sterility, relative, 540, 569.
- Sterility, varieties of, 470, 569, 570.
- Stevens, 522.
- Stieda, 91, 384.
- Stiehl, 124.
- Stille, 406.
- Stiller, 147.
- Stimulation, local, 237.
- Stimulation, mechanical, 15.
- Stimulation, thermic, 15.
- Stomach, ulcer of, 107.
- Storer, 414.
- Strabo, 415, 564.
- Strahan, 386.
- Strassmann, 16, 138, 140, 143, 241.
- Stratz, 24, 212.
- Striæ, 209.
- Strindberg, 206.
- Strogamoff, 593.
- Sudden frights, 84.
- Suesserot, 525.
- Suicide, 174.
- Suppression of menses, 158.
- Susruta, 48, 129, 307, 420, 463.
- Swieten, 333.
- Swift, 441.
- Sympathetic action, 549.
- Sympathetic nervous system, 237.
- Syncope, 150.
- Synkits, 482.
- Szukits, 28, 131, 134.
- Tachycardia, 23, 345.
- Tairi, 407.
- Talmud, 129, 276, 292, 294, 307.
- Talquist, 365, 383.
- Tardieu, 190, 195.
- Tarnowskaja, 382.
- Tarnowsky, 262.
- Tassenbroek, 142.
- Taste, acid, 107.
- Taste, pasty, 107.
- Taste, perverse, 107.
- Tauffer, 166, 496, 499.
- Taxil, 192.
- Taylor, 364, 482.
- Tea, 121.
- Tenderness of breasts, 46.
- Tetany, 247.
- Theaters, 120.
- Theilhaber, 235, 609.
- Theopold, 543.
- Thiery, 452.
- Thomas, 413.
- Thompson, 334, 404, 406.
- Thorn, 602.
- Thyroid, 108.
- Tilt, 29, 31, 43, 135, 518, 582, 594, 600, 626, 629, 631, 634, 666.
- Timan, 325.
- Tissier, 183.
- Tissot, 102.
- Toldt, 215.
- Tolstoi, 34, 206, 397, 401.
- Tonsils, hypertrophy of, 107.
- Touchon, 453.
- Tousenel, 443.
- Towels, sanitary, 125.
- Towers-Smith, 480.
- Traugott, 116.
- Travels, 121.
- Tribadism, 190.
- Troggler, 187.
- Troubles, domestic, 219.
- Tschowuloff, 382.
- Tuberculosis, 259.
- Tuke, 155.
- Tumors of rectum, 334.
- Tunica propria, 60.
- Tussenbeck, 235.
- Two-children-system, 384.
- Tyler-Smith, 522.
- Ultzmann, 287, 312.
- Uncle, 194.
- Underwear, 122.
- Undulatory movement, 18.
- 686Uneasy sensations, 46.
- Unhappy marriages, 190.
- Union of Social Harmony, 393.
- Upbringing, domestic, 120.
- Upjohn, 449.
- Urinary organs, 146.
- Urine, retention of, 126.
- Urnings, 197.
- Uterine annexa, 566.
- Uteromania, 184.
- Uterus, 91, 214, 297, 494, 499, 500, 515, 523, 558, 590, 614, 617.
- Vacher, 383.
- Vagina, 216, 526.
- Vaginal stricture, 346.
- Vaginismus, 335, 337, 341, 345.
- Vaginodynia, 343.
- Valenta, 406.
- Varge, 333.
- Vascular system, 13.
- Vasomotor disturbances, 104, 151.
- Vedeler, 521.
- Veins, 13.
- Veit, 60, 87, 308, 327, 342.
- Velpeau, 619.
- Venus apparatus, 412.
- Venus powder, 412.
- Vera, 35.
- Veraism, 263.
- Vertigo, 46, 154.
- Viault, 118.
- Villermé, 377, 379.
- Viraginity, 190.
- Virchow, 86, 91, 208, 379, 489.
- Virey, 132, 328, 545, 595.
- Virginity, moral, 123.
- Visceral neuralgia, 640.
- Vitreous body, 108.
- Vogel, 130.
- Voigt, 165.
- Voltaire, 285.
- Voluptuous sensations, 203.
- Vomiting, 107, 230.
- Vorst, 394.
- Vulva, 526.
- Wald, 191.
- Waldeyer, 58, 60, 605.
- Wallace, 400.
- Walter, 607.
- Wappaeus, 379, 423, 435.
- Waterbrash, 228.
- Waters, natural, 116.
- Waters, mineral, 116.
- Watson, 165.
- Weakly women, 28.
- Weight at age of puberty, 47.
- Weinbrunn, 332.
- Weinhold, 416.
- Weiss, 333.
- Wendeler, 591.
- Werne, 416.
- Wernich, 296.
- West, 474, 525.
- Westphal, 142, 158, 189, 195.
- Weybsbart, 210.
- Whitehead, 369.
- Wilhelm, 147.
- Wilkins, 445.
- Willbraud, 193.
- Wille, 157, 407.
- Williams, 137.
- Wilson, 635.
- Windmueller, 165.
- Windscheid, 150, 243, 247, 627, 640, 642.
- Winkel, 128, 342, 474, 509, 523, 527, 558.
- Winter, 84.
- Winterhalter, 138.
- Withrow, 165.
- Woman, influence of, 206.
- Women writers, 34.
- Wyder, 304, 332.
- Yamagiron, 217.
- Young, 482.
- Zarathustra, 202.
- Zeis, 331.
- Zeissl, 478, 535.
- Ziehl, 496.
- Ziemssen, 526.
- Zola, 193.
- Zoroaster, 269.
- Zunaikornustax, 210.
- Zweifel, 72, 528.
Changes made to medical terms, proper names, or foreign words. Does not include the index which was always corrected to agree with the text. In case of multiple changes only the first is listed:
| Page |
Original Text |
Changed Text |
| vii etc. |
Amenorrhoea |
Amenorrhœa |
| vii etc. |
Dysmenorrhoea |
Dysmenorrhœa |
| vii |
Anaesthesia |
Anæsthesia |
| x |
Asterahanthion |
Asterakanthion |
| x etc. |
Oligozoospermia |
Oligozoöspermia |
| x |
Uteras |
Uterus |
| 2 |
climateric |
climacteric |
| 3 |
coëxtensive |
coextensive |
| 8 |
manfestations |
manifestations |
| 13 |
hæmorrhoidal |
haemorrhoidal |
| 23 |
chorosis |
chlorosis |
| 39 |
Roberton |
Robertson |
| 55 |
Fraenum |
Frænum |
| 55 etc. |
Nymphae |
Nymphæ |
| 60 |
dentoplasm |
deutoplasm |
| 71 etc. |
Carunculae |
Carunculæ |
| 73 |
primæ |
primae |
| 78 etc. |
Præcox |
Praecox |
| 95 etc. |
amenorrhœic |
amenorrhoeic |
| 96 |
venticle |
ventricle |
| 98 |
teleangiectasis |
telangiectases |
| 99 |
patients complain |
patients who complain |
| 104 |
phychosis |
psychosis |
| 105 |
sexual |
sexually |
| 110 |
suderiferous |
sudoriferous |
| 116 |
hæmaglobin |
hæmoglobin |
| 119 |
Sænger |
Saenger |
| 128 etc. |
hyperæmic |
hyperaemic |
| 138 |
Strassman |
Strassmann |
| 148 |
chloasmia |
chloasma |
| 148 |
meatas |
meatus |
| 154 |
organism in predisposed |
organism is predisposed |
| 166 |
larnyx |
larynx |
| 194 |
Riccardi |
Ricardi |
| 207 |
overy |
ovary |
| 209 |
Spietshka |
Spietschka |
| 211 etc. |
Rothe |
Roth |
| 212 etc. |
uretha |
urethra |
| 215 etc. |
nulliparæ |
nulliparae |
| 220 |
organims |
organisms |
| 222 |
teleangiectases |
telangiectases |
| 222 |
splanchoptosis |
splanchnoptosis |
| 223 |
vulvular |
valvular |
| 240 |
hysterica |
hysteria |
| 240 |
hæmorhages |
hæmorrhages |
| 241 |
hyperæmias |
hyperaemias |
| 260 |
Rozières |
Rosières |
| 280 |
hygenic |
hygienic |
| 291 |
constictor |
constrictor |
| 291 |
ishiocavernosus |
ischiocavernosus |
| 291 |
Zanibar |
Zanzibar |
| 299 |
Hausmann |
Haussmann |
| 303 etc. |
aesthetic |
æsthetic |
| 303 etc. |
hetairae |
hetairæ |
| 303 etc. |
mediaeval |
mediæval |
| 306 |
mezalocephala |
megalocephala |
| 306 |
Nusbaum |
Nussbaum |
| 310 |
laminae |
laminæ |
| 310 |
speramatozoa |
spermatozoa |
| 314 |
spematozoa |
spermatozoa |
| 315 etc. |
azoöspermia |
azoospermia |
| 316 |
blenorrhœa |
blennorrhœa |
| 326 |
Brille |
Brill |
| 327 |
fistulae |
fistulæ |
| 332 |
foetaltal |
foetal |
| 334 |
cyctocele |
cystocele |
| 339 |
urethal |
urethral |
| 339 |
hymenal |
hymeneal |
| 339 |
kolpitis |
colpitis |
| 354 |
lupulin 0.5 (¾ grain) |
lupulin 0.05 (¾ grain) |
| 365 |
Rodsewitsch |
Rodzewitsch |
| 383 |
Tallquist |
Talquist |
| 396 |
Sänger |
Saenger |
| 404 |
cartarrhal |
catarrhal |
| 412 |
vaginia |
vagina |
| 414 |
Pomerey |
Pomeroy |
| 418 |
Arendt |
Arndt |
| 456 |
infusioria |
infusoria |
| 456 |
acquaria |
aquaria |
| 470 etc. |
anaemia |
anæmia |
| 472 |
climateric |
climacteric |
| 472 |
lupinars |
lupanars |
| 477 |
perenchymatous |
parenchymatous |
| 488 |
haematokolpos |
haematocolpos |
| 492 |
catarrahal |
catarrhal |
| 494 |
Güsserow |
Gusserow |
| 494 |
Renauldin |
Renaudin |
| 495 |
lacunae |
lacunæ |
| 496 |
columnae |
columnæ |
| 496 |
labiae |
labiæ |
| 499 |
dysmenorrhoeic |
dysmenorrhœic |
| 500 |
dysmenorrhoeal |
dysmenorrhœal |
| 502 |
tincae |
tincæ |
| 511 |
Hildebrandt |
Hildebrand |
| 513 |
Germany is believing |
Germany in believing |
| 515 |
blenorrhagia |
blennorrhagia |
| 516 |
parameterium |
parametrium |
| 524 |
hyperaesthetic |
hyperæsthetic |
| 529 etc. |
papillae |
papillæ |
| 539 |
avortment |
avortent |
| 539 |
sout |
sont |
| 539 |
conjuctival |
conjunctival |
| 540 |
urethae |
urethrae |
| 541 |
hyspospadias |
hypospadias |
| 541 |
hvpospadiac |
hypospadiac |
| 544 etc. |
anaemic |
anæmic |
| 549 |
dysmenorrhoeal |
dysmenorrhœal |
| 559 |
Pfankuch |
Pfannkuch |
| 564 |
overian |
ovarian |
| 580 |
mucuous |
mucous |
| 603 |
physionognomy |
physiognomy |
| 612 |
Munde |
Mundé |
| 631 |
Haematemesis |
Hæmatemesis |
| 633 |
seborrhoeic |
seborrhœic |
| 648 |
the casual agent |
the causal agent |
| 650 |
paroxyms |
paroxysms |
| 654 |
oesophagus |
œsophagus |
| 658 |
defaecation |
defæcation |
- Silently corrected typographical errors and variations in spelling.
- Archaic, non-standard, and uncertain spellings retained as printed.
- There are references to temperatures in Rankine units. I doubt this would be
meaningful when referring to human temperatures but I did not alter them.
- Footnotes were re-indexed using numbers and collected together at the end of the last
chapter.


